ENGLISH-NEW MIDWIFERY GNM TY UNIT 3 EMBRYOLOGY AND FETAL DEVELOPMENT
EMBRYOLOGY AND FETAL DEVELOPMENT:-
A) Oogenesis:-
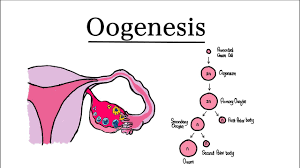
- Oogenesis is the process in which the development of a mature ovum (female reproductive cell) takes place.
- Oogenesis is the process that starts during the development of the embryo.
- When the embryo develops in a pregnant woman, the primordial Germ cells develop.
- In the female gonads, germ cells undergo rapid mitotic division( A type of division in which two daughter cells with the same number and type of chromosomes are obtained by division of the parent cell.) and then convert into oogonia.
- The majority of these oogonia divide continuously. Some of them enter the prophase of the first meiotic division and are called primary oocytes. They are covered by flat cells called primordial follicles which are present in the cortex of the ovary.
- At birth, there is no meiotic division and all the oogonia that have completed the prophase of the first meiotic division are replaced by primary oocytes which remain in the resting stage (dictyotene stage:- a stage between prophase and metaphase.)
- The total number of primary oocytes at birth is estimated to be about 2 million.
- Until Primary oocytes do not complete the first meiotic division until puberty. At puberty, about 40,000 primary oocytes are left behind, the rest are atretic. Of these, about 400 are ovulated during the entire reproductive period.
- Then, the oocytes mature. Now, the number of chromosomes is reduced to half.
- Before the start of the first meiotic division, the primary oocyte doubles its DNA through replication, so it has double the amount of normal protein content.
- It contains 22 pairs of autosomes that determine the characteristics of the body and one pair is the sex chromosomes such as XX.
- The first stage of maturation occurs with the full maturation of the ovarian follicles before ovulation. And final maturation occurs only after fertilization.
- Then, the primary oocyte undergoes the first meiotic division which gives rise to a secondary oocyte and a polar body. Both are of unequal size. The secondary oocyte has a haploid number of chromosomes (23, X) but almost all of the cytoplasm and the polar body also has half the number of chromosomes (23, X) but with less cytoplasm.
- Ovulation occurs immediately after the formation of the secondary oocyte.
- The secondary oocyte completes the second meiotic division (homotypical) only after fertilization by sperm in the fallopian tube.
This results in the formation of two unequal cells, each with 23 chromosomes (23 X), one larger, called the mature ovum, and one smaller. Which is called the second polar body. - In the absence of fertilization, secondary oocytes do not complete the second meiotic division and degenerate.
•>Chat Presentation of Oogenesis:-

Oogenesis
↓
Germ cells
↓
Mitosis
↓
Oogonia
(Oogonia)
↓
Primary Oocytes( 46 , XX)
↓
Arrested first meiotic division (up to puberty)
↓
Maturation of Graafian follicle
↓
Completion of first meiotic division
↓
——————————– ↓ ↓
Secondary
Oocytes
(23, X) and 1 st polar body
( 23,X )
↓
Ovulation
↓
↓ ↓
Not Fertilized
↓ Complete
Digestion Second
Within Meiotic
24 Division
Hours ↓
————————-
Fertilized
↓ ↓
Female Second
Pronucleus Polar
(23,x) Body End
( 23,x) Spermatogenesis
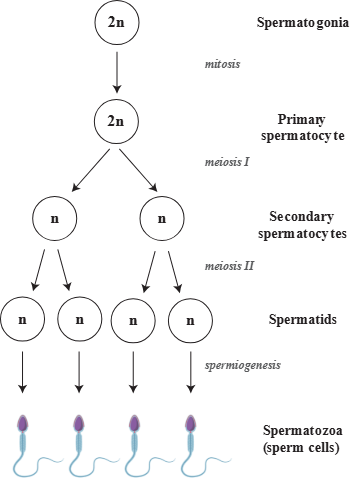
(B)spermatogenesis:-
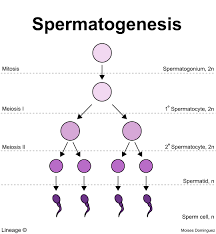
“The development of spermatids from primordial male germ cells and their subsequent differentiation into spermatozoa is called spermatogenesis. That is, the development and maturation of sperm is called spermatogenesis.”
- Before puberty, primordial germ cells are Spermatogonia develop through the process of mitosis and then reside in the seminiferous tubules.
- The spermatogonia then differentiate into primary spermatocytes (46,XY / diploid) through the process of mitosis. Which remains in the prophase of the first meiotic division for a long time.
- Each spermatocyte contains 22 pairs of autosomes and one pair of sex chromosomes such as XY.
- With the completion of the first meiotic division, two secondary spermatocytes (haploid) are formed. And it has an equal number of cytoplasm and a haploid number of chromosomes, such as,
23 X, or 23 Y. - Immediately after the second meiotic division, four spermatids (without tail sperm cells) are formed. It contains haploid number of chromosomes i.e.,
two 23 X, two 23 Y. - After the formation of spermatids, morphological changes occur without further cell division, which convert them into spermatozoa.
This process is called spermatogenesis. - In males, it takes about 61 days for mature spermatozoa to develop from spermatogonium.
•> Chart presentation of spermatogensis:-
Spermatogenesis
↓
Germ Cell
↓Mitosis
Primary spermatocyte
( 46, XY )
↓
First meiotic
division
↓
Secondary spermatocytes
↓
‐‐—————-
↓ ↓
23,X 23,Y
| |
—————————-
↓
—————————–
↓ ↓ ↓ ↓
23, 23, 23 23
X X Y Y
\ | | /
↓
Spermatids
↓
Morphological Changes
to Spermatozoa (Spermatogenesis)
(c)Ovulation:
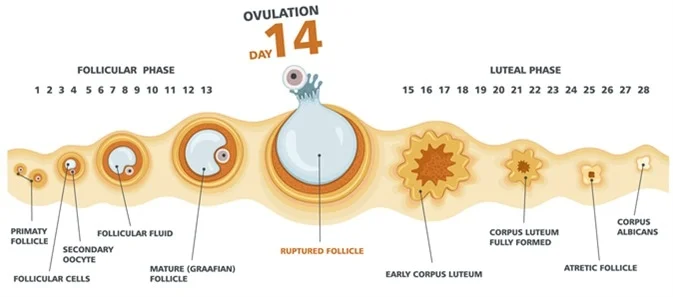
- Ovulation is the process of release of secondary oocytes from a mature Graafian follicle. Ovulation is called.
- The process of development and release of a mature ovum is called ovulation.
- Usually a woman has a menstrual cycle of 28 days and ovulation usually occurs in the mid-period of the menstrual cycle. That is, ovulation occurs on the 14th day.
- This process of ovulation starts during menarche, that is, the woman’s first menstrual cycle, and this process ends with menopause period. Stops. That is, the process of ovulation lasts from menarche to menopause.
- Usually only one secondary Oocyte is released from one ovary.
(D)Gametogenesis :
- The maturation of two specialized cells, spermatozoa in males and ovum in females, before they form a unit called zygote, is called gametogenesis.
•>(Ovem) Ovem:
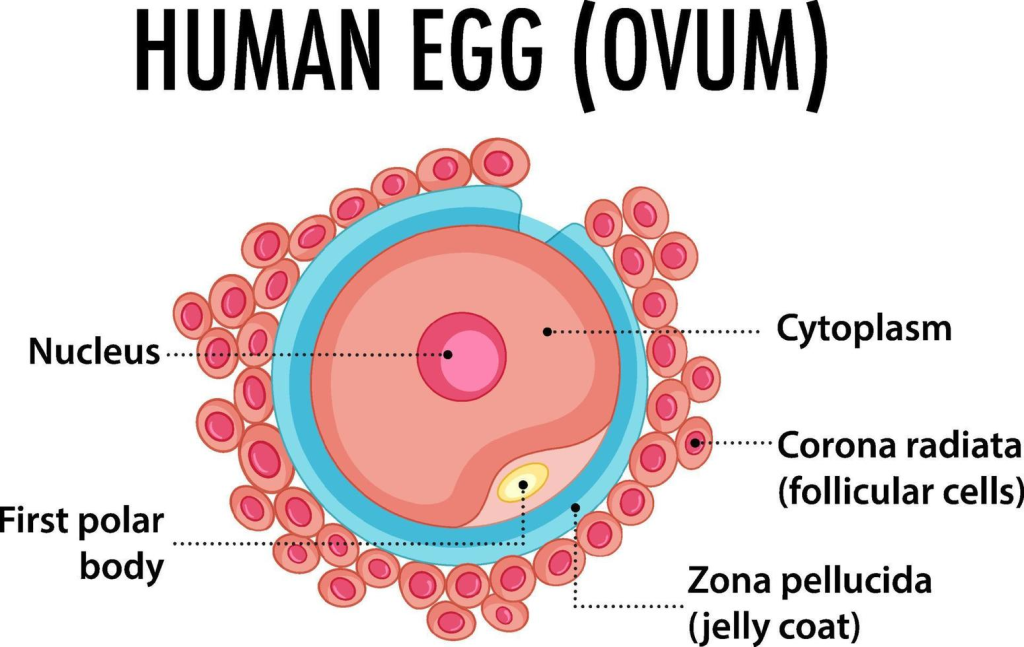
- The ovum is the largest cell in the female body and the smallest cell is the platelet cell.
- The size of the ovum is 120-150 μm.
- The lifespan of the ovum is 12 to 24 hours.
- The formation of the ovum takes place in 6-8 days.
- Ovum ma, nucleus, cytoplasm, first polar body, zona pellucida (hyaluronic acid), corona radiata …. are present.
•>(Sperm) Sperm:
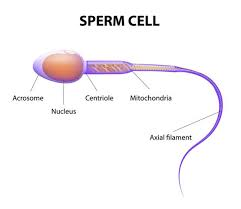
- Sperm is the smallest cell of the male body.
- The largest cell in the male is the neuron.
- The size of sperm is about 50 μm.
- Its life span is 48 to 72 hours. The formation time of sperm is about 61 days.
- Parts of sperm
- Head,
-nucleus,
-acrosomes (hyaluronic enzyme),
-neck,
-middle part which contains mitochondria (power house),
-and also a tail part.
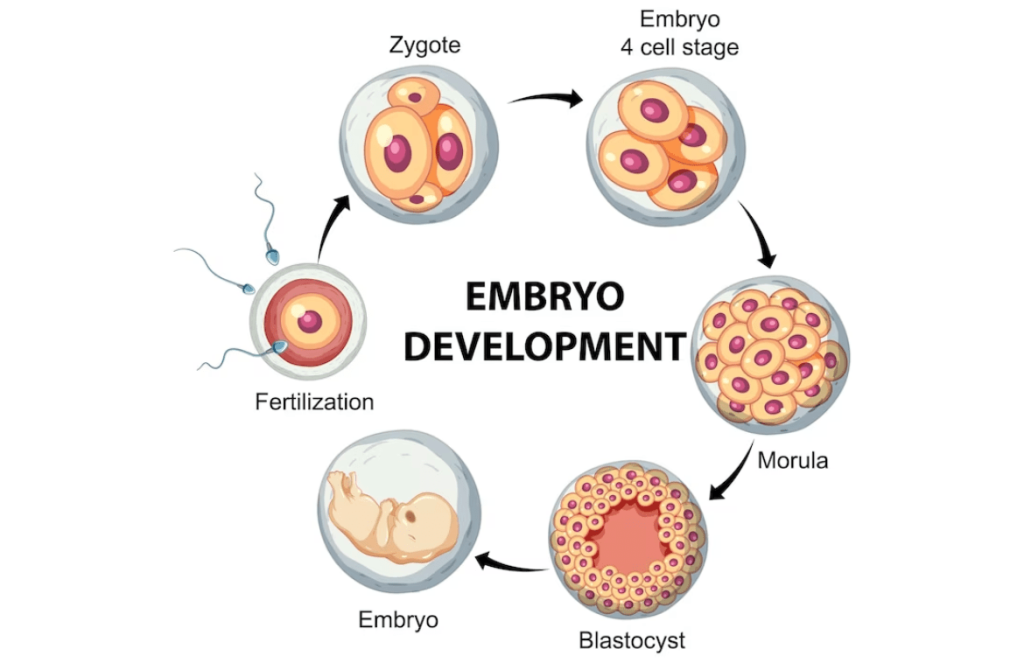
Fertilization :

- Fertilization is the process in which the male reproductive cell spermatozoa fuses with the female reproductive cell ovum in the ampulla part of the fallopian tube and fertilization occurs, which results in the formation of a zygote. Fertilization mostly occurs around the time of ovulation.
- The ovum is released from the ovary of the female reproductive system and this mature ovum is captured by the fimbriae of the fallopian tube. The ovum is then transported to the ampulla part of the fallopian tube by the peristalsis movement of the fallopian tube and the ciliary muscles present in it. And it lasts for 12 to 24 hours.
- During this time, the cervix secretes alkaline mucus due to the effect of estrogen which attracts sperm. During intercourse, 60 to 120 million sperm are deposited in the posterior fornix of the vagina.
- Many of these sperm enter the fallopian tube due to cervical action and their propelling action, while the remaining sperm are destroyed due to the acidic medium of the vagina.
- If ovulation has not occurred, the sperm cells It can survive in the cervix for 48 to 72 hours.
These sperm cells are transported from the cervical area and transferred to the fallopian tube. During this journey, many sperm cells are destroyed and only a thousand sperm reach the fallopian tube and meet the ovum in the ampulla.
When the sperm reaches the ovum, the sperm has to form its own environment. That is, the sperm needs an alkaline environment. And if there is an acidic environment, then the sperm is destroyed.
But, the external environment of the ovum is acidic due to hyaluronic acid.
Now, to convert this acidic environment into an alkaline environment, there is an acrosome layer on the head of the sperm, which contains hyaluronic enzyme which has an alkaline environment. It is secreted around the ovum.
Thus, the hyaluronic enzyme released from thousands of sperms at once destroys the corona radiata (outer layer of the ovum). Then the zona pellucida layer becomes soft so that the sperm can penetrate the zona pellucida and enter the ovum.
There are olema on all four sides of the zona pellucida. But only one sperm can enter an egg.
The most mature and developed sperm penetrates the zona pellucida layer.
Then the zona pellucida layer hardens. This is called zona hardening.
Cortical granules are deposited to fill the olema penetrated by the sperm and fill the penetrated area. After that, the ovum is sealed. Due to which other sperm cannot enter, and the sperm The tail remains outside. - Now, the fusion of the sperm and the nucleus of the ovum that has entered the ovum is called fertilization and then this fertilization results in the formation of a zygote.
Implantation (Implantation) :
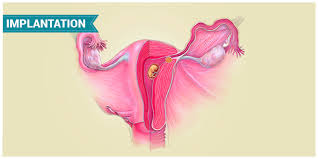
- Implantation is the process in which the zygote from the fallopian tube attaches to the endometrium of the uterine cavity to develop.
The process of implantation starts 4 to 5 days after the formation of the zygote and is completed by 11 days.
After the formation of the zygote, the zygote remains in the fallopian tube for four days and then it is implanted in the uterine cavity. During these four days, cell division occurs and the intrauterine wall also develops, which provides a proper environment for the development of the implanted egg. - The zygote with 46 chromosomes, covered by the zona pellucida, undergoes the first mitotic cell division within 24-30 hours by cleavage into a 2-cell stage called a blastomere.
- After the formation of the zygote, within 40 to 50 hours, it undergoes a four-cell division from a two-cell division.
Then within 72 hours of the formation of the zygote, from a four-cell division 8 cell divisions occur.
Then 16 cell divisions occur within 96 hours of zygote formation. In this, after cell A divides, a bunch-like structure is formed, which is called morula. This morula is covered by the zona pellucida layer.
All these stages are completed in four days, i.e. implantation starts from the 5th day and is completed by the 11th day.
During these four days, cell division takes place and along with this, the endometrium layer of the uterus also develops, due to which the implanted egg can get a properly favorable environment for its growth and development.
After the formation of the zygote, the zygote remains in the fallopian tube for four days, after which the journey of the zygote starts on the 4th to 5th day and reaches the uterus by the 11th day. - After the formulation of the morula, fluid in its cells The collection of cells also enlarges the size of the cell, which is called a blastocyst.
After the formation of the blastocyst, all the cells form their own individual mucus covering.
Now when each cell forms its own individual mucus covering, the zona pellucida layer starts to disappear, this process is called zonahatching.
Now after the zona pellucida layer of the blastocyst disappears, some cells of the blastocyst form the outer layer and some cells collect at a site inside the outer layer. - Therefore, the outer cell layer is called the outer cell mass and the outer The collection of cells collected at a site within the cell layer is called the inner cell mass.
The single layer of cells on the outside of the inner cell mass is called the trophoblast. - When the blastocyst enters the uterus, it remains free for two to three days. After that, part of the trophoblast remains on the inner cell mass. Then it sticks to the endometrium as a sticky substance. Then it secretes enzymes that cause the epithelium there to be eaten away. Due to this, the blastocyst implants in the endometrium, which is also called nesting (embedding), which is usually completed on the 11th day after fertilization.
- Implantation usually occurs in the posterior uterine wall but sometimes in the anterior wall of the fundus.
- The placenta and chorion form from the outer trophoblast, and the fetus, amnion, and umbilical cord form from the inner cell mass.
- Post-implantation changes in the uterus
Decidua :
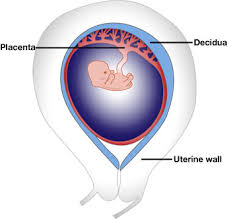
- In pregnancy, the endometrium is called decidua.
- It thickens 4 times due to increased secretion of estrogen and the size of blood vessels increases due to progesterone. It becomes a soft, vascular and spongy bed in which the fertilized ovum implants. After birth, the decidua is shed except for the zona basalis.
The Latin word decidua means falling off.
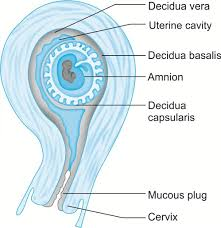
Area of Decidua:
There are three areas of the decidua.
1) Decidua basalis:
- The lower implantation site of the embryo is called the decidua basalis. Which is immediately above the myometrium. Which remains unchanged. It contributes to the placenta.
- In the peritoneum, it forms the neoendometrium.
2) Decidua capsularis:
- The superficial layer covering the rest of the embryo is called the decidua capsularis.
- During fetal growth, the decidua capsularis arises and merges with the decidua parietalis.
3) Decidua
Parietalis or Decidua Vera:
The lining of the decidua in the uterine cavity is called the decidua vera.
Layers of Decidua :
There are three layers of decidua.
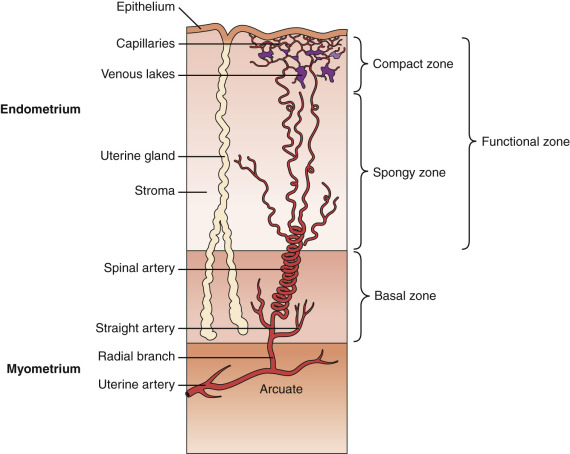
1)(Basal Layer) Basal Layer:
- This layer lies immediately above the uterine muscles. It is formed from the base of the endometrial glands and does not change. When the placenta separates, the base of the gland remains and a new endometrium is formed from it.
2)(Spongy Layer ) Spongy Layer:
- This spongy layer lies above the basal layer. It contains dilated glands and enlarged blood vessels.
- The chorionic villi invade this layer to form the placenta. A fibrous layer forms in the deep part of this layer. It is called the perforation layer or layer of Nitabuch. From this point the placenta separates from the uterine wall.
3) (Compect Layer ) Compact Layer:
- This is the surface layer of the decidua. It is located near the cavity where the neck of the glands is attached to the decidual cells.
- The decidual cells are large and contain glycogen.
(Function Of Decidua) Function Of Decidua:
- Provides a good place for the implantation of the blastocyst.
- Provides nutrition to the ovum in the early stages.
- Prevents deep penetration of the trophoblast.
- Contributes to the formation of the basal plate of the placenta.
(Development of Fertilized Ovum) Development of Fertilized Ovum:
- After the blastocyte is embedded in the endometrium, a layer is formed on the area of the outer trophoblast.
- Then three layers are formed.
1)Outer Syncytiotrophoblast (syncytium):
- Syncytiotrophoblast erodes the walls of blood vessels. And the maternal blood provides nutrients for the embryo to develop.
2) Inner cytotrophoblast:
The cytotrophoblast is a single layer of cells. Produces human chorionic gonadotropin (HCG). Which informs the corpus luteum that pregnancy is occurring.
The corpus luteum continuously produces estrogen and progesterone.
Progesterone thickens the decidua. Therefore, menstruation does not occur. High levels of estrogen do not produce FSH.
3)Primitive mesenchyme or mesoderm:
The third layer, mesoderm, with its membranous layer, forms the chorionic vesicles. The developing embryo is called the chorion. It forms the body stalk and the umbilical cord. The chorion is then connected to the embryo.
•> Finger-like buds of the trophoblast form on the outer surface of the embedded blastocyte. This is called chorionic villi.
The types of chorionic villi are as follows.
1)Primary villi:
A solid trophoblastic layer is formed on the 12th day of fertilization.
2) Secondary villi:
A mesenchymal lining is formed with villi on the 16th day.
3) Tertiary fusion:
Blood vessels are formed on the 21st day with secondary fusion.
The branches of the villi on the side of the uterine wall form the chorion frondosum to form the placenta. The villi on the side of the uterine cavity atrophy and the chorion disintegrates.
The placenta and chorion form from the trophoblast while the inner cell mass forms from the placenta.
Which has three layers:
Which has three layers:
1)Ectoderm
2)Mesoderm
3)Endoderm
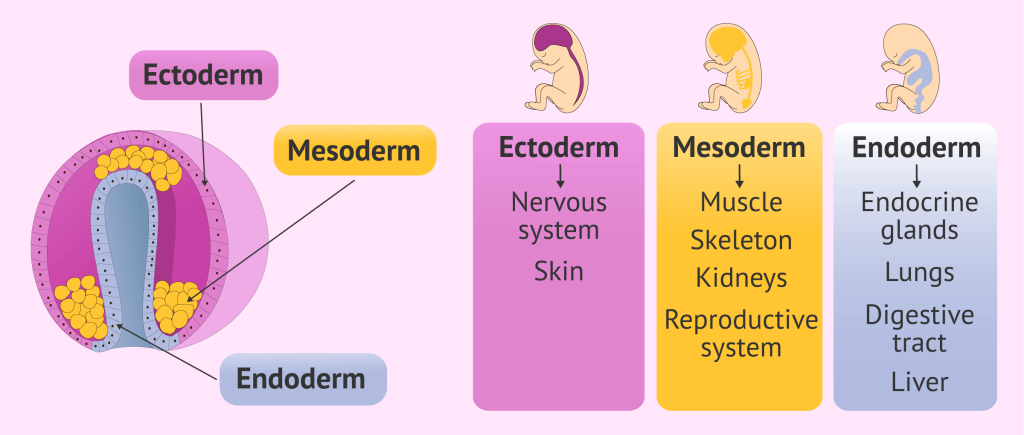
1) Ectoderm:
- The nervous system and skin are formed from ectoderm.
2) Mesoderm:
- The heart, blood vessels, liver, pancreas, bones, muscles and some internal organs are formed from the mesoderm.
3) Endoderm:
- The mucus membrane and glands are formed from the endoderm.
(Embryo) Embryo:
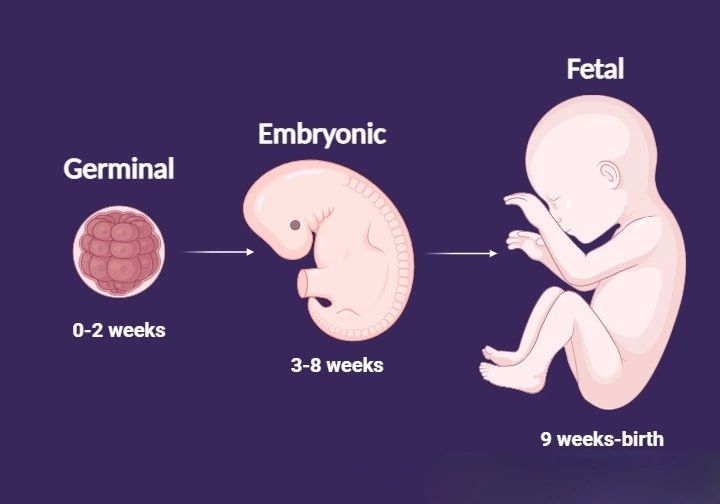
This is the stage of organ development. The offspring that develops up to 8 weeks after implantation is called an embryo. The offspring from 8 weeks to term is called a fetus.
A fertilized egg goes through three stages of development by the time it is born.
1) The stage of zygote (before Implantation)
2)The Stage of Embryo (Early in Pregnancy)
3)The Stage of Fetus (Later in Pregnancy)
- The growing organism from the 2nd to the 8th week is called an embryo.
- During this period, it grows from a tiny cell cluster to about 1 inch in length. During this time, the placenta develops between the embryo and the uterus.
- The embryo is connected to the placenta by the umbilical cord.
- The placenta acts as a filter and barrier. Through it, the embryo takes in food and oxygen from the woman’s blood and removes CO2 and other waste products. These two blood systems are completely separate.
- Humans in the 1st Month of Life The embryo is like any other animal but in the 2nd month it takes on human features. The face, eyes, legs, fingers, toes and sexual organs are undifferentiated (same for male and female).
- When it is clearly identified as human, it leaves the embryo stage and enters the fetus stage.
(Post-fertilization events) Post-fertilization events:
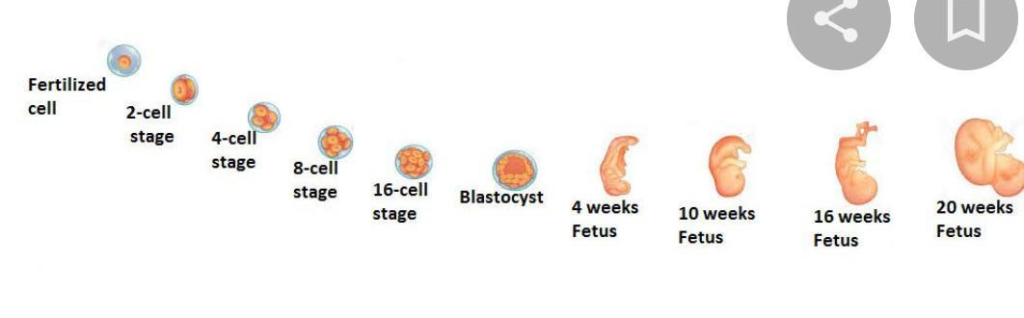
- 0 Hour-> Fertilization,
- 24 Hours -> 2 Cell Stage of Zygote (Blastomere),
- 42 Hours -> 4 Cell Stage of Zygote,
- 72 Hours-> 12 Cell Stage of Zygote,
- 96 Hours-> 16 cell stage. Morula enters the uterine cavity.
- 5th day-> Blastocyst.
- 7th day-> Implantation.
- 11th day-> Implantation is complete.
- 12th day-> Primary villi.
- 16th day-> Secondary Wilt.
- 21 St Day -> Tertiary Wilt.
- 21-22nd Day-> Fetal Heart, Feto Placental Circulation.
- 21- 40 Day -> Chorion Frondosum.
- 45 – 50 Day -> Cotyledons.
- 71-267 Day->Fital Stage
Development of fits (According to week)
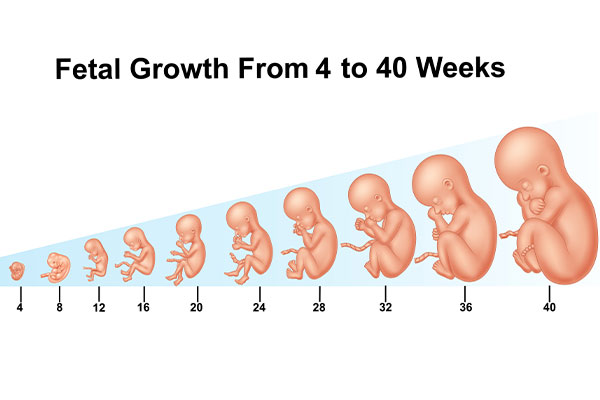
4 vix->
- Ovum diameter 2 cm,
- Embryo length 1 cm.
- Covered by villi.
- Head, tail and gill buds develop.
8 weeks->
- Ovum-diameter 5 cm,
- Fits length 2.5 cm.
- The nose, external nose, fingers and toes develop.
- And the head is tilted towards the chest.
12 weeks->
- Ovum diameter 7.5 cm.
- Fetus length 8 cm.
- Placenta forms, cord is twisted, external ears become more prominent, eyelids and nails are closed.
16 weeks->
- Fits length 18 cm.
- Eyes closed, skin red and transparent, external genital area recognizable.
20 weeks->
- Fits length 25 cm.
- Hair and lanugo (fine hair on the skin).
24 weeks->
- Fits length 30 centimeters cm.
- Eyelids are loose, eyebrows and eyelashes are visible.
28 weeks->
- Fits length 35 centimeters.
- Weight – 1250 gm.
- Skin is red, subcutaneous fat covered with lanugo begins to form,
- Testis descends And the fit is viable.
32 weeks->
- The fit length is 40 cm.
- Weight is 1500 gm.
- The nails reach the end of the finger. The skin looks less red. is.
- Subcutaneous fat increases,
- Varni cassiosa is present and wrinkles are less visible.
36 weeks->
- Fits length 45 cm,
- Weight-2500 gm.
- Skin is pink, vernix is thick, some lanugo, subcutaneous fat increases.
40 weeks->
- Fits length 50 Cm.
- Weight 3500 gm.
- Skin is pink, lanugo is disappearing, vernix is reduced. Subcutaneous fat increases. The skull and testicles descend into the scrotum.
(According to Trimester) According to Trimester:
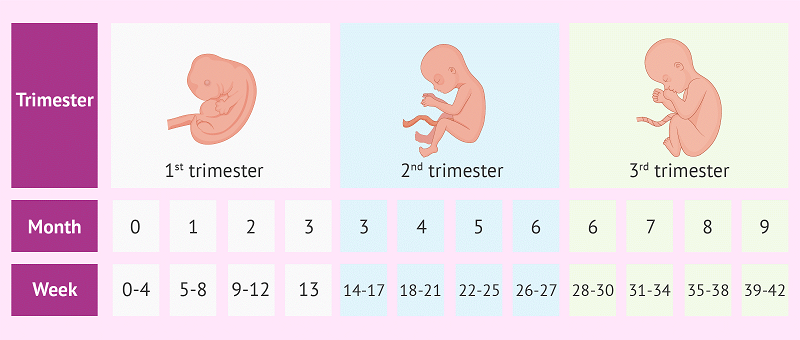
1) First Trimester (First Three Months):
- The following changes occur as the fertilized ovum develops into an embryo:
- All organs form and the heart begins to beat in 21 to 22 days.
- After the embryonic period, fetuses are less susceptible to drugs and infections.
- Facial features form, the brain develops rapidly, and the head becomes larger than the body, giving a human appearance.
- External sex organs are visible, but sex cannot be determined.
- The neck is well-developed, nails The beginning of the bed, nose, mouth, eyelids visible and teeth birds form.
- Urine from the early kidneys is released into the amniotic sac in small quantities.
- Movement of parts of the limb occurs but is not strong.
- The length of the fetus is about 2.9 inches and the weight is 14 gms.
2) Second Trimester (4th month, 5th month to 6th month):
- Fetal heart sounds are heard through a stethoscope, the ice is cold and body growth increases.
- Vernix caseosa protects delicate skin. The skin is wrinkled, transparent and pink.
- Sex can be differentiated.
- Small baby, uterus is frilly.
- Skeletal calcification.
- Average crown specimen length is 20 cm and weight is 568 gm.
3) Third Trimester (7th month, 8th month to 9th month)
- Skin is pink and white, strong sucking reflex, and eyes can open and close.
- Skull forms, hair appears loose.
- In male child, testes descend into scrotum.
- Skull bone forms, closure of Suture line.
- Lightening.
- Length-48-53 Cms,
Weight-3000 gm.
Placenta:
Introduction:
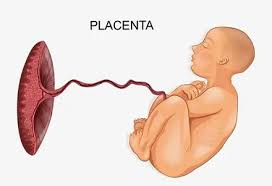
- The placenta is a mass-like structure. It develops from two sources, the fetal component chorion frondosum and the maternal component decidua basalis, usually on the anterior or posterior side of the upper uterine segment.
- The placenta is connected to the fetus by the umbilical cord and maintains pregnancy. The placenta supports the life of the embryo by providing it with oxygen and food and removing toxic materials.
Definition
- The placenta is “discoid shaped” due to its septum, it is “hemochorionic” because its chorion comes in direct contact with the maternal blood and it is “deciduous” because the placenta is shed off after birth.
Placenta Origination
- The placenta originates from the trophoblastic layer of the fertilized ovum.
- The placenta is closely linked to the maternal circulation to properly perform its functions, functions that it is unable to perform during intrauterine life.
- The survival of the fetus depends on the integrity and efficiency of the placenta.
Attachment of placenta
- The placenta is attached to the uterine wall of the mother and establishes a connection between the mother and the fetus via the umbilical cord.
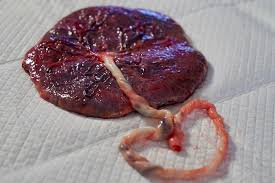
Placenta At Full Term
- The placenta at full term is a disc-like, spongy, flaky structure that is flat and round or oval in shape. The placenta is thick in the center and thin at the edges.
Diameter and thickness of placenta:
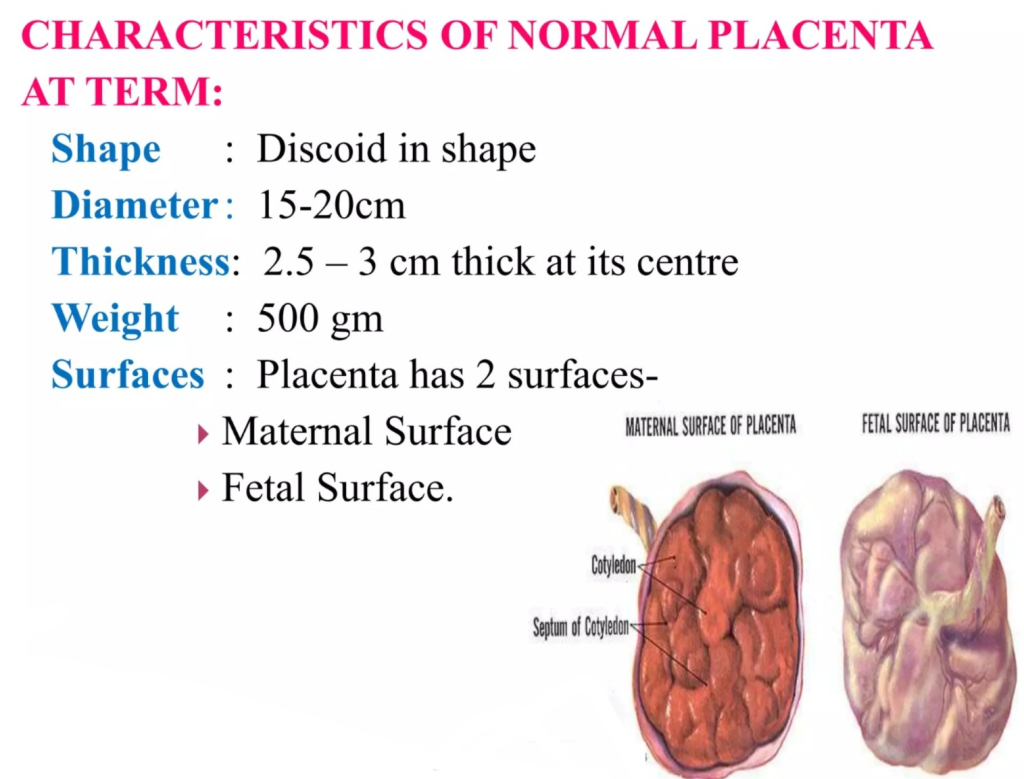
1)Average weight of placenta:= 500 gm
2)Ratio between fetus and placenta:= 1/6 ( 3kg / 500 gm).
3)Diameter of placenta:= 15-20 cm.
4)Surface area of placenta:= 243 sq cm (square centimeter).
5) Placenta volume:= 500 ml.
6) Placenta is thick in the center while thin at the edges.
Center part of placenta:=
2.5 to 3 cm.
Peripheral part of placenta:=
1 to 1.5 cm
The umbilical cord connects the fetus to the placenta, which contains one umbilical vein and two umbilical arteries.
Part of Placenta
The placenta has two surfaces.
1) Fetal surface (80%),
2) Maternal surface (20%)
1) Fetal surface (80%):
- Fetal The surface is smooth, sinuous and transparent, covered by a smooth and glistening amnion.
- In which the umbilical cord is connected at the center.
- Umbilical vessels are visible on this surface.
- The fetal surface is of a bright red color.
2) Maternal surface (20%):
- The maternal surface is “rough and spongy”.
- It is dull red in color.
- The maternal surface is divided into 15 to 30 cotyledons separated by sulci.
- Small calcified infarcts are visible on the maternal surface is.
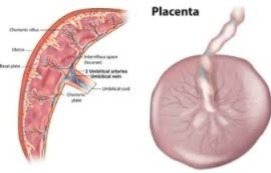
Structure of placenta
- The placenta consists of two plates. The chorionic plate is the innermost plate, which is covered by the amniotic membrane. The umbilical cord is attached to this plate. There is a basal plate on the maternal side.
- Between this chorionic plate (fetal site) and basal plate (maternal site) is the intervillous space.
- This intervillous space contains the stem cells and their branches and contains maternal blood.
1) Amniotic membrane
- The amniotic membrane is a single layer of cubical epithelium and connective tissue. And the amniotic membrane is loosely attached to the chorionic plate.
- It has no part in the placenta formation.
2) Chorionic plate
- The chorionic plate is the seat of connective tissue. It contains the branches of the umbilical vessels. This chorionic plate is covered by the amniotic membrane at the fetal site.
- The stem junction arises from the chorionic plate which forms the inner boundary of the choriodecydular space.
3) Basal plate.
- The basal plate is formed by cytoblasts, syncytoblasts, and decidua basalis.
- It is a compact and spongy layer.
- The basal plate is present near the maternal surface.
- The uterine arteries and veins enter the intervillous space from the basal plate.
- The basal plate forms a boundary in the maternal surface.
4) Intervillous space
- Which has the chorionic plate on the inner side and the basal plate on the outer side. There is a connection of two plates around it.
- Internally, it is lined on all sides by syncytotrophoblast and filled with slow flowing maternal blood.
- In this intervillous space, the stem villi and their branches are also located.
5) Stem villi
- Stem villi arise from the chorionic plate and grow to the basal plate.
- Primary, secondary and tertiary villi are formed in progressive development.
- The functional unit of the placenta is the fetal cotyledon or placentome. It is formed from major primary stem villi.
- These major stem villi pass through the intervillous space and enter the basal plate. The functional subunit is called a lobule, which is formed from tertiary villi.
- There are about 60 stem villi in the human placenta. Therefore, each cotyledon (total:=15-20) has three to four major stem villi. Some villi anchor the placenta and some remain free in the intervening space, which are called nutritive villi. The blood vessels in the villi do not connect with each other.
Circulation through the placenta
There are two types of circulation in the placenta.
1) Fetoplacental circulation,
2) Uteroplacental circulation
1) Fetoplacental circulation,
- In the fetoplacental circulation, two umbilical arteries bring impure blood from the fetus and enter the chorionic plate, each supplying 1/2 of the placenta.
- The arteries break into small branches and enter the stem of the chorionic villi, which divide into primary, secondary, and tertiary vessels. Maternal and fetal blood flow side by side in opposite directions.
- Fetal blood flow is 400 ml/minute which is mainly due to the pumping action of the fetal heart rate. The blood from the umbilical artery returns to the fetus through the umbilical vein after delivering carbon dioxide to the placenta and absorbing oxygen.
2) Uteroplacental circulation (maternal circulation)
- In the uteroplacental circulation, the uterine arteries and veins enter the intervillous space through the basal plate and transmit blood and nutrients from the mother to the intervillous space.
Function Of Placenta:
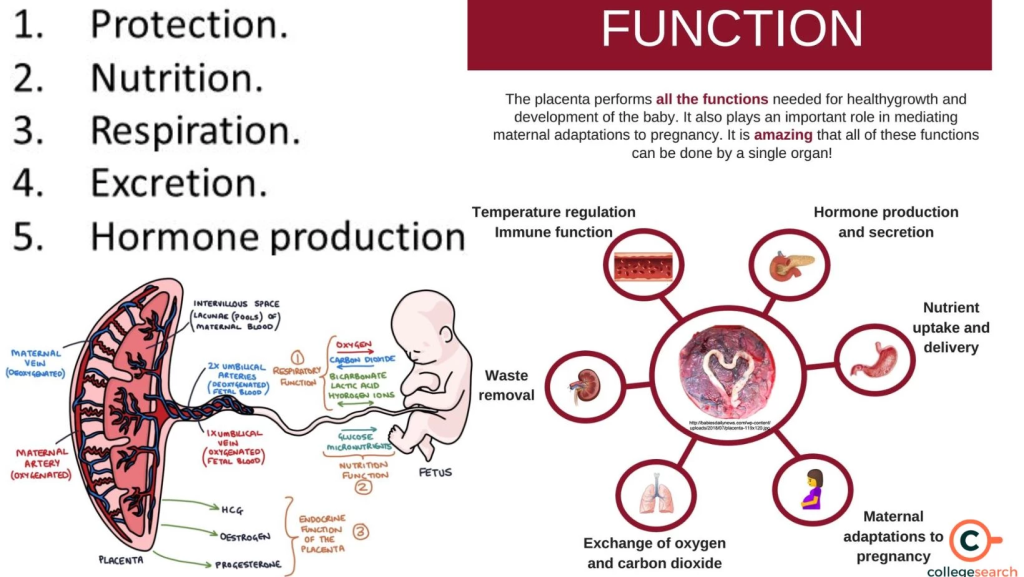
1) Respiratory Function
- Through the placenta, the fetus receives oxygen and excretes carbon dioxide.
- Just as oxygen passes from the mother’s blood to the fetal blood, carbon dioxide in the fetus is transmitted to the maternal blood through the placenta.
2) Nutritional function
- All types of nutrients such as amino acids, glucose, vitamins, minerals, lipids, water and electrolytes are transmitted from the mother to the fetus.
- The food taken in the maternal diet reaches the placental side where it is converted into simple forms. After that, the placenta selects the substances required by the fetus and transmits them to the fetus.
3) Storage Function
- The placenta stores glucose, iron, and vitamins. And the placenta provides it when the fetus needs it.
4) Excretory function
- The waste products in the fetus are transmitted to the placenta.
5) Protection
- The placental membrane has a limited barrier function. Some antibodies pass from the mother to the fetus, providing immunity to the baby for three months after birth.
6) Immunological function
- Antigens from the fetus and placenta act as foreign to the mother. However, graft rejection does not occur because the placenta provides immunological protection against rejection.
7) Hormonal function
- Steroid hormones
Oestrogen,
Progesterone. - Protein hormones
HCG(Human Chorionic Gonadotropin),
HPL(Human Placental Lactogen),
Relaxin,
PAPPA (Pregnancy Associated Plasma Protein:= A).
•>HCG(Human Chorionic Gonadotropin),
- HCG (Human Chorionic Gonadotropin) is produced by the cytotrophoblastic layer of the chorionic villi.
- HCG (Human Chorionic Gonadotropin) is highest during the 7th to 10th week of pregnancy and then decreases as the pregnancy progresses. It maintains the corpus luteum.
- HCG (Human Chorionic Gonadotropin) is used in pregnancy tests because it is excreted in the mother’s urine.
- HCG (human chorionic gonadotropin) is detected in the blood 7 days after fertilization and in the urine 9 days after fertilization, which indicates a positive pregnancy test.
••> HPL (Human Placental Lactogen)
- HPL (Human Placental Lactogen) is produced by the placenta and is involved in the lactogenic and metabolic processes of pregnancy. When the level of human chorionic gonadotropin decreases, the level of human placental lactogen (HPL) increases and continues throughout pregnancy.
- Human Placental Lactogen (HPL) works as an anti-insulin that increases the glucose level in the blood and supplies glucose to the fetus. Helps.
••>Relaxin
- Relaxin is produced by decidua cells. And it softens the cervix and helps in relaxing the pelvic ligaments and symphysis pubis.
••>PAPPA (Pregnancy Associated Plasma Protein:= A)
- Pregnancy Associated Plasma Protein:= A works as an immunosuppressant and works to maintain pregnancy.
••> Estrogen
- Estrogen is produced by the placenta throughout pregnancy. It is essential for the well-being of the fetus.
- Estrogen increases during labor, which helps release oxytocin, which increases uterine contractions.
••> Progesterone
- Progesterone is produced by the syncytial layer of the placenta and acts as a tocolytic agent and prevents uterine contractions, as well as acting as an immunosuppressant to help maintain pregnancy.
Placental Abnormalities (Placental Abnormalities):
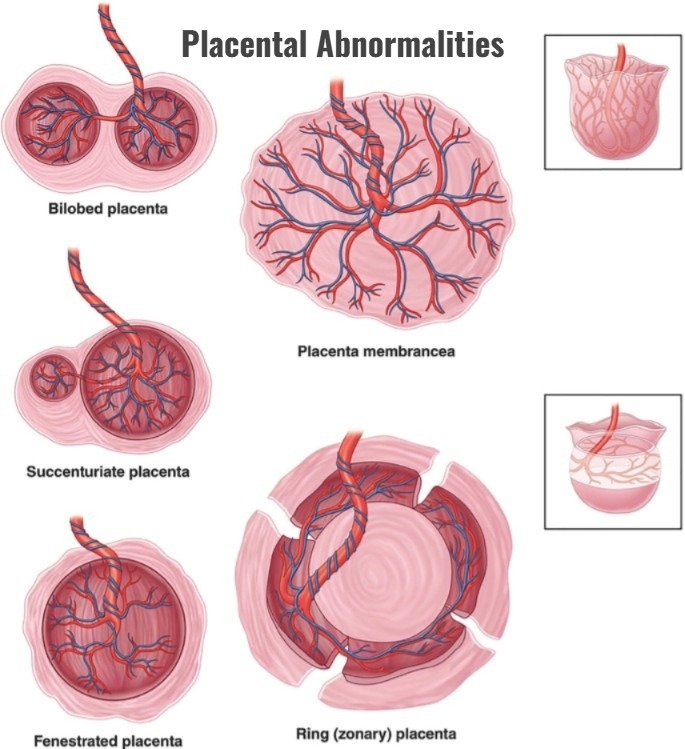
1)Placenta sacenturiata
2)Placenta spuria
3)Velmentus placenta
4)Bateldor Placenta
5)Placenta membranacea
6)Placenta marginata
7)Placenta circumvallate
8)Placenta accreta
9)Placenta incrita
10)Placenta percrita
11)Large placenta
12)Bipartite placenta
13)Tripartite placenta
14)Placenta fenestrata
15)Placenta previa
16)Abruptio placenta
1) Placenta sacenturiata (Placenta sacenturiata) :

- Placenta sacenturiata is when the placenta has one or more extra lobes that are connected to the main placenta by blood vessels.
- These extra lobes are not directly connected to the main placenta but are connected by a membrane.
- These lobes are distant from the main placental mass, so during expulsion of the placenta, these sacenturiata lobes There is a possibility of it remaining in the uterus. This can lead to severe postpartum hemorrhage (PPH).
2)Placenta spuria (placenta spuria):
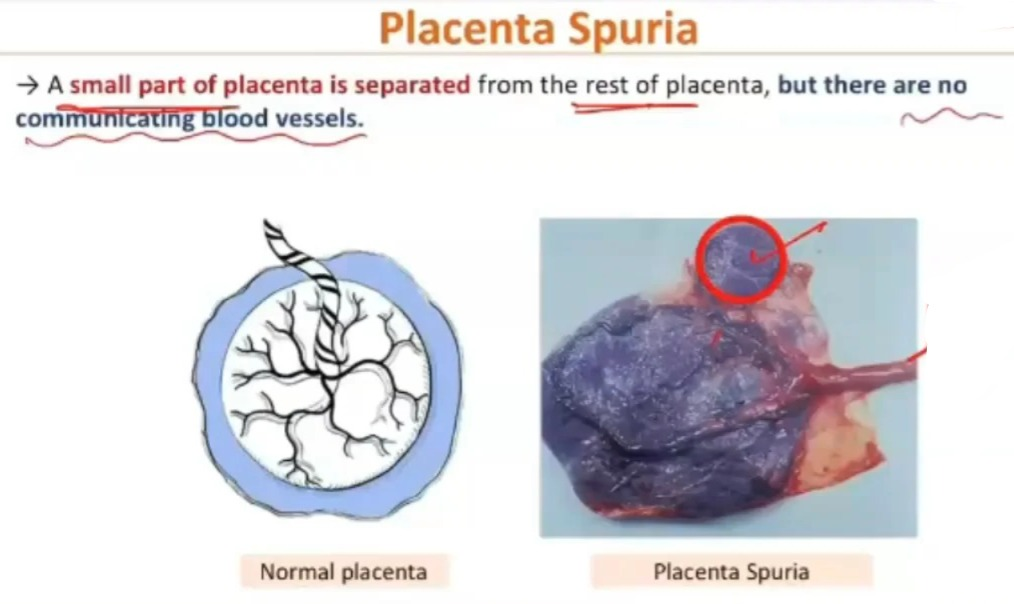
- Placenta spuria, also known as “false placenta” or “accessory placenta”, is a condition of the placenta where there is one or more small, extra lobes of placental tissue separate from the main placenta.
- The main The placenta is located at different distances from the margin. And the lobes do not have communicating blood vessels.
3) Velmentous placenta (Velmentous placenta) :
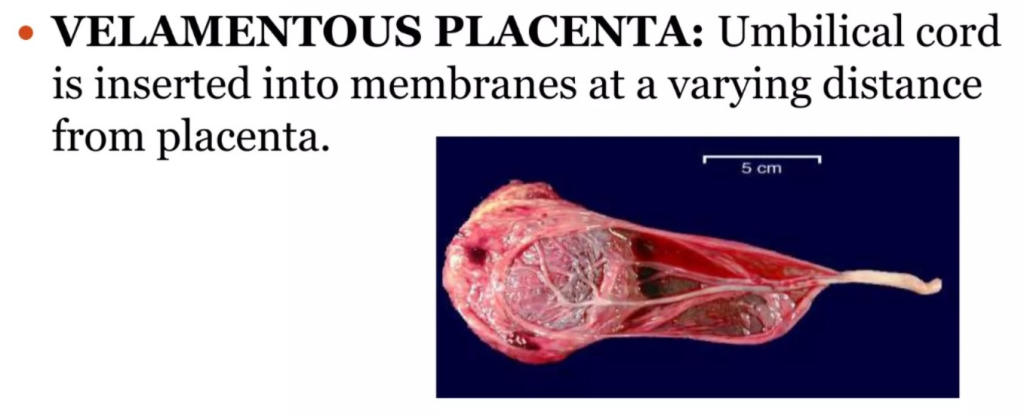
- In this, the umbilical cord is usually attached to a membrane one to three inches away from the placenta.
- This means that the blood vessels of the umbilical cord have to travel a long distance (the placental membrane) to get nutrients from the placenta. They have to, and they have to travel without the protection of Wharton’s jelly.
- Without easy access to nutrients from the placenta, the fetus develops more slowly.
- Without the protection of Wharton’s jelly, the exposed blood vessels from the umbilical cord are more likely to rupture and bleed.
- It can cause APH (antepartum hemorrhage) during artificial or spontaneous rupture of the membranes.
4)Battledor placenta:
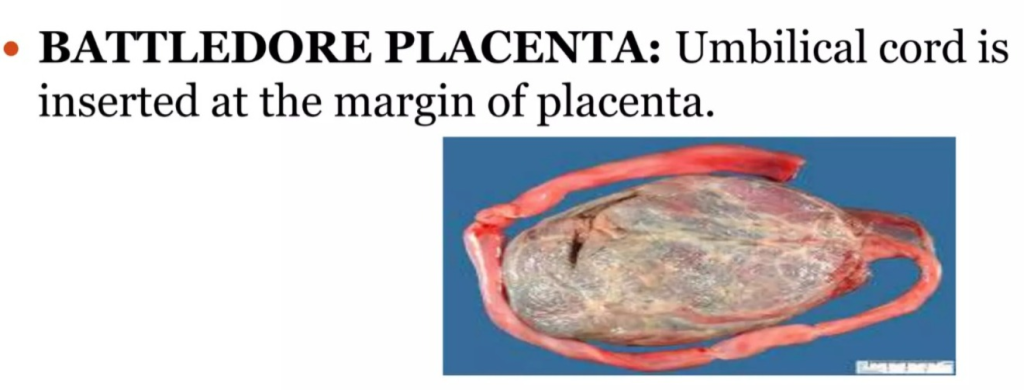
- In a placenta previa, the cord is attached to the margin of the placenta, meaning the umbilical cord is not in the center of the placenta.
- If associated with low implantation of the placenta, there is a possibility of cord compression during vaginal delivery, which can lead to anoxia or even death of the fetus.
5)Placenta membranacea (placenta Membranesia):
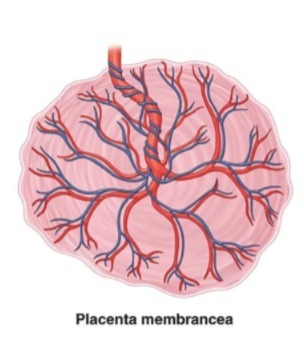
- It occurs as a result of the failure of the decidua capsularis to come into contact with the chorion.
- It has a very thin and large placenta that does not have a large area on the wall of the uterus.
In this, the chances of retained placenta are high and manual removal becomes difficult.
6)Placenta marginata (Placenta marginata):

- Double fold on the periphery of the placenta in placenta marginata The amnion and chorion are layered and form a structure similar to the whitish ring.
- When this whitish ring coincides with the placental margin, it is known as placenta marginata.
7)Circumvallate Placenta:
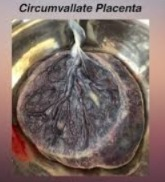
In this condition, an opaque ring is seen on the surface of the placenta. It is formed by the double layer of the chorion and the amnion and can result in a membrane that is usually located near the center of the placenta, rather than the edge of the placenta.
8) Placenta accreta (placenta accreta):
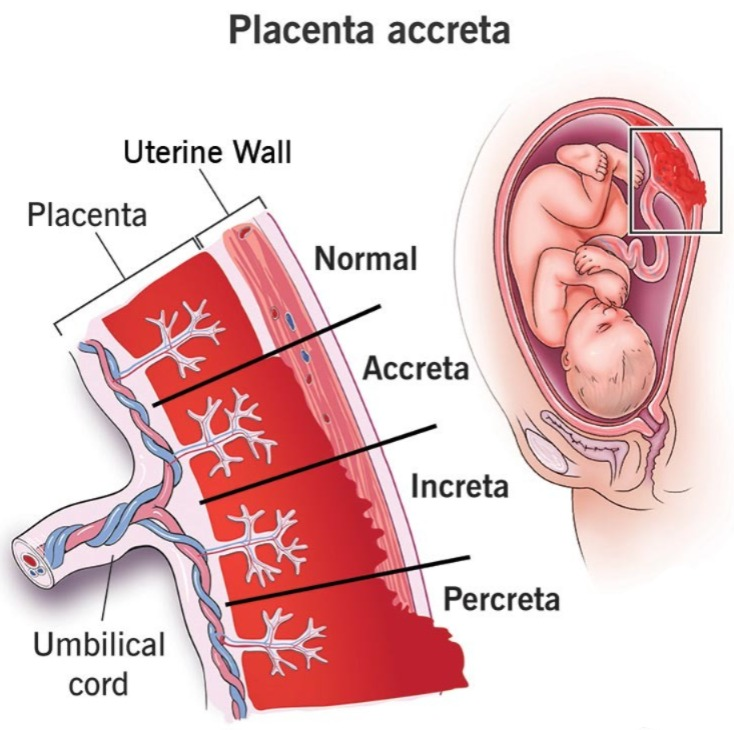
- In placenta accreta condition, the placenta is abnormally attached to the uterine wall.
- In other words, the placenta is attached to the myometrium.
9) Placenta increta (placenta increta) :
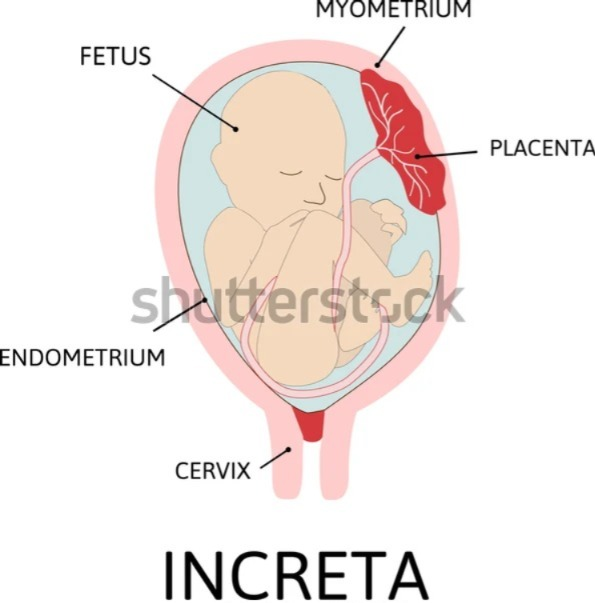
- In placenta incretin, the placenta develops into the deep layer of the myometrium.
10)Placenta percrita (Placenta percrita):
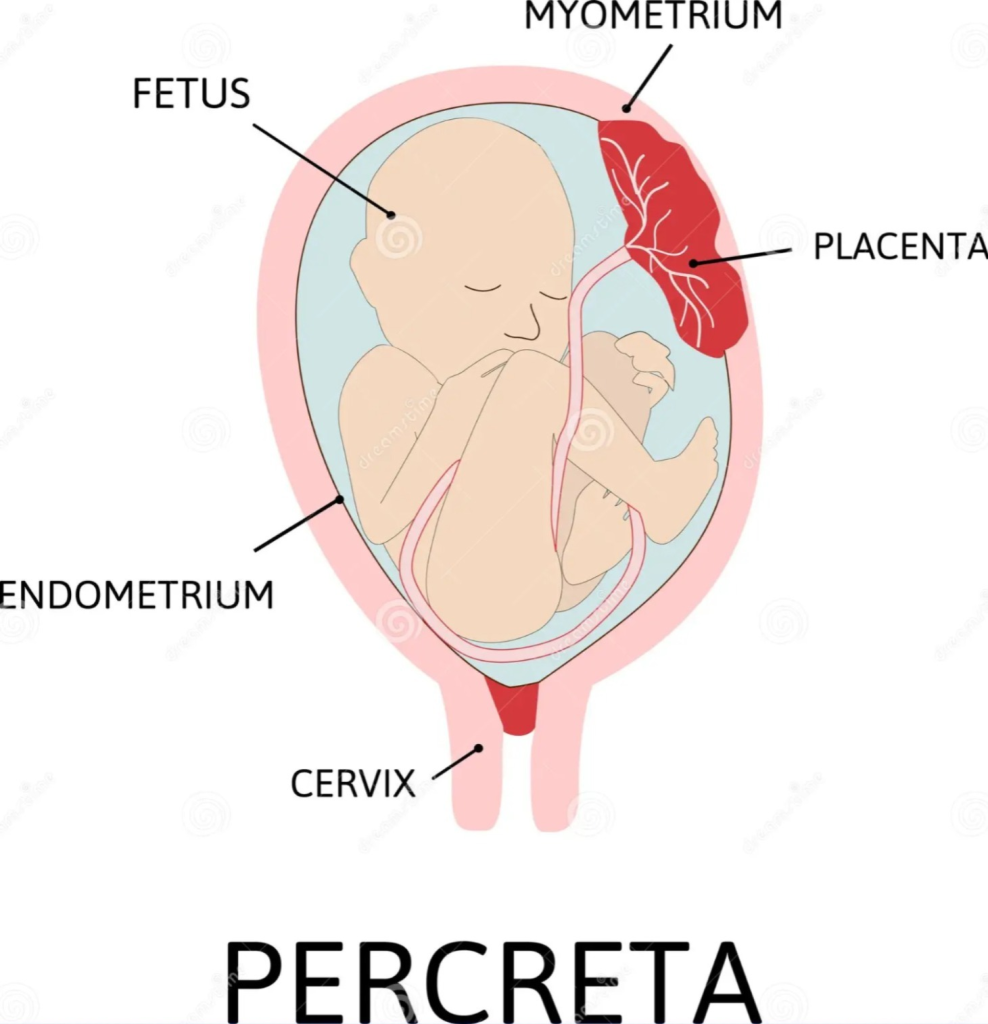
- In placenta percrita, the placenta develops up to the perimetrium layer of the uterus.
11) Large Placenta (more than 500 grams):
Large placenta, often referred to as placental hypertrophy, is a condition where the placenta is significantly larger than typical for the stage of pregnancy. It can be associated with various maternal or fetal conditions such as maternal syphilis, diabetes mellitus, etc.
12) Bipartite placenta (dimediata/bilobed):
Bipartita (dimediata)
In this condition, there is incomplete division of the placenta into two distinct lobes.
The umbilical vessels extend from one lobe to the other before uniting to form the umbilical cord.
13) Tripartite placenta (Tripartite placenta):
In tripartite placenta, the placenta is in three separate parts, meaning there are three complete lobes of the placenta.
14) Placenta fenestrata (Placenta fenestrata):
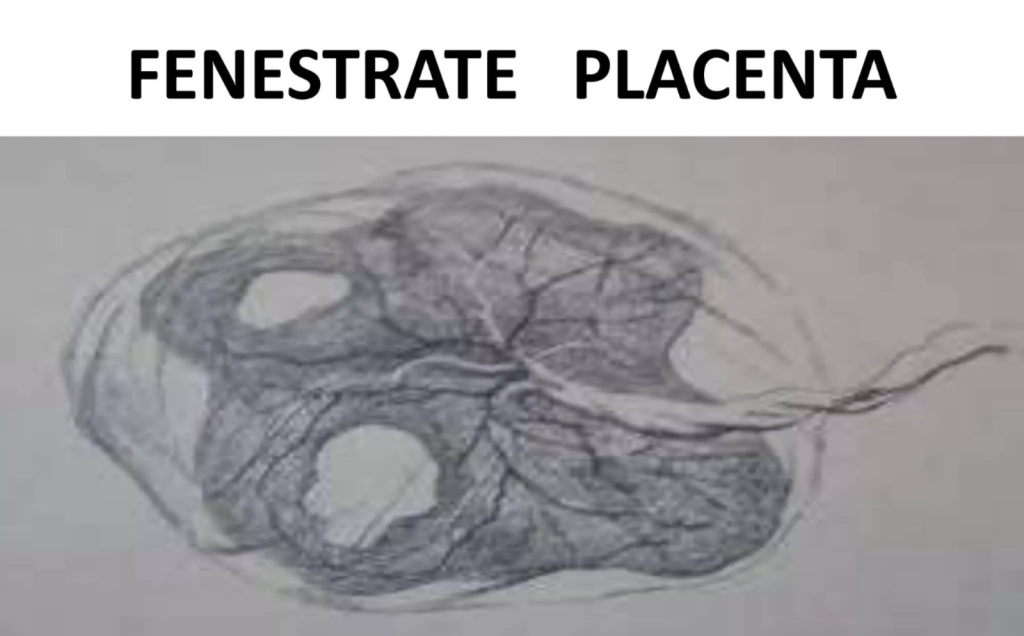
- Placenta fenestrata is a rare condition In which the central part of the discoid placenta is missing. Rarely, there may be an actual hole in the placenta, but more often the defect involves the villous tissue, and the chorionic plate remains intact.
- It causes the placenta to divide into two lobes. This is a rare condition.
15) Placenta Previa :
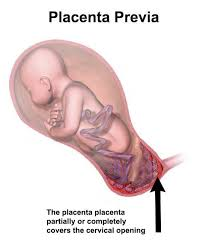
- When the placenta partially or completely implants near or above the internal os of the lower segment of the uterus, it is called “placenta previa”. 1/3 of cases of antepartum hemorrhage are due to placenta previa.
16)Abruptio Placenta:
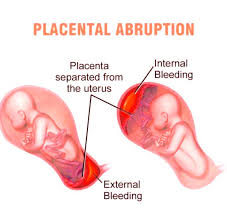
- Placental abruption is a form of antepartum hemorrhage (APH) in which the normally situated placenta prematurely separates from the uterine wall. And this causes bleeding which is called placental abruption.
Amniotic Fluid Amniotic Fluid (Liquor Amni):
Definition:
- Amniotic fluid is the “faint, slightly alkaline, colorless, and watery contents of the amniotic sac” which Embryo-fetus grows.”
- Amniotic fluid, or liquid amnio, is the fluid in the amniotic sac that covers the developing fetus during pregnancy. It is essential for the development and protection of the fetus.
- It is believed to be a secretion of amniotic cells. Fetal and maternal vessels are believed to secrete urine and transudates from the fetus, as well as from the cord placenta and decidua, which are believed to increase the quantity of amniotic fluid.
Origin:
- Its origin is not clearly understood. Its origin is thought to be due to a mix of maternal and fetal conditions.
Development:
- The amniotic cavity and its lining membrane, the amnion, originate from the development of an inner cell mass. Amniotic fluid is contained in the amniotic sac, which surrounds the fetus and is produced by the cells of the amnion. It transudates from the fetal vessels in the cord, from the maternal vessels of the placenta and decidua. In the latter half of pregnancy, its volume increases due to fetal urine. The fluid gradually fills the amniotic cavity and then the entire cavity is filled.
Circulation:
- The water in the amniotic fluid is completely changed and replaced every three hours. Because the clearance of radioactive sodium occurs directly in the amniotic cavity.
- The presence of lanugo and epithelial scales in the meconium indicates that the fluid is swallowed by the fetus and some passes through its intestine and into the plasma.
Physical Characteristics:
1)Early Pregnancy:
Amniotic fluid is clear.
2)Mid pregnancy:
Excess bile pigments make it yellow.
3)Late pregnancy:
Bilirubin is colorless as it becomes negligible,
particulate matters, i.e. vernix caseosa and desquamated epidermis appear as white flocs.
Volume:
Amniotic fluid is detected during the 8th week of pregnancy.
10 weeks := 30 ml
12 weeks:= 50 ml
20 weeks:= 300 ml
30 weeks:= 600 ml
36 – 38 weeks:= 1000 ml
38 – 40 weeks (at term):=600 – 800 ml
43 weeks:= 200 ml.
Composition:
1) Early Pregnancy:
Amniotic fluid is similar to maternal plasma with less protein.
2) Late Pregnancy:
Amniotic fluid mixes with fetal urine and desquamation occurs from the skin of the fetus.
Composition of Amniotic Fluid at Term:
1)Water:= 98 – 99%
2)Solid:= (organic and inorganic cells):=1-2 %.
a)Organic:
i ) Protein including ( ‘α’ fetoprotein) -0.25 g%
ii) Uric acid – 4 mg%
iii) Creatinine – 1.8 mg.
iv) Glucose – 20 mg%
v) Lipids
vi) Phospholipids
vii) Bilirubin (trace)
viii) Hormones (prolactin)
ix) Vitamins
x) Prostaglandins.
B) Inorganic
electrolytes (Na, K, CI).
C)Cells
1). Nucleated
2). A enucleated sample obtained from fetal skin, buccal mucosa, respiratory mucosa, bladder and umbilical cord.
3). During mid-pregnancy, it contains large eosinophilic nucleated cells.
4). During late pregnancy, large enucleated cells and nucleated cells are seen from the skin of the fetus.
Color
In early pregnancy, it is colorless but near term it becomes pale straw color due to the presence of exfoliated lanugo and epidermal cells from the skin of the fetus.
It may appear dirty due to the presence of vernix caseosa.
Abnormal color may be as follows:
1) Meconium stained green color:
In conditions of fetal distress Present.
Thickness with presence of flakes indicates chronic fetal distress.
2)Golden color:
Due to Rh incompatibility
3) Greenish yellow color:
Due to post maturity
4) Dark red Color:
Due to accidental hemorrhage
5) Dark brown color (tobacco color):
I.U.D (Due to intrauterine fetal death).
Functions:
The main function is to provide protection to the fetus.
The main function is to provide protection to the fetus.
During Pregnancy:
- 1) Amniotic fluid acts as a shock absorber and protects the fetus from external injuries.
- 2) It also works to maintain temperature.
- 3) Amniotic fluid distends the amniotic sac. Thus providing space for the fetus’ growth and free movements. Also prevents adhesion between fetal parts and amniotic sac.
- 4) The nutritional value is negligible but provides adequate water supply to the fetus.
During labor:
- Helps in dilation of the cervix.
- Prevents obstruction of the circulation of the placenta during uterine contractions.
- Works to protect the placenta and fetus during uterine contractions.
- Flushes the birth canal during the end of the first stage of labor and protects the fetus with its aseptic and bactericidal action. It also prevents ascending infection in the uterine cavity.
Clinical Importance
- The study of amniotic fluid provides information about the well-being and maternity of the fetus.
- Intra-amniotic instillation is used as an abortion method using chemicals
- Helps in the assessment of fetal malformations, i.e. during 16-18 weeks, cell culture of amniotic fluid obtained by amniocentesis can identify chromosomally defective babies, e.g. Down’s syndrome. Enzyme deficiencies are cultured. And amniotic fluid can identify metabolic errors in the fetus.
- A fetus with high levels of alphafetoprotein (AFP) in the amniotic fluid can be identified as having an open neural tube defect (anencephaly).
- The amniotic fluid index (AFI) is used to assess low or high volume.
- Rupture of the membranes and draining the fluid also helps in the induction of labor.
Umbelical Cord :
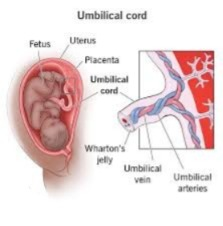
- The umbilical cord is also called the “funis”.
- “The funis or umbilical cord forms the connecting link between the fetus and the placenta”. Through which fetal blood flow goes to and from the placenta.
- The umbilical cord is connected between the fetus and the placenta, so the umbilical cord helps in providing blood flow to the fetus.
- The umbilical cord extends from the fetus’s umbilical cord to the fetal surface of the placenta.
Development
- It develops from the stalk of the body of mesodermal tissue extending between the disc of the fetus and the chorion.
Characteristics:
1) The length of the umbilical cord ranges from 30 – 90 cm.
However, its average length is: = 55 cm.
2) Color := It is bluish white.
3) Diameter := It is about 1-2.5 cm.
4) It is twisted from left to right in a spiral manner (40 twists).
5) Wharton’s jelly is present on the umbilical cord to provide protection to the cord.
6) Its thickness is not uniform but there are nodes or There is swelling. This swelling is due to dilatation of umbilical vessels or local collection of Wharton’s jelly. This swelling is also called false knot.
7) Initially, two arteries and two veins form. The arteries have a connection with the internal iliac artery of the fetus.
They carry venous blood (deoxygenated blood) from the fetus to the placenta.
Of the two developed umbilical veins, the right vein disappears by the 16th week (fourth month), leaving one vein carrying oxygenated blood from the placenta to the fetus.
8) Umbilical arteries do not have an internal elastic lamina but have a well-developed muscular coat. This helps in effectively closing the artery due to reflex spasm immediately after the birth of the baby.
Structure of Umbelical Cord :
1) Covering epithelium,
2) Wharton’s jelly,
3) Blood vessels,
4) Umbilical vesicle (yolk sac) and its remnant vitelline duct,
5) Allantois,
6) Obliterated extra embryonic Coelum
••>
1) Covering epithelium:
- Initially the umbilical cord is formed by a single layer of simple epithelium cells. But at term it forms a single layer of stratified epithelium.
2) Wharton’s Jelly:
- It is made up of a gelatinous fluid. It is formed from extra-embryonic mesodermal cells. It is rich in polysaccharides. It protects the umbilical vessels.
3) Blood Vessels:
- Initially, two arteries and two veins form. The artery has a connection with the internal iliac artery of the fetus.
- They carry venous blood (deoxygenated blood) from the fetus to the placenta.
- Of the two umbilical veins that develop, the right vein disappears by the 16th week (fourth month), leaving one vein carrying oxygenated blood from the placenta to the fetus.
4) Umbilical vesicle (yolk sac) and its Remnant of the vitelline duct:
- The remaining part of the yolk sac is attached to the placenta by the cord. It is rarely seen there as a small yellow body.
- Its proximal part remains as Mecklenburg diverticulum.
5) Allantois:
- Blind tubular structures are rarely seen near the fettle end. Which remain as continuous ureters and bladder within the fetus.
6) Obliterated extra embryonic coelom:
- In the early period, the intraembryonic column remains continuous with the extraembryonic column. With it, herniation of the intestine occurs.
- If the condition persists, it remains as a congenital umbilical hernia or exomphalos.
Function:
- It works as a lifeline between the placenta and the fetus. It provides oxygen and nutrients to the fetus and transports the fetus’s waste products to the placenta.
- The umbilical cord exchanges fluids and electrolytes between the umbilical vessels and the amniotic fluid.
- The softness of the cord stabilizes due to the flow of blood through the cord at a rate of about 400 ml/min.
- The umbilical cord does not have pain receptors, so cutting the cord does not cause pain, that is, it is painless.
Abnormalities of the umbilical cord (abnormalities of the umbilical cord):
“Cord abnormalities involve marked variations of the umbilical cord including anatomical and physiological alterations in the umbilical cord such as abnormal length, occlusion etc. which may cause disturbances in feto-placental circulation.”
Abnormalities of the umbilical cord are as follows:
1) Short Coda (short coda)
2)Long cord (long cord)
3)True knot (true knot)
4)False knot (false knot)
5)Loop of cord (loop of cord)
6)True cyst of cord (true follicle of cord)
7)False cyst (false follicle)
8)Single umbilical artery
•>
1)Short coda (short coda):
- Commonly the umbilical cord length is 30 to 90 cm but in the condition of short cord the length of the umbilical cord is less than 30 cm (12 inches) which is called short cord.
- 1) There may be no cord (accordia).
2) Breech presentation favors a short cord.
3) It causes abruptio placentae and uterine inversion. - Effects: May restrict fetal movement, may cause cord compression Or complications may arise during delivery.
2) Long cord:
- Long cord is a condition in which the length of the umbilical cord is more than 100 cm (40 inches).
- It can be as long as 300 cm.
- Effects:
Knots and loops can also develop due to a long cord.
A long cord can also increase the risk of cord accidents like cord prolapse.
A long cord can cover the neck of the fetus, which can also cause a condition of fetal distress.
3) True knot:
- The actual knot formed in the umbilical cord by the mother moving around the fetus is called a true knot.
- A true knot occurs in 1% of pregnancies and is rare.
It is common in monoamniotic twins.
The risk of perinatal loss is threefold. - Effects: Cord compression may occur, potentially affecting blood flow and oxygen supply to the fetus.
4) False Knot:
- It is seen due to tumor in the vessels and due to developmental variation.
It is usually seen due to accumulation of Wharton’s jelly.
It has the features of the chord that resemble a knot but it is usually due to normal variation in the structure of the chord. - Effects: It is usually benign but can be mistaken for a true knot.
5) Loop of chord (Cord Loop):
- This is a condition in which the umbilical cord forms a loop(s) around the baby’s neck.
Which is usually of three types: - 1)One loop(s) of cord around the baby’s neck (21%).
- 2)Two loops(s) of cord around the baby’s neck (3.5%).
- 3) Three loops of cord around the fetus’s neck (0.2%).
- Effects: May cause cord compression, affecting the fetus’s heart rate and potentially complicating delivery.
6) True cyst of cord (true folliculitis of cord):
- Caused by remnants of the vesicle or allantois.
- A true cyst is a fluid-filled cyst lined by epithelium and located within the umbilical cord.
- Effects: May be benign but requires monitoring for possible association with fetal anomalies.
7) False cyst (false cyst):
- Forms due to liquefaction of Wharton’s jelly.
- Effects: False cysts of the umbilical cord are usually benign. They resolve on their own. It does not cause any major fetal anomalies.
8) Single Umbilical Artery:
- Single Umbilical Artery (SUA) is a condition where only one artery is present in the cord instead of the usual two umbilical arteries.
- It occurs in about 1% of cases. It is more common in twins and diabetic mothers.
It is caused by a congenital anomaly of the fetus.
A single umbilical artery increases the chances of abortion, prematurity, dysmaturity and perinatal mortality.
Fetal Circulation:
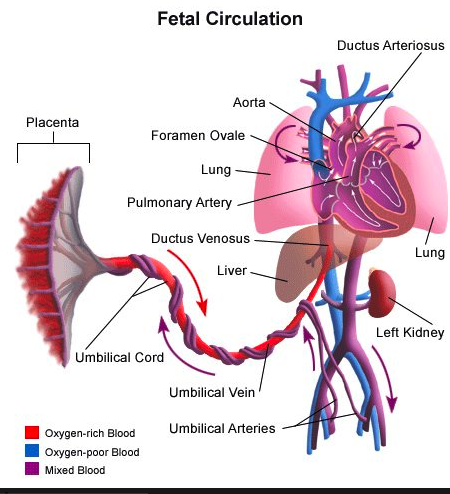
- Fetal circulation is a unique circulatory system that is essential for developing fitness. Present. The fetus is formed to fulfill its need for oxygen and nutrients while in the womb (uterus).
- Separate fetal circulation in the embryo starts during the 16th post-fertilization day.
- The fetal heart starts beating from the 21st day of fertilization. Also, the fetus in the uterus receives oxygen and nutrients from the placenta because its lungs and alimentary tract are functional, so fetal circulation is the circulation through which the fetus receives oxygen and nutrients from the placenta for its survival.
Features of Fetal Circulation
1) Umbilical cord:
- The umbilical cord contains two umbilical arteries and one umbilical vein.
- Umbilical artery:
The umbilical artery is a Waste products and deoxygenated blood are transferred from the fetus to the placenta. - Umbelic Vein:
The umbilical vein transfers oxygenated blood and nutrients from the placenta to the fetus.
2) Placenta:
- The placenta acts as an interface between the circulatory system of the mother and the fetus. is.
- The placenta works to exchange nutrients, oxygen and waste products between maternal blood and fetal blood.
- As the placenta delivers oxygen and nutrients to the fetus through the umbilical vein and receives the fetus’s deoxygenated blood and waste products through the umbilical artery to the placenta.
3) Ductus venosus (from the vein Vein):
- The ductus venosus is a channel through which oxygenated blood from the umbilical vein bypasses the liver and digestive organs into the inferior vena cava.
- This allows oxygenated blood to reach the fetus’s brain and heart in adequate amounts.
4) Foramen ovale( Oval opening):
- The foramen ovale is a fetal cardiac structure that is a small opening in the septum between the right atrium and the left atrium of the heart that acts as a shunt between the right atrium and the left atrium.
- This opening (shunt) allows blood in the right atrium to bypass the fetal lungs and shift to the left atrium.
- This shunt is important because the lungs of the fetus are It is functional during intrauterine life and is filled with fluid due to which the fetal lungs are not able to do their work properly.
5) Ductus arteriosus (artery to artery):
- The ductus arteriosus is a fetal vascular connection that is a communication (sant) between the pulmonary artery and the descending aorta.
- Due to this ductus arteriosus shunt, blood flows from the right ventricles to the systemic circulation through the shunt, bypassing the lungs.
Fetal Circulation:
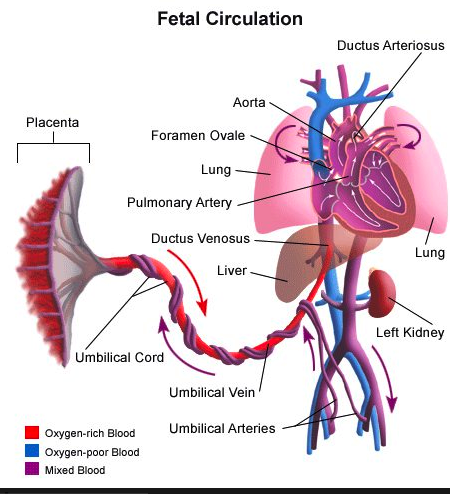
- Oxygen diffuses from the maternal blood into the choriodecidual space (placenta), where the placental villi and vessels unite to form the umbilical vein.
- The umbilical vein travels from the placenta to the fetus through the umbilical cord.
The umbilical vein passes through the umbilical wall and forms two branches of the umbilical vein.
One branch of the umbilical vein joins the portal vein of the fetus’s liver to provide nutrients and oxygen to the fetus’s liver. From the liver, it travels through the hepatic vein. The blood collected enters the inferior vena cava.
The 2nd branch of the umbilical vein connects directly to the inferior vena cava. The connection between the Inferior Vena Cava (IVC) and the Umbilical Vein is called the Ductus Venosus. The oxygenated blood in the umbilical vein mixes with the deoxygenated blood from the lower leg and trunk in the inferior vena cava.
But the oxygen content of the ductus venosus is not seriously affected.
The blood now enters the right atrium through the inferior vena cava.
Then the blood in the right atrium passes into the left atrium through the foramen ovale, a hole between the right atrium and the left atrium.
Then the blood in the left atrium passes into the left ventricle through the mitral valve.
Then the blood leaves the heart through the aorta in the left ventricle.
The coronary vessels of the aorta (coronary artery, brachiocephalic trunk (right common The carotid artery, right subclavian artery, left common carotid artery, left subclavian artery)) supply blood to the heart and branches of the head.
Blood from the head and neck enters the right atrium through the superior vena cava and crosses the inferior vena cava and enters the right ventricle through the tricuspid valve.
Most of the blood from the right ventricle passes through the pulmonary artery, bypassing the lungs (since the lungs are inactive), and passes through the descending aorta through the ductus arteriosus (no duct between the pulmonary artery and the descending aorta) to supply blood to the abdominal organs and lower extremities.
Then from the descending aorta, the right and left internal iliac arteries The right and left internal iliac arteries are again divided into two hypogastric arteries. The hypogastric artery enters the umbilical cord to form the two umbilical arteries. These two umbilical arteries return deoxygenated blood to the placenta. The fetal blood circulates rapidly and is constantly renewed. The mean cardiac output in the fetus is 350 ml/kg/min.
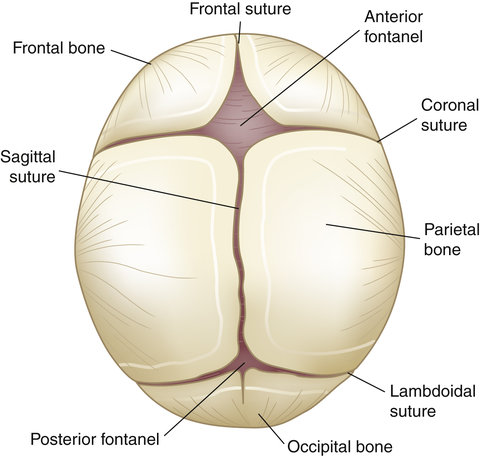
Fetal skull (Fetal skull):
Introduction :
- The shape of the fetal skull is ovoid or egg-shaped. The fetal skull is the skeletal structure of the unborn baby. Certain changes are seen in the fetal skull during delivery.
- The fetal skull provides a shape for the brain and facial features to grow.
The fetal skull is made up of many bones, such as the frontal bone, parietal bone, temporal bone, and occipital bone, along with other smaller bones such as the sphenoid and ethmoid bones. These bones are connected to each other by flexible joints called sutures, which help the child with head compression and slight movement during birth. There are also two soft fontanelles within the fetal skull that fuse after birth.
The skull of a fetus is somewhat compressible and is composed primarily of thin, flexible tabular (flat) bone that forms a vault.
This bone is anchored to a rigid, incompressible bone at the base.
Area of the fetal skull:
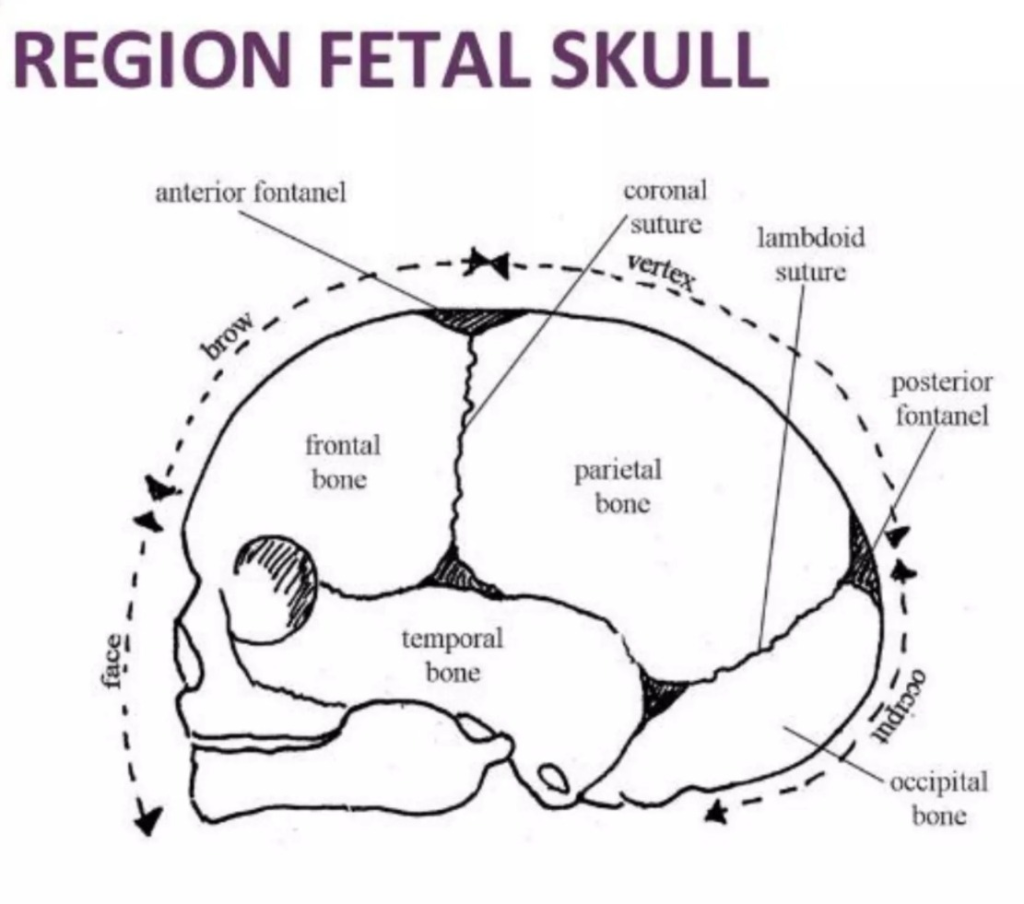
The skull of the fetus is divided into several zones for obstetrical importance. It is mainly divided into three parts.
Such as,
1)Vertex
2)Brow
3)Face
•>
1)Vertex:
It is a quadrangular (Quadrangular) area
It is bounded by:
a) Anteriorly (front):
By the bregma and coronal sutures.
b) Posteriorly (back):
By the lambda and lambdoid sutures.
C)Laterally (side):
By lines passing through the parietal eminence.
2)Brow:
It is the area bounded on one side by the anterior fontanelle and coronal sutures and on the other side by the root of the nose and the supraorbital ridges on both sides.
3)Face:
It is the area bounded on one side by the root of the nose and the supraorbital ridges and on the other side by the junction of the floor of the mouth with the neck.
Region of Skull:
The cranial skull is generally divided into six regions:
1)Vault
2)Base
3)Face
4)Vertex
5)Occiput
6)Sinciput or brow
•>
1)Vault:
- The vault is formed by the two parietal bones, the upper part of the occipital bone, the temporal bone, and the frontal bone, and is the uppermost compressible part of the skull in a large dome shape.
•> Bones of the Vault:
The following bones are located in the vault of the skull:
a) Two frontal bones:
The frontal bones are located in the front of the skull. They are called the forehead or the cranium.
Their center is called the frontal eminence. The frontal bone is separated by the frontal suture
b) Two parietal bones:
The parietal bones are located on either side of the skull, between the frontal bone and the occipital bone. It forms the superior and lateral aspects of the skull.
The two parietal bones of the skull are separated from each other by the sagittal suture running from front to back.
C) Two temporal bones:
The temporal bones are located on either side of the skull below the parietal bones. It contains the inner and middle ear.
d) Occipital bone:
The occipital bone is located at the back of the head and forms the occipital region. It is part of the base of the skull. It contains the foramen magnum which protects the spinal cord as it exits the skull. Its center is called the
occipital protuberance
.
2)Base:
- It is the lowest part that provides protection to the vital center in the medulla. It is made of firmly united bones.
3) Face:
- It is the area bounded on one side by the root of the nose and the supraorbital ridges and on the other side by the connection of the floor of the mouth with the neck.
4)Vertex:
- The area bounded in front by the anterior fontanelle, laterally by the two parietal eminences, and posteriorly by the posterior fontanelles.
5)Occiput:
- The area from the posterior fontanelle to the foramen magnum is.
6) Sinciput or brow:
- It is bounded anteriorly by the orbital region and posteriorly by the coronal suture and is mainly composed of the frontal bone.
Landmarks of the Fetal Skull:
1)Occiput,
2)Lambda,
3)Vertex,
4)Peritor Eminence,
5)Bregma,
6)Cinciputum,
7)Glabella,
8)Nase,
9)Mentum
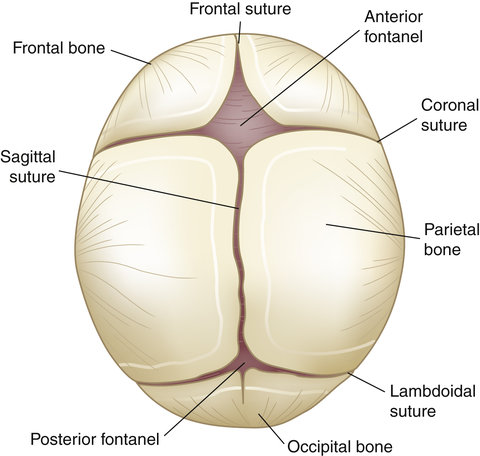
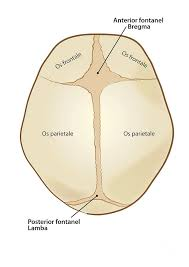
Sutures and Fontanelles:
- The flat bones of the vault are joined together by non-ossified membranes attached to the margins of the bones. These are called sutures and fontanelles. The area in front of the anterior fontanelle and corresponding to the area of the brow is called the sinciput.
Sutures:
Sutures are cranial joints and are formed when two bones come together. They are made of fibrous tissue, which allows mobility between the cranial bones. There are usually four sutures in the vault.
1) Sagittal or longitudinal suture
2) Coronal Suture
3) Frontal Suture
4) Lambdoid Suture
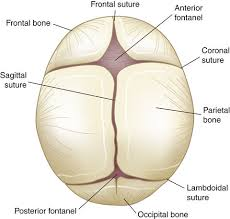
•>1) Sagittal or Longitudinal Suture:
- The sagittal suture is located between the two parietal bones.
2) Coronal Suture:
- The coronal suture is located between the frontal and parietal bones on either side of the head.
3) Frontal suture:
- The frontal suture is located between the two frontal bones.
4) Lambdoid suture:
- There are two lambdoid sutures. Each suture is located on either side of the head at the upper margin of the parietal bone and the occipital bone. Its shape resembles the Greek letter lambda ( λ ).
Importance:
- Sutures help the bones overlap and mold each other during labor, which is important when the head passes through the pelvis during labor.
- Palling the sagittal sutures during an internal examination in labor can help to identify the head The degree of engagement, internal rotation and molding of the.
Fontanels (fontanels):
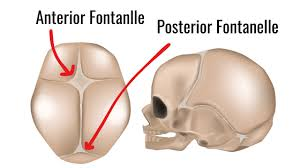
- There is a wide gap between two sutures in the skull bone, which is called fontanelles.
- Fontanelles are spaces made of non-ossified membrane formed by the two sutures coming together.
- There are six main types of sutures.
Such as,
1) Two anterolateral or sphenoid fontanelles, (of the parietal, temporal and frontal bones between)
2) Two posterolateral or mastoid bones (between the parietal, temporal and occipital bones),
3) One anterior fontanel
4) One posterior fontanel
Thus, there are a total of six fontanels.
Two of them are, i.e., 1) Anterior Fontanel/frontal or bregma and
2) Posterior fontanel/occipital or lambda are important in obstetrics.
•>1) Anterior fontanel/frontal or (Bregma):
Anterior/frontal or bregma suture is,
•Anteriorly:= frontal sutures
•Posteriorly:= sagittal sutures and
•At both sites:= coronal sutures The anterior fontanelle or It is formed in the brain.
Its shape is like a diamond (🔹).
Its anterior-posterior diameter is about 4 cm and transverse diameter is about 2.5 cm.
The time for ossification (closure) of the anterior fontanel is 16 – 18 months.
Importance:
- In internal examination, palpation of the head reveals the degree of flexion of the head.
- Molding of the head may occur.
- Helps in brain growth.
- Palpation of the floor reveals the intracranial status.
Example: Depression in dehydration and elevation when intracranial tension increases. - It is sometimes used for blood collection and exchange transfusion through the superior longitudinal sinus.
•It is rarely used to obtain CSF from the lateral ventricle through the lateral angle of the anterior fontanel.
2) Posterior fontanel/occipital or (lambda):
- The posterior fontanel is anteriorly connected to the sagittal suture and the lambda on both sides. The joining of the sutures forms the posterior fontanel or palatine.
- It is triangular in shape ( 🔺️ ).
- Its size is about 1.2 × 1.2 cm.
- Its ossification (closure) time is one and a half months (6-8 weeks).
•> Diameter of the fetal skull:
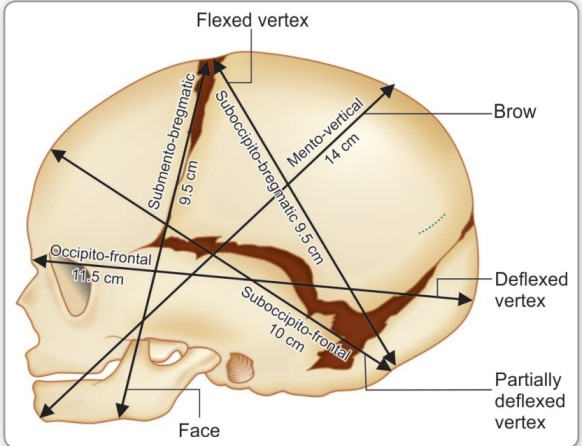
Anterior Posterior Diameter
1) Suboccipito-Begmatic:= 9.5 CM ,
From the lower part of the nape of the neck to the center part of the bregma (anterior fontanel).
2) Suboccipito-Frontal:= 10 CM
From the lower part of the nape of the neck to the anterior end of the anterior fontanel or sinciput to the center part of the.
3) Occipito Frontal:= 11.5 CM
From the occipital eminence to the root of the nose i.e. the glabella.
4) Mentovertical:= 14 CM
Mentovertical diameter is from the midpoint of the chin to the highest point of the sagittal suture.
5) Submento Vertical:= 11.5 CM
Submento Vertical Diameter from the junction of the floor of the mouth to the highest point of the sagittal suture.
6) Submento bregmatic:= 9.5 CM
Submento bregmatic is the distance from the junction of the floor of the mouth to the center of the lateral bregma (anterior fontanel).
Transverse diameter
1) Biparietal diameter:= 9.5 CM
Biparietal diameter is the diameter between the two parietal eminences.
2) Suprasubparietal diameter:= 8.5 CM
From the bottom of the parietal eminence on one side to the top of the parietal eminence on the opposite side.
3) Bitemporal diameter:= 8.2 CM
The distance between the anterior-inferior ends of both coronal sutures.
4) Bimastoid Diameter:= 7.5 CM
The distance between the tips of both mastoid processes.
Molding (molding) :
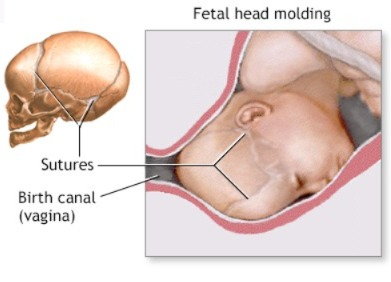
- As the fetus passes through the birth canal, the head of the fetus encounters resistance from the birth passage, which causes alterations (changes) in the shape of the fetus’s head. This is called “molding”.
- During normal delivery, the skull of the fetus usually changes by about 4 mm, which does not cause any problems in the brain.
- The bones of the skull of a newborn baby are soft and flexible, with gaps between the plates of the bones. The space between the plates of the skull bones is called the cranial suture. The anterior and posterior fontanelles have two gaps that are particularly large. These soft spots are felt when the top of the baby’s head is touched.
- During a head-first delivery, the narrowing birth canal (vagina and pelvic bones) can cause pressure on the head, molding the head into a rectangular shape.
- This gap or space allows the baby’s head to change shape depending on the amount and length of pressure, the skull bones may also overlap. This gap or space allows the brain to grow within the skull bones. They will close as the brain reaches its full size.
Mechanism:
- Compression of the engaging diameter of the head increases the length of its right angle diameter.
- Ex:= Engaging suboccipito-bregmatic in a well flexed head in anterior vertex presentation The compression of the diameter increases the length of its right angle manto-vertical diameter.
- During this process, the parietal bone overlaps with adjacent bones such as the occipital bone posteriorly, the frontal bone anteriorly, and the temporal bone laterally. At the vertex, the right parietal bone overrides the left parietal bone. The molding disappears within a few hours after birth.
Grading:
- Grade:= 1 (bones touch each other but do not overlap).
- Grade:= 2 (bones overlap but are easily separated).
- Grade:=3( Bone is a fixed overlapping).
Importance:
• A small amount of molding is necessary and beneficial, as it allows the fetal head to pass through the birth canal easily.
- The shape of the molding can help determine the position of the fetal head in the pelvis.
- Note: Excessive molding of the fit head can cause severe intracranial disturbance in the head, resulting in rupture of the tentorium cerebelli or subdural hemorrhage.
Caput Succadaneum (Caput Succadaneum):
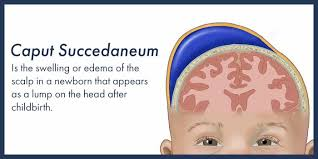
- Accumulation of serosanguineous fluid in the layers of the scalp Edematous swelling is called caput succedaneum. It is caused by the pressure of the girdle of contact. It can be anywhere from the bony pelvis, dilating cervix, or vulval ring. Caput succedaneum is also seen during birth. The swelling is boggy. And it crosses the suture line which disappears in 24-36 hours. It is mostly seen after membrane rupture.
Cephalohematoma (Cephalohematoma):
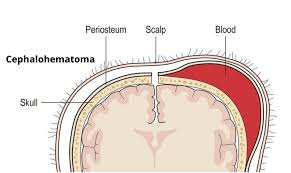
- A cephalohematoma is a condition in which blood collects under the pericranium and flat bones of the head that cover the skull bone, usually unilateral and over the parietal bone.
It is caused by rupture of a small emissary vein from the skull and may be associated with a fracture of the skull bone. This can be caused by forceps delivery but can also be seen after normal labor. Ventouse application does not increase the incidence of cephalohematoma. It is never present at birth but develops gradually after 12-24 hours. - This swelling is limited by the lines of the pericranium sutures of the skull which are fixed to the margin of the bone, soft, fluctuant and incompressible.
It grows and disappears on its own within a few weeks, approximately 6 weeks.
