ENGLISH-NEW MIDWIFERY GNM TY UNIT 4 NORMAL PREGNANCY AND ITS MANAGEMENT
NORMAL PREGNANCY AND ITS MANAGEMENT:

a) Preconception Care:
Definition :
- Preconception care is defined as the necessary care provided to women before they become pregnant, which involves the identification of problems and risk factors that may affect the health of the mother and child, and steps that can be taken to reduce these risk factors.
“Preconception care is defined as a set of interventions that aim to identify and modify, through prevention and management, biomedical, behavioral and social risks to a woman’s health or pregnancy outcome”. - Preconception care involves interventions for the biomedical, behavioral and social health of women and couples before pregnancy.
When couples are seen and counseled about pregnancy, providing information about its course and outcome before the time of actual conception is called preconceptional counseling.
Preconception Care Aims:
- To improve their health condition by reducing behavioral, personal, and environmental factors that contribute to poor maternal and child health outcomes.
- To improve maternal and child health, both in the short term and the long term.
- Opportunities to prevent and control disease are available at multiple stages of life; Strong public health programs that use a life-course perspective from infancy to childhood and adolescence to adulthood are essential.
- To improve maternal and child health, it provides health benefits to adolescents, women, and men, regardless of their plans to become parents.
- Securing optimal health and nutritional conditions in both parents can not only reduce the chances of conception but also the chances of prenatal death and many congenital anomalies.
- To ensure that the woman and her partner are in the optimal state of physical and emotional health in the early stages of pregnancy.
- To achieve normal health in childbearing women.
- To promote prenatal health which involves developing positive attitudes about sexuality, womanhood and childbearing.
- Sickle cell anemia, hypertension, heart To provide benefits to women undergoing treatment for conditions such as diabetes, these diseases can make pregnancy more risky.
Purpose of Preconception Care:
- To establish lifestyle behaviors that can maintain optimal health.
- To identify early risks (such as medical conditions, substance abuse, etc.).
- To prevent pregnancy without any risk factors To get people to conceive.
- To prepare people psychologically for pregnancy and to prepare them for the responsibility of parenthood. What is Pre-Conception Care for?
- To reduce maternal and child mortality rates.
- To reduce unintended pregnancies.
- To reduce complications during pregnancy and delivery.
- To reduce the rates of stillbirth, pre-term birth and low birth weight.
- To reduce birth defects in children.
- To prevent neonatal infections.
- To prevent underweight and stunting in children.
- To prevent vertical transmission of HIV/AIDS.
- To reduce the risk of childhood cancer.
- To reduce the risk of type 2 diabetes mellitus and cardiovascular disease in later life.
- Steps and Pre-Conception Planning:
- 1) Communication Skills,
2) Maternal Age,
3) Menstrual History,
4) Personal Medical History,
5) Obstetric History,
6) Risks to Health/Personal History,
7) Over the Counter Drugs,
8) Environmental Exposure,
9) Psychological History,
10) Family History.
•>
1) Communication Skills:
- Preconception care is ideally based on interviews. To make the interview productive, it requires patience, interest, thoughtfulness, and understanding of the client’s comfort and privacy concerns.
- No one interview approach works well with all women, especially when This is true when it comes to asking questions about sensitive subjects, social support, substance abuse, domestic violence, sexual abuse, emotional problems, mental illness, yet these topics are just as important as medical and obstetric factors.
2) Maternal Age:
- Pregnancy, labor, and birth are safest when a woman is between the ages of 20 and 34. There is. Premature delivery and intrauterine growth retardation (IUGR) babies are more likely to occur in teenage mothers.
- While, women aged 35 years and above face chronic diseases, chromosomal abnormalities or medical complications during delivery. Therefore, this age group needs genetic counseling. This should include the range of diagnostic testing options, as well as the timing of tests and procedures, although the spectrum of chromosomal abnormalities and their phenotypes should be fully discussed.
- The discussion should cover trisomies 21, 18 and 13 as well as sex aneuploidies of 47, xxx and 46, xxy.
- In addition, older gravida women are more likely to have medical problems such as spontaneous abortion, premature separation of placenta, intrauterine growth restriction, pre-eclampsia, Medical problems such as macrosomia (abnormally large baby) and stillbirth may arise.
3) Menstrual History:
- Menstrual history is an important part of the pre-conception interview because it provides information about when ovulation occurs.
- The normal menstrual cycle ranges from 18 to 40 days in two-thirds (2 / 3) of women, with menstruation occurring every 28 days. The interval can be plus or minus 3 days.
Ask questions about the following conditions in a woman whose menstrual cycle is abnormal:
Pubertal milestone,
Diet,
Employment,
Exercise habit,
Use of medication and drugs,
Environmental exposure,
Psychological stress,
Family history of amenorrhea and genetic anomalies, etc.….
Refer to a specialist if the client has irregularity in her menstrual cycle and wants to have a pregnancy.
4) Personal Medical History:
Personal medical history is related to the following medical history.
a) Organic Diseases:
- Certain types of medical conditions can affect both the mother and the baby, of which some medical conditions are more common such as seizure disorders, diabetes mellitus, hypertension, cancer, autoimmune diseases, heart diseases, hematological disorders and HIV disease etc.
b) Seizure Disorder:
- In most cases, seizures do not affect pregnancy, but in about 1/3 of cases, seizure activity may increase during pregnancy due to pregnancy.
- Women with epilepsy should take 4 mg daily instead of 0.4 mg (400) Folic acid is needed when a woman has a condition of epilepsy and should consult a physician before conception.
c) Insulin Dependent Diabetes Mellitus:
- Women who have insulin dependent diabetes mellitus are at risk for severe hypertension, pre-eclampsia, ketoacidosis, excessive amniotic fluid, and conditions such as blindness and renal failure. It can happen.
Fetal and congenital anomalies can also occur. Along with this, the baby can be large (macrosomic) or small i.e. intrauterine growth retardation (IUGR) can also occur.
If the baby is macrosomic, vaginal delivery can be traumatic for both the mother and the baby. And the condition of postpartum hemorrhage (PPH) can also occur.
Women with type II DM (diabetes mellitus) should follow an obstetrician or perinatologist whenever possible.
d) Hypertension:
- Most women with stage I and II chronic hypertension (systolic blood pressure 140/179 mm hg or diastolic BP 90/109 mm hg) are at low risk for cardiovascular complications during pregnancy and most will have good maternal and neonatal outcomes if normal renal function is present.
- Serum creatinine is a marker of renal function and if creatinine level is above 1.4 mg/dl at the time of conception, there may be loss of foetus and increased risk of progression of maternal disease.
Pre-eclampsia, along with chronic hypertension, significantly increases the incidence of fetal growth restriction and placental abruption. In addition, ultrasound examination during pregnancy is important to monitor fetal growth.
E) Cancer:
- Although spontaneous abortions are increased in cancer survivors, the risk of cancer in their offspring is not increased unless the parents are cancer carrier genes.
F) Autoimmune disorders:
- In autoimmune disorders, the immune system turns against itself, leading to severe illness.
Antiphospholipid syndrome and systemic lupus erythematosus (SLE) are two examples of these disorders. - During pregnancy, autoantibodies can cause thrombosis and stroke, as well as conditions such as pre-eclampsia and fetal death.
G) Tuberculosis:
- It is a serious and It is a potentially debilitating disease.
H) Thyroid Disease:
- Fatigue and menstrual irregularities occur in both hypothyroidism and hyperthyroidism.
Weight gain and cold intolerance are both symptoms of hypothyroidism, and weight loss and hot intolerance are both symptoms of hyperthyroidism. - Testing for thyroid disease is important because both hypothyroidism and hyperthyroidism can cause problems for women and their babies.
Pregnant women who do not have proper treatment for thyroid disease may have an increased risk of conditions such as low birth weight and stillbirth.
Hypothyroidism is a rare problem during pregnancy, as long as the woman continues to take thyroid medication (levothyroxine) until she is hypothyroid.
Women with hyperthyroidism are at increased risk of pre-eclampsia and heart failure. Their babies may develop neonatal thyrotoxicosis and die in utero.
I) Heart Disease:
- Pre-conception evaluation can identify any cardiovascular disease.
- Referring a client with cardiovascular disease to a specialist should be considered.
- Because pregnancy is contraindicated in some cardiac diseases.
J) Hematological disorders:
- Some anemias affect the health of both the mother and the child,
e.g. Some thalassemias are associated with: - i Pre-term labor
ii. IUGR
iii Increases fetal loss.
Babies may have severe anemia.
Pregnant women may develop urinary tract infections due to sickle trait.
Women who have hematological problems require consultation with a perinatologist.
Before making a final decision on whether to attempt pregnancy, testing should often be done to identify the nature and extent of the father’s risk to the child.
K)Sexually transmitted infections:
- Perinatal outcomes can be influenced by various sexually transmitted diseases. Infections caused by Chlamydia trachomatis and Neisseria gonorrhoeae can cause P.I. Pelvic inflammatory disease (PID), infertility and ectopic pregnancy, salpingitis The sequelae of this infection can increase the risk of infertility and ectopic pregnancy.
- A single incident of PID increases the risk of ectopic pregnancy in a woman.
If the mother has a condition called gonorrhea and her child is born through vaginal delivery, the risk of blindness in the child increases.
If left untreated, chlamydia can cause both conjunctivitis and pneumonia.
Women with herpes infection are at risk of neonatal herpes infection 40%. - The AIDS epidemic has not bypassed pregnant women, women are 8 times more likely than men to come into contact with HIV during intercourse.
Decisions about pregnancy in women who are HIV positive are extremely personal and complex.
5) Obstetric history:
- Information about previous pregnancies should be obtained to identify recurrent complications in subsequent pregnancies.
- This information often provides an opportunity to discuss fears or concerns about the new pregnancy, as well as emotional responses and reproductive problems. In which the following information is collected.
- Such as:
- Birth date, miscarriage, gestational age –>
- To identify prolonged labor, birth weight, sex of children, any complications during pregnancy, current health status of the child, whether the child is alive or not is discussed.
- a)Smoking
- b)Alcohol
- C)Illegal Drugs
- When the baby is in the uterine cavity, if the mother smokes half a pack of cigarettes a day, then the uteroplacental perfusion in the child may decrease and the child’s weight may also decrease compared to its normal weight.
- Children born in homes where people smoke have long-term effects. These include Sudden Infant Death Syndrome (SIDS), meningococcal disease, pneumonia, asthma, bronchitis, colds and ear infections. Includes.
- Women who smoke and are thinking about conception should stop smoking before conception.
- Pregnant women who have at least one or more drinks per day have a two-fold increase in spontaneous abortion.
Women who Those who drink during pregnancy are also at risk of the following risks to their children: - a) Fetal Alcohol Syndrome
b) A Syndrome of Abnormal Facial Features
c) Behavior Problems
d) Intellectual Handicaps - Preconception counseling helps the client to quit this habit.
- To identify barriers to quitting smoking such as living with a smoker. Offer them a treatment plan and provide psychological support and reassurance.
6)Risk to Health/ Personal History:
•>
a) Smoking:
b) Alcohol:
C) Illegal drugs:
- Medications used during pregnancy can cause problems during pregnancy, at birth, and in childhood. All women should be asked about past and present use of medications. You should specifically ask about marijuana use.
7) Over the Counter Drugs:
- Most pregnant women are aware that some medications are harmful to the growing baby.
Few women are concerned about the teratogenic effects of over-the-counter drugs and herbs. - For example, many women are unaware that vitamin A in amounts greater than 10,000 IU per day, when taken during the first 7 weeks of pregnancy, contributes to cranial neural crest defects. The effectiveness and safety of most herbal products are unknown.
8) Environmental exposure:
- Exposure to toxic elements in the environment can occur at work, at home, or during play.
- Women should obtain proper information about whether they have been exposed to any of the following products, such as:
- •Carbon monoxide,
- •Volatile organic compounds (VOCs) from furniture, paint, carpets, and office equipment,
- •Mold and bacteria from heating, ventilation, and air conditioning (HVAC) systems,
- •Smoke from people smoking cigarettes at the entrance of a building that is drawn back into the building when the doors are opened.
- •In carbon-less copy paper Possible carcinogens.
- •Pesticide sprays etc.
9) Psychological history:
- Preconception counseling is used to identify stressors and support sources, such as,
- Poverty,
- Inadequate housing,
- Relationship problems,
- History of abuse,
- Depression,
- Poor self-esteem,
- Low level of Education,
- High level of stress etc.
10) Family History:
- Collecting family history can identify the risk of birth defects in the child and the risk of any inherited disorders that may appear later in life.
- Family history can identify race/ethnicity, medical and obstetric problems.
If risk factors are identified, refer them for genetic counseling. - Preconception care is important for maternal and child health.
- b) Genetic counseling:
Genetics:
- The science related to heredity and variation is called genetics and the science of studying the structure and behavior of genes is called genetics.
Genetic Counseling:

- Genetic counseling is a process that is carried out by medical experts. In which genetic tests are performed and family history is taken and medical records are reviewed by experts, the aim of which is to identify whether there is a possibility of parents passing on any genetic disorder to their child.
In genetic counseling, parents are provided with education about genetic disorders.
Also, they are provided with psychological support and information about support groups and services. - Genetic counseling is a clinical genetic service that includes the provision of genetic information, education, and support to individuals and families with concerns and problems related to genetic health.
- The term ‘genetic counseling’ was first used by ‘Sheldon Reed’ in 1947.
•> According to American Society of Human Genetics (1975):
Genetic counseling is a communication process. It is related to human problems. In this process, one or more trained persons help the person and family:
- Understand the medical facts, including the diagnosis, probable course of the disorder, and available management.
- Appreciate how heredity contributes to the disorder and the risk of recurrence in specific relatives.
- Understand alternatives to the risk of recurrence in specific relatives.
- To make the best possible adjustment in affected family members. Genetic counseling is a screening procedure to identify high-risk individuals and their children for genetic abnormalities. The main purpose of genetic counseling is to help the patient and her husband make decisions about the future management of the pregnancy. Its objectives are to provide information, assist in counseling, and help the couple adjust to the problem. Thus, reducing the chances of giving birth to a genetically defective baby. Benefits of Genetic Counseling for Pregnancy Planning.
- Interested in prenatal diagnosis.
- Concerned about the results of first and second trimester screening.
•Known to be at risk of carrying a genetic disorder such as cystic fibrosis, muscular dystrophy, hemophilia, sickle cell disease or thalassemia. - Will be 35 years of age or older at the time of pregnancy and delivery. Implications of Genetic Counseling
- Previous miscarriage or pregnancy loss, or a family history of a parent diagnosed with or having a birth defect, genetic disorder, or mental retardation.
- Previously having a child with a birth defect, genetic disorder, or mental retardation. Laboratory tests such as maternal serum screening tests that indicate an increased risk for genetic disorders.
- A woman may have been exposed to certain medications or drugs, radiation, and infections during her pregnancy. Common Genetic Conditions: Genetic disorders arise due to abnormalities in a person’s genetic material. Mainly genetic disorders are differentiated into four types:
Such as,
1) Changes in single gene
2) Changes in multiple genes
3) Chromosomal changes:
Entire areas of chromosomes are missing or misplaced.
4) Mitochondrial:
Maternal genetic materials in mitochondria can also be mutated.
Common disorders are as follows:
1) Cystic fibrosis,
2) Down syndrome,
3) Fragile-X syndrome,
4) Inherited Clotting problems,
5) Familial combined hyperlipidemia and familial hypercholesterolemia,
6) Huntington’s disease,
7) Muscular dystrophies,
8) Sickle cell anemia,
9) Thalassemia,
10) Mutations affecting biochemical pathways,
11) Turner syndrome,
12) Alpha 1 antitrypsin deficiency,
13) Myotonic dystrophy,
14) Parkinson’s disease,
15) Alzheimer’s disease,
•>
1) Cystic fibrosis :
- Cystic fibrosis a It is a common inherited disease in Caucasians and is caused by a deficiency of a protein that controls the balance of chloride in the body.
- It causes difficulty breathing and frequent lung infections. It also causes problems with digestion and reproduction. Symptoms range from mild to severe.
- Both parents must be carriers for a child to be affected. After that, each child has a 25% (1 in 4) chance of being affected.
2) Down syndrome:

- Down syndrome is a common chromosomal abnormality in which there is an extra copy of a gene on chromosome number 21.
Down syndrome affects about 1 in 800 to 1000 newborn babies. It can be detected through prenatal testing.
It has a pattern of symptoms that are visible immediately after birth, such as,
•Facial characteristics,
•Decreased muscle tone,
•Defects in the heart and digestive system,
•Developmental delays. - Down syndrome can range from mild, moderate, and severe and is associated with the increasing age of the mother.
3) Fragile-X syndrome (Fragile-X syndrome):
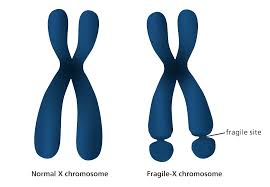
- Fragile-X syndrome is the most common type of inherited developmental delay and mental retardation. It is characterized by developmental delay and cognitive difficulties that range from mild to severe and may sometimes be associated with autism.
- Approximately 1/1500 males and 1/2500 females have fragile X syndrome, a condition in which part of the X chromosome is broken. The region on the X-chromosome that causes fragility
- It can be repeated on the chromosome – the greater the number of repeated areas, the greater the fragility and the more serious the syndrome.
4) Inherited clotting problem :

- The process of blood clotting is one of the most complicated biochemical pathways in the body, and there are different inherited clotting problems.
- These clotting problems can result in excessive bleeding and abnormal clotting throughout the body, usually in the veins.
- The most common factor V Leiden is an abnormality that occurs especially during pregnancy and can cause pre-eclampsia, small for gestational age, stillbirth, and placental problems.
Other inherited clotting problems include prothrombin deficiency, protein S deficiency, protein C deficiency, and antithrombin III deficiency.
Hemophilia is a non-violent clotting disorder. The most common types are hemophilia A (caused by a deficiency of clotting factor 7) and hemophilia B (caused by a deficiency of clotting factor 9).
Symptoms include excessive bleeding from the gums, nose, gastrointestinal system, and joints. Abnormal menstrual bleeding occurs. Excessive bruising and skin rashes also occur.
5) Familial combined hyperlipidemia and familial hypercholesterolemia (Familial combined hyperlipidemia and familial hypercholesterolemia):
- This is an inherited disorder in which the amount of lipids and cholesterol in the blood increases.
6) Huntington’s Disease :
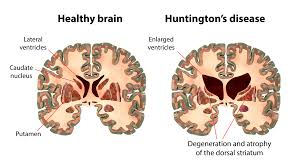
- This is an inherited disorder in which some nerve cells in the brain and central nervous system degenerate. Its symptoms include,
Behavior changes,
Unusual snake-like movements (chorea),
Uncontrolled movements,
Walking difficulties,
Loss of memory,
Changes in speech and cognitive function,
Swallowing difficulties. - Huntington’s disease is an autosomal dominant disorder, meaning that if one parent has Huntington’s disease, then there is a 50% chance of their offspring developing the disease.
7) Muscular dystrophies :
Muscular dystrophy is an inherited disorder in which weakness is seen in the muscles. is.
a) Becker muscular dystrophy:
- In Becker muscular dystrophy, the symptoms are similar to those of Duchenne muscular dystrophy but appear later and worsen more slowly. The symptoms involve:
i )Fatigue
ii)Possible mental retardation
iii )Muscle weakness starting in the legs. - The muscle weakness in the upper body is not as severe as in Duchenne. Again, boys are more likely to develop this disorder and are confined to a wheelchair by the age of 25-30.
b) Duchenne muscular dystrophy:
- Here, symptoms usually appear before the age of 6 and can appear even earlier.
- Its symptoms include
fatigue,
mental Retardation,
Muscle weakness starting from the leg and radiating to the upper body,
Heart problems,
Respiratory problems, etc…
8) Sickle cell anemia (Sickle cell anemia) :
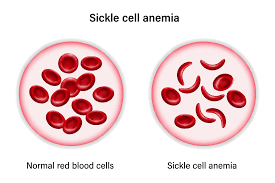
- “Sickle cell anemia” is a severe hemolytic anemia and a hereditary and genetic blood disorder that normally affects red blood cells, in which the red blood cells take on an abnormal sickle shape. In this disease, red blood cells become rigid, sticky, and abnormally shaped like crescents and sickles. The abnormal shape of these red blood cells blocks blood flow, which causes pain, organ damage, and an increased risk of infection. The life span of sickle-shaped red blood cells is only 30-40 days and their oxygen-carrying capacity is also decreased.
Its cause is due to a genetic mutation.
It is a hereditary condition.
It is caused by a family history of sickle cell disease. - Symptoms such as,
mild jaundice,
fever,
headache,
fatigue,
weakness,
skin, conjunctiva, and mucus Membrane becomes pale,
Shortness of breathing,
Dizziness,
Vision problems,
Leg ulcers,
Speech becomes absent,
Pain episodes occur,
Headache,
Rapid and irregular heartbeat,
Hands and feet become cold.
Nails become brittle.
Poor concentration.
Cognitive difficulties occur.
Growth and development delay occurs.
Loss of appetite.
Dizziness.
Tachypnea.
Tachycardia.
Palpitation.
Diarrhea and vomiting occur.
Cardiac enlargement with murmur sound.
Some In cases, jaundice, petechiae and ecchymosis may also be present.
Hepatomegaly may occur.
Irritability may occur.
Tiredness may occur.
Pneumonia may occur.
Traumatic rupture of an enlarged spleen may occur.
9) Thalassemia:
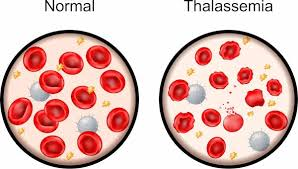
- Thalassemia is a group of hereditary hemolytic anemias. Which is an autosomal recessive genetic disorder in which the synthesis of hemoglobin is reduced/inadequate amount of production occurs. Thalassemia is a genetic blood disorder in which the body does not produce enough amount of hemoglobin (protein in red blood cells that carry oxygen into the body). In this, red blood cells are destroyed in large amounts due to which the condition of anemia arises.
Causes of Thalassemia:
- Due to genetic mutation,
- Due to impairment in alpha globin and beta globin.
Due to family history.
Its signs and symptoms include,
Fatigue,
Pale skin, conjunctiva and mucous membranes,
Shortness of breath,
Spleen and liver enlargement (hepatosplenomegaly),
Jaundice,
Growth and development delay,
Bone abnormalities,
Heart problems
Endocrine complications,
Infections.
Loss of appetite (anorexia),
Poor feeding habits,
Abdominal distension,
Failure to thrive,
Facial features – upper maxilla hypertrophied, exposing of upper teeth, depressed nasal bridge,
Mal occlusion of teeth,
Lymphadenopathy or hypogonadism,
Osteoporosis of
metacarpals and metatarsals.
Recurrent respiratory infections,
Lymphnode enlargement,
Poor nutritional status.
10) Mutation affecting biochemical pathways :
Phenylketonuria (PKU)

- Phenylketonuria (PKU) is the result of a deficiency of a liver enzyme that is needed to convert the amino acid phenylalanine into another amino acid, tyrosine. If it is not detected, phenylalanine accumulates in early, relatively high levels and causes mental retardation, brain damage, and seizures.
- Treatment includes a phenylalanine-restricted diet and the use of the cofactor tetrahydrobiopterin (BH₄) to reduce the amount of phenylalanine in the blood.
11) Turner syndrome syndrome):
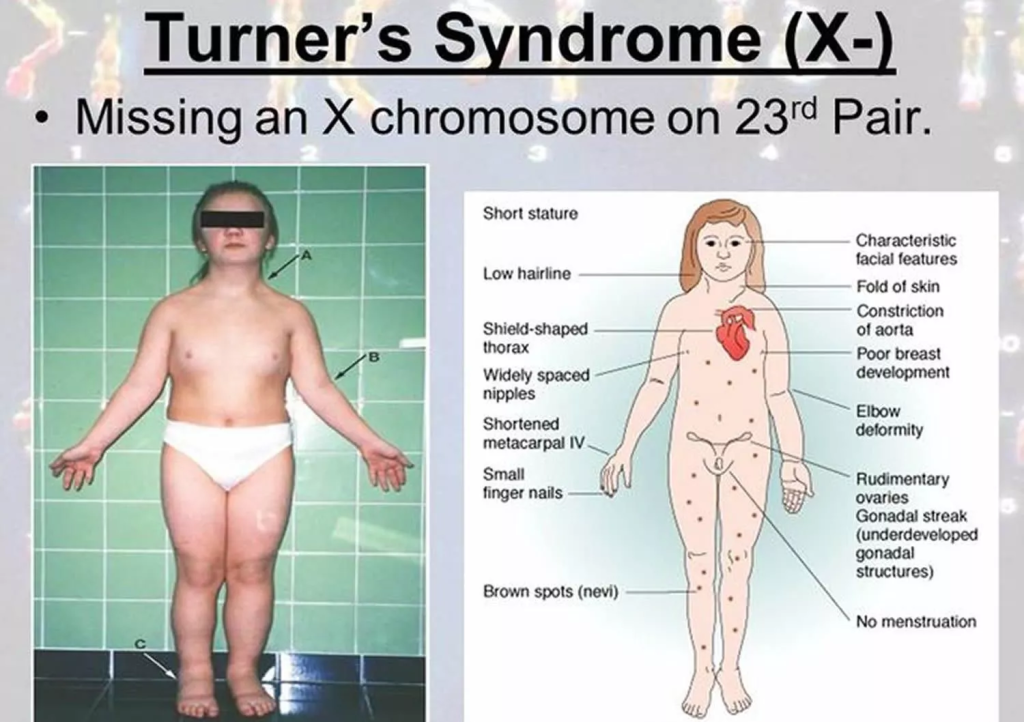
- Turner syndrome is a chromosomal condition that affects female development.
- Women with this condition are smaller than normal and are usually unable to conceive a child (infertile) due to the absence of ovarian function.
- A chromosomal disorder in which a woman is born with only one X chromosome. Turner syndrome results from a missing or incomplete sex chromosome, meaning the absence of one X chromosome.
Among its symptoms,
- Extra skin may be seen on the neck area,
- Swelling in the arms and legs (lymphedema).
- Skeletal abnormalities
- Heart defects
- Kidney problems
- Developmental Delay
- Learning disability
- Symptoms such as behavior problems are seen. 12) Alpha 1 Antitrypsin Deficiency: Alpha-1: Antitrypsin deficiency describes a decrease in the amount of alpha-1 antitrypsin in the lungs and blood. This results in lung diseases such as emphysema. Its early symptoms include:
•Shortness of breath.
•Wheezing
•Weight loss - Frequent respiratory infections
- Fatigue
- Symptoms such as rapid heart beat are seen. 13) Myotonic Dystrophy: Myotonic Dystrophy is an inherited disorder of the muscles and other body systems.
This is the most common muscular dystrophy seen in adults
- There are two types of muscular dystrophy as follows:
1) Myotonic Dystrophy Type-1
2) Myotonic Dystrophy Type-2 - The following symptoms are seen in it,
- Progressive muscle wasting and weakness are seen especially in the lower legs, head and neck and face.
•Clouding of the lens of the eye. - Heart abnormalities etc.
14) Parkinson’s Disease:
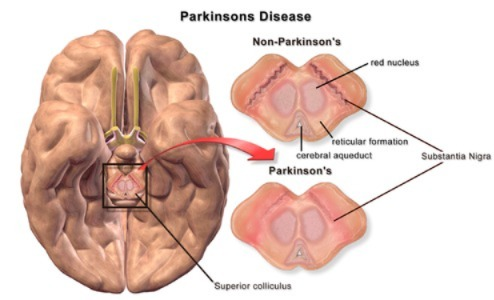
- Parkinson’s disease is a chronic, progressive, neurological disorder in which the muscles No control, movement, and balance are disturbed. Parkinson’s disease is a slow, progressive neurological movement disorder that can also result in disability.
Parkinson’s disease is a type of movement disorder. In which a person’s muscle movements are altered. - Parkinson’s disease was first described in 1817 by London surgeon James Parkinson.
There are 3 main cardinal signs of Parkinson’s disease.
1) Tremor:
2) Muscle rigidity:
3)Bradykinesia
1) Tremor:=Shaking,
- Voluntary movements are seen in fingers, hands, feet, etc. Tremor is mainly seen when the person is in the resting stage. But it is not seen when the person is in a task. Tremor occurs when a person is excited, tense and stressed.
2) Muscle rigidity:=stiffness,
- In this, stiffness occurs in the limbs and trunk. This stiffness increases during movement. Rigidity causes pain and ache in the muscles.
3)Bradykinesia
- Bradykinesia is a slowness of voluntary movement. Sometimes there is difficulty in movement. In bradykinesia, there is stiffness in the facial muscles, due to which a “mask-like” appearance is seen.
- Its symptoms include
tremors,
muscle rigidity,
bradykinesia,
postural instability,
difficulty in speech and swallowing.
sleep disturbances.
mood and cognitive changes.
constipation.
memory loss.
difficulty in swallowing.
problems in speech.
depression.
anxiety.
stress Come.
Confusion.
Memory loss.
Dementia.
Sense of smell is diminished.
Sweating increases.
Skin problems.
Impairment in speech.
Urinary frequency and urgency.
Loss of spontaneous movement.
Symptoms like these are seen
15) Alzheimer’s disease
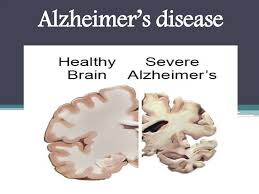
- Alzheimer’s disease is a progressive neurological disorder.Alzheimer’s disease It is also called senile dementia of Alzheimer’s type (SDAT).
- Alzheimer’s is the most common form of dementia (the inability to remember anything, whether short-term or long-term).
Alzheimer’s disease causes impairment in a person’s memory, judgment, language, cognitive function, and daily living activities. In Alzheimer’s dementia, brain cells are first destroyed, which leads to mental disorders. - Alzheimer’s disease primarily affects older adults. This leads to impairment in a person’s memory, cognitive function, behavior, and daily routine activities. In this disease, mainly due to the accumulation of protein in the brain, brain cells are first destroyed, due to which the neural pathway breaks down and the person experiences mental disorders.
- Among its symptoms,
Memory loss.
Difficulty in solving tasks.
Confusion.
Disorientation in time, place, and person.
Changes in mood and behavior.
Language problems. Declining judgment.
Impairment in solving tasks.
Memory loss.
Confusion.
Problems in daily living activities.
Problems in dressing and eating.
Changes in personality. Other symptoms are seen.
Nursing Activity in Genetic Counseling:
- The nurse refers the patient to a genetic specialist, contacts them, and participates in genetic counseling.
- Collects family history, prenatal, and health history
- Assess genetic conditions in family members.
- Helps family members understand genetic conditions.
- Refers clients for genetic evaluation and counseling when needed.
- Formulates a plan of care with family members and coordinates with other health care professionals.
- Provides education about the benefits and risks of genetic testing and available testing to families.
- Maintains privacy and confidentiality of family records and information.
- Provides families with information on early child stimulation programs, genetic resources, and support groups.
- Provides follow-up care and support for the child throughout their life.
- Provides support for the genetic counseling process to patients and families.
- Provides genetics-related health care through national support resources for relevant communities.
C) Physiological Changes in Pregnancy:
- Pregnancy is a condition that lasts from the time of conception to the time of delivery. Due to certain types of specific hormones, physiological changes are observed in the mother’s body during pregnancy. These changes are made to develop the fetus, prepare the mother’s body for labor, and produce the best milk during the postpartum period.
1) Changes in the reproductive system:
A)Vulva:=
- The vulva becomes more edematous and vacuolated.
- Superficial varicosities (varicose veins: = veins that become enlarged and swollen, usually in the legs and also in the pelvic area during pregnancy) are also seen in multiparas and the labia minora become pigmented and hypertrophy (increase in the size of the organ) occurs.
B) Vagina:=
- The vaginal wall becomes hypertrophied, edematous and more vascular.
- The increased venous blood supply to the vaginal wall results in a bluish coloration of the vaginal mucosa, which is called the “Jacquemier sign”.
The length of the anterior wall increases.
The vaginal secretion is more acidic, thin and curdy white.
The acidic pH of the vaginal secretion prevents the multiplication of pathogenic microorganisms.
(C) Uterus:=
- The uterus grows significantly during pregnancy. The weight and length of the uterus also increase during pregnancy.
- Weight of Uterus:
In the non-pregnant state, the weight of the uterus is about 60 gm, which increases to 900 – 1000 gm during pregnancy. - Length, Width and Thickness of Uterus:
- In the non-pregnant state, the weight of the uterus is about 60 gm. ,
- Length := 7.5 cm ,
Width :=5 cm and Thickness : = 2.5 cm.
While during pregnancy (at term) the length of the uterus is
= 30-35 cm ,
Width := 22.5 cm and
Thickness := 20 cm. - Volume of uterine cavity:
In non-pregnant state the volume of the uterus is 10 ml which During pregnancy (at term) its volume increases by 5 liters. - Body of uterus:
The body of the uterus grows and enlarges. - Muscles
- 1) Outer:= Longitudinal layer
2) Middle:= Vascular layer
3) Inner:=Circular layer - Hypertrophy (increase in size) and hyperplasia (increase in number) are seen in the muscles.
- After 20 weeks of pregnancy, the length of the uterine muscle fibers increases and the uterine wall becomes thinner, due to which the uterus becomes softer and more elastic in the gravid condition than in the non-gravid condition.
- Vascular system:
Blood supply starts to increase from 20 weeks due to vasodilation caused by estradiol and progesterone.
The diameter of the uterine arteries doubles and blood flow increases and veins dilate. Dilates. - During pregnancy, the endometrium of the uterus is called decidua.
- Braxton Hicks Contractions:
- In the beginning of pregnancy, the uterus contracts on its own. They are irregular, infrequent, spasmodic and painless, due to which there is no effect on the dilation of the cervix. They increase towards the term (37-42 weeks) and finally Mixed with painful contractions of labor.
D) Isthmus:=
- During pregnancy, the lower segment of the uterus forms an isthmus.
- In the non-pregnant state, the length of the isthmus is 0.5 cm, which increases significantly during pregnancy to 7.5 cm-10 cm.
- The muscle fibers of the isthmus are arranged circularly in the lower segment and form a sphincter-like structure, due to which the fetus stays in the uterus during early pregnancy. Helps. If this sphincter is incompetent, abortion can also occur.
E)Cervix:=
- During pregnancy, the cervix becomes vascular, edematous, and hypertrophied and hyperplastic.
- The cervix becomes soft, which is called “Goodell’s sign”.
- The length of the cervix doubles and its volume also increases.
F) Fallopian tubes:=
- The length of the fallopian tubes increases to a small extent. The tubes become congested. Muscles hypertrophy and epithelium becomes flat.
G)Ovary:=
- Ovulation stops during pregnancy. The ovary becomes hypertrophied and vascularized.
- The corpus luteum, which was the usual menstrual cycle, continues to enlarge by about 2.5 cm for 8 weeks and is caused by changes in the fertilized ovum (trophoblast) and helps in hormone production. By the 12th week, colloid degeneration occurs and the tissue becomes calcified. The corpus luteum produces estrogen and progesterone hormones and provides an environment to maintain the ovum until the placenta starts to act.
H) Brest (Breast) :=
- During pregnancy, due to the effects of estrogen and progesterone, the size, nodularity and sensitivity of the breast increase along with the increase in vascularity.
- The nipples become enlarged, dark and erectile.
- 5 to 15 sebaceous glands that are invisible in the non-pregnant state Hypertrophy is seen, which is called “Montgomery tubercles”. It is located around the nipple and its secretion keeps the nipple and areola moist and healthy.
- The areola becomes dark and pigmented and is called the primary areola.
- In the second trimester, a second pigmented zone forms around the primary areola, which is called the secondary areola.
- During the first three months, the growth of the ductal system in the breast increases, and as the pregnancy progresses, its alveolar cells become secretory.
- The total weight of the breast is about 0.4 kg.
- The breast enlarges due to alveolar proliferation and fat deposition, and a clear sticky fluid can be squeezed out of the breast at about 12 weeks.
- By 16 weeks, this clear sticky fluid becomes thick and yellow, which is called colostrum, and is an important sign of pregnancy.
Changes in other systems of the body.
1) Skin Changes:=
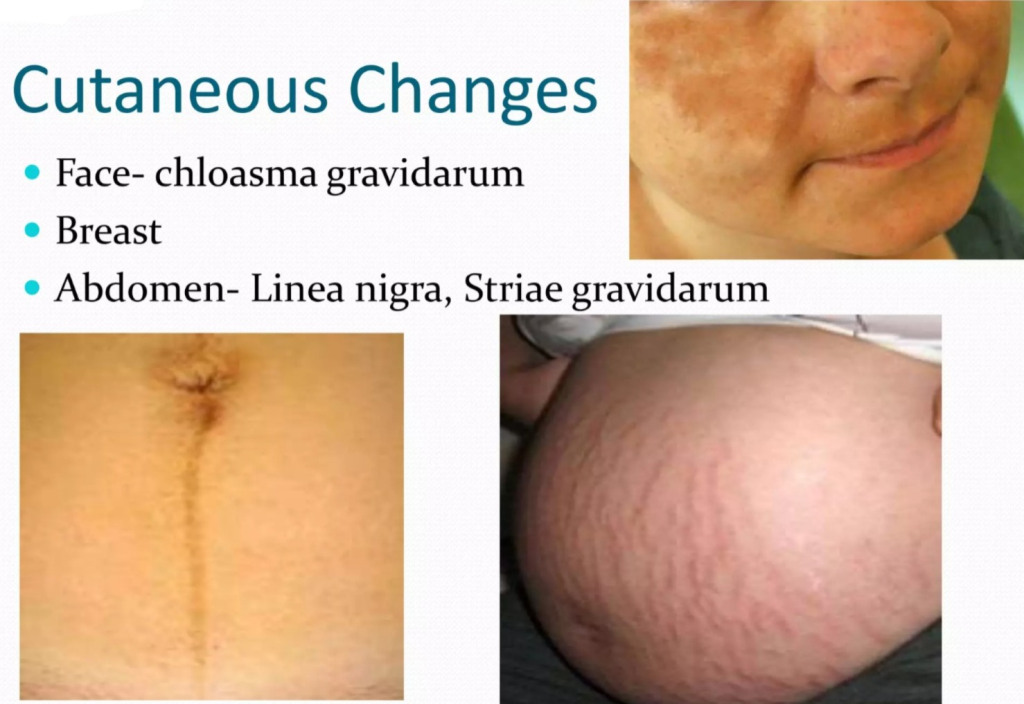
- A) Face:
Pigmentation is seen around the cheeks, forehead and eyes, which is called “graviderum in close proximity” or “pregnancy mask”, which disappears on its own after delivery. - B) Breast:
Visible pigmentation changes occur in the breasts. - C) Abdomen:
- Linea Nigra
Due to melanocyte stimulating hormone, a brownish black line becomes visible in the midline from the zyphisternum to the symphysis pubis, which is called linea nigra. - Straya Graviderum
Depressed linear marks are seen on the abdominal wall from the umbilicus down and sometimes on the breasts, which are initially pink but become glistening white after delivery, which are called striae albicans or striae graviderum.
High estrogen levels Vascular spider and palmar erythema are seen. Mild degree of hirsutism (excess hair) is seen on the skin and excess amount of hair is lost during the purpura period.
2) Weight gain
- Weight loss occurs during the early weeks of pregnancy due to nausea and vomiting. Weight gain is progressive from month to month.
A healthy woman gains an average of 11 kg (24 lbs) during pregnancy. - The amount of weight gain is.
- A) Reproductive weight gain
- During 1st trimester: 1kg,
2nd trimester: 5kg,
During 3rd trimester: 5kg, - 1) Weight of fetus: 3.3kg,
2)Weight of placenta: 0.6kg,
3)Weight of liker: 0.8kg,
4) Weight of uterus: 0.9kg,
5) Weight of breast: 0.4kg. - B) Net maternal weight gain
- 1) Increase blood volume:=1.3kg,
- 2) Increase extra Cellular fluid:=1.2kg,
- 3) Fat and protein:=3.5kg.
3) Cardiovascular system
- A) The heart has to work harder during pregnancy.
Cardiac volume increases by 10% but there is no change in ECG. No.
Cardiac output also increases due to increase in heart rate and stroke volume.
Pulse rate also increases.
Platelet count slightly decreases due to increase in concentration rate of 40 to 45 mm. - B) Blood pressure and blood volume:
- Blood pressure remains within normal limits. In some women, diastolic pressure drops by 5 to 10 mm during mid-pregnancy.
- C) Venous Pressure:
The pressure of the gravid uterus on the pelvic veins increases the femoral venous pressure by about 10 cm. After that, the blood volume also increases, the volume of red blood cells and the plasma volume also increase, and the blood flow increases in many parts of the body such as the uterus, pulmonary, renal, skin, and mucosa.
4) Respiratory System
- Hyperemia (increased blood flow) and congestion are seen in the upper respiratory mucosa.
- Oxygen intake also increases due to increased inspiration and oxygen supply to the fetus also increases.
- Carbon dioxide is released due to increased expiration, so due to low maternal carbon dioxide, carbon dioxide can be easily transferred from the fetus to the mother’s blood.
- In the last trimester of pregnancy In the weeks following the pregnancy, the pressure of the gravid uterus on the diaphragm causes complaints of breathing difficulty, which is relieved by lightening.
5) Digestive System
- Due to the effect of progesterone, the muscle tone of the gastrointestinal system decreases.
- Due to the relaxation of the cardiac sphincter Regurgitation of stomach contents and heartburn occur.
- As the gastric size decreases, it empties slowly, which continues even in labor.
- In many women, the gums become spongy and vascular, which can cause bleeding during brushing.
- The decrease in the size of the intestine leads to better absorption of food and constipation.
6) Nervous System
- Mood changes occur during pregnancy and the postpartum period. Psychological conditions include nausea, vomiting, mental irritability, and insomnia.
- Depression or psychosis can also develop in women.
- Compression of the median nerve in the wrist can cause numbness in the hands and arms. Pain and paresthesia (tingling) are common in the last months of pregnancy, which is called carpal tunnel syndrome. Similarly, sensory loss is seen in pregnancy due to cutaneous nerve pressure.
7) Urinary Tract
- Frequent urination is common in early and late pregnancy.
- Stress Incontinence may also occur.
- Dilitation of the uterus and pelvis continues from early pregnancy to mid-pregnancy, leading to urinary stasis and infection. Renal function also increases during pregnancy.
8) Locomotor system
- Due to the relaxin hormone in pregnancy Backache is common due to lordosis and relaxation of joints.
Leg cramps occur due to weight on the sacral and lumbar plexuses and difficulty in walking also occurs. - Thus, physiological changes are seen in women during pregnancy.
- Uterine Fundal Height at Different Weeks During Pregnancy:
- Non-Pregnant Uterus Pyre Shape (Pear-like) Uterus During 12 Weeks of Pregnancy Globular shape is formed.
The uterus enlarges again during the 28th week and becomes pyrexia foam.
And after the 36th week of pregnancy, it becomes spherical.
•> At 12 Weeks of Pregnancy:
- During 12 weeks of pregnancy, the uterus is no longer anteverted and anteflexed. The fundus is palpated abdominally over the symphysis pubis.
•> At 16 Weeks of Pregnancy:
- During the 16th week of pregnancy, the uterus is ovoid in shape. The uterus is located between the symphysis pubis and the umbilicus.
•> At 20 Weeks of Pregnancy:
- During the 20th week of pregnancy, the fundus of the uterus is two fingers below the umbilicus.
•> At 24 Weeks of Pregnancy:
- During the 24th week of pregnancy, the fundus of the uterus is at the level of the umbilicus and one finger below it.
•> At 30 Weeks of Pregnancy:
- During the 30th week of pregnancy, the fundal part of the uterine cavity is located between the umbilicus and the zygosternum
•> At 36 Weeks of Pregnancy:
- During the 36th week of pregnancy, the fundal part of the uterine cavity is at its highest level, i.e. up to the zygosternum
•> At 38 Weeks of Pregnancy:
- During the 38th week of pregnancy, the fundus part of the uterine cavity descends and reaches the level of 34 weeks, which is called lightening.
•> At 40 Weeks of Pregnancy:
- During the 40th week of pregnancy, the fundus of the uterine cavity reaches the level of 32 weeks and then the lower uterine segment relaxes and stretches while the cervix becomes soft and short and the uterus is ready for labor.
d) Diagnosis of Pregnancy:

Introduction:
- The ability of the mother to reproduce begins with menarche and ends with menopause. Reproductive age normally ranges from 13 years to 45 years.
Gestational age:
- The normal average duration of pregnancy is 9 months and 7 days, starting from the first day of a woman’s last menstrual period (LMP), i.e. 280 days or 40 weeks.
True Gestational Age:
- Fertilization occurs 14 days before the expected missed period. Thus, the true duration of pregnancy is calculated by subtracting 14 days from 280 days, i.e. 266 days. This age is called the fertilization age and the ovulatory age.
- A woman’s antenatal period usually starts from the first day of the last menstrual period (LMP) until the start of true labor.
- The total duration of pregnancy is 38 – 40 weeks, which is divided into three trimesters. It involves about 13 weeks or 3 months in one trimester.
1) Pregnancy
- First trimester:= First 12 weeks,
- Second trimester:= 13 to 28 weeks,
- And third trimester:= 29 to 40 weeks Involvement occurs.
•> Objective and subjective signs of pregnancy:
First trimester (1- 12(1-3 months) week):
Subjective signs:
- Amenorrhea,
- Morning sickness,
- Frequency of micturition,
- Breast discomfort,
- Fatigue
Amenorrhea:
6 weeks after the last menstrual period during the reproductive period in healthy married women Amenorrhea is mostly due to pregnancy.
Morning sickness:
In this, the mother mostly experiences nausea and vomiting.
Frequency of micturition:
Frequency of micturition is seen during the 8th to 12th week of pregnancy due to the pressure of the bulky uterus on the bladder.
Breast Discomfort:
During the 6th to 8th week, there is discomfort due to a fullness sensation in the breasts.
Fatigue:
These symptoms are seen during early pregnancy and are experienced by many pregnant women.
Objective Sign:
- Breast Changes,
- Changes on the Abdomen and Pelvic,
- Immunological Tests
Breast Changes:
Breast changes are more clearly seen in primigravidas.
These breast changes occur between 6 and 8 weeks.
Delicate under the skin Veins appear and the breast enlarges. The nipple and primary areola become more pigmented. The Montgomery tubercles become prominent and a yellowish secretion (colostrum) can be expressed from 12 weeks of pregnancy. Abdominal and pelvic changes: The uterus remains a pelvic organ until 12 weeks of pregnancy and then the uterus becomes a suprapubic organ on the abdomen. Feels like a bulge.
Pelvic Changes:
These changes are varied and appear at different times.
1)Jacquemere sign, Chadwick sign,
2) Vaginal sign (Osiander sign),
3)Cervical sign (Goodell sign),
4)Uterine sign (Picksack sign),
5)Hagar sign,
6) Palmer sign.
1) Jacquemier’s sign:
The vaginal wall becomes hypertrophied, edematous, and more vascular.
Bluish discoloration of the vaginal mucosa is seen due to increased venous blood supply to the vaginal wall, which is called “Jacquemier’s sign”.
•> Chadwick’s sign:
This sign is seen during the 8th week of pregnancy. It involves bluish discoloration of the cervix, vagina, and labia minora due to local vascular changes. Which is called “Chadwick’s sign”.
2) Vaginal sign (Osiander’s sign):
Bluish discoloration in the anterior vaginal wall, softening of the anterior vaginal wall, and non-irritating mucoid discharge are seen from 6 weeks.
Along with this, palpation is felt through the lateral fornix during 8 weeks, which is called “Osiander’s sign”.
3) Cervical sign (Goodell Sign):
Cervical sign is seen during 6 weeks of pregnancy.
In which the cervix is vascular, edematous and hypertrophied and hyperplasia occurs.
In which the cervix becomes soft it is called “Goodell sign”.
4)Uterine sign:
Size, shape and consistency:
At 6 weeks the uterus is the size of a hen’s egg, at 8 weeks it is the size of a cricket ball, and at 12 weeks it is the size of a fetal head.
No The pyriform septum in the non-pregnant stage becomes globular by 12 weeks. The uterus becomes soft and elastic.
Pisksek sign:
If lateral implantation occurs in the uterus, there may be symmetrical enlargement of the uterus. This is called the “Pisksek sign”, where one half is firmer than the other.
5) Hegar sign:
Hegar sign is seen between 6-10 weeks.
In which the upper body part of the uterus enlarges due to the growing fetuses.
The lower segment of the uterus becomes soft due to increased vascularity.
In this, there is cyanosis and softening of the cervix which is called “Hegar sign”.
6) Palmer’s sign:
In Palmer’s sign, regular and rhythmic contractions of the uterus occur during bimanual examination of the uterus between 4 and 8 weeks. It is called “Palmer’s sign”.
Immunological Test for Diagnosis of Pregnancy:
Pregnancy test is based on the presence of antigen (HCG) in maternal urine or serum.
- Ex: Agglutination Inhibition Test
- One drop of urine is mixed with one drop solution containing human chorionic gonadotropin (HCG) antibody
- If human chorionic gonadotropin is not present in the urine (the woman is not pregnant), then the antibody will be free.
- Now take one drop solution in which latex particles are coated with human chorionic gonadotropin Yes,
- If agglutination occurs, the pregnancy test is negative.
- Human chorionic gonadotropin (HCG) binds to the available antibodies if present in the urine. Now take one drop of solution in which latex particles are coated with human chorionic gonadotropin trophin, then no agglutination occurs because it binds the available antibody, hence the pregnancy test is positive.
Ultrasonography:
Fetal viability and gestational age are determined by transvaginal sonography.
2) Second Trimester (13 to 28 weeks (4-7 months)):
Subjective Symptoms:
- Most often nausea, vomiting and frequency of urination occur and amenorrhea remains continuous.
- New features appear such as quickening (a woman feels active fetal movement around 16 weeks in multiparas).
- It is mostly felt at 18 weeks in primiparas, which provides accuracy in calculating the expected date of delivery.
- Progressive enlargement of the lower uterus occurs.
Objective Symptoms:
- 1)General Examination,
- 2)Abdominal Examination,
- 3)Vaginal Examination,
- 4)Investigations.
1)General Examination:
a) Close:
- 24th week A pigmentation appears on the face, forehead and cheeks.
b) Breast Changes:
- Breast enlargement occurs with prominent veins.
Secondary areola appears during the 20th week. - Colostrum becomes thick and yellowish by the 16th week.
Striae appear in varying degrees with advanced weeks.
2) Abdominal Examination:
a) Inspection,
b) Palpation,
c) Auscultation.
a) Inspection:
- 20th week to linea nigra (brownish from symphysis pubis to nciform cartilage) Pigmented lines of color appear). Straia gravidarum is seen on the lower abdomen.
b) Palpation:
- The fundal height increases,
- At the 16th week, the height of the uterus is between the symphysis pubis and the umbilicus.
- At the 20th week, it is about 2.5 cm below the umbilicus.
- At the 24th week, it is at the umbilicus level. The uterus feels soft and elastic.
- At 28 weeks – at the junction of the lower third and upper two-thirds of the distance between the umbilicus and the ansiform cartilage.
- The uterus becomes ovoid in shape.
Brakestone Hicks contractions (irregular, infrequent, spasmodic, and painless uterine contractions) are felt.
The woman does not feel the contractions at this time but can be felt when the palm is placed on the uterus. - Active fetal movement is felt from the 20th week.
External ballotment occurs from the 20th week.
c) Auscultation:
At 18-20 weeks, fetal heart sound can be heard with an ordinary stethoscope. Its sound is like the ticking of a watch, its location depends on the position of the fetus, the rate is 110 – 160 / minute.
Vaginal Examination:
- Bluish discoloration of the vulva, vagina and cervix occurs and the cervix is soft.
- Internal ballotment occurs between 16 and 18 weeks.
Uterine Soft:
- This sound is from dilated uterine vessels, a soft blowing sound heard during auscultation and synchronized with the mother’s pulse.
Phynic or Fetal Supple:
- This sound is the rush of blood from the umbilical artery which is synchronized with the fetal hard sound.
Investigations:
Sonography:
Routine sonography is It is done between 18 and 20 weeks in which the fetal anatomy, placental site and integrity of the cervical canal are observed.
Radiography:
Radiography is done between 16 th week in which the fetal skeletal shadow becomes visible.
Last / Third Trimester (29-40 weeks/ 7-9 Month):
Subjective Symptoms:
- Amenorrhea,
- Fatigue,
- Lightening (i.e. descent of the presenting part of the fetus into the lower uterine segment).
- Frequency of micturition starts again.
- Increased fetal movement.
Objective Symptoms:
- Cutaneous changes become more prominent due to increased pigmentation and striae, i.e. linea nigra, stria gravidarum and clos
- The uterine septum changes from cylindrical to spherical after the 36th week.
- Fetal movement is easily felt. Fundal height is as follows:
1) At 32nd week:
- At 32nd week, the fundal height is seen up to the junction of the upper and middle third.
2)At 36th Week:
- The fundal height reaches the encyform cartilage.
3)At 40th week:
- The fundal height increases until the fundal height is reached by 32 weeks due to the engagement of the fetus.
- Braxton Hicks contractions are more pronounced in the last two weeks of pregnancy and become more regular during that time.
- The lie, presentation, and position of the fetus can be determined by palpation of the fetal parts.
- The fetal heart sound is audible.
Sonography can assess the growth of the fetus.
Assess the volume of amniotic fluid.
Fetal movement becomes more felt.
•>(Signs of pregnancy) Sign of pregnancy :

After combining the three trimesters, the three main signs of pregnancy are seen, which are as follows.
1) Presumptive sign,
2) Probable sign,
3) Positive sign.
1) Presumptive sign
- Mostly subjective i.e. the mother herself feels that she is pregnant when it could also be due to another illness.
- •Amenorrhea,
•Nausea and vomiting,
•Morning sickness,
•Tingling sensation in 3 to 4 weeks,
•Enlargement of breast and nipple, - •Appearance of Montgomery tubercles in the breast.
•Increase in micturition, - Colostrum is expressed from the nipple.
•Pigmentation occurs on the face and breast.(Chloasma, linea nigra, stria gravidarum),
•Quickening: The first movement of the mother and fetus occurs around 16 – 20 weeks.
2)Probable sign:
- Probable signs are maternal physiological changes. They can be detected during examination.
They are objective but cannot be called a definite confirmation of pregnancy. - Enlargement of the abdomen. Pregnancy can be detected by abdominal palpation.
- Changes in the size and shape of the uterus and enlargement of the uterus.
- External ballotment and internal ballotment.
- A positive pregnancy test means the detection of the human chorionic gonadotropin (HCG) hormone in the urine. The following signs are seen in it:
Jacquemier sign or Chadwick sign
This sign appears during the 8th week of pregnancy. In it, bluish discoloration of the vulva, vagina and cervix is called Chadwick sign, while bluish discoloration of the vagina is called Jacquemier sign.
Hatman sign
This sign is It occurs between the 1st and 3rd month of pregnancy and involves slight bleeding when the fertilized egg implants in the uterine cavity.
Palmer’s sign
This sign occurs between the 4th and 8th week of pregnancy. In this sign, when bimanual examination is performed, regular and rhythmic contractions of the uterus occur.
Goodell’s sign
Goodell’s sign is seen up to 6 weeks, in which the lower part of the cervix softens.
Hagar’s sign
This sign is seen between 6 and 10 weeks, in which the upper part of the uterus, i.e. the body part of the uterus, enlarges with the growth of the fetus and The lower part of the uterus becomes soft. Hegar’s sign is a cyanosis and softening of the cervix.
Pisksek’s sign
This sign is seen during 6-8 weeks in which the uterus enlarges asymmetrically due to implantation in the uterus.
Osiander’s sign
This sign is seen during 6-8 weeks. In this sign, the pulsation is felt in the lateral fornix in the vaginal area.
Braxton Hicks contractions
In early pregnancy, the uterus contracts on its own. They are regular, infrequent, spasmodic, and painless, so they do not affect the dilation of the cervix. They increase near term and eventually merge with the painful contractions of labor. The presence of a placenta in which,
internal placentation and external placentation occur:
Internal placentation: After the 16th week, vaginal examination shows the presence of a body that moves on tapping and later returns to its place with a thrust.
External placentation: Around the 20th week of pregnancy, a placentation is felt in the uterus under the hand palpating the uterus by hand. This is known as external ballotment.
3) Positive sign.
A positive sign confirms pregnancy. In which the examiner detects the fetus and documents it.
Visualization of Fetus by Ultrasound: This test confirms pregnancy and also assesses the lie, presentation, fetal heart sound, location of placenta, amount and distribution of amniotic fluid and internal os. Abnormalities of the fetus such as encephalitis, spina bifida, myelomeningocele, etc., as well as uterine and ovarian abnormalities are detected by this method.
A scan is routinely recommended during the mid-trimester before the 20th week of pregnancy. In cases of serious fetal abnormalities, the patient may be advised to terminate the pregnancy.
Pregcolor and pregcolor-card test: These are mostly used as home kits to confirm pregnancy. These color-changing card tests are simple and can be done by the woman herself. The presence of 2 lines on the card test on the 5th day after missed periods confirms pregnancy.
Hearing the fetal heart sound: The fetal heart sound is heard on the fetal scope after 20 weeks. • Fetal movements: Fetal movements are felt at 22 weeks. • Palpation of Fetal Parts: Fetal parts are palpable after 24 weeks • Frequency of micturition: It is usually experienced at the end of term in which frequency of micturition occurs due to engagement of the fetal head.
Radiography: It is not usually advocated in pre- sent day practice.
Radiographic pelvimetry is rarely indicated in selected cases of suspected cephalopelvic disproportion.
Radioimmunoassay: This is a very sensitive method and can be used to detect the presence of hCG in maternal serum and urine 7-8 days after ovulation or at the time of implantation.
It confirms the presence of pregnancy 3 weeks after conception. The concentration of hCG in the mother’s serum doubles every 2-3 days until it reaches a peak value 2-3 months after conception (Blackburn 2007).
The embryo is visible on ultrasonography by 6 weeks, after which the fetus is visible.
Radiological appearance of the fetal skeletal system.
Visualization of the fetal skeleton on X-ray.
Late Visualization of fetal movement in pregnancy.
Differential Diagnosis:
Whenever the positive signs of pregnancy are not clinically obvious, sometimes problems can arise in the diagnosis of pregnancy. The differential diagnosis for presumptive and probable signs is as follows:
Presumptive sign:= Differential diagnosis
1) Amenorrhea: Due to emotional stress, illness and hormonal imbalance.
2) Breast Changes: Due to contraceptive pills.
3) Nausea and Vomiting: Due to gastrointestinal disorders or cerebral irritation.
4) Frequency of micturition, bladder irritability: = Urinary tract infection or pelvic Due to tumor
5) Quickening:= Due to intestinal movement
Probable sign:= Differential diagnosis
HCG in urine:= Due to choriocarcinoma.
HCG in blood:= Due to hydatidiform mole.
Uterine Growth:= Due to tumors.
Ociander sign, Hegar sign, Chadwick sign:= Due to pelvic congestion.
Uterine Suffolk:= Increase Blood Flow to Uterus (Ovarian Tumor)
Important Note:
There is no alternative diagnosis for a positive sign of pregnancy.
Conformimetry Test:
A) Urinary Immunological Test –
- Urinary immunological tests include latex agglutination slide test and immunochromatographic test.
• Latex agglutination slide test –
In slide test, when hCG antisera are combined with hCG in urine, if no agglutination is seen, then pregnancy is positive. If there is visible agglutination, then there is no pregnancy. This test comes positive after 2 weeks of missed menstruation.
•Immunochromatographic test- This test is available as a pre-color card or ascutest hCG etc. This test is more sensitive than the previous test and comes positive after one week of missed menstruation.
•ELISA or Radioimmunoassay (RIA)-
This test is especially indicated for patients with trophoblastic disease. It can detect hCG on the 8th day of fertilization, before the missed period.
B )Ultrasonography-
The following diagnoses can be made through abdominal ultrasonography:
•5th week:
Spherical gestational sac becomes visible.
•At 6th week –
fetal pole can be seen.
•At 7th week –
crown-rump length can be seen.
•At 10th week:
fetal heart sound is heard by ultrasound Doppler.
•At 12th week:
biparietal diameter is seen as much as (2.1 cm).
transvaginal Ultrasonography:
Transvaginal ultrasonography can make an earlier diagnosis than abdominal sonography.
At 4 weeks:
Visualization of gestational sac is done.
At 5 weeks:
Assessment of yolk sac and fetal cardiac motion can be done.
Antenatal care (Antenatal Care):

Definition:
- Antenatal care is also called prenatal care, in which comprehensive health care is provided to pregnant women from conception to the birth of a child.
- This period is a crucial time for monitoring the mother and the developing fetus. Because it allows for early identification and management of any potential health complications for the mother and the developing fetus. And the mother can be prepared physically and emotionally for childbirth and the postpartum period.
- The systematic supervision (examination or advice) of a woman during pregnancy, which is regular and periodic, is called “antenatal or prenatal care”. Antenatal care starts before pregnancy and ends when the baby is delivered.
•>Aim and Objectives of Antenatal Care :
Antenatal Care Aim:
- The aim of antenatal care is to improve the overall health of the fetus and mother and to improve the well-being of the mother and fetus and to prevent complications.
1) Monitoring maternal health
- Regular health checkups can monitor the overall health of the mother, such as properly assessing blood pressure, weight gain, and overall well-being, which can help identify any complications the mother may have early. And it can be prevented from happening further by treating it early.
2) Monitoring Fetal Health
- Assessment of the fetus in antenatal care, which includes ultrasound scans, fetal heartbeat monitoring, and other tests, can ensure proper growth and development of the fetus. If the child has any abnormality, it can be detected early and managed properly.
3) Health Education
- Antenatal care provides the opportunity for appropriate education to expectant mothers. It provides the opportunity for education about pregnancy, childbirth, breastfeeding, nutrition and parenting. This education can be helpful for the antenatal mother in taking proper decisions.
4) For early detection and proper management of pregnancy-related complications
- Antenatal care visits can help in early detection of pregnancy-related complications and timely management. Such as, gestational diabetes, preeclampsia, infections and other pregnancy-related risks that can affect pregnancy.
- Gestational diabetes, preeclampsia, infections and other pregnancy-related risks that can affect pregnancy.
5) Preparation for Childbirth
- Antenatal care sessions discuss birth planning, preparation for labor, and delivery options. By having this discussion, the mother and her family members can prepare mentally and practically for childbirth.
6) Psychological support
- Pregnancy causes emotional and psychological changes. Antenatal care provides a supportive environment in which the expectant mother can discuss and clear her anxieties, fears and doubts and can reduce her anxiety and fear and feel emotionally well-being.
7) Prevention and Management of Maternal and Infant Complications
- Antenatal care interventions include immunization, iron and folic acid Supplementation, and preventive treatment are provided to prevent pregnancy and childbirth related risks and complications.
8) Promotion of Healthy Behavior
- Education is provided to promote healthy behavior in antenatal care, including smoking cessation, avoiding alcohol and drugs, maintaining a balanced diet, and being physically active. Behavior is important for healthy pregnancy outcomes.
9) Postpartum Planning
- Antenatal care also discusses postpartum care, including postpartum care,
- Breastfeeding support and family planning options are discussed.
- The objectives of overall antenatal care are to have a healthy pregnancy, properly manage any risks and complications, prepare the mother for childbirth, and properly maintain the health of the mother and fetus during the throw-out pregnancy.
Objectives:
- The main objective is to deliver a healthy baby by a healthy mother with a normal pregnancy.
- The first visit should be before the second missed period.
- To assess the health status of the mother and fetus. For early screening if there is a case of high-risk pregnancy.
- To formulate a plan for further management.
- To promote, protect and maintain good physical and mental health of the mother during pregnancy.
•> Component of Antenatal Care:
1) Initial Assessment: The first antenatal visit should be done early in pregnancy. Ideally, it should be done within the first 8 to 12 weeks of the last menstrual period.
During this assessment, health care providers properly assess the woman, which includes a complete assessment of the woman’s
medical history, including previous pregnancies, medical conditions, medications, and relevant family history.
This information is provided to the mother It is collected to identify potential risk factors and provide appropriate care to the mother.
2) Physical Examination: During the pregnancy, a physical assessment of the mother is done to assess the health status of the mother and the fetus.
In this examination, the mother’s blood pressure, weight, and urine tests are done, due to which if the mother has a condition like gestational diabetes and preeclampsia, it can be identified early.
The mother’s blood test is also done, due to which the mother’s hemoglobin level, blood group, is done.
The mother is also screened for hepatitis and HIV infection.
3) Fetal Monitoring: In antenatal care, the growth and development of the fetus is also monitored. In this, the fetus is assessed through different methods such as, Ultrasound: Ultrasound is used to confirm pregnancy, to assess gestational age, to assess fetal growth and to identify any structural problems i.e. malformations in the fetus. Fetal Doppler: Fetal heart rate is monitored through fetal Doppler. Kick counting: Advise the mother to feel fetal movement and count the number of fetal kicks throughout the day to monitor fetal well-being.
4) Nutritional Guidance: Proper nutrition is important for supporting maternal health and for healthy development.
Antenatal health care providers provide guidance to the mother about a balanced diet, as well as education is provided to pregnant women about the importance of maintaining proper weight and taking adequate amounts of vitamins and minerals (Ex: iron and folic acid). And education is also provided to women that by consuming an adequate diet, congenital birth defects in fetuses and anemia in pregnant women can be prevented.
5) Health Education and Counseling: In antenatal care, pregnant women are provided with education on pregnancy-related topics. Such as,
1) Exercise:
Safe physical activity and exercise are important for maintaining the health of the mother and the fetus.
2) Labor and Birth Preparation
Educating the mother about the stages of labor Information is provided as well as education about pain relief strategies and birth plans.
3) Breastfeeding:
Provide education to the mother about the techniques and benefits of breastfeeding.
4) Emotional and Mental Health:
Properly assess the emotional and mental health of the mother and provide adequate education and psychological support to the mother to relieve her fears and anxiety and clear all the doubts of the mother
6) Screening and Testing: Proper genetic testing should be done during the mother’s antenatal period so that any genetic complications, if any, can be identified. Genetic Screening:
In this, ultrasound and blood tests are done on the mother, due to which if there is a risk of genetic disorder, it can be identified. (Ex: Ultrasound). Screening for Infection:
The mother is screened to identify any sexually transmitted diseases and any other infections that may affect the pregnancy. Glucose Tolerance Test:
A glucose test is done to identify whether the mother has any gestational diabetes condition.
7) Preparation for Labor and Birth: In antenatal care, birth preferences, options for managing labor pain, and preparation for potential complications are discussed.
8) Postpartum Planning: In antenatal care, planning is also done about postpartum care, in which breastfeeding support, newborn care and education are provided to the mother. Thus, antenatal care is important for maintaining the health condition of the mother, for the proper growth and development of the fetus, and for early identification and management of potential risk factors, if any.
Antenatal visit (Antenatal Visit):
- Usually, antenatal mothers should visit the antenatal clinic once a month for the first five months of pregnancy, then twice a month for the first six months and up to nine months, and then weekly antenatal clinic visits after nine months. is.
- A large number of mothers in India come from families with low socio-economic status and majority of women are working women.
Thus, women who come from families with low socio-economic status and are working women and find it difficult to attend clinical visits during pregnancy, it is necessary for them to have a minimum of 4 antenatal visits during the entire pregnancy.
Such as,
(WHO) Based on a review of the effectiveness of different models of antenatal care, a minimum of four antenatal visits are recommended.
- The first visit should be made as soon as pregnancy is suspected;
- The second visit should be scheduled between 4-6 months (approximately 24-28 weeks).
- The third visit should be scheduled between 8 months (approximately 32 weeks) and
- The third visit should be scheduled between 8 months (approximately 32 weeks) and
- The fourth visit should be done during the 9th month (36-40 weeks). Thus, it is important for a pregnant woman to have at least 4 antenatal visits
Antenatal assessment (antenatal assessment):
- Antenatal assessment is an essential assessment of the health level of a pregnant woman, in which a detailed history is collected from the woman, her physical examination is performed properly, abdominal examination is performed and screening tests are performed.
- The aim of antenatal assessment is to assess the recording of blood pressure, urinalysis, blood volume, uterine growth and fetal development, which can be used as a standard for comparison with advanced pregnancy.
Pregnant woman A detailed history of the patient’s past and present health status, obstetric history, medical history, family history, and personal history should be taken in accurate detail so that risk factors can be identified early. The initial assessment with a pregnant woman provides an opportunity to build a trusting relationship with the woman, which can then provide her with proper care during the pregnancy period. - The woman’s first visit involves her general health history, obstetric history, physical and pelvic examination, and laboratory investigations.
Objectives:
- To assess the health status of the mother and fetus.
- To assess the fetal gestational age.
- To conduct a baseline investigation.
- To provide continuous obstetric care.
- To screen for high-risk cases.
History Taking:
History Taking Pregnant Pregnant Woman’s
1) Name
2) Date of Examination
3) Address
4) Age
If a woman’s first pregnancy is at the age of 30 or above 35 years, it is called elderly primi gravida.
Extreme of age i.e. teenage pregnancy and elderly pregnancy are obstetric risk factors.
5) Gravida
6) Mercury
7) Religion
8) Duration of Marriage
(It helps in noting fertility and fecundity)
9) Occupation
(It helps in interpreting symptoms due to fatigue or occupational hazards).
10) Occupation of Husband
(To assess the socio-economic status of the family).
11) Period of Gestation(POG).
(Pregnancy is known by how many weeks have been completed which is counted from the first day of the last menstrual period. The most reliable method is ultra sonography.
12) GPTPAL score
In which,
G: Gravida
P: Para
T: Term Delivery
P: Pre Term
A: Abortion
L: Live Birth.
Information is written about.
13) Complaint
Ask about them, sleep pattern, appetite, bowel habit and urination etc.
History of Present Illness
- Collect the history of the chief complaint along with its onset, duration, severity, progress, medication, etc.
History of present pregnancy
- Note if there are different complications in different trimesters of pregnancy.
Such as hyperemesis in the first trimester Gravidarum, - Threatened abortion and pyelitis in the second trimester (infection and inflammation of the renal pelvis, which is the part of the kidney in which urine collects before it goes to the ureters, is called pyelitis).
And ask about anemia, preeclampsia and antepartum hemorrhage (APH) in the last trimester.
Check the status of previous antenatal visits, including immunization status, medical or radiation exposure in early pregnancy and medical surgical events.
Health History:
- Finding out medical conditions that affect pregnancy can range from common urinary tract infections to serious cardiac conditions. Certain medical conditions require special care.
- Such as,
urinary tract infection,
women with a history of thrombosis,
hypertension,
other conditions including asthma, epilepsy, generalized infections,
psychiatric disorders,
diabetes,
and cardiac conditions require the support of a medical specialist.
Obstetrical history:
- The midwife asks the pregnant woman for information in a friendly and sympathetic approach; Such as, age, last menstrual period etc.
- The midwife calculates the expected date of delivery from the last menstrual period and records it in the history sheet along with the present and past pregnancies and other information related to the pregnancy.
- Such as,
- 1) The woman’s age should be less than 18 years or more than 40 years.
- 2) Having the condition of grand multipara i.e. having given birth to more than 5 previously.
- 3) Vaginal bleeding at any time during pregnancy.
- Collect history of miscarriage and medical termination of pregnancy (MTP).
Menstrual history:
- It collects a history of the woman’s age at the time of menarche.
- It assesses the frequency, duration and amount of menstrual blood flow of menstruation.
- It also collects a history of the first day of the last menstrual period (LMP).
- EDD (Expected Date of Delivery) is calculated using Nigel’s formula. is.
- Collect history about dysfunctional uterine bleeding such as,
- Example: Menorrhagia, Metrorrhagia, and Intermenstrual Spotting…
Past Medical History:
- Information about any past medical history, if any Collect, such as tuberculosis.
- Past Surgical History:
- Collect information about the history of previous general and gynecological surgeries.
Family History:
- Does any family members have a genetic disease? Collect information about whether there is a history of certain genetic diseases such as hypertension, diabetes, tuberculosis, and a history of twin pregnancies in the family.
- Collect information about whether there is a history of certain genetic diseases such as hypertension, diabetes, tuberculosis, and a history of twin pregnancies in the family.
Personal History:
- Collect history of pre-pregnancy contraceptive practices, smoking or alcohol habits, blood transfusions, corticosteroid therapy, drug allergies, immunizations, anti-D and immunoglobulins, etc.
Post Obstetric History:
- Post obstetric history,
- Still birth,
- Neonatal death,
- Small for gestational age baby,
- Postmature baby,
- Congenital defect,
- Rhesus iso immunization,
- Having a history of previous abortion, miscarriage and termination.
- Having a history of previous preterm labor.
- Having a history of previous cesarean section and uterine surgery.
- Having a history of antepartum and postpartum To have.
- Multiple pregnancy and
- Collect information about whether there is a history of precipitated labor.
- Thus, the antenatal history is collected from the mother and the general health of the mother is assessed. And if any complications are likely to arise, they can be identified early.
Gravida:
- Gravida means “pregnant woman” and the number of pregnancies a woman has had indicates how many times she has been pregnant, regardless of the outcome. This does not mean how many children are born from a pregnancy, but it is the total number of pregnancies that are counted and not the number of children.
- Gravida means the past and present state of pregnancy, regardless of the station period. Overall gravida means the total number of pregnancies of a woman is called gravida.
• Primi gravida:
- A woman who is pregnant for the first time is called primigravida.
- Or
- A woman who First-time pregnancies are called primigravida.
• Multigravida:
- A pregnant woman who has been pregnant more than once is called multigravida, regardless of the outcome of the pregnancy.
•Grand multigravida:
- A woman who has been pregnant five or more times is called grand multigravida.
• Nulligravida:
- A woman who has never been pregnant is called nulligravida. is.
•Para:
- It involves the number of times a woman has given birth to a child that has survived the period of viability (28 weeks), excluding abortions.
• Parity:
- Parity is the ratio of the number of viable (28 days) Status of pregnancy after period.
• Nullipara:
- If the pregnancy is not completed until the period of viability or if there is a previous abortion or not, it is called Nullipara.
•Primipara:
- Primipara means if one viable child has been delivered, then she is called a primipara. If there are more than one fetus at a time, then the parity does not increase.
Ex:=Twins, triplets do not increase. - Ex:=Twins, triplets do not increase.
• Multipara:
- A pregnancy that is complete up to the stage of viability or beyond is called multipara. is.
- Calculation of Expected Date of Delivery (EDD)
- To calculate the Expected Date of Delivery (EDD), first of all, one should know about the normal duration of pregnancy.
•> The normal duration of pregnancy is 9 months + 7 days, 40 weeks or 280 days.
- Now, to calculate the expected date of delivery (EDD), the woman is asked to
1) 1st day of the last menstrual period (LMP)
and
2) the length of the menstrual cycle. - The length of a normal menstrual cycle is 28 days.
- 1) If a woman’s menstrual cycle is 28 days, then the expected date of delivery (EDD) is calculated using the Nagels formula.
- Like,
- Expected date of delivery (EDD) := In this, +9 months +7 days are added to the first day (1st day) of the woman’s last menstrual period (LMP).
- EX:= First day (1st day) of the last menstrual period (LMP) It is
March 3, 2022. - EDD:= March 3, 2022
↓ ↓ - 7 days 9 months Expected Date of Delivery (EDD):= December 10, 2022
- 2) If a woman says that her menstrual cycle is less than 28 days or more than 28 days, then the Expected Date of Delivery (EDD) can be obtained using the Modified Nigel’s Formula.
- ••> In Modified Nigel’s Formula, first use Nigel’s Formula to get Approximate Expected Date of Delivery (EDD).
••>★ If menstrual cycle is less than 28 days
- EX:= If menstrual cycle is 24 days and EDD calculated by Nigel’s Formula is: 10 December 2022.
Then: - 28 days – Cycle Length = X
- 28 – 24 = 4 days
- Correct EDD = Approximate EDD obtained –” X “
- EDD = 10 December 2022 — 4 days
- EDD = 6 December 2022 will be.
••> ★ If menstrual cycle is more than 28 days
- EX:= If menstrual cycle is 31 days and EDD calculated by Nigel’s formula is: 10 December 2022.
Then: - Cycle Length – 28 days = Y
- 31 – 28 = 3 days
- Correct EDD = Approximate EDD obtained +” Y “
- EDD = 10 December 2022 + 3 days
- EDD = 13 December 2022.
3) If the length of a woman’s menstrual cycle is a variable,
- In this, the approximate cycle length of the menstrual cycle of the next three months is measured. To do:
- C1+C2+C3
—- = Average
3 Menstrual
Cycles - Now, ask what was the first day of the woman’s last menstrual cycle.
- If the average menstrual cycle is 28 days, then calculate the Expected Date of Delivery (EDD) using Nigel’s Formula.
- And if the average If the length of the menstrual cycle is less than 28 days or more than 28 days, use the Modified Nigel’s Formula to calculate the expected date of delivery.
- 4) Alternatively, to calculate the expected date of delivery (EDD), go back three months from the first day of the last menstrual period (LMP) and add 7 days and 1 year. Due to which the expected date of delivery can be found.
- EX:= The first day (1st day) of the last menstruation period (LMP) is
3 March 2022. - EDD=
3 March 2022 — 3 months
= 3 December 2021. - EDD:
= 3 December 2021
↓ ↓
+ 7 days + 1 year - EDD:
= 10 December 2022 - Thus, the EDD (Expected Date of Delivery) for pregnancy can be obtained as follows.
Physical Examination:
- Physical examination is usually done during the early antenatal period of the mother and the expectant mother. It is done to find out if there is a disease or abnormality.
- Before starting the initial antenatal examination, obtain the woman’s consent and provide her with a comfortable position.
- Examine the body system through observation, inspection, auscultation and measurement techniques. Attend to the woman gently and respectfully and perform her physical examination in a properly organized manner. During the entire physical examination, the woman’s privacy should be properly respected Maintain.
Antenatal examination is usually performed in two parts:
1) General Examination
2) Obstetric Examination
•> General Physical Examination:
1) Build:
- Assess whether the mother is obese, average or thin.
2) Nutritional status of the mother Status:
- Assess whether it is good, average, or poor.
3)Height:
- A woman’s height is usually measured when she comes for her first antenatal visit. If the woman is short, then there are chances of her having a small pelvis.
- In Western countries, 5 feet and 4′.7″ in India are considered short. And most of them have a small pelvis. Therefore, it is important for every woman to get her height measured during her antenatal visit.
4)Weight:
- Weigh the mother with the same weighing machine during every antenatal visit and measure her accurately.
- The average woman usually gains about 11 kg of weight during her pregnancy.
- If the mother has a condition of obesity, she usually develops gestational diabetes, pregnancy induced hypertension (PIH) and It may be due to shoulder distortion. Obesity increases the risk during pregnancy. If the mother has OBCD, there is difficulty in palpating the fetal parts and assessing the presentation, position and engagement of the presenting part of the fetus.
5) Pallor:
- Lower palpebral conjunctiva, dorsum of tongue and nail bed 52 Look for pallor.
6) Jaundice:
- The condition of jaundice should be assessed on the sclera, conjunctiva, underside of the tongue, hard palate and skin.
7)Eyes:
- Inspect for conditions of anemia and jaundice.
8)Ears:
- Ear pain in the ears, and any discharge, and tinnitus is a condition that Why assess it?
9) Tongue, Teeth, Gums and Tonsils:
- Assess whether there is a condition of malnutrition. Assess whether there is a condition of glossitis and stomatitis.
10) Neck:
- Check for abnormalities in the neck veins, thyroid gland, and lymph glands.
- Slight enlargement of the thyroid gland can occur in up to 50% of pregnancy cases.
11) Edema of Legs:
- Check for edema on the medial malleolus and 1/3 rd anterior surface of the tibia on both legs by pressing the area with the thumb for 5 seconds. Then assess whether there is a condition of varicosities in the leg.
- The causes of edema are seen due to pre-eclampsia, cardiac failure, and nephrotic syndrome.
12) Heart, Lungs, Spleen, and Liver:
- Assess the patient for cardiomegaly, splenomegaly, liver enlargement, and lung abnormalities.
13) Blood Pressure:
- It is checked to ascertain normality and provide baseline information for comparison during the throwout pregnancy. A blood pressure of more than 126/94 is an indicator of a worrying situation. Special care and rest are mandatory to maintain normal blood pressure and placental perfusion during the prenatal period.
14) Breast:
- Breast examination is not only used to identify the presence of pregnancy but also to assess the skin condition of the nipple and areola. Used.
- Breast examination can identify any abnormality or difficulty, which can prevent difficulties during best fitting Can be.
15) Urine Analysis:
- Urine analysis is usually done during the first visit of pregnancy and further during pregnancy to assess the condition of proteinuria, ketone bodies in urine and glycosuria.
- When In conditions of vomiting, hyperemesis, starvation and exercise, there is a background of fat for energy in an adequate amount according to the demand of the fetus and ketone bodies are found in the urine.
- The amount of glucose in the urine is found due to higher circulating blood levels, reduced renal threshold or renal disease.
- The amount of protein in the urine is also found due to conditions of pre-eclampsia or infection.
Blood Tests During Antenatal Examination:
- Blood tests are used during antenatal examinations to assess a woman’s hemoglobin level, hematocrit level, ABO blood group, Rhesus (Rh) factor, and VDRL (Venereal Disease Research Laboratory Test), HIV (Human Immunodeficiency Virus Test), and rubella immune status.
ABO Blood Group and Rhesus ( Rh ) Factor:
- Blood analysis is usually done to find out the ABO blood group and Rhesus ( Rh ) factor. To prevent hemolysis in newborn babies, blood analyses are performed to identify the status and presence of antibodies in red blood cells.
- Rising titration indicates an antibody response, so frequent blood assessments are done in Rh-ve women. Blood titration should be done during the 28th and 34th weeks of gestation and antidegamma globulin should be administered.
- To prevent hemolytic disease in newborn babies in conditions like threatened abortion, amniocentesis, trauma, antidegamma globulin should be administered within a few days of this event. Provide additional doses.
Hemoglobin and Hematocrit:
- Estimation of hemoglobin is done to assess whether iron is in an adequate amount. It is important because if the mother is anemic, her need for iron intake (dietary or supplement) increases.
- Red blood cell count is important for providing adequate amounts of oxygen to the mother and her growing fetus.
- Repeat at 28 weeks of pregnancy, as the physiological effects of hemodilation become apparent, and at 36 weeks to assess Hb levels and to treat appropriately before delivery if Hb levels are below the normal range. Along with this, the mother should be advised to take iron supplementation, folic acid and iron-rich foods.
Venereal Disease Research Laboratory Test (VDRL):
- This test is usually performed to identify the presence of syphilis in women. If syphilis is detected early, it can prevent the transmission of this disease to the fetus. Not all positive results indicate the presence of active syphilis in a woman.
Human Immunodeficiency Virus (HIV) Test:
- To obtain informed consent and prevent active transmission of infection in the fetus, proceed with HIV screening and counsel couples as soon as possible if the results are unsatisfactory.
Rubella Immune Status:
- This is done by measuring the rubella antibody titer. Exposure to rubella infection during pregnancy can cause deformities in the fetus, so if a woman has If rubella is positive, they should be advised to terminate the pregnancy.
- Then the woman is advised to take live vaccination during the puerperium period and to avoid pregnancy for the next three months.
- Other investigations involve investigation for Hepatitis B, C and Chlamydia based on the history of contracting diseases/infections in the first trimester.
- Accordingly, the mother should be advised to take Blood tests are performed or education is provided about them.
Obstetrical Examination of Pregnant Women :

- Obstetrical examination involves abdominal examination and vaginal examination.
- The midwife examines the woman after obtaining her consent. Before performing the obstetrical examination, the mother is advised to evacuate the bowel properly. After that, the mother is provided with a dorsal position and her knees are flexed to provide a comfortable position and the obstetrical examination of the woman is performed. The examination involves palpating the woman’s abdomen Exposure is performed as required and the examiner should stand on the mother’s right side during the examination.
- The midwife should maintain rapport with the mother throughout the procedure by inquiring about the pregnant woman’s health, investigations performed and breastfeeding of the newborn baby.
- Usually an abdominal examination can be performed by the obstetrician after 12 weeks but for the best assessment of fetal growth after 25 weeks of gestation The best assessment of fetal growth can be done by performing an obstetric examination.
- Fetal growth cannot be properly assessed by abdominal palpation performed before 25 weeks.
- Physical examination and abdominal assessment can be beneficial as follows:
- 1) The midwife should assess the size of the uterus, shape, abdominal contour, scars, injury marks, linea nigra and striae gravidarum, etc. Observations can assess the gestational age and growth pattern of the fetus.
- 2) The growth of the fetus, By assessing the presentation, position and engagement of the fetal head, the well-being of the fetus and any deviation from the normal condition can be detected.
- 3) By measuring the fundal height and abdominal girth of the pregnant woman, palpating the fetal position, and auscultating the fetal heart sound, the midwife can minimize the risks of pregnancy and labor.
★ Inspection:
Preliminaries:
- To properly prepare the woman for the examination, advise her to lie down in a flat position, then advise her to keep her arms at her sides, and advise her to relax the abdominal muscles.
- Expose only the area of the abdomen that needs to be examined, keeping the remaining area properly covered.
- Before performing an abdominal examination, ensure that the woman properly empties her bladder because a full bladder can make the examination uncomfortable and difficult. If there is a full bladder, the fundal height can also be inaccurately detected. Discuss the investigation report with the mother and maintain proper records.
Inspection:
- The size and shape of the uterus can be assessed through inspection. The movement of the fetus can also be observed. If there is a multiparous woman, then a pendulous abdomen can be noted, in which the uterus is tilted forward. The condition of the skin and any incisional scars and herniations present are noted.
- A distended colon and OBCD provide a false impression. If there is polyhydramnios or multiple pregnancy, both the length and breadth of the uterus are enlarged. If there is a large baby, the length of the uterus also increases.
- In the occipito-posterior position, a saucer-shaped depression of the abdomen can be seen below the umbilicus.
- Due to melanocyte stimulating hormone, a brownish-black line is visible in the midline from the zygosternum to the symphysis pubis on abdominal inspection, which is called linea nigra.
- Depressed marks are seen on the abdominal wall below the umbilicus and sometimes on the breast, which are initially pink but after delivery become glistening silvery white in color, which are called stria albicans or stria gravidarum.
- The fundus of the uterus is palpated slightly above the symphysis pubis during the 12th week of gestation. is.
- Inspection should be done to see if the uterus is ovoid longitudinal, transverse, or oblique.
- Assess the shape of the uterus, its fundal notch and anterior wall are convex or flat, and its shape is cylindrical or spherical.
- Inspect whether the uterus is enlarged.
★ Palpation:( Leopold Maneuver )
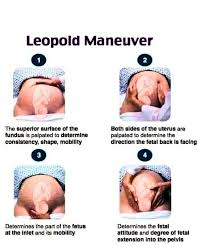
Before palpating the abdomen, wash the hand properly and turn it to the left. This left hand evokes a sense of touch but does not induce premature contractions. The midwife should keep her hands properly relaxed while palpating. Use hand pads instead of finger tips for proper palpation. Avoid induction of contractions by using rough methods of palpation.
•> Measurement of Fundal Height:
- The midwife places the ulnar border of her left hand below the xiphosternum to find the fundal height. Slowly, she moves her hand down the abdomen, feels for a curve at the upper border of the fundus, and places the ulnar border of her hand between the fundus and the xiphosternum to find the gestational sac. Fundal height can be measured using a measuring tape. Fundal height is measured from the top of the pubic bone (symphysis pubis) to the top level of the uterus (fundus). Thus, the measurement between the fundal border and the symphysis pubis is called the symphysis fundal height (SFH). This measurement approximately corresponds to the number of weeks of pregnancy.
- Recording: The measurement of fundal height is recorded in centimeters ( Cm ). For example, if the fundal height is 28 cm, it usually indicates that the pregnancy is approximately 28 weeks.
•> Uterine Fundal Height at Different Weeks During Pregnancy:
- Non-pregnant uterus pyri shape (pear-like) The uterus becomes globular in shape during the 12th week of pregnancy.
- The uterus enlarges again during the 28th week to form pyri form and becomes spherical in shape after the 36th week of pregnancy.
•> At 12 Weeks of Pregnancy:
- During the 12th week of pregnancy, the uterus is no longer anteverted and anteflexed. The fundus is palpated abdominally over the symphysis pubis.
•> At 16 Weeks of Pregnancy:
- During the 16th week of pregnancy, the uterus is ovoid in shape. The uterus is located between the symphysis pubis and the umbilicus.
•> At 20 Weeks of Pregnancy:
- During the 20th week of pregnancy, the fundus of the uterus is two fingers below the umbilicus.
•> At 24 Weeks of Pregnancy:
- During the 24th week of pregnancy, the fundus of the uterus is at the level of the umbilicus and one finger below it.
•> At 30 Weeks of Pregnancy:
- During the 30th week of pregnancy, the fundal part of the uterine cavity is located between the umbilicus and the zygosternum
•> At 36 Weeks of Pregnancy:
- During the 36th week of pregnancy, the fundal part of the uterine cavity is at its highest level, i.e. up to the zygosternum
•> At 38 Weeks of Pregnancy:
- During the 38th week of pregnancy, the fundus part of the uterine cavity descends and reaches the level of 34, which is called lightening.
•> At 40 Weeks of Pregnancy:
- During the 40th week of pregnancy, the fundus of the uterine cavity reaches the level of 32 weeks and then the lower uterine segment relaxes and stretches while the cervix becomes soft and short and the uterus is ready for labor.
- The lie, presentation, attitude and position of the fetus can be determined through the Leopold maneuver. Leopold has mainly given 4 maneuvers.
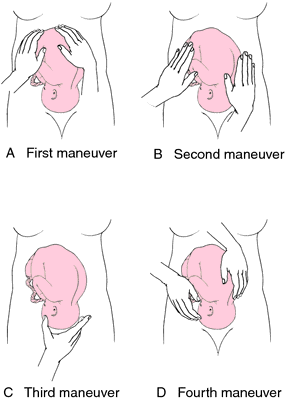
1) Fundal Palpation
( Fundal Grip/ First Leopold/First Maneuvers):
- Fundal palpation (fundal grip) is used to assess which part of the fetus is present at the fundal site, i.e. whether the head is present or the buttocks (breech).
- In fundal palpation, the examiner should palpate with the patient’s face facing the patient.
- Then place both hands on the woman’s fundus and wrap the fingers slightly around the top part of the fundus.
- Then gently palpate the fetal parts.
- If the fundus part is palpated,
- a)If there is a broad, soft and irregular mass, it indicates that the buttock part of the fetus is present at the fundus site.
- b) If a smooth hard and globular mass-like structure is felt, it indicates that the head part of the fetus is present at the fundus side.
- C) In transverse lie, no part of the fetus is palpated at the fundus site.
2) Lateral palpation
( Umbilical grip/ Second Leopold/Second manual):
- This maneuver assesses the position of the back and limbs of the fetus, due to which the position of the fetus in the uterus can be assessed
- In this maneuver, palpate the patient’s face while facing the side.
- Then place both hands directly on both sides of the umbilicus.
- Then provide support to the fundus with one hand and palpate the fundus with the other hand. In this way, palpate alternately on both sides of the umbilicus.
- In this, palpate the back parts of the femur, limbus and anterior shoulder.
- If the smooth covered shape part of the femur and the resistant feel are felt while palpating, then it can be said that the back part is present.
- If while palpating An irregular mass that is palpable or movable suggests that a limb of the patient is present.
3) (Povlik Grip/ Third Leopold/Third Maneuvers):
- This maneuver assesses the size, flexion, and mobility of the head, as well as whether the presenting part is engaged. It can be known.
- In this manual, the examination should be done facing the patient’s face. Then advise the patient to bend the knee so that the abdomen can relax.
- Then place the thumb and forefinger of the examiner’s stretched hand on the lower pole of the uterus and place the ulnar border of the palm on the symphysis pubis. When the fingers and thumb are almost aligned, grasp the presenting part of the fetus properly.
- If the presenting part of the fetus is not engaged, a movable mass is felt, and if the presenting part is engaged, the part of the fetus felt by examination is movable. No.
4) (Pelvic grip/ Fourth Leopold/Fourth maneuver):
- This maneuver can assess head presentation, head flexion, and head breech presentation.
- In this maneuver, the patient is examined with the patient facing the feet and the woman is asked to bend her knees.
- Then place the four fingers of both hands on the midline on both sides of the lower pole of the uterus and parallel to the inguinal ligament.
- Then press the fingers downwards and backwards to palpate which part of the fetus is present in the lower pole of the uterus.
- Keep moving the hands towards the pelvic inlet. If the hands separate i.e. do not overlap each other, then it shows that the presenting part is engaged. If the hands are overlapping, it indicates that the head is not engaged.
- If a hard mass with a definite round shape and smooth surface is felt on palpation, it indicates the head as the presenting part.
- The sinciput will be felt on the opposite side of the occiput and is higher than the occiput – indicating a well flexed head.
- If the prominences – sinciput and occiput are the same Level – indicates a deflected head.
- If If the head is on the same side as the back, it indicates an extended head.
Auscultation:
- The midwife uses a Pinard fetal stethoscope to auscultate the fetal heart sound.
- Using a Pinard fetal stethoscope, the examiner can listen to the fetal heart sound. It is placed on the mother’s abdomen, at a right angle to the fetus’s back. The ear is placed in firm contact with the fetus, without touching the fetus. The fetoscope is moved to the maximum intensity point of the voice and F.H.S is heard.
- Auscultation not only diagnoses a live baby from the fetal hard sound but also identifies its presentation through the maximum intensity of its location.
- a) In vertex and breech presentations, FHS can be heard well from the back side of the fetus.
- Because the convex portion of the back of the fetus comes in contact with the uterine wall.
- b) In cephalic presentation, the heart sound can be heard well from the chest of the fetus.
- According to the rules, in cephalic presentation, the maximum intensity of the fetal heart sound (FHS) is heard below the umbilicus and in breech presentation, the fetal heart sound (FHS) is heard around the umbilicus.
- In occipito lateral, the FSH is heard laterally and in occipito posterior position it is heard towards the flanks.
- In the left occipito posterior position, it is difficult to detect F.H.S.
- Fetal hard sound (FHS) is heard at different places depending on the presentation and position of the fetus, such as,
- Cephalic: It is heard in the part between the umbilicus and the anterior superior spine.
Breech: At or above the level of the umbilicus.
Anterior: Near the abdominal midline.
Transverse: On the lateral side of the abdominal area
Posterior: In the flank area or Abdominal Near the midline.
Accordingly, the fetal heart sound (FHS) can be heard at different locations depending on the presentation and position of the fetus.
- This maneuver can assess head presentation, head flexion, and head breech presentation.
- In this maneuver, the patient is examined with the patient facing the feet and the woman is asked to bend her knees.
- Then place the four fingers of both hands on the midline on both sides of the lower pole of the uterus and parallel to the inguinal ligament.
- Then press the fingers downwards and backwards to palpate which part of the fetus is present in the lower pole of the uterus.
- Keep moving the hands towards the pelvic inlet. If the hands separate i.e. do not overlap each other, then it shows that the presenting part is engaged. If the hands are overlapping, it indicates that the head is not engaged.
- If a hard mass with a definite round shape and smooth surface is felt on palpation, it indicates the head as the presenting part.
- The sinciput will be felt on the opposite side of the occiput and is higher than the occiput – indicating a well flexed head.
- If the prominences – sinciput and occiput are the same Level – indicates a deflected head.
- If If the head is on the same side as the back, it indicates an extended head.
Auscultation:
- The midwife uses a Pinard fetal stethoscope to auscultate the fetal heart sound.
- Using a Pinard fetal stethoscope, the examiner can listen to the fetal heart sound. It is placed on the mother’s abdomen, at a right angle to the fetus’s back. The ear is placed in firm contact with the fetus, without touching the fetus. The fetoscope is moved to the maximum intensity point of the voice and F.H.S is heard.
- Auscultation not only diagnoses a live baby from the fetal hard sound but also identifies its presentation through the maximum intensity of its location.
- a) In vertex and breech presentations, FHS can be heard well from the back side of the fetus.
- Because the convex portion of the back of the fetus comes in contact with the uterine wall.
- b) In cephalic presentation, the heart sound can be heard well from the chest of the fetus.
- According to the rules, in cephalic presentation, the maximum intensity of the fetal heart sound (FHS) is heard below the umbilicus and in breech presentation, the fetal heart sound (FHS) is heard around the umbilicus.
- In occipito lateral, the FSH is heard laterally and in occipito posterior position it is heard towards the flanks.
- In the left occipito posterior position, it is difficult to detect F.H.S.
- Fetal hard sound (FHS) is heard at different places depending on the presentation and position of the fetus, such as,
- Cephalic: It is heard in the part between the umbilicus and the anterior superior spine.
Breech: At or above the level of the umbilicus.
Anterior: Near the abdominal midline.
Transverse: In the lateral side of the abdominal area
Posterior: In the flank area or abdominal Near the midline.
Accordingly, the fetal heart sound (FHS) can be heard at different places depending on the presentation and position of the fetus.
Vaginal Examination:
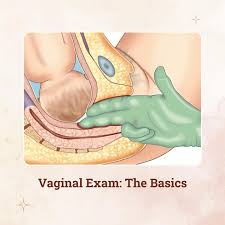
- When a woman comes to the antenatal clinic for a checkup, a vaginal examination is done.
- •The pregnancy is diagnosed by It is used to assess the size of the uterus during periods of amenorrhea. Examination:
- Vaginal examination is performed in the antenatal clinic.
- Then provide the patient with a dorsal position and advise him to flex his legs and keep his buttocks on the foot end of the table.
- Then wash his hands properly and wear gloves on the examining hand, preferably on the right hand.
Inspection:
- Separate the labia with the thumb and index finger to check for vaginal discharge, cystocele, rectocele, or uterine prolapse.
Speculum Examination:
- Speculum examination should be performed before bimanual examination and cervical smear and vaginal swab should be taken using a bivalve speculum.
Bimanual Examination:
- Separate the labia with the left hand and introduce two fingers (index and middle finger) of the right hand into the vagina. Place the left hand suprapubically. Perform a slow systemic examination and note the following:
1) Cervix:Consistency, direction, and pathology
2) Uterus:Size, shape, position, and consistency
3) Adnexa: Note any mass felt.
If the introitus is narrow, a finger can be introduced for examination. No attempt should be made to assess the pelvis during this stage.
Purpose of Vaginal Examination:
- • To assess the extent to which the labor process is progressing or to what extent the labor process is delayed.
- * To assess the dilatation of the service.
- •To apply a fettle scalp electrode.
- * To exclude cord prolapse after rupture of the water, especially if the presenting part is not fitted appropriately.
Observe the following findings:
- Observe the labia for any signs of varicosities, edema, or vulvar warts or sores.
- Observe whether there are scars from previous tear or episiotomy.
- Properly note whether there is any bleeding from the vaginal orifice. Do.
- If the membranes have ruptured, assess the color and order of the amniotic fluid (e.g., offensive amniotic fluid due to infection, green amniotic fluid due to presence of meconium).
Vagina:
- A warm, moist vagina with a small soft distensible vaginal wall is good for delivery.
- A hot and dry vagina is It is a sign of obstructed labor.
Cervix:
- A long and tightly closed cervix indicates that the labor process has not yet started.
- The cervix should normally be soft and elastic, if it is tight and rigid, labor may be prolonged.
Uterine OS:
- The dilation of the external OS is assessed in centimeters. Normally, the cervix is dilated to 10 cm, with one finger = 2 cm of dilation.
Forwater:
- Fill the membrane through the dilating OS to see if it is an intake.
Station of presenting part:
- Maternal ischial spines nu Evaluate the descent of the fetus during labor by estimating the relationship with the presenting part. The distance from the presenting part above or below is expressed in centimeters.
Presentation:
- Filling the sutures in the hard bone of the vault of the skull bone and the fontanelles and vertex.
Special Investigations :

- Clinical evaluation along with biochemical and biophysical methods are used for diagnosis to find the cause of congenital malformations, chromosomal abnormalities, first trimester spontaneous abortion and stillborn infants etc. and to prevent fetal death and unnecessary treatment in late pregnancy.
1) Serological Test:
- Serological tests are performed to identify rubella, hepatitis B, and HIV infections.
2) Maternal Serum Alpha Phyto Protein (MSAFP) Estimation:
- Maternal Serum Alpha Phyto Protein (MSAFP) Estimation or Triple Test at 16-18 weeks is performed for mothers who are at risk for neural tube defects, There is a risk of carrying a fetus with Down syndrome or other chromosomal abnormalities.
3) Blood test:
- Blood test is done to detect and diagnose conditions such as thalassemia and sickle cell anemia, which allows for early detection and appropriate measures to be taken.
4) Ultrasound Examination:
- Ultrasound examination is done in the first trimester by transabdominal sonography (TAS) or transvaginal (TVS).
- From it
- * Early pregnancy,
- * Accurate date,
- * Number of fits,
- * Gross fetal anomaly,
- • Any uterine pathology and adnexal pathology can be detected.
- Ultrasound examination is usually performed between 18 – 20 weeks.
- Biparietal diameter ( BPD ),
- Abdominal circumference ( AC ),
- Head circumference ( HC ),
- Femur length ( FL )
- And the diagnosis of intrauterine growth retardation (IUGR) can also be made by serial measurement of amniotic fluid volume.
5) Repeat Investigations:
- At the 28th week of pregnancy and at the 36th week of pregnancy, The mother’s hemoglobin level is tested again during the week.
- A urine test is done during each antenatal visit to check for the amount of protein and sugar present in the urine.
Screening and Assessment for High Risk:

- Pregnancies that are at risk of developing serious complications are considered high-risk pregnancies.
- All pregnancies are evaluated to identify whether there are risk factors or the chances of them occurring. By classifying pregnancies as high risk, if they require extra attention, they can be provided in an adequate amount.
- Screening options are available to assess the risk for specific congenital anomalies during pregnancy and do not involve the risk of miscarriage.
- If evaluation of high-risk women is done early, high-risk pregnant women can be referred to a perinatal center before delivery, which can reduce neonatal morbidity and mortality rates.
- The most common reason for referral is preterm delivery, which is usually due to premature rupture of membranes.
- A major benefit of screening and assessment of high-risk mothers is that if there are any complications or problems in the mother and baby, they can be detected early, leading to better outcomes in the health status of the mother and baby. And the mother can give birth to a healthy baby.
- High risk cases such as,
- Obstetrical history:
- Previous stillbirth,
- Previous neonatal death,
- Previous premature infant,
- Previous premature infant,
- History of recurrent abortion.
- Mother’s medical history such as,
- Maternal illness,
- Chronic hypertension,
- Abnormal PAP Smear test,
- Insulin dependent diabetes,
- Renal disease,
- Rh- isoimmunization,
- Maternal physical risk factors,
- Incompetent cervix,
- Uterine Malformation.
- Risk factors of current pregnancy,
- Moderate to severe preeclampsia (which is characterized by hypertension, edema (weight gain), proteinuria (protein in urine), and albuminuria),
- Polyhydroamnios (i.e. when the amount of amniotic fluid exceeds 2000 ml),
- Oligohydroamnios (when the If their amount is less than 200 ml at term, it is called oligohydroamnios.
- Placenta previa (when the placenta partially or completely implants near or above the internal os of the uterus, it is called placenta previa).
- Multiple pregnancy (when more than one fetus develops in the uterus at the same time, it is called multiple pregnancy).
- Abruptio placentae (abruptio placentae) Placenta abruptio is a form of antepartum hemorrhage (APH) in which the normally situated placenta prematurely separates from the uterine wall, causing bleeding called placental abruption.)
Other High Risk Pregnancy:
- Abnormal fetal position,
- Vaginal bleeding,
- Malpresentation,
- Fetus is small for gestational age,
- Hb level is less than 10 g/dl,
- Poor weight gain,
- Proteinuria,
- Glycosuria,
- Systolic BP. More than 155 mm of Hg.
- Vaginal infection. etc.
- Things to consider during early pregnancy are —
- Blood testing which monitors the mother’s hemoglobin level, ABO and Rh group, and blood sugar level.
- Excessive weight gain in the mother is usually seen due to fluid retention. And if the weight of the mother decreases, then there is also a risk of developing the condition of intrauterine growth retardation (IUGR).
- A history of previous hypertension or pregnancy induced hypertension (PIH) can be a risk factor for the mother as well as the fetus.
- If the amount of amniotic fluid is high or the amount of amniotic fluid is reduced, then these are also called risk factors.
- For high-risk cases, another approach should be followed as follows As follows:
Maternal Serum Alpha Phyto Protein (MSAFP):
- Alpha Phyto Protein (AFP) is an oncofetal protein and is produced in the yolk sac and fetal liver.
- Fetal serum and amniotic fluid have their highest levels at approximately 13 weeks and maternal serum 32 weeks is a.
- Maternal serum and amniotic fluid are tested for alpha-feto protein (AFP). This is usually done when the fetus is at risk for neural tube defects and other congenital defects. If the level of alpha-feto protein (AFP) is high, it indicates fetal pathology, open neural tube defect and if the level of alpha-feto protein (AFP) is low, it suggests conditions like Down syndrome and gestational trophoblastic disease.
- In some cases, the amount of maternal serum alpha-feto protein (MSAFP) is increased, such as conditions like multiple pregnancy, open neural tube defect, renal anomaly, Rh isoimmunization, IUFD (intrauterine fetal death), anterior abdominal wall defect etc.
- This test is done between 15 and 18 weeks of gestation. Chorionic villus sampling (CVS):
Chorionic villus sampling (CVS):
- For prenatal diagnosis of genetic disorders, chorionic villus sampling is done transcervically at 10-12 weeks and transabdominally at 10 weeks under ultrasound guidance.
- A few of these cells can be collected from the chorion frondosum, transcervically (a catheter is introduced through the cervix), or transabdominally (a needle is inserted through the uterine wall into the maternal abdomen into the placental tissue). Diagnosis is obtained within 24 hours.
- The positive aspect of this test is that the results are obtained early, and if termination is necessary, it can be done only in the first trimester. This test is also associated with fetal loss, limb deformities, and vaginal bleeding, etc. In addition to miscarriage, there is a risk of infection and amniotic fluid leakage.
- As a result, amniotic fluid can leak, which can develop into a condition known as oligohydramnios, which is low amniotic fluid levels.
- The best time to test is after 10 weeks.
Cordocentesis (Percutaneous Umbilical Blood Sampling):
- In this test, a fetal blood sample is collected during pregnancy and then any chromosomal abnormality or blood disorder is diagnosed. In this, a needle is inserted by puncturing the umbilical vein under the guidance of ultrasound. And then 0.5 to 2 ml of fetal blood is This test can cause preterm labor, abortion or intrauterine fetal death.
- The time to do this test is after 18 weeks.
Triple test:
- This test combines three tests, in which,
- Maternal serum alpha fetoprotein (MSAFP), human chorionic gonadotrophin (HCG), and unconjugated estriol (UE) are involved.
- This test is used to detect Down syndrome.
- If the pregnancy is affected, maternal serum alpha fetoprotein (MSAFP) and estrogen levels are low and human chorionic gonadotrophin (HCG) levels are high.
Amniocentesis:
- This is an invasive procedure that is usually done at 16 – 18 weeks using ultrasound Guidance includes a genetic analysis of fetal cells for DNA analysis and biochemical testing of the fluid.
- In this procedure, a fine needle is inserted trans-abdominally into the amniotic cavity and amniotic fluid is aspirated from it.
Procedure –
- Before the actual procedure, a local anesthetic is given to relieve pain while inserting the needle used to withdraw the amniotic fluid.
- The needle is inserted through the mother’s abdominal wall and the wall of the uterus into the amniotic sac. The insertion is done.
- Using ultrasound guidance, the needle is guided to an area of the sac that is away from the fetus and about 20 ml of amniotic fluid is withdrawn for testing. Amniotic fluid contains cells that are shed by the developing fetus.
- The cells are examined for the number and size of chromosomes (karyotype) to see if there are any problems that put the baby at risk for certain conditions. After removing the amniotic fluid, the cells of the fetus are separated from it.
- The cells are grown in culture medium, then fixed and stained.
- Under a microscope for abnormalities of chromosomes The test detects the most common abnormalities, including chromosomal disorders such as Down syndrome, Edwards syndrome (trisomy 18) and Turner syndrome, and neural tube defects such as spina bifida and anencephaly. Amniocentesis can also detect whether the mother or baby is Rh-negative and whether the baby’s lungs are healthy enough to deliver if immediate termination is needed. Whether it is mature. Amniocentesis cannot detect every type of abnormality, such as – For example, it cannot tell whether the baby has a cleft lip or a cleft palate.
- Amniocentesis is performed during pregnancy when:
- A woman who has had a previous chromosomally affected pregnancy or a genetic disorder, such as Down syndrome or other defects, is at increased risk of having a baby with a chromosomal abnormality detected by ultrasound examination. Does.
- When there is a history of any genetic disorder or birth defect in the parents or anyone in the family.
- In women who are older than 35 years.
- In women who are concerned about the possibility of a chromosomal abnormality in their child due to their request.
- Risks Associated with Amniocentesis:
- Maternal and fetal hemorrhage,
- Infection,
- Fetal injury,
- Miscarriages.
- During late pregnancy:
- Biophysical
- For uteroplacental insufficiency Biophysical investigations like Fetal Movement Count, Cardiotocography, Non-Stress Test, Fetal Biophysical Profile (BPP), Doppler Ultrasound, Contraction Stress Test (CST), Amniotic Fluid Volume etc. are performed.
Fetal Movement Count :

Cardiff Count 10 Formula:
- In this patient a Start counting fetal movements from 9.am and stop when there are 10 movements. If there are less than 10 movements within 12 hours for two consecutive days or no movement in a day, the doctor is asked to inform them.
Daily Fetal Movement Count (DFMC):
- In this test, three counts are counted in each period of morning, afternoon and evening and multiplied by four if it is more than 12 hours. A fit is considered to be problematic if there are fewer than 10 or three fit movements per period.
Diagnosis Modalities Invasive and Noninvasive:
- Different invasive and non-invasive methods are used for prenatal screening and diagnosis.
- •> In which non-invasive methods (methods that do not require any instruments to be inserted into the body by opening them),
- * Examination of the uterus from outside the body.
- * Ultrasound detection.
- * Listening to the fetal heart sound (FHS).
- * External fetal monitoring such as a non-stress test (NST) may be involved. is.
- •> Invasive method (a medical procedure that invades (enters) the body, usually by cutting or puncturing the skin or by inserting an instrument into the body)
- Such as,
- * Chorionic villus sampling,
- * Amniocentesis,
- * Cordocentesis,
- * Methods such as maternal serum alpha-feto protein (MSAFP) are involved.
Ultrasound scan:
- Ultrasound scan is generally a safe, non-invasive, accurate and cost-effective investigation. In an ultrasound scan, high frequency sound waves are transmitted into the uterus. In ultrasound, the baby’s bouncing off and returning echoes are translated by a computer into an image on a screen that shows the baby’s position and movements. Hard tissues, such as bone, reflect the largest echoes and appear white in the image, and smooth tissues appear gray and speckled. Fluid (such as the amniotic fluid in which the baby is located) does not reflect any echoes and therefore appears black.
- It is the difference between these different colors of white, gray, and black that allows the sonographer to interpret the image when scanning the abdomen early in pregnancy, when the procedure often requires a full bladder.
•> Uses of Ultrasound:
- • To check the viability of the fetus
- The heartbeat of the fetus can be checked through ultrasound.
- • To check how many fetuses are surviving in the uterine cavity/ To check the number of fetuses
- Usually before 14 weeks of pregnancy it tells whether a woman is pregnant with a baby or not. Ultrasound scanning is used to determine whether the fetus is alive and whether it is a fetus or not. It is used to check whether there is one of the twins or triplets.
- • To detect ectopic pregnancy
- Any abnormality It is used to detect conditions such as ectopic pregnancy or to detect conditions in which the fetus implants outside the uterine cavity, mainly in the fallopian tube. Doppler Umbilical Velocimetry Doppler Ultrasonography can detect RBCs in the blood vessels of the uterus and fetus. R.B.C.) measures the speed at which it travels. This is helpful in determining whether a woman with diabetes or gestational hypertension has a high vascular resistance and is therefore developing placental insufficiency.
• Placental grading
- Placental grading is usually based on the amount of calcium deposited in the placenta. The placenta is graded as 0 (12-24 weeks), 1 (30-32 weeks), 2 (36 weeks) or 3. (38 weeks) can be provided.
• Amniotic Fluid Volume Assessment
- If the fetus is As the amniotic fluid decreases, stress in the uterus puts the fetus at risk of umbilical cord compression and interferes with its nutritional levels.
- By 20 weeks, the uterus is divided into two vertical lines with a midpoint (linea nigra). The vertical diameter of the largest pocket of amniotic fluid present on each side is measured in centimeters (cm). The amniotic fluid index (AFI) is the sum of the two.
- After 20 weeks, the uterus is divided into four parts and the sum of the four is taken. Average AFI: 12-15 cm (28-40 weeks); 5-6 (oligohydramnios), 20-24 (polyhydramnios).
- •To detect the cause of vaginal bleeding
- Ultrasound helps to find the cause of any bleeding that the mother experiences. In cases of vaginal bleeding, the viability of the fetus is measured by ultrasound.
- Visible heartbeats can be seen and detected by pulse Doppler ultrasound in about 6 weeks and are usually clearly Can be depicted at 7 weeks.
• To find out the accurate date of pregnancy
- The exact date of pregnancy can also be determined by measuring the baby. For patients with an uncertain last menstrual cycle, such measurements must be done as early in pregnancy as possible to arrive at the correct dating. The measurements taken are:
a) Crown-rump length (CRL):
- This measurement can be taken between 7 and 13 weeks and provides a very accurate estimate of gestation.
b) Biparietal diameter (BPD)
- The diameter between the 2 sides of the head.
- This is measured after 13 weeks. It ranges from about 2.4 cm at 13 weeks to about 9.5 cm at term. Increases to .
c) Femur Length (FL)
- Measures the longest bone of the body and reflects the longitudinal growth of the fit. Its utility is similar to BPD. It increases from about 1.5 cm at 14 weeks to about 7.8 cm at term.
d) The Abdominal Circumference ( AC )
- The single most important measurement to take in late pregnancy.
- It reflects the size and weight of the fetus more than its age.
- •Risk of Down syndrome To assess
- The presence of Down syndrome can be detected by measuring the fluid at the back of the baby’s neck (called a nuchal translucency scan) at 11-14 weeks.
- Some major abnormalities can also be detected at this stage. At 11 to 14 weeks, a measurement of the thickness of the skin at the back of the neck (known as a nuchal translucency measurement) can be used to measure the risk of a fetus having a chromosomal abnormality.
- * To find out why the blurb test is abnormal.
- • To assist in performing diagnostic tests
- Some tests to assess the well-being of the fetus, such as CVS or amniocentesis, are safely performed using ultrasound to show the position of the baby and placenta.
•Development of the fetus
After 18 weeks, it is possible to examine the fetus in more detail. Most organ systems can be examined to ensure that the fetus is developing normally.
•To diagnose certain types of abnormalities
Such as spina bifida. Many structural abnormalities in fetuses can be reliably diagnosed by ultrasound scan, and this can usually be done before 20 weeks.
• To assess the amount of amniotic fluid and locate the placenta
Liker, i.e., too much or too little amniotic fluid, can be clearly detected by ultrasound, and both of these conditions can adversely affect the fetus.
Ultrasonography is also important for detecting the location of the placenta. Due to which any abnormal site of presentation can be detected early, such as placenta previa.
• Ultrasonography is also important for other obstetric conditions such as,
a) When intrauterine death needs to be confirmed.
b) To check fetal presentation in some cases.
c) When evaluation of fetal movement, tone and breathing is needed in the biophysical profile. Then.
d) To diagnose uterine and pelvic abnormalities during pregnancy.
Ex: fibromyomata, ovarian cyst.
•> Ultrasound scan can be done both vaginally and abdominally
•Vaginal scan
- Vaginal scans are only done during the first 12 – 14 weeks of pregnancy. Because the fetus is very small at this stage, a vaginal scan provides a better view than an abdominal scan. In a vaginal scan, the mother is asked to lie down on her back, and then a lubricated sensor is inserted into the vagina. This sensor is usually covered by a condom. Abdominal scan Used after 14 weeks. In an abdominal scan, the mother is asked to lie on her back. A gel is applied to her skin over her lower abdomen. The gel allows the sensor to slide easily over her skin and helps produce a clear image. The sensor is held firmly against the skin and moved over the abdominal surface.
•Doppler ultrasound
- Doppler ultrasound is currently most widely used to detect the fetal cardiac pulsation and the pulsation in the fetal various blood vessels. Further developments in Doppler ultrasound technology in recent years have enabled a great expansion in its application in obstetrics. is, especially in the area of assessing and monitoring the well-being of the fetus,
- Its progression is a challenge in diagnosing intrauterine growth restriction and cardiac malformations.
Cardiotocography (CTG):
- Cardiotocography (CTG) measures the fetal heart rate and Uterine contractions are recorded graphically.
- It is generally done during the third trimester. The machine used to monitor is called a cardiotocograph and is also known as an electronic fetal monitor (EFM) or external fetal monitor (EFM).
- Two transducers are used externally, strapped to the abdominal wall. One measures the fetus’s heart rate and the other measures uterine contractions.
- Internal measurements can also be done. It requires a certain degree of cervical dilation, as it involves inserting a pressure catheter into the uterine cavity and attaching a scalp electrode to the fetus’s head to adequately measure the pulse. It is preferred when there is a possibility of a complicated birth. Cardiotocography is also used to perform non-stress tests (NST) and contraction stress tests (CST).
Non-stress tests (NST):
- In a non-stress test (NST), the fetal well-being is evaluated by monitoring the fetal heart rate (FHR) in response to fetal movement. This test does not put any special stress on the fetus.
- In a non-stress test, a belt is attached around the mother’s abdomen to monitor the fetus’s heart rate and uterine contractions.
- A non-stress test is a common prenatal procedure that is usually performed during the third trimester to assess fetal health.
- The heart rate is recorded for about 20-30 minutes, during which the mother indicates whether she feels any movement of the fetus. The short-term variation in baseline should be between 10 and 15 bpm. If the variation cannot be reduced over a long period of time with other abnormalities, then there may be fit distress.
Purpose:
- The primary goal of a NST (non-stress test) is to monitor the baby’s heart rate and assess how the fetal heart rate (FHR) responds to movement. It helps evaluate the fetus’s well-being and can provide insight into the baby’s oxygen levels and overall health. NST is usually used in cases where there is concern about the health of the fetus or when there is a risk of complications.
Position and Preparation of Mother:
- Non-stress stress (NST) is usually performed by providing the mother with a properly comfortable position. The fetus should not be in a sleeping condition while performing this test because it can cause variations in the fetal heart rate, i.e. fetal heart rate. A decrease in rate may be seen. The fit is evoked by abdominal palpation or a buzzer. Advise the woman to press the button when she feels fetal movement and monitor the fetal heart rate (FHR).
Advantages:
- * This is a non-invasive test.
- * This test is simple,
- It is inexpensive and less time consuming.
- * This test does not have any contraindications or complications.
- * No special expertise is required to perform this test.
- * Immediate answers can be obtained through this test.
- Interpretation of test:
Reactive Test (Normal Stress Test (NST)):
- The test is considered reactive when there is an acceleration of the fetal heart rate (FHR) of 15 beats/minute above baseline for 15-30 seconds in relation to the fetus’s movement.
- The test is considered normal when there are two or more such events in a 10-minute period or five or more accelerations in a 20-minute period.
Non-reactive test (abnormal non-stress test):
- Non-reactive test is called when the fetal heart rate is absent in response to fetal movement.
- When the fetal heart rate is less than 15 beats/minute in response to fetal movement and it lasts less than 15 seconds, then this test This is called abnormal.
Suspicious non-stress test
- In this, there is an acceleration of the heart rate of the fit in relation to the movement of the fit, but the beats above baseline, the number of accelerations, or the length of duration do not meet the criteria for being reactive or non-reactive.
Indications of Non Stress Test ( NST ):
- A woman who has any pre-existing medical condition such as diabetes or a condition that arose during pregnancy, such as,
- High blood pressure.
- When a pregnant woman reports that fetal movement is less than usual.
- Intrauterine growth retardation (IUGR) is a condition in which a child does not grow properly for its normal age.
- When the amount of amniotic fluid is too high or the amount of amniotic fluid is too low.
- A woman who has lost her baby in a previous pregnancy.
- This test is performed to check the baby’s breech position in women whose pregnancy continues beyond 40 weeks of pregnancy.
- After a woman undergoes a procedure such as external cephalic version (to turn a breech baby) or amniocentesis in the third trimester (to determine whether the baby’s lungs are mature enough for birth or to rule out an infection in the uterus), a health care practitioner may perform a non-stress test (NST) to ensure the baby’s well-being.
Contraction Stress Test (CST):
Contraction Stress Test
- (CST) is used to assess the health condition of the fetus and the fetal heart rate (FHR) in a woman when the fetus’s oxygen level is reduced during uterine contractions. This test assesses the fetal heart rate response to oxytocin-induced uterine contractions. External heart monitoring is used in this test. During uterine contractions, the fetus’s blood and oxygen supply drops for a short time. This condition is not a problem for most babies, but in some babies, their heart rate slows down. These changes in heart rate are monitored on an external fetal monitoring device. This test is usually performed when a woman is 34 weeks or more pregnant.
Preparation of Mother:
- In this, the woman is provided with a semirecumbent position, a lateral tilt position, and a properly comfortable position. Then the uterine contractions are recorded for 20 to 30 minutes. If uterine contractions are three or more in 10 minutes and their duration is usually more than 40 seconds, then no stimulation is required. If spontaneous stimulation is absent, stimulation is induced by providing oxytocin.
- In the oxytocin challenge test, a diluted oxytocin solution is administered intravenously. The rate of infusion is then increased at small intervals until three or more uterine contractions are present in 10 minutes. Stop the oxytocin infusion after recording until the contractions are not observed for more than 30 minutes.
- Contraction stress test is performed to check the following conditions such as,
- It is used to assess the well-being of the fetus and to assess the fetal heart rate (FHR) during the process of labor or during uterine contractions when the amount of oxygen is low is.
- Contraindications
- If the woman has a condition of placenta previa,
- If the woman has a condition of antepartum hemorrhage (APH),
- If a previous classic cesarean section has been performed,
- If the client is at high risk of preterm labor
- Risk
- Labor is usually expected to start early if the expected date of delivery is met. can occur.
- Problems in the baby may arise due to prolonged contractions.
Interpretation:
- This contraction stress test (CST) is performed when the blood and oxygen supply to the fetus is reduced for a short period of time while the woman is in the labor process. This reduced blood and is used to assess the health status of the fetus due to oxygen supply.
Normal Contraction Stress Test (CST)
- The results of the normal test It is called negative. In which the baby’s heart rate does not slow down (decelerate). But the contractions (late deceleration) slow down later.
Abnormal Contraction Stress Test (CST)
- A positive result of an abnormal contraction stress test (CST) is one in which the fetus’s heart rate slows and remains continuously slow even after contractions, meaning that the fetus may have problems during normal labor. It can also mean that
- If the delivery time is delayed, the baby may have problems.
Hyperstimulation
- In hyperstimulation, contractions last for 90 seconds or more.
Suspicious
- There is a late declaration of fetal heart rate, but this is not repetitive and does not occur with continuous contractions.
Unsatisfactory
- The quality of the recording is not that good.
Antenatal Health Education:
- Antenatal education is a Provided during pregnancy.
Principles:
- * To provide knowledge of regular health check-up to the mother.
- * To improve the health status of pregnant women till delivery.
- * To provide advice on diet, drugs and hygiene to improve the health status of the woman.
- During pregnancy, the mother is provided with the following health education:
- 1) Diet which also involves supplementary therapy
- 2) Antenatal hygiene
- 3) Rest and sleep
- 4) Travel
- 5) Comfort Measures
- 6) Coitus
- 7) Smoking and Alcohol
- 8) Avoidance of Drugs
- 9) Immunization
- 10) Preparation for Confinement
- 11)Child Care
- 12)General Advice
- 13)Antenatal Exercise
Antenatal diet (Antenatal diet) :

- Providing adequate amounts of diet to the mother during pregnancy maintains good maternal health and ensures optimal fetal growth. Good food and optimal maternal nutrition are important for pregnant women. The first three months of pregnancy are very important because most of the baby’s physical and mental growth occurs during this time. Nutrition plays a very important role in maintaining a healthy pregnancy. Pregnancy is the most demanding period for a woman, therefore, taking a balanced diet becomes even more important. Consuming adequate amounts of nutrition provides the necessary strength during labor and leads to successful lactation. If the mother consumes an adequate amount of diet during pregnancy, it can reduce spontaneous abortion, stillbirth, and neonatal death and promote fetal growth.
- Adequate antenatal diet is very important due to the following factors:
- * To maintain the physical health of the mother.
- * To fulfill the needs of the growing fetus.
- •Helps develop and maintain the necessary strength and vitality during labor.
- * Helps develop successful lactation.
- * A pregnant woman’s diet should ideally be light, nutritious, easily digestible and rich in protein, minerals and vitamins.
- * Advise the mother to avoid excessively salty and spicy foods.
During Pregnancy
- The basal metabolic rate (BMR) increases due to the growth of maternal tissues, fetuses and placenta, due to which the calorie requirement increases by about 2500 kcal. During pregnancy, a pregnant woman normally gains about 11 kg of weight.
Carbohydrates and Fat
- Carbohydrates are necessary to produce energy in the body. It is necessary to consume an adequate amount of carbohydrates during pregnancy. If adequate amount of carbohydrates is not consumed, the mother’s weight is not maintained properly, which can lead to complications for the mother and the fetus.
- Carbohydrate rich foods such as rice, wheat, potatoes, sugar, fruits, etc. are included along with fatty foods such as butter, ghee, vegetables, oil, milk, meat and eggs.
Protein
- A mother should eat a variety of protein-rich foods, as her needs increase during pregnancy. Vitamin B6 is essential for the proper utilization of protein. Fish, meat, nuts, peas, beans, and dairy foods such as milk and eggs all provide a good supply of protein. The daily requirement of protein in a pregnant woman is about 60 grams.
Minerals
- Calcium, phosphorus, iron, zinc, sodium and iodine should be taken during pregnancy. Due to the deficiency of these minerals Complications can occur and have adverse effects on the mother and fetus.
- Important minerals such as calcium and iron are discussed below:
Iron:
- Why Iron helps build bones and teeth and is responsible for the production of hemoglobin. Iron deficiency can cause a condition called anemia. In this case, iron supplements need to be taken once or twice a day. Eat more potatoes, raisins, dates, broccoli, leafy green vegetables, whole grain bread, and iron-rich foods. Iron-fortified cereals can prevent anemia.
Calcium:
- Calcium needs are twice as high during pregnancy as they are during normal times. This is important for the healthy development of the baby’s bones and teeth, which begin to form around 8 weeks. Milk, eggs, cheese, and green vegetables are good sources of calcium. The recommended daily amount of calcium increases significantly from 800-1200 mg during pregnancy and breastfeeding.
Folic acid:
- Folic acid is one of the most important nutrients needed during pregnancy. It is essential for the development of the baby’s nervous system, especially in the first few weeks. Folic acid helps prevent neural tube defects (defects in the spine, brain, or their coverings) and other congenital defects such as cleft lip and congenital heart disease. Folic acid supplements can be taken during pregnancy. Folic acid is found in dark green leafy vegetables (such as spinach or kale), liver, yeast, legumes, and citrus fruits, and fortified cereals and breads. Folic acid is easily lost during cooking; Such as green vegetables after steaming or boiling.
- The daily requirement of folic acid is about 400 micrograms.
Vitamins
- Vitamins have a special role in the physiological state of the mother and fetus. Therefore, its daily intake should be increased.
- The important vitamins during pregnancy are A, B, C, and D . Therefore, women should be advised to consume a diet rich in vitamins.
Vitamin A
- It increases vision and cell integrity, which is obtained from vegetables, liver, and fruits.
Vitamin B
- Vitamin B prevents the condition of anemia.
- It is found in yeast, seeds, beans, nuts, dairy foods, and whole grains.
Vitamin C
- Vitamin C is essential for the formation of the placenta, it is also necessary for fighting infections and is also useful in the absorption of iron. Its requirement is 70 mg/ day. Its rich sources include citrus fruits and vegetables.
Vitamin D
- A vitamin important for maternal calcium absorption and infant calcium metabolism.
Vitamin E
- It is used to prevent abortion.
Vitamin K
- Neonatal Hemorrhage Prevention It happens.
- Fiber
- Incorporating fiber in your daily diet can help relieve constipation.
- It is found in fruits, vegetables, brown rice, nuts,
- Cereals, oats, beans, and pulses.
- Antenatal hygiene
Daily Bathing:
- Pregnant women should be advised to take daily baths to maintain personal hygiene, but proper care should be taken to ensure that there is no fall-down due to imbalance while taking daily baths.
Dental Care:
- Pregnant women should be advised to maintain good dental care and oral hygiene and consult a dentist when necessary.
Breast Care
- Pregnant women should be advised to maintain good dental care and oral hygiene and consult a dentist when necessary.
Breast Care
- Pregnant women should be advised to maintain good dental hygiene and oral hygiene during the antenatal period. Advice on care to be taken so that breastfeeding can be promoted and lactation can be properly maintained during the postpartum period.
Rest and Sleep
- Usual activities can be done throughout pregnancy, but strenuous work should be avoided, especially in the first and last trimesters. Pregnant women should sleep for a total of 10 hours, including eight hours at night and two hours in the afternoon.
- Advise the mother not to stay in one position for a long time continuously and advise her to keep her legs elevated while resting so that the pressure on the legs and heels can be relieved. Advise the mother to sleep on her left side as much as possible, which will help her sleep better. Blood circulation can be affected.
Traveling
- Pregnant women should be advised to avoid heavy and jerky traveling in the first trimester and the last trimester. Because the chances of miscarriage are high during this time. Especially if it is a high-risk pregnancy, the woman should be advised to avoid traveling.
- After 32 weeks of gestation, the mother should be advised to avoid air travel because air travel can damage the membranes of the uterus and can prove dangerous.
- If the woman has placenta previa, severe anemia, and sickle cell disease, she should be advised to avoid air travel.
Comfort Measures
- Pregnant Women Should Not Lose Advise on wearing clothes that can relieve discomfort and provide a comfortable environment and advise women to avoid wearing high-heeled shoes.
Coitus
- Advise pregnant women to avoid sexual activity, especially in the first and third trimesters, as the chances of abortion are highest in the first trimester. There is a chance of infection in the third trimester, so pregnant women should be advised to avoid coitus activity.
Smoking and Alcohol
- Advise the mother that smoking is harmful to health, so smoking should be avoided during pregnancy because, if she is a heavy smoker, then there are chances of the baby being small and there are also chances of abortion. Also, if the mother is ingesting alcohol, then she should also be advised to avoid it because it can cause fetal maldevelopment and growth restriction. Thus, smoking and alcohol are harmful to health and should be advised to stop.
Avoidance of drugs
- Reproductive asthma Drug intake should be kept in mind while considering the possibility of pregnancy because most drugs can cross the placenta and reach the fetus and many of them have teratogenic effects which can harm the fetus. And women should also avoid taking over-the-counter drugs.
- During pregnancy, the mother should be advised to take iron and folic acid tablets as prescribed.
Radiation
- Advise the mother to avoid abdominal X-ray during pregnancy as it increases the chances of leukemia or cancer in the fetus.
Family Planning
- Educate and motivate the mother to have a small family size and to keep a gap between two children only when she is pregnant. Should.
Immunization
- During pregnancy, the mother should be immunized for tetanus. It not only protects the mother but also the fetus.
- Pregnant women should usually be given two doses of tetanus.
- In which the 1st dose is 0.5 ml. Intramuscular. It should be provided early in pregnancy in the upper arm.
- The 2nd dose of tetanus toxoid should be provided 1 month after the 1st dose of vaccination.
- If the pregnant woman has received tetanus toxoid vaccination during pregnancy in the last three years, then a booster dose of tetanus toxoid should be provided to the pregnant woman.
- Live virus vaccines (rubella, measles, mumps and yellow fever) should be given to pregnant women. Fever) cannot be given. And like non-pregnant state, rabies, hepatitis A & B, and toxoid can be given.
Preparation for confinement
- This includes properly collecting articles for mother and baby.
- Provide education to the mother about the signs of true labor.
- Untoward the mother Provide education about symptoms and advise them to report any of them immediately if they occur:
- •Severe headache with disturbed sleep and restlessness.
- * Urinary troubles.
- * Epigastric pain and vomiting.
•Skinty Urine.
- * If painful uterine contractions occur at 10 minute intervals or early or uterine contractions occur continuously for 1 hour, then it suggests the onset of labor.
- * If there is a sudden surge of watery fluid pervaginally, then it suggests the condition of premature rupture of membranes.
- * Active vaginal bleeding.
Child Care
- To educate mothers on various aspects of child care such as care during pregnancy, child bearing, best feeding, growth, development, immunization etc.
General Advice
- Advise the mother to come for proper check-ups as per the schedule of antenatal visits. If any signs like excessive headache, dysentery, blurred vision, baby not feeling movement, sleep disturbance, restlessness, urinary troubles, swelling on hands, feet and face are noticed, immediately inform the health care personnel.
Antenatal Exercise:
- Mother Provide education on proper antenatal exercises because exercising strengthens the abdominal muscles and pelvic floor muscles, which makes the labor process easier and also helps promote recovery after childbirth.
Antenatal exercises
- Properly Standing
- Stand with your weight evenly distributed on both feet.
- Keeping balance between heels and toes. When the mother has to stand in one place for a long time, she can put one foot forward and put all her weight on that foot for a few minutes. Then she can do the same with the other foot.
- Sit well in a chair with your back and thighs supported, legs slightly apart, feet flat on the floor. Use your leg muscles to lower and raise
- Don’t sit on the edge of a chair.
Sit properly
Lifting things off the floor (Licking)–
- Get close to the object. Sit down, bend your knees, and keep your back straight. Hold the object in front of your body with your elbows bent. Use your leg muscles to straighten slowly and smoothly into a standing position. Bend the hips and knees, not the back.
Special Exercise:

Walking
- Walking is a good exercise and one of the best exercises for pregnant women because it does not put much pressure on the knees and ankles. A pregnant woman can last for nine months.
•> Abdominal Exercises
- These exercises help strengthen the abdominal muscles, support the back, and help with pushing during childbirth.
Benefits:
- • Abdominal exercises tone the abdominal muscles Increases and strengthens.
- * Reduces back pain.
- * Provides better posture, which eliminates discomfort.
- * Helps reduce strain on the back.
- * Helps enhance stability.
- * Stability also improves balance, which prevents falls and Can help prevent injuries.
- * Improved abdominal strength can help with breathing and during labor.
- * Quick recovery can also occur after childbirth.
- * Strong abdominal muscles can help support the pelvis and reduce pelvic pressure.
Resisted Knee to Chest
- Instruct the woman to lie flat on her back, then bend her knees and place her feet flat on the floor. Start with a pelvic tilt and then lift your head towards your chest and lift one knee towards your abdomen. Using both hands, grab your leg below the knee. Using your leg muscles, try to push your knee towards your foot while your hands pull the knee towards your abdomen. Hold for a count of 5, then release. Repeat on the opposite knee. Do these exercises 5 times first. and do up to 10 repetitions.
Time for resisted knee to chest exercises: –
- First trimester (1-3 months): If there are no complications, this is usually a good time to do knee to chest exercises.
- Duration: – Usually around the end of pregnancy Safe up to 7th month. After this, due to the changes in your body and growing belly, you should seek the consent of your healthcare provider for personal advice.
Straight Curl-Up Exercise
- Lie on your back with your knees bent and feet flat on the floor. Then, keep your hands straight just below your knees.
- Exhale and bring your chin to your chest, moving forward continuously for about 8″ (20 cm). Try to arch your back without raising your waist. Then, lower back down.
- Do this curl-up exercise 5 times at first. Do it for 10 repetitions.
Time for Straight Curl-Up Exercise: –
- First Trimester (1-3 Months): It is generally safe to do straight curl-up exercises if you have no complications.
Duration:
It is generally safe for about 5 months. After this period, as your pregnancy progresses, straight curl-ups may become uncomfortable or impractical due to the growing belly and changes in your body.
•> Pelvic Exercise:
- • Pelvic exercises strengthen the lower back and provide proper support to the spine and relieve discomfort. Helps to do.
- * Increases the strength and elasticity of the pelvic floor muscles, which helps in bladder control and can also prevent the condition of urinary incontinence.
- * Provides support for the alignment of the pelvis and spine, due to which posture can also be improved.
- * Due to strong pelvic floor muscles, the labor process can also be easier during childbirth.
- * Helps in faster recovery after childbirth
Pelvic Tilt:
- For pelvic tilt exercises, advise women to get on their hands and knees with their head and back parallel to the floor. Tighten your stomach muscles and tuck your buttocks downward to round the lower back. Hold for a slow count of 5, then Release. Do not hold your breath. Repeat this pelvic tilt first 5 times. Then repeat 10 times.
Time for pelvic tilt exercises: –
- Pelvic tilt exercises are usually started around the fourth month (16 weeks) of pregnancy and can be safely done until the seventh month (28 weeks) of pregnancy.
- After this period, Changes or alternative exercises may be necessary due to the increasing size of the belly and the possibility of discomfort.
Pelvic floor exercises
- The muscles of the pelvic floor are under a lot of strain during labor and pregnancy. Exercising these muscles helps maintain muscle tone and quickly regain their previous strength after pregnancy. The main exercises performed here are Kegel exercises Has
Kegel Exercises:
- This exercise can be done anywhere, such as sitting, in a car, at someone’s desk, or while standing in line at a store. In this, the urethral and vaginal openings are squeezed, and the muscles of the pelvic floor are tightened to prevent bowel movements. Similarly, the muscles are squeezed to prevent the flow of urine. In this, the muscles are drawn inward and this condition is maintained for a count of 10, then relaxed. It can be repeated up to 10 times.
Time for Kegel exercises: –
- Kegel exercises can be started at any time during pregnancy, usually around the 4th month (16 weeks), and can be continued throughout the pregnancy, up to the 9th month (until delivery). These exercises help strengthen the pelvic floor muscles, which are important during labor, delivery, and postpartum recovery. Benefits can be provided.
•> Circulatory Exercise
- As we know, the venous return is low during pregnancy. Therefore, to prevent such complications, it is advised to do the following exercises:
Foot and leg exercises:
- Ask the mother to stay in a semi-sitting position and advise her to support her legs. Bending and stretching of the ankles is done. After this, the mother is asked to rotate both the legs clockwise and counterclockwise. This exercise can be repeated many times.
Time for circulatory exercises: –
- Circulatory exercises, such as leg and foot exercises, can ideally be started around the 4th month of pregnancy (16 weeks) and continued until the 9th month of pregnancy (until delivery). These exercises are beneficial for improving blood circulation and reducing swelling throughout pregnancy.
Benefits
- * Blood flow improves.
- * Swelling is reduced.
- * Blood flow improves. Due to this, the condition of deep vein thrombosis can also be reduced.
- * Energy levels increase.
- * Proper posture improves.
- * Chances of conditions like varicose veins are reduced.
•> Breathing Exercises
- Knowing how to do deep breathing helps the mother during labor and also strengthens her abdomen.
- In a semi-sitting position, bend your knees and keep your feet flat on the floor. Slowly inhale and contract your abdominal muscles. Then breathe out slowly and deeply, relax your muscles, and then breathe naturally. Repeat deep breathing two to three times. This helps the mother during labor and also increases the strength of the muscles.
Time for breathing exercises: –
- Breathing exercises can ideally be started around the fourth month of pregnancy (16 weeks) and practiced throughout the pregnancy, up to the 9th month (until delivery). This exercise helps in relaxation, pain management and overall well-being during pregnancy and labor.
Benefits
- • This exercise helps in reducing stress and anxiety.
- * Improves the overall health of the mother and fetus by supplying adequate amounts of oxygen is.
- * Increases focus and concentration.
- * Increases lung capacity and strengthens respiratory muscles.
- * Provides relaxation to the body and mind, which improves sleep quality and reduces anxiety levels is reduced.
•> Points to keep in mind while exercising:
- * Warm up and cool down during each exercise.
- * Drink plenty of fluids.
- * Advise the woman to stop exercising if she feels dizzy or uncomfortable.
- * Do not overheat the body as overheating can cause birth defects.
- * Maintain good posture while exercising.
- •Your pregnancy Avoid exercising on your back from the middle of the pregnancy as it puts too much pressure on the main veins and reduces the supply of oxygen to the placenta and baby.
- Stop exercising if you notice any of the following signs, such as,
- * Vaginal bleeding,
- * Dizziness or fainting,
- •Increased shortness of breath,
- •Chest pain,
- •Headache,
- •Muscle weakness,
- •Calf muscle pain and swelling,
- •Uterine contractions,
- •Decreased fetal movement,
- •Leakage of fluid from the vaginal area. etc..
Antenatal Counseling
- Antenatal counseling is an important part of antenatal care that starts from conception and continues until safe delivery with positive results without any complications. Antenatal counseling is the process of enabling the pregnant woman to know herself and her current condition and possible changes during pregnancy so that she can make a significant contribution to the solution of her own problems and be able to take decisions for its solution.
Aim of Antenatal Counseling:
- To bring about desire changes for self-realization in the pregnant woman and her family and to adjust her physiology to the conditions of pregnancy and adjust accordingly.
- Provide assistance to solve problems through close personal relationships.
Objectives of Antenatal Counseling
- * Help women plan and prepare for birth, including decisions about the place of delivery and who will conduct the delivery.
- * Provide education about the benefits of institutional delivery and the risks involved in home delivery.
- * Advise women on where to go in case of an emergency and how to arrange for emergency transport, money, and blood donors.
- * Provide education to pregnant women and their family members about signs of labor and danger signs of obstetric complications.
- * Prepare pregnant women and their family members for emergency situations.
- * Inform women that any abnormality should be detected early and treated as early as possible.
- * Emphasize the importance of breastfeeding and exclusive breast feeding Place.
- * Advise women on nutritious diet, rest and immunization.
- * Provide information about sexual activity during pregnancy.
- * Provide information about Janani Suraksha Yojana to women and also provide education about other incentives offered by the state.
Type of Counseling During Pregnancy:
- Follow-up,
- Appraisal Services,
- Antenatal Care Importants,
- Immunization During Antenatal,
- Regular Follow-up Visit,
- Role of Mother During Pregnancy,
- Importance of Institutional Delivery,
- Incentives Available to Mother,
- Family Planning,
- Where to Go for Delivery,
- Crisis Counseling
- Promoting family planning.
- Providing information about nearby integrated counseling centers and health facilities and motivating her to connect with future services.
- Removing unknown fears by talking sympathetically and improving psychology by providing assistance in successfully going through the process of pregnancy and labor.
Counseling Process
- Counseling involves personal interaction between a client with an individual problem, which can be solved with the help and education provided by the counselor. The counselor will help educate the situation and enable the pregnant woman to decide what is right for her in the current situation. The counselor midwife does not suggest, order or pressure the woman to choose a specific course.
- She provides education to the woman so that she can make her own decisions:
- The counselor makes reports with the pregnant woman during home visits, antenatal clinics, immunization clinics or special contacts arranged for a particular purpose.
- Advise the woman to express and talk about her feelings, fears and anxieties without any hesitation should.
- By encouraging the woman to analyze her motives, the midwife gains insight into her behavior.
- Counseling is a very delicate undertaking that relies on personal feelings and private behavior, so it would be wise for the midwife to listen carefully and observe without interrupting.
- The midwife should be friendly, intelligent, and approachable. It should be neither critical nor judgmental.
- The nurse midwife explains the various ways to solve the problem or contact the situation and helps the woman decide what is right for her and her unborn child.
Minor disorders in pregnancy and their management (Minor disorders in pregnancy and their management):

1) Digestive System:
Nausea and Vomiting:
- Nausea and vomiting are very common in primigravidas and are especially common when women wake up in the morning.
- Nausea and vomiting are caused by hormones like HCG, Oestrogen, Progesterone.
- Nausea and vomiting are common It is more common in primigravida and first trimester.
- Management
Dietary Changes
- When the mother wakes up in the morning, advise her to eat dry toast, biscuits, salty crackers and protein-rich food.
- Advise the mother to eat small and frequent amounts of food.
- Advise the mother to eat low-fat food.
- Advise the mother to avoid fried and spicy food.
- Advise the mother to take proper antiemetic medication.
Constipation
- Constipation is the most common problem in pregnancy. Constipation is mainly seen during the second and third trimesters.
- Constipation is caused by the effects of progesterone, decreased intestinal tone and mobility, decreased physical activity,
- Intake of iron supplements,
- Constipation is caused by the pressure of the gravid uterus on the colon.
Management
- Advise the mother to eat high-fiber foods.
- Advise the mother to consume adequate amounts of vegetables and fruits.
- Advise the mother to drink 6-8 glasses of water throughout the day.
- Advise the mother to Drinking a glass of water in the morning activates the bowel movement.
- Advise the mother to eat frequent, small, and low-fat meals.
- Advise the mother to exercise regularly.
- Advise the mother to take small amounts of milk of magnesia.
Acidity and Heartburn
- Acidity and heartburn are common during pregnancy due to the relaxation of the esophageal sphincter.
- It is usually seen in mothers in greater numbers during the second and third trimesters.
- Acidity and heartburn are caused by the increase in progesterone levels, the decrease in intestinal volume, and the enlarged uterus. Due to displacement of the stomach, the condition of acidity and heart burn is mostly seen.
Management
- Advise the mother to eat in small and frequent amounts.
- Advise the mother not to overeat.
- Pregnant women are advised not to lie down immediately after eating. Wait at least 30 minutes after eating. Stay in an upright sitting position.
- Advise to avoid fatty and spicy foods.
- Advise the mother to sleep in a reclining position with the support of five to six pillows.
- Advise the mother to perform tailor-made sitting exercises.
- Advise the mother to take antacid medication prescribed by the health care personnel. Giving.
Bleeding from gums, glossitis and gingivitis.
- During pregnancy, high levels of progesterone can increase the blood supply, which can lead to bleeding.
Management
- Advise the mother to use a soft toothbrush.
- Advise the mother to maintain oral hygiene.
- Advise the mother to take vitamin-B complex, green leafy vegetables, yeast, eggs and cheese.
2) Circulatory System
Design and Fainting
- It is mainly caused by the relaxation of the muscles of the blood vessels due to the effect of progesterone.
- It subsides due to the increase in blood volume.
- Later in pregnancy Uterine pressure is caused by reduced blood supply to the heart due to pressure on the inferior vena cava.
Management
- Advise the mother to sleep on her back as little as possible in the last month. And advise the mother to avoid standing for long periods of time.
Giddiness (dizziness)
- Dizziness can also occur during pregnancy and due to this, balance can be lost and the possibility of falling is also seen more.
- It is usually due to cardiovascular changes during pregnancy and low blood sugar levels and also due to anemia. Can be done.
Management
- Advise the mother to take adequate rest.
- Advise the mother not to stay in a standing position for a long time.
Varicose Veins
- The condition of varicose veins is usually seen more frequently during the second and third trimesters of pregnancy.
- Varicose veins mainly develop in the lower extremities and vulva during pregnancy and hemorrhoids in the rectum are also a problem that occurs due to obstruction of venous return by the pregnant uterus.
Management
- Advise the mother to wear supportive shoes.
- Elastic crepe bandages and elevation of the limb during movement in varicose veins provide release in the symtoms.
- Ensure the mother not to remain in sitting and standing positions for long periods of time Advise to do.
- The condition of varicocele is relieved after delivery.
- Complications like bleeding or prolapse are seen in hemorrhoids. Advise to use laxatives in small quantities to keep the bowel soft and
- Advise to apply hydrocortisone ointment locally and replacement of prolapsed piles is necessary. Avoid surgical treatment as the condition reduces after delivery It occurs.
Ankle heel
- Ankle heel is usually seen during the second and third trimesters.
- It is usually seen due to vasodilation,
- Venous stasis and increased venous pressure in the uterus. is.
Management
- The mother should properly mark whether there is excess fluid retention or weight gain, as fluid retention can also be caused by pregnancy-induced hypertension (PIH).
- Advise the mother to keep her legs elevated twice throughout the day.
- Advise the mother to wear supportive stockings.
- Advise the mother to avoid sitting in one position for long periods of time. And advise to avoid standing position.
- Do not give diuretics to pregnant women until they are well because it subsides on its own with rest and elevation of the limbs.
- If there is physiological ED or orthostatic ED, there is no need to give any treatment.
3) Musculoskeletal System
Backache
- 50% of problems during pregnancy are backache.
- Backache can occur at any stage of pregnancy, but it is most common during the second and third trimesters of pregnancy.
- Backache is a joint ligament laxity (relaxin and Estrogen), weight gain, hyperlordosis, pelvic anterior tilt etc. Physiologic changes Backache is seen due to.
- Other reasons include faulty posture, high-heeled shoes, muscular spasm, constipation, and urinary infection, etc.
Management
- Advise the mother to take proper rest.
- Advise the mother to use correct body mechanism and improve body posture.
- Advise the mother to keep the legs elevated while resting.
- Advise the mother not to wear high-heeled shoes.
- Advise the mother to avoid wearing high-heeled shoes.
- Advise the mother to avoid wearing high-heeled shoes.
- Advise on performing pelvic rocking and abdominal and breathing exercises. A well-fitted pelvic girdle belt that corrects lumbar lordosis during walking.
- Advise the mother to sleep on a firm mattress.
- Massage, analgesics and rest of the back muscles can reduce pain due to muscle spasms.
Leg Cramps
- Leg cramps usually occur during the second and third trimesters of pregnancy.
- Leg cramps can usually be caused by an altered calcium phosphorus balance.
- And can also be caused by pressure from the uterus.
- Leg Cramps can be more common at night.
- Leg cramps can also be caused by calcium and vitamin B12 deficiency.
Management
- Advice on proper leg massage.
- Advise the mother to do regular exercise, especially walking.
- Advise the mother to apply local heat to the area where there is pain in the leg.
- Advise the mother to take vitamin B1 and calcium orally.
4) Genito-urinary system
Vaginal discharge
- Vaginal discharge that occurs from the first trimester to the third trimester.
- It is usually caused by hyperplasia of the vaginal mucosa and increased mucus production.
- Advise the mother to maintain proper cleansing and hygiene.
- Advise the mother to wear cotton undergarments and avoid tight undergarments.
- If there is any condition of vaginal infection, then apply vaginal application of metronidazole and miconazole as per the doctor’s advice.
Urinary Urgency and Frequency
- Frequency of micturition is observed during the 12th week of pregnancy due to the pressure of the uterus and during the 3rd trimester of pregnancy due to the pressure of the fetal head, which is relieved after delivery.
Management
- Advise the mother to have adequate fluid intake during the day.
- Advise the mother to have limited fluid intake in the evening.
- Advise the mother to void at regular intervals.
- Advise the mother to sleep in a side-lying position at night.
- Advise the mother to wear a perinatal pad if necessary.
- Advise the mother to perform eagle exercises.
5) Intengumetry System
Etching
- Straya gravidarum, poor personal hygiene, heat, race, minor skin diseases cause itching in the body.
Management
- Mother should bathe regularly and daily Advise the mother to apply calamine lotion.
- Advise the mother to apply calamine lotion.
- Advise the mother to apply talcum powder to provide a soothing effect to the mother’s skin.
- Advise the mother to maintain proper hygiene conditions.
6) Nervous System
Carpal Tunnel Syndrome
- Fluid retention causes pressure on the median nerve and the wrist, causing numbness and pins and needles in the fingers and hand.
Management
- Advise the mother to reduce salt intake in the diet.
- Advise the mother to keep her hand under the pillow.
Insomnia and headache
- Insomnia and headaches are usually more common during the second and third trimesters.
Management
- Take a bath with properly warm water at night while sleeping.
- Advise the mother to sleep in a cool and well-ventilated room.
- Advise the mother to sleep in a lateral position with the support of a pillow.
- Advise the mother to share her anxiety and fear.
- The following are the minor ailments seen during pregnancy and their management.
