ENGLISH-NEW MIDWIFERY GNM TY UNIT 7 Management of Normal Purperium
MANAGEMENT OF NORMAL PUERPERIUM

Physiological changes that occur during the puerperium period (પુરેપેરિયામ પેરિયાદ તેથી ફેસીયોલોગીકલ ચંજીસ) :
puerperium :
- The period of 6 weeks (42 days) after childbirth in which the tissues of the body, especially the pelvic organs, return to their pre-pregnancy stage both anatomically and physiologically is called puerperium.
- Duration:
The onset of puerperium is from the expulsion of the placenta to about 6 weeks, during which the uterus becomes almost non-pregnant in size.
The period is roughly divided as follows: - • Immediate:
Within 24 hours, - • Early:
Up to 7 days, - • Remote:
Up to 6 Vic
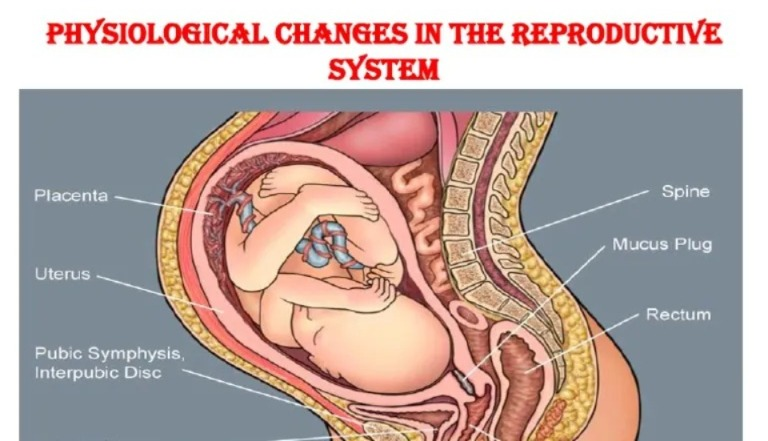
1) Physiological Changes in Reproductive System in the Puerperium Period (Physiological Changes in Reproductive System in Puerperium Period) :
( a )Involution of the uterus:
- Involution is the process in which the The process by which the uterus progressively returns to its normal pre-pregnant state after delivery is called involution of the uterus.
Anatomical Considerations
- After the placenta is delivered, it heals in the endometrium of the placental site. After delivery, the uterus becomes firm and restricted with alternate hardening and softening.
- The size of the uterus during pregnancy is approximately,
Length: 20 cm, Breath: 12 cm,
Thickness: 7.5 cm
.
And the weight of the uterus is about 900-1000 gm. Which,
The puerperium period i.e. at the end of 6 weeks of child birth, the uterus returns to its pre-pregnant state such as, the measurement of the uterus during the puerperium period is
Length: 7.5 cm, Breath: 5 cm,
Thickness: 2.5 cm and the weight of the uterus is about 60 gm.
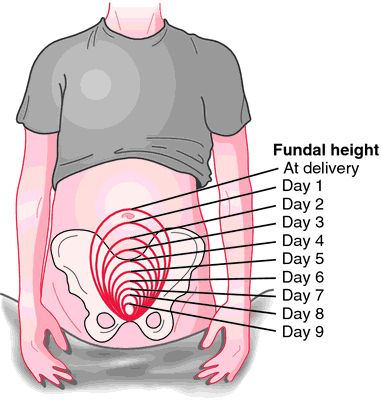
Reduction of the Size and Position of the Uterus:
- After labor, the fundus is 5 cm below the umbilicus and 12 cm above the symphysis pubis.
- After 24 hours, it is at the level of the umbilicus. The uterus descends into the pelvic cavity at a rate of 1.25 cm/hr and is not palpable abdominally above the symphysis pubis after 10 days.
Consistency of the uterus:
- The frequent strong myometrial contractions cause the uterus to become hard due to uncontrolled blood flow to the uterus. Its consistency can be felt by palpation. It should feel firm and round if If the funds are soft, it is called a boggy uterus, indicating that contractions are inadequate and blood loss is ongoing.
( b ) Involution of the cervix :
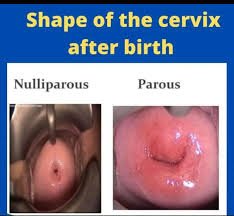
- After delivery, the lower uterine segment and cervix remain loose, thin and stretched
- They may be edematous, bruised and have small tears and lacerations. It takes a few weeks for the isthmus to return to its normal shape and size.
- The consistency of the cervix on the first post-partum day remains normal enough to admit two fingers. Then by the end of the first week, it remains soft enough to admit the tips of the fingers. The evolution of the cervix continues for 3-4 months. But the perianal cervix never looks like a non-perianal cervix. The external os, which first looked like a dimple, now looks like a slit.
(C) Vaginal canal (vaginal canal):
- It takes about 4 to 8 weeks for the distensible vagina to involute. After delivery, the vaginal canal appears swollen and smooth, gradually becoming smaller and firmer but never reaching its pre-pregnancy size. The introitus remains permanently large, and the hymen is lacerated. Represented in the form of nodular tags.
(d) Perineum:
- The muscles of the perineum floor become stretched, swollen and bruised, with a scar resembling an episiotomy.
( e ) Broad ligaments and round ligaments :
- The broad ligaments and round ligaments take some time to recover from stretching. Initially the ligaments are stretched but by the end of the puerperium period the ligaments return to their non-pregnant length.
( f ) Pelvic Floor and Pelvic Fascia :
- The pelvic floor and pelvic fascia take a long time to involute from the stretching effect.
(f) Lochia :
- The vaginal discharge that occurs during the first 15 days of the puerperium period is called lochia and comes from the uterine body, cervix and vagina.
- It contains blood vessels, decidual tissue, epithelial cells of vaginal mucus, bacteria, membrane fragments and small clots.
- Odor of lochia
- The odor (smell) of lochia is fishy.
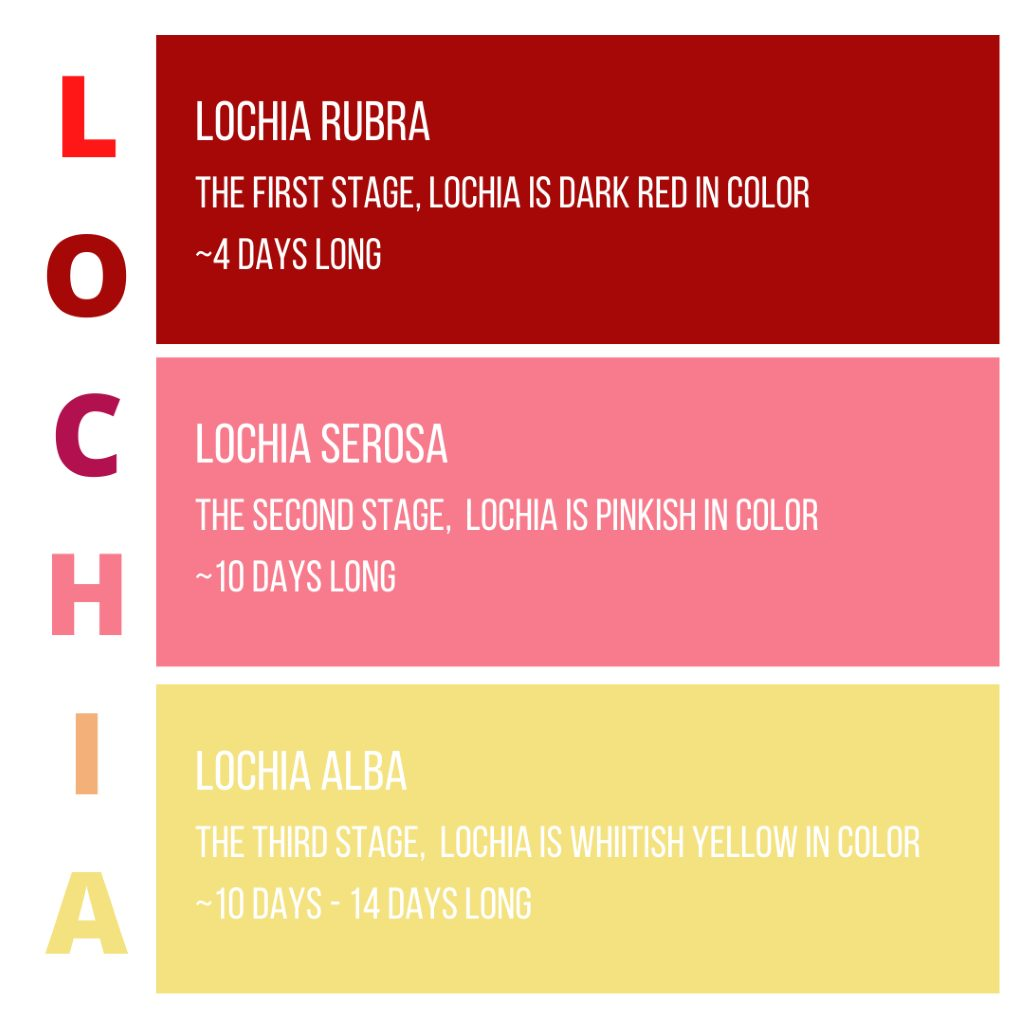
Type of lochia:
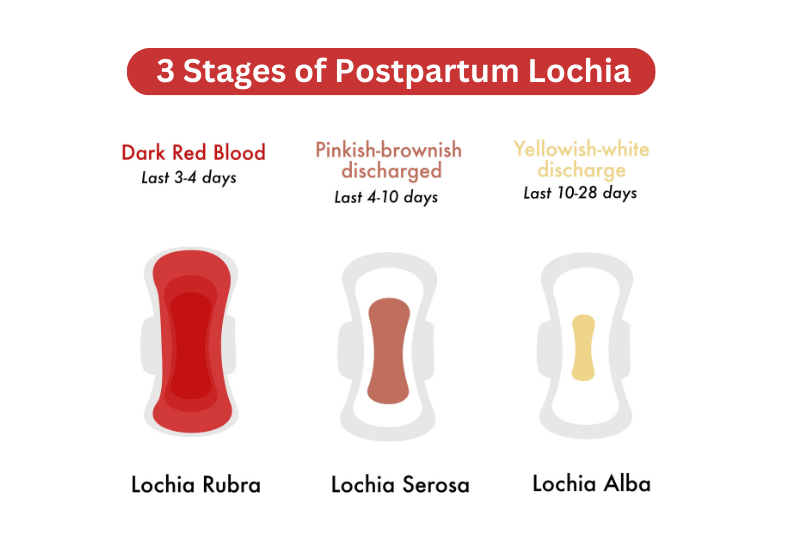
There are three types of lochia.
- 1) lochia rubra,
- 2) lochia syrosa,
- 3) lochia Alba.
1) Lochia Rubra :

- Lochia rubra is the first phase of lochia. In which the discharge is red and bloody and lasts for 1 to 4 days after childbirth.
- Lochia rubra contains blood, fetal membrane, decidua, vernix caseosa and lanugo.
2) Lochia Serosa (Lochia serosa):

- Lochia seroosa is the second phase of lochia.
Which is seen as yellowish pale or pale brownish in color. - Lochia seroosa lasts for 5 to 9 days.
It has a small amount of red blood cells but a high amount of leukocytes,
wound exudate,
mucus and microorganisms are found in it.
3) lochia Alba (Lochia Alba):

- Lokia Alba is the third phase of Lokia. It is usually pale white in color.
- Lochia alba is visible for 10-14 days.
- It contains a large amount of decidual cells,
- Leukocytes,
- Mucus,
- Cholesterol crystals,
- Fatty and grandular epithelial cells
- And microorganisms are found in it.
Amount:
- The average amount of lochia is about 250 ml during the first 5 to 6 days.
Normal Duration:
- The normal duration of lochia is up to three weeks. If it persists beyond three weeks, it may be a local lesion.
Clinical Importance of Local Discharge:
- As lochia provides information about the mother’s perinatal state, it is important to assess lochia.
- Odor (smell): May be due to offensive infection.
- Odor: Scanty or absent infection May be due to.
- Amount:May be due to scanty or absent infection.
- Color: Continuous red lochia may be due to subinvolution.
- Duration: If lochia lasts for three weeks or more Even then, if it is for a longer period of time, there may be local listening.
(2) Breast and lactation :
Breast:
- Breasts develop during pregnancy due to hormonal stimulation. For a few days after delivery, both the feeding and non-feeding breasts secrete colostrum. Colostrum is the creamy yellow precursor to milk. This makes the breasts soft and non-tender.
- After three days, prolactin levels increase and the breasts become firm and tender. Then milk secretion starts. Due to increased blood flow, venous and lymphatic congestion, the breast becomes distended, hard and warm. This is called physiological engorgement.
- It lasts for 24 to 48 hours and then resolves on its own. Milk production is stimulated by the baby’s sucking. The breast feels firm, full and tender until it is empty.
Lactation (lactation):
- Lactation is the process of breastfeeding that is based on the interplay of hormones, instinctive reflexes, and learned behaviors of the mother and newborn.
Lactation is particularly under the control of the hormones prolactin and oxytocin and is maintained by three factors: - 1) The anatomical structure of the mammary gland, the development of the alveoli, ducts, and nipples.
- 2) The initiation and maintenance of milk secretion.
- 3) Milk ejection or propulsion of milk from the alveoli to the nipple.
Physiology of Lactation :

Lactation
- Lactation is the process of breastfeeding by which the mammary glands produce and release milk to provide nourishment to the child. It is caused by hormones Complexity occurs through interplay. Prolactin and oxytocin are the main hormones that act to induce lactation.
- The establishment and maintenance of lactation is generally determined by three factors:
- 1) The anatomical structure of the mammary gland, such as the development of the alveoli, ducts, and nipples.
- 2) The initiation and maintenance of milk secretion.
- 3) The movement of milk from the alveoli to the nipple The ejection or propulsion of milk.
The two main hormones responsible for lactation are:
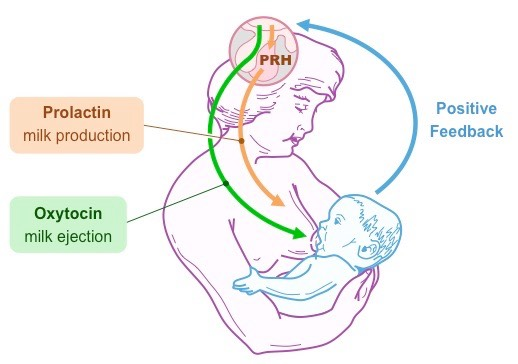
Prolactin and oxytocin work as important hormones for lactation.
1) Prolactin:
- Prolactin hormone is secreted from the anterior pituitary gland.
- It is the primary hormone for the stimulation of milk production (lactogenesis).
- During pregnancy, the hormones estrogen and progesterone are increased. These hormones prepare the breasts for milk production but inhibit lactation.
- After the birth of the child, the hormones estrogen and progesterone The level decreases due to which the effect of prolactin hormone can be felt on the mammary gland and the secretion of milk increases.
2) Oxytocin:
- Oxytocin is released from the posterior pituitary gland.
- The release of oxytocin is usually triggered by the baby’s sucking and nipple stimulation. It is crucial for milk ejection (let-down reflex) that depends on stimulation.
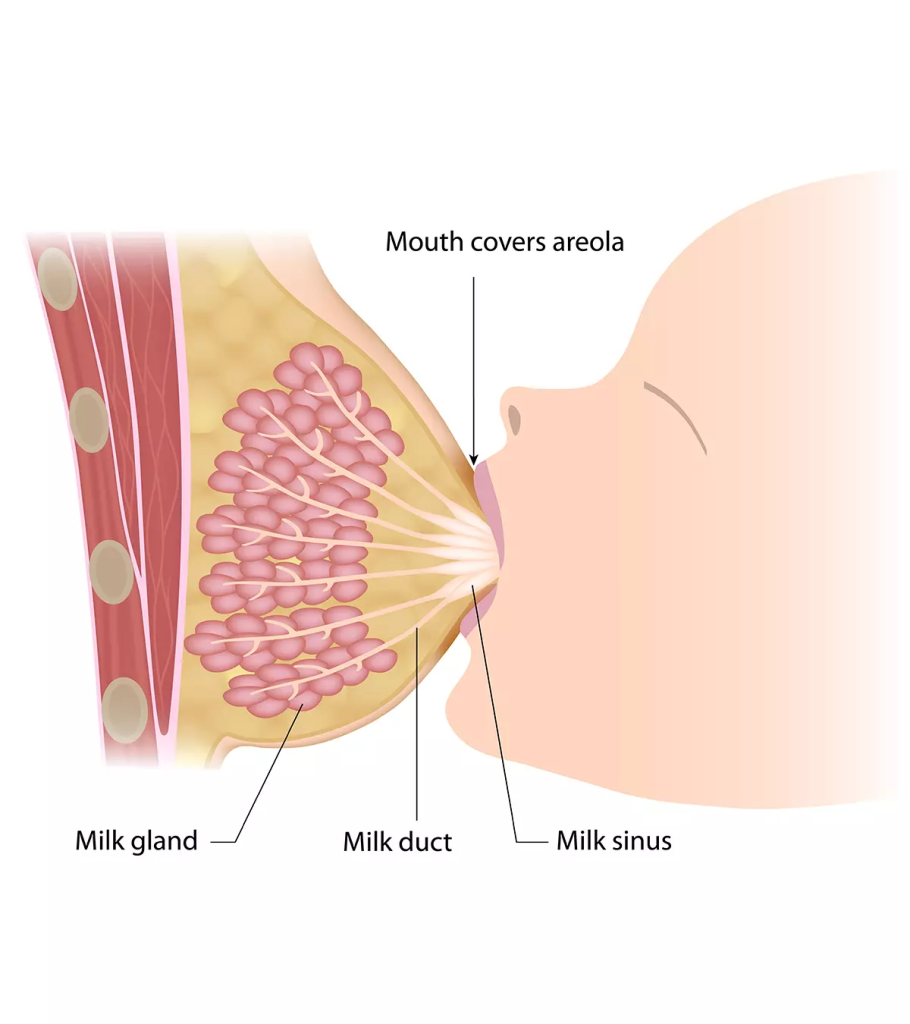
- Oxytocin is an important hormone for the contraction of myoepithelial cells surrounding the alveoli (milk producing glands), due to which milk enters the duct from the alveoli and then from the duct to the nipple for breastfeeding.
•> Lactation is divided into four phases based on physiological basis.
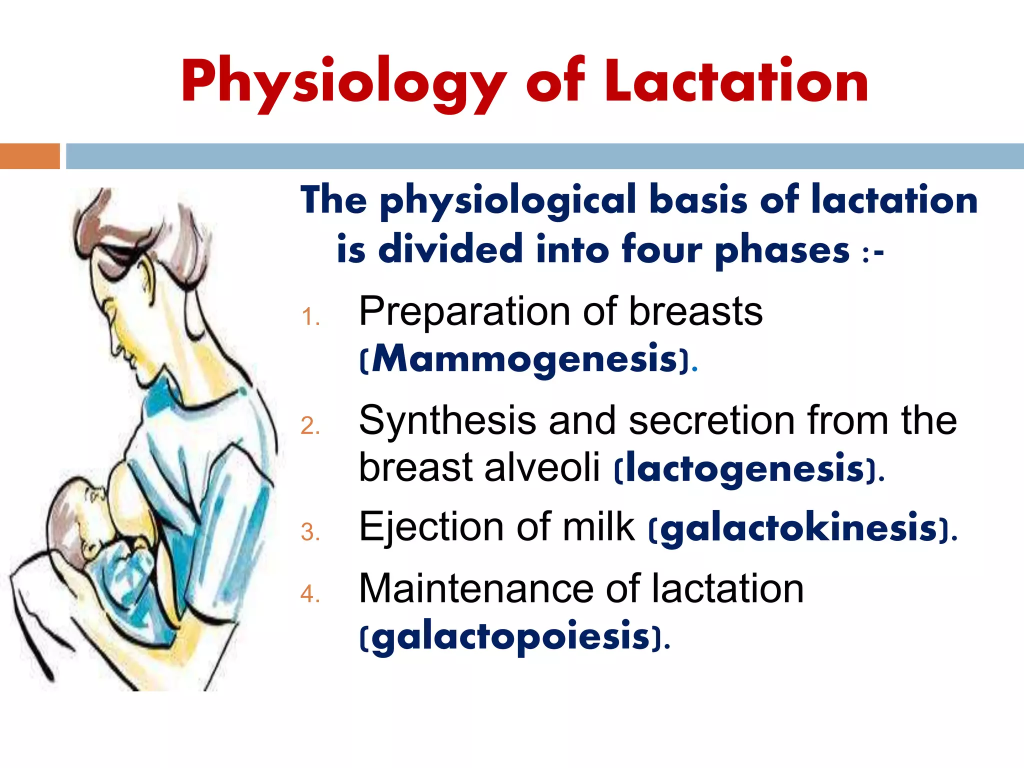
1)Mammogenesis (preparation of breast),
2)Lactogenesis (synthesis and secretion of milk from breast alveoli),
3)Galactokinesis (ejection of milk),
4)Galactopoiesis (maintenance of lactation)
1)Mammogenesis (preparation of breast):
- During this stage, the ductal and lobuloalveolar system of the breast grows during pregnancy, in which the breast is prepared for the secretion of milk.
2) Lactogenesis (synthesis and secretion of milk from the breast alveoli):
- Some secretory activity (colostrum) that occurs during pregnancy increases after delivery.
- Actually, milk secretion starts on the third or fourth day postpartum. During this period, the breast feels engorged, tense, tender and warm.
- Despite high prolactin levels during pregnancy, due to the effects of steroid estrogen and progesterone hormones, the breast tissue does not respond to prolactin hormone and milk secretion does not occur. However, after delivery, as estrogen and progesterone levels fall (decrease), prolactin hormone Milk secretion activity starts in the mammary gland. Prolactin and glucocorticoid hormones are important at this stage.
- Secretory activity is increased directly or indirectly due to growth hormone, thyroxine and insulin.
3)Galactokinesis (Ejection of Milk):
- Milk is not only released by the baby’s shaking but also by a contractile mechanism.
- The hormone oxytocin is the major galactokinetic (milk ejection) hormone.
- The reflex is set up during the baby’s shaking.
- Then the impulses from the nipple and areola pass through the thoracic sensory nerves and release oxytocin in the hypothalamus. Synthesizes and then reaches the hypothalamus to transport the synthesized oxytocin to the posterior pituitary gland.
- The oxytocin hormone is released from the posterior pituitary gland, which then causes the myoepithelial cells surrounding the alveoli (milk producing glands) to contract.
- This process is called “milk ejection” or “milk let-down reflex”.
- Where milk is forced From there it enters the ampulla of the lactiferous duct, from where it is released by the mother’s expression or by the baby’s sucking.
- The let-down reflex is triggered by the baby’s crying even without shaking.
- The pressure of the milk in the breast that increases before the baby sucks is called “draft”. It is also produced by injection of oxytocin.
- Milk ejection reflex is inhibited due to pain, breast engorgement. If the ejection reflex is inhibited for more than a few days after the start of milk secretion, breast engorgement occurs.
4)Galactopoiesis (Maintenance of lactation):
- Prolactin is a It is a single and important galactopolytic hormone.
- For effective and continuous lactation, suckling is necessary not only for the milk to come out of the gland but also for the release of prolactin.
- The production rate of milk decreases due to the pressure of milk in the breast, so periodic breast feeding can reduce that pressure and maintain the secretion of milk.
- A healthy mother produces 500-800 ml of milk to feed her baby.
- Accordingly, the physiology of lactation is divided into 4 phases.
Milk Production:
- A healthy mother produces 500 to 800 ml of milk to feed her baby.
(3) Cardiovascular Changes:
- Blood Volume The blood volume that increased during pregnancy decreases and the circulatory system returns to its prepregnancy state.
- Cardiac Output Excess water in the body is removed from the body due to diuresis and diaphoresis and cardiac output returns to its normal range.
Hemoglobin and Hematocrit Levels:
- During pregnancy, due to blood loss, the hemoglobin and hematocrit levels initially decrease, but within a few weeks, the blood stabilizes within its normal range.
4) Respiratory Function:
- After delivery, the diaphragm descends as abdominal pressure decreases, improving lung expansion and ventilation, but there are no noticeable changes in respiratory rate.
(5) Endocrine Changes:
Hormone Shift:
- Pregnancy-related hormones such as estrogen, progesterone and human chorionic gonadotropin (HCG) hormone are reduced.
- Prolactin hormone The level is elevated to maintain breast feeding.
(6) Renal Changes
Diuresis
- Urine output increases due to which the fluid accumulated in the body during pregnancy is Excreted from the body.
Bladder Function
- The bladder regains its tone and function, although some temporary issues such as urinary retention or urinary incontinence may occur.
(7) Gastro intestinal changes:
Bowel function
- Bowel function takes some time to normalize but due to its motility being reduced, a condition of constipation is seen.
- Appetite in women becomes normal in a short time but bowel changes are seen in some women for a short time is.
(8) Musculoskeletal Changes:
Abdominal Muscles
- The tone of the abdominal muscles regains in a short time while the pelvic floor muscles also return to normal in a short time, but the pelvic floor Kegel exercises are important in strengthening the muscles.
(9) Psychological Changes
- Hormonal fluctuations, physical recovery, and the demands of newborn care impact emotional well-being. It is also common to experience mood swings such as the “baby blues”. And some women also experience postpartum depression.
- Thus, such physiological changes are seen in women during the postpartum period.
Management of Normal Puerperium (Management of Normal Puerperium):
Postnatal Care of Mother: Postnatal Care in Mother And along with systemic examination of the baby, appropriate advice is provided to the mother.
Aim and Objectives:
- To provide support to the mother and family in the new changes that are taking place.
- To provide early diagnosis and treatment to prevent any complications in the mother and infant.
- To provide early referral services to the mother and infant if needed, such as,
a) To support breastfeeding,
b) To provide counseling services in nutrition, complementary feeding and immunization.
c) Proper counseling about contraception To provide.
Principles of Normal Puerperium:
- 1) To restore the health status of the mother.
2) To prevent infection.
3) To promote lactation.
4) To motivate the mother to accept contraceptives. - In puerperium management To make a woman physically and emotionally normal, the following principles should be kept in mind, such as,
1) Maintaining the health status of the mother.
2) Preventing infection.
3) Promoting best feeding.
4) Providing care to the baby.
5) Motivating and guiding for family planning.
6) Providing health education as per the need.
Management of Normal Puerperium (Management of Normal Puerperium)
Immediate Attention:
Immediate Post Natal Care
- The period up to one hour after the expulsion of the placenta is called the fourth stage of labor, in which the general condition of the patient and the behavior of the uterus are monitored.
Observation of Women
- This includes the mother’s vital signs such as,
- Temperature,
- Pulse,
- Respiration,
- And blood pressure is properly monitored. If it is slightly elevated, it is usually due to fatigue and dehydration, and Check vital signs every 15 minutes for the next 1 to 2 hours until the patient is stable. Then assess the condition of the uterus, which is firmly contracted and in the midline.
Rest and Ambulation:
- It is beneficial to ambulate the patient immediately after delivery, as the patient feels well, bladder complications and constipation are reduced, followed by ureteral drainage, which leads to rapid involution of the uterus and reduces embolism. After normal delivery, the patient can do some work.
Diet:
- The patient should be given a normal diet as per his/her wish. If the patient is lactating, then a high calorie diet, adequate protein, fat, more fluid, minerals and vitamins should be given. If the mother is non-lactating, then a diet should be given according to the non-pregnant state.
Bladder Care:
- After delivery, the patient should be encouraged to pass urine as per his convenience. Sometimes, the patient’s position is not proper or the patient cannot pass urine due to pain from perineum injury. Then, the patient should be properly provided with privacy. Then, the patient should be encouraged to urinate and if the patient cannot pass urine, then catheterization should be done properly. Continuous catheterization should be kept until the bladder tone returns. Proper bladder care should be used to prevent infection and cystitis.
Bowel Care:
- Early ambulation and proper diet reduce the problem of constipation. Adequate fiber-rich food and fluids do not cause bowel problems and if required, mild laxatives should be provided to the patient such as mild milk of magnesia 4-6 teaspoons at bed time.
Slip:
- The patient needs both physical and mental rest, so the patient should be provided with proper work and a comfortable environment. The patient gets adequate amount of sleep to support them physically and mentally. If the patient has any problems like painful piles and engorged breasts, proper analgesic medicine should be provided.
- The mother should be advised to get at least 7-8 hours of sleep during the night and 1-2 hours of sleep during the day.
Care of the Vulva and Episiotomy Wound:
- After delivery, clean the vulva and buttocks with saline, lotion, soap, and water. Apply antiseptic ointment or lotion to the episiotomy and provide a sterile pad. Provide care after each urination and defecation. This will reduce the pain.
- Many women find relief from warm water sitz baths.
Care of Breast:
- Wash and clean the breasts and nipples with water. Apply soap while taking a bath. Provide frequent and short fitting to prevent nipple soreness.
- Maintain aseptic technique especially in the first week of puerperium and use local and antiseptic dressings in the wound. Use of clean bed linen and clothing, clean surroundings, and limiting visitors to a limited number can help reduce nosocomial infections.
- If Rh negative, give Anti-D gamma globulin within 72 hours of delivery. If a second dose of tetanus toxoid was not taken during pregnancy, it should be provided at the time of discharge.
- Objectives of Postnatal Exercises:
- Improve abdominal and perineal muscle tone.
- Advise the mother to do small amounts of daily routine activities.
Aseptic and antiseptic:
Immunization:
Postnatal Exercises:
Attachment and warmth (bonding):
Family Welfare :

- India is the first country in the world to implement a family welfare program on a national basis through the government. Family welfare is also known as the family planning program. This family planning program was included as an official program since 1952.
Definition (Definition) :
- Family planning means planning a family size that is affordable by the parents and is for the health and welfare of the family. Family planning is a program that helps an individual or couple to achieve the following objectives.
- 1) Avoiding unwanted births.
2) Achieving wanted births.
3) Maintaining a gap between two pregnancies.
4) Appropriate use of contraception methods.
Objectives of Family Welfare Program:
- The National Family Welfare Programme in India is a comprehensive initiative aimed at improving the health and well-being of families.
- The Family Welfare Programme is designed to achieve various objectives to improve family life and societal health.
- Here are the objectives of the Family Welfare Programme.
Objectives of Family Welfare:
- The objectives of family welfare include improving the overall health and well-being of the family.
- The objectives of family welfare are as follows:
1) Promoting re-productive Health:
- Ensure access to reproductive health-related services to maintain the reproductive health of families, including,
- Family planning, maternal and child health care, and prevention and management of reproductive tract infections. They get involved.
2) Reducing Maternal Mortality Rate:
- Maternal death and complications can be reduced by providing skilled care to the mother during pregnancy, childbirth, and the postpartum period.
3) Reduce Infant and Child Mortality:
- Proper nutrition, immunization and proper health care services for infants and children can reduce child morbidity and mortality rates.
4) Promoting Family Planning:
- Encourage individuals or couples to use contraceptive methods to space their pregnancies and plan pregnancies according to choice.
5) Ensuring Safe Motherhood:
- Promoting safe child birth practices, prenatal care and postnatal care to improve maternal health outcomes.
6) Improving Nutrition and Hygiene:
- Assess malnutrition and promote hygienic practices to improve the overall health and well-being of families.
7) Preventing and Management of Communicable Diseases:
- Infections that affect reproductive health such as sexually transmitted and other communicable diseases Identify and treat diseases in this way.
8) Social Support:
- Social support should include providing a social support system to families and mainly vulnerable populations such as single-parent households, low-income families, and families with disabilities and chronic illnesses. This support involves financial assistance, counseling services, and community-based support.
9) Promotion of Small Family Sizes:
- Encourage families to voluntarily choose small family sizes to improve maternal and child health outcomes and overall family well-being.
10) Promotion of spacing method:
- Advising the use of contraceptives to keep space between pregnancies. Due to which healthier outcomes for the mother and her child can be promoted.
11) Ensuring access to contraceptives:
- Ensuring that adequate contraceptives reach all eligible couples to properly adopt family planning.
12) Prevention of Unwanted Births:
- Providing information and services to prevent unintended pregnancies, which can lead to better maternal health and improved socio-economic outcomes for families.
13) Promotion of Plan Pregnancy:
- Encourage couples to plan and prepare for pregnancy in order to promote the health of both mother and child.
14) Promotion of birth spacing:
- Encourage families to keep adequate space between pregnancies To provide advice that can maintain the overall well-being of the mother and child and reduce complications due to close pregnancy.
15) Appropriate Childbearing:
- Advise families to plan appropriate pregnancies to reduce complications due to early or late pregnancy.
- These objectives collectively aim to empower individuals and families to make informed choices about their reproductive health and family planning, thereby improving overall health outcomes and enhancing the quality of life for families.
Role of Nurse in Family Welfare Program :

- The role of a nurse in a family welfare program is diverse and multifaceted. Nurses play different roles in different settings of family welfare services. It usually depends on their post and their capacity to perform the work.
- The role of a community health nurse (CHN) in family welfare services is important in promoting reproductive health, family planning and overall well-being in the community. Here are the main aspects of their role:
1) Survey work:
- The nurse collects demographic facts through surveys.
- She makes a list of the house numbers and their locations in the community.
- The nurse collects demographic facts through surveys. Collects information on pregnant mothers, eligible couples,
- Contraceptive users, children and children below school-going age. Then, couples are classified into high, medium, and low priority.
- To collect feedback on how many couples are using contraceptives and how many people are not using them to form the next action plan.
2) Health Education:
- To educate individuals, families, and communities To provide education on health and family planning.
- To make people aware about the available family planning services.
- To provide education and detailed information to couples about different types of contraceptives so that they can adopt them according to their choice.
- To provide education to mothers to breastfeed their children for at least one year as it works as a natural contraceptive.
- Provide education on immunization, nutrition, first aid and personal and environmental hygiene in the community.
3) Coordinator and Provider of Family Welfare Services:
- Supply various types of contraceptives available to eligible couples.
- To arrange family planning clinics and camps to create awareness about the needs of the people and the available services.
- To follow the rules and regulations of the State Government and the State and provide direct services within legal and professional limits.
- It coordinates the services of gynecologists and other family welfare services personnel.
5) Motivation function:
- Motivates eligible couples to adopt small family norms by using contraceptives.
- Works to explain the need and importance of family planning.
- Identifies women who need medical termination of pregnancy and refers them to doctors early.
- For adequate contraceptive supply and distribution in every village Establishing depots to ensure adequate supply of contraceptives.
6) Administrative Role:
- Determining dates and locations of family planning clinics, arranging equipment, supplies and other resources in the clinics.
- Supervision of multipurpose health workers in the clinics To provide guidance and distribution of contraceptives and insertion and removal of IUD.
- Provide assistance to the Medical Officer in conducting the clinic.
- Organize camps for family planning and assist doctors in male-female and female sterilization operations.
- Maintain aseptic technique during the operation.
- Couples who have accepted the method of family planning Provide them with follow-up services.
- Plan and evaluate education programs.
7) Consultant:
- As a coordinator in family welfare services and as a direct care provider, it is important to consult with them before starting any type of health care program in the community. is.
8) Counselor:
- The nurse counsels eligible couples and target couples on different contraceptive methods and provides them with the opportunity to choose the best suitable method for spacing.
9) Supervisory Role:
- As a supervisor, the nurse working in the family welfare department encourages her staff to actively participate in the family welfare program.
- As a supervisor, the nurse organizes in-service education programs for health workers, professionals, and nursing personnel.
10) Domiciliary Services:
- Home visits are an important part of the family program. These services are provided by multipurpose health workers and health assistants.
- The services include,
- Providing education and motivation to eligible couples.
- Providing advice for follow-up if using IUD and pills and providing education for follow-up in cases of vasectomy, tubectomy, medical termination of pregnancy (MTP).
- Providing domiciliary care for antenatal, postnatal, newborn and toddler.
- Providing referral services if anyone has post-operative complications.
11) Record Maintenance:
- The nurse is responsible for maintaining all records in the family planning program such as,
- eligible couple records,
- target couple records,
- intrauterine devices records,
- sterilization operation records,
- Clinic and Camp Records,
- Health Education Activity Records,
- Training Records,
- Medical Records etc.
- The nurse is responsible for preparing monthly reports and submitting them to the authorities.
12) Role in Research:
- The community health nurse is a primary member of a multidisciplinary research team. The nurse is required to cooperate and participate in the research activities of the Family Welfare Services.
13) Evaluation Role:
- The nurse evaluates the work performed in the Family Welfare Program and prepares its reports. On the basis of this evaluation, any further changes are made in the implementation of the program and the desirable targets are achieved.
14) Collaborator:
- Community Health Nurses work in collaboration with health teachers and non-governmental organizations in the community to improve health care services.
- Nurses work collaboratively with doctors, dispensers, vaccinators, trained birth attendants, and lady health visitors to provide family welfare services in the community.
- Community health nurses play a crucial role in empowering individuals and families to make informed decisions about their reproductive health, supporting healthy pregnancy and childbirth, and contributing to the overall well-being of the community through effective family welfare programs.
Contraception method :

- A contraceptive method is a method by which a woman can prevent an unwanted pregnancy. Contraception means all measures, temporary or permanent, that prevent pregnancy caused by the coital act.
Characteristics of an ideal contraceptive:
- They are usually expensive.
- They are effective in preventing pregnancy.
- They are safe for health and free from harmful effects.
- They are simple and some contraceptive methods do not require the supervision of a doctor and medical personnel.
- Some contraceptives are reversible That is, it does not obstruct when there is a desire for pregnancy.
Types of contraceptives (Types of contraceptives):

A) Spacing Method/Temporary Contraception:
Barrier Method:
- •Physical Methods.
•Chemical Method.
•Combined method. - Intrauterine device,
Hormonal method,
Postconceptional method,
Miscellaneous
B) Terminal method /permanent contraception:
- Male sterilization (vasectomy),
- Female Sterilization (Tubectomy).
A) Spacing Method/Temporary Contraception :
- Temporary methods are generally used to postpone births and to keep space between births. This method is used more by couples who do not want more children or who want to keep space between children.
Barrier method:

The barrier method prevents the sperm from connecting with the egg. This is called the barrier method.
This barrier method prevents sperm from being deposited in the vagina and also prevents sperm from penetrating the cervical canal. It usually uses mechanical, chemical and combined methods.
Physical method: Includes male condoms, female condoms, diaphragms, vaginal sponges.
Chemical Method:
Cream: Delfen/Pharmatex
Jelly: Coromax, Volper Paste.
Foam Tablet: Aerosol Foams, Chlorimin T, Contab.
Combination: It usually uses a combination of mechanical and chemical methods.
Combined Method:It uses a combination of mechanical and chemical methods. is.
1.Male condom:

- The male condom is a male barrier contraceptive that comes from the Latin word “condom” and was invented by Dr. Condom. The latest condoms are available in different sizes, ranging from 160-180 mm in length, 49-52 mm in width and 0.04-0.07 mm in thickness. They are plain or teat shaped with a tip for semen collection. They are available in different colors. Among them, dry type Ex: Nirodh (Government Supply) and Kohinoor, prelubricated type Ex: Durex, Kamasutra and or spermicidal ones Ex: Raksha etc. are available.
- It is an effective and very widely used device which does not have any side effects and can also prevent pregnancy. Condom prevents both male and female from sexually transmitted diseases (STD).
Advantages:
- Inexpensive and has no contractions or side effects.
- Disposable for use, simple and easy to carry.
- It provides protection against sexually transmitted diseases (STDs) and pelvic inflammatory disease (PID).
- Tubal fertility and ectopic Reduces the incidence of pregnancy.
- Used when coitus is irregular and infrequent.
- Prevents premature ejaculation.
- Used when pills and IUCD are contraindicated.
DishAdvantages:
- Sleep or break occurs during coitus.
- Sexual pleasure remains insufficient. Psychological disturbances remain.
- Latex allergy may be created.
Female condom (Female condom) :

- Female condom is a newly developed female barrier contraceptive. It combines the features of a diaphragm and a condom. It is made of synthetic latex or polyurethane. It is a pouch-like structure in which the internal ring covers the cervix and the external ring remains on the outside of the vagina. It is prelubricated with silicone and does not require spermicide.
Advantages:
- It prevents STDs (sexually transmitted diseases) more effectively than male condoms because some female condoms also cover the perineum.
- It is made of polyurethane, so it does not cause allergic reactions.
- It is more convenient than male condoms because it has to be inserted before intercourse and the chances of breakage are less.
Disadvantages:
- It is expensive.
- Some women have difficulty in insertion.
- Failure rate 5-21/100 women.
Vaginal diaphragm:
- This is an intravaginal device made of synthetic rubber, flexible metal, or plastic material. Its diameter is 5 to 10 cm. It has a flexible rim, which is usually made of spring or metal. A medical or paramedical person is required to measure its size. Its rim extends from the upper end of the posterior fornix in the vagina to its lower end at the back of the symphysis pubis, completely covering the cervix. It should be kept in place for a minimum of 6 hours after sexual intercourse. Failure rate is 4-12/ 100 women.
Vaginal sponge:
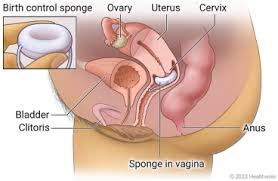
- This combined vaginal barrier contraceptive is a sponge made of polyurethane. It contains 1gm of Nonoxonal-9 spermicide. Its cap is like a mushroom cap. Its concave side covers the cervix in the upper vagina. The vaginal sponge is easy to use. It needs to be moistened with water and inserted into the vagina. It remains effective for 24 hours. It releases 125 – 150 mg Nonoxonal in 24 hours.
Chemical Method:

- Its other name is also spermicide because it kills sperm thus chemical contraceptive prevents pregnancy.
- Ex: Foam tablet, aerosol, cream, jelly, paste, suppository, soluble film etc. All these spermicides should be inserted deep into the vagina 15 minutes before the side coats.
Advantages:
- It is easy to use.
- It is not very expensive and increases vaginal lubrication.
DishAdvantages:
- It has to be inserted deep into all the areas where the form reaches and before every sexual activity. The couple may experience irritation and burning sensation.
Combine method (Combine method):
- If barrier method is used with chemical method, it is called combined method It is called a double protection device.
Intrauterine device (IUCD) IUCD ( intrauterine contraceptive device )
Introduction
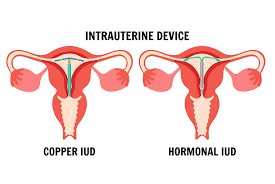
- Intrauterine device is a small, T-shaped, flexible device that is inserted into the uterine cavity to prevent pregnancy. Intrauterine devices (IUCDs) are a popular method of long-term contraception that has been involved in family welfare programs due to their effectiveness. After Grafenberg Ring was used in Germany in 1929 by Grafenberg, many different types of devices were invented, which are mainly divided into two categories.
In which,
1) Copper IUCD (Copper T)
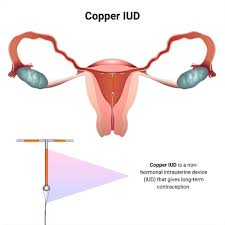
- Description:
Made of plastic and copper Is. Copper acts as a spermicide, preventing fertilization. - Duration
Effective for 5-10 years, depending on the specific type. - Examples: Copper T 380A, Multiload 375.
2) Hormonal IUCD (LNG-IUD)
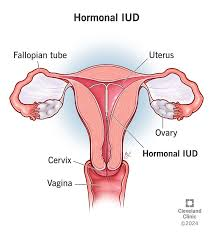
- Description:
Made of plastic and releases levonorgestrel, which thickens cervical mucus, prevents sperm, and thins the uterine lining. - Duration
Effective for 3-5 years. - Examples:
Mirena, Skyla, Liletta, Kyleena.
The following contraceptive devices are involved in intrauterine contraceptive devices.
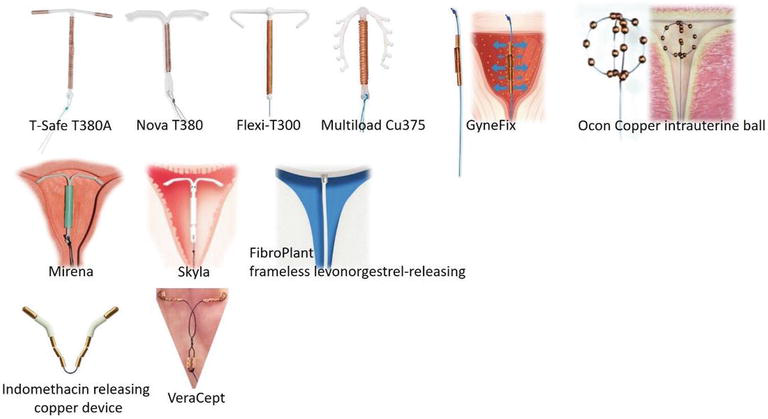
1)lippes loop
2)CU T 200 B
3)CuT 380 A,
4)Multiload Cu 250,
5)Multiload 375,
6)progesttasert,
7)Levonorgestrel IUCD.
1)lippes loop:
- The Lipis Loop is a first-generation intrauterine device by Lipis The loop is made of polyethylene. It is double S-shaped and has a nylon thread attached to it which remains in the vagina, which helps in removing the loop from the intrauterine cavity. It is available in four sizes, namely,
- A, B, C and D.
The Lipis loop is nontoxic, reliable and stable. It can also perforate the uterine wall. It contains a small amount of barium 5, which makes it visible on X-rays, but it is not currently used.
2) CU T 200 B:

- CU T 200 B is a widely used medicated device. In which a copper wire with a surface area of 215 sq mm is wound around the vertical stem of the device.
- The stem of the T-shaped device is made of a polyethylene frame. It has a polyethylene monofilament which is tied to the end of the vertical stem.
- This device is removed after 4 years.
3)CuT 380 A:

- CuT 380 A is a government supply CuT 380 A. It consists of a T-shaped device with two solid copper slim transverse arms and a copper wire on the vertical stem.
- The total surface area of copper is 380 Sq mm, of which 314 mm is on the wire and 33 sq mm on each copper sleeve. It has a monofilament white thread. It remains effective for about 10 years.
4) Multiload Cu 250:

- The device is available in a sterile packet with an applicator. It does not include an introducer or plunger.
- The device releases 60-100 µg of copper per day over a period of one year. The device has to be replaced after 3 years.
5)Multiload 375:

- It has a surface area of 375 mm² of copper wire around its vertical stem. Replacement is every 5 years.
6)progesttasert:
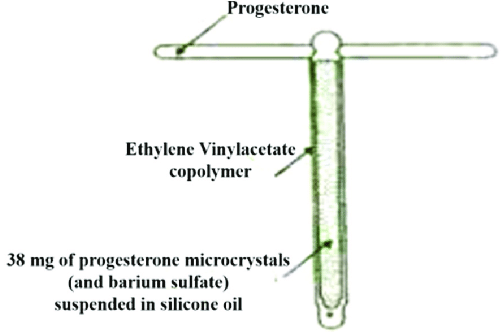
- A bioactive core containing microcrystals of progesterone (38 Mg) is enclosed within a plastic wall that releases approximately 65 µg of progesterone into the uterine cavity each day. The release continues for only one year. Thus, it should be replaced after one year.
7)Levonorgestrel IUCD:

- This is a T-shaped device
- A polydimethylsiloxane membrane around the stem acts as a reservoir for the steroid. The total dose of levonorgestrel is 52mg, which is released at a rate of 20 µg/day. This device is replaced every 5 years.
•>Mechanism of Action
Hormonal IUD
Releases copper ions, creating an environment inaccessible to sperm. Prevents sperm from fertilizing the egg. Can prevent implantation if fertilization occurs. Releases levonorgestrel to thicken cervical mucus, preventing sperm from entering the uterus.
Suppresses endometrial growth, making the lining of the uterine cavity unsuitable for implantation. Partially suppresses ovulation in some females.
Benefits
Effective:
More than 99% effective in preventing pregnancy.
Long-lasting:
Works as a contraceptive for many years.
Reversible:
Fertilization quickly returns after removal Comes.
Convenience:
Little maintenance is required after insertion.
Cost-effective:
Economically affordable.
Insertion and Removal
Insertion:
Is performed by trained health care personnel. Pregnancy can usually be terminated during the menstrual period or at any time.
In the procedure, the IUD is inserted into the uterine cavity through the cervix.
Removal:
Can be done at any time by a healthcare provider.
Fertilization usually returns immediately after removal.
Common side effects:
Camping pain during and after insertion.
Irregular erections and ejaculations, especially during the first month.
Heavy menstrual bleeding.
Shortened or missed periods with hormonal IUDs.
Risks
- Expulsion (the IUD moves out of the uterus).
- Perforation (rarely, the IUD can puncture the wall of the uterus during insertion).
- Infection (the risk of infection is slightly increased during the first few weeks after insertion).
Nursing Responsibility
- Pre-insertion Counseling
- Explain to the patient the type of IUD device, its benefits and its side effects.
- The patient should be completely informed about the procedure, its effectiveness and its duration. Make sure he/she understands.
Insertion Procedure
- Assist health care providers during insertion.
- Ask the patient to rest properly and provide reassurance.
- If there are any complications, Treat immediately.
Post insertion care
- Provide patient with proper education about the side effects of the intrauterine device.
- Provide patient with education about signs of complications such as pain, fever, infection, heavy discharge, and bleeding etc.
- Advising the patient for proper follow-up.
- Thus, intrauterine devices (IUDs) are a popular method of long-term contraception.
Hormonal method (hormonal method) :
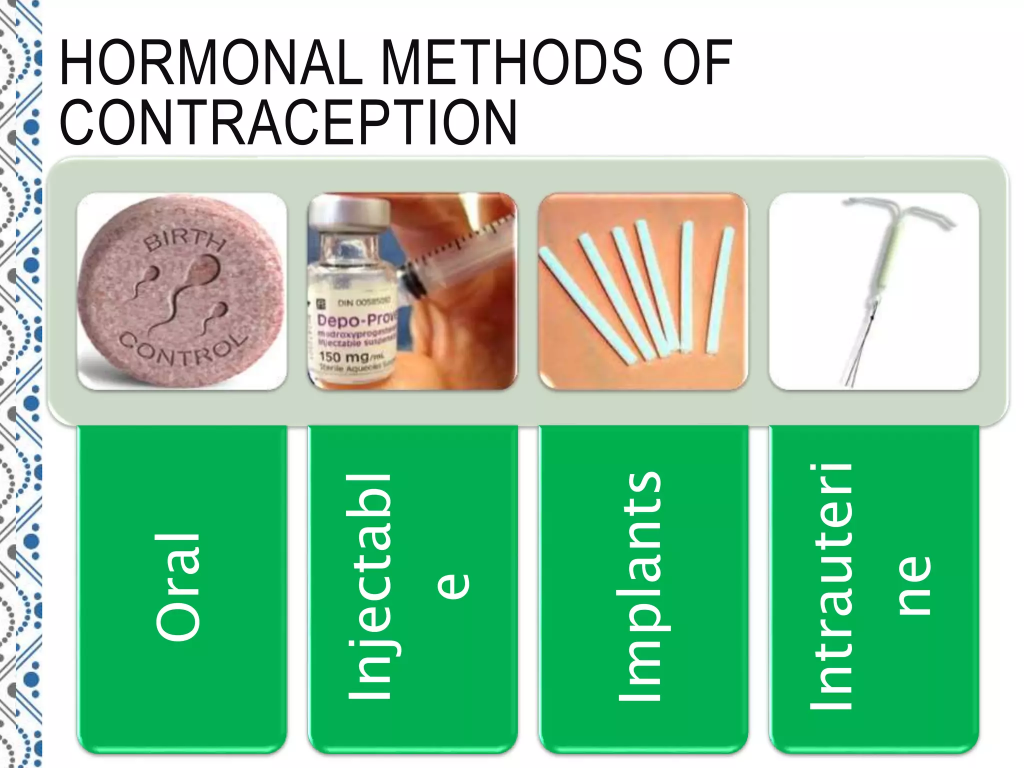
Steroidal Contraceptives:
A) Oral: They are commonly known as pills.
B) Injectable: They are mainly provided through injection.
C) Newer Sustained Release System
A) Oral Pills:
Combine Pills:
Mala N (norethisterone acetate + ethinyl estradiol).
Mala D (D norgestrel + ethinyl estradiol).

Mini Pills: These contain only progestin, i.e. norethisterone + levonorgestrel.
Combined Pills:

It contains 28 tablets in a packet to complete the menstrual cycle. There are 21 tablets in the combination of estrogen and progesterone, while 7 tablets are of iron and vitamins. Usually estrogen contains ethinyl estradiol, 30 mg and progesterone norethisterone 1 mg, DL norgestrel, levonorgestrel, ethinyl diol diacetate, linestrenol etc. It can be started in the first 5 days of the menstrual cycle and is taken every day at night for 21 days. The second pack is started after 7 days of the menstrual cycle.
MALA-N is free of charge by the government in the Family Planning Program. It contains 30 mg of estrogen and 1.0 mg of thorethisterone.
POP (Progesterone-Only Pills): It is called micropill or minipill. It is taken during the throw-out menstrual cycle. It contains only progestogen. It has not become very popular due to its high failure rate. It is usually used more in older women for whom the combined pill is contraindicated.
Postcoital contraception: Postcoital contraception is usually taken within 72 hours of unprotected intercourse, in which two methods are usually used, namely,
1) IUD,
2) Hormonal
1) IUD: This is the simplest technique, which is a copper device that can usually be used within 5 days.
2) Hormonal: Hormonal methods are preferable. Levonorgestrel 0.75 tablets are advised as emergency contraception.
One tablet of levonorgestrel 0.75 mg is given within 72 hours and the second tablet is given 12 hours after the first dose.
Or two oral contraceptive pills containing 50 mcg ethinylestradiol
are given within 72 hours after coitus and the same dose is repeated after 2 hours.
Or four oral contraceptive pills containing 30-35 mcg ethinyl- estradiol
are given within 72 hours and four tablets are given 12 hours after.
Long acting pills (once a month): These are long acting estrogens Ex: quinestrol which is provided in combination with short acting progestogen but is not recommended due to high pregnancy rates.
Nonsteroidal weekly oral pills:

This medicine is famous as the brand name of Saheli. It has less side effects like nausea, vomiting, weight gain, dysentery, etc. The name of this tablet is “Santchroman” and it is to be taken once a week.
When to start?
- Start on the 1st day of the Menstruation Cycle
(Can be started on any day of the Menstruation Cycle, but it is safer to use condoms for the first 1 month)
How to take? (How to take)
✅ First 3 months
- 2 pills a week
- Example:
👉 Sunday and Wednesday (keep a fixed day)
✅ After 3 months
- 1 pill per week
- The same fixed day (such as every Sunday)
Mode of action of combination pills:If we look at the mechanism of action of combination pills, this medicine prevents the release of an ovum from the ovary, which normally blocks the secretions necessary for the release of an ovum, such as gonadotropins. Progesterone makes cervical mucus thick and scanty, which can prevent sperm from penetrating. Progesterone also inhibits tubal maturation and delays the transport of ovum and sperm into the uterine cavity.
Advantages:
- It is easy to use.
- It is inexpensive and readily available.
- It has a high safety rate.
- Menstrual cycle remains regular.
- Chances of breast cancer are reduced.
Disadvantages:
- Not used in patients with cardiovascular disease.
- Weight gain occurs.
- High blood pressure occurs.
- Not suitable after the age of 40 years.
- Its side effects include breast tenderness, pain, headache, and irregular bleeding.
- Other problems such as liver disease, reduced lactation, and sometimes ectopic pregnancy can also occur.
B) Injectable contraception:

Injectable contraception includes two types:
1) Long acting progestin:
1) Depot- Medroxyprogesterone Acetate (DMPA) – 150 mg every 3 months.
2) Norethisterone Enanthate ( NET – EN) – 200 mg every 2 months.
2) Combined Injectable:
DMPA 25 mg + Estradiol Cypionate 5mg (Cyclofem)- Monthly.
NET – EN 50 mg + Estradiol Valerate 5mg (Mesigyana)- Monthly.
1) Long Acting Progestin:
1) Depot- Medroxyprogesterone Acetate (DMPA) – 150 mg intramuscular injection is provided every 3 months.

- It usually provides protection in pregnancy for up to three months.
- 1) It suppresses ovulation.
- 2) It has an indirect effect on the endometrium.
- 3) It decreases the motility of the fallopian tubes. is.
- Due to all these mechanisms of action, pregnancy can be prevented.
Time: Within 7 days of menstrual cycle, immediately after abortion, and MTP, within 7 days of postpartum, 6 weeks postpartum in breast feeding patients.
2) Norethisterone Enanthate ( NET – EN): – 200 mg every 2 months.
This injectable usually provides protection from pregnancy for up to two months.
Advantages:
- Highly effective,
- Provides long-term protection from pregnancy.
- Does not interfere with sexual activity.
- Can be used at any age.
- Endometrial cancer and uterine fibroids are reduced.
Side-effects:
- Irregular menstrual bleeding.
- Amenorrhea.
- Weight gain.
- Breast Tenderness.
- Nausea.
- Hair loss.
Contraindications:
- Hypertension.
- Cardiovascular disease.
- Breast cancer.
2) Combined injectables:
DMPA 25 mg + Estradiol Cypionate 5mg (Cyclofem)- Monthly.
NET – EN 50 mg + Estradiol Valerate 5mg (Mesigyana)- Monthly.
Combined injectables usually contain estrogen and progesterone, which are usually taken every month, which can be plus or minus 3 days.
Sustained release System:
Norplant (Norplant):

The Norplant 2 rod system, which consists of two silicone rods containing a total of 140 mg of levonorgestrel, is implanted in a woman’s arm using a minor surgical technique. Its failure rate is 0.5 per hundred women. It usually works for 5 years and is then removed using a minor surgical technique.
Biodegradable implant: It delivers progesterone and dissolves slowly, so it does not need to be removed.
Silastic vaginal ring: Progesterone is slowly released from the ring and is gradually absorbed into the vagina. The woman can insert and remove it herself. It remains effective for 12 months.
Contraceptive Patch: The combined estrogen + progesterone patch is to be applied to the abdomen, buttocks, thighs, and upper outer thighs, and upper back. A new patch has to be applied on that day.
Post Conception Contraception
Emergency Contraception: Emergency contraception is a method of contraception used as an emergency procedure to prevent pregnancy after unprotected intercourse. This method is effective, safe and simple.
Yuzpe Method: In this, combined oral contraceptive pills are used, two pills as early as possible and two pills 12 hours after the first dose. is given.
Progesterone Only Pills: Levonorgestrel 0.75 mg 2 doses are provided two hours apart, with a single dose being as effective as 1.5 mg.
IUCD: IUCD should be inserted within 5 days of intercourse.
Antiprogesterone: Mifepristone (RU-486) 600 mg single dose is provided within 72 hours of unprotected intercourse.
Miscellaneous:
Natural Family Planning Method:
Total Abstinence:
It involves complete abstinence from the act of coitus.
Coitus Interruption: In this, the penis is withdrawn from the vagina before ejaculation during sexual activity.
Latent Amenorrhea Method (LAM): In this, the chances of conception are less in women who breastfeed for 6 months after the birth of a child.
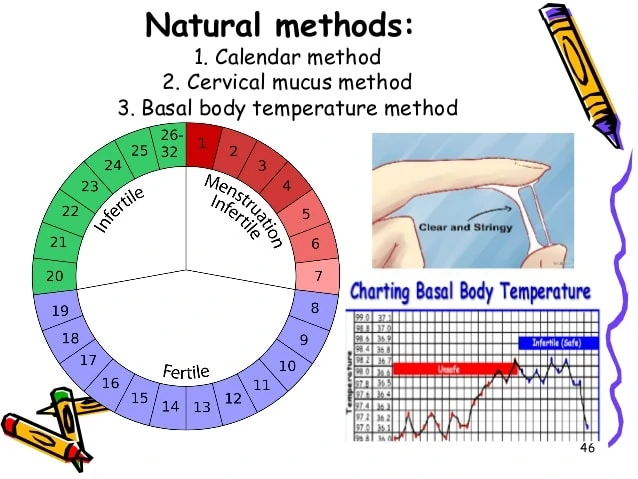
Method Based on Fertility Awareness
Calendar or Rhythm Method:
Record the days of the previous six menstrual cycles and subtract 18 days from the last cycle (28 – 18 = 10) to find the day of her first fertile period. Then subtract 11 days from the longest cycle and that is the last day of the fertile period (31-11= 21). Avoid sexual intercourse during this period.
Basal Body Temperature Method (BBT):Monitor your temperature every morning before waking up from bed. Due to the effect of progesterone, your temperature increases by 0.3°C – 0.4°C. After the temperature increase, avoid coitus until the fertile period ends three days later.
Cervical Mucus Method (Billing Method): Mucus during ovulation is watery, clear, smooth and slippery. Thus, coitus activity should be done during ovulation and for three days after ovulation.
Symptothermic Method: In this method, conception is prevented by combining basal body temperature (BBT) + cervical mucus method + calendar method.
Sterilization/Permanent Contraception:
Permanent surgical contraception, also known as voluntary sterilization, is a surgical method in which the reproductive organs of an individual male or female are The function is purposefully and permanently destroyed.
Such as,
1)Male sterilization: Vasectomy,
2)Female sterilization: Tubectomy
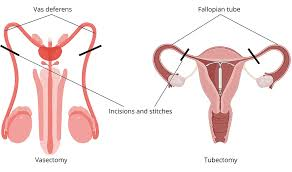
1)Male Sterilization: Vasectomy:
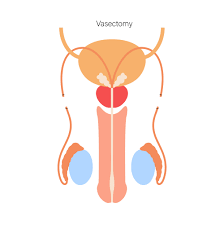
- This is a permanent stylization operation performed in the mail in which both sides of the vas deferens are resected and its ends are cut and ligated.
Advantages:
- Its operation technique is simple and complications are less.
- Its operation can be done as an outdoor procedure in camps and villages as well.
- The failure rate is 0.15% and the success chance of reversal anastomosis operation is 50%.
- Equipment, Hospital Stay, doctor training all costs are low.
Deadvantages:
- Additional contraception is required for 2-3 months after the operation until the semen is free of sperm.
- Frigidity or impotence may occur, which is mostly psychological.
Non Scalpel Vasectomy( NSV ):
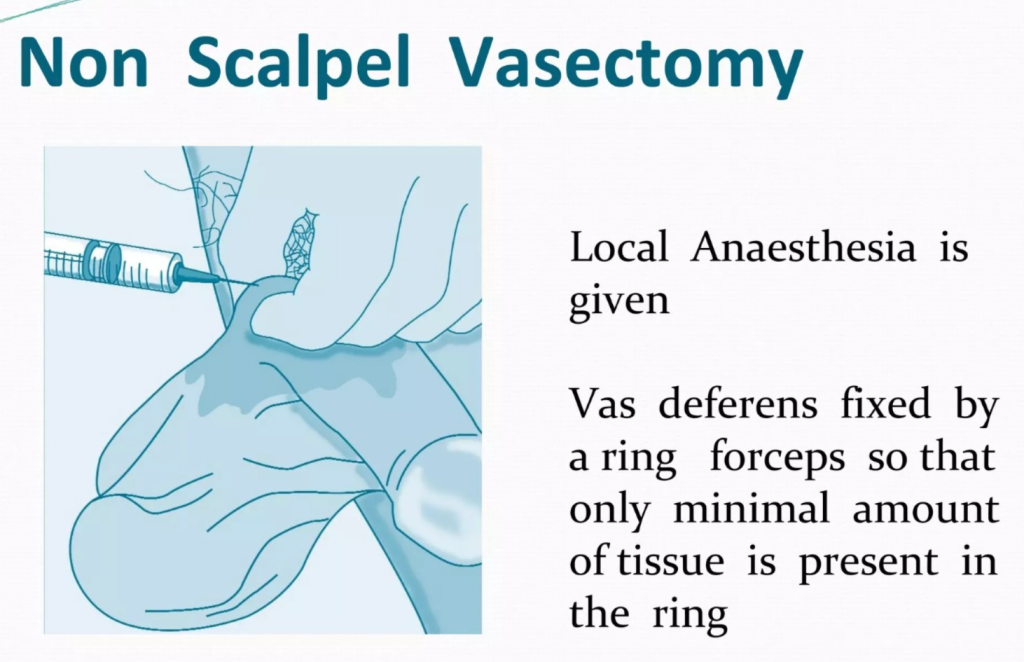
- This operation is provided under local anesthesia in which the vas is caught with specially designed forceps, after which the stretched skin over the vas is punctured with the sharp point of the forceps without using a scalpel and then the vas is dissected. There is no need for sutures and the time is also less. There is a fast recovery but the surgeon’s skill is required to a greater extent.
2) Female Sterilization/ Tubectomy:
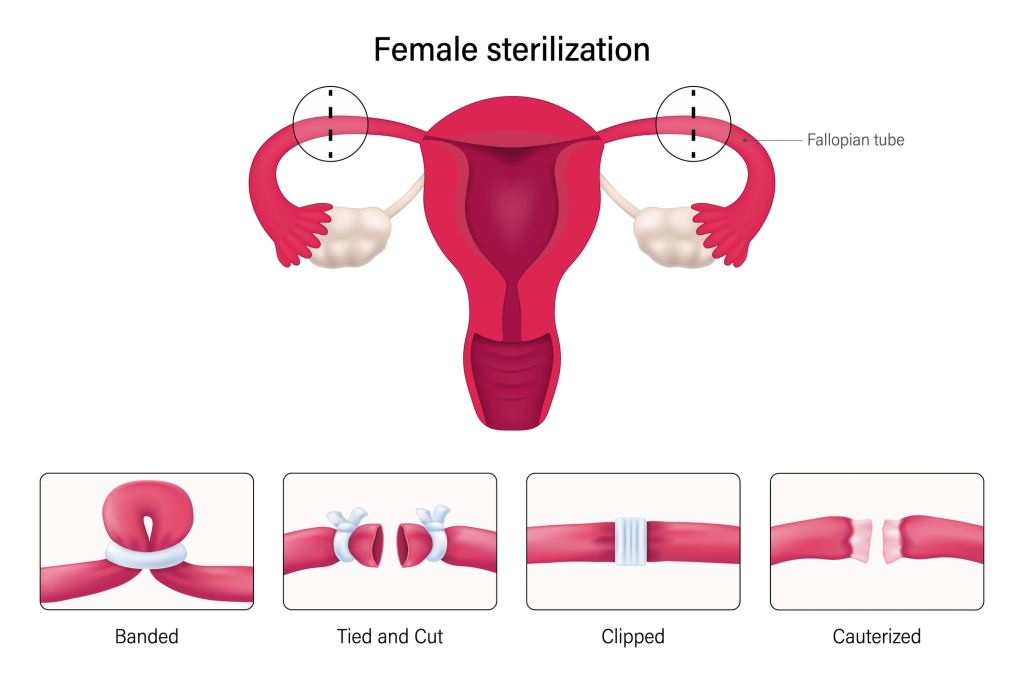
- Tubectomy is a method of permanent sterilization performed in females. In this, the fallopian tubes are cut and then ligated to block the passage of the ovum.
Time of operation:
- Postpartum sterilization: If the patient is healthy, tubectomy can be done 24-48 hours after delivery.
- Internal sterilization: When the operation is When performed at a time other than childbirth and abortion, it is called internal sterilization.
Traditional tubectomy:
- This method is also known as abdominal tubectomy. This method is usually performed under general anesthesia or spinal anesthesia in which an incision is made in the lower abdominal area and then the fallopian tube is cut and tied or clamped. The layers of the abdomen are then closed, which usually works as a permanent contraceptive that blocks the path of the fallopian tube, which usually requires five to six days of hospitalization and the sutures can be removed after the 5th day after the operation.
Post-operative advice:
- Heavy weights should not be lifted for 6 weeks.
- Avoid heavy work for three months.
- Sexual activity can be resumed 4 weeks after the operation.
Minilap operation:
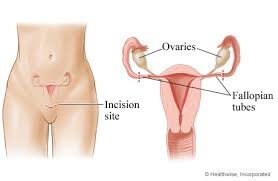
- This is a minor form of abdominal tubectomy which is usually done under local anesthesia in which a 2.5 to 3 cm incision is made in the lower abdominal area and then parts of the fallopian tube are cut and clamped and then the layers of the abdomen are sutured again. The method is a very safe and effective method. This procedure can be performed generally at the Primary Health Center (PHC) level and also in the community. This procedure acts as a good technique for postpartum sterilization.
Advantages:
- This technique is generally suitable for postpartum sterilization.
- This procedure is generally less traumatic than an abdominal tubectomy.
- It generally has fewer complications.
Laproscopic Sterilization:
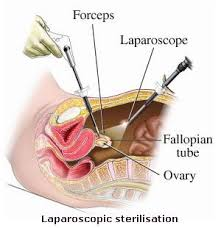
- This laparoscopic sterilization technique is a very popular procedure of female sterilization in which the fallopian tubes are blocked or a rubber ring is placed in the fallopian tubes due to which the ovum cannot reach the uterus. Before inserting the laparoscope, the abdomen is expanded with carbon dioxide, nitrous oxide or air. Then the laparoscope is inserted through the abdomen and the tubes are visualized. After that, when the tubes are visualized, the fallopian tubes are opened. A tube is placed or a clip is applied which blocks the tube, then the laparoscope is removed and the layers of the abdomen are sutured and closed.
Advantages:
- The incision is very small and the scar is also small.
- It requires less time for the operation.
- This is a less expensive procedure.
- It has minimal complications.
- The hospital stay is short, usually up to 48 hours.
Disadvantages:
- It is not usually performed in postpartum patients.
- It is not suitable for patients who have medical diseases such as heart disease, respiratory disease, diabetes and hypertension.
Complications:
- Pain,
- Stretching,
- Irregular menstrual cycle,
- Local infection.
