ENGLISH-NEW MIDWIFERY GNM TY UNIT 6 MANAGEMENT OF NEWBORN
MANAGEMENT OF NEWBORN :
Immidiate Care Of Newborn :
- Immediate newborn care involves properly assessing and stabilizing the newborn.
- Immediate newborn care is the process of transitioning the fetus from intrauterine life to extrauterine life. It is crucial for stabilization.
Goal of Immediate Newborn Care:

- 1) To establish, maintain and provide support to the newborn’s respiration.
- 2) To prevent the newborn from fever and hypothermia.
- 3) To prevent infection in the newborn.
- 4) To provide safety to the newborn and prevent him from injury.
- 5) To provide immediate treatment for any actual or potential problems in the newborn by early identification.
- Immediate newborn care is provided.
Immediate Newborn Care(Immediate Newborn Care):
1) Establishment of Respiration
- When the newborn is received, immediately patent the newborn’s airway and clear the airway properly. Due to which the newborn can breathe effectively.
- As soon as the newborn’s head is bent, wipe the mouth and nose and suck the mouth and nose so that the newborn can breathe properly. Suck the mouth first and then the nose so that secretions can be prevented from being aspirated.
2) Initiation of Cry
- Normally 99% of newborns cry immediately and spontaneously after delivery, this cry is known as a good sign for the newborn’s breathing.
- If the newborn does not cry properly, follow the following steps:
- a) If the baby does not cry spontaneously or if the cry is weak, then lightly simulate the baby to cry.
- b) To stimulate your baby’s cry, lightly rub the soles of their feet instead of slapping their bottom. After removing the secretions of the newborn, stimulate the baby to start crying.
- C) The cry of the newborn is usually loud and husky and if there is any abnormal cry as follows, then the newborn should be properly monitored such as,
- High pitch cry:= Due to hypoglycemia and increased intracranial pressure,
- Weak cry:= Prematurity,
- Hosacri:= Laryngeal Strider
3)Care of Cord
- Cord care is an important immediate care of the newborn.
- The newborn’s cord should be clamped within 30 seconds of birth and then cut properly. To do.
- After the newborn is delivered, place the newborn on the mother’s abdomen.
- Then clamp the cord properly from two opposite sites using a cord clamp.
- Apply the first clamp 5 cm away from the umbilicus, then apply the second clamp 2.5 centimeters from the first clamp.
- Then cut the cord properly between the two clamps.
- Do not apply anything to the cord, let it dry and fall naturally.
- The cord naturally falls down within seven to ten days after birth.
- Prevent the cord from getting wet with water and urine.
- If any discharge or bleeding is present in the cord, immediately access the cord clamp and loosen it properly.
- If the cord shows any of the following signs: And if symptoms are seen, report them immediately, such as,
- Foul odor coming from the cord,
- No discharge is seen,
- Redness is seen around the cord,
- The cord is wet,
- The cord does not fall down in 7-10 days,
- Inflammation,
- Fever etc.
4)Maintain position of the newborn
- The newborn is usually prone to choking, coughing and gagging during the first 12-18 hours after birth. Therefore, the newborn should be provided with a proper position.
- In which the fitters should be provided with a proper side lining position so that mucus can be removed and drained.
5) Identification and Banding
- After the baby is born, a proper identification band should be applied to the baby Due to which the baby can be properly identified.
6) Eyecare
- Clean the newborn’s eye from the inner canthus to the outer canthus with sterile gauze.
- If necessary, apply erythromycin or tetracycline ointment to the eye from the lower lead.
7) Attachment and warmth (bonding)
- After the birth of the baby, place the baby on the mother’s abdomen to bond with the mother and allow proper skin-to-skin contact, which helps the mother and baby attach and prevents the baby from hypothermia.
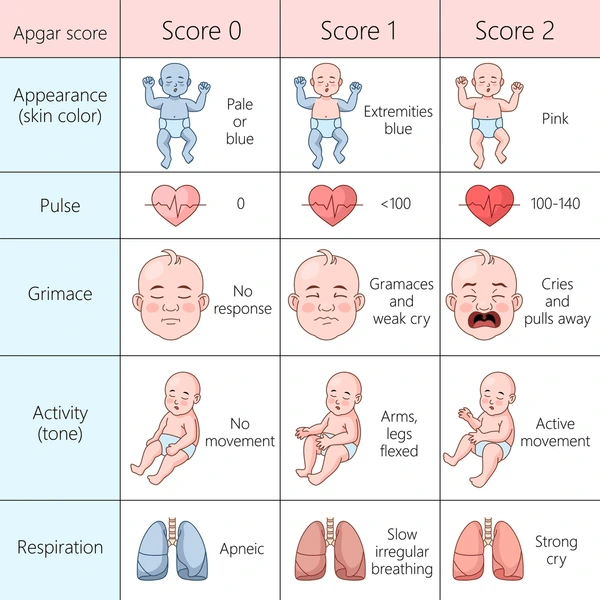
8) APGAR score
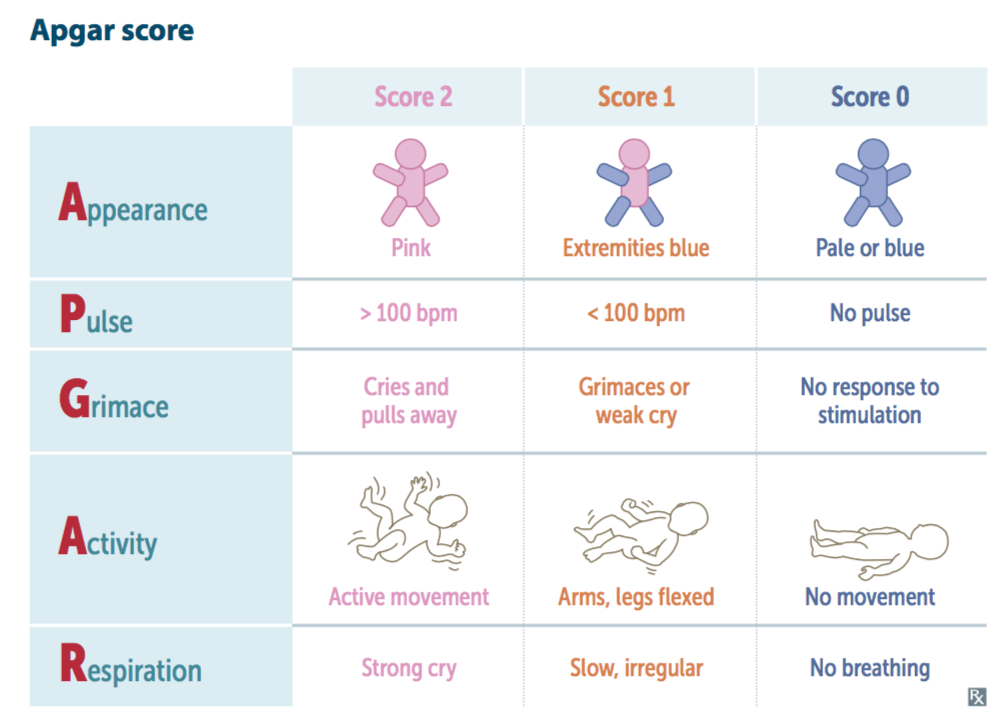
- APGAR score is the most important in immediate newborn care The APGAR score is assessed at 1 minute and then at 5 minutes after birth. In the APGAR score, A: Appearance (skin color), P: Pulse (heart rate), and G: Grimace (reflex) Irritability),
- A:=Activity (muscle tone),
- R:= Respiration (respiratory efforts) is assessed.
The total score of the APGAR score is 0-10.
The APGAR score is a score given 1 week after birth. Per minute:
-
- If the Apgar score is between 7-10, it is considered normal, meaning no depression, in which the baby is provided with normal post-delivery routine care.
-
- If the APGAR score is between 4-6, it indicates mild depression, in which the child requires assistance for breathing.
-
- If the APGAR score is between 0-3, it indicates severe depression, in which the child requires resuscitation. Remains.
APGAR score at 5 minutes after birth:
-
- If the APGAR score is between 7-10, it is considered normal, but if the Apgar score is below 7, the baby needs to be monitored for another half hour.
9) Vitamin K:
-
- The intestines of a newborn are sterile for a short time after birth, meaning their intestines There are no bacteria present in the body that are responsible for manufacturing vitamin K, due to which the newborn cannot manufacture vitamin K, i.e. vitamin K is responsible for a clotting factor. If this vitamin K is not present in the body of the newborn, then there is a possibility of bleeding in the newborn, so as a prophylactic measure, artificial injection of vitamin K is provided to the newborn baby.
Dose:=
In pre-term:=0.5 mg,
Full term:= 1 mg.
Intra muscularly ( IM ) is provided on the vastus lateralis (lateral anterior).
APGAR Score:
- Apgar scoring A Developed in 1952 by obstetric anesthesiologist Virginia Apgar, it has become the standard method for evaluating newborns.
- The Apgar is an instant, quick, and complete assessment of the health of a newborn or a neonate.
- The APGAR score is the most important part of immediate newborn care.
- The APGAR score is,
- 1) Immediately after birth,
- 2) 1 minute after birth
- 3) Assess at 5 minutes after birth.
- The Apgar scoring performed at one minute provides information about the baby’s physical health and helps the physician assess and determine whether immediate or future medical treatment will be needed.
- While, 5 The 1-minute Apgar score, if performed, provides information about the infant’s response to pre-resuscitation measures. is.
In APGAR score,
A:= Appearance (skin color),
P:=Pulse (heart rate),
G:=Grimes (reflux irritability),
A:=Activity (muscles tone),
R:= Respiration (Respiratory Efforts) is assessed.
Five Criteria of the Apgar Score:
1) (A: Appearance) Skin Color:
- Score 0: Entire body blue or pale Should be.
- Score 01: Body pink and extremities blue.
- Score 02: Body and extremities pink, no cyanosis seen.
2) P: Pulse rate:
- Score 0 : Sabsant.
- Score 01 : Less than 100 pulses per minute.
- Score 02 : More than 100 pulses per minute.
3) G : Grimace (reflex irritability)
- Score 0 : No response to stimulation Not responding.
- Score 01 : Grimaces on suction or aggressive stimulation.
- Score 01 : Crying on stimulation.
4) A : Activity:
- Score 0 : None.
- Score 01 : Some flexion.
- Score 02 : Flexed arms and legs that resist extension.
5) R : Respiratory effects
- Score 0 : Absent,
- Score 01 : Weak irregular and gasping,
- Score 02 : Strong and lusty.
- The total score of the APGAR score is 0-10.
APGAR score is the score at 1 minute after birth On:
- If the Apgar score is between 7-10, it is considered normal i.e. no depression in which the baby is provided with normal post-delivery routine care.
- If the APGAR score is between 4-6, it indicates mild depression in which the child requires assistance for breathing.
- If the APGAR score is between 0-3, it indicates severe depression in which the child requires resuscitation. is.
APGAR score at 5 minutes after birth:
- If the APGAR score is between 7-10, it is called normal,
- But if the Apgar score is below 7, then the baby needs to be monitored for another half hour.
After Birth Observation of Newborn Baby:

- Immediate observation of the newborn after birth is crucial to assess their overall health, well-being and development.
- Here are some aspects of newborn observation:
1) General Appearance:
Color:
- Assess the child’s skin color, most children are pink or red in color. If there is cyanosis (bluish discoloration), it Indicates breathing difficulties.
Posture:
- Note the baby’s muscle tone. A healthy newborn baby has slightly flexed hands and slightly arched feet along the spine.
Activity:
- Observe spontaneous movements, involving the sucking reflex and the grasping reflex.
2) Vital signs:
Heart rate:
- Normal range is 120-160/minute.
Respiratory Rate:
- A normal respiratory rate is 30-60 breaths.
Temperature:
- Normal temperature is 36.5-37.5°C (97.7-99.5°F).
3) Head and Face:
Fontenelles:
- The anterior fontanelle (soft spot) and posterior fontanelle of a newborn are Palpate. To assess proper closure and tension of the fontanelles.
Ice:
- Check the ice for its cementation. Assess for red reflex (indicative of normal eye structure) and response to light.
Nose:
- Assess the patency of the nose to ensure that breathing is appropriate.
4) Mouth and Neck:
Oral Mucosa:
- Assess the oral mucosa for cleft palate, oral thrush and any lesions.
Neck:
- Assess whether there is any mass-like structure or abnormality in the neck.
5) Chest and Lungs:
Breathing Sound:
- Listen to the child’s breathing sound properly.
Chest Movement:
- Properly assess whether the child’s chest rises and falls symmetrically with breathing.
6) Heart and Abdomen:
Heart Sound:
- Proper auscultation of the heart sound to assess for any murmur-type abnormal sounds and abnormalities.
Abdomen:
- Palpate the abdomen and auscultate the bowel sounds to assess whether the child has any mass-like structures in the abdomen.
7) Genital area and anus:
Genital Area:
- Assess whether the anatomical structure of the genital area of the child, i.e. male (presence of testes in male child) and female (labial structure in female child), is proper or not.
Ans:
- Assess the patency of the anus and any abnormalities Assess whether it is or not.
Urine and stool:
- Urine is passed within 24 hours of birth and the first stool, called meconium, is greenish black in color, which occurs in the first 48 hours, three to four times a day for three to four days, and then transitional stools, which are greenish brown, are seen for three to four days.
8) Extremities:
Hands and Feet:
- Count the child’s fingers and toes. And assess symmetry or assess whether there are any abnormalities.
Movement:
- Assess whether the child has spontaneous movement and the range of motion of the hands and legs.
9) Skin and Umbilical Cord:
Skin:
- Assess the child to see if there are any birthmarks, lesions and ridges on their skin.
Umbelics:
- Provide proper cord care to the child and assess for any signs and symptoms of infection and bleeding.
10) Behavioral Assessment:
State of Alertness:
- The baby’s level of consciousness is Properly assess and properly assess the amount of response to stimuli.
Crying:
- Properly assess whether the child is crying properly or not so that the child’s respiratory status can be properly assessed.
Additional Considerations:
Documentation:
- Accurately record all findings on the newborn assessment chart.
Parenteral Education:
- Provide education to parents about newborn care including proper breast feeding technique, maintaining hygiene, and to immediately go to a health care center if any signs and symptoms of infection are seen in the child.
- Proper observation of the child after birth can help in early identification of any congenital abnormality or potential risk factor for any disease and adequate measures can be taken and The child’s condition can be prevented from becoming complicated.
Physiological Adaptation of Neonate/Newborn :

Newborn
- A healthy newborn is one who is born at term, i.e. between 38 and 42 weeks, cries immediately after birth, starts breathing individually, rhythmically, and accepts extrauterine life, and whose weight is a normal weight The neonate which is the same and does not have any congenital anomaly is called normal neonate.
Physiological Adoption of Newborn :

- Physiological adaptation in newborns is important for the fetus to survive from intrauterine life to extrauterine life.
- Physiological adaptations in newborns:
1) Respiratory system :
- Fetus to Neonate Transition:
- Before birth, the fetus receives oxygen from the placenta.
- After birth, the fetus’s lungs expand and mature to oxygenate the blood.
Clearance of Lung Fluid:
- After the birth of a newborn, when the newborn takes its first breath, the fluid in the lungs is cleared and the lungs pass from the fetal circulation to the neonatal circulation Transferred to.
Surfactant Production:
- Surfactant is a substance that works to reduce the surface tension of the lungs. and prevents the alveoli from collapsing so that gas exchange can take place properly.
Closure of Fetal Sinus:
- After birth, the sinuses present in the newborn such as the ductus arteriosus (a shunt between the descending aorta and the pulmonary artery) and the foramen ovale (a shunt in the septum between the right atrium and the left atrium) close, redirecting blood to the lungs. is.
2) Cardiovascular system:
Circulatory changes:
- After birth, the umbilical cord is clamped and cut After this, the umbilical vessels constrict and the umbilical arteries and umbilical veins close.
Increases Pulmonary Blood Flow:
- After birth, the newborn lungs expand, which is able to oxygenate the blood, which increases pulmonary circulation.
Closure of Ductus Arteriosus:
- These blood vessels connect the pulmonary artery and the aorta, which close shortly after birth.
Closure of foramen ovale:
- The foramen ovale is a hole in the septum between the right atrium and the left atrium, which closes a few months after birth.
3)Thermoregulation:
Maintenance of body temperature:
- Newborns have a limited ability to regulate their body temperature and are dependent on brown fat metabolism, vasomotor response (shivering), and They are kept in a warm environment (incubator or skin to skin contact).
4) Gastrointestinal system:
Production of digestive enzymes:
- Fetuses after birth Digestive enzymes increase, which allows the newborn to digest breast milk and formula milk.
Meconium Passage:
- For a few days after birth, the baby passes meconium (the baby’s first stool), which indicates a normal digestive tract.
5) Metabolism:
Glucose Metabolism:
- After the birth of the baby, insulin secretion increases, which can decrease maternal blood glucose and maintain the fetus’s blood glucose level properly.
Adjustments in Feeding:
- The gastrointestinal tract and metabolism of the fetus are adjusted to transition from placental nutrients to feeding.
6) Renal system:
Urine Production:
- After the birth of the baby, the kidneys filter the fetus’ blood and produce urine Works for.
Fluid Balance:
- The urinary system of the fetus adjusts to maintain the fluid and electrolyte levels of the fetus.
7) Immune system:
Passive immunity:
- Newborns receive antibodies through the placenta and breastmilk, increasing their immunity and working to fight infections.
8) Neurological adaptation:
Sensorimotor integration:
- The newborn adjusts to maintain coordination of sensory and motor responses to sensory stimuli after birth.
Cephalocodal Development:
- The newborn develops head to toe after birth, such as lifting the head, grasping objects, etc.
- This adaptation is a hormonal, neural, and metabolic process through which the newborn transitions from intrauterine life to extrauterine life can survive properly and this physiological adaptation is important for the proper growth and development of the newborn.
First Day Examination of Newborn Baby:
After the birth of the newborn, all its parameters should be properly checked such as:
1) Vital signs
- Temperature is often taken by the auxiliary method as a vital sign. And count the heart rate and respiratory rate for a full minute.
2) Physical Measurement:
a) Weight:
- Check the weight on the infant weighing machine. If the baby’s weight is less than 2.5 kg, take it Birth weight is considered as baby. While weighing baby, place a thin cloth or paper on the weighing scale properly.
b) Length:
- Assess crown-to-hill length with tape measure.
C) Head Circumference:
- Take the measuring tape from above the eyebrows and pinna of the ear back to the occipital protuberance and record it in centimeters (Cm).
D) Chest Circumference:
- Chest circumference is measured around the chest, at the level of the nipple. Make sure the tape is placed around the widest part of the chest, under the armpit and on the upper back, and the measuring tape should not be too tight.
- Usually the chest circumference is 2-3 cm less than the head circumference.
3) Color:
- The skin color should usually be normal pink. Should be.
- If the heart rate is high with pallor, then it indicates the condition of anemia.
- If there is a gray color with pallor, then it indicates the condition of acidosis. And if the baby is pale, it indicates a condition of hyperthermia or sepsis.
- Acrocyanosis, in which the hands and feet are blue, usually occurs when the baby is exposed to a cold environment.
- If the condition of general cyanosis is seen in a newborn, it is usually seen in the condition of the cardiac or lungs and in it, the color of the lips and tongue is usually brown.
- If the body of the newborn is excessively red, it is usually polycythemia, i.e. red blood cells. It is seen when it is high.
Harlequin color :
- Harlequin color is a temporary color change in newborn babies, in which one half of the body appears red / pink and the other half remains pale.
- Ecchymosis: in which the color does not return when pressure is applied to the skin and indicates a condition of bleeding within the skin
- If yellow discoloration is seen in the baby’s skin, it usually indicates the condition of jaundice.
4) Cry:
- The newborn’s cry immediately after birth can indicate whether his lung function has been established or not. A loud and vigorous cry is normal, low birth weight Weak and fabled cries are seen in babies, while high pitched or shrill cries are seen in meningeal irritation, and horse cries are seen in vocal cord paralysis, hypothyroidism, and trauma.
5) Activity:
- Check for spontaneous and uniform movements. In which the child lifts and stretches the legs, opens and closes the fist, moves the hand, and shakes the fingers, it shows a good activity level. Whereas, in central nervous system (CNS) damage, the child is flaccid (loose) and convulsions occur, while in birth trauma, there is asymmetrical movement. Thus, activity or crying is less common in abnormalities.
6) Skin:
- Normal skin is smooth, like a rose petal and has good skin turgor, meaning that the skin returns to its original state when grasped with the fingers and released. In this variation, tiny white papules are seen on the cheeks, chin, and nose, which are called milia.
Lanugo:

- The thin hair on a baby’s body is called lanugo. Look for the distribution of vernix caseosa (white cheesy substance on the baby’s skin) all over the baby’s body and in the skin folds.
7) Head to Toe Examination:

Head :
- To check the fontanelles in the head, the anterior fontanelle of a newborn is diamond-shaped, which is normal It usually closes at 16-18 months, while the posterior fontanel is triangular in shape and usually closes within 6 weeks. The fontanelles are usually smooth and palpable at the space between the two sutures.
- Check the head for size, septum, fontanelles, caput, and any abnormalities such as hydrocephalus, meningitis, meningomyelocele encephaly, and molding.
Ice:
- Normal Typically, the eye color is slate gray or brown, does not produce tears, and has a blinking reflex, can only see from the front when an object is held in front of the eye, and has clear eyebrows, a bright and shiny cornea, uniform, and responsive to light.
- Pupillary reaction to light, epicanthal fold, and inner canthus of the eye should be properly checked.
- Squint, nystagmus, trauma, lacrimal duct obstruction, corneal opacity, congenital cataract, conjunctivitis, blinking reflex, and doll’s eye Look for reflexes.
Ear:
- Usually the pinna is easily palpable and cartilage is present. The top of the ear is parallel to the outer corner of the eye and the startle reflex is present. Look for the shape and position of the ear and look for any additional lobes present. Low set ears indicate Down syndrome.
Neck:
- The neck is usually short and thick and can bend in both directions. The clavicle is complete and the tonic neck reflex is present. There is some control over the head.
- Look for mass and shortness in the neck. Check the cervical spine posteriorly. Check for lateral sternomastoid muscles, trapezius muscles, and thyroid gland.
- Palpate lymph nodes and check neck motion.
- Look for torticollis (neck muscles contracting on one side, causing the arm on that side to droop).
Nose:
- Assess if there is any blockage in the nose and see if the baby can breathe through the nose. Assess if there is any discharge from the nose. Flaring of the nostrils (nascorha fulva) indicates respiratory distress or depressed nasal bridge Down syndrome.
Mouth :
- Usually the uvula is in the midline of the mouth and the palate is small or absent and the cheek fat is well developed and the mucosa is moist. The palate is high and shaking, rooting and gag reflexes are present. And inspect the lips, tongue, palate and oropharynx. Properly identify the child for any cleft lip, cleft palate, small chin, and small head.
Chest:
- Examine the chest for symmetry, including properly assessing whether the nipple is symmetrical.
Heart :
- The lower part of the heart is between the fourth and fifth ribs of the left sternal border, the intensity of the S2 heart sound is greater than that of the S1 when the heart rate is 120- 160 beats/minute.
- Assess whether severe respiratory distress is present by observing for retraction of intercostal and subcostal muscles.
Breasts:
- Look at the breasts for size, consistency, color, turgor, and discharge. Auscultate for air entry into the lungs. To check the heart sound properly.
Abdomen:
- The abdomen is usually cylindrical in shape and is soft during palpation. The umbilical cord is well developed and palpable two to three centimeters below the right costal margin, while the kidney is palpated two to three centimeters above the umbilicus. Both femoral pulses are equal on that side, and bowel sounds are auscultated within two hours after birth.
- Check the abdomen counter. In pre-mature neonates, the abdomen is distended due to poor muscle tone.
- Drug or neurological depression can cause a flat, flabby abdomen.
- A concave abdomen suggests a diaphragmatic hernia.
- The intestinal organs protrude outside the omphalocele. Look for an inguinal hernia when the baby relaxes or cries. Look for the femoral artery pulsation to be the same on both sides. Look for lymph node enlargement in the groin.
Genital organs:
Female:
- Labia and clitoris are There is swelling in which the labia majora completely covers the labia minora and there is vernix between the labia. Urine is passed in adequate amounts within 24 hours after birth.
- Look to see if the labia majora completely covers the labia minora. And check for vaginal discharge and pseudomenstruation. Look for the size and shape of the clitoris.
Mail:
- The urethral opening is usually located at the tip of the glans penis. The testicles are palpable as a large, swollen, pendulous lump in the scrotum. Urine is passed in adequate amounts within 24 hours after birth.
- Check the scrotum for lumps. Palpate the scrotum to see if the testicles have descended. Examine the prepuce for retraction and the urethral opening in the penis. Flash a light on the scrotum to look for congenital hydrocele and inguinal hernia. Look for ambiguous genitalia.
Rectum:
- The rectum usually has an open passage. Meconium is passed within 24 to 48 hours after birth.
- Check for patency of the anus and whether meconium has passed. Fistula, and anal muscle tone to rule out legibility.
- Assess the patency of the anal opening by passing a catheter or with a gloved finger.
Extremities:
- Maintains a flexed position. Movement and tone are the same at both sites. All joints have an adequate amount of movement, and there are ten fingers on each hand and foot. The feet appear bow-shaped and the soles of the feet appear flat. The palms are lined. The anterior two-thirds of the soles of the feet are lined, and the Babinski reflex is present.
- Range of motion (ROM) for extra digits (polydactyly), syndactyly, and lines on the soles of the feet and the condition of dislocation of the foot.
- If there is a congenital hip dislocation, flexion of the leg reveals that the femur is short, making the affected side appear short.
Back :
- Normally the spinal cord is straight, in the midline and complete.
- Normal curvature and abnormalities of the back Such as checking for spina bifida and Mongolian sports in the sacral area, which are common variations. Make those observations.
Reflexes of the Normal Neonate :

1) Rooting reflex:
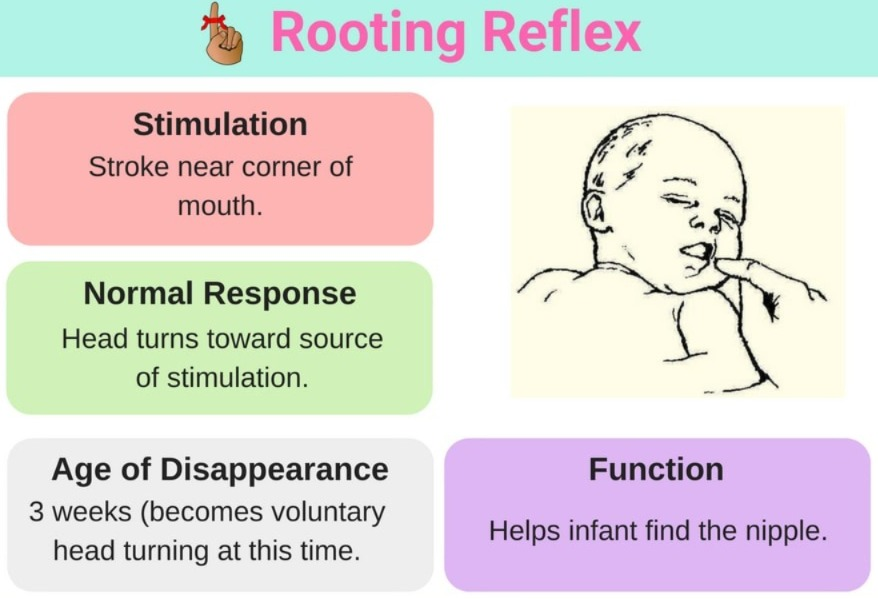
stimulation
- Touching or stroking the cheek near the corner of the mouth.
Response
- Head will turn towards the stimulation, mainly to find food.
Disappear
- When the baby is awake, 3 to 4 months and during sleep, 7 to 8 months.
2) Sucking reflex

stimulation
- Touching the lips of the newborn with the mother’s nipple or the examiner’s little finger.
Response
- Shaking moment for food.
Disappear
- Does not disappear.
3)Swallowing reflex
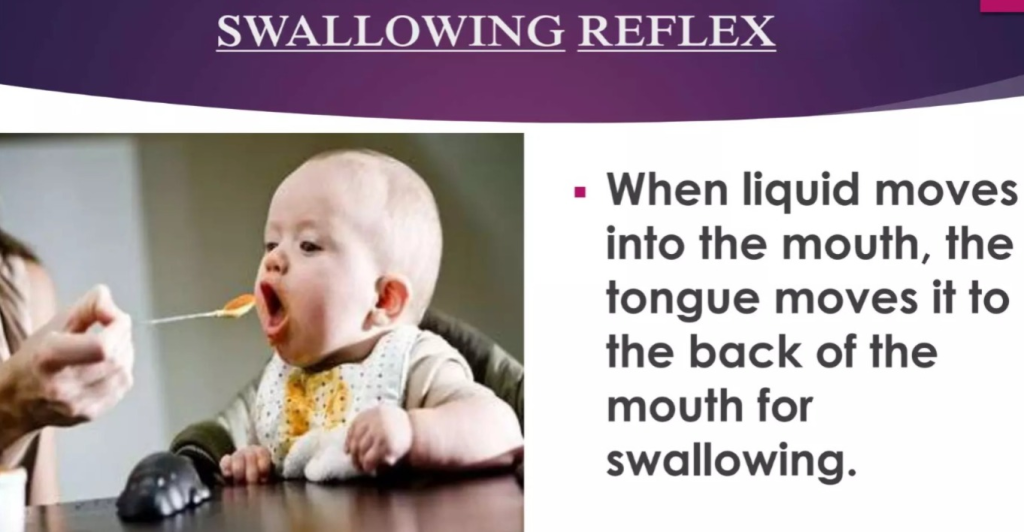
Stimulation
- Shock reflex is seen only with it.
Response
- Swallowing occurs when food reaches the posterior part of the mouth.
Disappear
- It does not disappear.
4) Gag reflex:
Stimulation
- The baby gags when the posterior fairings are stimulated by food or a suction tube.
Response
- The child immediately coughs and regurgitates food.
Disappears
- It does not disappear.
5) Sneezing and Coughing Reflex :
Stimulation
- Foreign substance enters the upper and lower airways.
Response
- Upper Air Passage Cleared by sneezing and lower air passages by cuffing.
Disappear
- Does not disappear.
6) Blinking reflex
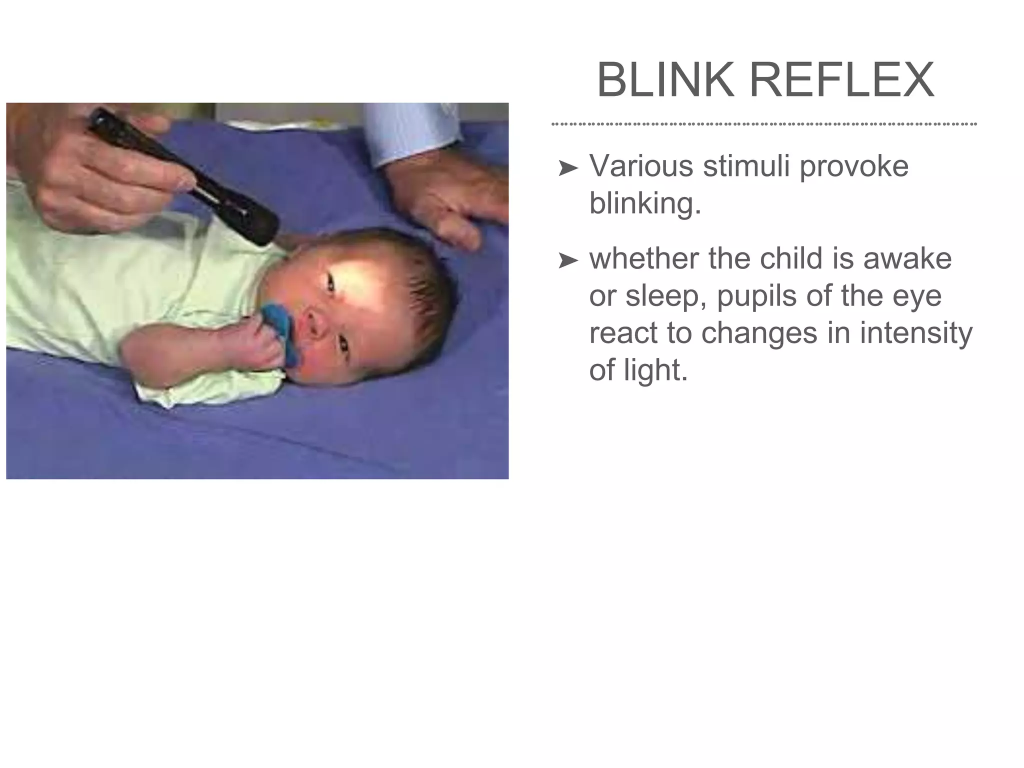
Stimulation
- Eye exposure to bright light.
Response
- Closes the eye lead and protects the eye.
Disappears
- Disappears No.
7) Doll’s Eye Reflex :
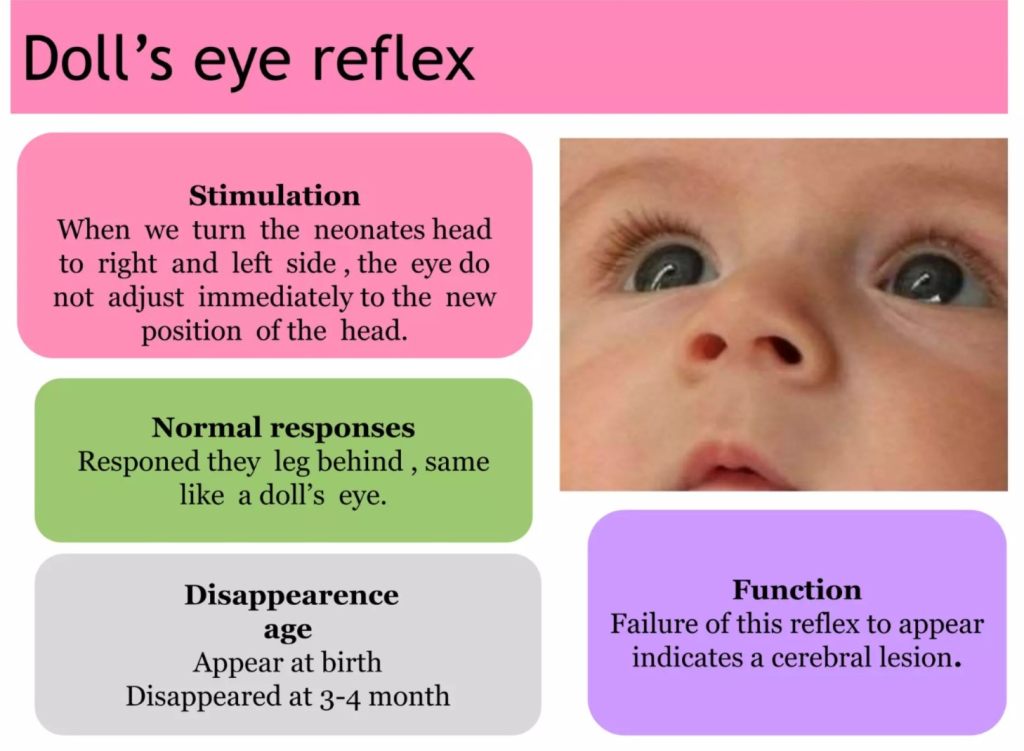
Stimulation
- Slowly turn the neonate’s head to the right or left side.
Response
- The ice moves in the opposite direction.
Disappear
- Disappears when the child has focus.
8) Palmer grasp (Palmer grasp):

Stimulation
- Place an object in the neonate’s palm.
Response
- Close the fingers and grasp the object.
Disappear
- Disappears in 6 weeks to 3 months.
- Disappears in 6 weeks to 3 months.
9)Stepping and dancing reflexes :

Stimulation
- Hold the neonate in a vertical position and place its feet on a flat and firm surface.
Response
- The legs flex and extend rapidly, like a step.
Disappear
- Disappears in three to four weeks.
10) Tonic neck reflex :
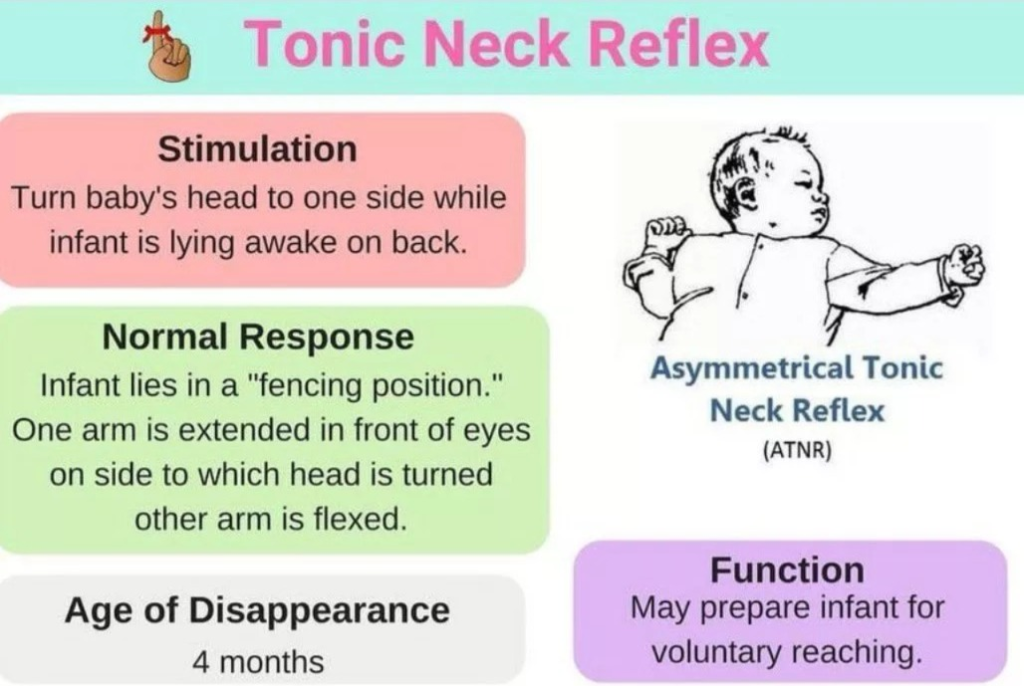
Stimulation
- Provide the neonate with a supine position and turn its head to one side.
Response
- The arms and legs on the side to which the head is turned straighten and the arms and legs on the opposite side bend.
Disappears
- Disappears in 3 to 4 months.
11) Babinski:
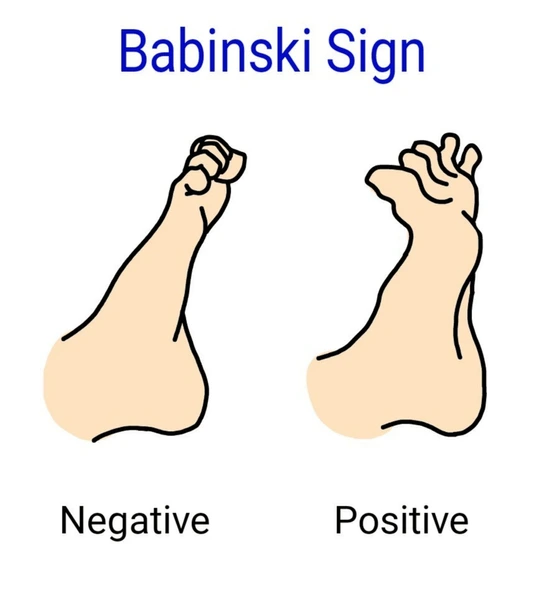
Stimulation
- Start stroking from the heel to the outer sole of the foot, moving up the lateral aspect to the fingers.
Response
- Dorsiflexion of thumb and other digits become fan-shaped.
Disappears
- It disappears after one year.
12)Moro reflex (Moro Reflex):

Stimulation
- Place the neonate on a firm surface on the examination table, make a loud noise with your hand or mouth, and hold the neonate in a supine position, supporting the upper back and head with one hand and provide support to the lower back with the other hand, then suddenly drop the head downwards about an inch.
Response
- With a sudden change in balance, the index finger and thumb form a “C” shape with extension and abduction of the arms and legs and fanning of the fingers, followed by flexion and adduction of the arms and legs, and the infant cries.
Disappear
- Disappears in 3 to 4 months and is strong in 2 months.
Infant Feeding (Infant Feeding) :

- The growth rate of an infant is fast during the first six months. Its weight doubles in the first 5 to 6 months and triples by the end of a year. Therefore, feeding them in adequate amounts (both in quality and quantity) improves digestion and absorption.
Breastfeeding (breastfeeding) :

- Every baby should be given early and exclusive breastfeeding for six months. Exclusive breastfeeding means giving the baby nothing else except colostrum and breastmilk. Medicines and vitamins can be given in it.
- The 10 steps of BFHI (Baby Friendly Hospital Initiatives) were given by WHO/UNICEF in 1991 which help protect, promote and support breastfeeding.
BFHI : (B.F.H.I) (Baby Friendly Hospital Initiative)

- Baby Friendly Hospital Initiatives is a global program that It was launched in 1991 by the World Health Organization (WHO) and the United Nations International Children’s Emergency Fund (UNICEF).
- Its main goal is to promote, protect, and provide support for breastfeeding and strengthen maternal practices so that the newborn can have the best start in life.
Objectives of BFHI (Baby Friendly Hospital Initiative):
1. To recognize and encourage hospitals and birthing centers that provide optimal levels of care for infant feeding and mother-baby bonding.
2. To properly implement the Ten Steps for Successful Breastfeeding in maternal facilities.
Components of BFHI (Baby Friendly Hospital Initiative):
The Baby Friendly Hospital Initiative has several components that can promote, protect and support breastfeeding.
Here are the main 10 components of the Baby Friendly Hospital Initiative:
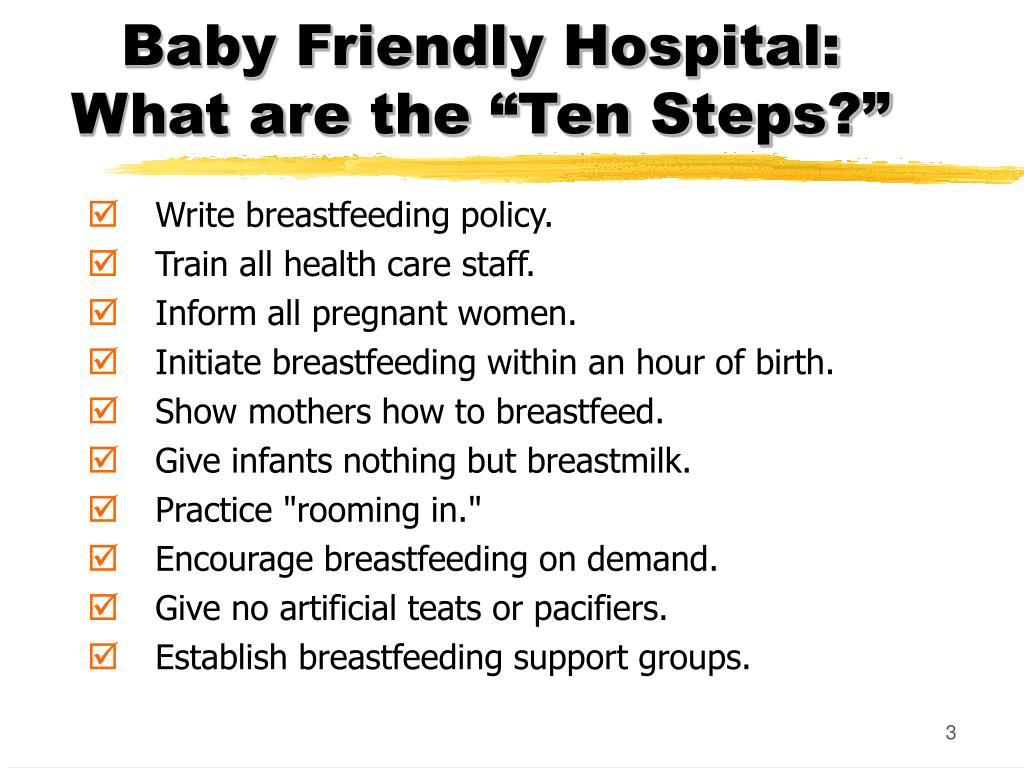
- 1) Have a written breastfeeding policy that is regularly shared with all healthcare personnel To tell.
- 2) To effectively implement the breastfeeding policy, all the necessary skills must be developed. Provide proper training to healthcare staff.
- 3) Provide proper education to all pregnant women about the management of breastfeeding and its benefits.
- 4) Provide proper help to the mother to start breastfeeding the baby within one hour of the birth of the baby.
- 5) Show the mother how to breastfeed and how to maintain breastfeeding, even if the mother is separated from her baby.
- 6) Unless medically indicated, newborns Do not give any food or drink other than breast milk.
- 7) Practice rooming-in-place – Allowing the mother and her baby to be together 24 hours a day.
- 8) Encourage breast feeding on demand – Advise the mother to provide breast feeding whenever the baby shows signs of hunger.
- 9) Do not give artificial teats or pacifiers (also called dummies or soothers) to a breastfeeding infant.
- 10) Promote the establishment of breastfeeding support groups and refer mothers to them upon discharge from the hospital or clinic.
- This component forms the core of the BFHI and is designed to create an environment that supports and encourages breastfeeding as the best way to nourish the infant, promote mother-infant bonding, and improve health outcomes for both mother and infant.
Benefits of (Baby Friendly Hospital Initiative) Benefits of (Baby Friendly Hospital Initiative) :

Health Benefits:
- Best feeding provides many health benefits to both the mother (reduces the risk of breast and ovarian cancer) and the child (reduces the risk of infection, allergies and chronic diseases).
Psychological Benefits
- Breastfeeding promotes bonding between mother and infant.
- It causes emotional attachment between mother and infant.
Economic Benefits
- Breastfeeding helps reduce healthcare costs associated with artificial feeding.
- The Baby Friendly Hospital Initiative (BFHI) is a comprehensive initiative that aims to provide a supportive environment for breastfeeding in health care settings, which can lead to improvements in maternal and child health.
Advantages of Breastfeeding:
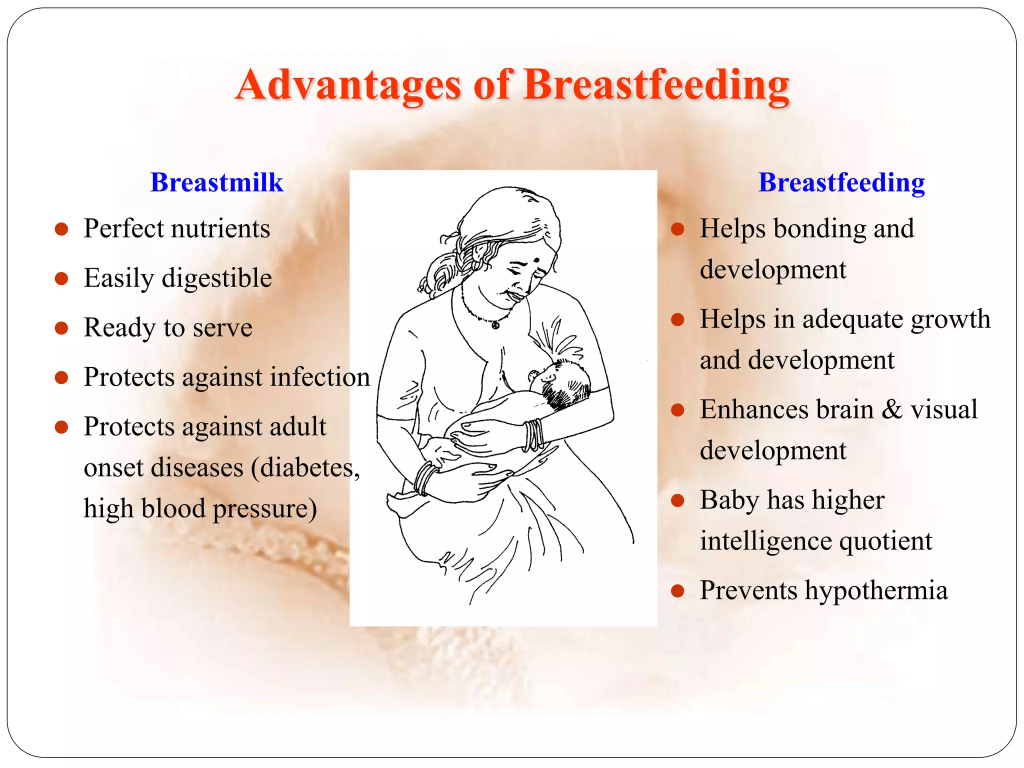
- The benefits of best feeding are as follows:
- Best feeding is the safest, cheapest and best protective food for infants. Human milk is the preferred food for infants due to its superior nutritional and protective value and helps in fulfilling the total nutrient requirement of the infant in the first six months. Due to the best feeding, the child can grow and develop properly.
1) Nutritional value:
- Breast milk is an ideal composition and is easily digestible and contains all the essential nutrients that a baby needs.
- Which is given to a child between the ages of 4 and 6 Milk is essential for growth and development.
- It contains a high percentage of lactose and galactose, which are essential for brain growth.
- It facilitates the absorption of calcium for the growth of the body. Best feeding provides specific nutrients for preterm babies in preterm delivery.
- Best feeding contains amino acids such as cysteine and taurine, which are important during the neonatal period.
- Breastfeeding contains polyunsaturated fatty acids, which are necessary for the myelination of the nervous system.
- Best feeding contains vitamins, minerals, electrolytes, and water, which are necessary for the maturation of the intestinal tract.
- 100 ml of breast milk contains 66 calories, 1.2 grams of protein, 3.8 grams of fat, 7 grams of lactose, 170 to 160 IU of vitamin A, 2 to 6 mg of vitamin C, 2.2 IU of vitamin D, 35 mg of calcium, and 15 mg of phosphorus. mg.
2) Digestibility:
- Breast milk is easily digested due to lactoalbumin and lactoglobulin. Its enzyme lipase facilitates the digestion of fat and provides free fatty acids.
3) Protective Value
- IgA, IgM, macrophages, lymphocytes, unsaturated lactoferrin, lysozyme, etc. present in breast milk provide protection to the baby against infections and allergies.
- Exclusive breastfeeding reduces the chances of diseases like malnutrition, hypertension, diabetes mellitus, coronary artery disease in the baby.
4) Psychological Benefits
- The close physical and emotional bond between the mother and the child due to breastfeeding also improves psychomotor and social development.
- Intelligence and feelings of security increase in the child.
5) Maternal Benefits
- Breastfeeding reduces the chances of postpartum hemorrhage in the mother and improves uterine involution.
- Lactational amenorrhea causes iron recovery.
- Exclusive breastfeeding in the first 6 months provides protection against pregnancy.
- Reduces the risk of breast and ovarian cancer in the mother.
- The body becomes thinner due to the use of excess fat.
- Metabolic efficiency increases and the mother can provide her child with fresh, pure, ready, clear and proper temperature milk.
6) Other Benefits
- Breastfeeding Properly It is convenient, due to which there is no need for preparation.
- Bestfeeding works as a natural contraceptive. Therefore, the chances of conception during the lactation period are low. And Bestfeeding has a laxative action.
- It is used to treat stomach ulcers, gastrointestinal infections, and The chances of eczema are reduced, and the incidence of scurvy and rickets is also reduced.
7) Family and Community Benefits
- Breastfeeding is a proper food for saving money, time and energy.
- The family’s expenses on milk, health care and illness are reduced. Breast milk is economically beneficial for families, hospitals, communities and countries.
Different Composition of Breast Milk:
1) Colostrum
- First after delivery The milk secreted from the breast for 1–5 days is called colostrum. It is thick, yellow and in small quantity. It contains high levels of antibodies, protein and fat soluble vitamins (A,D,E,K) in sufficient quantities. Since it is protective, it is also called the baby’s first immunization.
2) Transitional Milk:
- Breast milk produced for 5–14 days after colostrum in the postnatal period is called transitional milk. It is high in fat and sugar and low in protein and immunological content.
3) Mature Milk:
- Milk produced after 14 days of delivery is called mature milk. It is watery and contains nutrients required for the optimum growth of the baby.
4) Preterm Milk:
- Preterm milk is secreted by mothers who have had a preterm delivery. It contains the right amount of protein, sodium, iron, immunoglobulins and calories for a preterm baby.
5) Foremilk:
- In regular breast feeding, the milk secreted initially is called foremilk. It is more watery and satisfies the baby’s thirst. It is high in protein, sugar, vitamins, and minerals.
6) Hindmilk:
- In regular breastfeeding, the milk secreted last is called hind milk. It is high in fat and energy. It satisfies the baby’s hunger. Therefore, the mother should breastfeed on the other breast only after one breast is completely empty. This way, the baby can get the necessary fluid and nutrients from both the fore and hind milk.
Preparation for Breastfeeding (Preparation for Breastfeeding):

- Preparation for breastfeeding starts during the antenatal period itself. In this, education should be provided to the mother about the benefits of breastfeeding and its technique during the antenatal period itself.
- Examination of the breast should be done during the antenatal period and if there is any problem in the breast, it should be identified early, such as retracted nipple, cracked nipple, and depressed nipple condition, if there is any, it should be treated properly. And the pregnant woman should be provided with necessary advice and intervention regarding its treatment. Adequate amounts of nutritionally rich food should be consumed for energy and nutrients during the prenatal period.
- Advice should be provided to the mother during the antenatal period to maintain adequate amounts of micronutrients, rest, regular exercise and proper hygiene. Counseling should be provided to the mother during the antenatal period for proper breastfeeding techniques.
- Provide adequate counseling to prepare the mother psychologically for breastfeeding immediately after birth. Advise pregnant women to express colostrum and maintain breast cleanliness by proper breast massage during the last 4 weeks of pregnancy.
Management of Breast Feeding
- In modern practice, advise mothers to do breast wash and nipple cleansing at least once a day.
- Advise the mother to wash hands properly before providing breast feeding, and provide the baby with a comfortable position and advise the mother for frequent feeding i.e. 8 to 12 feeds in 24 hours.
Starting breast feeding:
- Breast feeding should be started as soon as possible after birth i.e. half an hour to an hour (1/2-1 hour/ (30 – 60 minutes) should be started.
- If a cesarean delivery has been done, then breastfeeding should be started within the first four hours.
Frequency of Feeding:
Time Schedule:
- Advise the mother to provide feeding at intervals of two to three hours in the first 24 hours after birth, then advise to start a pattern of three to four hours from the end of one week and advise the mother to provide feeding according to the baby’s demand.
Demand feeding:
- In it Breastfeeding when the baby is hungry does not have any restrictions on the amount of feeding and its sequence.
Duration of feed:
- Initially, feed on both breasts for five to ten minutes (5-10 minutes). Therefore, it can help in letdown reflex and then gradually increase the time. Only after one breast is completely empty, put the baby on the other breast so that the baby can get both fore and hind milk.
Night feeding:
- Night feeding is provided to avoid intervals of more than five hours in the initial period so that the baby can get adequate sleep by completely emptying the breast. is.
Amount:
- Average Milk Requirement: First day- 60 ml/ kg/ 24 hours for 10 days. And provide feeding to the baby on demand.
Technique/Position of Breastfeeding:

- The first requirement for providing proper breast feeding to the child should be the mother’s desire due to which successful lactation can occur.
- The mother should be psychologically prepared to provide feeding to the child .
- The mother should drink adequate amounts of milk, juice and water before providing feeding to the child.
- The mother should wash her hands properly before providing feeding.
- The mother should be physically and emotionally relaxed and comfortable, after which the mother can sit comfortably with support behind her back. And it is advised to hold the baby on her lap.
- If she is unable to sit up, she can provide feeding by lying on the child’s side with a pillow under her shoulders.
- The baby’s head should be supported and slightly elevated. Advise the baby to keep his head close to the breast in a semi-sitting position and then support him with one hand.
- The baby’s cheek should touch the nipple so that the baby’s rooting reflex can reach the nipple and the let-down reflex can be anchored.
- If the breast is firm and full, first press the breast with the first finger to prevent the baby from pressing his nose.
- While breastfeeding, alternately and completely breastfeed on both breasts. Advise the mother.
- During the first few days, most babies fall asleep after a few moments. They should be stimulated by gently tickling behind the ear or on the sole of the foot. If possible, one breast should be completely emptied during alternate feedings.
Burping :

- Every baby swallows some air during feeding and the child should be held upright and gently patted on the back until he burps. If too much air is swallowed and not removed, the baby may vomit and have colic. After feeding, diapers should be changed if necessary.
Factors for Successful Lactation:
Positioning, Attachment of Breasts.
Difficulties in Breastfeeding and Its Treatment:
Due to Mother :
- If the mother does not like to provide breast feeding, then listen to the mother calmly and counsel her and solve her problem.
- If the infant’s attachment to the breast is poor, teach him the correct best feeding technique.
- Avoid prelacteal feed Do.
- Provide reassurance and proper support to the mother in case of anxiety and stress.
- Provide proper positioning and emotional support if milk secretion is inadequate.
- Provide proper treatment if the mother has breast engorgement, cracked nipples, depressed nipples, mastitis.
Due to Infant:
- If a low birth weight baby, temporary illness may cause difficulties in breastfeeding.
- Make him burp properly due to air swallowing.
- Surgically correct congenital malformations (cleft lip, cleft palate).
Complimentary Feeding or Weaning:

- Only breastfeeding is sufficient for the growth and development of the infant for 4 to 6 months. Weaning or complementary feeding is the gradual and progressive transfer of the baby from breastfeeding to the family’s usual food. When breastfeeding is insufficient for the child, weaning food is provided in addition to it.
- Weaning food is usually provided first in the form of liquid food, then semi-solid, and then solid food. In which, liquid food includes vegetable soup, tomato Pulsates and fruit juices are involved.
- In semi-solid food, potatoes, pulses and root vegetables should be cooked well and washed before feeding. Bananas can be fed mashed. Soft cooked rice and soft cooked fish can be fed mashed before feeding.
- To increase the nutritional value, foods like ragi + jaggery + gram + ghee + sugar can be used. This will supply protein, calories and iron and in solid food, cooked rice, chapati, idli, bread, biscuits, peanuts, roasted gram, bananas. Solid foods can be started when children learn to chew properly.
- The period for weaning foods is usually between six months and one year.
Artificial feeding :

- When an infant is fed preparations other than human milk, drugs or vitamins, it is called artificial feeding. When it is given by a bottle, it is called bottle feeding and it can also be given without a bottle.
Indications:
- When there is a temporary or permanent contraindication to best feeding When.
- When there is an inadequate amount of breast feeding.
- When there is a change in the woman’s lifestyle or socio-economic condition.
Food used:
- As a substitute for breast milk There is no perfect formula but the following foods can be used. Such as, boiled cow’s milk,
- Dried milk formula,
- Cow’s milk,
- Buffalo milk.
Principles of Artificial Feeding :

- When all efforts to breastfeed the baby fail, when human milk is not available, consider artificial feeding.
- Provide the baby with a properly comfortable position during feeding.
- The purpose of artificial feeding is the same as that of breastfeeding. As it provides adequate nutrients, it is sterile and economical and according to the needs of the baby.
- Artificial feeding should be given from a spoon, bowl, or cup. It should be given through a dropper in sick and preterm infants and through a nasogastric tube in hospitalized babies.
- Bottle feeding should be avoided and the mother should be explained about the risk of diarrhea.
- Strict cleanliness should be maintained in the preparation and feeding procedure and the leftover milk should not be reused.
- Fluid and calories should be counted according to the baby’s weight and fed in an adequate amount.
- Correct feeding schedule The method should be maintained and the milk should be lukewarm.
- The time should be kept for 15 to 20 minutes according to the total quantity, in which the frequency of feeding in infants should be six to eight times and in older babies 3 to 5 times.
- If cow’s milk is available, then provide it by diluting it in cow’s milk for the first two months and then provide it with undiluted milk, cool lukewarm milk with sugar added.
- If dried milk (milk powder) is to be used, then it should be used as prescribed and It should be made according to the manufacturer’s instructions.
- If the infant has any illness, then feed frequently and in small quantities as the calorie requirement is high during the illness. If air has been swallowed, then remove it and Burping to prevent vomiting and discomfort.
- Provide supplementation if the baby has any vitamin and mineral deficiencies.
- After feeding the baby, clean all the utensils properly and sterilize them by boiling them.
Successful Feeding
- The most satisfactory guideline for successful feeding is regular weight gain of the baby after 10 days which should be at the rate of 25-30 g/day for 3 months.
Care of Skin, Eyes , Buttocks, Cord of Newborn (Care of Skin, Eyes, Buttocks, Cord of Newborn) :

Care of Skin:
- Blood, mucus and meconium on the baby’s body should be gently cleaned with a sterile moist swab and should not be given a deep bath until it falls off on its own. Since vernix caseosa provides protection to the baby’s smooth skin, it should not be rubbed off. Baby’s clothes and equipment should be kept separate to prevent cross-infection from other infected persons.
Baby Bath
- When giving a baby bath in the hospital or at home, proper instructions should be followed, such as giving the baby a bath slowly and gently in a separate room, drying him from head to toe and covering him with a warm towel or cloth. In winter, sponge baths should be provided instead of dip baths.
- Massaging the baby using olive oil or coconut oil three to four weeks after the birth improves circulation and muscle tone. Oil massage should be done before providing the baby with a bath. Do not use mustard oil (castor oil) for massage as it causes skin irritation.
- Keeping the baby in sunlight exposes his body to sunlight and provides adequate amount of vitamin D.
- When bathing the baby, his behavior may be abnormal, Observe for infection, Mongolian sports, milia and toxic erythema.
Clothing of the baby/ Care of buttocks:
- The baby should be dressed in loose, soft and cotton clothes.
- Thick, soft and absorbent cotton cloths should be used as napkins. But synthetic clothes should not be used.
- Clean the baby’s clothes with a little detergent and let them dry properly in sunlight should be used to prevent skin irritation.
- Wet napkins should be changed immediately.
Care of ice:
- Clean the ice properly from the inner canthus to the outer canthus by dipping a sterile cotton swab in normal saline or sterile water.
- Clean both eyes with separate swabs.
- Erythromycin (0.5%) and silver nitrate drops (1%) can also be used.
- Do not apply mascara to the eyes, this can prevent ophthalmia neonatorum.
- Redness in the eyes Observe for sticky eyes and excessive tears.
- According to cultural practice, human colostrum can be used to prevent sticky eyes.
Care of Umbilical Cord:
- After delivery, the umbilical cord should be cut 2-3 inches away from the navel.
- To maintain aseptic precautions, the cord should be ligated using sterile cotton thread or a plastic cord clamp.
- Then inspect the cord ligature for looseness or bleeding.
- Usually the cord is The fall down will occur in 5 to 10 days, if not, then observe to see if there is a condition of infection.
- Do not apply dressing on the cord. It should be kept open and dry.
Bonding (Bonding) :

Definition:
- Bonding is the emotional connection that develops between parents and their newborn. It is a crucial aspect of a child’s early development, influencing the child’s emotional, social, and psychological well-being.
- Bonding is a critical component of early childhood development and involves the dynamic interplay of emotional, physical, and behavioral elements. It lays the foundation for a secure and supportive parent-child relationship, which is essential for the child’s overall well-being and future development.
Importance:
1) Emotional Security
- Baby’s Early bonding after birth provides the baby with a sense of security and comfort, which is important for the baby’s growth and emotional development.
2) Attachment
- Bonding is the foundation for a strong parent-child relationship, and contributes to better social and emotional development for the child.
3) Parental Satisfaction
- Bonding helps in developing a strong connection, understanding and relationship between both the parent and the child. And helps develop parental satisfaction and confidence.
How bonding happens:
Skin to skin contact:
- Keeping the child close, often with skin-to-skin contact immediately after birth It helps control the baby’s body temperature and heart rate and it Helps promote bonding.
Breastfeeding:
- Best feeding not only provides nutrients but also promotes bonding between mother and child through physical closeness and eye contact.
Gentle touch and voice:
- Hugs, soothes and talks to the baby strengthens the parent-child bond.
Challenges:
Postpartum Depression:
- This condition can affect the bonding process, making it difficult for parents to bond with their child.
Premature Birth:
- Premature babies and their parents may have different bonding experiences due to medical interventions and time spent in the neonatal unit.
Rooming-in :

- Rooming-in means that after the birth of a newborn, the mother and her baby are kept together in the same room instead of keeping them in a separate nursery for care. Rooming-in maintains the body temperature of the newborn, allows them to breastfeed in an adequate amount, and also improves the bonding relationship between the mother and her child.
- The concept of keeping the mother and her child in the same room in the hospital for the care of the child after the birth of the child or after hospitalization is called rooming-in.
Objectives:
1) Promote bonding
- The rooming-in concept maintains a continuous physical connection between the mother and her child, which allows for proper bonding to be established between them. And a strong emotional connection can be established.
2) Support breastfeeding:
- Due to the rumination-in concept, the mother can immediately recognize the food signals made by her child, due to which the child gets breast feeding properly.
3) Enhance Parental Involvement:
- Rooming-in allows parents to be more involved in their child’s care from the very beginning, due to which Promotes a sense of competence and confidence in parenting.
4) Integrated Care:
- When the mother and her child are together, health care providers can properly monitor the health of both. and provides facilities for coordinated care.
Implementation:
Hospital Arrangement:
- In a rooming-in setup, the baby is placed in a bassinet next to the mother’s bed. Hospitals that implement rooming-in usually have appropriate facilities such as private or semi-private rooms.
Care Procedures:
- Health care personnel make daily room visits to assess, provide care, and provide support to the mother for breastfeeding and newborn care. This includes assisting with any necessary medical procedures and ensuring the well-being of both the mother and baby. It happens.
Parenting Guidance:
- Parents receive guidance on newborn care, safe sleep practices, and breastfeeding techniques. This support helps them manage their baby’s immediate needs.
Benefits:
1) Improve bonding:
- Continuous contact strengthens the emotional bonding between mother and baby. Which is crucial for the baby’s emotional development and well-being.
2) Better Breastfeeding Outcomes:
- Due to the rooming-in concept, the child can get adequate amount and frequent breastfeeding. Which improves milk supply and supports the baby’s nutritional needs.
3) Reduce Stress:
- Keeping a parent and their child close can reduce anxiety and stress for both the mother and the child. And the mother and her child get a more comfortable and stable environment.
4) Enhancing Monitoring:
- If the mother and child are together, the health care provider can properly assess both of them and provide proper health care facilities as per their needs and if there is any complication, it can be identified early.
Challenges:
1) Sleep disturbances:
- The needs of the baby can cause interruptions in the mother’s sleep, which can be challenging, especially for those recovering from childbirth.
2) Resource Limitations:
- Not all hospitals have facilities available for the concept of rooming-in and the availability of adequate amount of health care personnel who can provide rooming-in care can also be a challenge.
3)Parental Overwhelm:
- New parents may become overwhelmed by the constant presence of their newborn care and may occasionally need rest or extra support.
Minor Disorder of Newborn :
Minor disorders are mainly seen in newborns and can lead to complications if not treated properly. Minor alignment is a physical condition that can cause disturbances in normal function.
Minor disorders such as,
1)Stuffy nose,
2)Sticky eyes,
3)Skin rashes:
Types:
a) Blotchy Erythematous,
b) Napkin rash (ammonia dermatitis),
c) Perianal dermatitis,
d) Intertrigo,
E) Oral thrush.
4) Congenital phimosis,
5) Genital Crisis,
6) Birth marks,
7) Physiological jaundice,
8) Constipation.
1) Stuffy nose:
If there is a stuffy nose, then the newborn is breathing through the mouth, due to which the newborn is taking in excessive air. Swallows and due to this, conditions like abdominal distension and vomiting are seen in newborns.
Treatment:
The nostrils are flushed with normal saline through clean cotton. The eye can be cleaned by soaking it.
2) Sticky eye:
Sticky eye can be caused by a chemical irritant or bacterial conjunctivitis caused by Streptococcus bacteria.
Treatment:
Erythromycin to treat sticky eye Eye ointment should be used every six hours for seven to ten days.
3)Skin rashes:
Types:
a) Blotchy erythematous,
b) Napkin rash (ammonia dermatitis),
c) Perianal Dermatitis,
d) Intertrigo,
E) Oral thrush,
a) Blotchy erythematous:
Blotchy erythematous is located on the trunk, limbs and face and disappears within a day or two.
Treatment:
Blotchy erythematous can be treated by applying only powder after bathing the baby.
b) Napkin Race:
Napkin rash is more common in artificially fed babies.
It is also called ammonia dermatitis.
Napkin rash is
Diarrhea,
Frequent loose stools,
Strong ammoniacal urine,
Due to poor hygiene,
Due to wet nappies staying in for a long time,
Due to fungal infections,
Using nylon or water tight plastic napkins.
Napkin rash can occur.
Prevention:
Napkin rash can be prevented by providing frequent care and attention to the napkin area and by changing the napkin properly when it becomes soiled.
This condition can be prevented by changing the wet napkin immediately and keeping the skin dry.
Washing the napkins properly with an antiseptic solution.
c) Perianal dermatitis:
Perianal dermatitis is a condition that occurs around the anal opening.
The skin around the anus appears red, indurated, and excoriated. It is usually caused by the alkalinity of the stool. It is more common in babies who are formula fed and artificially fed.
Treatment:
Can be prevented by changing the wet napkin immediately and keeping the skin dry.
Wash the napkin properly with an antiseptic solution.
Keep the napkin in air or sunlight and apply coconut oil or anti-fungal cream to the perianal region.
d) Intertrigo:
This is a variant of napkin rash in which soreness occurs in the groin area and flexures (folding areas).
It also occurs in the folds of the neck.
It is caused by the contact of two surfaces of wet skin and the cut-off of air in this skin, which gradually becomes infected.
Treatment:
Treatment involves exposing the infant’s buttocks to warm air to promote healing.
Advise the mother to avoid plastic pants. Avoid as it prevents evaporation and increases skin damage due to urine breakdown.
E) Oral Thrush:
Oral thrush is an infection of the buccal mucous membrane and tongue caused by Candida albicans.
Treatment:
Oral Thrush
Its treatment is 1% gentian violet solution or nystatin suspension (100,000 units/ml) applied to each side of the mouth 3-4 times a day with a cotton-tipped swab.
4) Congenital phimosis:
In this, the prepuce in newborns is pinpoint due to which the newborn feels discomfort during urination, which causes the baby to cry.
Treatment:
Congenital phimosis is treated by dilatation using Mosquito forceps.
5) Genital crisis:
Genital crisis does not require any treatment. Only reactions are provided and the mother is assured and explained that genital crises are likely to occur in a short time, including,
Mastitis neonaterum,
Hydrocele of the newborn,
Vaginal bleeding during the first week.
Etc. involvement.
6. Birthmarks:
Introduction:
The main cause of birthmarks is unknown but they are less common in Asian people but more common in Spain, Italy and some Arab countries.
They believe that these birthmarks are caused by the unsatisfied and unfulfilled desires of the pregnant mother.
Ex: Any twenty of the antenatal mother and If the baby’s vulva has not fully developed, birthmarks can be seen on the child’s skin.
Birthmarks are benign irregularities that appear on the skin of a newborn at the time of birth or shortly after birth. They are called birthmarks.
Birthmarks are divided into two types.
a) Pigmented birthmarks:
Pigmented birthmarks are caused by excessive skin cells becoming pigmented, including,
Mole,
Café à lait spots,
Mongolian spots.
b) Vascular birthmarks:
Vascular birthmarks are red Birthmarks are called that are usually seen due to increased blood vessel size.
Such as,
Muscular stain
(salmon patches),
Hemangiomas,
Port wine stain.
Etc. There are
Types of Birth Marks:
1) Café au Lait Spots:
-
- This is a type of pigmented birth mark. This is one of the most common birthmarks that is usually oval in shape and is found in light brown to milky coffee color.
-
- This birthmark is seen at the time of birth and sometimes presents itself some time after birth.
-
- These birthmarks do not fade with increasing age.
b) Silver mark:
-
- This appears as a silver streak on the right or left side, where the forefade and hairline meet. It is hereditary.
C) Port Wine Stain:
-
- This is a vascular birthmark that appears as red and purple marks on the face and can also be found elsewhere on the body.
-
- Port wine stains are caused by abnormal bleeding from blood vessels in the affected area. They can vary in size. It is a few millimeters in size and can even become dark if left untreated.
d) Salmon patches/Stroke beats/Telangectatic nevus:
- This is a vascular birthmark that usually presents as slightly reddened skin patches on the face.
- It is also seen on the nape of the neck, upper eyelid, forehead, and nose. It resolves on its own within a few months.
e) Hemangiomas:
- This is a vascular birthmark and is a strawberry mark. It is a red and raised mark.
- Initially it is small and flat but it enlarges during the fourth to fifth month of life Rapid growth occurs and then it fades (shrinks).
f) Mongolian spot:
- This is a pigmented birthmark.
- This Mongolian spot is a harmless mark. Its color is bluish gray.
- Mongolian spots are a type of skin pigmentation disorder in Down syndrome, affecting the sacral area of a newborn baby, and sometimes the back and extremities. Irregular blue patches are seen and resolve on their own within six months to one year of age.
G) Congenital melanocyte nevus:
- This is a pigmented birthmark that can be found anywhere on the body but is usually more common on the head and parts of the body. It is light brown to black in color. It is irregular in shape, flat, raised and lumpy.
- They are often dark and become hairy during puberty.
Treatment:
- Most birthmarks are harmless and do not require treatment.
- Pigmented marks resolve on their own while vascular birthmarks need to be removed for cosmetic reasons. is.
H) Milia:
- Many small raised white or yellowish white spots are seen on the nose, nasolabial fold, cheeks and forehead of the neonate due to sebum retention. These are called milia.
- Initially, they resolve on their own within a few weeks.
I) Epstein Pearl:
- Epithelial cysts in the lateral to midline of the hard plate are seen as whitish sporulations, which are called Epstein Pearls, and do not require any treatment.
7) Physiological Jaundice :
- Physiological jaundice is usually seen in newborns, also called neonatal jaundice.
- In this condition, the skin and sclera of the newborn turn yellow due to an increase in the amount of bilirubin in the body.
- This jaundice appears within two to three days after birth and its peak level is seen on the sixth to seventh day. It is usually due to the immaturity of the liver, in which As the liver functions properly, the pair is relieved.
Treatment:
- Physiological jaundice resolves within a week.
- Provide adequate extra fluids to the child.
- Provide proper phototherapy to reduce the child’s bilirubin.
8) Constipation:
- Constipation is more common in artificially fed babies.
Treatment:
- Correct dietary errors properly.
- Provide some fluids to the neonate.
- Do not provide laxatives to the neonate.
- If the above measures fail, provide some milk of magnesia.
- Avoid insertion of suppositories and catheters in the neonate.
Caput Sucadenium (Caput Sucadenium) :
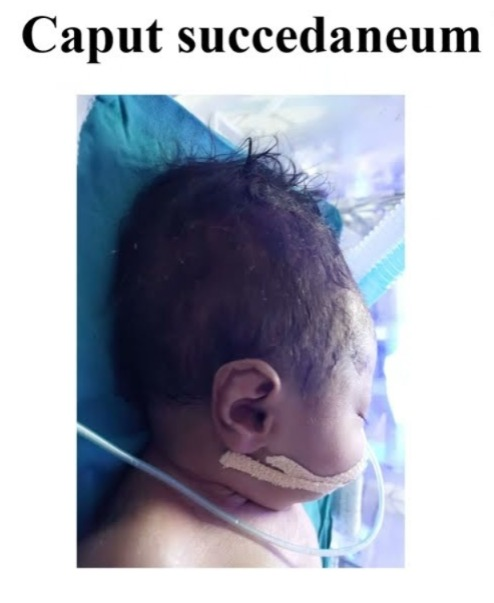
- Edematous swelling due to accumulation of serosanguineous fluid in the layers of the scalp is called caput succedaneum. It is caused by pressure from the girdle of contact. It is sometimes the bony pelvis, dilating cervix or vulval ring. Due to reduced venous return, swelling and lymphatic drainage are seen.
- Caput succedaneum is also seen at the time of birth. And when pressed, it forms a pit. The swelling is boggy. And it crosses the suture line which disappears in 24-36 hours. It is mostly seen after membrane rupture.
Cephalohematoma (Cephalohematoma) :
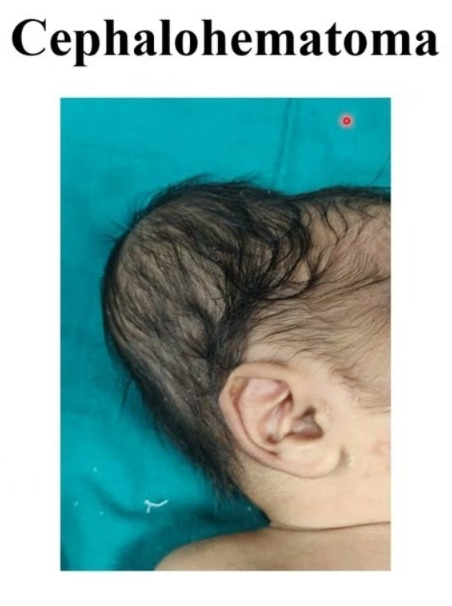
- A cephalohematoma is a condition in which the head is not Collection of blood under the pericranium and flat bones that cover the skull bone, usually unilateral and over the parietal bone.
- It is caused by rupture of a small emissary vein from the skull and may be associated with a fracture of the skull bone. It can be caused by forceps delivery but can also be seen after normal labor. Ventouse application does not increase the incidence of cephalohematoma. It is never present at birth but develops gradually after 12-24 hours.
- This swelling is limited by the lines of the pericranium sutures of the skull which are fixed to the bone margin, soft, fluctuant and incompressible.
- It grows and disappears on its own within a few weeks, i.e. approximately 6 weeks.
- Difference between Captive Succedenium and Cephalohematoma
Cephelohematoma:
- It develops within a few hours after birth.
- It increases in size for 2-3 days.
- In it, the swelling is limited to the bone, i.e. it does not cross the suture line.
- It is confined.
- It does not make a dent when pressed.
- Double cephalohematoma usually appears bilaterally.
- The border of the cephalohematoma may be marked and well defined.
- The cause of cephalohematoma is subperiosteal hemorrhage.
- It disappears about 6 weeks after birth.
- Its complications may include jaundice, skull fracture, intracranial bleeding, and shock. is.
Caput Succadenium:
- Caput Succadenium is present at birth.
- It does not increase in size.
- Its swelling is unlimited and can cross the suture line.
- It is diffuse.
- It is indented when pressed.
- Double caput is always unilateral.
- The border in caput succadenium is indistinct and poorly defined.
- Cause of caput diffuse There is edematous swelling and soft tissue involvement.
- It disappears a few days after birth.
- Complications are rare. And if present, anemia may be present.
Birth asphyxia or asphyxia neonatorum :
Definition:
- Asphyxia neonatorum means that satisfactory pulmonary respiration is not established at the time of birth, which means It may be the absence of a pulse. Clinically, it is also defined as the failure to initiate and maintain spontaneous respiration within one minute of birth. This leads to varying degrees of hypoxic and ischemic injury to body tissues and organs. It is also accompanied by hypoventilation, anaerobic glycolysis, and lactic acidosis.
- Its characteristics include progressive hypoxia, hypercapnia, hypoperfusion, and metabolic acidosis. It results in hypoxic ischemic encephalopathy and neuromotor sequelae (neuromotor sequelae are long-term neurological and motor impairments due to brain injury or dysfunction) with multi-organ dysfunction.
Etiology:
- Obstruction of the air passages due to inhaled mucus or amniotic fluid.
- Lungs expansion failure due to low alveolar surfactant.
- Morphine, pethidine and anesthetic agents given to the mother during the prenatal and intranatal periods can cause asphyxia due to depression of the baby’s respiratory center.
- In the placental circulation Intrauterine hypoxia is the main cause of neonatal hypoxia due to disturbances such as anatomical changes in the placenta, prematurity of the placenta, separation, post-dated pregnancy, retroplacental hemorrhage, pregnancy-induced hypertension, and cord compression. Birth trauma. Difficult forceps delivery, prolonged labor, contracted pelvis, breech delivery, oblique lie, occipito posterior position etc.
- Due to weak respiratory muscles, immature respiratory center, and poor lung expansion in premature babies.
- Due to congenital heart disease, blood loss, and circulatory collapse in shock.
Classification:
It is divided into two parts according to the intensity of clinical features such as:
1) Asphyxia Livida / Stage of Cyanosis / Blue Asphyxia
This is the primary condition of respiratory failure in which the APGAR SCORE may be 4-6.
2) Asphyxia Pallida / Stage of Shock / White Asphyxia
This is a condition of respiratory and vasomotor failure in which the APGAR SCORE is 0 – 3 May be.
Clinical Features:
- The clinical features of neonatal asphyxia depend on the degree of depression, duration of low oxygen, plasma CO2 level, and cause.
- Muscle tone decreases.
- Respiratory distress may be seen is.
- Breathing difficulties are seen.
- Irregular breathing is seen.
- Cyanosis (bluish discoloration of the skin, especially around the lips and face.)
- Heart rate abnormalities (such as bradycardia and tachycardia).
- Alertness and reduced responsiveness.
- Seizures.
- Feeding difficulties.
Management:
Asphyxia neonatorum The management of is divided into two parts, namely,
1) Prophylactic Management,
2) Definitive Management
1) Prophylactic Management:
- Identify high-risk pregnancies during the antenatal period.
- Early detection of early fetal distress can be done in high-risk pregnancies. Due to which, early identification can be done if there is a condition of fetal distress.
- Use electronic fetal monitoring during intrapartum period and do scalp blood pH assessment as needed.
- Proper use of anesthetic agents and anti-depressant medication during labor.
- Definitive nursing management
- Assess the baby’s APGAR score and provide proper treatment accordingly.
- If the APGAR score is between 7 – 10, it is considered normal.
- If there is mucus in the baby’s oropharynx and laryngopharynx, suction it properly and clear it.
- If necessary, provide supplementary oxygen.
- Then reassess the neonate’s condition after five minutes. If normal, send the infant to the nursery.
- If the baby’s APGAR score is between 4-6,
- Suction the baby’s mucus from the oropharynx and nasopharynx immediately using a mucus sucker or suction operators.
- Then, place the baby on a flat surface and in a head-down position, turning his face to one side so that the mucus can drain through gravitational force.
- Simultaneously, oxygen should be administered to the baby through a bag and mask at a pressure range of 25-30 cm H2O.
- If necessary, provide intermittent positive pressure ventilation to the infant.
- Provide stimulation to the infant on the back and sole.
- In the majority of cases, the baby can take independent respiration using these simple measures.
- Then assess the baby’s APGAR score at five minutes and if satisfactory, return the infant to the mother.
- If the above measures fail,
- Perform oral suctioning and start endotracheal intubation.
- Connect the endotracheal tube to the resuscitation bag, through which O2 can be administered at a rate of 6-8 liters/minute.
- Intermittent positive pressure airway (IPPV) ventilation should be maintained at 30 – 40/min.
- If the heart rate is less than 60/min, perform central external cardiac massage.
- If the mother has a history of using central depressant drugs such as pethidine or morphine within 3 hours of delivery. An appropriate antidote, e.g. naloxone hydrochloride 60 mg/kg IM (single dose) or 10 µg/kg IV, is given and may need to be repeated.
- To combat acidosis, 8.4% NaHCO3 (sodium bicarbonate) 1 mEq/kg in 5% dextrose (diluted 1:1) is given very slowly (at a rate of 1 ml/min) via umbilical or peripheral vein in the minimum dose.
- If the baby’s APGAR score is below 4,
- Immediately perform tracheal intubation and start intermittent positive pressure ventilation.
- If the mother has a history of using central depressant drugs such as pethidine or morphine within 3 hours of delivery. An appropriate antidote, e.g. naloxone hydrochloride 10 µg/kg IV is given to the neonate.
- It is repeated every 2 – 3 minutes.
- Complications:
- Respiratory distress syndrome,
- Cardiac failure,
- Respiratory infection,
- Septicemia,
- Disseminated intravascular coagulation (DIC),
- Hyperbilirubinemia,
- Cerebral depression,
- Failure to thrive,
- Mental retardation,
- Cerebral palsy,
- Convulsive disorders.
Prevention:
- To prevent asphyxia, detect risk factors and provide intensive internal care.
- Manage risk factors through necessary facilities or referral.
- To detect fetal hypoxia, intranatal assessment of fetal condition
- Assess and manage fetal distress.
- Prevent birth injuries through efficient management of malpresentation, contracted pelvis, instrumental delivery.
- Carefully use anesthetic and depressant agents during labor.
Prognosis:
- The prognosis of neonatal hypoxia depends on the baby’s maturity, duration and intensity of hypoxia, acidosis, and competent management.
Respiratory Distress Syndrome (RDS)
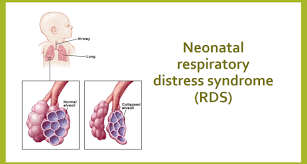
Definition:
- Respiratory distress syndrome is a lung disease seen in newborns/neonates. Which is mainly seen in premature babies, neonates whose mothers are diabetic, children whose birth is by cesarean section or children who have breech delivery.
- Respiratory distress syndrome (RDS) is usually seen due to the deficiency of surfactant {SURFACTANT(an enzyme that works to reduce the surface tension of the alveoli.)} in the neonate’s body.
- The main reason for this is that when the newborn child’s body does not produce an adequate amount of surfactant The baby cannot produce surfactant and due to this surfactant not being in adequate amount, the baby’s lungs cannot function properly due to which gaseous exchange also does not take place properly due to which the amount of oxygen in the child’s body is reduced due to which the condition of hypoxia and acidosis arises.
Surfactant:
Introduction
- Surfactant is a type of lipoprotein substance produced by a combination of phospholipids, mainly lecithin and sphingomyelin. Its ratio is usually (lecithin (L)): sphingomyelin (S)) 2: 1. Thus, lecithin and sphingomyelin combine to produce surfactant.
Function
- Surfactant works to reduce the surface tension inside the alveoli, its functional unit in the lungs, due to which both the lungs and the alveoli do not collapse and gaseous exchange continues to take place properly within them.
Production
- Surfactant starts to be produced in the 20th week of gestation period and its maximum production occurs during the 37th week of gestation period. The hormone cortisol helps in the production of surfactant.
- Surfactant is produced by the alveolar type 2 epithelial cells of the lungs in the newborn. And its storage takes place in the laminar bodies (LBS) of the alveolar cells. The maximum activity of surfactant for the maturation of the lungs occurs at 34 weeks of gestation.
- A child born before 37 weeks of gestation is called a preterm baby and is more likely to develop the condition of respiratory distress syndrome (RDS) due to insufficient production of surfactant. Therefore, among all premature children, respiratory distress syndrome is seen in 50 – 80% of them.
Etiology:
- Prematurity,
- Low birth weight baby,
- Asphyxia,
- Maternal diabetes.
Signs and symptoms:
- Rapid and shallow breathing,
- Respiratory rate >60/minute,
- Expiratory audible grating sound,
- Rib retraction,
- Intercostal or subcostal retraction,
- Cyanosis,
- In AD,
- Respiratory acidosis,
- Electrolyte disturbance,
- Dyspnea.
Diagnostic Evaluation:
- History collection,
- Physical examination,
- Chest X ray.
- Management:
Aim of treatment:
- Provide surfactant replacement therapy.
- Provide breathing support through a nasal continuous positive airway pressure (NCPAP) machine or ventilator to help the infant breathe properly.
- Provide oxygen therapy.
Nursing Management:
- If infants and neonates are suffering from respiratory distress syndrome (RDS), they should be provided with artificial surfactant by inserting an artificial airway or breathing tube into the trachea/windpipe, which allows the surfactant to enter the lungs directly.
- Usually, surfactant in the lungs of a fetus is Formation starts from 24 weeks of gestation and is completely formed at 37 weeks of gestation. If adequate amount of formation is not achieved, then artificial surfactant should be provided in such conditions.
- Proper ventilatory support should be provided to the infant.
- Infants with respiratory distress syndrome need ventilatory support, which is provided by a mechanical ventilator connected to a breathing tube and this tube is inserted into the infant’s mouth. Or provide mechanical ventilatory support through the nose into the windpipe.
- Provide breathing support to the neonate through nasal continuous positive airway pressure (NCPAP).
- To condition and treat hypoxia and acidosis in the neonate, provide warmed and humidified oxygen therapy at 35% to 40% positive pressure through endotracheal intubation.
- If the arterial oxygen tension PO2 is 50 mm of Hg Provide continuous positive airway pressure (CPAP) to the neonate when it is not more than .
- Check the levels of PO2, PCO2, and PH to identify any metabolic and respiratory acidosis condition early.
- If there is a condition of acidosis, administer sodium bicarbonate 4.2%. (0.5 meq/ ml Ex: 0.5 meq/ ml amount to 1 meq/kg weight 1:1 with 5% glucose as minimum dose.)
- Excessive use of alkaline can cause intraventricular hemorrhage or even death in preterm babies.
- An infant suffering from respiratory distress syndrome (RDS) may be admitted to the NICU. (NICU) and are kept in a radiant warmer or incubator to keep them warm and reduce the risk of infection.
- In this, the infant’s air passages are periodically cleaned by endotracheal suctioning.
- Continuous monitoring of heart rate, breathing and temperature through sensors taped to the infant’s body, in addition to using sensors on the fingers or toes to check the amount of oxygen in the infant’s blood.
- As prescribed by the pediatrician Administer albumin or colloid solution to treat the condition of hypovolemia.
- If there is a condition of anemia or electrolyte imbalance, then treat it properly.
- Maintain the nutritional level of the child properly by administering intragastric feeding or intra-veinal 10% glucose i.e. 70ml/kg body weight daily to prevent malnutrition followed by breast milk and infant formula through feeding tube.
- Regularly monitor fluid intake to ensure fluid does not build up in the child’s lungs.
Complications:
- Intraventricular hemorrhage,
- Pulmonary hemorrhage,
- Retrolental fibroplasia,
- Neurological abnormalities.
Prevention:
- Betamethasone should be administered to patients who are likely to deliver before 34 weeks.
- Assess lung maturity before inducing pre-mature labor and delay induction to minimize fetal risk.
- Prevent fetal hypoxia in diabetic mothers.
Neonatal jaundice:

Definition:
- When yellow discoloration is seen in the skin, sclera, and mucous membranes and in body secretions due to the accumulation of excessive bilirubin in body tissues, it is called “neonatal jaundice”.
- Normal bilirubin in the blood is 0.1 to 0.8 mg/dl. Now when the level of bilirubin in the body is 5 mg/dl, it is called neonatal jaundice, also called icterus neonatorum or neonatal hyperbilirubinemia.
Incidence:
- Approximately 60% of full-term babies and 80% of preterm babies are seen in the first week of life.
- About 6% of term babies have severe jaundice with bilirubin levels of 15 mg/dl Or it develops in a greater proportion than that.
Types of Jaundice:
There are generally two types of jaundice, such as,
1) Physiological jaundice,
2) Pathological jaundice.
1) Physiological jaundice:
- Physiological jaundice is a non-hemolytic jaundice caused by immaturity.
- In which the life span of neonatal RBC (red blood cells) is short and the conversion of urobilinogen is reduced. Defective uptake of bilirubin from plasma into liver cells, poor conjugation of bilirubin, increased enterohepatic circulation increases the load on the liver and causes defects.
Characteristics:
- This jaundice mainly appears within 24 – 72 hours after birth.
- The maximum yellow discoloration occurs in full term babies on the 4th – 5th day and It is seen in preterm babies up to 6th – 7th day.
- It mostly disappears by 7th day in full term babies and by 14th day in pre-preterm babies.
- The bilirubin level in it does not exceed 12 – 15 mg/dl.
- It mostly does not require treatment and gets relieved on its own.
Causes:
- Due to excessive hemolysis of red cells.
- Due to defective conjugation of bilirubin.
- Due to failure of excretion of conjugated bilirubin.
- Due to Rh incompatibility.
- Due to cephalohematoma.
- ABO incompatibility.
- Vitamin K therapy.
- Congenital spherocytosis.
- Due to glucose 6 phosphate dehydrogenase deficiency.
- Prematurity causes decreased production of enzymes such as glucuronyl transferase by immature liver cells. Due to.
Types:
- Prolonged unconjugated hyperbilirubinemia
- It is mainly caused by hemolytic disease of the breast milk.
- Prolonged conjugated hyperbilirubinemia: It is mainly caused by infection.
Clinical Features:
- Yellow staining is seen on the face, trunk, palms and soles (bottom of the feet).
- Urine staining is seen on clothes.
- The color of the stool is clay, white or dark.
- Bilirubin level 5 mg/dl/day.
- Then other features such as lethargy, drowsiness, poor sucking reflex, fever, infection, etc. are seen.
- When bilirubin develops more than 15 mg/dl, kernicterus (a pathological condition of the brain due to unconjugated bilirubin) develops.
- Its features include vomiting, high-pitched cry, convulsions, opisthotonus position, Nystagmus, hyperpyrexia, and spasticity are seen.
Treatment:
- The following methods are used to treat jaundice:
- 1) Phototherapy
- 2) Pharmacologic therapy
- 3) Exchange Transfusion
Phototherapy:
- Phototherapy is best used in moderate cases when the bilirubin level rises above (12 mg%).
- Phototherapy is stopped when the serum bilirubin level is about 10 mg %. Once phototherapy is discontinued, there may be a rebound increase in serum bilirubin. Adequate hydration of the newborn is essential. Special blue lamps with an output of 420 to 470 nm wavelength are most effective in treatment.
- Phototherapy should be started as early as possible to allow maximum surface area to be exposed and ice to be applied.
- Phototherapy causes insensible fluid loss in the newborn. Hydration is promoted by breastfeeding. Administering intravenous fluid therapy during phototherapy.
- Phototherapy blanket protects the infant.
Phenobarbital therapy:
- Phenobarbital therapy induces hepatic microsomal enzymes and increases bilirubin conjugation and excretion. A dose of 5.8 mg/kg every 24 hours. is used. It takes 3-7 days to become effective. However, as a prophylaxis, it can be used in. In which the mother is provided with a rate of 90 mg/dl for two weeks before delivery.
Exchange Transfusion:
- Exchange transfusion is usually used to prevent kernicterus.
- In which double volume exchange replaces about 80% of red blood cells and about 50% of Helps reduce bilirubin levels.
Indication of Exchange Transfusion
- Despite phototherapy, the bilirubin level in the body is progressively increasing (more than 1mg/dl/hour).
- In cases where the neonate has anemia and congestive cardiac failure In.
- If the newborn’s serum bilirubin level is more than 20 mg/ dl.
- If the cord blood hemoglobin is less than 12 g/ dl and the bilirubin level is more than 5 mg/ dl.
Phototherapy (Phototherapy) :

- Phototherapy is a non-invasive, effective and unconjugated bilirubin reduction It is a simple and less expensive method to do. In it, light waves are converted from unconjugated bilirubin to a water-soluble non-toxic form through photooxidation which is easily excreted from the blood.
- Phototherapy should be started when the bilirubin level reaches 15 mg/dl and in preterm babies when it is 5 mg/dl or more.
- The blue wavelength is 450-460 nm. The tubelight and plexiglass are covered with a shield. The phototherapy unit is fixed on the crib or incubator. Fluorescent or halogen lights can also be used.
Nursing Responsibilities in Phototherapy:
- The baby should be completely exposed to the light source.
- The light should be kept at a distance of 45 cm.
- The child’s eyes and genital area should be properly covered.
- Advise the mother to provide frequent breast feeding to the child during phototherapy.
- Extra fluids if needed Provide feeding through intravenous infusion or nasogastric tube. The child’s position should be changed every two hours and in a way that allows maximum light exposure. The child’s temperature, pulse, and respiration (TPR) should be checked every two hours. Continuously monitor the child for any side effects of phototherapy and serum bilirubin levels should be measured every 12 hours. –>
- Phototherapy is indicated when serum bilirubin levels reach 10 mg/dl. Discontinue.
- Most phototherapy should be continued for 2-3 days.
- 6 hourly/day and,
- 2 hourly 3 times / day.
- Involve the mother in the baby’s care.
- Proper explanation, instruction and emotional support to parents are important.
Complications and side effects of phototherapy:
Immediate problems:
- Dehydration, hypothermia, hyperthermia,
- Loose stool/green stool,
- Bronze Baby Syndrome (Bronze Baby Syndrome is a condition in which dark green brown pigmentation is seen in the child’s skin, mucous membranes and urine after providing phototherapy.)
- Skin rashes,
- Hypocalcemia etc. are seen.
Long-term Problem:
- Disturbances occur in endocrine and sexual maturation.
- Damage to the testicles.
- Skin cancer (rare condition) occurs.
Exchange blood transfusion (EBT):

- This is an effective method to remove circulating bilirubin and antibodies in patients with Rh incompatibility. In Rh+ Ve babies with direct comb test positive, the syndrome develops rapidly and anemia also increases due to low Hb%, in which case exchange blood transfusion is indicated.
Nature and amount of blood for exchange blood transfusion:
- Rh isoimmunization – Use Rh negative, ABO compatible blood.
- ABO incompatibility: Use “o” group Rh compatible blood.
- Prefer fresh blood with an age of less than 72 hours. And its content is 160-180ml/kg for an exchange transfusion. It replaces 80 – 90% of fetal blood.
Procedure:
- Exchange Blood Transfusion (EBT) is performed by an expert team in a well-equipped setup, maintaining strict aseptic technique.
- This process is Slow and continuous for up to one hour.
- Keep the baby in a left and well restrained position. Stomach contents should be aspirated. Vital signs should be monitored properly.
- 10 ml of blood should be withdrawn at one time and 10 ml of blood should be transfused.
- Toxic effects, shock, embolism, thrombosis Steps should be taken to prevent acidosis and cardiac failure.
- The recording of the procedure includes the time of initiation, how much blood was withdrawn in each cycle and in what amount, how many cycles were given, and the total exchange amount in the blood.
- After the procedure, the bilirubin level and Hb% of the blood should be done. Post-transfusion antibiotics should be given And observation for signs of complications is important.
Complications after exchange blood transfusion:
Immediate complications:
- Cardiac failure,
- Air embolism,
- Acidosis,
- Tetany,
- Sepsis,
- Hyperkalemia,
- Umbilical or portal vein perforation,
- Hypoglycemia,
- Thrombocytopenia.
Delayed complications:
- Extrahepatic Portal Hypertension,
- Portal Vein Thrombosis,
- HIV,
- Hepatitis B&C Infection,
- Uncertain Colitis etc.
Hemorrhagic Diseases of the Newborn
Definition
- Hemorrhagic disease is a syndrome characterized by spontaneous internal and external bleeding, usually due to hypothrombinemia and low levels of vitamin K-dependent coagulation factors (5, 7, 9, 10), which is called hemorrhagic disease of the newborn. It is usually seen between the 2nd and 5th day of life but if treated early, blood values can return to normal within a week. Prevalence: It is most commonly seen in preterm and breastfed babies (breast milk contains very little vitamin K). is).
Symptoms and Signs:
- Hematemesis and melena may occur due to hemorrhage in the alimentary tract.
- Bleeding from the umbilical cord stump may occur.
- Urinary Hematuria may occur due to track hemorrhage.
- Sometimes cutaneous ecchymosis is also seen.
- It may also increase the risk of bleeding after any operative procedure or from the injured site.
- It may cause the baby to become anemic and sometimes a condition of shock may also occur.
- In some cases, bleeding may also occur from the nose and vagina. is.
Investigation:
- It includes prolonged prothrombin time and partial thromboplastin Time is observed.
- Low platelet count is observed.
Prevention:
- Intramuscular administration of Vitamin K 1 mg I/M to the child immediately after birth or administration of 2:5-5 mg to the mother at least 2 hours before delivery.
Treatment and Nursing Care:
- Vitamin K: Intramuscular administration of 1-2 mg and if necessary, repeat after 24 hours.
- If shock condition has arisen due to blood loss, then compatible whole blood transfusion at 15-20 ml/kg/ body weight should be administered over 4-6 hours.
- Fresh frozen plasma can also be used in alternative treatment.
- In chronic anemia, appropriate liquid iron preparations with 20-30 mg elemental iron content may be prescribed along with medication.
- Local application of pressure dressings with coagulants such as thrombin and fibrin is valuable at accessible sites.
- It is given in 2 divided doses daily.
- Avoid unnecessary handling of fits.
- If If there is a condition of hematemesis, the child is placed in a head-down position with the head turned to one side.
