ENGLISH-NEW MIDWIFERY GNM TY UNIT 12 Obstetrics Operations
Unit: 12 Obstetrics Operations:

Induction Of Labor:

- Induction of labor means that after the period of viability of the fetus and before the spontaneous labor process starts, usually artificial initiation of uterine contractions is done in which uterine contractions are started for vaginal delivery through medical, surgical or both combined methods. This is called induction of labor. is.
Purpose of induction of labor:
- Induction is done when continuation of pregnancy may pose a risk to the health of the mother or fetus. Therefore, in cases where it is necessary to ensure the safety of both, induction is indicated.
Indications of Induction of Labor:
- Induction of labor is required when there is any deviation in the normal physiological process of childbirth.
Maternal Indications:
- Prolonged pregnancy,
- Pre-eclampsia and eclampsia,
- Maternal medical complications such as diabetes mellitus, chronic renal failure, cardiac disease, hypertension, cholestasis, postmaturity, intrauterine death,
- Intrauterine growth retardation,
- APH especially abruptio Placenta,
- Polyhydramnios associated with maternal distress,
- Oligohydramnios,
- Premature rupture of membranes,
- Congenital malformation in fetuses Due to.
Fetal Indications:
- Intrauterine growth retardation (IUGR) due to chronic placental insufficiency,
- Intrauterine fetal death,
- Rh-isoimmunization,
- Unstable ly,
- Congenital, malformation of the fetus.
Contraindications:
- Contracted pelvis,
- Cephalopelvic disproportion (CPD),
- Malpresentation,
- Previous classical cesarean section or hysterotomy,
- Vaginal bleeding,
- Vaza Previa,
- Placenta Previa,
- Active Genital Herpes Infection,
- High Risk Pregnancy, Heart Disease, Pelvic Tumor,
- Obstetrics and Medical Complications with Elderly Primi Gravida,
- Umbilical Cord Prolapse,
- Or cord presentation,
- In cervical carcinoma,
- In HIV-positive women not taking highly active antiretroviral therapy
- In cervical carcinoma.
Risks due to induction of labour:
Mother:
- Psychological upset,
- Tendency to prolong labour,
- Increased need for analgesics Occurs,
- Operative interference,
- Morbidity.
Fits:
- Iatrogenic prematurity,
- Hypoxia,
- Uterine dysfunction,
- Prolonged labor,
- Operative delivery.
Method of Induction of Labor (Method of Induction of Labor) :
1.Medical,
2.Surgical,
3.Combined.
Medical:
For medical induction, prostaglandins PGE2 (prostaglandin), PGE1 (mizostol), oxytocin or mifepristone are used.
For medical induction, prostaglandins (PGE2): Affect locally contiguous cells. This causes biomaterial contraction. But (PGE2) is responsible for survival ripening while PGF2 is responsible for myometrial contractions. PGE2 dinoprostone intracervical application is used for cervical ripening. It is repeated after 6 hours, 3 to 4 doses can be given if necessary. After application, the patient should remain in bed for 30 minutes and uterine activity and fetal heart rate should be monitored.
Misoprostol (PGE1): Currently used transvaginally or orally. 25 mg vaginally every four hours is used for cervical ripening and labor induction. A total of 6-8 doses can be given.
Oxytocin: is an endogenous uterotonic. It stimulates uterine contractions. It is most effective when the cervix is ripe. It is given by intravenous infusion.
Mifepristone: It is a progesterone receptor antagonist and blocks progesterone and glucocorticoid receptors. It is used for vaginal cervical ripening and labor induction.
Surgical induction:
1) Artificial Rupture of Membranes (ARM),
2) Stripping the Membrane
Low Rupture of Membranes (LRM):
Procedure: The membrane below the presenting part and above the internal OS is ruptured and a small amount of amniotic fluid is drained. It is done in the labor room or operation theater with full aseptic precautions by emptying the bladder and placing the fetus in the lithotomy position using Long Couture forceps or amnio hook. After that, a sterile valvular pad is placed and antibiotics are administered. After rupture of membranes, the color of the amniotic fluid, the station of the cervix, cord prolapse, and fetal heart rate should be assessed.
Indications: Antepartum hemorrhage (APH),
Hydroamnios, severe preeclampsia, eclampsia.
Contraindications: Intrauterine fetal death, maternal AIDS, active genital herpes infection.
Advantages:
Blood pressure in pre-eclampsia and eclampsia It reduces,
Maternal distress in hydroamnios is reduced,
Leaked amniotic fluid can be assessed,
Internal fetal monitoring can be done,
Uterine cavity is assessed,
Blood sample is taken from the fetal scalp,
Catheter is placed to measure intrauterine pressure,
Bleeding is controlled in antepartum hemorrhage (APH) and
Tension is reduced in placental abruption and initiation of labor.
Risks: Cord prolapse, excessive amniotic fluid escape, placental abruption, traumatic amnionitis, etc.
Striping the membranes: This procedure is useful for cervical ripening, before ARM, and for induction of labor. Stripping of the membranes involves the digital separation of the chorioamniotic membrane from the wall of the cervix and lower uterine segment. This releases endogenous prostaglandins from the membranes and decidua. This method is simple, safe and beneficial. Its criteria include the fetal head being applied to the cervix and the cervix being dilated to the extent that the examiner’s finger can reach it.
Mechanical: Dilator
Releases prostaglandins from the membrane a decidua for labor induction and survival ripening.
Transcervical balloon catheter (Follis catheter): Extra-amniotic saline infusion is performed for cervical repair.
Combined Method:
This method uses both medical and surgical methods. Its advantages include being more effective than a single procedure, reducing the induction-delivery interval, thus reducing infection and reducing the observation period.
Manually Removal of Placenta (Manually Removal of Placenta):
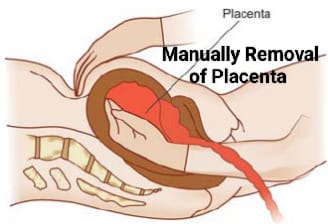
- When the placenta is not delivered for 30 minutes after the birth of the baby and the placenta remains in the uterine cavity, then in this condition there is a need to remove the placenta manually.
- This procedure is done under general anesthesia and in emergency if there is no anesthetist, by giving deep sedation.
- First of all, the patient is provided with lithotomy position, the operated area is painted and the operated area is covered with sterile linen.
- Catheterize the bladder using aseptic measures.
- Then hold the umbilical cord tightly with the left hand and make a cone shape with the right hand, dip it in an antiseptic solution and introduce it into the vagina in the direction of the cord. When the placenta is located, release it so that the fundus can be supported from the abdomen with the left hand.
- Guide the finger movements by applying steady pressure to the fundus with the abdominal hand until the placenta is completely separated from the uterine cavity.
- After reaching the margin of the placenta, separate the entire placenta with a slicing movement of the fingers between the placenta and the uterine wall.
- When the placenta is completely separated, the cord is pulled out by traction with the left hand and the right hand is used to support the placenta. Introduce and check properly for any retained bits of placenta.
- Then give intravenous methazine 0.2 mg and continue to massage the uterus with the left hand and remove it from the uterus with the right hand. Inspect for cervical-vaginal canal injury.
- Then check for completeness of placenta and membranes and whether the uterus is hard and contracted.
Version:
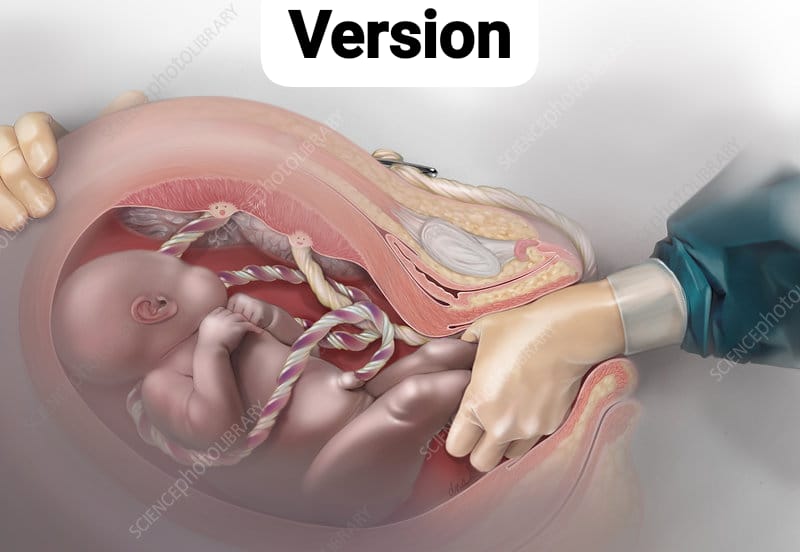
Definition:
- Version is a manipulative procedure to change the position of the fetus or to bring the fetus to a favorable position in the lower pole of the uterus. When the cephalic pole is brought into the lower pole of the uterus, it is called cephalic version and when the podelic pole is brought into the lower pole of the uterus, it is called podelic version.
Types (type) :
1)Spontaneous,
2)External,
3)Internal,
4)Bipolar
1)Spontaneous version: In this type, the version occurs automatically and is more common in multiparas. About 55% of the versions occur spontaneously after 32 weeks of presentation and about 25% after 36 weeks.
2) External version: In this type of version, the favorable cephalic or podelic pole is brought into the lower pole of the uterus by manipulation only from the outside (on the abdomen).
ECV (External Safelike Version):
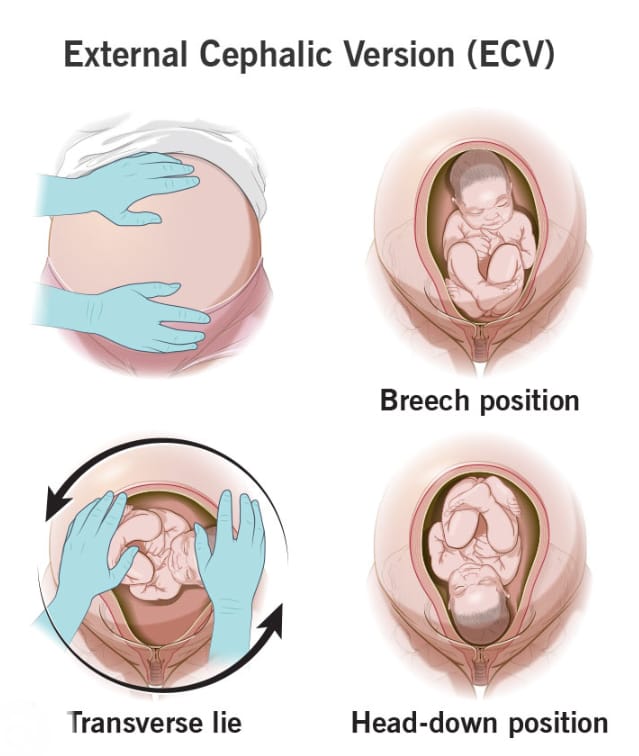
In the external cephalic version, the cephalic pole of the fetus is brought into the lower pole of the uterus.
Advantages:
- The incidence of breech presentation and breech delivery at term can be reduced is.
- Cesarean delivery can be reduced.
- Maternal morbidity rates associated with cesarean or vaginal breech delivery can be reduced.
- The risk of fits in vaginal breech delivery can be reduced.
Contraindications:
- Antepartum hemorrhage (APH), hyperextension of the head, large fetus, major congenital anomaly, dead fetus, intrauterine growth retardation (IUGR).
- Multiple pregnancy, ruptured membranes, congenital malformations in the uterus, contracted pelvis, previous cesarean section, obstructed complications, rhesus isoimmunization.
Procedure (Procedure) :
- External cephalic version (ECV) should be done after 36 weeks, as doing it earlier increases the chance of reversion. Tocolytic drugs are given to keep the uterus relaxed during external cephalic version.
- Before the procedure, real-time USG is performed to confirm the diagnosis and volume of amniotic fluid and a non-stress test is performed to assess the well-being of the fetus.
- First, empty the bladder. Then provide the patient with a comfortable supine position. Then, keep the shoulders slightly elevated and flex the thighs. Then the position of the fetus’s back, presentation, limbs, FHS, etc. are checked.
- Then hold the podelic pole with the right hand and the cephalic pole with the left hand. Now the head and breech are turned in opposite directions until the lie becomes transverse, and the fetal heart sound (FHS) is checked again.
- After bringing the fetus into the transverse lie, change hands to cross, and intermittent pressure is given until the head reaches the lower pole of the uterus.
- After the procedure, the mother should be observed for 30 minutes and vital signs should be checked. Check the fetal heart sound (FHS) and non-stress test (NST) of the fetus. Check the mother for vaginal bleeding and rupture of membranes. Give Anti-D gammaglobulin 100 micrograms to Rh negative women.
- External version is easy in transverse lie. Its contractions include placenta previa and congenital malformations.
- External podalic version: External podalic version is performed when external cephalic version fails in transverse lie and the second baby is a twin.
Complications of external version
Premature rupture of membranes, premature labor, abruptio placentae, bleeding, true knot in the cord, or cord fetal part Amniotic fluid embolism and feto-maternal bleeding increase as it wraps around.
3) Internal Version:
In this type, versioning is done by introducing one hand into the uterus and placing the other hand on the abdomen. Internal version is always a podalic version and is completed with the extraction of the fetus.
Conditions for internal version: Full dilation of the cervix, adequate like amniotic fluid and live fetus.
Indications:
Internal version is rarely performed in singleton pregnancies. It is only indicated when the second baby is lying transverse in twins. However, in some cases such as when there is no facility for cesarean section and when there is transverse lie or cord prolapse, full dilation of the cervix, head high up and baby is alive, internal version is also performed in single pregnancies.
Contraindications:
Neglected obstructed labor.
Procedure:
- The first assessment of the fetus’s position, presentation, and heart rate is performed by an experienced obstetrician through abdominal palpation, vaginal examination, and transabdominal ultrasound examination. Internal version is performed under general or epidural anesthesia, i.e., the patient is first placed in the dorsal lithotomy position, painted with antiseptic, and then draping and catheterization are performed. If the podelic pole of the fetus is on the left side of the mother, then introduce the right hand and similarly if the podelic pole of the fetus is on the right side, then introduce the left hand. Make a cone shape of the hand and reach the podelic pole in such a way that its back side comes against the uterine wall.
- Take the hind leg to the breech and thigh and hold the cephalic foot.
- Now give steady traction to the leg, bring it downwards and push the cephalic pole upwards from outside with the other hand.
- Put one leg below the After bringing the second leg towards the side, there is no difficulty in delivering it and delivery is completed by breech extraction during uterine contractions.
- After delivery, check for uterovaginal canal injury or uterine rupture.
Complications:
- Maternal: Placental abruption, Rupture of uterus, and morbidity rate increases.
- Fetal risk: Asphyxia, cord prolapse, intracranial hemorrhage, high perinatal mortality.
4) Bipolar Version:

- In this method, by introducing one or two fingers into the uterus and the other hand The version is performed by placing the abdomen on top. Its indications include the involvement of low-grade placenta previa, dead, deformed or previable fits. In this, the cervix should be dilated to the size of eight to two fingers and the hand is pushed towards one iliac fossa and one leg is brought downwards.
Sterilization:
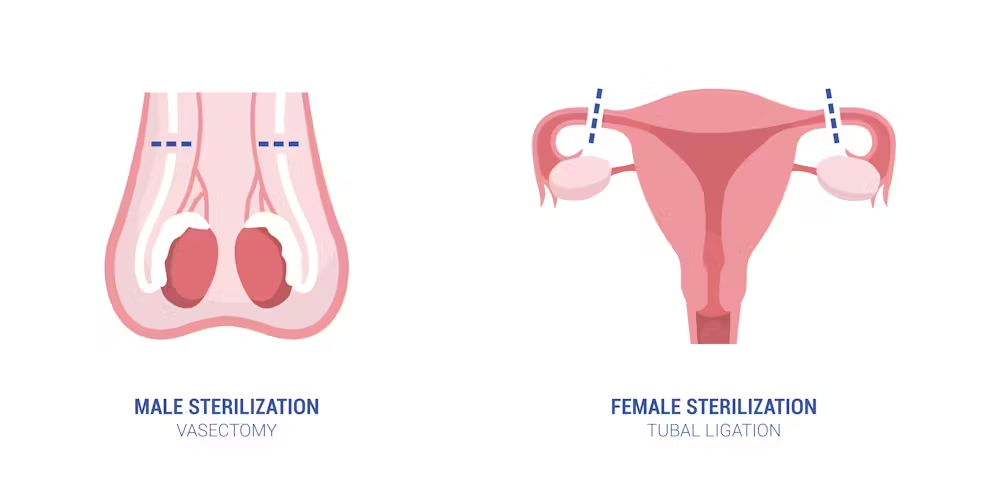
Permanent surgical contraception, also called voluntary sterilization, is a surgical method in which the reproductive function of an individual male or female is purposefully and permanently destroyed. Such as,
1) Male Sterilization: Vasectomy,
2) Female Sterilization: Tubectomy.
1) Male Sterilization: Vasectomy:
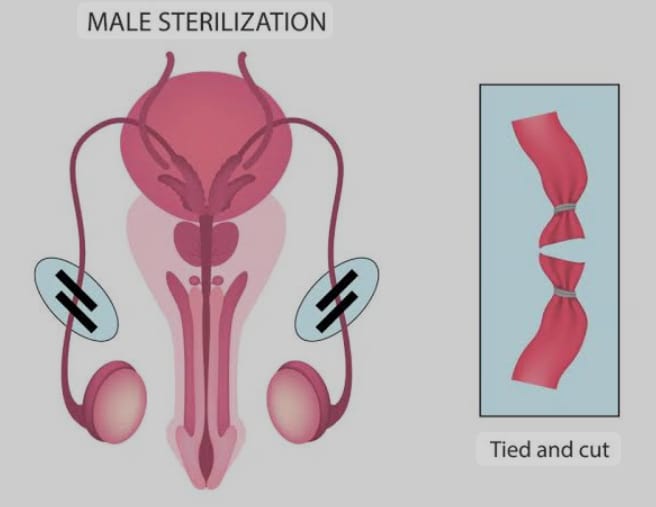
- This is a permanent sterilization operation performed in the mail in which both sides of the vas deferens are resected and its ends are cut and ligated.
Advantages:
- Its operation technique is simple and complications are less.
- Its operation can be done as an outdoor procedure in camps and villages as well.
- The failure rate is 0.15% and the success chance of reversal anastomosis operation is 50%.
- Equipment, hospital stay, doctor training are all relatively inexpensive.
Deadvantages:
- Additional contraception is required for 2-3 months after the operation until the semen is free of sperm.
- Frigidity or impotence may occur, which is mostly Psychological.
- Non-Scalpel Vasectomy (NSV): This operation is provided under local anesthesia in which the vas is caught with specially designed forceps, then the stretched skin over the vas is punctured with the sharp point of the forceps without using a scalpel and then the vas is dissected. There is no need for sutures and the time is also less. There is a fast recovery but the skill of the surgeon is required to a greater extent.
2) Female Studialarization / Tubectomy:
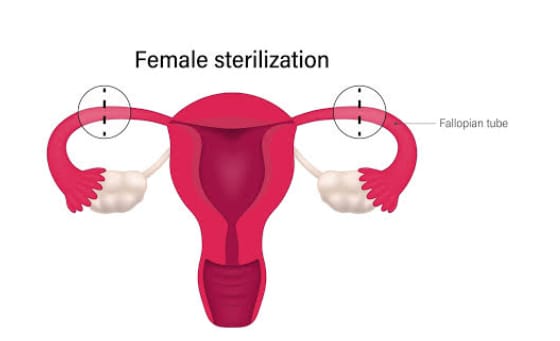
- Tubectomy is a method of permanent sterilization performed in females. It involves cutting and then ligating the fallopian tubes to block the passage of the ovum.
Time of Operation:
- Postpartum sterilization: If the patient is healthy, tubectomy can be performed 24-48 hours after delivery.
- Internal sterilization:When the operation is performed at a time other than childbirth and abortion, it is called internal sterilization.
- Traditional tubectomy:This method is also known as abdominal tubectomy. This method is usually performed under general anesthesia or spinal anesthesia. It is performed in which an incision is made in the lower abdominal area and then the fallopian tube is cut and tied or clamped. After that, the layers of the abdomen are closed. This usually works as a permanent contraceptive that blocks the path of the ovum, which usually requires hospitalization for five to six days and the sutures can be removed after the 5th day after the operation.
Post-operative advice:
- Heavy weight should not be lifted for 6 weeks.
- Avoid heavy work for three months.
- Sexual activity can be resumed 4 weeks after the operation.
- Minilap operation: This is a minor form of abdominal tubectomy which is usually done under local anesthesia in which a 2.5 to 3 cm incision is made in the lower abdominal area and then parts of the fallopian tube are cut and clamped and then the layers of the abdomen are sutured again. This method is very safe and effective. This procedure can be performed generally at the Primary Health Center (PHC) level and also in the community. This procedure acts as a good technique for postpartum sterilization.
Advantages:
- This technique is usually suitable for postpartum sterilization.
- This procedure is usually less traumatic than abdominal tubectomy.
- It usually has fewer complications.
- Laparoscopic sterilization: This laparoscopic sterilization technique is a very popular procedure for female sterilization in which the fallopian tubes are blocked or the fallopian tubes are closed. A rubber ring is placed so that the ovum cannot reach the uterus. Before inserting the laparoscope, the abdomen is expanded with carbon dioxide, nitrous oxide or air. Then the laparoscope is inserted through the abdomen and the tube is visualized. Then, when the tube is visualized, the fallopian ring is placed in the fallopian tube or a clip is applied, due to which the tube is blocked. Then the laparoscope is removed and the layers of the abdomen are sutured and closed.
- The incision is very small and the scar is also small.
- It takes less time for the operation. is required.
- This is a less expensive procedure.
- It has minimal complications.
- Hospital stay is short, usually up to 48 hours.
Disadvantages:
- It is not usually performed in post-partum patients.
- It is not suitable for patients with medical conditions such as heart disease, respiratory disease, diabetes and hypertension.
- Complications:
Pain,
Stretching,
Irregular menstrual cycle,
Local infection.
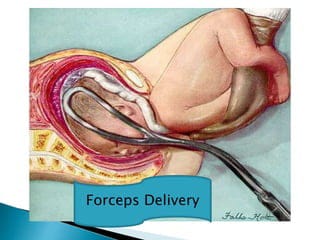
Forceps Delivery :
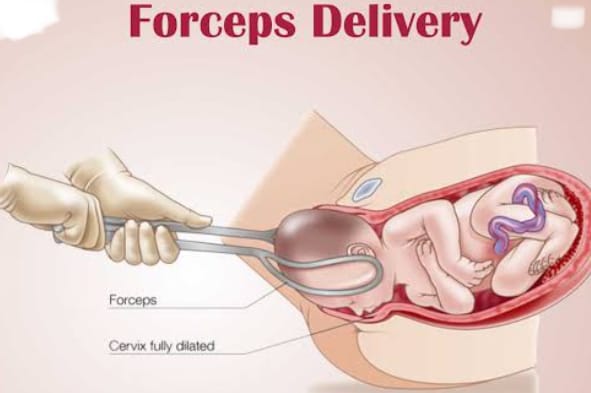
- The obstetric forceps were invented in England in the 11th century by doctors of the Chamberlain family. Obstetric forceps are a pair of instruments, and they are specially designed to extract the fetal head.
Simple Classification:
1)Conventional Traction Forceps
Short:
Wrigley’s, Simpson’s Short, Elliot. Short forceps are usually used.
Long:
a) E.X. without axis traction. Simpson’s Long, Elliot’s Long, Das Forceps.
b) With axis traction E X. Milne Murray, Barnes- Neville, Hague-Ferguson.
2) Rotational forceps: Killand, Mulgaocar, Barton.
3) Special forceps: Piper’s forceps for the coming head in the breech, LSCS Bhate Hale forceps, New Rubberized Forceps (Greenberg).
Classification or Types of Forceps Application:
1) High forceps:
- Involves the application of forceps to the head of the fetus where the biparietal diameter has not passed through the pelvic inlet plane (non-engaged head).
- In high forceps, the head is not engaged.
2)Mead forceps operation:
Involves the application of forceps where the biparietal diameter has passed through the plan of the inlet but has not passed the level of the ischial spines. It involves the fetal head being engaged but the station is above +2.
It also has two subtypes:
1) High Mid,
2) Low Mid.
1) High Mid:
The biparietal diameter has passed through the plane of the inlet but remains above the level of the ischial spines. Manual rotation is performed using forceps, an example of such a forceps operation. is.
2)Low Middle:
The biparietal diameter has passed through the plan of the inlet and is up to the level of the ischial spines. Therefore, the lower pole is below the level of the ischial spine.
3)Low forceps operation:
When the biparietal diameter of the fetal head has passed the ischial spine and forceps are applied, it is called low forceps operation.
Fetal skull +2 cm station or more, but has not reached the pelvic floor.
Rotation 45 degrees or less and 45 in anterior or posterior position °.
4) Outlet forceps:
It is a variation of the low forceps operation, where the forceps are applied to the head of the fetus on the perineum and the head is visible in the introitus between contractions. The sagittal suture should be in the anterior-posterior diameter of the outlet. Thus, while all outlet forceps are low forceps, not all low forceps are outlet forceps operations.
Outlet forceps should be performed with the scalp visible above the introitus, without separating the labia. The fetal skull is above the pelvic floor, the sagittal suture is in a direct antero-posterior diameter or right/left occiput anterior or posterior position, the fetal head is above the perineum, and the rotation is greater than 45°.
The following are the fundamental parts of the forceps:
Blades: Each blade is usually fenestrated but may also be solid. The fenestrated blade is light for rotation and its grip is good for traction. Each blade has two covers.
1) Cephalic curve: Its cover is flat and fits over the fetal head.
2) Pelvic curve: Its covered part is on the edge and fits over the maternal pelvis.
Shank: The part between the blade and the lock is called the shank and can be parallel or overlapping.
Lock: Lock is also available in the forceps.
Handle: This is a long metal rod with finger grips on the outside and traction forceps have an axis traction mechanism.
Measurement:
- Cephalic Covered Radius: 11.5 cm,
- Pelvic Covered Radius: 17.5 cm,
- Distance between two blades: Maximum 8.5 Cm and Minimum: 1.5 to 3.5.
- Shank: 6.25cm.
- Handle: 12.5cm.
Functions of forceps
- Traction: Approximately 20 kg of traction force is required in primigravida and approximately 13 kg of traction force is required in multipara.
- Rotation: Killand forceps are best for rotation of the head. But simple long forceps can also be used.
- Compression: Forceps are the first type of lever. If the forceps are correctly placed in a biparietal, bimalar placement, their impact on the cranium is reduced.
- Stimulation of uterine action: Traction should be given only when uterine contractions are present.
- Protective cage: The protective cage acts as a protective cage to protect the premature baby’s head from the pressure of the birth canal.
- The risk of sudden decompression is lower in breech delivery after the baby’s head has come down.
Indications
- Maternal: The second stage of labor is prolonged when the mother is unable to push down the baby and to reduce the strain on the mother in some obstetric and medical conditions. In obstetrics, pregnancy induced hypertension, eclampsia.
- Medical: Valvular heart disease, pulmonary tuberculosis, other lung diseases, liver and kidney diseases, general debility, anemia, diabetes etc.
- Fetal: Fetal distress or failure to progress in the second stage of labor, malrotation, large fetuses, full dilation of the cervix with cord prolapse, postmaturity, and after coming head in breech.
Contraindications:
- Incomplete dilation of the cervix, moderate or severe degree of contracted pelvis, malpresentation, contracting ring, pelvic tumor.
Pre-requisites:
- Vertex presentation, face presentation, after coming head (favorable presentation) in China anterior or breech delivery, fit head +2, K + 3 station or 0/5 palpable above symphysis pubis (engaged head), adequate pelvis, full dilation of cervix, ruptured membranes, empty bladder and rectum, adequate anesthesia, episiotomy and facilities for resuscitation of the baby are the primary requirements.
Low Forceps Application:
- First consult the patient and his family members.
- Provide the patient with proper lithotomy position. Then painting and draping.
- Then administer proper anesthesia.
- Empty the bladder through a simple catheter.
- Properly introduce the IV line to the patient and keep the IV line properly patent.
- Do an internal examination and assess the cervix, membranes, and pelvic outlet.
Steps of Operations:
- First, separate the right and left blades by articulating the blades in front of the patient. Then, introduce the left blade first. Hold it vertically in the left hand and then introduce two fingers or the entire right hand into the vagina and depress the posterior vaginal wall. Introduce the blade posteriorly into the hollow of the sacrum. Push with the thumb of the right hand. Push it upwards with the guidance of the fetal head and internal fingers. Move the handle downwards and backwards.
When applied correctly, the blades will be on the parietal eminence, the shank in contact with the perineum and the superior surface of the handle will be directed upwards. Then rotate the blade with the guidance of the internal fingers and bring it to the left side of the maternal pelvis. - Now change hands and hold the right blade in the right hand and bring it in front of the left blade in the same manner.
- Then depress the blade and lock it, if there is proper application then there is no problem in locking.
- After checking the proper application of the blades, give steady but intermittent traction during the contraction. Depending on the station of the head in the low forceps, push the head in a downward and backward direction until the head comes to the perineum, then push horizontally towards the operator until the crown is reached. After this, slowly move the head in an upward and forward direction towards the mother’s abdomen to deliver it from extension. Then remove the blades one by one, removing the right blade first.
- After head delivery, follow the same procedure as for normal delivery. And give the patient Inj. Methagin 0.2 mg after delivery of the anterior shoulder. Repair the episiotomy and check for tar and take next steps.
Complications:
- Maternal: Injury to the birth canal, bowel, bladder and in rare cases, bone may also be injured. Hemorrhage, infection, obstetric shock, uterine rupture, and anesthetic complications may also occur.
- Fetal: scalp injury, facial nerve injury, cephalohematoma, birth asphyxia, intracranial hemorrhage, linear or depressed skull fracture.
Nursing Interventions:
- When the obstetrician decides to collect the forceps and prepare for their application.
- Before applying the forceps, check the fetal heart rate record and report.
- Provide psychological support to the patient and inform them about the procedure.
- After applying the forceps, check the fetal heart rate record and report before applying traction again.
- After the procedure, the mother and baby Observe for signs and symptoms of complications.
- Record the forceps delivery and monitor the vital signs of the mother and baby.
- Advantages of delivery
- Forces are more effective when there is a need for rapid delivery, such as fetal distress.
- Forces are more effective when moderate traction is needed.
- It is safer for premature babies because the fetal head remains inside the protective cage.
- It is useful in cases where Ventos is contraindicated, such as after coming head in anterior face or breech presentation.
- Less incidence of neonatal scalp trauma, hemorrhage, jaundice or cephalohematoma than Ventos.
- More successful in vaginal delivery than Ventos.
- If the vacuum is not maintained in the ventouse, the problem of the cup falling off does not occur after applying the blades correctly.
- Forces for outlet, mid-cavity or rotational delivery are available.
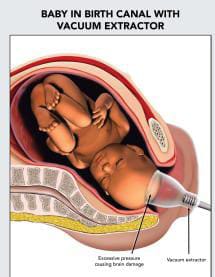
Vacuum Extraction (Wintos/Vacuum Extractor) :
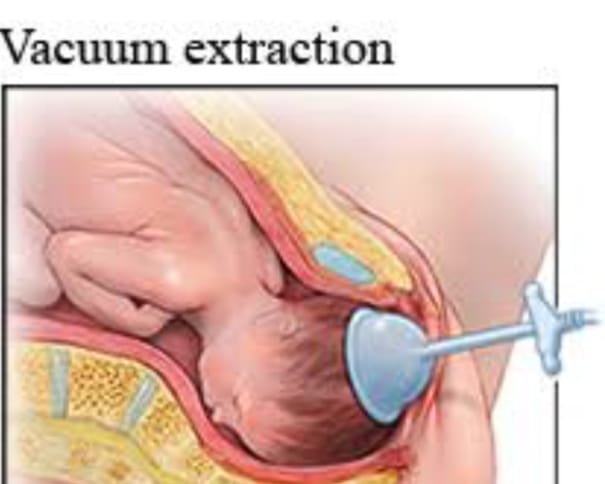
- Ventos was introduced by Malmstorm in 1956. Ventos is an instrumental device designed to assist delivery by creating a vacuum between the device and the fetal scalp.
- It involves the following components:
- 1. Suction cups made of metal in 4 sizes (30, 40, 50, 60 mm).
- 2. Vacuum pump with a manometer attached (modern vacuum extractors have an electrical pump).
- 3. Traction rod device.
- 4. In the center Rubber tubing is available with the chain.
Parts Of Instruments:
- Parts involve suction cups-4 sizes (30, 40, 50, & 60 mm) vacuum generator and traction tubing.
- Initially metal cups Used but soft cups, silk cups (silicone rubber/disposable plastic cups) provide better attachment to the fetal scalp. These cups can be folded and introduced into the vagina without difficulty and have a low chance of trauma and injury while rigid plastic cups are safe and effective for rotational delivery.
- The cup is connected to the pump by a thick-walled rubber tube which is used to evacuate the air.
- Vacuum is created by a hand pump or an electric pump.
Indications (Indications) :
- Attachment of the pelvis with deep transverse arrest.
If it is the second baby of twins and the head is high and the descent is delayed.
Fetal distress or prematurity.
In the condition of uterine inertia or primary cervical dystocia in the first stage. - Symphysiotomy As an adjunct.
- In conditions where the second stage of labor is prolonged.
- In rotation of the caput from posterior to anterior.
Contraindications:
- Presentation other than vertex (such as face, brow, breech, etc.)
Face presentation,
Preterm birth (< 34 weeks), suspected fetal coagulation disorder, suspected fetal macrosomia (> 4 kg),
Unengaged fetal head,
cephalopelvic disproportion,
fetal bleeding disorder,
scalp avulsion or sub-aponeurotic hemorrhage are more likely to occur prematurely. - Precautions: Only basic necessities like forceps application It can be applied even if the cervix is less than fully dilated and the head is not rotated. Other conditions include vertex presentation, term delivery, fetal head at least 0 station, and no more than 2/5 of the symphysis pubis should be palpable. Uterine contractures are helpful but not necessary. Keep obstetric forceps ready for use.
Procedure:
- Advise the patient to assume the proper lithotomy position.
- Maintain proper aseptic technique or precautions while handling the patient.
- Advice on proper bladder emptying.
- Perform perineal infiltration or pudendal block depending on the station of the fetal head.
- Perform vaginal examination.
- Application of the cup
- Select the largest possible cup according to the dilation of the cervix.
- The cup is in the other hand Retract the perineum with your fingers and introduce.
- Keep the cup close to the occiput (flexion point) of the fetal head so that the knob of the cup is towards the occiput. This will flex the head and the knob shows the degree of rotation.
- Apply betadine antiseptic solution on the rim of the Malstrom metal cup. Then introduce a vacuum of 0.2 kg/cm² with the pump for two minutes.
- Check to see if cervical or vaginal tissue is in the cup.
- Create an effective vacuum of 0.8 kg/cm² for 10 minutes at a pressure of 0.1 kg/cm².
- The scalp is sucked into the cup to produce an artificial caput succedaneum.
- It disappears in a few hours. It is done.
Principles of traction:
- The traction cup should be at a right angle and should be in sync with uterine contractions. If descent does not occur even after three pulls, abandon operative vaginal delivery. Traction should not be given for more than 30 minutes.
- After the head is delivered, open the screw release valve and remove the vacuum. and release the cup, then complete the delivery as per normal procedure.
Complications:
Maternal:
- Usually the injury is minor, but the injury to the soft tissues such as the cervix or vagina Can occur.
- Failure rate is high.
Neonate:
- Superficial scalp abrasion and cephalohemorrhage, intracranial hemorrhage, retinal hemorrhage, jaundice etc.
Advantages:
- It is easy to use and requires less anesthesia.
- Can be used even if the cervix is less than fully dilated. But in modern obstetrics it is applied after full dilation.
- Ventos is used in unrotated or malrotated heads. It helps in autorotation.
- Forces do not occupy space like blades.
- The traction force is (10 kg), which is less than forceps and due to the safety factor, the cup comes out due to vacuum break due to high pressure.
- If applied correctly, maternal tissues It does not cause injury. It is the instrument of first choice because it reduces perineal injury.
- Postpartum maternal discomfort is less than forceps.
Difference Between Forcep Delivery and Vacuum Delivery (Difference Between Forcep Delivery and Vacuum Delivery):
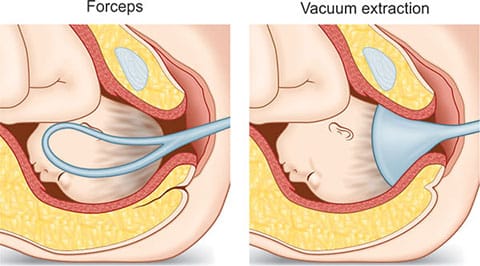
1)Forcespe Delivery:
- In forceps delivery, the baby is delivered using forceps.
- Obstetric forceps are a pair of instruments that are specially designed to bring out the fetal head.
- Maternal assistance is not required in forceps delivery.
- The equipment in forceps delivery is less complex.
- The incidence of cephalohematoma in forceps delivery is lower.
- Forces delivery is safer for premature babies because the fetal head remains inside a protective cage.
- Ventos delivery is performed using forceps in contracted cases such as anterior face or breech presentation.
- Used in non-safe presentation.
- Full dilation of the cervix is necessary for applying forceps.
- For application of forceps, the fetal head should be at the +2, +3 station.
- Adequate anesthesia is required for forceps delivery.
- In this, the blade of the forceps is on the parietal eminence, the sink is The superior surface of the handle will be directed downwards in contact with the perineum.
- Forcespe delivery is associated with third and fourth degree perineal lacerations.
- The blades of the forceps occupy the space.
- Maternal tissues are injured.
- It consumes less time and enables quicker delivery in conditions like fetal distress.
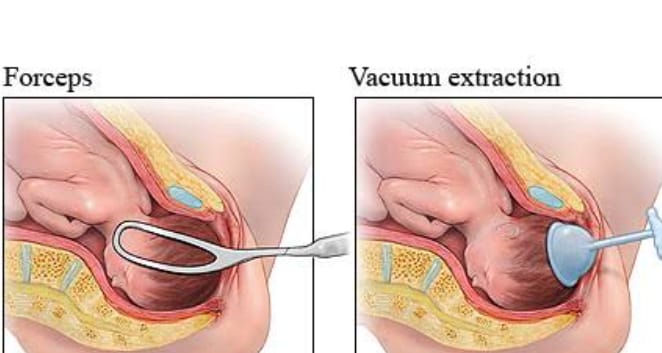
2) Vacuum delivery:
- In a vacuum delivery, the baby is delivered using a vacuum.
- A vacuum is an instrumental device designed to assist delivery by creating a vacuum between the device and the fetal scalp.
- A vacuum delivery requires minimal maternal assistance.
- It can be performed with minimal expertise.
- It may have a higher incidence of cephalic hematoma.
- It is contraindicated in premature babies because the fetal head is soft.
- It is contraindicated in presentations other than vertex (face, brow, breech).
- It is not used in non-cephalic presentations.
- Vacuum delivery is a procedure that can be performed even if the cervix is less dilated than full dilation. Can be used. But in modern obstetrics it is applied after full dilation.
- The fetal head should be at the zero station for vacuum application.
- Vacuum delivery requires less anesthesia.
- The cup of the vacuum is placed close to the occiput of the fetal head.
- Vacuum delivery is associated with solder dystocia and cephalohematoma.
- Vacuum does not occupy space like forceps blades.
- If vacuum is applied correctly, it does not injure maternal tissues.
- Vacuum has a high failure rate.
Destructive Surgeries:
Definition:
Destructive surgery is performed when the fetus has died during intrauterine life and this dead fetus is removed from the uterus. Destructive surgery is performed to reduce the bulk of the fetus to expel it from the cavity through the vaginal canal and for easy delivery.
Four types of surgeries can be performed, such as,
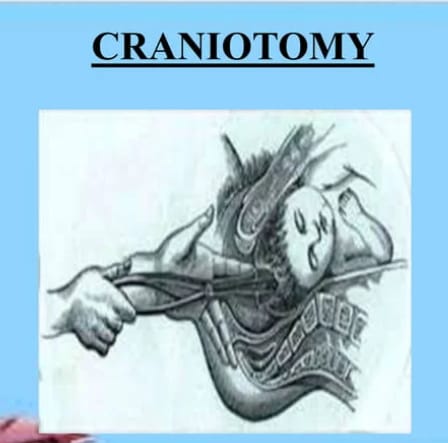
1. Craniotomy,
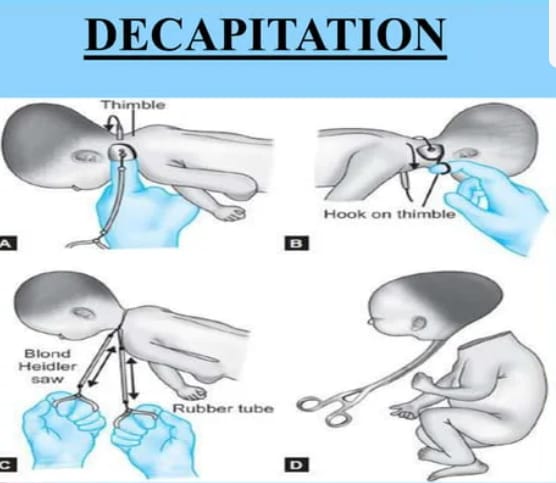
2. Decapitation,
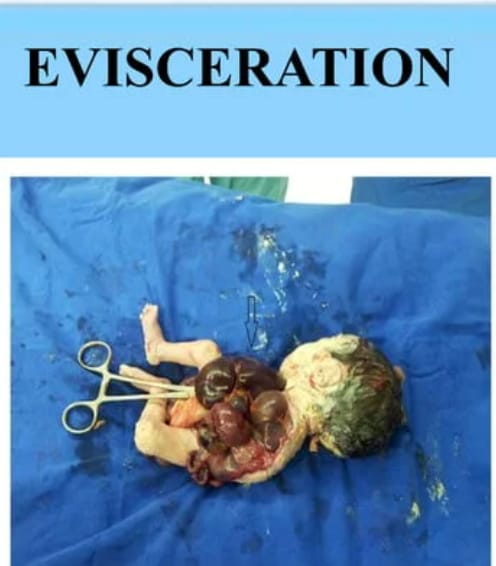
3. Evisceration,
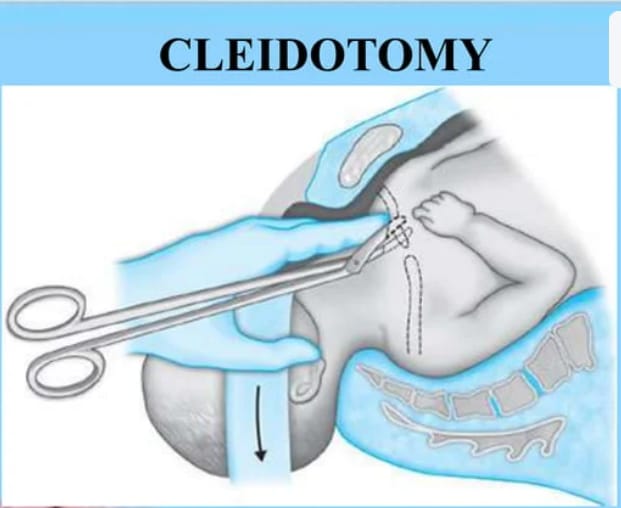
4. Clidotomy.
1. Craniotomy: The operation to expel the fetus from the uterine cavity by making a perforation in the head of the fetus and reducing the content is called craniotomy. This operation is performed when obstructed labor occurs due to dead fetuses in cephalic presentation.
2. Decapitation: In this type of operation, the fetal head is cut from the trunk and the delivery is completed with the extraction of the trunk. This operation is performed in the neglected solder presentation and interlocking heads of twins in dead fits.
3. Evisceration: The thoracic and abdominal cavities are opened and their contents are reduced and delivered. This operation is performed in neglected solder presentation and fetal malformation in dead fetuses.
4. Clidotomy: In this type of operation, part of the shoulder girdle is reduced by dividing one or two clavicles. It is performed only when there is shoulder dystocia with dead fitters.
Complications: Injury to the utero-vaginal canal and viscera (bladder),
Rupture of the uterus,
Postpartum hemorrhage,
Shock,
Pupillary sepsis, etc.
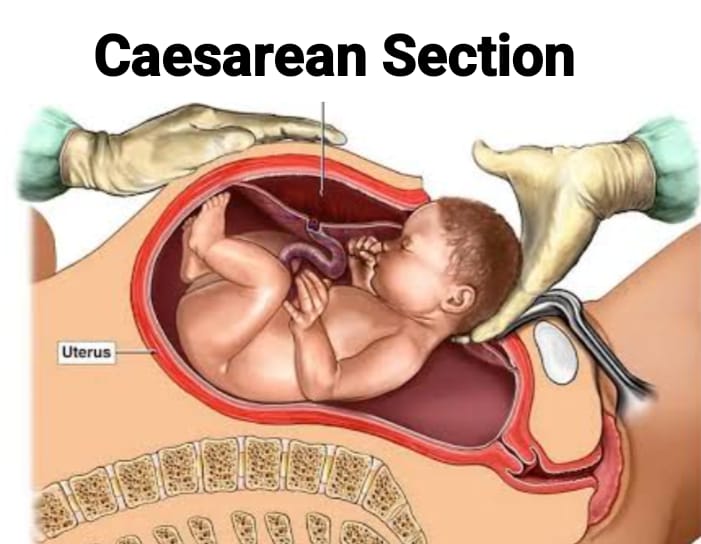
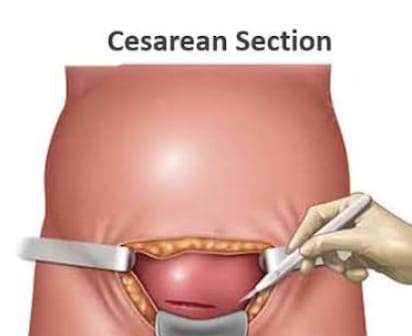
Caesarean Section:
Definition:
- After 28 weeks of pregnancy, an incision is made on the abdominal and uterine walls to deliver the fetus abdominally. This is called a cesarean section. If the operation is performed for the first time, it is called a primary cesarean section, and if it is performed in a subsequent pregnancy, it is called a repeat cesarean section.
Types :


1.Transperitoneal.
(a)Lower segment (most common),
(b) Upper segment (classical-rare)
2.Extraperitoneal.
3.Caesarean hysterectomy.
Indications for caesarean section:
Indications for caesarean section are divided into two categories:
1)Absolute, (in which vaginal Delivery not possible)
2) Relative (in which vaginal delivery is possible but there is a risk to the mother and baby)
1) Absolute, (in which vaginal delivery is not possible):
- Central placenta previa,
- Severe degree of contracted pelvis,
- Cervical or broad ligament fibroid,
- Vaginal atresia/obstruction,
- In advanced cervical carcinoma,
- Cephalopelvic disproportion,
- Obstruction due to pelvic mass,
- The fetus is dead.
2) Relative (in which vaginal delivery is possible but there is a risk to the mother and baby):
- cephalopelvic disproportion,
- contracted pelvis,
- Previous Cesarean Delivery,
- Fetal Distress,
- Abnormal Uterine Contractions,
- Large Fetus,
- Small Pelvis,
- Failed Induction,
- Antepartum Hemorrhage Like K, placenta previa, abruptio placentae.
- Malpresentation or abnormal lie (transverse lie).
- Bad obstetric history,
- Hypertensive disorders such as preeclampsia,
- Prolapse of umbilical cord,
- Elderly primigravida ,
- Medico- Gynecological Disorders:
- Chronic Hypertension,
- Chronic Nephritis,
- Diabetes,
- Heart Disease,
- Pelvic Tumor,
- Vaginal atresia,
- Carcinoma of cervix,
- Cervical dystocia.
Common indications of cesarean section:
1) Failure to progress in labor:
Prolonged labor in which The cervix does not dilate properly and the fetus does not descend properly into the birth canal, which necessitates a cesarean section.
2) Fetal distress:
A sign that the fetus is not able to tolerate labor properly, such as an abnormal fetal heart rate, indicates reduced oxygen supply to the fetus, which necessitates a cesarean section.
3) Malpresentation of baby:
When the baby is in a breech presentation (buttocks as the presenting part), transverse position, vaginal delivery is required. becomes impossible and a cesarean section is required.
4) Placental Abnormality:
Placenta Previa: In which the placenta is partially or completely implanted on the lower uterine segment, i.e. when the placenta is present as the presenting part.
Placental Abruptio: In which the placenta separates prematurely from the uterine wall, a cesarean section is also required.
5) Maternal health conditions such as genital herpes,
heart disease,
severe hypertension,
such as Condition .
6) Previous Cesarean Section: If a previous Cesarean Section has been performed, then the repeat Cesarean Section depends on the scar of the previous CS and the duration of the pregnancy.
7) Multiple Pregnancy: When there is a multiple pregnancy such as twins, triplets and depending on the presenting part and position of the fetus, there is a need to perform a Cesarean.
8) Umbilical Cord Prolapse: In which the umbilical cord slips down through the cervix, due to which there is a possibility of cutting off the blood supply to the fetus.
9) Maternal Request: In some cases, the mother herself selects a cesarean section due to any personal or psychological reason.
10) Emergencies During Labor: Complications during labor such as uterine rupture, severe bleeding, and maternal illness require immediate cesarean section to protect the health and safety of the mother and baby. Thus, in all these conditions, a cesarean section is required.
Time Of Operation (Time of Operation) :
1. Elective: When the operation is planned in advance during pregnancy and the best quality of obstetrics, anesthesia, neonatal resuscitation and nursing services is observed, it is called elective cesarean section.
2. Emergency: When the operation is performed during an acute period during pregnancy If performed in an obstetric emergency, it is called an emergency cesarean section. Its reasonable time from decision to start the procedure is 30 minutes.
Lower Segment Cesarean Section (LSCS): In this operation, the baby is delivered by making an incision on the lower segment through a transperitoneal approach. This method is not used in present day obstetrics unless it is specific.
Pre Operative Nursing Care:
- Obtain return permission for procedures, anesthesia, and blood transfusion.
- Prepare the operative area properly.
- Do not give premedication sedatives.
- Provide antacids, H2 blockers, or antiemetics, and antibiotic medications to the patient as ordered.
- Send for blood cross-match.
- Emptying the stomach through a stomach tube in an emergency.
- Checking the fetal heart sound repeat.
- Keeping a neonatologist available.
- Emptying the bladder through a Follis catheter in the perioperative period.
- General preoperative care such as physical and mental preparation.
- Advise the patient for Neil By Mouth (NBM).
- Obtain proper consent from the patient and his/her family members.
- Prepare the patient properly for cesarean section.
- Maintain all patient records and reports properly and provide proper psychological support to the patient.
Steps Of Operation:
Provide anesthesia to the patient.
Position of the patient: Provide the patient in a proper dorsal position. In some cases, to prevent the effect of venacaval compression, use wedges to tilt the left side to 15° until delivery of the baby.
Antiseptic painting: 7.5% povidone-iodine solution/Sevlon lotion After painting, drape with sterile towels.
Incision on the Abdomen: A vertical or transverse skin incision is made 3 cm above the symphysis pubis. There are some specific advantages to the transverse incision. As it is good for patient comfort, cosmetic value and reduces the chances of wound dehiscence and incisional hernia.
Packing: By introducing a Doyan retractor, the peritoneal or VT is packed off with arterial forceps on a large taped swab.
Uterine incision: A peritoneal incision is made followed by a muscle incision, the most common incision (90%) being the transverse one.
Delivery of head: If the membranes are intact Rupture. Suck blood mixed amniotic fluid with suction. Remove the Doyen retractor and deliver the head by hooking it with fingers and using Wrigley or Barton’s forceps.
Delivery of trunk: After the head is delivered, suck mucus from the mouth, pharynx and nostrils. After delivery of the solder, provide intravenous oxytocin 20 units or mithralazine 0.2 mg. And deliver the rest of the body slowly. Cut the cord by applying two clamps. Reintroduce the Doyen retractor. The time between uterine incision and delivery should be less than 90 seconds.
Removal of the placenta and membranes: The placenta will separate spontaneously and should be delivered with controlled cord traction. The uterine cavity should be explored and checked.
Suture of the uterine wound: The suture should be made in three layers of deep muscles, superficial muscles and fascia.
Remove the swabs placed in the uterine cavity and count them properly. Remove the blood clot and examine the tubes and ovaries.
Remove the retractor and check if the uterus is contracted before closing the abdomen.
Remove the blood clot from the vagina and place a sterile vulval pad.
Post Operative Nursing Care:
- First 24 hours (0 days):
- Properly assess the patient’s vital signs such as pulse, blood pressure during the first six to eight hours of observation.
- Record the amount of vaginal bleeding and the behavior of the uterus.
- Properly maintain the patient’s hydration status, including, Sodium Chloride (0.9%)/Ringer Lactated Continue the drip until 2-2.5 liters of solution is given.
- If blood transfusion is required in an anemic mother, prepare for it.
- Maintain the patient’s intake-output chart properly.
- Drugs such as inj. Oxytocin 5 units IM/IV (slow) or Methergine 0.2 mg IM, followed by prophylactic antibiotics and analgesics as ordered.
- Ambulation: If the patient’s general condition is good, he/she can sit up in bed and go to empty the bladder.
- Encourage the patient to move the legs and ankles and to anchor for deep breathing.
- Advise the mother to start breastfeeding within three to four hours when she is stable and her pain has subsided.
- Also, monitor the baby’s vital signs and general condition. If any abnormality is found, refer immediately.
- Day:1 After checking active bowel sounds at the end of the day, give him plain or electrolyte water and start oral feeding.
- Day:2 Give the patient a light solid diet and if the stool does not pass, provide three to four teaspoons of lactulose while sleeping.
- Day: 5/Day: 6: Abdominal skin stitches and D Prepare the patient for removal of D – 5 (transverse) or D – 6 (longitudinal).
- Discharge: Provide proper education on discharge advice such as nutrition, hygiene, baby care, etc. when the patient is discharged the next day after stitches are removed.
Classical/Upper Segment Cesarean Section:
This The operation involves making an incision in the upper segment of the uterus to deliver the baby. Its indications in current obstetrics are limited.
Indications:
- Dense adhesions,
- Severely contracted pelvis with pendulous abdomen,
- Big fibroid in lower segment,
- Carcinoma of cervix,
- Complete anterior placenta previa etc.
Complications of Cesarean Section:
Intraoperative: Severe hemorrhage, bladder injury, ureteral Injury.
Postoperative Complications:
Maternal:
Immediate: Postpartum hemorrhage, shock, anesthesia hazards, infection, intestinal obstruction, thromboembolic disorders, wound complications.
Maternal mortality rate 0.1-1%.
Remote: Menstrual excess or irregularity, chronic pelvic pain, back, Incisional hernia, intestinal obstruction, increased risk of scar rupture in future pregnancies.
Fetal: iatrogenic prematurity, respiratory distress syndrome.
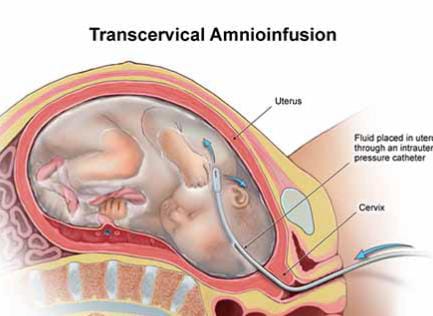
Amnioinfusion:
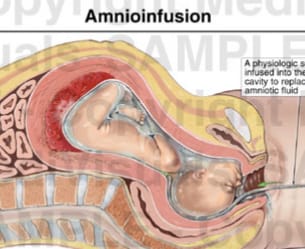
- In amniinfusion, fluid (isotonic fluid) is instilled into the amniotic cavity. This procedure is performed during labor after rupture of the fetal membranes via a transcervical intrauterine pressure catheter.
Indications:
Helps to thin the meconium passed in the amniotic fluid.
It is used to prevent compression of the umbilical cord in cases of oligohydramnios.
Reduces meconium aspiration syndrome.
Contraindications:
Placenta previa is a major contraindication.
Manual Vacuum Aspiration (MVA):
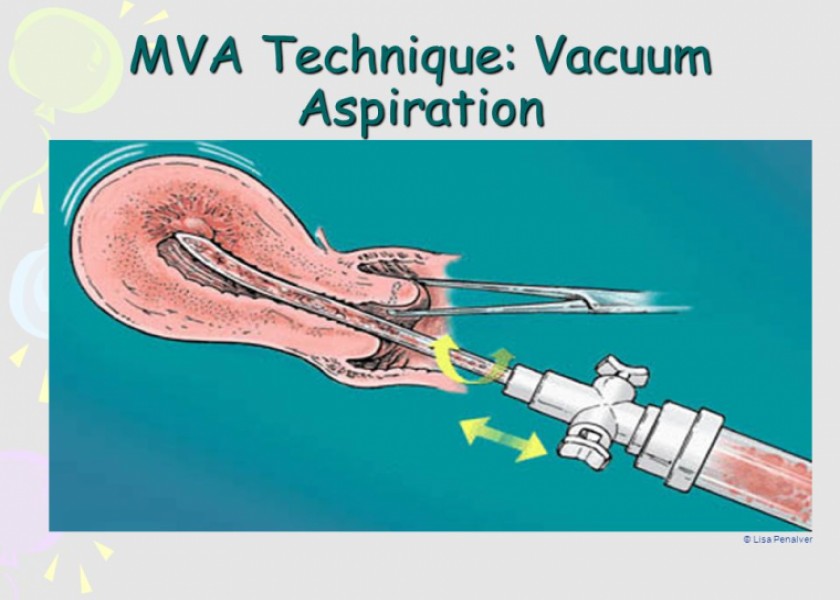
- Manual vacuum aspiration is a safe and effective method of abortion. It involves a plastic aspirator through which all the contents of the uterus (uterine cavity) are evacuated. This procedure is also performed if there is a 12-week pregnancy and it is to be aborted.
- When there is a miscarriage, there is a condition of spontaneous abortion, then if there is a need to remove the retained product after an induced abortion or when an endometrial biopsy is to be taken, the procedure of manual vacuum aspiration (MVA) is performed.
Indications:
- Manual vacuum aspiration is indicated in the following situations:
- Early abortion (up to 12 weeks of gestation).
For the management of incomplete or missed miscarriage.
For the treatment of abnormal uterine bleeding.
Used to remove retained placental tissue after childbirth.
Procedure:
Preparation:
- Inform the patient about the procedure, including explaining the potential risks and benefits, and then obtaining proper consent.
Anesthesia:
- Local anesthesia is usually administered to minimize discomfort. Sedation is also provided.
- Dilatation: The cervix is usually dilated using sterile instruments, although manual vacuum aspiration requires less dilation compared to other procedures.
- Evacuation: A handheld suction device is introduced into the uterine cavity and a vacuum is manually created using a syringe to remove the contents.
Complications:
- After evacuation, the contents are examined and observed for completeness.
Benefits:
Minimally invasive:
It is a less invasive option than surgical options and has a shorter recovery time.
Quick Procedure:
It is usually completed in 10-15
minutes.
Outpatient Basis:
It is usually performed in an outpatient setting.
Risks and Complications:
- Infection Such as pelvic inflammatory disease (PID) and endometritis.
- Accidental perforation of the uterine wall.
- Bleeding before and after the procedure.
- Damage to the cervix during the procedure.
- Retained products of conception may remain, such as incomplete evacuation, requiring further treatment.
- Emotional effects can also occur such as anxiety, depression, etc.
Aftercare:
- Properly monitor for excessive bleeding and signs of infection.
- Manage pain as needed.
- Then advise the patient to follow up properly.
Dialatation & Evacuation (Dilatation and Evacuation (D&E):
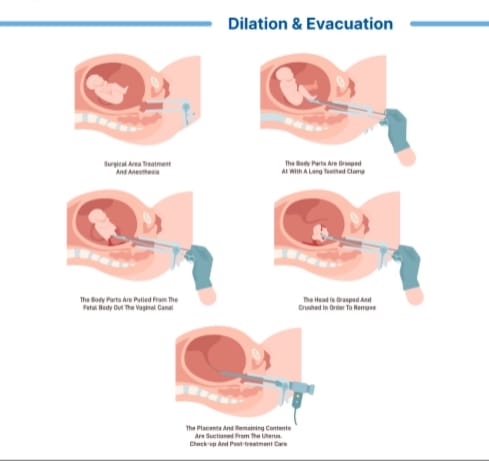
- The surgical procedure of dilating the cervix and removing the contents of the uterus is called dilation and evacuation (D&E).
- Its other names are ERPOC (Evacuation of Retained Product of Conception) and TOP or STOP ((Surgical)Termination of Pregnancy).
- D&E is normally a specific second trimester procedure. However, D&E refers to any procedure involving dilation and evacuation, including manual and electric vacuum aspiration in the first trimester.
Instrument:
- Swab Holder,
- Sims Speculum,
- Anterior Vaginal Wall Retractor,
- Volcellum,
- Uterine Sound,
- Cervical Dilators,
- Curette,
- Uterine Dressing Forceps,
- Suction Cannula,
- Suction Tube with Electric Operated Hand Operated Vacuum Flask.
Indication:
- Therapeutic abortion (First trimester MTP – suction evacuation), Inevitable abortion, Incomplete abortion, Missed abortion, Vesicular mole evacuation.
To remove the remaining placental tissue in some cases after second trimester MTP by medical method. - Stretchaway evacuation when the cervix is already dilated and cervical dilation when the cervix is not dilated by rapid method (metal dilator) or slow method (prostaglandins, hygroscopic agents) is done by.
Pre-operative measures:
- Except for emergencies, full routine pre-operative preparation including local saving, antiseptic cleaning, evacuation of bowel, neil by mouth 6 hours before then take proper sedative and return consent.
Anesthesia:
- Properly provide general anesthesia or local anesthesia to the patient.
Procedure:
- Pre-operative With preparation, the patient should have their bladder emptied.
- Then provide the patient with proper lithotomy position on the operation table.
- After providing the patient with proper lithotomy position, paracervical block is given after catching the cervix with valselum.
- Pervaginal examination is done to check the size, position and mass of the uterus.
- Then introduce Sims speculum By swabbing the cervix, its anterior lip should be caught with a valselum. Then dilate the uterus by half to one mm more than the size of the vagina with a dilator.
- Introduce the ovum forceps and remove the complete product. Remove the remaining product by curettage with blunt or sharp curettage.
- Provide Inj. Methylergometrine IV.
- After checking whether the uterus is well contracted and the size is reduced or not, examine all the products and check whether they are complete or not.
Post-operative Care:
- Prophylactic antibiotics should be given to the patient.
- The patient is discharged after four to six hours.
Complications:
- Cervical Injury,
- Incomplete Evacuation,
- Perforation of the Uterus,
- Operation Failure,
- Excessive Blood Loss,
- Anesthetics Complications,
- Infection,
- Increased chances of injury to the bowel and bladder,
Delayed complications:
- Infertility,
- Repeated abortion,
- Chronic pelvic inflammatory disease, PID,
- Ectopic pregnancy.
Suction Evacuation (Suction Evacuation) :
- This is a procedure in which In which the products of conception are sucked out of the uterine cavity.
Indications
- For medical termination of pregnancy during the first trimester.
- Involuntary abortion.
- Recent incomplete Abortion.
- Hideti form mol.
Procedure:
Preliminaries:
- Provide proper anesthesia to the patient. Involves general or local anesthesia.
- Provide the patient with proper lithotomy position.
- Perform the procedure with full surgical asepsis.
- Advise the patient to empty the bladder.
- Perform a proper vaginal examination.
Procedure:
- Perform a vaginal examination to properly note the size and position of the uterus and to properly note the state of the cervix.
- Introduce the posterior vaginal speculum and advise to hold it properly.
- Then grasp the anterior lips of the cervix properly with Ellis forceps.
- Then introduce the uterine sound and visualize the uterine cavity. Note the length and its position properly.
- Dilate the cervix with a smaller sized graduated metal dilator up to one size smaller than the suction cannula (especially in primigravidas, instead of dilation by metal dilators). If available, it is beneficial to introduce laminaria tent or intravaginal prostaglandin E2 pessary 3-5 mg every 12 hours.
- To prevent postpartum hemorrhage in the 3rd stage of labor, 10 units of oxytocin I/M intramuscularly in 500 ml saline or lactated Ringer’s solution or 20 units of oxytocin intravenously I/V infusion should be routinely administered.
- Appropriate suction cannula is fitted into the uterus, the tip should be placed in the middle of the uterine cavity. is.
- Then the suction pressure is raised to 400 – 600 mmHg. When the pressure is turned on, the cannula moves up and down and rotates in the uterine cavity.
- The suction bottle is then inspected to determine the amount of products of conception and blood loss.
- The suction is regulated by fingers placed on the holes in the base of the cannula.
- The end point of suction is denoted by:
- No further materials are Not being sucked out.
- Contracting small size uterus by gripping the cannula.
- Grating sensation.
- Appearance of bubbles in the cannula or transparent tubing.
- Before withdrawing the vacuum from the cervical canal, the vacuum should be properly broken to prevent injury to the internal os of the cervical canal.
- At the end of the suction, it is best to curette the uterine cavity with a small blushing curette and reintroduce the cannula to suck out any remaining uterine cavity product.
- After being satisfied that the uterus is firm and there is minimal vaginal bleeding, the patient is placed on a sterile vulval pad and brought down from the table.
Complications:
- Infection,
- Hemorrhage,
- Uterine perforation,
- Cervical injury,
- A small amount of retained product of conception may be seen. is.
- Anesthesia complications.
- Allergic reactions.
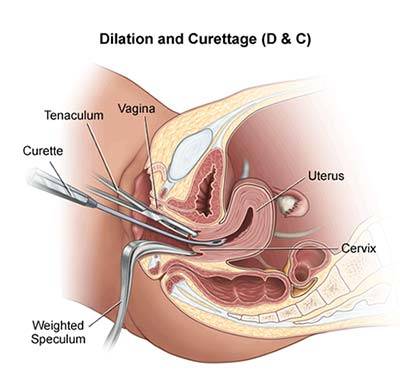
Dilatation and Curettage (D&C):
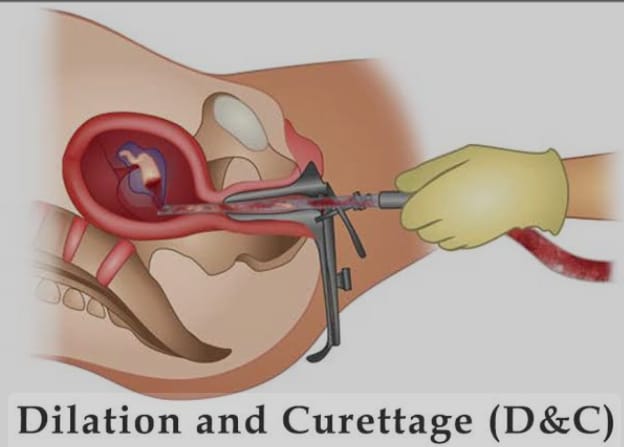
- Dilation and curettage (D&C) is a surgical procedure commonly performed in obstetrics and gynecology. It usually involves dilation of the cervix followed by scraping or suctioning of the uterine lining.
Indications:
- Dilation and curettage can be done for different reasons. Such as,
For diagnostic purposes: To collect tissue samples for examination. (Ex: Abnormal bleeding and suspected pregnancy). - Therapeutic Use: To remove retained placental tissue after miscarriage or abortion.
To manage incomplete abortion or uterine bleeding. - Endometrial Hyperplasia: To treat abnormal thickening of the uterine lining.
- Polyps Removal: To remove uterine polyps.
Procedure Steps:
- Preparations: Perform a complete pre-operative evaluation of the patient, including blood tests.
- Advise the patient on proper fasting before the procedure.
- Anesthesia: Administer local or general anesthesia depending on the case or patient preference.
- Dilation: Properly dilating the cervix using a dilator, which allows proper access to the uterus.
- Curettage: A curette (surgical instrument) is used to scrape or suction the uterine lining.
- Completion: After the procedure is complete, the instrument is removed and the patient is properly observed.
Recovery:
- After the procedure is completed, the patient should be observed for a reasonably short duration.
- Light bleeding and cramping are common. And it can be managed with over the counter pain relief.
- Then advise the patient to follow up properly.
Risks and complications:
- Infection,
- Heavy Bleeding,
- Perforations of the uterus,
- Scarring of the uterine lining (Asherman’s syndrome)
Aftercare:
- Properly assess the patient for any signs and symptoms of infection Make observations (e.g., fever, foul-smelling discharge).
- Advise the patient to follow proper medical advice to resume normal activities.
- Advise the patient to avoid sexual activity for a few weeks.
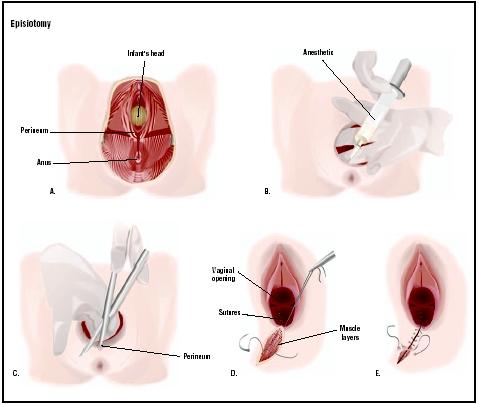
Episiotomy:
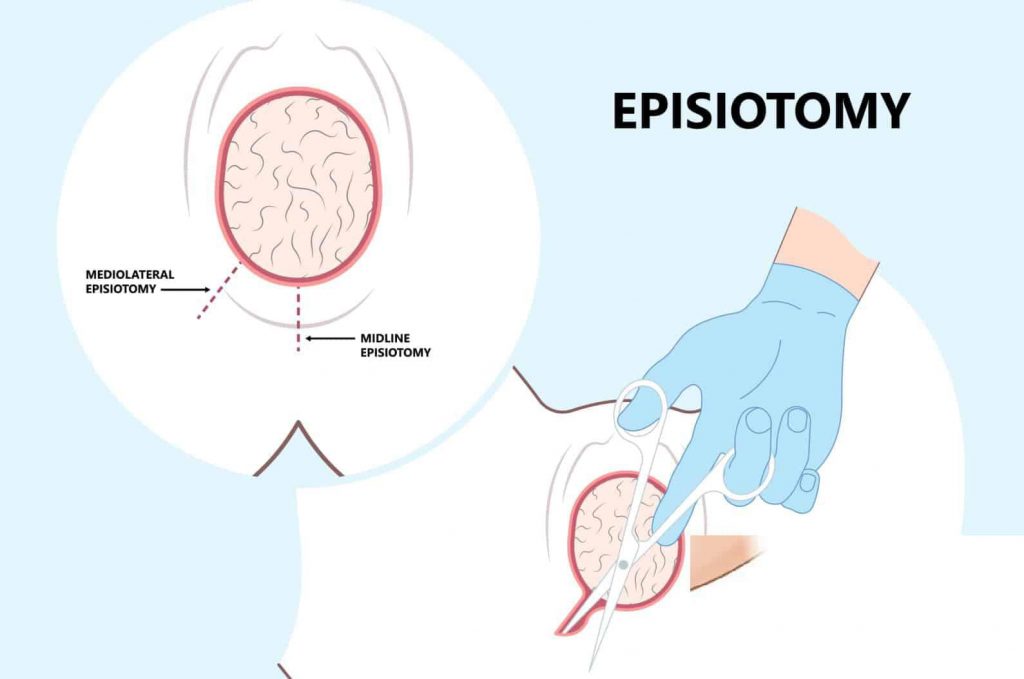
- A surgically planned incision is made on the perineum and posterior vaginal wall during the second stage of labor (2nd stage) and is called an “episiotomy”. An episiotomy is performed to widen the vaginal opening for spontaneous or manipulative easy and safe delivery of the fetus. An episiotomy is performed to reduce excessive stretching and rupture of the perineal muscles and fascia and to reduce stress and strain on the fetal head.
Objectives:
- To enlarge the vaginal opening for spontaneous or manipulative easy and safe delivery of fetuses.
- To reduce excessive stretching and rupture of the perineal muscles and fascia.
- To reduce stress and strain on the fetal head.
Indications:
- Episiotomy is not performed routinely but only in cases where it is considered necessary. Its indications are as follows, such as,
- When the perineum is rigid: In elderly primigravida, the presenting part cannot descend down. Or it is delayed.
- When there is a possibility of perineal tear: Big baby, face to pubis delivery, breech delivery, solder dystocia.
- Operative delivery such as forceps delivery, ventouse delivery.
- Previous perineal surgery: pelvic floor repair, perineal reconstructive surgery.
- In mild indications – in primigravida When there is a risk of perineal injury, when the perineum is rigid, when there is an occiput posterior or face delivery.
- Timing of episiotomy: The ideal time is when the head is 3 – 4 cm visible just before crowning, when the perineum is bulging and thickening during contractions. Forceps are given after the blades are inserted in the delivery.
Advantages:
Maternal:
Easy for repair and healing.
The duration of the second stage is reduced.
Trauma to the pelvic floor muscles is reduced. Hence prolapse and urinary incontinence do not occur.
Protects the perineum from lacerations, tar and hematoma.
Fetal:
Prevents fetal asphyxia.
Reduces intracranial injury in premature babies and breech.
Disadvantages:
Blood Loss-100-200ml occurs through the episiotomy wound.
Perineal trauma increases.
Vulval hematoma and infection may occur.
Pain.
Type of episiotomy:
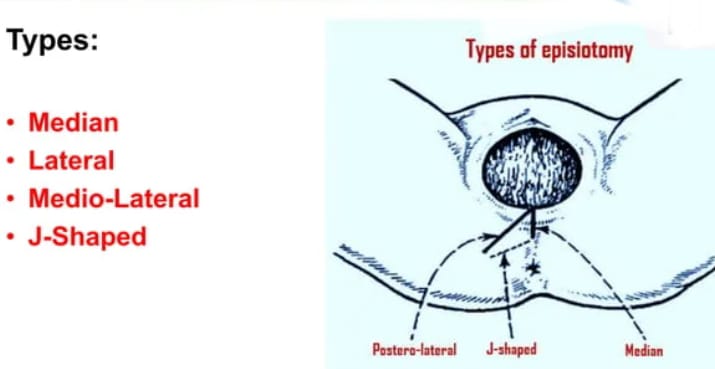
There are generally four types of episiotomy, such as,
1) Medio-lateral
2) Median
3) Lateral
4) ‘J’ sep
1) Medio-lateral: In this, an incision is made from the midpoint of the forechet to the right or left side, downwards and outwards. It is placed 2.5 cm from the anus.
2) Median: In this, the incision starts from the centre of the forechet and extends posteriorly 2.5 cm. As much as it is extended in the midline.
3)Lateral: In this, the incision is started from 1 cm away from the center of the foreskin and extended laterally, which leaves the possibility of injury to the Bartholin gland.
4)’J’ sep: In this, the incision is started from the center of the foreskin and is posterior 1.5 cm from the midline and then downward and outward
The anal sphincter is avoided at the 5 or 7 o’clock position It is placed in this way.
Articles and Supplies for Episiotomy:
- Episiotomy and Suturing Tray/ Articles:
- Local anesthetic: Xylocaine or Lignocaine 1%.
Syringe: 10ml.
Needle: g 18 to 21 one each.
Episiotomy scissors: 1.
Dissecting forceps: Toothed: 1.
Needle holder: 1.
Straight artery forceps: 2.
Myo scissors: To cut the suturing material.
Suturing material: Chromic catgut with eyelets round body needle.
Cutting needle: 1.
Kidney tray.
A pair of sterile gloves. - Linen: The perineal sheet that is used while conducting the delivery should be removed after the 3rd stage of labor is completed, and then another perineal sheet should be used for suturing. The length of which is approximately 90 cm × 90 cm, it covers the lower abdomen and the edge of the table. Cover the whole seat, exposing the vulva and vaginal outlet.
- Cotton swabs: Place 10 to 30 (large size) cotton swabs in the bowel. It is used to clean and wipe the episiotomy and to be used during suturing.
- Perineal pad: The pad is placed in the vagina to prevent blood from dripping into the suturing site and is kept with the cord facing outward. Another pad is used during suturing and is to be removed before cleaning the vagina after suturing.
Steps of the Procedure:
- Provide the patient with a lithotomy or dorsal position.
- Properly swab the perineal area with antiseptic lotion (povidone iodine).
- Properly drape the episiotomy site.
- Local anesthesia: Infiltrate 10 ml of 1% solution of lignocaine along the incision line on the perineum.
- Incision:
In an episiotomy, two fingers are placed between the presenting part of the vagina and the posterior vaginal wall. - Then the incision is made with episiotomy scissors, one blade of which is placed inward between the fingers and the posterior vaginal wall and the other on the skin.
- The incision should be made when the level of ureteral contractions is at its highest.
- Then the cut is made starting from the center of the forechest and extending to somewhere Right or left lateral extension is made.
Procedure of Suturing Episiotomy:
- Timing of Repair: Repair should be done immediately after expulsion of the placenta. Early repair can prevent sepsis and vaginal bleeding.
Preparation:
- Place the patient in the lithotomy position and then provide a proper light source.
- Clean the perineum and wound area with antiseptic lotion.
- The repair is performed with strict aseptic precautions.
- A vaginal pack is placed and elevated.
- The pack should be removed immediately after suturing is complete.
- Episiotomy repair is performed in the following order:
- Vaginal mucosa and submucosal tissue: chromic catgut on a covered round needle into the vaginal wall Take interrupted sutures from the edge of the wound to the margin of the hymen.
- Perineal muscles: Then take interrupted sutures from the chromic catgut to the margin of the wound from the hymen to the forechest with a round needle.
- Skin and subcutaneous tissues: Then join the skin and subcutaneous tissues and take sutures.
After the procedure is complete, remove the pad and place a sterile pad on the perineum to provide a comfortable position.
Postoperative Care for Episiotomy:
- Dressing: Clean and dry the wound after each urination and defecation.
Swab a cotton swab in antiseptic solution and then apply antiseptic powder or ointment. - Comfort: Magnesium sulfate dressing or infrared heat can also be used to reduce pain. Ice packs reduce swelling and pain. Provide appropriate analgesic drugs if necessary.
- Ambulations: Ambulate the patient after 24 hours. Before that, they can roll in bed and sit properly but advise them to keep their feet properly together.
- Removal of stitches: If the stitches are from cat gut or dexone, they do not need to be removed. But if silk or nylon is used, it should be removed after 6 or 7 days.
Complications of episiotomy:
Immediate:
The incision may involve the rectum, cause vulval hematoma, injury to the anal opening, recto-vaginal fistula, etc.
Remote:
Dyspareunia,
Chances of perineal injury in second delivery etc.
Post Abortion Care :

Nursing management of abortion involves comprehensive care and support for women undergoing termination of pregnancy.
1) Patient Assessment:
History Collection
- Collect a complete history of the woman’s medical, obstetric and gynecological conditions. Assess the gestational age of the pregnancy.
- Identify the reason for the abortion.
Physical Examination:
- Vital signs
- Completely monitor the mother’s vital signs, including,
- Blood pressure,
- Pulse,
- Properly and continuously monitor respiration and temperature, etc.
- Assess the client for any signs of hemorrhage, such as excessive bleeding, pallor, etc.
- Perform an abdominal examination to assess the tenderness of the uterine cavity.
- Then perform a pelvic examination to assess cervical dilation and whether the products of conception are present in the uterine cavity.
2) Psychological support:
- Mother and family Provide proper emotional support and counseling to members. Advise the patient to explain and express their feelings.
- Provide education about available resources for psychological support such as support groups and counseling services.
3) Pain Management:
- Provide prescribed analgesic medications to relieve the patient’s pain, such as NSAIDs or Acetaminophen.
- Advise the patient to use non-pharmacological measures to relieve pain, such as heating pads and relaxation techniques.
4) Management and Monitoring of Complications:
- Hemorrhage
Assess the patient for signs of excessive bleeding.
Properly assess the amount of blood loss the mother has suffered. If the patient needs it, prepare a blood transfusion. - Infection
Assess the patient for signs and symptoms of infection such as fever, foul smelling, purulent discharge, and lower abdominal pain.
Properly assess the patient for appropriate antibiotic medication as prescribed. To do. - Retained product of conception
Properly monitor the patient for signs of incomplete abortion such as continuous heavy bleeding and cramping pain.
Prepare the patient for possible surgical intervention such as dilation and curettage (D & C).
5) Patient education:
- Post-abortion care
Provide patient education about signs and symptoms that require immediate medical care, such as heavy bleeding, pain, and fever.
Provide instructions to maintain perineal hygiene to prevent and treat infection. - Follow-up care
Advise patient to schedule a follow-up appointment one to two weeks after abortion to properly assess complete recovery.
Provide patient education about the importance of follow-up visits. - Contraceptive Counseling Provide information to the patient about available contraceptive options to prevent unintended pregnancy.
Also provide education to the patient about the timing of using contraceptives after abortion.
6) Discharge Planning:
- Discharge Planning should include ensuring that the patient is able to go home and that adequate support and a safe environment are available to the patient at home. Provide written instructions that include information about the use of medication, activity restrictions, and signs of complications. Provide information about support services and resources available in the community.
Documentation:
- All assessments, interventions, patient responses, and Properly and accurately document the education received.
Record the patient’s emotional states and provide counseling and psychological support. - Nurses play a critical role in the comprehensive management of women who have had an abortion, which involves providing compassionate care, ensuring the patient’s physical and emotional well-being, and providing education to the patient about post-abortion care and contraceptive options.
Proper assessment, monitoring, and appropriate intervention of the patient can prevent complications and The recovery process can also be made easier. Thus, proper management of abortion plays an important role in improving the well-being of the mother.
