ENGLISH-NEW MIDWIFERY GNM TY UNIT 8 Management of Complications During Pregnancy
Unit : 8 Management of Complications During Pregnancy (Management of Complications During Pregnancy) :

Bleeding In Pregnancy (Bleeding In Pregnancy) :
Ectopic Pregnancy (Ectopic Pregnancy) :
Definition:
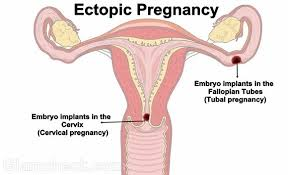
- When a fertilized ovum implants and develops outside the endometrial cavity of the normal uterus, it is called an ectopic pregnancy.
Anatomical site of implantation of ectopic pregnancy:
- Tubal pregnancy is more common, normally occurring in the right fallopian tube than the left fallopian tube. The ampulla of the fallopian tube is the most common site of implantation of an ectopic pregnancy.
- If an ectopic pregnancy occurs in the isthmus of the fallopian tube, it is considered a dangerous site, which can also lead to tubal rupture.
Etiology:
- Some factors delay the migration of the fertilized ovum into the uterine cavity.
- Factors that provide a favorable environment for the fertilized ovum to implant in the tubal mucosa.
- Hormonal factors,
Birth defects,
Medical conditions.
Risk Factores:
- Due to a previous ectopic pregnancy,
- Due to a previous surgery in the uterine tube,
- Due to tubal reconstructive surgery,
- Due to failure of use of intrauterine contraceptive device,
- Due to certain types of infections such as,
- Pelvic inflammatory disease,
- Chlamydia infection,
- Gonorrhea etc.,
- Having a history of infertility Due to,
- Assisted Reproductive Techniques (ART),
- Infertility Treatments such as,
- In Vitro Fertilization (IVF),
- Mother’s age is more than 35 years,
- Previous abortion induced,
- Because of a history of endometriosis.
Sign And Symptoms:
The signs and symptoms of ectopic pregnancy are classified into two types:
1)Acute type
2)Chronic type
1)Acute type
- Acute type of ectopic pregnancy is characterized by triad of symptoms such as:
- Amenorrhea,
Sharp colicky abdominal pain,
Vaginal bleeding,
Nausea and vomiting,
Palence usually depends on the amount of hemorrhage.
Signs and symptoms of shock are seen, such as,
Rapid and weak pulse,
Blood pressure fall,
Extremities are cold and clammy.
On abdominal examination, the abdomen is tense, tender and Tender feeling. Abdominal tenderness. Bowel distension. Tubal rupture and tubal abortion are accompanied by massive intraperitoneal hemorrhage. - Positive Cullen sign: Dark bluish peri-umbilical ecchymosis due to hemoperitoneum.
Pale vaginal area during pelvic examination.
Uterus appears to float in water.
2) Chronic Type
- In the chronic type, tubal moles are common
- It is not detected in the beginning.
- Its signs include anemia, bladder irritability, tachycardia, and increased temperature.
- Amenorrhea,
- Abdominal Pain,
- Vaginal bleeding that is dark in color occurs shortly after abdominal pain.
- Bladder irritation such as dysuria, frequency of urination, retention of urination.
- Increase in body temperature.
- On examination, the patient appears ill,
- Pallence,
- Increased pulse rate even at rest.
- Abdominal tenderness on the affected side.
- A mass-like structure that is irregular in shape may be felt on the lower abdominal site.
- Extreme tenderness of the cervix.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History Collection,
- Physical Examination,
- Blood Examination,
- Caldosynthesis (Tapping of Pouch of Douglas),
- Sonography,
- Assessment of hCG level,
- Laparoscopy,
- Laparotomy,
- Dilatation and curettage,
- Trans vaginal ultrasonography (USG)
Management Of Ectopic Pregnancy:
The management of ectopic pregnancy is divided into two types,
such as,
1) Acute ectopic pregnancy management,
2) Chronic ectopic pregnancy management
Principles of Management
Preventing maternal complications.
In case of ectopic pregnancy, immediate laparotomy should be performed because the fertilized ovum cannot survive outside the uterine cavity, so the tissue is removed to prevent serious complications.
1) Acute ectopic pregnancy management:
- Provide anti-shock treatment to the patient and prepare for urgent laparotomy.
- Advise the patient to lie down flat on the bed.
- Provide the patient with inj.morphine 15 mg ( IM ).
- Start 5% dexrose drip if necessary.
- Arrange blood for blood transfusion.
- If blood is not available or not arranged and the patient is in a state of shock, it is still essential to perform laparotomy.
- The fallopian tube containing the gestational sac is removed through laparotomy and partially surgical procedures.
- Performing a salpingectomy. In which step,
- Refer the patient to the hospital,
- Advise the patient to lie down on a flat bed.
- If the patient is collapsed, raise the bed towards the foot end.
- Assess the patient’s hemoglobin level.
- If the patient needs a blood transfusion, pour the blood Keep.
- Administer adequate intravenous fluid to the patient until blood is available
- Ex:=Ringer lactate,
- Dexran.
- Perform a quick laparotomy on the patient under general anesthesia for salpingectomy.
- Then make an incision on the line of the intra-umbilical incision.
- Then recognize the uterus and continuously suction out the blood To do.
- Then both the sites of the uterus are accessed so that the gestational sac in the fallopian tube can be identified.
- Then the affected tube and ovary are observed.
- Then the clamps are applied.
- Then the gestational sac and the affected fallopian tube are removed with or without the ovary.
- The clamps are tied with chromic catgut ligature is replaced which should not be tightened.
- Then proper hemostasis is ensured.
- When the patient desires sterilization, tubectomy or salpingectomy is performed for hydrosalpinx for the other fallopian tube.
- When, a blood clot is present free in the peritoneal cavity, it should be aspirated as possible.
- Then the pelvic cavity is properly washed with normal saline and Close the abdomen quickly.
- In case of pregnancy in the interstitial part of the tube, only the gestational sac should be removed but sometimes for the purpose of better hemostasis, a quick subtotal hysterectomy is necessary.
2) Chronic ectopic pregnancy management:
- Admit all cases of chronic ectopic pregnancy to the emergency department.
- Keep the patient under proper observation.
- Properly conduct all investigations of the patient.
- Control bleeding quickly and effectively.
- Keep blood transfusions available.
- Provide the patient with intravenous infusion as prescribed.
- Advise the patient to perform laparotomy as early as possible.
- Prepare the patient for laparoscopy or laparotomy.
- Then advise to perform salpingectomy.
- Ectopic pregnancy with medical management Ectopic pregnancy is removed by making an incision on the fallopian tube or removing a section of the tube.
- If the patient has a suppurative pelvic hematocele, provide proper antibiotics and drain the pus.
- Remove the tubal mole by laparotomy and partial incision on the fallopian tube.
- Provide proper management to the patient after surgery.
- Provide systemic methotrexate 50 mg IM to the patient in medical treatment.
- Rh antigen does not sensitize in Rh positive women. Anti D gamma globulin -50 micrograms should be given to the patient immediately after the operation to prevent isoimmunization.
- Provide care to bring the patient out of shock in acute rupture of the fallopian tube.
- Properly maintain the patient’s vital sign intake output chart.
- Provide antibiotic medication to the patient.
- Encourage the patient to move early To do.
- Advise the patient to follow up properly.
Abortion (abortion) :
Definition of Abortion:

Abortion is the process by which a pregnancy is terminated. In abortion, the product of conception is Partial or complete separation and expulsion of the embryo from the uterine wall before the age of viability (28 weeks) is called “abortion”. If abortion occurs spontaneously, it is called “miscarriage”. And if it is done intentionally, it is called “induced abortion”.
The majority of abortions or miscarriages occur during the first trimester of pregnancy, i.e. during the first 12 weeks of pregnancy, it is called “early miscarriage”. And a miscarriage that occurs after 13 weeks of pregnancy is called a “late miscarriage”.
Etiology:
The etiology of abortion is often complex and unclear but may include the following:
1. Ovular or fetal factor
2. Maternal environment
3. Paternal factor
4. Unknown (25%).
Ovular or fetal factor: Autosomal trisomy in which there are three homologous chromosomes instead of two autosomes. Any chromosome other than the sex chromosome (common).
A condition of monosomy without a missing chromosome from a pair of homologous chromosomes.
Gross congenital malformation.
Blighted ovum (ovum without embryo).
Due to hydropic degeneration of the villi.
Knots, twists or interference with the circulation of the umbilical cord can cause fetal death and expulsion.
Due to multiplacental formation.
Twins or hydroamnios.
Maternal environment:
1.Maternal illness: such as,
Infection:
Viral infections – Rubella, Cytomegalovirus, Hepatitis Parvovirus, Influenza Virus etc.
Parasitic – Malaria
Protozoal – Toxoplasmosis.
Maternal Hypoxia and Shock: It can be caused by the production of anoxic conditions due to the following conditions.
Acute Reproductive Disease,
Chronic Reproductive Disease,
Heart Failure,
Severe Anemia,
Anesthesia Complications,
Severe Gastroenteritis,
Cholera.
Chronic Illness:
Hypertension
Chronic Nephritis
Chronic Wasting Disease.
Endocrine Factors:
Hypothyroidism,
Hyperthyroidism,
Diabetes Malitis.
2. Trauma:
Direct trauma to the abdominal wall,
Psychic: Emotional upset or changes in the environment can lead to abortion.
c In susceptible individuals, even minor trauma, e.g.
rough road.
Internal examination in early months.
Eliciting Hager sign.
Sexual intercourse in early months.
3.Toxic Agents: Toxic agents are involved:
Environmental toxins such as:
a.Lead
b.Arsenic
c.Anaesthetic gases
d. Tobacco
e. Caffeine
f. Alcohol
g. Radiation in excess amount.
4. Cervico-uterine factors:
Cervical incompetence,
Congenital malformation of the uterus,
Uterine tumor (fibroid),
Retroverted uterus,
5.Immunological factors:
Lupus anticoagulant.
Antiphospholipid antibodies.
Alloimmune factors.
6.Blood group incompatibility: It involves Rh incompatibility.
7.Premature rupture of membranes can lead to conditions of abortion.
8. Diabetic factor: Due to deficiency of folic acid and vitamin C.
Paternal factor:
Due to defective sperm.
Due to contribution of half the number of chromosomes of the ovum.
Common non-causes of abortion:
First trimester:
Defective germ plasma,
Hormonal deficiency,
Trauma,
Acute infection.
Mid Trimester:
Cervical incompetence,
Due to uterine malformation,
Uterine fibroid,
Low implantation of placenta,
Twins and hydroamnios
The condition of abortion can arise due to causes like.
Types Of Abortion (Types of Abortion) :
The types of abortion are as follows.
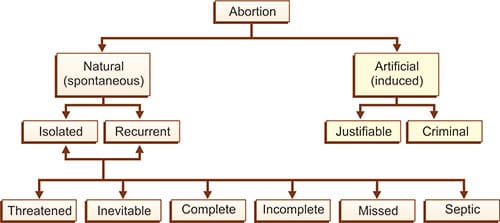
1)Spontanious Abortion
A)Threatened abortion,
B)Inevitable abortion,
C) Complete abortion,
D)Incomplete abortion,
E)Silent or missed abortion,
D) Septic abortion,
E) Recurrent abortion or habitual abortion,
2)Induced Abortion :
1)Spontanious Abortion
When an abortion occurs naturally without any kind of medical or surgical intervention, it is called spontaneous abortion. Its cause can be any genetic abnormality and maternal condition.
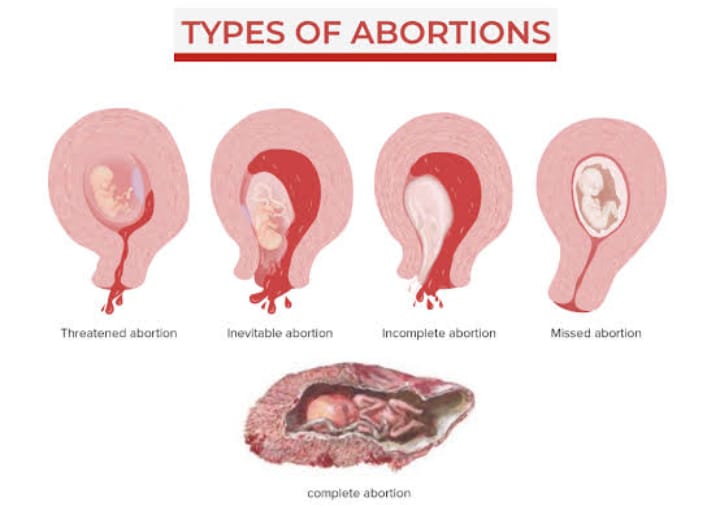
A)Threatened abortion:
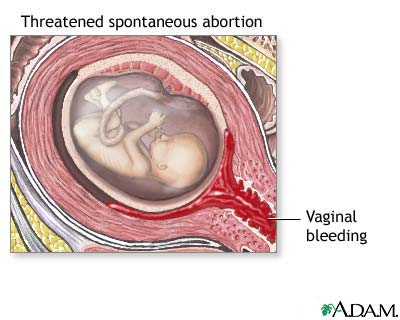
- In threatened abortion, the process of abortion starts but the abortion does not reach the stage where recovery is impossible, that is, if proper care is taken, recovery can occur.
B) Inevitable Abortion:
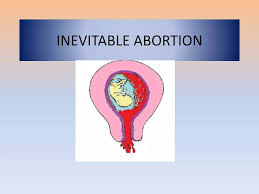
- Inevitable abortion is a type of abortion in which the expulsion of the conceptus progresses with cervical dilation. In this case, the pregnancy cannot be saved because most of the placenta has detached (from the uterine wall). This is a clinical type of abortion in which the changes of the abortion have progressed to the point where the continuation of the pregnancy becomes impossible.
C) Complete abortion:
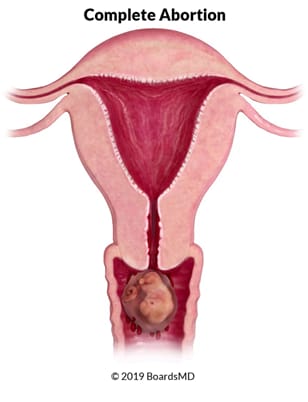
- Complete abortion is a type of abortion in which the products of conception are expelled as a mass, called a complete abortion. Abortion says
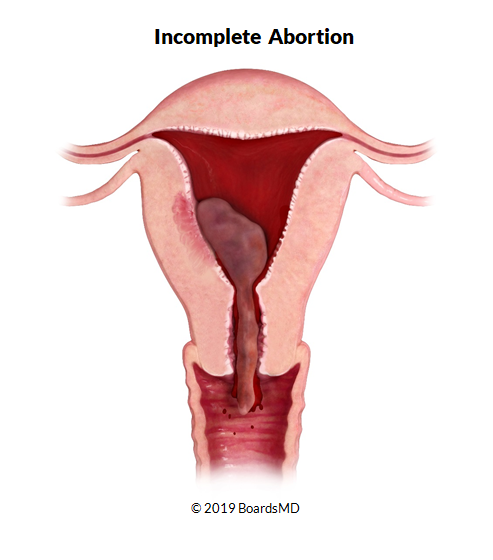
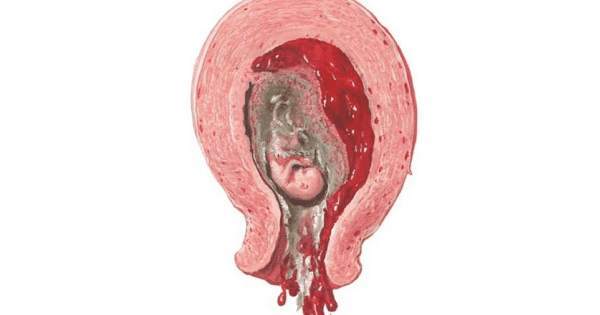
D) Incomplete Abortion:
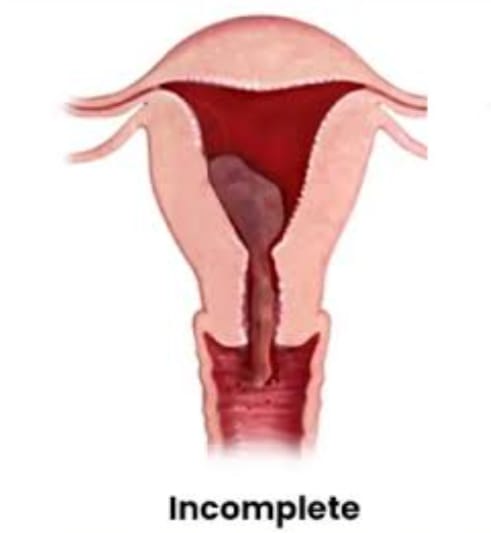
- Incomplete abortion is a type of abortion in which the entire product of conception does not exit the uterine cavity but some part of it remains in the uterine cavity, then this abortion is called incomplete abortion.
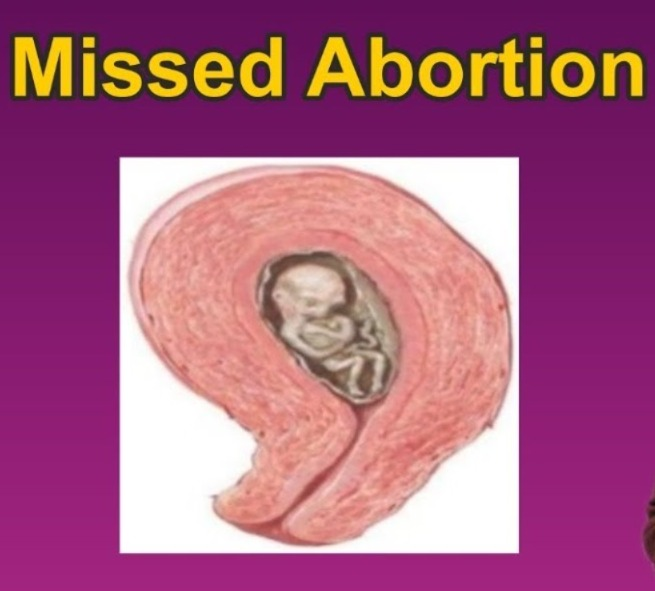
E)Silent or missed abortion:

- Silent or missed abortion is said to occur when the fetus dies in the uterine cavity and is retained in it for more than 4 weeks.
D) Septic abortion:
- When there is evidence of infection of the uterus and its contents with abortion, i.e. if the abortion is due to any infection, then this abortion is called septic abortion.
E) Recurrent abortion or habitual abortion:
- When three or more spontaneous abortions occur in a sequence before 20 weeks, it is called recurrent abortion.
- It is caused by immunoglobulin G, hormonal deficiency, and cervical incompetence. Other causes include
genetic factors,
infection,
endocrine and It is also caused by anatomical abnormalities.
2)Induced Abortion
- Induced abortion is when a pregnancy is terminated voluntarily using any medical or surgical procedure.
Medical Abortion:
- Medical abortion uses medication to terminate pregnancy and
- Medical abortion is effective up to 10 weeks of pregnancy.
Ex:= combination of Mifeprostone and misoprostol.
Surgical abortion:
In this, a surgical procedure is performed by health care personnel and the pregnancy is terminated. It is called surgical abortion Ex: vacuume Aspiration.
Threatend Abortion (Threatend Abortion) :

- In threatened abortion, the abortion process starts but the abortion does not reach a condition where recovery is impossible, meaning that if proper care is taken, recovery can occur. And the pregnancy can continue.
Sign And Symptoms:
- Vaginal erection,
- Mild abdominal pain and cramping,
- Bleeding is light,
- Blood color is bright red,
- Mild abdominal pain,
- Bleeding is painless,
- Mild back pain,
- Dull pain in the lower abdominal area,
- No fresh lump or expulsion of any kind,
- Cervical or closed,
- Discharge seen.
Sign:
- Abdominally: The gravid uterus feels soft and enlarges like a period of menorrhagia.
- Speculum examination or vaginal palpation: The os of the cervix is closed and a stained discharge is present.
Diagnostic Evaluation:
- Blood investigation including,
- HB, ABO and Rh grouping.
- Urine test,
- Bimanual palpation,
- Pelvic ultrasonography,
- Transvaginal ultrasonography.
Management Of Threatened Abortion:
Proper assessment and monitoring of pregnant women in nursing management of threatened abortion. Provide proper supportive care to the woman.
1)Assessment
Continuously monitor the mother’s vital signs. Such as,
Pulse,
Blood pressure,
Temperature,
Respiration etc.
Bleeding assessment
Assess the color, amount, intensity and consistency of vaginal bleeding.
History collection
Collect a proper history of the mother including a complete history of previous pregnancies and abortions.
2) Monitoring and Observation
Continuous observation of the mother should be done to assess whether she has any signs and symptoms of shock (hypotension, tachycardia, pallor).
Proper investigations of the mother should be done including hemoglobin, hematocrit, ultrasonography, ABO & Get Rh grouping done routinely.
3) Bedrest and Physical Activity
Advise the mother to take complete bed rest.
Advise the mother to limit physical activity.
Advise the mother not to do household work for a month.
4) Emotional Support
Provide emotional support and reassurance to the mother and her family.
Properly clear the doubts and queries of the mother and her family members.
Do not give false reactions to the mother and her family members.
5) Education
Provide education to the mother about the signs and symptoms of abortion such as increased bleeding, severe pain etc. and give advice or any such If signs and symptoms are seen, seek immediate medical treatment.
Provide education to the mother for proper follow-up.
6) Hydration and Nutrition
Advise the mother to have adequate fluid intake.
Continuously monitor the mother’s intake output chart.
Advise the mother to have a properly balanced diet.
Advise the mother to have a high fiber diet to prevent constipation.
Provide supplements to the mother with good fitting.
Ex:= Ferrous Sulphate 200 mg( BD. ),
Folic acid 5 mg/ day( TDS ).
Provide the mother with a diet rich in high protein and vitamin E.
7) Medication Administration
Provide the mother with prescribed medication.
Provide medication to control bleeding and relieve pain.
Provide education to the mother about the dosage, direction and side effects of the medication.
If the mother has problems of sleep and anxiety, then to relieve it
Tab.Diazepam, ( 5-10 mg before night meal ),
Or
Tab.Calmpose, ( 5-10 mg before night meal ),
Or
Tab.valium ( 5-10 mg before night meal ), should be provided.
Provide mild amount of laxative to mother at bed time for good bowel activity.
Ex:= Milk of Magnesia.
Do not provide enema to mother as enema is responsible for stimulating uterine contractions in mother.
Provide mild amount of laxative or suppository to mother after 48 hours of signs and symptoms of threatened abortion To relieve constipation if present.
8) Consultation and referral
Properly collaborate with other health care personnel for care.
Provide timely referral services to the mother if needed.
9) Documentation
Timely documentation of the mother’s assessment findings, interventions provided, and any changes in the mother’s condition Do.
10) Follow-up
Advise regular follow-up for the mother’s progress and reassessment.
Nursing management of threatened abortion is usually provided to provide proper comprehensive care to the mother and to bring about improvement in the mother’s condition.
Inevitable abortion (Inevitable Abortion) :
- Inevitable abortion is a type of abortion in which the expulsion of the conceptus product progresses with cervical dilation. In this abortion, the pregnancy cannot be saved/continued because most of the placenta has detached (from the uterine wall). This is a clinical type of abortion in which the changes of the abortion have progressed to the point where the continuation of the pregnancy becomes impossible. It is called “Inevitable abortion”.
Sign And Symptoms (Signs and Symptoms):
- Symptoms:
- Increased vaginal bleeding,
- This bleeding is due to the detachment of the placenta from the uterine wall,
- Severe colicky lower abdominal pain,
- No tissue is expelled,
- Dizziness due to heavy blood loss.
- Signs
- In the majority of cases, vital signs are normal, but in some cases, signs of shock are seen due to excessive bleeding.
- Skin becomes cold and clammy,
- Uterus feels firm (contracted),
- The cervix may be seen to dilate. The product of conception is felt by the finger while admitting the index finger.
Management:
- Properly assess the patient’s general condition.
- Properly assess the loss of conception.
- If there is excessive blood loss, administer intravenous (I.V.) fluid appropriately.
- If the patient has excessive blood loss, administer blood transfusion appropriately.
- If there is abortion, perform blood Hb, ABO Rh group and random blood glucose level test.
- Provide intramuscular (I.M.) injection of morphine 15 mg.
- In case of unavoidable abortion, if the cervix is fully dilated and the size of the uterus is less than 12 weeks, then administer injection of Methergine 0.2 mg to control excessive bleeding.
- If the patient is in shock, treat the shock condition properly by providing intravenous fluid (I.V.) or blood transfusion.
- If the abortion procedure was done before 12 weeks, then GA (general anesthesia) should be provided followed by dilation and After evacuation, curettage is performed. Alternatively, suction and evacuation can be used.
- If the abortion procedure is beyond 12 weeks, oxytocin drip (10 units in 500 ml of 5% dextrose) at a rate of 40-60 drops per minute enhances uterine contractions.
- If the fetus has been expelled and the placenta is retained, the ovum is removed with forceps.
- If the placenta is not separated, digital separation can be performed by providing GA Comes.
- If bleeding is excessive due to cervix closure (suggesting low implantation of placenta), then abdominal hysterotomy may be required to empty the uterus.
- If shock condition has arisen due to excessive blood loss, then it should be treated properly.
Complete Abortion (Complete Abortion) :
- Complete abortion is such type Abortion in which the product of conception is expelled in the form of a mass in which the fetus and placenta are completely expelled. The product of conception is not retained in the uterine cavity, i.e. the uterus is empty, is called complete abortion.
Sign And Symptoms:
- History of expulsion of a flabby mass-like structure,
- Mild abdominal pain,
- Vaginal bleeding is minimal or absent,
- The uterus appears smaller than during amenorrhea,
- The uterine cavity appears empty on transvaginal ultrasonography.
Management:
- Properly assess the patient’s general condition.
- Properly assess the loss of the product of conception.
- Continuously monitor the mother’s condition.
- Properly assess the amount of blood loss the patient has suffered.
- If excessive blood loss occurs If there is, administer intravenous (I.v.) fluid properly.
- If the patient has lost an excessive amount of blood, administer blood transfusion properly.
- If there has been an abortion, test blood Hb, ABO Rh group and random blood glucose level.
- If the patient is in a state of shock, treat the condition of shock properly by providing intravenous fluid (I.v.) or by transfusing blood.
- If shock condition has arisen due to excessive blood loss, then treat it properly.
- If there is any doubt that the product of complete conception will be expelled, advise the patient to undergo uterine curettage.
- To prevent unnecessary surgical procedure, advise the patient to undergo transvaginal sonography.
- In case of early abortion, Rh negative patient without antibodies in her system should be treated within 72 hours Respectively, Anti-D gamma globulin 100 micrograms I/M should be protected.
Incomplete Abortion :
- Incomplete abortion is a type of abortion in which the entire (complete) product of conception is not expelled from the uterine cavity but some part of it remains in the uterine cavity, then this abortion is called incomplete abortion.
Sign And Symptoms:
- History of expulsion of small amounts of mass-like structure from the vaginal area,
- Colic pain in the lower abdominal area,
- During internal examination The uterus appears smaller than the period of amenorrhea,
- Vaginal bleeding is observed,
- Explosion of an incomplete mass-like structure is observed during examination.
Management:
- Properly assess the patient’s general condition.
- Properly assess the loss of products of conception.
- Properly administer intravenous (I.V.) fluids if excessive blood loss occurs.
- Properly administer blood transfusion if excessive blood loss occurs.
- If abortion has occurred, blood Hb, ABO Rh group and random blood glucose level should be tested.
- Provide 15 mg of morphine by intramuscular (I.M.) injection.
- In the case of unavoidable abortion, if the cervix is fully dilated and the size of the uterus is less than 12 weeks, administer 0.2 mg of metharrhine injection to control excessive bleeding.
- If the patient If there is a condition of shock, treat the condition of shock properly by providing intravenous fluid (I.V.) or by doing blood transfusion.
- If the abortion procedure is before 12 weeks, then after providing GA (general anesthesia), dilation and evacuation are done and then curettage is done. Alternatively, suction and evacuation can be used.
- If the abortion procedure is beyond 12 weeks, oxytocin drip (10 units in 500 ml of 5% dextrose) at a rate of 40-60 drops per minute enhances uterine contractions.
- If the fetus has been expelled and the placenta is retained, the ovum is removed with forceps.
- If the placenta is not separated, provide GA and perform digital Separation (dilation and evacuation) is performed.
- If bleeding is excessive due to cervix closure (suggesting low implantation of placenta), abdominal hysterotomy may be required to empty the uterus.
- If shock condition has arisen due to excessive blood loss, then it should be treated properly.
- In the condition of incomplete abortion, the products of conceptus should be properly removed by ovum forceps or blunt curettage. To do.
- In late cases (dilation + curettage) the tissue that is left behind is operated on to remove the bits of tissue, and the removed material is sent for histological examination.
Silent or Missed Abortion:
- Silent or missed abortion is when the fetus is in the uterus. If the embryo dies in the cavity and is retained in the uterine cavity for more than 4 weeks, this abortion is called silent or missed abortion.
Sign And Symptoms:
- Persistent brownish vaginal discharge,
- Pregnancy related symptoms subside,
- Uterine growth arrest,
- Fetal heart sounds are not heard,
- Cervix is flaccid,
- Fetal skeletal collapse on radiology,
- Fetal movement is absent.
Diagnostic Evaluation:
- Blood investigation including,
- HB, ABO and Rh grouping.
- Urine test,
- Bimanual palpation,
- Pelvic ultrasonography,
- Transvaginal ultrasonography.
Management:
- When the uterus is less than 12 weeks:
- Vaginal evacuation is performed without delay.
- Slow dilation of the cervix by suction and evacuation or laminaria tent and emptying of the uterus under GA is done.
- Keep in mind the risk of hemorrhage during the operation.
- Uterus more than 12 weeks: For this, induction is done by the following methods:
Oxytocin:
- Initially starts with: 10-20 units of oxytocin in 500 ml of 5% dextrose saline is given in a drip at 30 drops/minute.
- If the above regimen If that fails, increase the dose of oxytocin to 100 units in a pint of 5% dextrose saline at a drip rate of 30 drops/minute.
- Use the above method with caution.
Prostaglandins:
- It is more effective than oxytocin.
- Inj. 15 methyl PG F 2α (carboprostromethamine) 250 µg I/M is given every 3 hours. This is provided at intervals for a maximum of 10.
- Prostaglandin E₁ analogue (gemiprost pessary) is inserted into the posterior vaginal fornix every 3 hours for a maximum of 5 pessaries.
- Proper assessment and monitoring of pregnant women in the management of abortion. Provide proper supportive care to women.
Assessment:
- Vital signs
- Continuously monitor the mother’s vital signs. Such as,
- Pulse,
- Blood pressure,
- Temperature,
- Respiration etc.
Bleeding assessment
- Assess the color, amount, intensity, and consistency of vaginal bleeding.
History Collection
- Collect a proper history of the mother, including a complete history of previous pregnancies and abortions.
Monitoring and Observation
- Continuously observe the mother and assess her for any signs and symptoms of shock (hypotension, tachycardia, pallor).
- Proper investigations of the mother including hemoglobin, hematocrit, ultrasonography, ABO & Rh grouping should be done routinely.
Bedrest and physical activity
- Advise the mother to take complete bed rest.
- Advise the mother to limit physical activity.
- Keep the mother in the household for one month Advise not to work.
Emotional support
- Provide emotional support and reassurance to the mother and her family.
- Properly clear the doubts and queries of the mother and her family members.
- Do not give false reactions to the mother and her family members.
Education
- Provide education to the mother about the signs and symptoms of abortion such as increased bleeding, severe pain, etc. and advise her to seek immediate medical treatment if any such signs and symptoms are observed.
Hydration and Nutrition
- Advise the mother to have adequate fluid intake.
- Continuously monitor the mother’s intake output chart.
- Advise the mother to have a properly balanced diet.
- Advise the mother to eat a high-fiber diet to prevent constipation.
- Provide supplements to the mother with good fitting.
Medication Administration
- Provide the prescribed medication to the mother.
Provide medication to control bleeding and relieve pain.
Provide education to the mother about the dosage, duration and side effects of the medication. - Provide the mother with a mild amount of laxative at bedtime for good bowel activity.
Ex:= Milk of Magnesia.
Consultation and Referral
- Properly collaborate with other health care personnel for care.
- Provide timely referral services to the mother if needed.
Documentation
- Timely document the mother’s assessment findings, interventions provided, and any changes in the mother’s condition.
Follow-up
- Advise regular follow-up for the mother’s progress and reassessment. The management of abortion is usually It is provided to provide proper comprehensive care to the mother and to bring about improvement in the mother’s condition.
Septic Abortion (Septic Abortion) :
- When there is evidence of infection of the uterus and its contents with abortion, i.e. if the abortion is due to any infection, then this abortion is called septic abortion.
Etiology:
1. It is caused by microorganisms involved in sepsis that are normally present in the vagina (endogenous).
2. Microorganisms are:
Such as,
a Anaerobic:
Bacteroides group (fragilis)
Anaerobic streptococci
Clostridium welchii
Tetanus bacilli
b Aerobic:
E. coli
Klebsiella
Staphylococcus
Pseudomonas
Haemolytic Streptococcus.
3. The increasing association of sepsis in illegal induced abortion is due to the fact that:
Proper antiseptic and asepsis are not taken.
Incomplete evacuation
Due to unintentional injury to the genital organs and adjacent structures, especially the (gut) intestine.
Sign And Symptoms (Signs And Symptoms):
- Septic abortion, signs of infection such as,
- Fever,
- Feeling cold,
- Ringers,
- Foul-smelling vaginal discharge and purulent vaginal discharge.
- There is a possibility of transmission of infection into the bloodstream.
- Abdominal pain and tenderness,
- Tachycardia,
- Increased pulse rate to more than 100-120, which indicates the infection has spread to the uterine cavity,
- Vaginal bleeding,
- History of septic shock,
- History of jaundice, oliguria and anuria,
- The gravid uterus is felt as if it were small, firm, and tender with movement.
- Foul purulent discharge from the uterus.
Diagnostic Evaluation:
The two main investigations of septic abortion are:
Routine Investigation,
Special Investigation
Routine Investigation:
- Cervical and upper vaginal swabs are taken before internal examination (to find out the dominant micro-organism).
- Blood test to estimate Hb.
- WBC – Total and Differential Count.
- Culture and Urinalysis.
- ABO and Rh grouping.
Special Investigations:
Pelvis and Abdomen Ultrasonography,
Pelvis and Abdomen X ray,
Blood Study: Culture, Serum Electrolyte, and Coagulation Profile.
Grading:
Septic abortion is generally divided into three grades.
1) Grade 1: In this the infection is usually localized in the uterus and is usually associated with spontaneous abortion.
2) Grade 2: In this the infection usually spreads to the pelvic structures.
3) Grade 3: In this the infection usually spreads to the generalized peritoneum i.e. peritoneum or sometimes a condition of septic shock may also arise.
Management:
- Management of the condition of a patient with septic abortion usually depends on the severity of the patient’s condition.
- Obtain a high-quality vaginal or cervical swab culture, medication sensitivity test, and Gram stain from the mother.
- A vaginal examination is performed to note the condition of the abortion. If the product of conception is found loose in the cervix, it should be removed with sponge holding forceps.
- Overall assessment of the case and grading for further treatment is done.
- Properly conduct all investigations of the patient.
- Properly treat the patient to remove sources of infection and sepsis.
- Properly provide supportive therapy to the patient. Provide.
- Provide maternal supportive therapy to restore normal homeostatic and cellular metabolism.
- Grade I or mild septic abortion: Drug of choice or antibiotic used is capsule.
- Ampicillin/amoxicillin (Mox, Coymox)
500 mg TDS × 7 days
cap. Cephadroxil (Cephodar) 500 mg BD × 7 days
cap. Chloromycetin 500 mg 6 hourly x 7 days. - When giving Cap.Chloromycetin. Blood tests are done for Hb, TLC, DLC and platelets.
- In Grade 1, prophylactically anti-gas gangrene serum 8000 units and antitetanus serum 3000 units I/M are given.
- Analgesic and sedative medications are given as per the doctor’s prescription.
- To minimize oliguria, anemia or shock, blood transfusion is done.
- Grade 1 After providing antibiotics after abortion, perform incomplete evacuation within 24 hours.
- When performing curettage, maintain gentleness to prevent injury.
- The medicine given in Grade II is according to the type of organism, i.e. Gram positive and Gram negative. For Gram positive:
- inj. Aqueous penicillin G5 million units every 6 hours.
Inj. Ampicillin 0.5-1 g IV every 6 hours. - For Gram Negative:
Inj. Gentamicin 1.5 mg/kg IV every 8 hours.
Inj. Ceftriaxone 1.5 IG, IV every 12 hours. - For Anaerobes:
Inj. Metronidazole 500 mg IV every 8 hours.
Inj. Clindamycin 600 mg IV every 6 hours. - Properly monitor the mother’s vital signs.
- Uterus is emptied by suction evacuation with antibiotic treatment within 6 hours.
- If the uterus and intestines are injured, laparotomy is performed.
- If the uterus is injured or infected, hysterectomy is performed.
- When the infection is localized to the pouch of Douglas, a posterior colpotomy is performed.
- In grade III, it is referred to as severe septic abortion with antibiotic therapy. The mother is resuscitated and fluid and electrolyte balance is maintained.
- Laparotomy is performed by an experienced surgeon, simple drainage of pus is also effective.
Recurrent abortion or habitual abortion:

- When a sequence of three or more spontaneous abortions occurs before 20 weeks of pregnancy, it is called recurrent abortion. It is caused by immunoglobulin G, hormonal deficiency, and cervical incompetence. Other causes include
- Genetic factors,
- Infection,
- Endocrine and anatomical abnormalities.
Etiology (Etiology):
- Due to genetic chromosomal error,
- Due to anatomical defect,
- Such as cervical incompetence and uterine anomalies,
- Uterine infection,
- Endocrine Disorder,
- Immunological Factor,
- Idiopathic
Sign And Symptoms:
- Absent fetal heart sound,
- Multiple spontaneous abortions (recurrent)
Diagnostic Evaluation (Diagnostic Evaluation) :
- History Collection,
- Physical Examination,
- VDRL Test,
- Thyroid Function Test,
- ABO and RH Grouping,
- Topzoplasma IgG and IgM,
- Ultrasonography,
- Hysterosalpingography,
- Hysteroscopy,
- Laparoscopy,
- Endocervical Swab,
- Semen Analysis.
Management (Management ):
- Collect and properly record the complete history of the patient in the non-pregnant state.
- Assess the patient’s general health status.
- Perform pelvic examination to assess cervical incompetence.
- Perform laboratory tests such as blood test, urine test, cervical culture,
hysteroscopy, ultrasonography, and dilation and curettage (D&C) to look for uterine cavity abnormalities. - Treat any infection during post-conception.
- Emphasize health promotion in proper prenatal care of the patient.
- If the patient has cervical incompetence, perform cerclage operation, Sirodkar or Mc Donald operation. Then remove the stitches at or before the 38th week.
- If the mother has a bleeding condition, report it immediately.
- Provide the patient with regular antenatal checkups and education for hospital delivery.
- Management of abortion involves comprehensive care and support for the woman undergoing termination of pregnancy, whether it is spontaneous (miscarriage) or induced (therapeutic) abortion.
- History Collection
Collect a complete history of the woman’s medical, obstetric and gynecological conditions. - Assess the gestational age of the pregnancy, identify the reason for the abortion.
- Monitor the mother’s complete vital signs, including blood pressure, pulse, respiration, and temperature, properly and continuously.
- Assess the client for any signs of hemorrhage, such as excessive bleeding, pallor, etc.
- Perform an abdominal examination to assess the tenderness of the uterine cavity.
- Perform a pelvic examination to assess cervical dilation and the presence of products of conception in the uterine cavity.
- Provide proper emotional support and counseling to the mother and family members.
- Advise the patient to explain and express his/her feelings.
- Provide education about available resources for psychological support, such as support groups and counseling services.
- Provide prescribed analgesic medications, such as NSAIDs or Acetaminophen, to relieve the patient’s pain.
- Advise the patient on the use of nonpharmacological measures, such as heating pads and relaxation techniques, to relieve the patient’s pain.
- Assess the patient for signs of excessive erections.
- Properly assess the amount of blood loss in the mother and prepare for blood transfusion if the patient needs it.
- Assess the patient for signs and symptoms of infection such as fever, foul smelling discharge, and lower abdominal pain.
- Properly assess the patient for signs and symptoms of infection such as fever, foul smelling discharge, and lower abdominal pain.
- Provide adequate antibiotic medication to the patient as prescribed.
- Properly monitor the patient for signs of incomplete abortion such as continued heavy bleeding and cramping pain.
- Prepare the patient for possible surgical intervention such as dilation and curettage (D & C).
- Provide patient education about signs and symptoms that require immediate medical care, such as heavy bleeding, pain, and fever.
- Provide instructions to maintain perineal hygiene to prevent and treat infection.
- Advise patient to schedule a follow-up appointment one to two weeks after abortion to properly assess complete recovery.
- Provide patient complete education about the importance of follow-up visits.
- Provide patient information about available contraceptive options to prevent unintended pregnancy.
- Provide education to the patient regarding the timing of use of contraceptives after an abortion.
- Discharge planning should ensure that the patient is able to go home and that adequate support and a safe environment are available at home.
- Provide written instructions that include information about the use of meditation, activity restrictions, and signs of complications. Provide information about support services and resources available in the community.
- Properly and accurately document all assessments, interventions, patient responses, and education provided.
- Recording the patient’s emotional states and providing counseling and psychological support.
- Nurses play a critical role in the comprehensive management of women who have had an abortion, which involves providing compassionate care, ensuring the patient’s physical and emotional well-being, and providing education to the patient about post-abortion care and contraceptive options.
- Proper assessment, monitoring, and intervention of the patient can prevent complications and facilitate the recovery process.
- Proper management of abortion plays an important role in improving the well-being of the mother.
Induced abortion:
- Induced abortion is the termination of pregnancy voluntarily using any medical or surgical procedure.
Medical Termination of Pregnancy (MTP)
- Medical termination of pregnancy is a medical procedure in which a woman, taking into account certain criteria, terminates her pregnancy to maintain her health or well-being. Termination can be done.
- Termination of pregnancy before the stage of viability of the fetus by medical or surgical method is called induction of abortion, it is legal or illegal. Abortion was legalized in India as medical termination of pregnancy in August 1971 and it was implemented from April 1972 and revised in 1975.
Indication
- When the woman’s life is in danger and her physical and mental health is seriously damaged.
- There is a risk of physical and mental abnormalities in the child.
- In a condition where the child has any congenital anomaly.
- Pregnancy is due to rape.
- The mother’s health is damaged due to social or economic reasons and Contraceptive measures have failed.
- As per Indian law, abortion is allowed up to 20 weeks. In pregnancy up to 12 weeks, the opinion of one registered medical practitioner is required and in 12 to 20 weeks, the opinion of two registered medical practitioners is required.
- The written consent of the patient and in cases where the patient is under 18 years of age or mentally handicapped, the consent of the guardian is required.
Contraindications
- Uncontrolled blood pressure greater than 160/100,
- Cardiovascular disease,
- Women over 35 years of age,
- Severe renal failure, liver disease, or respiratory disease
- Use of systemic corticosteroids,
- Coagulopathy or woman receiving anticoagulant therapy,
- Mother has anemia,
- Uncontrolled seizure disorder.
Who can perform medical termination of pregnancy?:
- The Chief Medical Officer or Civil Surgeon grants permission for medical termination of pregnancy to the following doctors:
- Holding a Post Graduate Degree or Diploma in Obstetrics and Gynaecology.
- Six months training as a resident in Obstetrics and Gynaecology.
- One year of experience in the Department of Obstetrics and Gynaecology.
- Assisted a Registered Medical Practitioner in 25 cases of Medical Termination of Pregnancy (MTP).
Place for MTP (Medical Termination of Pregnancy):
- The hospital is established or maintained by the Government or the Chief Medical Officer or Civil Surgeon has approved the place.
Records:
Recording Medical Termination of Pregnancy in the Form. Confidentiality should be maintained and the report should be made to the Director of Health Services.
Penalty:
A person who does not comply with this Act can be punished with imprisonment for a term of 2 to 7 years.
Methods of Medical Termination of Pregnancy (MTP):
First Trimester (Up to 12 weeks):
Medical
Pregnancy is terminated using medications such as,
Mifepristone,
Mifepristone and Misoprostol,
Mithotrexate and Misoprostol,
Tamoxifen and misoprostol.
Surgical
Pregnancy is terminated using surgical procedures such as,
Menstrual regulation, vacuum aspiration,
Suction evacuation and curettage,
Dilatation and evacuation.
Second Trimester (13-20 weeks):
Prostaglandins,
Dilation and evacuation,
Intrauterine instillation of hyperosmotic solutions,
Oxytocin infusion,
Hysterotomy.
Complications:
A complication is usually a medical termination of pregnancy. Pregnancy (MTP) depends on the method used.
Immediate complications
Cervical lacerations,
uterine perforation,
Hemorrhage,
Shock,
Thrombosis,
Embolism,
Post-abortal triad of pain, bleeding and low grade fever may occur and depends on the method used in medical termination of pregnancy.
Remote
Gynecological complications,
Obstetric complications,
Failed Abortion,
ectopic pregnancy etc.
Nursing Role with the Patient Undergoing MTP:
- The nurse should provide comfort and support to the mother and her family members and provide proper reassurance by clearing all their queries.
- If the mother has decided to have an abortion, then obtain her written permission along with the consent of her husband and the patient.
- Continuous monitoring of the patient and support should be provided before, during and after the procedure for medical termination of pregnancy.
- Provide proper education to the mother about the complications that may arise after abortion, such as,
continuous vaginal bleeding with clots for three weeks after abortion,
fever, continuous pain, and burning urination, etc. - Advise the woman that the first menstruation starts between 2 and 8 weeks after abortion.
- Advise the woman that if lactation starts, it should be mild It is in the amount and if the breast is not stimulated, it lasts only for 48 hours.
- Provide them with education or come for a follow-up visit two to eight weeks after the medical termination of pregnancy (MTP) to ensure that the reproductive organs have returned to their pre-pregnancy state.
- Thus, in medical termination of pregnancy, the pregnancy is terminated.
Anti Partum Hemorrhage (APH):
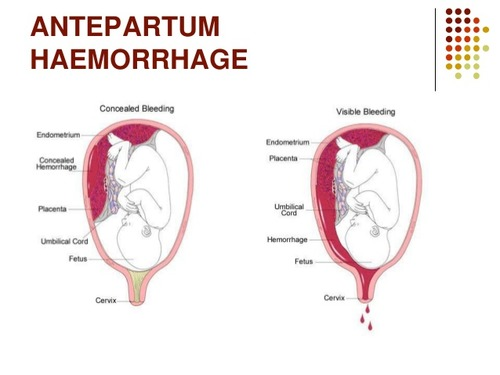
- If bleeding occurs from the genital tract after the 28th week of pregnancy but before the birth of the child, this condition is called APH (antepartum hemorrhage).
Or
“Bleeding from or in the genital tract that starts from the 24th week of pregnancy and occurs before the birth of the child” This condition is called antepartum hemorrhage (APH). - It can be caused by various conditions such as placenta previa (where the placenta is abnormally implanted low in the uterine cavity) or placental abruption (where the placenta separates prematurely from the wall of the uterine cavity).
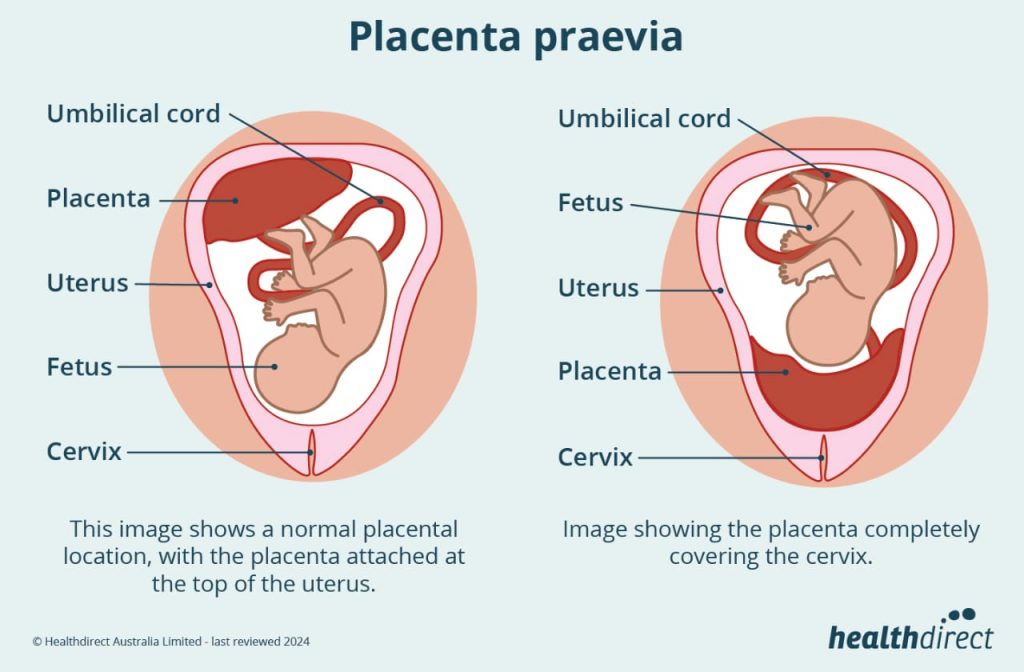
Placenta Previa (Placenta Previa) :
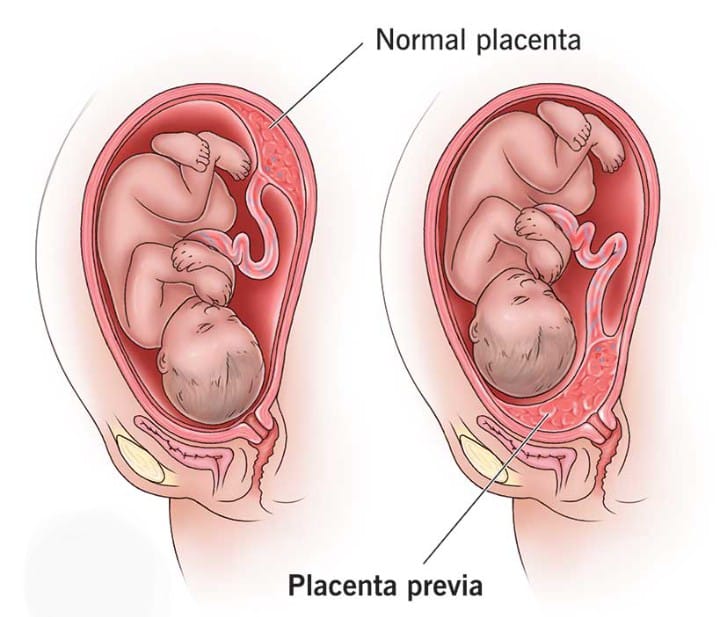
- When the placenta Partially or completely implanting near or above the internal os of the lower segment of the uterus is called “placenta previa” . 1/3 of cases of antepartum hemorrhage are due to placenta previa.
Etiology:
- The exact cause of placenta implantation in the lower uterine segment is unknown.
- Some theories are given below:
Dropping Down Theory:
- According to this theory, the fertilized ovum drops down into the lower uterine segment and implants in the same location.
Persistence of Chorionic Activity
- It explains the formation of capsular placenta from chorion coming into contact with decidua vera of lower segment of uterus.
Defective decidua
- In this chorionic villi spread over a large area of uterine wall to obtain nourishment
- During this process, not only does the placenta become membranous but it can also implant in the lower part of the uterus.
Large surface area of the placenta:
Large surface area such as twins also causes the placenta to implant in the lower segment.
High risk factor:
Multipara.
Increases Maternal age
( > 35).
History of previous lower segment cesarean section (L.S.C.S).
Any other scar present in the uterus.
Big placental size and abnormality,
Placental hypertrophy due to smoking,
Previous curettage.
Types Of Placenta Previa (Types Of Placenta Previa):
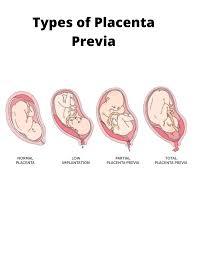
There are four types of placenta previa depending on the degree of extension of the placenta into the lower segment of the uterine cavity.
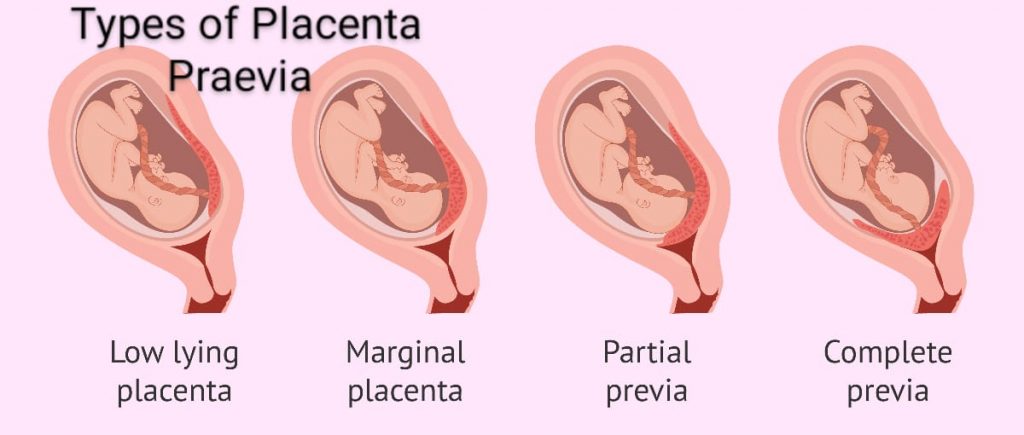
1) Type I (Lateral placenta previa),
2) Type II (Marginal placenta previa),
3) Type III(Incomplete placenta previa),
4) Type IV(Complete placenta previa)
1) Type I (Lateral placenta previa):
In this type, the major part of the placenta is attached to the upper segment but only the lower margin enters the lower segment but does not reach the OS.
2) Type II (Marginal Placenta Previa):
In this type, the placenta only reaches the margin of the internal os but does not cover it. If the placenta is anterior, vaginal birth is possible. Blood loss is average. The risk of fetal hypoxia is higher than maternal shock.
3) Type III (Incomplete Placenta Previa):The placenta partially covers the internal os, but not centrally, while in late pregnancy the cervix eaves and dilates. Bleeding occurs due to the lowers stretching as they begin to occur.
4) Type IV (Complete Placenta Previa): In this, the placenta covers the internal os even when it is fully dilated. Severe hemorrhage requires a cesarean section to save the life of the mother and baby.
Sign And Symptoms:
- Symptoms
Vaginal bleeding,
Bleeding that occurs suddenly.
Bleeding that is painless.
Bleeding that is causeless.
Bleeding that is recurrent.
Bleeding that is accompanied by activity Unrelated and often occurs during sleep and the patient wakes up startled to find herself in a pool of blood. - In placenta previa, the blood is bright red because of bleeding from the separated ytero-placental sinus. Signs
The patient has evidence of late pregnancy.
There is also evidence of blood loss such as shock, anemia depending on the degree of hemorrhage.
Abdomen
The size of the uterus is according to the gestational period.
The uterus feels soft, relaxed, and elastic.
Breech, transverse, unstable lie is seen as malpresentation
The head is floating.
Fetal heart sounds are usually present.
Bright red blood is seen in placenta previa.
Diagnostic Evaluation:
Diagnostic evaluation is done by two methods:
1) Placentografy,
2) Clinically
1) Placentografia:
- a)Sonography: Trans Abdominal Ultrasound
- (TAS).
- Trans Vaginal Ultrasound
- (TVS).
- Transperineal ultrasound.
- Magnetic resonance imaging (MRI),
- Radiography,
- Radioactive isotope,
2) Clinically:
- By internal examination (double set-up examination),
- Direct visualization during cesarean section,
Management of placenta previa:
Principles of management of placenta Prev
- To prevent injuries to the feet,
- To reduce the risk of infection,
- To control vaginal bleeding,
- To promote health and reduce anxiety.
Management:
- Provide adequate antenatal care to the patient to improve the health status of the mother.
- To confirm the type of placenta previa, perform an ultrasound at 20 weeks and then repeat the ultrasound at 34 weeks.
- Ask the pregnant woman to take bed rest and then gently palpate the uterus for tenderness and tone.
- Properly assess the amount of blood loss.
- Color of bleeding and complete blood count (CBC) test should be done.
- Provide the patient with inj. Morphine 15 mg IM as per hospital policy and prescription.
- Properly assess the amount of blood loss in the client.
- Properly note the client’s vital signs such as,
temperature,
pulse,
respiration,
blood pressure. - Properly assess the client for anemia.
- Regularly and frequently check the fetal heart sound.
- Perform abdominal examination of the pregnant woman, then note the fetal heart sound and properly note whether there is any tenderness present in the uterus.
- Do not perform vaginal examination in the condition of placenta previa as it may increase bleeding.
- Properly monitor the pregnant woman for continuous bleeding or if it stops in between.
- If the pregnant woman needs it, arrange for further well-equipped hospital shift to a hospital with blood transfusion facility available, cesarean section facility and neonatal care unit.
- If the client has a condition of hemorrhage, start intravenous dextrose normal saline drips.
- Advise the client to avoid stress and advise him to take complete bed rest.
- When the client is admitted to the hospital, follow the following treatment such as,
- Give immediate attention,
- Then plan properly what kind of treatment is required.
- In the immediate assessment, the amount of blood loss, general condition, pallor, pulse rate and blood pressure should be properly noted.
- Blood samples should be sent to the laboratory immediately for cross-matching and assessment of hemoglobin level.
- Start infusion of normal saline to the patient.
- After cross-matching of blood, keep the blood ready for transfusion.
- Perform gentle abdominal palpation to assess whether any active bleeding is present.
- Formulation of line of treatment:
In this, proper treatment should be provided according to the condition. - Proper estimation of hemoglobin level should be done and it should be 10 gm or more.
- Expectant treatment should be provided till 37 weeks are completed.
- Termination is performed in case of any of the following conditions:
Recurrent hemorrhage,
Dead fetus,
Congenital malformation of fetus,
Intrauterine growth retardation (IUGR),
In such conditions, termination is performed. - After admission to the hospital, specific treatment is started. For example, vaginal examination is performed in the operation theater after preparing properly for cesarean section.
- After examination, artificial rupture of membranes is done, then oxytocin is started, and then delivery is conducted as per the condition.
- If the labor process is progressing satisfactorily without any bleeding, then perform vaginal delivery.
- If bleeding is continuous, perform cesarean section on the pregnant woman.
- If the baby is malformed or dead, assess its presentation, if it is breech presentation, perform ventouse delivery, and if it is breech, perform breech delivery.
Abruptio placenta:
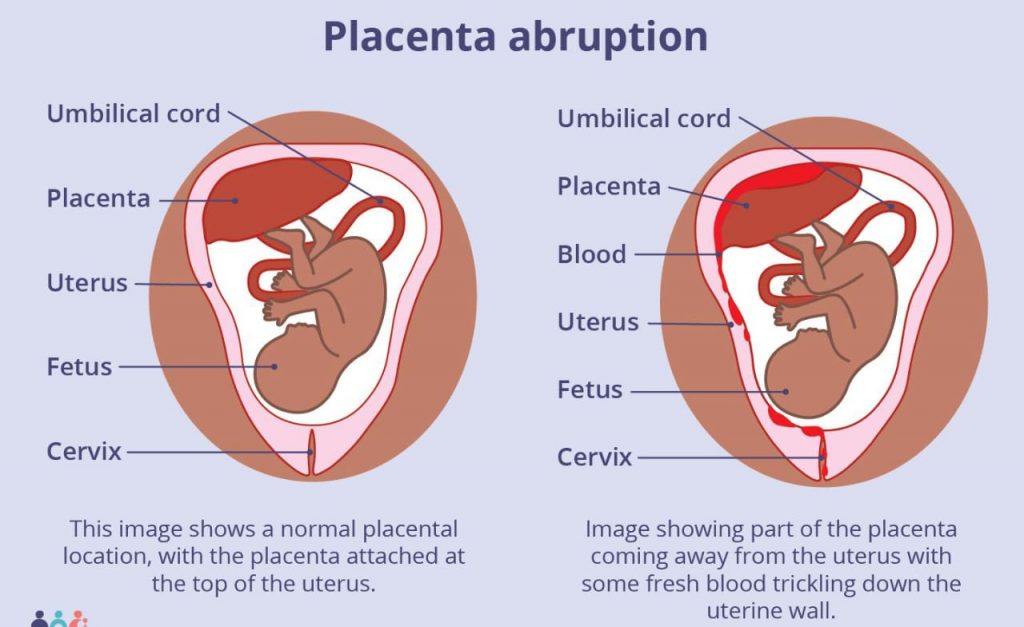
Definition:
- Placenta abruptio is a form of antepartum hemorrhage (APH) in which the normally situated placenta prematurely separates from the uterine wall, causing bleeding called placental abruption.
Types Of Abruptio Placenta:
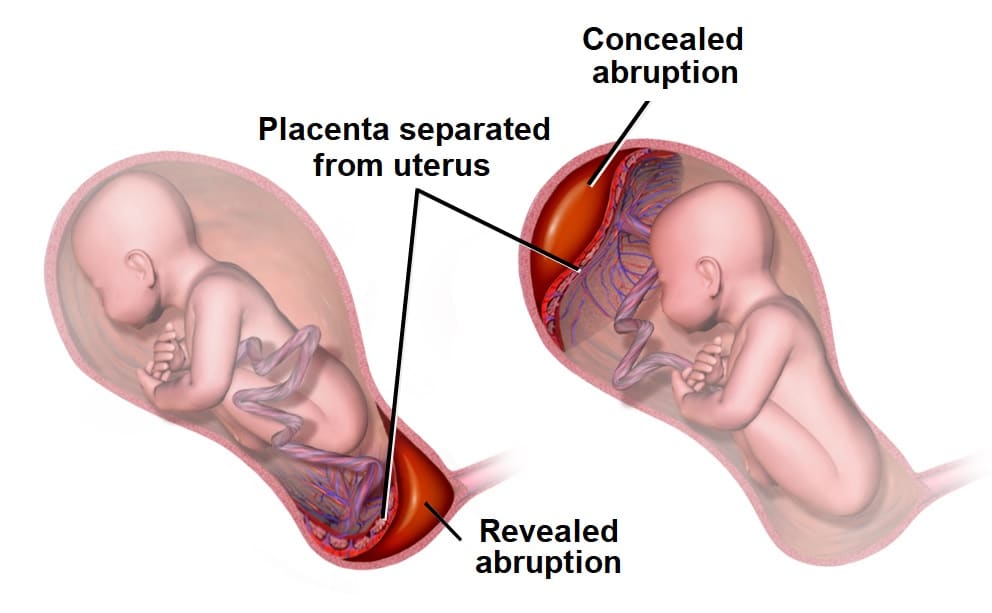
There are mainly 3 types of placental abruption, such as,
1)Revealed,
2)Concealed,
3)Mixed.
1)Revealed or Mild Type: In this type, after the separation of the placenta, the blood comes downwards from between the membrane and the decidua, that is, the blood is externally visible. This type is a common type of abruptio placenta.
2) Concealed: In this concealed type of abruptio placenta, the blood collects behind the separated placenta or between the membrane and the decidua, that is, the blood is not externally visible. This type is a rare type of abruptio placenta.
3)Mix: In this type, the blood is collected in a small amount (concealed) and is visible outwards (revealed), meaning that both revealed and concealed types of placental abruption are seen. It is called mixed abruptio placenta.
Etiology:
- The exact cause is unknown,
- It is more common in the 5th trimester,
- Due to the advanced age of the mother,
- Due to poor socioeconomic conditions,
- Malnutrition,
- Smoking.
- Other factors such as,
- Preeclampsia,
- Sudden uterine decompression,
- Short cord,
- Supine hypotensive syndrome,
- Folic acid deficiency,
- Due to torsion of the uterus,
- Due to direct trauma to the uterus, high parity or uterine overdistension.
Risk Factores:
- Short cord,
- Due to premature rupture of membranes,
- Due to uterine leiomyomas,
- Chorioamnionitis,
- Polyhydramnios,
- Anticoagulant Therapy,
- Cocaine use,
- Smoking,
- Due to trauma to the abdomen,
- Hypertension,
- Due to intrauterine growth retardation (IUGR),
Diagnostic Evaluation (Diagnostic Evaluation) :
- History collection,
- Physical examination,
- Blood test e.g. hematocrit, urea, electrolytes
- Fibrinogen level, thromboembolin time, blood group and To assess cross match.
- Urine Examination,
- Placentography,
- Ultrasound,
- Cardiotocography.
Sign And Symptoms (Sign And Symptoms) Symptoms):
- Painful vaginal bleeding,
- Tender board-like uterus (especially when vaginal bleeding is concealed hemorrhage),
- Fetal bradycardia and late decelerations,
- Fetal heart rate (FHR) absent,
- Signs of shock are present.
- Bleeding occurs due to preeclampsia or trauma.
- Bleeding can be visible, invisible, and mostly mixed.
- The blood is of dark red color.
- In this, the condition of anemia is seen more than the amount of visible blood loss.
- Features of preeclampsia in placental abruption are seen in 1/3 of the cases.
- In placental abruption, the height of the uterus is larger than the gestational age.
- In placental abruption, the uterus may be tense, tender, and rigid.
- In placental abruption, malpresentation is unrelated and the head may also be engaged.
- Heart sounds are often absent in placental abruption.
- The placenta is found in the upper segment of the uterus.
Management:
Prevention:
- The objectives of prevention are as follows, such as,
Eliminate the causes responsible for placental separation.
Early identify preeclampsia and hypertensive disorders and provide effective treatment for them.
Properly correct anemia in the patient.
Start early treatment to prevent complications in the patient.
Avoid trauma, sudden decompression of the uterus, supine hypotension. - Immediately shift the patient to the maternity hospital.
- Completely assess the patient in the hospital.
- Properly assess the amount of blood loss in the patient.
- Properly assess the maturity of the fetus.
- Properly assess the patient’s general condition.
- Perform a complete diagnostic evaluation of the patient. Such as, blood hemoglobin level,
hematocrit level,
coagulation profile,
ABO and RH grouping, urine analysis. - Provide the patient with Ringer’s latest (RL) solution.
- Prepare the patient for blood transfusion properly.
- Closely monitor maternal or fetal condition.
- Prepare the patient for delivery.
- Manage any complications if the patient has them properly.
- Definitive treatment: If the patient is in labor, perform low rupture of membranes, if necessary, start oxytocin drip, then vaginal delivery, then delivery.
- Provide adequate antenatal care to the patient to improve the health status of the mother.
- Ask the pregnant woman for bed rest and then gently palpate the uterus for tenderness and tone.
- Properly assess the amount of blood loss.
- Check the color of the bleeding and perform a complete blood count (CBC) test.
- Properly assess the amount of blood loss in the client.
- Properly note the client’s vital signs such as,
temperature,
pulse,
respiration,
blood pressure. - Properly assess the client for anemia.
- Regularly and frequently check the fetal heart sound.
- Perform abdominal examination of the pregnant woman, then note the fetal heart sound and properly note whether any tenderness is present in the uterus.
- Properly monitor the pregnant woman for continuous bleeding or if it stops in between.
- If the pregnant woman needs it, arrange for further well-equipped hospital shift to a hospital with blood transfusion facility available, cesarean section facility and neonatal care unit.
- If the client has a condition of hemorrhage, start intravenous dextrose normal saline drips.
- Advise the client to avoid stress and advise him to take complete bed rest.
- When the client is admitted to the hospital, follow the following treatment such as, immediate attention,
- Then plan properly what kind of treatment is required.
- In the immediate assessment, the amount of blood loss, general condition, pallor, pulse rate and blood pressure should be properly noted.
- Blood samples should be sent to the laboratory immediately for cross-matching and assessment of hemoglobin level.
- Start infusion of normal saline to the patient.
- After cross-matching of blood, keep the blood ready for transfusion.
- Perform gentle abdominal palpation to assess whether any active bleeding is present.
- Formulation of line of treatment:
In this, proper treatment should be provided according to the condition. - Proper estimation of hemoglobin level should be done and it should be 10 gm or more.
- Expectant treatment should be provided till 37 weeks are completed.
- Termination is performed in case of any of the following conditions:
Recurrent hemorrhage,
Dead fetus,
Congenital malformation of fetus,
Intrauterine growth retardation (IUGR),
In such conditions, termination is performed. - After admission to the hospital, specific treatment is started. For example, vaginal examination is performed in the operation theater after preparing properly for cesarean section.
- After examination, artificial rupture of membranes is done, then oxytocin is started, and then delivery is conducted as per the condition.
- If the labor process is progressing satisfactorily without any bleeding, then vaginal delivery should be performed.
- If bleeding is continuous, then advise the pregnant woman to perform cesarean section.
- If the baby is malformed or dead, then assess its presentation, if it is breech presentation, then perform ventouse delivery, and if it is breech, then perform breech delivery.
- If the patient has any complications, then properly assess them and take proper measures to prevent them.
Vesicular mole :
Definition:
- Vesicure mole is also called hydatidiform mole (H. mole). It is an abnormal condition of the placenta. In which some degenerative and some proliferative changes occur in the young chorionic villi, and due to this, a cluster (cluster-like shape) is formed in the cyst. And because it resembles a hydatid cyst, it is called a hydatidiform mole (H. mole) or a vesicular mole. When the chorionic villi transform into a mass of translucent vesicles, they form a structure resembling a bunch of grapes, which is called a hydatidiform mole.
Etiology:
- Its exact cause is unknown,
- Due to ovulatory defects,
- It can also be caused by the following reasons:
- Hemorrhagic pregnancy,
- More common in teenage pregnancies,
- In women over 35 years of age,
- Due to faulty nutritional habits such as low Due to excessive protein intake,
- Due to low calorie intake in the diet,
- Due to disturbed maternal immune mechanism,
- History of hydatidiform mole,
- Women who have had ovulation simulated by clomiphene,
- Poor socioeconomic condition have.
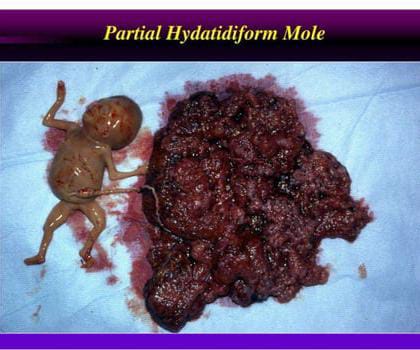
Type of vesicular mole:
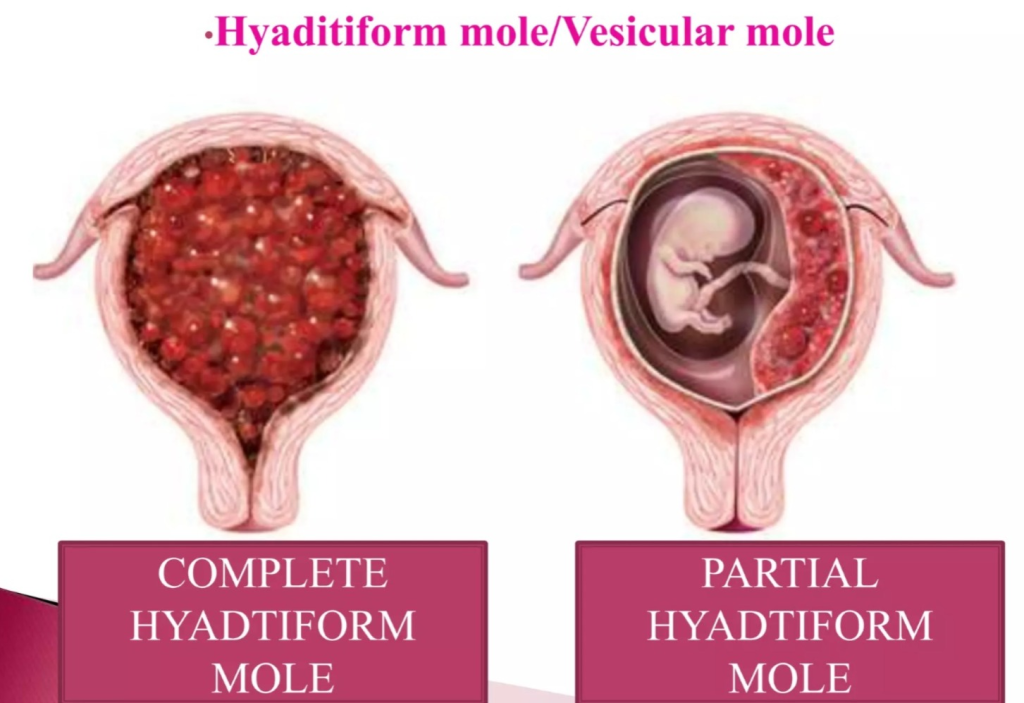
There are two types of vesicular moles:
1) Complete mole,
2) Incomplete mole
1) Complete mole: A complete or classic H. mole occurs when an egg whose nucleus is lost and inactivated undergoes fertilization. It forms due to the formation of a mass.
In this, the mole resembles a bunch of white grapes.
In this, the fluid-filled vesicles grow rapidly, causing the uterus to become larger than the expected duration of pregnancy.
In a complete mole, the fetus, placenta, and amniotic membrane are involved.
A complete mole can also progress to carcinoma and does not contain an embryo.
2) Incomplete mole
It contains embryonic or fetal parts and the amniotic sac is present It is.
Congenital anomalies are present.
It contains an underdeveloped embryo that fails to survive.
Sign And Symptoms:
- Abnormal vaginal bleeding,
- Bleeding may appear brownish and watery because the blood mixes with the fluid coming out of the ruptured system, giving the appearance of blood as a discharge.
- In this case, Painless vaginal bleeding is seen during the fourth and fifth months of pregnancy.
- Lower abdominal pain.
- The patient appears to be ill for no apparent reason.
- Hyper emesis gravidarum occurs.
- Early features of pre-eclampsia are seen in a period of less than 20 weeks.
- Dyspnea occurs due to pulmonary embolism.
- The uterus appears larger than for the gestational period.
- Thyrotoxic features are seen such as,
- Tremors, and anxiety etc.
- Fetal heart sounds and fetal patency are absent.
- Expulsion of grape-like vesicles from the vaginal area.
- USG:=Snow storm appearance is seen.
Diagnostic Evaluation:
- Full blood count,
- ABO and Rh grouping and blood clotting tests,
- Hepatic, renal and thyroid function tests,
- Sonography,
- Straight X-ray abdomen,
- Pelvic angiography,
- CT scan and MRI.
Management:
- Provide proper supportive therapy to the mother to restore lost blood.
- When a vesicular mole is diagnosed, evacuation by suction and surgical curettage as early as possible can prevent the risk of choriocarcinoma.
- Test ABO and Rh in the mother’s blood investigation.
- Immediately Start fluid infusion.
- If there is excessive blood loss, provide blood transfusion to the mother.
- Empty the uterus by suction procedure i.e. suction the mole.
- After the suction is complete, when no vesicles come in the suction cannula and the uterine cavity contracts, start 10 units of oxytocin by adding it to the glucose drip and introduce 0.2 mg of metharazine in the drip.
- Avoid oxytocin during suction procedure as it embolizes the vesicles in the patient’s venous channel.
- Cure the uterine cavity gently and properly by blunt curettage.
- After curetted, send the vesicles to the laboratory for histological examination.
- Properly monitor the mother’s vital signs such as pulse rate, respiration, and blood pressure every half hour. To assess.
- The mother should be given 10 units of oxytocin intramuscularly (IM) or if intravenously (IV) infusion is to be given, 20 units of oxytocin in 500 ml of normal saline or Ringer’s solution should be administered to the patient to prevent postpartum hemorrhage.
- If the patient is above 40 years of age, advise the patient to undergo hysterectomy.
- Advise the mother to have regular follow-up Give.
- If the mother is Rh negative, administer Anti D immunoglobulin 100 microgram (IM).
- Advise the woman to use a proper contraceptive method.
- Advise the mother to avoid pregnancy for one year.
- Advise the mother to follow up for at least two years. Its aim is to find out choriocarcinoma.
- Advise women to follow up after 4 to 6 weeks and then every 3 months for at least 2 years. This includes collecting the woman’s history and conducting a clinical examination.
Hyperemesis gravidarum:
- Severe nausea and vomiting during pregnancy that can have a negative impact on the mother’s health, leading to dehydration, weight loss, and electrolyte imbalance, and impairing the mother’s daily routine activities. This condition is called “hyperemesis gravidarum”.
- Hyperemesis gravidarum (HG) usually occurs during the first trimester of pregnancy, usually starting around 4-6 weeks of pregnancy and symptoms last for about 9-13 weeks. This period corresponds to the time when pregnancy hormones, especially human chorionic gonadotropin (hCG), are at their highest levels.
- In most cases, symptoms of hyperemesis gravidarum begin to improve by the end of the first trimester, although some women may experience symptoms that persist into the second trimester or throughout pregnancy in severe cases. Nausea and vomiting are very common in primigravidas and are especially common when the woman wakes up in the morning.
- Vomiting is caused by hormones such as HCG, Oestrogen, and Progesterone. Nausea and vomiting are commonly seen in primigravida and the first trimester. If persistent vomiting persists, it can lead to dehydration, electrolyte imbalance, and vomiting and aspiration.
Etiology:
- Hormonal causes: Due to chronic increase in the amount of gonadotrophin, estrogen, and progesterone hormones,
- Psychogenic,
- Due to deficiency of vitamin B, carbohydrates, and proteins,
- Allergic/Immunological
Sign And Symptoms:
- Nausea,
- Forceful vomiting,
- Abdominal pain,
- Electrolyte imbalance,
- Fever,
- Fatigue,
- Loss of appetite,
- Dehydration,
- Changes in bowel movements,
- Irritability,
- Lethargy,
- Malnutrition,
- Dehydration and ketoacidosis Symptoms: Dry coated tongue, sunken eyes, systolic blood pressure less than 100 mm Hg, acetone odor on breath, tachycardia, hypotension, increased temperature. Jaundice is a late feature.
Diagnostic Evaluation:
- History Collection
- Take a proper history of the frequency, duration and amount of vomiting.
- Properly assess body weight.
- Laboratory investigation.
- Complete blood count test (CBC).
- Assess electrolyte levels.
- Perform urine analysis.
- Properly assess blood glucose levels.
- Properly assess liver function tests.
- Imaging studies.
- Abdominal ultrasound.
Management:
- If the woman has a condition of severe hyperemesis gravidarum, she should be properly hospitalized.
- Properly assess the woman.
- Properly assess the woman’s hydration status.
- Properly assess the woman’s electrolyte balance and continuously observe the woman.
- Continuously assess the consistency, frequency, and duration of the woman’s vomiting.
- Properly assess the woman’s hydration status and properly assess the woman’s vital signs.
- Provide intravenous fluids to maintain the woman’s hydration status and prevent electrolyte imbalance.
- Provide the woman with prescribed antiemetic medication. Such as, promethazine (Phenergan), prochlorperazine (Stematil), triflupromazine (Sequil), metaclopramide, hydrocortisone, etc.
- Properly investigate the woman’s blood.
- Provide the woman with small amounts of easily digestible bland food if vomiting subsides.
- Provide proper comfort measures to the woman.
- Properly maintain the patient’s fluid and electrolyte balance.
- Advise the woman to maintain proper hygienic conditions.
- Maintain the patient’s proper intake-output chart.
- Use proper aseptic technique and maintain universal precautions to prevent cross-infection.
- Work with other health care personnel for proper care of the woman. Collaborate.
- Provide education to parents to provide proper medication to the woman.
- If vomiting subsides, advise the patient to drink small amounts of water and also advise him to eat carbohydrate foods such as biscuits, bread and toast. Provide the patient with small and frequent feeds and then provide a full diet.
- Advise the woman to have regular follow-up.
Diabetes Mellitus:

- Diabetes is a chronic metabolic disorder in which carbohydrate, protein and lipid metabolism are impaired. Diabetes is a group of metabolic disorders in which the blood sugar level of a person’s blood is high. This is mainly due to any impairment in insulin secretion and insulin action in the body, so high blood sugar level is seen in the body. The ”3 P” syndrome is mainly seen in diabetes mellitus.

- 1)P: Polyuria (passing a lot of urine)
- 2)P: Polydipsia (excessive thirst),
- 3)P: Polyphagia (excessive hunger).
GDM Gestational Diabetes Mellitus :
- Gestational diabetes mellitus is mainly seen in women and even in those women, diabetes mellitus is seen during pregnancy due to glucose intolerance. Gestational diabetes refers to a woman who is diabetic during pregnancy. Gestational diabetes mellitus is a type of diabetes that occurs during pregnancy because hormonal changes during pregnancy cause resistance to insulin.
- Here, the mother does not have diabetes before pregnancy. Thus, if a woman develops diabetes during pregnancy, the condition is called gestational diabetes. This condition can affect the baby’s health and development in many ways, requiring careful monitoring and management immediately after birth to manage potential complications such as low blood sugar, respiratory problems, jaundice, and an increased risk of congenital anomalies.
Etiology:
- Inherited
Environmental factors
Genetic factors,
Obesity (Obesity),
During pregnancy due to hormonal imbalance.
Due to insulin deficiency.
Despite insulin, cells become resistant to insulin.
Due to excessive sugar intake.
Due to a sedentary lifestyle.
Due to excess cholesterol in the body.
The growing fetus is supplied with nutrients and water by the placenta. To maintain pregnancy, a number of hormones are produced (cortisol, estrogen, human placental lactogen) which can block insulin. This usually occurs between the 20th and 24th week of pregnancy. - On the other hand, the growth of the placenta also increases hormonal production, which increases insulin resistance. Normally, the pancreas produces extra insulin to counteract insulin resistance, but when insulin production is not enough to overcome the effects of placental hormones, gestational diabetes occurs.
- A woman with pre-existing diabetes has an increased need for insulin, e.g. Insulin dependent mothers may need more insulin as the pregnancy progresses.
Sign And Symptoms:
Effects of gestational diabetes on fitness:
- The effect of diabetes on fitness during pregnancy is a matter of concern because the increase in the mother’s blood sugar level during pregnancy can lead to This causes the child’s body to secrete more insulin, which causes tissue growth and fat deposition, causing the newborn to be larger than expected for the gestational age (macrosomia).
- Newborns of diabetic mothers are at risk of developing congenital anomalies. Congenital anomalies can cause problems in the heart, brain, spinal cord, urinary tract, and gastrointestinal system.
- Other conditions:
- Hypoglycemia,
- Macrosomy,
- Birth injury,
- Respiratory distress.
Signs and symptoms:
- Large size baby (due to excessive fat and glycogen accumulation in tissues),
- Face and cheeks,
- Hyperbilirubinemia,
- Signs of hypoglycemia:
- Twitching,
- Lethargy,
- Seizures,
- Difficulties in feeding,
- Apnea,
- Cyanosis.
- Signs of Respiratory Distress:
- Cyanosis,
- Nasal Flaring,
- Grunting,
- Tachypnea,
- Other Symptoms:
- The “3 P” syndrome is mainly seen in diabetes mellitus.
- 1)P: Polyuria (passing a lot of urine)
- 2)P: Polydipsia (excessive thirst),
- 3)P: Polyphagia (excessive hunger).
- Fatigue.
- Weakness.
- Visual impairment.
- Tingling and numbness sensation in hands and feet.
- Dry skin.
- Sores that heal slowly.
- Frequent infections.
- Nausea.
- Vomiting.
- Slow wound healing process
- Weight To decrease.
Diagnostic Evaluation (Diagnostic Evaluation) :
History Collection,
Physical Examination,
1) Fasting Blood Sugar (FBS)
This test is done without eating or drinking anything for at least eight hours. Its normal value should be less than 110 mg/dl milligrams per deciliter and if the fasting blood glucose level is more than 125 mg/dl milligrams per liter If it is present, it is diagnosed as diabetes.
Random blood sugar ( RBS )
In this test, the sample is taken at any time and no preparation is required. If the random blood glucose is more than 200mg/dl, it is indicated as diabetes.
PP2bs (Postprandial Blood Sugar)
This test is done 2 hours after taking a full meal. is subtracted.
Usually the blood glucose level returns to the fasting glucose level two hours after a meal, but if there is any smoking or drinking of caffeine, then there is an alteration in it.
glycosylated HB
This test is done to assess the amount of glucose attached to the blood molecule.
glycocilated Albumin:
Usually glucose is attached to albumin, so glycosylated albumin is It is used to assess the average glucose level.
oral glucose tolerance test.
In this, the patient is provided with 150 mg of carbohydrate for three days. Then the patient’s fasting blood glucose level is checked. Then the client is given 75 grams of glucose to drink, after which the patient’s glucose tolerance level is checked.
ketonuria
If ketones are present in the urine, it is a sign of body fat. It indicates that it is used as a source of energy.
proteinuria:
If protein is present in the urine, it indicates that protein is used as a major source of energy.
Serum lipid profile.
Serum BUN.
Serum creatinine.
Management:
- Principles of Management
- To eliminate the symptoms of hyperglycemia.
- To reduce the microvascular and macrovascular complications of diabetes mellitus.
- To reduce the blood glucose level.
- The patient can achieve a normal lifestyle as far as possible.
- Blood glucose level can be reduced by educating the patient, dietary management, and using exercise and pharmacological therapy.
- Patient Education
- Provide appropriate health education to the patient and his family members.
- Including teaching how to do glucose self-monitoring.
- Teaching the patient how to administer insulin.
- Teaching the management of hypoglycemia.
- Provide education to the patient about foot and skin care.
- Teach the management of diabetes before, during, and after exercise.
- Provide education to the patient about lifestyle modification.
- Properly check for any signs and symptoms of respiratory distress.
- Dietary management
- Aim of dietary management
- To relieve symptoms of hyperglycemia.
- To reduce symptoms of hypoglycemia if hyperglycemia is treated.
- To reduce overall blood glucose levels in the body.
- Avoid diets that increase blood glucose levels.
- If the patient is obese, advise him to lose weight.
- Make the patient take regular food intake.
- Tell the patient not to take sugar.
- Ask him to take a diet that contains adequate amounts of protein, carbohydrates and fat.
- The main goal of dietary management is to improve metabolic control in the diabetic client.
- Maintain the patient’s blood glucose level and lipid level.
- Make a daily food intake plan for the patient.
- Make a plan for the patient’s weight management.
- Provide adequate nutrition to the patient.
- A person’s lifestyle and habits play an important role in controlling and managing his disease.
- A balanced nutritional diet is very important for all patients.
- Ask the patient to take protein in his diet. Excessive protein intake increases renal function. And glomerular filtration rate increases.
- Maintain the level of fat in the patient’s diet. Maintain daily cholesterol level in the diet and limit saturated fat and cholesterol.
- Provide carbohydrates according to the patient’s body requirement.
- Ask the patient to take adequate amount of carbohydrates so that the energy requirement of the body can be maintained.
- Avoid foods that are sweet and contain sugar such as cakes, ice cream, jam etc.
- Check the patient’s blood glucose level regularly.
- Carbohydrates should be taken in small amounts before exercise.
- The patient should be asked to check the amount of glucose, ketones and albumin in the urine, all of which are found during fasting.
- Calorie restriction should be done for obese clients.
Exercise:
- Provide advice to the patient to do regular exercise to prevent his disease condition from getting worse.
- Ask him to walk regularly.
- Ask him to take adequate amount of carbohydrates before and after exercise.
- Pharmacological management is responsible for maintaining blood glucose levels.
- If insulin is given to the abdomen, its absorption is faster. When given on the arm and leg, its absorption decreases.
- The patient is provided with oral medication.
Oral antidiabetic agents:
- 1)sulfonyle uria,
- 2)meglitinides,
- 3)thiazolidinediones,
- 4)bigunides,
- 5)alpha glucoside inhibitor.
- Proper teaching should be provided to the patient for proper administration of insulin because if insulin is not administered properly, tissue damage or conditions like insulin shock can occur.
Nursing Management :
1)Impaired nutritional status more than body requirement related to intake inexcess of activity expenditure.
- The primary goal of a diet plan is to control glucose levels, so assess the patient’s glucose levels, and assess the patient’s lifestyle, cultural background, activity level, dietary habits, and food preferences.
- Instruct the patient to eat adequate amounts of food and to snack in between.
- The patient should eat an extra meal before engaging in physical activity. Make arrangements.
- Administer insulin as per doctor’s order.
2)imbalance fluid volume related to increased stress hormone as evidenced by polyuria.
- Assess patient’s intake output chart.
- For patient to take oral fluids Tell.
- Provide intravenous fluids to the patient.
- Check the patient’s serum electrolyte levels.
- Check the patient’s vital signs.
3)activity intolerance related to weakness as evidenced by limited activities.
- Assess the patient’s activity level.
- Plan the patient’s activity.
- Provide the patient with analgesic medicine before resuming the activity.
- Instruct the patient to take rest between activities.
- Provide the patient with carbohydrate and protein rich food.
- Provide the patient with prescribed medicine.
4)knowledge deficite related to cause and disease as evidence by asking questions.
- Assess the patient’s knowledge level.
- Provide education to the patient about the diabetic diet.
- Provide education to the patient about foot and nail care.
- Provide education to the patient to cover their feet with soft shoes.
- Provide education to the patient to self-inject insulin. Provide education about administration.
5)fear related to insulin injection.
- Monitor the patient’s blood glucose level.
- Provide education to the patient about self-administration of insulin.
- Insulin therapy to the patient Provide education about complications of.
- Provide education to the patient about the signs and symptoms of hyperglycemia and hypoglycemia.
PIH Pregnancy-induced hypertension:
- PIH is called Pregnancy Induced Hypertension. In which a woman does not have any hypertension condition before pregnancy, but if the woman’s blood pressure increases to 140/90 mmHg or more due to the gravid uterus, then this condition is called Pregnancy Induced Hypertension.
- It is generally divided into three parts, namely,
- Eclampsia
- Gestational Hypertension,
- Preeclampsia,
1. Gestational hypertension:
- In a normotensive woman before pregnancy, blood pressure of 140/90 mmHg or higher for 4 or more hours on at least two occasions after 20 weeks of pregnancy or within the first 24 hours of delivery is called gestational hypertension.
- In its criteria,
- The underlying cause of hypertension is absent.
- Other signs of pre-eclampsia are not seen.
- Most cases occur at 37 weeks of pregnancy or later.
- Blood pressure returns to normal within 6 hours after delivery.
Preeclampsia:

- Preeclampsia a It is a complication of pregnancy. Its etiology is unknown but it is a multisystem disorder. In which high blood pressure is seen along with damage to other organs and most commonly the liver and kidneys are affected. Preeclampsia is mainly seen after the 20th week of pregnancy and also varies in severity.
- Among the main symptoms of preeclampsia,
- 1) Hypertension that increases to more than 140/90 mmHg (hallmark sign of preeclampsia),
- 2) Edema (mainly in the hands, face, and legs) and excessive weight gain ,
- 3) Proteinuria (excess amount of protein in urine),
- 4) Albuminuria (albumin present in urine).
- These symptoms of preeclampsia are seen after the 20th week.
Etiology (Etiology):
- The exact cause is unknown.
- Elderly or young primigravida,
- Hypertension during pregnancy,
- Family history of hypertension,
- Placental abnormalities such as,
- Hyperplacentosis: Excessive exposure of chorionic villi,
- Ex: molar pregnancy, twins, diabetes,
- Placental ischemia.
- Obesity,
- Pre-existing vascular disease,
- Thrombophlebitis,
- Pregnancy complications such as,
- Multiple pregnancy,
- Hydatidiform mole pregnancy,
- Hydroamniosis,
- Rh. incompatibility,
- Medical diagnoses such as, nephritis and diabetes mellitus,
- Vasospasm: Circulating pressure such as angiotensin II and increased sensitivity to prostaglandins causes dilator depression.
- Placental perfusion is reduced due to endothelial cell dysfunction.
- Can also be caused by immune complex diseases.
- Can also be caused by insufficient protein, calcium, magnesium, vitamins E and A in the diet.
- Because of genetic factors
- Because of immunological factors.
- Because of endocrine factors.
- Because of environmental factors.
- Because of chronic health conditions such as hypertension, gestational diabetes, kidney disease and autoimmune disorders.
Classification of pre-eclampsia:
- 1.Primary 70%
2.Secondary 30% - 1.Primary (70%) It is of two types:
a.Pre-eclampsia.
b.Eclampsia with convulsions. - 2.Secondary 30%:
- a Pre-eclampsia, eclampsia superimposed on chronic hypertension (25%).
- b Pre-eclampsia superimposed on chronic nephritis (5%).
- or
- Mild : Proteinuria and hypertension are present. Blood pressure is less than 170/110 mmHg.
- Moderate : Proteinuria and hypertension are present. Blood pressure is greater than or equal to 170/110 mmHg.
- Severe : Proteinuria and hypertension are present. Blood pressure is greater than 170/110 mmHg and the pregnancy is less than 32 weeks or with maternal complications, e.g. Help, eclamptic fit.
Sign And Symptoms:
- The signs and symptoms of pre-eclampsia can vary depending on the severity.
- They may include the following:
- Main symptoms: High blood pressure (hypertension):
Blood pressure consistently above 140/90 mmHg. - Proteinuria:
Protein is detected in the urine. - Edema: Edema, especially in the hands, face, or feet. While some edema is normal during pregnancy, or sudden edema, if accompanied by other symptoms and signs, may indicate pre-eclampsia.
- Albuminuria: Albumin in the urine.
- Alarming symptoms:
- Headache: Often severe and persistent headaches that do not go away with treatment.
- Visual disturbances: This may include blurred vision, flashing lights, or seeing spots.
- Upper abdominal pain: Especially in the upper right abdomen, which suggests liver involvement.
- Decreased urine output:
Oliguria (reduced urine production) - Other symptoms:
- Nausea and vomiting: especially if persistent and severe.
- Breathing difficulties: especially if associated with fluid accumulation in the lungs (pulmonary edema).
- Hyperreflexia: Exaggerated reflex response.
- Thrombocytopenia: A decrease in the number of platelets, which can lead to blood clotting problems.
- Reduced fetal movement: Fetal movement is less than normal for that stage of pregnancy.
- It is important to note that not all women with pre-eclampsia will experience all of these symptoms. The presence of hypertension and proteinuria after 20 weeks of pregnancy in a previously normotensive woman is the primary diagnostic criteria for pre-eclampsia.
Diagnostic Evaluation:
- History collection,
- Physical Examination,
- Urine test: To assess proteinuria.
- 24-hour urine collection to measure protein levels.
- Ophthalmic examination.
- Blood tests for liver and kidney function such as,
- Serum uric acid,
- Blood urea level,
- Serum creatinine level,
- Hepatic/liver enzymes
- Antenatal fetal monitoring:
- Clinical examination,
- Daily fetal kick count,
- Ultrasonography,
- Cardiotocography,
- Umbilical artery flow velocimetry,
- Biophysical profile: This includes ultrasonography and non-stress tests to assess fetal breathing and muscle tone.
Complication :
1.Maternal Complications:
During Pregnancy:
Eclampsia,
Accidental hemorrhage,
Oliguria and anuria,
Vision diminution,
Preterm labor.
HELLP syndrome:
Hemolytic anemia, elevated liver enzymes, low platelet count,
During labor: eclampsia,
Shock, sepsis.
Fetal complications: Intrauterine death, intrauterine growth restriction, asphyxia, prematurity.
Remote complications:
Residual Hypertension,
Severe preeclampsia,
Chronic nephritis.
Management:
The management of preeclampsia involves close monitoring of the mother, prevention of complications, and nursing management to improve the well-being of the mother and fetus.
1) Assessment and Monitoring
Vital signs
Continuously monitor the mother’s vital signs, which include pulse, blood pressure, respiration, and temperature.
Fluid intake output monitoring
Monitor the mother’s intake output chart. Due to which kidney function and fluid balance can be monitored.
Fetal assessment
Fetal assessment involves assessing the fetus’s heart rate and fetal movement.
Symptom assessment
Regularly assess the mother’s signs and symptoms, including headache, visual disturbances, epigastric pain, and edema.
2) Bedrest and Positioning
Advise the mother to rest on the left side to improve uteroplacental circulation and reduce vena cava compression.
Advise the mother to limit activity to prevent an increase in blood pressure.
3) Fluid Management
Maintain the mother’s intravenous access to maintain her hydration status and administer medication.
Continuously monitor the mother’s intake output To maintain the mother’s hydration status and prevent fluid overload in the mother.
4) Medication Administration
Provide the mother with medication as prescribed by the healthcare provider.
Such as,
Antihypertensive drug to control blood pressure
Ex:=
labetalol
(Orally 100 mg (TDS)
I.V infusion :=1-2 mg / min.),
Hydralazine(Orally
100 mg / day in four divided doses).
If the mother has a condition of fluid overload, then provide diuretic medication such as,
Ex: Lasix(Frusemide)( 40 mg up to 5 days).
If the mother has a condition of convulsion, then provide anticonvulsant medication.
Ex:=Magnesium sulfate.
Provide sedative medication to the mother.
Ex:=
Diazepam 10-20 mg I.v. followed by:
Tab.Diazepam 5mg ( TDS),
Tab.phenobarbitone 60 mg ( hs).
If the mother has a condition of constipation, then provide a mild laxative at bedtime.
Ex:= milk of magnesia.
Maintain the mother’s progress chart in which,
Monitor the blood pressure four times during the day.
Monitor the mother’s daily weight and assess the condition of edema.
Monitoring the mother’s fluid intake and urine output.
Conducting a urine examination of the mother to assess the condition of protein urea.
Conducting a blood investigation of the mother to assess the mother’s hematocrit, platelet count, uric acid, creatinine level, and liver function test (LFT) once a week.
Conducting an ophthalmic examination of the mother.
Continuously assess the well-being of the fetus.
5) Monitor for complications
Assess the mother for warning signs and symptoms of severe pre-eclampsia and eclampsia, including,
seizures, severe headache,
epigastric pain,
blurred vision.
Hellp syndrome in the mother:
(1)H :=Hemolytic anemia,
(2) EL:=Elevated liver enzyme,
(3) LP:=Low platelet count)
Assessment of complications like.
6) Patient education
Advise the patient and her family members to get regular antenatal check-ups of pregnant women so that the condition of pre-eclampsia can be detected early.
Pregnant Provide complete information and education to the woman and her family members about the condition of pre-eclampsia, its causes, symptoms and signs, diagnosis, complications and its treatment. Advise the pregnant woman and her family members to seek immediate medical treatment to prevent the condition of pre-eclampsia from worsening. 7) Emotional Support Provide proper reassurance and psychological support to the patient and her family members. Provide advice to improve proper coping mechanisms.
8) Collaboration and Communication
Properly collaborate with other health care personnel for proper treatment of the mother, including communication with obstetricians, neonatologists and anesthesia providers, so that proper care of the mother can be provided.
Properly communicate and collaborate with other health care team members for the care of the mother and provide proper treatment to the mother.
9) Preparation for Delivery
Preparation for timely delivery to prevent complications for the mother and baby based on the condition, gestational age, and severity of the mother’s pre-eclampsia.
Keep all necessary emergency equipment ready such as airway, catheterization equipment, oxygen, suction apparatus, emergency medicine tray, and caesarean section tray, etc. properly prepared.
10) Follow-up and discharge Planning
Planning for the mother’s postpartum care and properly planning for the mother’s recovery from the condition of pre-eclampsia.
Advising the client and her family members to follow up the client properly and to monitor blood pressure continuously.
Thus, nursing management of pre-eclampsia is provided for continuous monitoring of the pregnant woman, timely intervention, comprehensive care, and prevention of complications for the mother and baby.
Eclampsia
Definition:
- Eclampsia is a life-threatening complication that occurs in women during pregnancy. The term eclampsia comes from the Greek word “like a flash of lightning” . Tonic-clonic convulsions or coma are complications of pre-eclampsia. When the condition of pre-eclampsia, which includes,
- Hypertension,
- Edema (weight gain),
- Proteinuria
- (Protein in urine) and
- Albuminuria (albumin present in urine) can be complicated and can lead to a condition called “eclampsia” that can lead to convulsions and coma. This is an obstetric emergency. It is important to take immediate measures to manage it.
Etiology:
- The exact cause is unknown.
- Elderly or young primary gravida,
- During pregnancy Due to hypertensive disorders: Ex: Preeclampsia,
- Family history of hypertension,
- Placental abnormalities such as,
- Hyperplacenosis: Increased exposure to chorionic villi,
- Ex: Molar pregnancy, twins, diabetes,
- Placental ischemia.
- Obesity,
- Pre-existing vascular disease,
- Thrombophlebitis,
- Pregnancy complications such as,
- Multiple pregnancies,
- Hydatidiform mole pregnancy,
- Hydroamniosis,
- Rh. incompatibility,
- Medical diagnoses such as nephritis and diabetes mellitus,
- Vasospasm: Circulating pressure such as angiotensin II and increased sensitivity to prostaglandins cause dilator depression.
- Endothelial cell dysfunction reduces placental perfusion.
- Can also be caused by immune complex diseases.
- Can also be caused by insufficient protein, calcium, magnesium, vitamins E and A in the diet.
- Due to genetic factors
- Due to immunological factors.
- Due to endocrine factors.
- Due to environmental factors.
- Due to chronic health conditions such as hypertension, gestational diabetes, kidney disease and autoimmune disorders.
Sign And Symptoms:

The symptoms and signs of eclampsia are divided into four stages are:
1) Premonitory stage
(30 seconds),
2) Tonic stage
(30 seconds),
3) Clonic stage
(1 to 4 minutes),
4) Coma stage
1) Premonitory Stage
(30 seconds):
- In this the patient becomes unconscious,
- There is twitching of the muscles of the face, tongue and limbs,
- The eyeballs roll, turn to one side and then fixate.
- This stage lasts for 30 seconds.
2) Tonic Stage
(30 seconds):
- In this stage the whole body goes into tonic spasm, trunk = opisnotonis (abnormal body posture in which the head, neck, and spine are bent backwards.)
- Limbus = Flex,
- Hands clenched,
- Respiration stops and tongue protrudes between teeth,
- Cyanosis is seen,
- Eyeballs are fixed,
- This stage lasts for 30 seconds.
3) Clonic Stage
(1 to 4 minutes):
- All voluntary muscles go into alternate contraction and relaxation,
- Twitching starts from the face and involves the extremities of one side,
- Tongue biting occurs,
- Breathing is stutterous,
- Mouth is filled with blood-stained frothy secretion,
- Cyanosis gradually reduces,
- Respiration is labored and noisy,
- Temperature increases to 40°C due to fits,
- This stage lasts from 1 to 4 minutes.
4) Stage of Coma:
- After the seizure, the patient goes into a coma stage that lasts from a few minutes to a few hours,
- The patient remains in a deep coma until another convulsion occurs. In this, the patient is seen in a state of confusion after the convulsion and does not remember what happened to the patient.
- If the fits occur consecutively, it converts into status epilepticus.
Diagnostic Evaluation (Diagnostic Evaluation):
- History Collection,
- Physical Examination,
- Urine Test: To assess proteinuria.
- 24 Hour Urine Collection to Measure Protein Levels.
- Ophthalmic Examination.
- Blood tests for liver and kidney function such as,
- Serum uric acid,
- Blood urea level,
- Serum creatinine level,
- Hepatic/liver enzymes
- Antenatal fetal monitoring:
- Clinical Examination,
- Daily Fetal Kick Count,
- Ultrasonography,
- Cardiotocography,
- Umbilical Artery Flow Velocimetry,
- Biophysical Profile: This includes ultrasonography and non-stress tests to assess fetal breathing and muscle tone. For.
Complication (Complications) :
- Hazards of conversion
Injury-tongue bite,
Vomiting aspiration,
Exhaustion, - Acute left ventricular failure,
Pulmonary In AD,
Pneumonia,
Cerebral hemorrhage,
Hyperpyrexia,
Anuria,
Disseminated intravascular coagulopathy (DIC),
Hepatic necrosis,
Postpartum shock,
Pueral sepsis,
Psychosis,
Pulmonary embolism,
Abruptio placentae,
Vision disturbance,
Blindness due to involvement of optic nerve,
But vision recovers after four to six weeks after delivery.
Management of Eclampsia
Medical and Nursing Management of Eclampsia
Management:
- Controlling convulsive fits.
Controlling blood pressure.
Preventing complications.
Safely delivering the fits. - Principles of Management
- Maintain the mother’s airway, breathing and circulation.
- Properly administer 8-10 liters of oxygen to the mother.
- Prevent the mother from convulsing.
- Provide proper ventilatory support to the mother.
- Prevent injury to the mother.
- All the laboratory investigations of the mother should be done properly.
General Management
Hospitalization
The mother should be hospitalized in a hospital with properly well-equipped facilities.
Rest Advise the mother to take adequate rest and also advise her to stop all activities and restrict visitors. To do.
Positioning Advise the mother to rest in a proper left lateral position to reduce vena cava compression and prevent heel spurs.
History Collection Collect a complete history of the mother, including the frequency and duration of the fits and any medications the mother is taking.
Sedation and then general examination Provide the mother with proper drugs and sedate her.
Ex:=phenobarbiton 15-30 mg ( TDS)
Or
Diazepam 1.5 mg ( TDS).
After the mother is properly sedated, do a general and abdominal examination of the mother properly and quickly.
Vital signs Note the mother’s vital signs every half hour, including,
temperature,
pulse,
respiration,
and blood pressure.
If there is any abnormality in the vital signs or the vital signs are raised above their normal range, treat them immediately. Do.
Urinary Output
Monitor the mother’s urine output every hour.
Nutrition Start the mother on 10% Dextrose to maintain the mother’s fluid, nutritional and calorie levels. Fluids should not increase by more than 2 liters in 24 hours.
In addition, to maintain the mother’s calorie level, 50 ml of 5% Dextrose should be provided to the mother at an interval of 8 hours.
Specific management or medical management
Eclampsia can be treated by providing the mother with the following medications:
Eclampsia can be treated by providing the mother with the following medications:
a) Anticonvulsant,
b) Antihypertensive,
c) Sedatives,
d) Diuretic,
e) Antibiotics,
f) Other Medication.
a) Anticonvulsant,
Magnesium sulfate ( MgSO4 )
is the drug of choice for treating the condition of eclampsia. Because it helps in preventing eclamptic fits in pregnant mothers. Magnesium sulfate can be administered both IV (intravenously) and IM (intramuscularly).
Dose and route
IM (intramuscularly):
Initial dose: Initially 4 gm IV (intravenously) bolus, administer magnesium sulfate very slowly over 3-5 minutes.
Continuous dose: 5 gm magnesium sulfate IM (Intramuscular) Administer every four hours in alternate buttocks.
IV( Intravenously)
Initial Dose:
Initial dose: 4-6 gm magnesium sulphate IV( Intravenously) administered slowly over 15-30 minutes.
Continuous Dose:
1-2 gm magnesium sulphate IV( Intravenously) administered every hour.
Magnesium sulfate is a toxic agent and if not provided within therapeutic levels, it can cause a condition called deep tendon reflux. The therapeutic level of magnesium sulfate (MgSO4) is 4-7 mEq/L (milliequivalents per litre). In case of magnesium sulfate (MgSO4) overdose, calcium gluconate is used as its antidote.
Magnesium sulfate is administered only when there is a low level of sodium, urine output is greater than 30 ml/hr and respiratory rate is greater than 12/min.
b) Antihypertensive,
Antihypertensive is used to control and reduce blood pressure.
Ex:
a) Hydralazine:
5 to 10 mg over 2 up to minutes.
b)Labetalol:
Initial dose: 20mg slowly over 2 minutes.
Then 40-80 mg IV over 10 minutes.
Total dose should not exceed 300 mg.
c)Sedatives
Ex:=Diazepam
Dose:=5-10mg IV at the rate of 2-5mg/minute.
Maximum dose: Should not be increased more than 10mg.
d) Diuretic:
Diuretic medication should be provided only when pulmonary AD is present during pregnancy.
Ex:=Frusemide, Mannitol.
e) Antibiotics:
Antibiotics are provided as prophylactics to reduce the complications of pulmonary and pleural infections.
These antibiotics include the use of broad spectrum antibiotic medications.
f) Other medications:
i) In case of pulmonary ED: frusemide 40 mg IV followed by 10% Mannitol Provide.
ii) Heart Failure:
Ex: Use of Lasix and Digitalis Medication.
iii) Hyperpyrexia:
Antipyretic medication is used.
Nursing Management of Eclampsia:
- Eclampsia Place the pregnant woman in a side-lying, padded side-railed cot.
- Place a padded tongue blade between the teeth.
- Place the mother in a lateral position to avoid aspiration.
- Keep the airway patent during convulsions and provide the mother with adequate amounts of oxygen.
- Properly monitor the mother’s oxygen level with pulse oximetry To do.
- Properly suction to remove oral secretions and any vomiting.
- Properly note the time and duration of the mother’s convulsions.
- Properly and regularly provide prenatal care to the mother with pregnancy-induced hypertension.
- Protect the mother from self-injury.
- Keep the mother in a dark room to minimize stimuli such as bright light, noise, and visitors.
- Keep the foot of the bed slightly elevated so that secretions can drain properly from the respiratory tract.
- Assess the mother’s vital signs, including the height of the fundus, presentation and position of the fetus, and fetal heart sounds, and test the urine for protein.
- Properly assess the mother’s urine output.
- Provide intravenous infusion of glucose saline and Ringer lactate solution as prescribed to maintain the mother’s fluid and nutritional levels.
- Advise the mother to maintain personal hygiene.
- Provide the mother with properly prescribed medications.
- Assess the mother’s uterine activity, cervical status, and fetal status as membranes may rupture and Delivery can occur.
Obstetrical Management:
- Most often, when a woman has convulsions, she comes for labor. If labor has not started, then artificial membrane rupture, prostaglandin gel or oxytocin is done for induction of labor or a cesarean section is also done. If the baby has died, then spontaneous labor is waited for.
- Continue to start the hypertensive regimen as prescribed during the postpartum period.
- Continue to monitor the mother for any complications other than eclampsia.
- Advise the mother to have regular follow-up.
(PID)Pelvic Inflammatory Disease:
- PID (P.I.D) is called pelvic inflammatory disease, in which there is infection and inflammation in the upper genital tract organs of the female reproductive system, then this condition is called pelvic inflammatory disease. This infection is usually transmitted through the vagina by bacteria responsible for sexually transmitted diseases, which are transmitted to the upper genital tract in an ascending (downward from the vagina) manner, due to which a condition of infection and inflammation arises in the female reproductive organs. In this infection, organs such as the vagina, cervix, uterus, fallopian tubes, ovaries etc. can be involved.
- If the infection is in the vagina, it is called vaginitis is.
- If the infection is in the cervix, it is called cervicitis.
- If the infection is in the uterus, it is called metritis.
- If the infection is in the fallopian tubes, it is called salpingitis.
- If the infection is in the ovary, it is called oophoritis.
Types of Inflammatory Disease:
Pelvic Inflammatory Disease is generally divided into two types,
1.Acute Pelvic Inflammatory Disease
2.Chronic Pelvic Inflammatory Disease
1.Acute Pelvic Inflammatory Disease: Acute pelvic inflammatory disease means that if severe symptoms are seen in a short time, then this condition is called acute pelvic inflammatory disease. Disease is called.
2. Chronic pelvic inflammatory disease: In chronic pelvic inflammatory disease, if attacks of acute infection occur repeatedly, this condition converts into chronic pelvic inflammatory disease.
Etiology:
- Bacteria such as chlamydia and gonorrhea,
- Viral infections such as herpes simplex,
- Parasitic infections,
- Fungal infections
Risk Factores (Risk Factores):
- Due to low socio-economic status,
- Due to multiple sexual partners,
- Due to a past history of PID,
- Cigarette smoking,
- Due to low immunity,
- Due to abortion,
- Due to the use of an IUD (intrauterine device).
Sign And Symptoms:
- Lower abdominal pain,
- Fever,
- Headache,
- Irregular menstrual bleeding,
- Nausea,
- Vomiting,
- Anorexia,
- Tenderness,
- Vaginal discharge,
- Pain during periods,
- Pain during voiding and defecation.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History Collection,
- Physical Examination,
- Complete Blood Count (CBC) Test,
- Ultrasonography (USG),
- Cervical and vaginal swab culture,
- Urine test,
- CT scan,
- MRI,
- Endometrial biopsy.
Management ):
Medical Management:
- The aim of medical management is to prevent infection and further transmission and to prevent complications from arising.
- If the patient has a bacterial infection, then provide broad spectrum antibiotic medicine. Such as,
ceftriaxone,
metronidazole,
tetracycline,
erythromycin. - Provide advice to the patient to take proper rest.
- Advise the patient to take adequate amounts of oral fluids.
- If the patient has an intrauterine device (IUD), remove it properly.
- Provide the patient with a proper semi-fowler position.
- Advise the patient to avoid sitz baths if there is an acute infection.
- Continuously monitor the patient’s vital signs To do.
- Provide analgesic medicine to relieve the patient’s pain.
- If the patient has abdominal pain, advise him to apply a heating pad to the abdomen to relieve the pain.
- Advise the patient to use a proper barrier contraceptive method to reduce the risk of pelvic inflammatory disease.
- If the patient has pelvic Advise the patient to seek medical treatment if any symptoms of inflammatory disease are observed.
- Advise the patient to avoid sexual activity during the puerperal period after delivery, abortion.
- Advise the patient to maintain personal hygiene.
Surgical Management:
- This surgical management is usually done when the infection has involved the fallopian tubes and ovaries.
- Laparoscopy: In this, a small incision is made on the abdominal wall and then a laparoscope (a thin flexible tube containing a camera and a light) is inserted, due to which any infection and inflammatory conditions in the reproductive tract can be visualized on the screen.
- Salpingectomy: In this, the fallopian tubes are removed surgically.
Multiple Pregnancy:
Definition:
- When more than one fetus develops in the uterus at the same time, it is called a “multiple pregnancy.”
- When two fetuses develop in the uterus at the same time, they are called twins.
- When three fetuses develop in the uterus at the same time, they are called triplets.
- When four fetuses develop at the same time, they are called quadruplets.
Varieties and Types of Twin Pregnancy
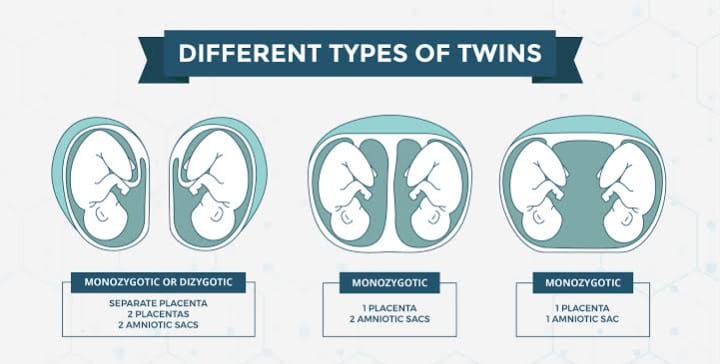
1) Dizygotic Twins:
This is a common condition, i.e. fertilization of two ova by two spermatozoa.
In this, two placentas are found.
In this, the communicating vessels are absent.
In this, there may be two amnions and two chorion membranes.
In this, the genetic features may be different.
They do not accept skin grafts.
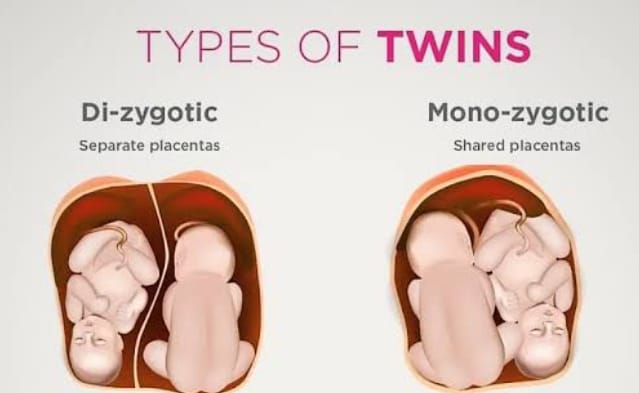
2) Monozygotic Twins
In this, the fertilization of a single ovum occurs by a single sperm, due to which monozygotic twins develop.
In this, communication vessels are present.
In this, two amniotic membranes are seen.
In monozygotic twins, most of the time, they are of the same sex.
In them, genetic features are also found to be similar. It has physical features like eyes, hair color, ear shape, palmar creases. It also accepts skin grafts. Etiology: The exact cause is unknown. Maternal environmental factors such as: Race: Highest in Negroes. Hereditary: This is mainly maternal side. It is more commonly transmitted.
Advanced age of mother:
Due to the advanced age of the mother such as 30-35 years.
Due to influence of parity:
Increases parity mainly in 5th gravida.
Iatrogenic
Due to drugs used in ovulation.
2)Superfecundation
In this, two different ova are released in the same cycle and fertilization occurs in a short period of time through separate acts of coitus, it is called superfecundation.
3) Superfetation
In this, two ova are released and fertilized by different menstrual cycles, this is called superfetation.
4) Fetus papyrus or compressus
In this, one fetus dies early and the dead fetus is flattened and compressed between the membrane of the living fetus and the uterine wall.
5) Fetal acardiosis
This is seen in uniovular twins.
Lie and Presentation
The common lie of the fetuses is usually longitudinal but malpresentation is common.
Presentation
Both vertex,
first vertex and second breech,
first breech and second vertex,
both breech,
first vertex and transverse,
both transverse.
Diagnostic Evaluation (Diagnostic Evaluation):
History collection,
Physical examination,
Symptom assessment
Excessive enlargement of the uterus,
Nausea and vomiting are more common in the early months,
Palpitation and shortness of breath are seen in the last months of pregnancy,
Swelling in the legs, varicose veins,
Hemorrhoids,
Abnormal abdominal enlargement and excessive fetal movement.
General examination
Anemia,
Abnormal weight gain,
Pre-eclampsia,
Abdominal Examination
Inspection:
Barrel septum and large abdomen,
Palpation:
Increased height of uterus compared to amenorrhea period,
Two fetal poles filling the fundus of uterus,
Increased abdominal girth,
Auscultation
Two fetal heart sounds are located at two different spots.
Investigation
Sonography,
Biochemical tests such as maternal serum chorionic gonadotrophin,
fetoprotein and unconjugated install.
Management:
- Antenatal Management
Early diagnosis should be done to detect chorionicity, amniosity, fetal growth pattern and congenital malformations if any.
Serial sonography, non-stress test and Doppler velocimetry should be done for further surveillance.
Advice
Advise the mother to increase her diet by 300 kcal/day. - Advise the mother to increase her protein intake.
- Supplement therapy
Advise the mother to take iron therapy 100 to 200 mg/day. And also advise the mother to take additional vitamins, calcium and folic acid. - Advise the mother to take adequate rest to prevent preterm labor and other complications.
- Advise the mother to visit frequently and advise the mother to undergo antenatal check-ups at regular intervals so that early identification of anemia, complications of preterm labor and preeclampsia can be done.
- Regular assessment of fetal growth through ultrasound at 2-3 week intervals.
- Provide adequate knowledge about breastfeeding and bottle feeding to the mother during the antenatal period so that the mother can feed her baby properly.
- During labor
Since twin pregnancy is a high-risk pregnancy, the patient should be admitted to a well-equipped hospital facility where available. Vaginal delivery can be performed when both or one fetus is in breech presentation. - Care during first stage of labor
Take extra precautions with normal conduction of singleton fetuses in the first stage. - An experienced obstetrician, an experienced anesthetist, and a neonatologist should be present at the time of delivery.
- Ultrasound facility should be available in the labor room.
- Adequate rest should be given to the mother to prevent early rupture of the mother’s membranes.
- Limited use of analgesic drugs and if necessary, epidural analgesia should be given.
- Close monitoring of the fetus should be done.
- After membrane rupture, perform internal examination and check for cord prolapse.
- Start Ringer lactate solution in intravenous line.
- Keep 1 unit of blood cross-matched and grouped and ready.
- Delivery of first baby
- Conformational examination of second stage should be done properly through vaginal examination.
- Multiple pregnancy is considered a high risk pregnancy, hence obstetrician, anesthetist and pediatrician should be present during delivery.
- Multiple pregnancy is considered a high risk pregnancy, hence operation theatre should be properly prepared for caesarean section in case of emergency.
- Continuous monitoring of fetal heart sound should be done till both babies are delivered.
- Delivery of the first baby is usually spontaneous and then a proper episiotomy is done.
- After delivery of the first baby, provide information to the mother about its sex.
- Then label the baby as number 1 immediately.
- Delivery of the second baby
After delivery of the first baby, observe the second baby by lie, presentation and fetal heart sound, abdominal examination or real-time ultrasound. - Perform vaginal examination to check for membrane and cord prolapse.
- If the lie is longitudinal, perform low rupture of the membrane and check again for cord prolapse.
- If contractions are poor, add oxytocin to the infusion and administer it to the mother.
- Keep the interval between two deliveries less than 30 minutes, if it is too late, then interference has to be done. If the head is low down, then forceps delivery, if there is no cephalopelvic disproportion in high up, then internal version should be done under general anesthesia and ventouse delivery should be done.
- Perform breech delivery through breech extraction.
- If the fetus’s lie is transverse, then external version should be done to bring the fetus into longitudinal lie and if that fails, then internal version should be done and breech extraction should be done under general anesthesia.
- Indications for Cesarean Section for Second Twin:
Non-cephalic presentation with larger twin,
Immediate closure of cervix after delivery of first baby,
Fitus distress. - Third stage
- After delivery of second baby’s second baby’s second leg, to prevent postpartum hemorrhage, administer 10 International Units (IU) IM or 20 International Units (IU) oxytocin in 500 ml of normal saline (NS) or Ringer’s lactate solution intravenously (IV) to the mother.
- Then deliver the placenta by controlled cord traction (CCT).
- After delivery of second baby, start oxytocin drip for at least one hour.
- If there is excessive blood loss, give a blood transfusion.
- Monitor the mother closely for two hours after delivery.
- Provide additional support and health education to the mother for caring for the baby.
Indications for Cesarean Section:
Obstetric Indications
Placenta previa,
Severe preeclampsia,
Previous cesarean section,
Cord prolapse,
Abnormal uterine contractions,
Contracted pelvis.
For twins
Both fetuses or the first fetus should be in non-cephalic presentation (breech, transverse).
Conjoint Twins.
Complications such as intrauterine growth retardation.
Elderly primigravida:
Definition:
When a woman conceives her first pregnancy after the age of 30 or 35, such a condition is called It is called elderly primigravida.
Category:
Elderly primigravida is generally divided into two categories.
1) High fecundity: In this, women marry late but conceive immediately after marriage.
2) Low fecundity: Women marry early but conceive after a long time after marriage.
Complications:
During Pregnancy:
- Abortion,
- Pre-eclampsia,
- Abruptio placentae,
- Uterine fibroids,
- Medical Complications: Hypertension (HTN), Diabetes, Organic Heart Disease.
- Post Maturity,
- Intra Uterine Growth Restriction (IUGR),
During Labor:
- Premature Labor,
Pro Long labor,
Maternal and fetal distress,
Retained placenta. - During puerperium:
Increased morbidity rate.
Failing lactation.
Management:
- Elderly primigravida is considered a high-risk pregnancy.
- It requires proper antenatal supervision.
- The labor process in elderly primigravida is longer, due to which proper supervision of the mother is required.
- Abnormal uterine action converts into complicated labor.
- Obstetrical intervention is required in elderly primigravida because the perineum is rigid and there is a possibility of prolonged labor.
- In elderly primigravida, the chances of neonatal morbidity and mortality rate are higher due to increase in maternal age because of prematurity, prolonged labor, hence there is a need for proper management.
- In elderly primigravida, the mother should be advised to prefer hospital delivery.
- Proper sonography should be advised for early identification of complications.
Polyhydroamnios (Hydroamnios):
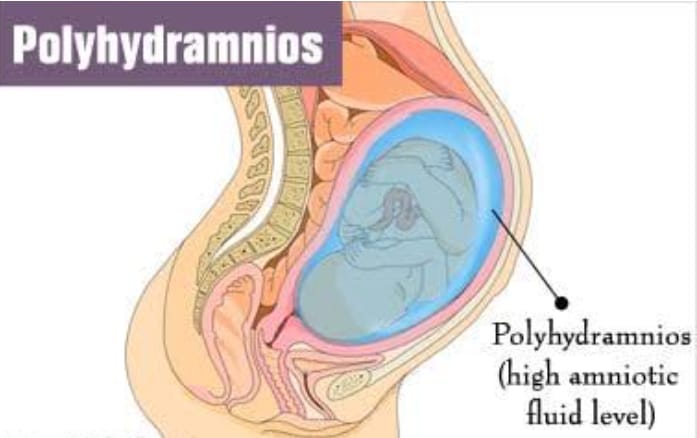
Definition:
- Poly: Excessive.
Hydroamnios: Amniotic fluid/liker amni. - Polyhydroamnios is a condition in which the amount of liker amni (amniotic fluid) increases to more than 2000 ml. This condition is called polyhydroamnios (hydroamnios). (During late pregnancy, the amount of liker amni (amniotic fluid) is usually 500 – 800 ml.)
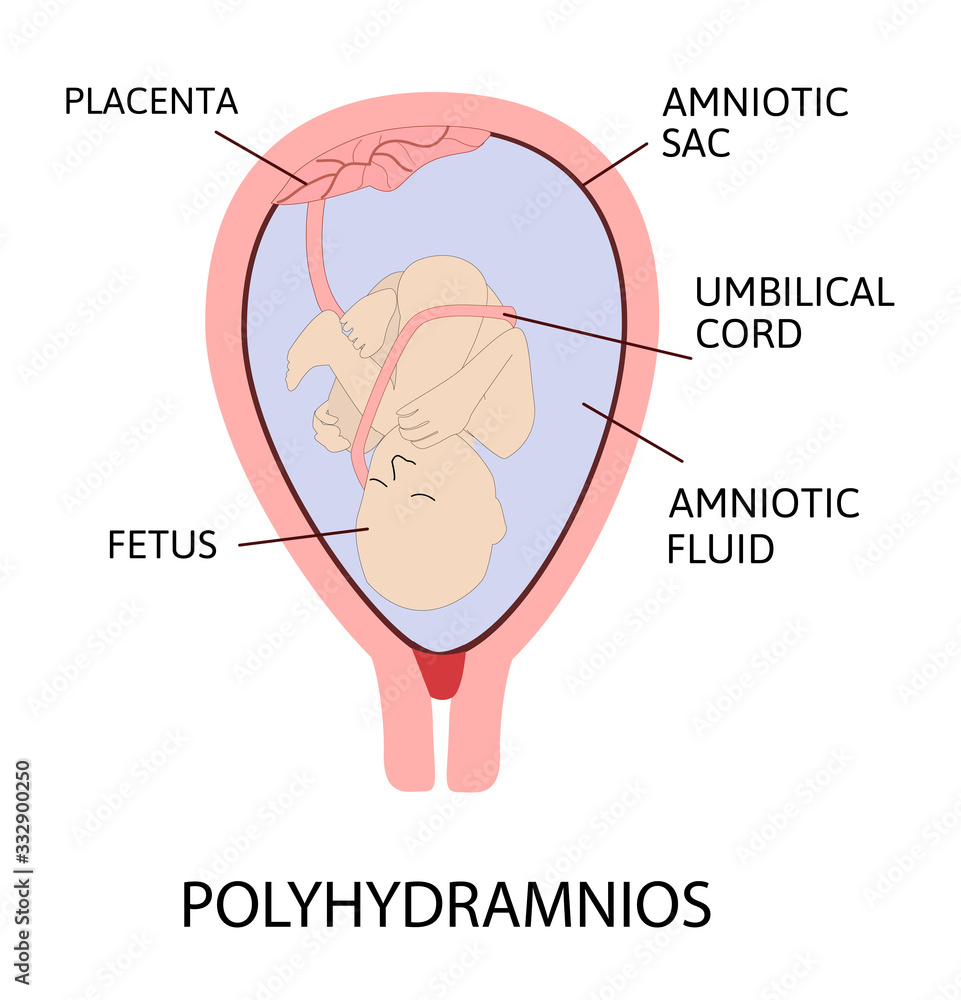
Etiology:
1)Fetal anomalies,
2)Maternal causes,
3)Placental factors,
4)Multiple pregnancies.
1)Fetal anomalies:
Anencephaly,
Open spina bifida,
Esophagia and duodenal atresia,
Facial cleft,
Neck masses,
Hydrops fetalis.
2)Maternal causes:
Diabetes mellitus,
Cardiac and renal diseases.
3)Placental factors:
Choriocarcinoma of the placenta.
4)Multiple Pregnancy.
Multiple pregnancies especially monozygotic twins.
Types Of Polyhydroamnios:
Polyhydroamnios is generally divided into two types based on the speed of its onset.
1.Acute polyhydramnios
2.Chronic polyhydramnios.
1.Acute polyhydramnios: This type of acute polyhydramnios is rare and mostly seen before 20 weeks of pregnancy, meaning that this condition usually develops rapidly, usually during the 4th month of pregnancy, due to which the abdomen enlarges rapidly and the abdominal girth usually enlarges to more than 100 cm. The onset is rapid and the uterus reaches the zygosternum in about three to four days.
Etiology:
- Gross quinquenil fetal anomaly,
- Uniovular twins,
Sign And Symptoms:
- Severe shortness of breath.
- Severe abdominal discomfort.
- In the heel, usually in the ankle and leg.
- Varicose veins Vein.
- Abdominal symptoms such as abdominal pain, nausea and vomiting may be seen.
- Vital parts are not felt.
- The patient appears ill and features of shock are absent.
- The abdomen is large and full, the skin is tense, there are scars, large striae, fluid is felt.
2. Chronic Polyhydramnios: This condition of chronic polyhydramnios usually develops slowly and usually develops in the second half of pregnancy (30 weeks).
Sign And Symptoms:
- Dyspnea,
- Palpitation,
- Abdominal discomfort,
- Swelling in the leg,
- Painful varicose veins,
- Vital part not palpable,
- Fetal heart sound (F.H.S) is not audible.
- Abdominal girth increases more than 100 cm.
- Due to accumulation of amniotic fluid.
Sign:
- Pregnancy signs are present,
- Pre-eclampsia signs such as edema, hypertension and proteinuria may also be seen,
- During abdominal examination:
- Inspection: Abdomen appears large, globular with fullness on the sides.
- Skin is tense, large striae with signs are seen is.
- Palpation: The height of the uterus and the abdominal girth are more noticeable than during the period of amenorrhea.
- Fluid thrill is felt in all directions of the uterus and the fetal parts are not palpated well.
- Auscultation: Fetal heart sounds are not heard clearly.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History collection,
Physical examination,
Internal examination: If the cervix is dilated enough to pull and the finger tip is admitted, the tense bulge membrane is felt. - Investigation: Sonography, radiography, blood studies such as,
ABO and Rh grouping,
Post prandial blood sugar,
Glucose tolerance test,
Amniotic fluid-alpha feto protein.
Management:
Mild polyhydramnios:
- This type is seen in the mid-trimester and usually does not require treatment, only bed rest is required.
- Severe polyhydramnios: This type The main principles of treatment for patients considered high risk are to reduce symptoms, assess the cause, and prevent complications.
Supportive therapy:
- Advise the patient to take adequate amount of bed rest.
Advise the patient to take less amount of salt in diet. Give.
Provide analgesic and sedative medication to the patient as per the condition of the patient.
Proper investigations should be done to assess fetal malformations and to assess the condition of complications such as diabetes and Rh isoimmunization. - If the patient has associated conditions such as preeclampsia or diabetes, treatment of indomethacin (25 mg every 6 hours) to the mother reduces amniotic fluid.
- In uncomplicated cases: If the response is good, then the pregnancy should be continued till term. Pregnancy should be allowed to continue.
- In unresponsive cases, if there is maternal distress and the gestational age is less than 37 weeks, amniocentesis should be performed and amnioreduction should be done – 500 ml/hourly should be removed slowly (do not remove more than 1-1.5 liters).
- If the gestational age is more than 37 weeks, labor induction should be done.
- If there is congenital fetal anomaly, then pregnancy should be terminated without assessing the duration of pregnancy. To do.
- Check for postpartum hemorrhage after rupture of membranes during internal examination during labor and prevent postpartum hemorrhage and properly check for fetal anomalies.
- Provide support in obstetric management of the patient.
- Assess the cause and degree of polyhydramnios.
- Determine the mode of delivery and the presence of fetal abnormalities. Assess time.
- Advise the patient to take adequate amount of bed rest.
- Advise the patient to restrict extra salt and excess amount of drink.
- Provide proper comfort measures to the patient.
- Provide proper upright position to the patient.
- If the patient has conditions like heartburn and nausea, then provide antacid medication to relieve them.
- Take proper measures to prevent postpartum hemorrhage and shock.
- Allow reduction of amniotic fluid.
- If the pregnancy is more than 37 weeks, then labor is induced and pregnancy is terminated in case of fetal anomalies.
- After delivery, check the baby for abnormalities and patency of the esophagus.
- Properly monitor the mother and fetus for any complications.
Oligohydramnions (oligohydroamnios) (oligomnios):
Definition:
- Oligo: Reduces
Hydroamnios Amniotic Fluid - When the liker amniotic (amniotic Fluid) at term is less than 200 ml, it is called oligohydroamnios. Oligohydroamnios is a medical condition in which the amount of amniotic fluid surrounding the fetus during pregnancy is less than its normal amount. Amniotic fluid is important for cushioning the fetus and facilitating normal development. Oligohydroamnios can be associated with various complications, such as fetal distress, preterm birth or fetal development problems.

Etiology:
- The exact cause is unknown. It is related to the following conditions.
- Postpartum gestation,
- Renal dysfunction,
- From obstetric Europe,
- The secretion of amniotic fluid by the amniotic cells covering the placenta fails.
- Because the kidneys are absent.
- Because fetal urine formation is reduced.
Sign And Symptoms:
- Uterine size becomes smaller than the gestation period.
- Fetal movement is reduced.
- Brech presentation is common.
- Fetal Growth retardation or deformity.
- The uterus feels full of fits due to low amniotic fluid.
- Thick meconium is passed during labor.
Complication:
- Maternal: Prolonged labor, operative interference,
- Maternal morbidity.
Management:
- If the fetus has congenital malformations, then delivery should be done without considering the period of pregnancy.
- Vaginal delivery is favorable.
- If there is a normal fetus with third trimester, conservative management should be done and advice given to increase fluid intake. Simultaneously perform amnio infusion in meconium liker.
Intrauterine Growth Retardation (IUGR)/Intrauterine Growth Restriction (IUGR) Dysmaturity/Small for Date/Chronic Placental Insufficiency:
Definition:
- J baby If the birth weight of a fetus is less than the tenth percentile (10%) of its average gestational age, the condition is called intrauterine growth restriction/retardation (IUGR). Growth restriction/retardation can occur in preterm, term, or post-term babies.
- Incidence of IUGR
- Dysmaturity accounts for about 1/3 of all low birth weight children.
- Its overall incidence in developed countries is 2-8%.
In term babies – 5%,
In post-term babies – 15%. - Types: Small fetuses are divided into the following two types based on clinical evaluation and ultrasound examination.
- 1) The fetus is small and healthy but its birth weight is less than the tenth percentile (10%) of its gestational age.
- 2) Growth restriction is due to pathological process hence it is again divided into two parts as That is,
- (a) Symmetrical Type I (20%),
(b) Asymmetrical Type II (80%).
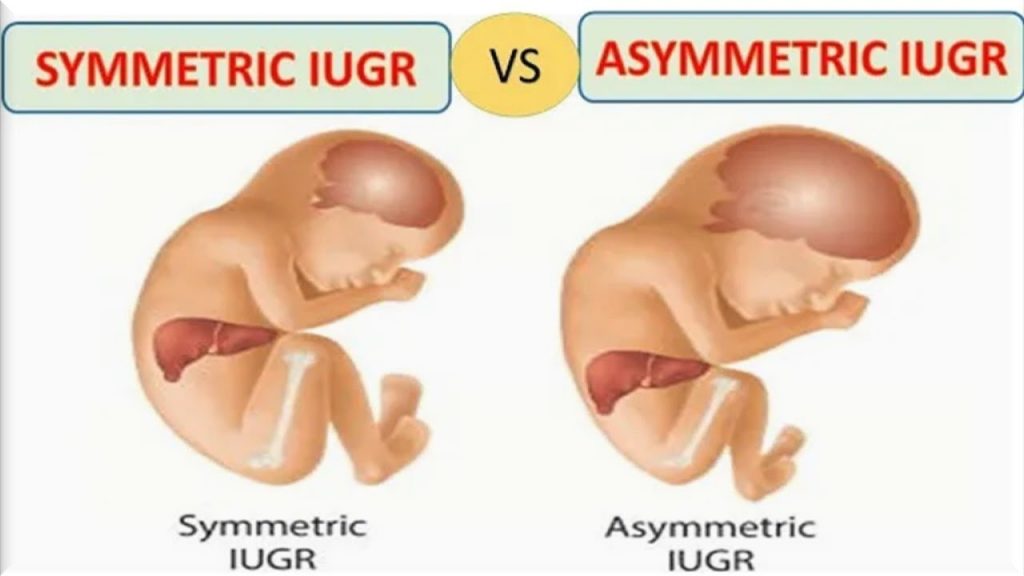
(a)Symmetrical Type I (20%):
- 1.Uniformly small in size.
- 2.Ponderal Index (Birth Weight/Crown Hill Length): Normal.
- 3.HC(Head Circumference: AC(Abdominal Circumference) and Femur Length (FL):AC(Abdominal Circumference) ratio is normal.
- 4.Etiology: Due to genetic disease or infection.
- 5.Total cell number: Low, and cell size: Normal.
- 6.Neonatal- Complicated with Poor Prognosis.
(b)Asymmetrical Type II( 80%):
- 1.Head is larger than abdomen.
- 2.Ponderal index (birth weight/crown-hill length): Low.
- 3.HC(head circumference):AC(abdominal circumference) and femur length (FL):AC(abdominal circumference) ratio are elevated.
- 4.Etiology:Chronic placental insufficiency Cause.
- 5.Total cell number: Normal, smaller size.
- 6.Neonatal- Mostly uncomplicated with good prognosis.
Etiology:
Fetal growth retardation is generally divided into four groups as That is,
1.Maternal,
2.Fetal,
3.Placental,
4.Unknown.
1.Maternal:
Constitutional: Small women due to maternal genetic and racial factors,
due to maternal nutrition before and during pregnancy.
due to poor weight gain.
due to low blood oxygen levels in cyanotic heart disease.
inadequate substrate levels
e.g. Malabsorption syndrome.
Toxins such as alcohol, smoking, chronic renal failure, chronic urinary tract infection etc.
2.Fetal:
In this, maternal blood contains sufficient substrate and it crosses the placenta but it is not utilized by the fetus due to the following:
1.Congenital anomalies: such as cardiovascular, renal and other factors.
2.Chromosomal abnormalities: such as trisomy 21, trisomy 18 (Edward syndrome) trisomy 16, trisomy 13 and Turners Syndrome.
3. Acceleration of the metabolism process of fetuses due to TORCH agents.
4. Due to multiple pregnancy.
3. Placental: Due to poor uterine blood flow. Abruptio, circumvallate placenta, infraction
4.Unknown. Unknown is seen in about 40% of cases.
Diagnostic Evaluation:
-
- History collection,
Physical Examination,
Clinical: This includes palpation of fundal height, liker volume and screening of fetal mass. Symphysis fundal height is correlated with gestational age after 24 weeks. If it is 4 cm or less, it indicates growth restriction. If there is no maternal weight gain, abdominal girth does not increase.
Biophysical: HC, AC ratio, femur length, amniotic fluid, anatomical survey ultrasound Doppler parameters etc.
Biochemical markers: Levels of MSAFP and HCG are elevated in the second trimester.
- History collection,
-
- Physical features at birth:
-
- Physical Features at Birth:
-
- Birth weight deficit is about 600 gm less than the percentile standard.
-
- Length is not affected.
-
- Asymmetrical head circumference is greater than body circumference.
-
- Baby’s appearance due to dry and wrinkled skin, scaphoid abdomen, meconium stained umbilical cord Looks like a “grumpy man”. The cartilaginous ridges of the pinnae and plantar creases in the ears are well developed.
-
- The baby is alert, active, and cries normally, and keeps his eyes open.
-
- Reflexes are normal.
Management:
- Nursing management of the patient with intrauterine growth restriction usually occurs during the antenatal period, if possible.
- Whenever a fetus is suspected to be small for gestational age, a careful search is made by sonography to determine the presence of growth retardation.
- When growth retardation is present, possible causes should be found out.
- If growth retardation is present, the possible cause is identified.
- If the fetus is symmetrically growth retarded, a meticulous search should be made to identify fetal anomalies.
- To prevent unnecessary caesarean section in malformed babies, blood samples and karyotyping of the fetus should be done.
- Adequate rest should be given to the mother in the pre-birth period, i.e. (in left lateral position).
- Then there should be a 2 hour break after lunch and a rest period of 8 hours during night time.
- Provide the mother with a balanced diet in adequate amount to correct the condition of malnutrition. For example, 300 extra calories should be provided.
- In selected cases, low dose aspirin (50 mg) daily is helpful.
- The patient should be properly hospitalized.
- The condition of IUGR should be properly confirmed.
- If the patient has any congenital malformation and genetic disorder, identify it.
- If there is any specific cause of intrauterine growth retardation, treat it first.
- Check the fetal heart sound and the condition of the mother regularly.
- Check the mother’s vital signs properly.
- Provide proper support and reassurance to the mother.
- If the pregnancy is more than 38 weeks, termination is done.
- If the pregnancy is less than 38 weeks, the degree of IUGR should be checked.
- If there is a condition of mild amount of retardation, advise the mother to take adequate amount of rest and provide adequate amount of supplementary therapy.
- Assess lung maturation of the fetus in severe cases.
- If lung maturity is achieved. It is assessed by L.S ratio (lecithin-sphingomyelin ratio), which is an indicator of lung maturity if the value of L.S ratio is more than 2.0-2.5. In such cases, delivery is done where the growth of the fetus cannot be improved by induction at 32-34 weeks and then vaginal delivery/cesarean delivery is done.
- If lung maturity is not achieved:
- Evaluation of lung maturity is done.
- Assess the level of phosphatidyl glycerol.
- If the lungs are not mature, dexamethasone therapy is given and termination is done.
- Delivery can be done by:
- Lower rupture of membranes followed by oxytocin
- In cases of more than 34 weeks of pregnancy, the cervix is favorable and the head is deep in the pelvis. If the cervix is favorable, prostaglandin gel (PGE2) can be used.
- In unfavorable conditions, a cesarean section is performed.
- The following precautions are taken during vaginal delivery:
- Delivery should be done in a well-equipped hospital where intensive intranatal monitoring is possible and it has the facility of an intensive neonatal care unit.
- Otherwise, the child should be transferred to a well-equipped hospital.
- Precautions should be taken during pregnancy.
- The patient should be placed in the left lateral position.
- If there is even slight evidence of hypoxia (meconium staining and abnormal CTG), then immediate measures should be taken by cesarean section in the first stage and forceps in the second stage.
- A pediatrician should also be available for the care of the baby.
- The baby should be provided with care in the intensive neonatal care unit.
- If there is a condition of hypoglycemia, special precautions should be taken for it.
- Provide the mother with proper work and a comfortable environment.
Post Term Pregnancy (Post Maturity/Post Term Pregnancy/Post Dated Pregnancy)
Definition:
- When a woman’s pregnancy continues beyond 2 weeks of her expected date of delivery (EDD), the delivery is called post-maturity or post-term pregnancy. “Postmaturity means a condition in which pregnancy continues for more than 294 days, calculated from the first day of the last menstrual period, it is called postmaturity”.
Etiology:
- Unknown,
- Hereditary,
- Last Menstruation Period (LMP) being inaccurate-due to wrong date.
- Due to sedentary habit.
- Due to hydroamnios.
- Elderly primi gravida.
- Elderly multipara.
- Fetal factors such as congenital anomalies, anencephaly.
- Placental factors such as low estrogen levels.
Diagnostic Evaluation:
- History collection,
- Physical examination,
- Clinical findings: Weight is reduced, abdominal girth is reduced, history of false pain should be noted.
- Assess the height of the uterus, size of the fetus and hardness of the skull bone by palpation.
- The uterus will be filled with fetuses due to low amniotic fluid.
- On internal examination, the cervix is dilated and the skull bones are hard to see.
- Investigation: Sonography, amniocentesis, stereotactic X ray abdomen.
- Non-stress test every two weeks to assess fetal well-being.
- Biophysical Profile,
- Ultrasonographic to estimate amniotic fluid volume.
- Modified biophysical profile.
Sign And Symptoms:
- Baby: Its Normal Appearance: Thin and old, wrinkled skin, vernix caseosa absent, body and cords greenish-yellow in color. Nails are long, with hard heads and nail beds.
- The baby weighs more than 3 kg and its length is about 54 cm.
- The amniotic fluid may be scanty and meconium stained.
- Placenta: Infarction and calcification occur.
- Uncomplicated: Selective induction: Allow for spontaneous labor. Modified biophysical profile should be done twice a week.
- Routine induction: Expected date of delivery is 7 – Induce labor after 10 days.
- Induction:If the cervix is favorable (ripe), induce rupture of membranes and start oxytocin infusion.
- If the cervix is unfavorable (unripe), administer prostaglandin gel vaginally.
- Complicated group: If postmaturity is accompanied by high-risk factors such as primiparesis, preeclampsia, Rh- incompatibility, fetal compromise or Elective cesarean section is also performed in oligohydroamnios placental insufficiency.
- During labor, labor may be prolonged due to any big baby and prematurity. Analgesics should be provided to relieve pain and careful fetal monitoring should be performed. If fetal distress occurs, immediate delivery should be performed by cesarean section or forceps and ventouse.
- Fetal: Reduced placental function, oligohydramnios, and meconium stained stools can cause hypoxia and fetal distress.
- During labor: Fetal hypoxia, acidosis, labor dysfunction, meconium aspiration, birth operative delivery dysmaturity or macrosomia.
- Following birth: Chemical pneumonitis, atelectasis, and pulmonary edema due to meconium aspiration The risk of hypotension, hypoxia, respiratory failure, hypoglycemia, and stillbirth increases.
Management:
Complications:
Intra Uterine Death:

- Intrauterine death is also called stillbirth. Intrauterine death is when the fetus dies after 20 weeks of pregnancy and before and during the delivery of the fetus. If the fetus dies, this condition is called intrauterine death (IUD). All fetuses whose weight is 500 gm or more. If the fetus dies during pregnancy, antepartum or labor (intrapartum), it is called intrauterine death.
Etiology:
The exact cause is unknown.
Placental causes:
Placenta previa,
abruptio placentae,
placental insufficiency.
Umbilical cord problem:
Due to umbilical cord prolapse,
Due to umbilical knot.
Due to maternal conditions:
Due to preeclampsia and eclampsia,
Due to diabetes mellitus,
Infection (cytomegalovirus, toxoplasmosis),
Due to chronic diseases such as hypertension, kidney disease. Etc.
Fetal conditions such as:
Genetic and chromosomal abnormalities,
Congenital anomalies.
Due to infection:
Miternal infections (such as syphilis, HIV group B, streptococcus).
Due to fetal infection.
Trauma: Maternal trauma (Ex : Accident and physical injury.
Other factors: such as multiple gestations such as twins.
Due to drug and substance abuse.
Environmental factors (such as exposure to toxins).
Sign And Symptoms:
- Fetal movement Absent.
- Uterine height appears smaller than for gestational period.
- Uterine tone is diminished.
- Brakestone Hicks contractions are not felt.
- Fetal movement is not felt during palpation.
- First the fetal heart sound (FHS) is audible, then the fetal heart Sound (FHS) is found absent.
Diagnostic Evaluation:
- History collection,
- Physical examination,
- Sonography: It shows absent fetal movement.
- Gradual oligohydroamnios condition and cranial bone collapse are seen in the fetus.
- Straight abdominal X-ray:
- a. Spalding’s sign: Irregular overlapping of the cranial bones, usually seen 7 days after fetal death.
- b. Hyperflexion of the spine is seen.
- C. Loss of normal parallel A with crowded rib shadows.
- d. Appearance of gas shadow (Robert’s sign).
- Estimation of fibrinogen level and partial thromboplastin time (especially if the fit is maintained for more than 2 weeks).
- Hytological examination such as,
- ABO and Rh grouping.
- VDRL.
- Post prandial blood sugar.
- HbA1C.
- BUN.
- Thyroid profile.
- TORCH test.
- Lupus anticoagulant and anticardiolipin antibody.
Management:
Prevention:
- The patient should be -Provide conception counseling and care.
- Proper prenatal diagnosis of the patient.
- Proper screening of high risk mothers.
- Terminate the pregnancy if fetal compromise is suspected.
Expectant management:
- In 80% of cases, spontaneous delivery occurs within two weeks of the onset of labor, and the patient is provided with education for admission to the hospital.
- Fibrinogen estimation of the patient should be done every week.
- In early delivery, admit to the hospital and induce labor.
- Oxytocin infusion is done when the cervix is favorable.
- When the cervix is unfavorable, prostaglandin gel is placed in the posterior fornix.
- Misoprostol (PGE 1) 25-50 micrograms vaginally or orally is effective.
- Caesarean section is mostly performed in cases of major degree placenta previa and transverse lie.
- Provide proper psychological support to the patient.
- Fits a Properly explain the cause of death.
- Since the patient is at high risk of postpartum depression, provide support through a psychologist or counselor when needed.
- Review the patient’s investigation reports and then provide counseling for future pregnancies.
- Advise the patient to follow up regularly.
High-risk pregnancy:
Screening and Assessment for High Risk:
Pregnancies that are at risk of developing serious complications are considered high-risk pregnancies.
All pregnancies are evaluated to identify whether there are risk factors or the chances of them occurring. By classifying pregnancies as high risk, if they require extra attention, they can be provided in an adequate amount.
Screening options are available to assess the risk for specific congenital anomalies during pregnancy and do not involve the risk of miscarriage.
If evaluation of high-risk women is done early, high-risk pregnant women can be referred to a perinatal center before delivery, which can reduce neonatal morbidity and mortality rates.
The most common reason for referral is preterm delivery, which is usually due to premature rupture of membranes.
A major benefit of screening and assessment of high-risk mothers is that if there are any complications or problems in the mother and baby, they can be detected early, leading to better outcomes in the health status of the mother and baby. And the mother can give birth to a healthy baby.
High risk cases such as,
Obstetrical history:
Previous stillbirth,
Previous neonatal death,
Previous premature infant,
History of recurrent abortion.
Mother’s medical history such as,
Maternal illness,
Chronic hypertension,
Abnormal PAP smear Tests,
Insulin dependent diabetes,
Renal disease,
Rh- isoimmunization,
Maternal physical risk factors,
Incompetent cervix,
Uterine malformation.
Risk factors of current pregnancy,
Moderate to severe preeclampsia (including hypertension, edema (weight gain), proteinuria (protein in urine), and albuminuria) found),
Polyhydroamnios (i.e. when the amount of amniotic fluid exceeds 2000 ml),
Oligohydroamnios (when the amount of amniotic fluid at term is less than 200 ml, it is called oligohydroamnios.),
Placenta previa (when the placenta partially or completely implants near or above the internal os of the uterus, it is called placenta previa).
Multiple pregnancy (When more than one fetus develops in the uterus at the same time, it is called multiple pregnancy).
Abruptio placentae (Abruptio placentae is a form of antepartum hemorrhage (APH) in which the normally situated placenta prematurely separates from the uterine wall, causing bleeding called placental abruption.)
Other high risk Pregnancy:
Abnormal fetal position,
Vaginal bleeding,
Malpresentation,
Small for gestational age,
Hb level less than 10 g/dl,
Poor weight gain,
Proteinuria,
Glycosuria,
Systolic BP. More than 155 mm of Hg.
Vaginal infection. Etc.
Things to consider during early pregnancy are —
Blood testing, which monitors the mother’s hemoglobin level, ABO and Rh group, and blood sugar level.
Excessive weight gain in the mother is usually due to fluid retention. And if the weight of the mother is reduced, then due to this there is also a risk of developing the condition of intrauterine growth retardation (IUGR).
A history of previous hypertension or pregnancy induced hypertension (PIH) can be a risk factor for the mother as well as the fetus.
If the amount of amniotic fluid is high or the amount of amniotic fluid is reduced, then these are also called risk factors.
For high-risk cases, another approach should be followed as follows is:
Maternal Serum Alpha Phyto Protein (MSAFP):

- Alpha Phytoprotein (AFP) is an oncofetal protein and is produced in the yolk sac and fetal liver.
- Fetal serum and amniotic fluid have their highest levels at approximately 13 weeks and maternal serum at 32 weeks.
- Maternal serum and amniotic fluid are tested for alpha phytoprotein (AFP). This is usually done when the fetus is at risk of neural tube defects and other congenital defects. If the level of alpha-feto protein (AFP) is high, it indicates fetal pathology, open neural tube defect and if the level of alpha-feto protein (AFP) is low, it suggests conditions like Down syndrome and gestational trophoblastic disease.
- In some cases, the amount of maternal serum alpha-feto protein (MSAFP) is increased, such as conditions like multiple pregnancy, open neural tube defect, renal anomaly, Rh isoimmunization, IUFD (intrauterine fetal death), anterior abdominal wall defect etc.
- This test is done between 15 and 18 weeks of gestation. It is done during the week.
Chorionic Villus Sampling (CVS):
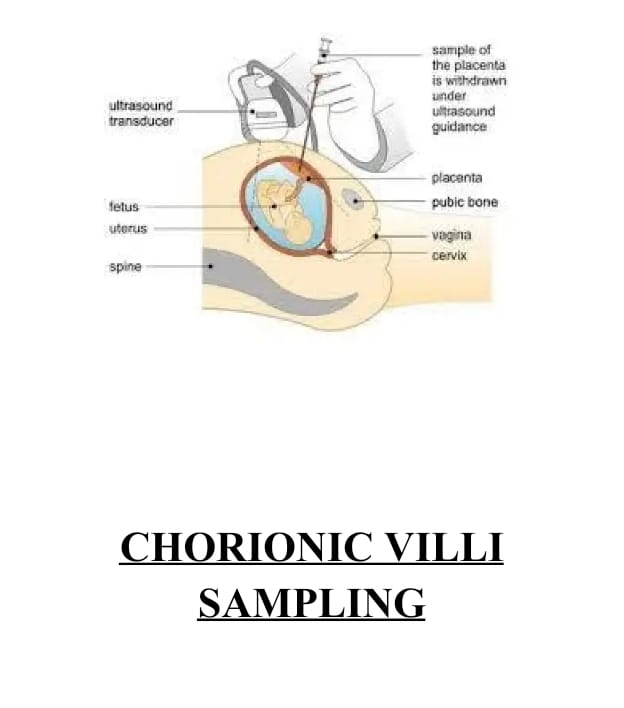
- Chorionic villus sampling is done under ultrasound guidance transcervically at 10-12 weeks and transabdominally at 10 weeks for prenatal diagnosis of genetic disorders.
A few of these cells can be collected from the chorion frondosum, transcervically (a catheter is introduced through the cervix), or transabdominally (a needle is inserted through the uterine wall into the maternal abdomen into the placental tissue). Diagnosis is usually obtained within 24 hours. - The positive aspect of this test is that the results are obtained early, and if termination is necessary, it can be done only in the first trimester. This test is also associated with fetal loss, limb deformities, and vaginal bleeding, etc. In addition to miscarriage, there is a risk of infection and amniotic fluid leakage.
As a result, amniotic fluid can leak, which can develop into a condition known as oligohydramnios, which is low amniotic fluid levels.
The time to test is after 10 weeks.
Cordocentesis (percutaneous umbilical blood sampling):
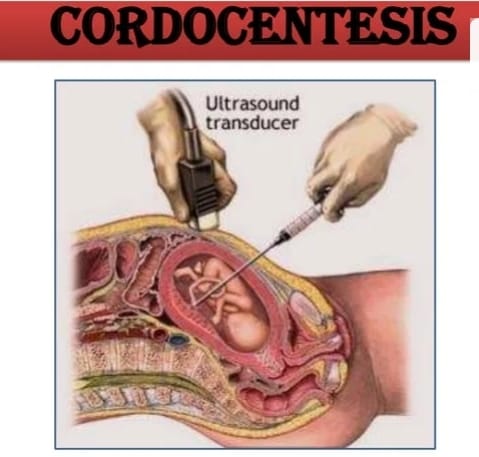
- In this test, a fetal blood sample is collected during pregnancy and then any chromosomal abnormality or blood disorder is diagnosed. In this, the umbilical vein is punctured under the guidance of ultrasound and a needle is inserted. And then 0.5 to 2 ml of fetal blood is collected. This test can cause conditions such as preterm labor, abortion or intrauterine fetal death.
- The time to do this test is after 18 weeks.
Triple test:

- This test combines three tests, including,
- Maternal serum alpha fetoprotein (MSAFP), human chorionic gonadotrophin (HCG), and unconjugated estriol (UE) Involvement occurs.
- This test is used to detect Down syndrome.
- If the pregnancy is affected, the levels of maternal serum alpha feto protein (MSAFP) and estrogen are low and the levels of human chorionic gonadotropin (HCG) are high.
Amniocentesis:
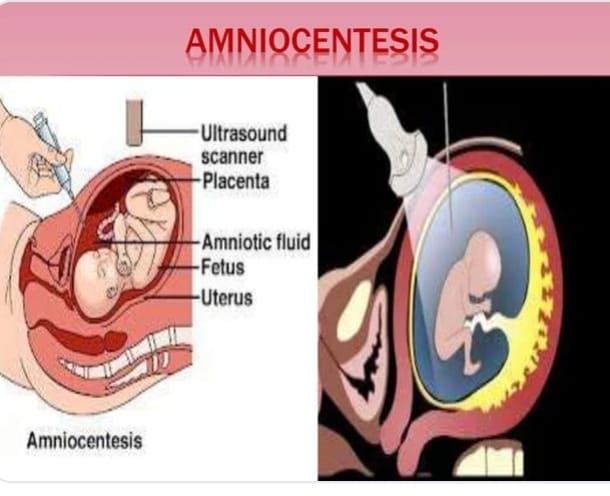
- This is an invasive procedure that is usually performed under ultrasound guidance at 16-18 weeks to identify the sites of fetal cells. The analysis is done for DNA analysis and biochemical tests of the fluid.
- In this procedure, a fine needle is inserted trans-abdominally into the amniotic cavity and amniotic fluid is aspirated from it.
Procedure –
- Before the actual procedure, a local anesthetic is given to relieve pain while inserting the needle used to withdraw the amniotic fluid.
The needle is inserted through the mother’s abdominal wall and through the wall of the uterus into the amniotic sac. - Using ultrasound guidance, the needle is guided to an area of the sac that is away from the fetus and approximately 20 ml of amniotic fluid is withdrawn for testing. Amniotic fluid contains cells that are shed by the developing fetus.
- The cells are checked for the number and size of chromosomes (karyotype) to see if there are any problems that put the baby at risk for certain conditions. After the amniotic fluid is removed, the fetal cells are separated from it.
- The cells are grown in a culture medium, then fixed and stained.
The chromosomes are examined under a microscope for abnormalities. - This test detects the most common abnormalities, most commonly chromosomal disorders such as Down syndrome, Edward syndrome (trisomy 18) and Turner syndrome, and neural tube defects such as spina bifida and anencephaly.
This test can identify hundreds of genetic disorders. - Amniocentesis can also detect whether the mother or baby is Rh-negative and whether the baby’s lungs are mature enough for birth if immediate termination is needed. Amniocentesis cannot detect every type of abnormality, for example, it cannot tell whether a baby has a cleft lip or a cleft palate.
- Amniocentesis is performed during pregnancy when:
- A woman who has had a previous chromosomally affected pregnancy or a genetic disorder, such as Down syndrome or other defects, is confirmed to have a chromosomal abnormality detected by ultrasound examination. Indicates an increased risk of chromosomal abnormalities.
- When there is a history of any genetic disorder or birth defect in the parents or someone in the family.
- In women who are older than 35 years.
- In women who are concerned about their child having a chromosomal abnormality due to their request.
- Risk Associated with Amniocentesis:
- Maternal and fetal hemorrhage,
infection,
fetal injury,
miscarriage.
During late pregnancy:
- Biophysical
- Fetal movement count, cardiotocography, non-stress test for uteroplacental insufficiency, Biophysical investigations like Fetal Biophysical Profile (BPP), Doppler Ultrasound, Contraction Stress Test (CST), Amniotic Fluid Volume etc. are done.
Fetal Movement Count:
- Cardiac count 10 formula :
- In this, the patient starts counting fetal movements from 9 am and stops when 10 movements occur, within 12 hours for two consecutive days. If you have fewer than 10 movements or not even one movement in a day, you are asked to inform your doctor.
Daily Fetal Movement Count (DFMC):
- In this test, you count three counts in each period of morning, afternoon and evening and multiply it by four. If you have more than 10 movements in 12 hours or less than three movements in each period, then it is indicated that you have a problem with the fetus.
Diagnosis Modalities Invasive and Noninvasive:
- Different invasive and non-invasive methods are used for prenatal screening and diagnosis.
- In which non-invasive methods (methods in which no instrument needs to be inserted into the body by opening it),
- Examination of the uterus from the outside of the body.
- Ultrasound detection.
Fetal heart sound Hearing (FHS). - External fetal monitoring, such as a non-stress test (NST), may be involved.
- Invasive methods (a medical procedure that invades (enters) the body, usually by cutting or puncturing the skin or inserting an instrument into the body)
Such as, - Chorionic villus sampling,
Amniocentesis,
Cordocentesis,
Maternal serum alpha-fetoprotein (MSAFP) Involvement of.
Ultrasound Scan (USG):

- Ultrasound scan is a generally safe, non-invasive, accurate and cost-effective investigation. In an ultrasound scan, high-frequency sound waves are transmitted into the uterus.
- In ultrasound, the echoes bounced off and returned by the baby are translated by a computer into an image on a screen that shows the baby’s position and movements. Hard tissues, such as bone, reflect the largest echoes and appear white in the image, and smooth tissues appear gray and speckled. Fluid (such as the amniotic fluid in which the baby is located) does not reflect any echoes and therefore appears black.
- It is the difference between these different colors of white, gray, and black that allows the sonographer to interpret the image when scanning the abdomen early in pregnancy, as the procedure often requires a full bladder.
Uses of Ultrasound:
To check the viability of the fetus
- The heartbeat of the fetus can be checked through ultrasound. *To check how many fetuses are surviving in the uterine cavity/To check the number of fetuses. Usually before 14 weeks of pregnancy, it tells whether a woman is pregnant with a single baby. Ultrasound scanning is used to check whether the fetus is alive and whether it is a single fetus or one of twins or triplets.
Ectopic To detect pregnancy
- It is used to detect any abnormality such as an ectopic pregnancy or a condition in which the fetus implants outside the uterine cavity, mainly in the fallopian tube.
- Doppler Umbilical Velocimetry Doppler ultrasonography measures the speed at which R.B.C. travel in the blood vessels of the uterus and fetus. This is helpful in determining whether a woman with diabetes or gestational hypertension is experiencing increased vascular resistance and resulting placental insufficiency.
Placental Grading:
- Placental grading is generally based on the amount of calcium deposited in the placenta. The placenta can be graded as 0 (12-24 weeks), 1 (30-32 weeks), 2 (36 weeks) or 3 (38 weeks).
Amniotic Fluid Volume Assessment
- If the fetus is stressed in the uterus as the amniotic fluid decreases, the fetus is put at risk of umbilical cord compression and this can interfere with its nutritional levels.
Before 20 weeks, the uterus is divided into two vertical lines with a midpoint (linea nigra). The vertical diameter of the largest pocket of amniotic fluid present on each side is measured in centimeters (cm). The amniotic fluid index (AFI) is the sum of the two. After 20 weeks, the uterus is divided into four parts and the sum of the four is taken. Average AFI: 12-15 cm (28-40 weeks); 5-6 (oligohydramnios), 20-24 (polyhydramnios). - To detect the cause of vaginal bleeding
Ultrasound helps to find the cause of any bleeding that the mother experiences. In cases of vaginal bleeding, the viability of the fetus is measured by ultrasound. Visible heartbeats can be seen and detected by pulse Doppler ultrasound at about 6 weeks and are usually clearly delineated at 7 weeks. - To find out the accurate date of pregnancy
The exact date of pregnancy can also be determined by measuring the baby. Such measurements should be done as early in pregnancy as possible to arrive at the correct dating for patients with an uncertain last menstrual cycle. The measurements taken are:
a) Crown-rump length (CRL):
This measurement can be taken between 7 and 13 weeks and gives a very accurate estimate of gestation.
b) Biparietal diameter (BPD)
The diameter between the 2 sides of the head. This is measured after 13 weeks. It increases from about 2.4 cm at 13 weeks to about 9.5 cm at term.
c) Femur Length (FL)
Measures the longest bone in the body and reflects the longitudinal growth of the fetus. Its utility is similar to BPD. It increases from about 1.5 cm at 14 weeks to about 7.8 cm at term.
d) The Abdominal Circumference ( AC )
The single most important measurement to take in late pregnancy. It reflects the size and weight of the fetus more than its age.
To assess the risk of Down syndrome
At 11-14 weeks The presence of Down syndrome can be detected by measuring the fluid at the back of the child’s neck (called a nuchal translucency scan). Some major abnormalities can also be detected at this stage. At 11 to 14 weeks, a measurement of the thickness of the skin at the back of the neck (known as a nuchal translucency measurement) can be used to measure the risk of the fetus having a chromosomal abnormality. A Blurred test can be done to find out why the abnormality is present.
To assist in performing diagnostic tests
Some tests to assess the fetus’s well-being, such as CVS or amniocentesis, can be safely performed using ultrasound to show the position of the baby and placenta.
Development of Fetus
After 18 weeks, it is possible to examine the fetus in more detail. Most organ systems can be examined to ensure that the fetus’s development appears to be normal.
To diagnose certain types of abnormalities
Such as spina bifida. Many structural abnormalities in fetuses can be reliably diagnosed by ultrasound scan, and this can usually be done before 20 weeks.
To assess the amount of amniotic fluid and locate the placenta
Liker, i.e., too much or too little amniotic fluid, can be clearly detected by ultrasound, and both of these conditions can adversely affect the fetus. Ultrasonography is also important for detecting the location of the placenta. Due to which, if there is any abnormal site of presentation, it can be detected early, such as placenta previa.
Ultrasonography is also important for other obstetric conditions such as,
a) When there is a need to confirm intrauterine death.
b) To check fetal presentation in some cases.
c) When there is a need to evaluate fetal movement, tone and breathing in the biophysical profile. Then.
d) To diagnose uterine and pelvic abnormalities during pregnancy.
Ex: fibromyomata, ovarian cyst.
Ultrasound scan can be done both vaginally and abdominally
Vaginal Scan (Vaginal Scan)
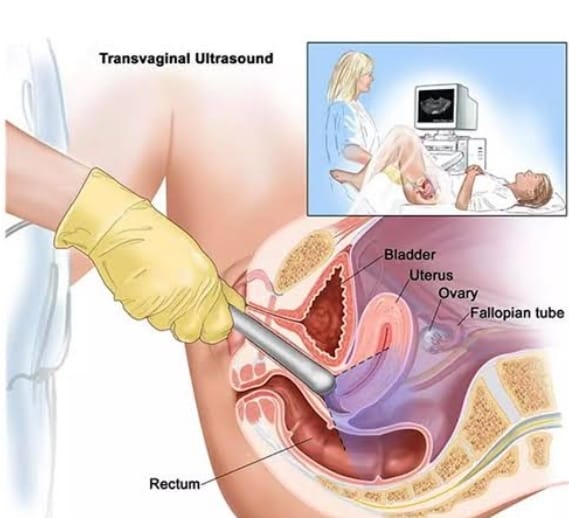
- Vaginal scan It is only done during the first 12-14 weeks of pregnancy. This is because the fetus is very small at this stage and a vaginal scan provides a better view compared to an abdominal scan. In a vaginal scan, the mother is asked to lie down on her back and a lubricated sensor is inserted into the vagina. This sensor is usually covered by a condom.
Abdominal scan
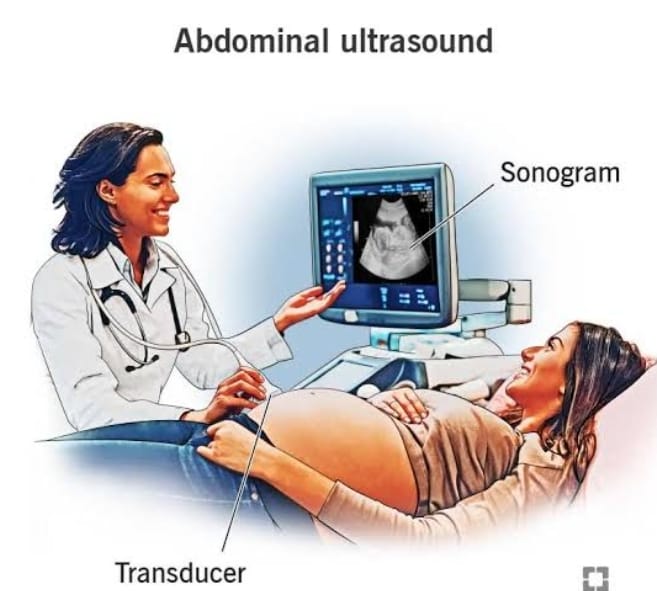
- Abdominal scans are usually used after 12 to 14 weeks of pregnancy. In an abdominal scan, the mother is asked to lie on her back. A gel is applied to her skin over her lower abdomen. The gel allows the sensor to slide easily over her skin and helps produce a clear image. The sensor is held firmly against the skin and moved over the abdominal surface.
Doppler ultrasound
- Doppler ultrasound is currently most widely used to detect the fetal cardiac pulsation and the pulsation in the fetal various blood vessels. Further developments in Doppler ultrasound technology in recent years have enabled a great expansion in its application in obstetrics. It is particularly useful in the area of assessing and monitoring the well-being of the fetus, its progression, and in diagnosing intrauterine growth restriction and cardiac malformations.
Cardiotocography (CTG):
- Cardiotocography (CTG) graphically records the fetal heartbeat and uterine contractions.
It is generally performed during the third trimester. The machine used to perform the monitoring is called a cardiotocograph and is also known as an electronic fetal monitor (EFM) or external fetal monitor (EFM). - Two transducers are used externally, strapped to the abdominal wall. One measures the fetus’s heart rate and the other measures uterine contractions.
- Internal measurements can also be performed. This requires a certain degree of cervical dilation, as it involves inserting a pressure catheter into the uterine cavity and attaching scalp electrodes to the fetus’s head to adequately measure the pulse. It is preferred when there is a possibility of a complicated birth. Cardiotocography is also used to perform non-stress tests (NST) and contraction stress tests (CST).
Non-stress tests (NST):

- In the non-stress test (NST), the well-being of the fetus is evaluated by monitoring the fetal heart rate (FHR) in response to fetal movement. This test does not put any special stress on the fetus. In a non-stress test, a belt is attached around the mother’s abdomen to monitor the fetus’s heart rate and uterine contractions.
- A non-stress test is a common prenatal procedure that is usually performed during the third trimester to assess fetal health. The heart rate is recorded for about 20-30 minutes, during which the mother indicates whether she feels any movement of the fetus. The short-term variation in the baseline should be between 10 and 15 bpm. And if the variation cannot be reduced for a long time with other abnormalities, then there may be fetal distress.
Purpose:
- The primary goal of the NST (non-stress test) is to monitor the baby’s heart rate and assess how the fetal heart rate (FHR) responds to movement. It helps evaluate the fetus’s well-being and can provide insight into the baby’s oxygen levels and overall health. NST is usually used in cases where there is concern about the health of the fetus or when there is a risk of complications.
Position and Preparation of Mother:
- Non-stress stress (NST) is usually performed by providing the mother with a properly comfortable position. The fetus should not be in a sleeping condition while performing this test because it can cause variations in the fetal heart rate, i.e. fetal heart rate. A decrease in rate may be seen. Fetuses are evoked by abdominal palpation or a buzzer. Advise the woman to press the button when she feels fetal movement and monitor the fetal heart rate (FHR).
Advantages:
- This is a non-invasive test.
- This test is simple,
- Inexpensive and less time consuming.
- This test has no contraindications or complications.
- No special expertise is required to perform this test.
- This test can provide an immediate answer.
Interpretation of Test:
Reactive Test (Normal Stress Test (NST)):
The test is considered to be valid when the fetal heart rate (FHR) in response to fetal movement is 15-30 seconds above baseline and the test is considered to be valid. Reactive. When there are two or more such events in a 10-minute period or five or more accelerations in a 20-minute period, the test is considered normal.
Non-reactive test (abnormal non-stress test):
A non-reactive test is said to be when the fetal heart rate is absent in response to the fetus’s movement. The test is considered abnormal when the fetal heart rate is less than 15 beats/minute in response to fetal movement and lasts less than 15 seconds.
Suspicious non-stress test
In this, there is an acceleration of the fetal heart rate in response to fetal movement, but the beats above baseline, the number of accelerations, or the length of duration do not meet the criteria for being reactive or non-reactive.
Indication of non-stress test (NST) ):
A woman who has any pre-existing medical conditions such as diabetes or conditions that arose during pregnancy, such as
hypertension.
When a pregnant woman reports that fetal movement is less than usual. Intrauterine growth retardation (IUGR) is a condition in which a child does not grow properly for its normal age. When the amount of amniotic fluid is too high or the amount of amniotic fluid is too low. In a woman who has lost her baby in a previous pregnancy.
This test is performed to check the baby’s breech position in a woman whose pregnancy continues after 40 weeks of pregnancy.
The woman may undergo external cephalic version (to turn the baby breech) or amniocentesis (to After performing a procedure (such as determining whether the lungs are mature enough for birth or to rule out an infection of the uterus), the health care practitioner may perform a non-stress test (NST) to ensure the baby’s well-being.
Contraction Stress Test (CST):

Contraction Stress Test
- (CST) is used to assess the health condition of the fetus and the fetal heart rate (FHR) in a woman when the oxygen level of the fetus is reduced during uterine contractions. This test assesses the response of the fetal heart rate to uterine contractions induced by oxytocin.
- External heart monitoring is done in this test. During uterine contractions, the fetus’s blood and oxygen supply drops for a short time. This condition is not a problem for most babies, but in some babies, their heart rate slows down. These changes in heart rate are monitored on an external fetal monitoring device. This test is usually performed when a woman is 34 weeks or more pregnant.
Preparation of Mother:
- In this, the woman is provided with a semirecumbent position, a lateral tilt position, and a properly comfortable position. Uterine contractions are then recorded for 20 to 30 minutes. If uterine contractions are three or more in 10 minutes and their duration is usually more than 40 seconds, no stimulation is required. If spontaneous stimulation is absent, stimulation is induced by providing oxytocin. In the oxytocin challenge test, a diluted oxytocin solution is administered intravenously. Then increase the rate of infusion at small intervals until three or more uterine contractions are observed in 10 minutes for more than 30 minutes, then stop the oxytocin infusion after recording,
- Contraction stress test is done to check the following conditions, such as,
- It is used to assess the well-being of the fetus and to assess the fetal heart rate (FHR) during the process of labor or during uterine contractions when the amount of oxygen is low.
Contraindications
- If the woman has the condition of placenta previa,
- If the woman has the condition of antepartum hemorrhage (APH),
- If a previous classic cesarean section has been performed,
- Clients who are at high risk of preterm labor
Risk
- Labor may start earlier than the normal expected date of delivery.
- Problems in the baby may arise due to prolonged contractions.
Interpretation:
- This contraction stress test (CST) is used to assess the health status of the fetus due to the reduced blood and oxygen supply when a woman is in labor.
Normal Contraction Stress Test (CST)
- A normal test result is called negative. In which the baby’s heart rate does not slow down (decelerate). But the contractions (late deceleration) become slow.
Abnormal Contraction Stress Test (CST)
- A positive result of an abnormal contraction stress test (CST) is one in which the fetus’s heart rate slows and remains continuously slow even after contractions, meaning that the fetus may have problems during normal labor. It can also mean that if the delivery time is delayed, the baby may have problems.
Hyperstimulation
- In hyperstimulation, contractions last for 90 seconds or more.
- Suspicious
- There is a late declaration of fetal heart rate, but this is not repetitive and does not occur with continuous contractions.
- Unsatisfactory
- The quality of the recording is not that good.
Anemia.
- Anemia is the most common blood disorder seen in women during pregnancy. It is usually more common in areas with poor socioeconomic conditions. Anemia is a condition in which the circulating red blood cells and hemoglobin levels are lower than their normal levels (reduced number). Due to this, the oxygen carrying capacity of the red blood cells decreases. It is usually seen due to various reasons such as nutritional deficiency (iron, vitamin B12, or folate), chronic disease, genetic condition, and blood loss.
- Normal Hb in females: 12-16 gm/ dl.
- If the hemoglobin level in females is between 10 gm/ dl – 11.9 gm/ dl, it is called mild anemia.
- If the hemoglobin level in females is 7 gm/ dl – If it is between 9.9 gm/ dl, it is called moderate anemia.
- If the hemoglobin level in a female is less than 7 gm/ dl, it is called severe anemia.
Classification:
1. Physiological anemia.
2. Pathological anemia.
1. Physiological anemia: Plasma volume red in pregnancy Blood cell (RBC) volume and hemoglobin mass increase, so the demand for iron increases during pregnancy, especially in the second half of the trimester. Even with an adequate amount of diet, the extra demand for iron is not met, so physiological iron deficiency occurs during pregnancy. Therefore, hemoglobin concentration falls down in pre-pregnancy due to the effect of hemodilution and negative iron balance.
2.Pathological anemia:
Deficiency anemia: Due to iron deficiency, folic acid deficiency, vitamin B 12 deficiency, protein deficiency, etc.
Hemorrhagic:
Acute: Due to bleeding in the early months or antepartum hemorrhage (APH).
Chronic: Hookworm infestation, bleeding piles, etc.
Hereditary: Thalassemia, Sickle Cell Hemoglobinopathy, Other, Hemoglobinopathy, Hereditary Hemolytic.
Bone marrow insufficiency: Hypoplasia or aplasia due to radiation, drugs (aspirin, indomethacin.
Anemia of infection (malaria, tuberculosis).
Chronic disease (renal) or neoplasm.
Etiology:
- Due to nutritional deficiency.
- Due to chronic diseases.
- Due to genetic factors.
- Due to blood loss.
- Due to infection.
- Bone marrow disorder Due to.
- Due to vitamin deficiency.
- Due to impaired production of red blood cells.
- Due to excessive blood loss.
- Due to decreased production of red blood cells.
Sign And Symptoms:
- Fatigue,
- Weakness,
- Paleness of the skin, conjunctiva and mucous membranes,
- Shortness of breath,
- Dizziness,
- Headache Pain,
- Rapid and irregular heartbeat,
- Cold hands and feet.
- Brittle nails.
- Poor concentration.
- Cognitive difficulties.
- Growth and development Delay.
- No appetite.
- Dizziness.
- Tachypnea.
- Tachycardia.
- Palpitation.
- Diarrhea and vomiting.
- Cardiac enlargement with murmur sound.
- Jaundice, petechiae and ecchymosis may also be present in some cases.
- Hepatomegaly may occur.
Diagnostic Evaluation:
- History Taking,
- Physical Examination,
- Complete Blood Count Test.
- Peripheral Blood Smear.
- Additional Blood Tests.
- Bone Marrow Aspiration and Biopsy.
- Imaging test.
- X-ray.
- CT scan.
- M .R .I.
- Genetic testing.
- Stool examination
Management:
- Assess the cause of anemia in the woman.
- If the woman’s anemia condition is due to nutritional deficiency, provide the child with adequate nutritional supplements such as iron, vitamin B12 and folate.
- Provide the woman with a nutritious diet rich in iron. To do.
- Provide adequate supplementary diet to the woman according to nutritional deficiency.
- If the woman’s condition of anemia is due to any infection or chronic disease, then treat that condition of the woman immediately.
- If the woman has a condition of severe anemia, then do proper blood transfusion.
- Monitor the woman regularly.
- If the woman’s anemia is due to excessive blood loss, stop it and start intravenous infusion immediately.
- Provide complete education to the woman and her family members about her condition, its causes, its symptoms and signs, and its treatment.
- Do all the laboratory investigations of the woman.
- Regularly screen the woman to prevent her from anemia. To do.
Iron Deficiency Anemia:
- Iron deficiency anemia is the most common nutritional and hematological disorder seen in pregnancy. It is usually more common in areas with poor socioeconomic conditions.
- Ion deficiency anemia is a condition in which the production of red blood cells decreases due to iron deficiency in children. The condition of anemia caused by the deficiency of iron, which helps in the production of hemoglobin, is called iron deficiency anemia.
Etiology:
- Inadequate iron storage during intrauterine period,
- Prematurity,
- Twin baby,
- Maternal anemia,
- Poverty,
- Certain types of disease conditions Due to reasons like
- Diarrheal disease,
- Infection, malabsorption syndrome,
- Hookworm infestation,
- Due to chronic illness,
- Due to insufficient iron supply at birth.
- Ion Due to impaired absorption.
- Due to blood loss.
- Due to nutritional deficiency.
- Due to chronic diseases.
- Due to genetic factors.
- Due to blood loss.
- Infection Due to.
- Due to bone marrow disorders.
- Due to vitamin deficiency.
- Due to impaired production of red blood cells.
- Due to excessive blood loss.
- Due to increased iron requirement in the body.
- Due to intensive breastfeeding.
- Due to hereditary and genetic factors.
Sign And Symptoms:
- Fatigue,
- Weakness,
- Paleness of the skin, conjunctiva and mucous membranes,
- Shortness of breath,
- Dizziness,
- Headache Pain,
- Rapid and irregular heartbeat,
- Cold hands and feet.
- Brittle nails.
- Poor concentration.
- Cognitive difficulties.
- Growth and development Delay.
- No appetite.
- Dizziness.
- Tachypnea.
- Tachycardia.
- Palpitation.
- Diarrhea and vomiting.
- Cardiac enlargement with murmur sound.
- Jaundice, petechiae and ecchymosis may also be present in some cases.
- Hepatomegaly may occur.
- Irritability may occur.
- Tiredness may occur.
- Atrophy of the tongue papillae may occur.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History Taking,
- Physical Examination,
- Complete Blood Count Test.
- Additional blood tests.
- Bone marrow aspiration and biopsy.
- Serum ferritin level test.
- Total iron binding capacity test.
- Imaging tests.
- X Ray.
- CT scan.
- M .R .I.
- Genetic testing.
- Stool examination
Management:
- The hemoglobin level of a pregnant woman should be checked during the first antenatal visit, then at 28 weeks and finally at 36 weeks.
- Advise the mother to take an adequate well-balanced diet that involves iron, protein and vitamins. Such as,
liver
meat
eggs
green vegetables
peas
figs
beans
whole wheat
green plantain
jaggery
peanuts etc. - The mother should be advised to use iron utensils for cooking and not to discard the water used for cooking rice and vegetables.
- In addition to a well-balanced diet, the mother should be given regular supplementary iron when she is free from nausea. It involves the following:
- Ferrous sulphate -200 mg containing 60 mg elemental iron.
- Tablet folic acid 1 mg (it should be given with ferrous sulphate).
- This tablet should be given till the haemoglobin level does not exceed 13 g/dl.
- Advise the mother to avoid frequent child birth and advise the woman to avoid excessive alcohol consumption during pregnancy. A minimum interval of three years is necessary to allow for replacement of lost iron.
- If the mother’s hemoglobin level is less than 10 g/100 ml, she should be admitted for investigation.
- She should be given oral preparations in the form of medication or capsules.
Available preparations are: - Ferrous gluconate,
Ferrous fumarate,
Ferrous succinate
Three times a day with or after meals Give. - A widely used tablet is Fersolate tablet which contains 200 mg (3 gm) ferrous sulfate and 60 mg elemental iron, copper and manganese.
- The initial dose is one tablet three times a day, given with or after meals. If larger amounts are required, a maximum of six tablets are given daily. This is usually stopped after 3-4 days and the treatment is continued until the blood levels return to normal.
- Mother Advise the mother to start iron preparations as maintenance doses for at least 3 months after delivery to replenish iron stores.
- In cases where the mother is unable to take oral therapy, parenteral therapy should be provided.
It is provided to the mother intravenously (i.v.) or intramuscularly. - Provide adequate supplementary diet to the woman according to nutritional deficiency.
- If the woman has an anemic condition due to any infection or chronic If the woman’s condition is due to a disease, treat it immediately.
- If the woman has a condition of severe anemia, then do a proper blood transfusion.
- Monitor the woman regularly.
- If the woman’s condition of anemia is due to excessive blood loss, then stop it and start intravenous infusion immediately.
- Inform the child and his family members about the child’s condition. Provide complete education about the condition, its causes, symptoms and signs and its treatment.
- Do all types of laboratory investigations on the woman.
- Do regular screening of the child to prevent the woman from the condition of anemia.
- Advise the woman to take adequate rest.
- Provide proper emotional support to the woman and her family members. To do.
- Properly monitor the woman’s condition, including properly recording the vital sign intake output chart.
Sickle Cell Anemia
- “Sickle cell anemia” is a severe hemolytic anemia and a hereditary and genetic blood disorder that normally affects red blood cells, in which the red blood cells have an abnormal sickle shape. In this disease, the red blood cells become rigid, sticky, and abnormally crescent and sickle shaped. The abnormal shape of these red blood cells blocks blood flow, which increases pain, organ damage, and the risk of infection. The life span of sickle-shaped red blood cells is only 30-40 days and their oxygen-carrying capacity is also decreased.
Etiology:
- Due to a genetic mutation.
- Due to a hereditary condition.
- Due to a family history of sickle cell disease.
Sign And Symptoms (लक्षणो तथा चिन्हो (संस्तान अधिक्षणो सिंपतोमान्हो):
- Mild jaundice,
- Fever,
- Headache,
- Fatigue,
- Weakness,
- Skin, conjunctiva and mucous membranes may become pale. ,
- Shortness of Breathing,
- Dizziness,
- Vision Problems,
- Leg Ulcers,
- Speech and Absence,
- Pain Episodes,
- Headache,
- Rapid and irregular heartbeat,
- Cold hands and feet.
- Brittle nails.
- Poor concentration.
- Cognitive difficulties.
- Growth and development delays.
- Loss of appetite.
- Dizziness.
- Tachypnea.
- Tachycardia.
- Palpitation.
- Diarrhea and Vomiting.
- Cardiac enlargement with murmur sound.
- Jaundice, petechiae and ecchymosis may also be present in some cases.
- Hepatomegaly.
- Irritability.
- Tiredness.
- Pneumonia.
- Traumatic rupture of an enlarged spleen.
Diagnostic Evaluation:
- History taking,
- Physical Examination,
- Complete Blood Count Test.
- Peripheral Blood Smear.
- Additional Blood Tests.
- Hemoglobin Solubility Test,
- Bone Marrow Aspiration and Biopsy.
- Serum Ferritin level test.
- Total iron binding capacity test.
- Genetic testing.
Management:
- Regularly supervise the health of the woman.
- Provide adequate hydroxyurea medication to the woman.
- Properly maintain the hydration status of the woman.
- Properly maintain the woman’s blood and electrolyte levels.
- Properly provide antibiotic medication to the woman. To do.
- Improve the woman’s dietary intake, especially providing iron and protein-containing foods to the child.
- If the woman’s condition of anemia is due to nutritional deficiency, then provide the child with adequate nutritional supplements such as iron, vitamin B 12 and folate.
- Provide the woman with a nutritious diet containing iron.
- Provide adequate supplementary diet to the woman according to nutritional deficiency.
- If the woman’s condition of anemia is due to any infection or chronic disease, then treat that condition of the woman immediately.
- If the woman has a condition of severe anemia, then do proper blood transfusion.
- Monitor the woman regularly.
- If the woman has anemia If the condition is due to excessive blood loss, stop it and start intravenous infusion immediately.
- Provide analgesic medication to the woman if she has a pain condition.
- Provide complete education to the woman and her family members about the child’s condition, its causes, its symptoms and signs, and its treatment.
- Perform all types of laboratory investigations on the woman.
- To prevent women from the condition of anemia, screen women regularly.
- To advise women to take adequate rest.
- To provide proper emotional support to the woman and her family members.
- To properly monitor the woman’s condition, including recording vital signs and intake output charts.
Thalassemia:
- Thalassemia is a group of hereditary hemolytic anemias. It is an autosomal recessive genetic disorder in which there is a reduction in the synthesis of hemoglobin/inadequate amount of production. Thalassemia is a genetic blood disorder in which the body does not produce enough hemoglobin (a protein in red blood cells that carries oxygen into the body). This results in large amounts of red blood cells being destroyed, causing the condition of anemia.
- There are two main types of thalassemia.
1) Alpha thalassemia,
2) Beta thalassemia,
1) Alpha Thalassemia,
Alpha thalassemia is caused by a missing or mutated alpha chain of hemoglobin.
1)Silent carrier
In this, one or both alpha globin genes are missing or mutated but no symptoms are seen.
2)Alpha thalassemia trait
In this, two alpha globin genes are missing or It is mutated. And due to this, a condition of mild anemia arises, and mild symptoms are seen such as fatigue or pale skin.
3) Hemoglobin H Disease
In this, three alpha globin chains are missing and mutated, causing a condition of moderate to severe anemia. It is characterized by more pronounced anemia, jaundice, enlarged spleen and other symptoms.
4) Alpha Thalassemia Major
In this, all four alpha globin genes are missing and severely mutated. Due to this, severe anemia and other health problems are seen.
2) Beta Thalassemia,
Beta thalassemia is seen due to the missing or mutation of the beta chain of hemoglobin.
1) Beta thalassemia trait
In this, one beta globin gene is missing and mutated and mostly symptoms are not seen.
2) Beta Thalassemia Intermedia
In this, both beta globin genes are affected to a moderate degree, the symptoms are very wide. Due to this, the condition of mild to severe anemia is seen. Sometimes transfusion is also required in it.
3) Beta Thalassemia Major (Coolis Anemia)
In this, both beta globin genes are severely affected. Due to which the condition of severe anemia arises. In this, transfusion is required starting from childhood and continuing throughout life.
Other Classification of the Thalassemia
1) Thalassemia Major,
2) Thalassemia Intermedia,
3) Thalassemia Minor
1. Thalassemia Major (Cooley Anemia):
Thalassemia Major is the most severe form of thalassemia.
It occurs when a child inherits two mutated beta globin genes, one from each parent. This results in a significant reduction or absence of beta globin chains, which is a condition of severe anemia.
A person with thalassemia major requires lifelong blood transfusions from childhood to maintain hemoglobin levels and prevent complications.
Without treatment, thalassemia major can cause growth retardation, organ damage, and bone problems, and other health-related conditions.
2. Thalassemia intermedia:
Thalassemia intermedia is an intermediate form of thalassemia, which is less severe than thalassemia major but more severe than thalassemia minor. People with thalassemia intermedia have two mutated beta globin genes, but the degree of severity varies.
Symptoms can range from mild to moderate anemia, and some patients may also require blood transfusions to manage symptoms. Treatment needs vary depending on the severity of symptoms in patients with thalassemia intermedia. Patients with thalassemia intermedia may develop complications such as bone deformities, enlarged spleens, and gallstones, but these are usually less severe than those with thalassemia major.
3. Thalassemia minor (trait):
Thalassemia minor, also known as thalassemia trait, is the mildest form of thalassemia. It occurs when a child inherits a mutated beta globin gene from one parent and a normal beta globin gene from the other parent. Patients with thalassemia minor usually have no symptoms or only mild symptoms of anemia.
Thalassemia minor carriers usually have slightly lower hemoglobin levels than normal, but they usually do not need treatment. However, carriers of Thalassemia Minor can pass on the gene mutation to their children.
Etiology:
- Due to genetic mutations,
- Due to impairment in alpha globin and beta globin.
Due to family history.
Sign And Symptoms :
- Fatigue,
- Pale skin, conjunctiva, and mucous membranes,
- Shortness of breath,
- Spleen and liver enlargement (hepatosplenomegaly),
- Jaundice,
- Growth and development may be delayed,
- Bone abnormalities,
- Heart problems,
- Endocrine complications,
- Infections.
- Loss of appetite (anorexia),
- Feeding habits become poor,
- Abdominal distension,
- Failure to thrive,
- Facial features – upper maxilla hypertrophied, exposing of upper teeth, depressed nasal bridge,
- Mal occlusion of teeth,
- Lymphadenopathy or hypogonadism,
- Osteoporosis of
- Metacarpals and metatarsals.
- Recurrent respiratory infection,
- Lymphnode enlargement,
- Poor nutritional status.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History Taking,
- Physical Examination,
- Complete Blood Count Test,
- Hemoglobin Electrophoresis,
- Peripheral Blood Smear,
- Iron Studies,
- Genetic Testing,
- Bone Marrow Examination,
- General
- Serum Bilirubin Test,
- Serum iron level,
- Bone marrow studies,
- Osmotic fragility test,
- Radiological findings,
Management:
- The patient requires repeated blood transfusions. The patient requires blood transfusions starting from early childhood and throughout life.
- Provide proper iron chelation therapy to the patient. The patient is at risk of iron overload due to long-term transfusion, due to which iron chelation therapy is provided to the patient to prevent this condition.
This iron chelation therapy involves (deferoxamide, deferiprone, deferasirox). - Properly provide folic acid supplement to the patient.
- Perform bone marrow transplantation to the patient.
- Properly provide gene therapy to the patient.
- Provide proper supportive care to the patient.
- Nursing Management of Thalassemia:
- Provide complete education to the patient about the condition, its causes, its symptoms and signs, and its treatment.
- Continuously monitor the patient.
- Provide proper blood transfusion to the patient. Do.
- Assess the patient for any reaction to the blood transfusion.
- Perform regular health supervision of the patient.
- Properly maintain the patient’s hydration status.
- Properly maintain the patient’s blood and electrolyte levels.
- Properly provide antibiotic medication to the patient. To do.
- Improve the patient’s dietary intake, especially by providing iron and protein-containing foods to the child.
- If the patient’s anemia condition is due to nutritional deficiency, then provide the patient with adequate nutritional supplements such as iron, vitamin B 12 and folate.
- Provide the patient with a properly iron-rich nutritious diet.
- Provide adequate supplementary diet to the patient according to nutritional deficiency.
- If the patient’s anemia condition is due to any infection or chronic disease, then treat that condition of the child immediately.
- If the patient has a condition of severe anemia, then do proper blood transfusion.
- Monitor the patient regularly.
- If the patient has anemia If the condition is due to excessive blood loss, stop it and start intravenous infusion immediately.
- Provide analgesic medication if the patient is in pain.
- Provide complete education to the patient and his family members about the child’s condition, its causes, its symptoms and signs, and its treatment.
- Perform all types of laboratory investigations on the patient.
- To prevent the patient from the condition of anemia, screen the child regularly.
- To advise the patient to take adequate rest.
- To provide proper emotional support to the patient and his family members.
- To properly monitor the patient’s condition, including proper recording of vital signs and intake output charts.
Jaundice:

- Jaundice is also called icterus. Jaundice is not a disease but it is seen as a sign of disease after many diseases. Jaundice is a condition that when the amount of bilirubin in the body increases, the skin, mucous membranes, sclera of the body become yellow in color, it is called jaundice. Jaundice is seen when the amount of bilirubin in the body increases more than 2 mg/dl, then the condition of jaundice is seen.
- (Note:=Normal bilirubin level is 0.8 to 1.2 mg/dl.) In jaundice: Bilirubin level increases more than 2mg/dl.
- { Direct/Unconjugated/Fat Soluble Bilirubin Level is 0.1-0.3 mg/dl.}
- { Indirect/Conjugated/Water Soluble Bilirubin Level is 0.2-0.8mg/dl.}
- Bilirubin is a natural product that is released as a byproduct due to the breakdown of red blood cells and is excreted out of the body by the liver. The condition of jaundice arises when the amount of conjugated bilirubin is too high to be removed from the body by the liver using the biliary system. Bilirubin is not excreted. And the condition of jaundice arises due to the accumulation of bilirubin in the body.
Types of jaundice
There are four types of jaundice in total:
1. Hemolytic jaundice,
2. Obstructive jaundice,
3. Hepatocellular jaundice
4. Hereditary jaundice
1. Hemolytic jaundice:
- Hem means: “Blood”
Lytic means:
“Breakdown of cells” - Hemolytic jaundice is also called prehepatic jaundice. In this jaundice, the level of bilirubin is raised due to excessive breakdown of red blood cells.
Etiology:
- Sickle cell anemia,
- Transfusion reaction,
- Malaria,
- Thalassemia,
- Autoimmune disorders.
2. Obstructive jaundice:
- Obstructive jaundice is called extrahepatic type of jaundice. Obstructive jaundice occurs when the bile ducts are blocked and bilirubin is not excreted from the liver and remains in the liver. Therefore, it is called cholestatic jaundice because due to obstruction of the bile duct, bilirubin cannot be excreted from the liver.
- Obstructive jaundice causes extreme levels of itching in the body because of the buildup of salts in the body.
Etiology:
- Goal Due to carcinoma in the bladder and bile duct,
- Due to the presence of gallstones in the biliary system,
- Due to infection and inflammation.
3. Hepatocellular jaundice:
- Hepatocellular jaundice is the most common type of jaundice.
Hepatocellular jaundice occurs when the liver cells are damaged for any reason, due to which the liver is unable to excrete bilirubin from the body and due to this, bilirubin increases in the blood. - Hepatocellular jaundice is mainly caused by
liver failure,
liver disease,
liver cancer,
hepatitis,
viruses such as,
yellow fever,
Epstein Barr virus,
certain types of drugs.
4.Hereditary jaundice
- Hereditary jaundice is mainly seen in a person through inheritance from his family. Hereditary jaundice is mainly due to impairment in bilirubin metabolism from birth itself, which causes excessive amounts of bilirubin to accumulate in the body. It is mainly seen when there is excessive production of bilirubin or its inability to be excreted from the body.
1) Dubin/Johnson Syndrome:
This is an inherited disorder. In this jaundice, the level of conjugated bilirubin increases in the liver.
2) Gilbert’s Syndrome
Gilbert’s syndrome is an inherited condition that mainly It is seen due to a benign condition in which the level of bilirubin increases to a mild level.
3) Rotor’s syndrome:
This is an inherited disease in which intermittent jaundice is seen.
Etiology:
- In the body Due to the accumulation of excessive amounts of bilirubin.
- Due to any liver cell abnormality.
- Due to blockage of the bile duct.
- Due to inflammation of the liver and bile duct.
1) Prehepatic Cause:
- Due to the destruction of red blood cells,
- Conditions in which red blood cells break down such as:
- Malaria,
- Sickle cell anemia,
- Thalassemia,
- Glucose 6 Phosphate,
- Due to drugs and other toxins,
- Due to autoimmune disorders.
2)Hepatic causes:
- Hepatic jaundice is mainly seen when there is an inability of the liver due to which the condition of jaundice is seen.
- Due to hepatitis,
- Cirrhosis of the liver,
- Due to certain types of drugs,
- Gilbert’s syndrome,
- Cancer
3)Post-hepatic causes:
- This is mainly seen due to any obstruction.
- Due to gallstones.
- Due to cancer.
- Due to stricture of the bile duct.
- Cholangitis
Sign And Symptoms:
- Yellowish discoloration of the skin, mucous membranes and sclera is seen in the body.
- Stool appears light in color.
- Yellow discoloration of urine.
- Itching of the skin.
- Fatigue.
- Abdominal pain.
- Nausea
- Vomiting
- Fever.
- Weakness.
- Loss of appetite
- Headache.
- Confusion.
- Swelling in the legs and abdomen.
- Loss of appetite.
- History taking,
- Physical examination,
- Blood Tests
- Complete Blood Count Test
- Liver Function Test
- Urine Analysis
- Liver Biopsy
- Imaging Study
- CT Scan.
- MRI.
- Abdominal ultrasonography.
- Hepatitis A,B,c test.
Diagnostic Evaluation:
Management:
- Provide intravenous fluids to the patient to prevent dehydration.
- If the patient is experiencing nausea and vomiting, provide antiemetic medicine.
- If the patient is experiencing pain, provide analgesic medicine.
- If the patient has any bacterial infection, provide antibiotic medicine.
- Provide antiviral medicine to the patient.
- Provide blood transfusion when the patient needs it.
- Provide chemotherapy and radiation therapy to the patient.
- Provide steroids and immunoglobulin to the patient.
- Provide a high carbohydrate and low protein diet to the patient.
- Provide nutritional supplementation to the patient.
- Provide vitamin K injection to prevent bleeding.
- Avoid any drugs, toxic chemicals, and alcohol as they can cause jaundice.
Surgical Management:
- If there is a cancer condition, then surgical treatment is required.
- If the condition of jaundice is due to obstruction of the bile duct, then it should be opened surgically.
- Many times, liver transplantation is also required.
- If the patient has gallstones, then surgery is performed to remove them.
- If If the patient has hemolytic jaundice, provide medication and treatment.
Nursing Management
Advise the patient to drink plenty of fluids.
Tell the patient to take adequate rest.
Tell the patient to avoid coffee, alcohol, junk food, soda, Avoid things like.
Tell the patient to eat fruits and vegetables.
Avoid foods that contain preservatives.
Tell the patient to avoid meat and animal fats.
The patient should not take dairy products like cheese, milk etc.
The patient should avoid fats like ghee, butter, cream, oil for 2 weeks.
According to the patient’s condition, soybeans, eggs,. Dale, milk should be provided in small quantities.
Ask the patient to take carbohydrate-rich food such as roti, bread, boiled potato etc. in small quantities.
Take medicine as prescribed by the health care personnel.
Hepatitis (Hepatitis):
- Hepatitis is a condition in which there is infection and inflammation of the liver. Viral hepatitis is mainly caused by
Hepatitis A virus,
Hepatitis B virus,
Hepatitis C virus,
Hepatitis D virus,
Hepatitis E virus. - Epstein Barr virus,
Yellow fever virus
Rubella virus
Herpes simplex
Varicella virus
Adeno virus
Hepatitis is also seen due to all these viruses.
The hepatitis virus enters the liver and multiplies there, then damages the liver and causes inflammation and necrosis of hepatocytes. When the hepatitis virus enters the body, its signs and symptoms are seen in three phases.
1. Preicterus phase or prodomal phase
2. Icterus phase
3. Convulsant phase
1. Preicterus phase or prodomal phase:
- This phase lasts for one to two weeks. In this phase, the patient experiences flu-like symptoms.
- Such as,
- Fatigue,
- Loss of appetite,
- Body aches,
- Nausea,
- Vomiting,
- Diarrhea, and
- Constipation.
2. Icterus face:
- The icterus phase is the onset of signs and symptoms five to ten days after exposure to the hepatitis virus. This phase lasts for two to six weeks. In this phase, the level of bilirubin increases in the body, due to which the skin and mucous membranes of the body appear yellowish in color.
- The condition of jaundice is seen in this phase.
- In this phase, the patient’s skin becomes itchy due to bile salt deposits.
- In this phase, the stool appears light brown and clay-colored due to bile not being excreted through the normal fecal pathway.
3. Convulsant Phase:
- The convolvular phase occurs after the icterus phase. This phase can last for a few weeks or even months. During this phase, her signs and symptoms gradually improve.
Hepatitis A ( A ) During Pregnancy:
- Hepatitis A (A) is a viral infection in which the liver is infected or inflamed, mainly by the RNA virus. Hepatitis A is transmitted mainly through the fecal-oral route. It is mainly transmitted through food or liquids contaminated with the hepatitis A virus. Hepatitis A virus is mainly transmitted by a person who is infected with the hepatitis A virus and does not wash his hands properly after a bowel movement and when that person prepares food.
- The incubation period of hepatitis A is between 15 and 50 days. And the average is 30 days.
- The hepatitis A ( A ) virus can be seen for four to eight weeks ( 4 to 8 weeks).
Etiology:
- 1. Contaminated food or water:
Transmitted through food and food materials prepared by an infected person. - 2. Person to person contact:
Due to direct contact with an infected person or contact with their items.
3) Due to poor sanitation.
4) Due to poor hygiene.
5) Due to overcrowding.
6) Due to not washing hands properly after bowel movement.
7) Drinking contaminated water.
8) Eating undercooked seafood Due to.
9) Due to blood transfusion.
Due to sexual contact with a person who has hepatitis A virus infection, due to reusing contaminated needles.
Sign And Symptoms (Signs And Symptoms):
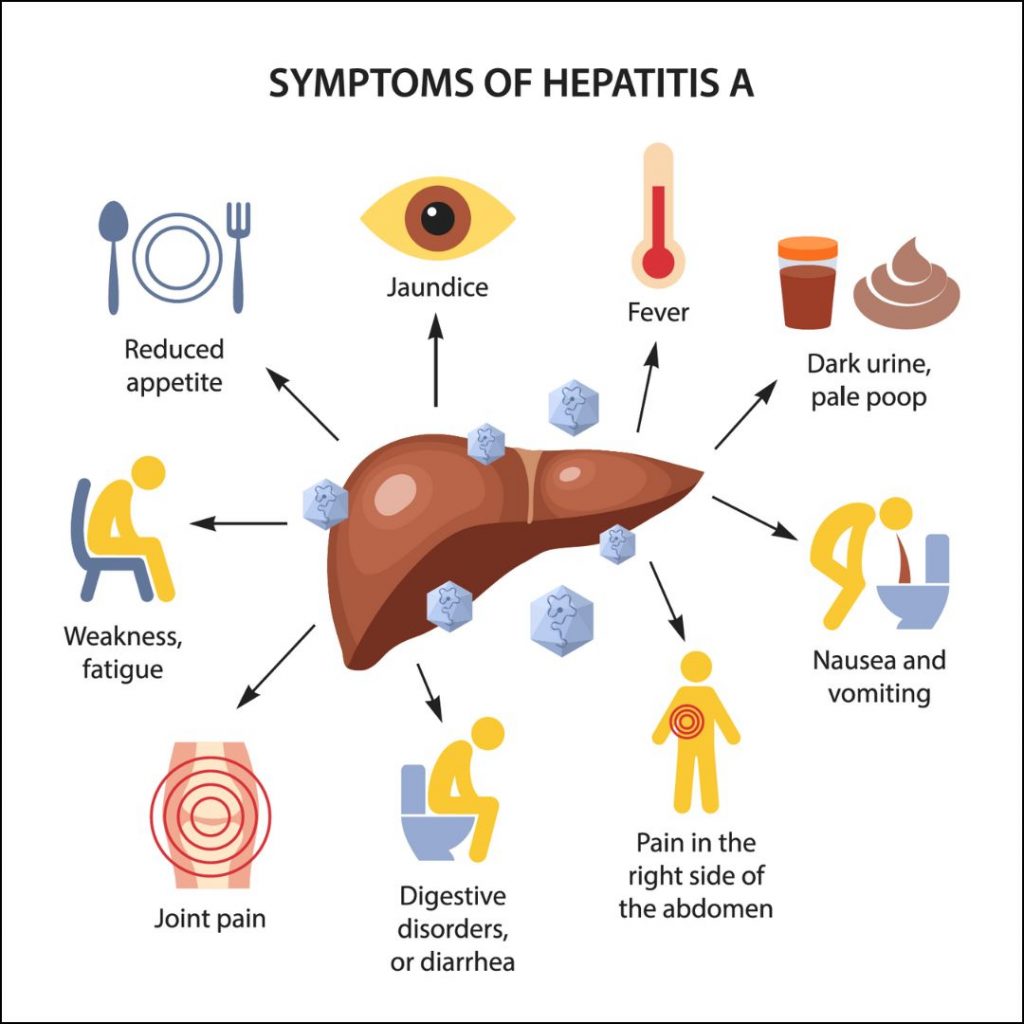
- In this, the patient experiences flu-like symptoms.
- Upper respiratory tract infection
- Low grade fever Come.
- Not feeling hungry.
- Indigestion.
- Nausea,
- Vomiting
- Diarrhea
- Clay colored stool
- Heart failure
- Jaundice
- Weakness.
- Headache.
- Fatigue.
- Generalized weakness
- Stomach cramps
Diagnostic Evaluation (Diagnostic Evaluation) :
- History Collection,
- Physical Examination,
- Blood Test,
- Assess the Immunoglobulin level,
- Assess the liver function test
- Ultrasound
- CT scan.
- MRI.
Management:
- Tell the patient not to drink alcohol.
- Tell the patient to avoid eating fatty foods.
- Tell the patient to maintain personal hygiene.
- Tell the patient to wash their hands properly.
- Tell the patient to avoid unprotected sex.
- Instruct the patient to take a nutritional diet.
- Provide intravenous glucose to the patient.
- Advise the patient to maintain body weight.
- Instruct the patient to take adequate bed rest.
- Instruct the patient to avoid physical activity.
- Instruct the patient to do small amounts of activity.
- Provide antiemetic medicine if the patient is experiencing nausea and vomiting.
Nursing Management:
- Monitor the patient’s vital signs frequently.
- Monitor the patient’s daily weight.
- Frequently assess the patient’s stool.
- Frequently provide oral fluids to the patient.
- Provide intravenous fluids to the patient.
- Monitor the patient’s intake-output chart.
- Monitor the patient’s nutritional status.
- Instruct the patient to eat in a sitting position.
- Provide the patient with small, free-of-charge dietary supplements.
- Maintain the patient’s oral hygiene.
- Provide mouth care to the patient.
- Ask the patient to eat small and frequent amounts of food.
- Provide the patient with a quiet environment to work and eat while eating.
- Ask the patient to take adequate rest.
- Monitor the patient’s daily intake output chart.
- Provide the patient with proper oxygen.
Hepatitis B during pregnancy:
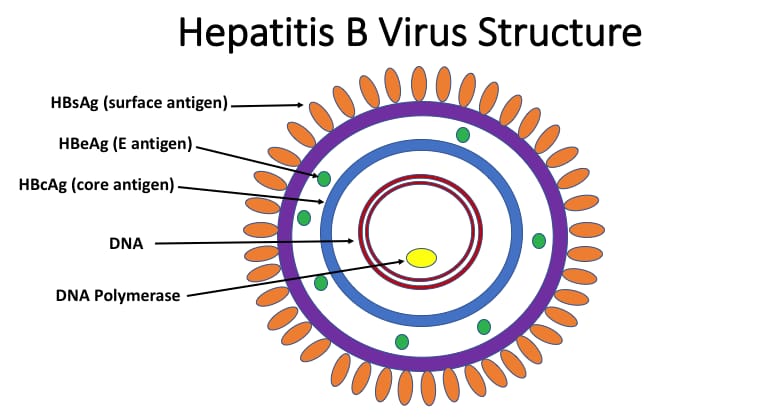
- Hepatitis B is also called serum hepatitis. Hepatitis B is mainly transmitted by the hepatitis B virus. The hepatitis B virus is mainly found in the blood, saliva, semen, and vaginal secretions of an infected person. Hepatitis B virus creates infection and inflammation in the liver which is called severe form of life threatening infection. Hepatitis B virus is a life long infection due to which
- Liver cirrhosis
- Liver failure
- Liver cancer
- And death can also occur.
- Hepatitis B acute ( acute :Rapidly developing) and chronic (chronic:long lasting) forms are seen. The incubation period of hepatitis B is from one to six months. Hepatitis B is mainly transmitted by the hepatitis B virus which is mainly present in blood, semen, and other body fluids.
Etiology:
- Caused by the hepatitis B virus.
- Transmitted through blood, saliva, semen, vaginal secretions, etc. of an infected person.
- Unprotected sexual contact
- Through.
- Through contact with infected needles and syringes.
- Mother to child transmission.
- Intravenous drug Users.
- Health care workers.
- People who receive frequent blood transfusions.
- From sexual contact with an infected person.
- From sexual contact with multiple partners.
- From intravenous drug abuse.
- Due to repeated exposure to blood.
- Due to sharing toothbrushes and razors.
- Patients undergoing dialysis.
- Due to repeated medical procedures.
Sign And Symptoms :
- Hepatitis B virus is seen after contact with the virus
- 12 weeks.
- Jaundice
- Fever.
- Loss of appetite.
- Respiratory symptoms appear.
- Abdominal discomfort.
- Recess.
- Abdominal pain.
- Nausea.
- Vomiting.
- Generalized pain.
- Weakness Come.
- Dark yellow urine.
- The liver is tender and enlarged.
- Clay colored stools
- Lethargy.
- In some cases, the spleen is enlarged and palpable.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History Collection,
- Physical Examination,
- Assess the Albumin Level,
- Assess the Liver Function Test,
- Assess the prothrombin time,
- Assess the presence of antibody HBsAG( anti -HBs).
- antibody to hepatitis B core antigen( Anti – HBc).
- hepatitis B surface antigen( HBsAG).
- hepatitis E surface
- Antigen ( HBeAG).
Management:
medical management
- If the patient has acute hepatitis, then his lifestyle should be modified.
- Ask the patient to take proper bed rest.
- Ask the patient to take adequate fluids.
- Advise the patient to take a nutritional diet.
- If the patient has a condition of chronic hepatitis, then ask him to avoid alcohol.
- Ask the patient to avoid over-the-counter medicines.
- Provide interferon alpha medication to the patient who has a condition of chronic hepatitis B.
- Interferon-alpha increases the activity of the body’s immune system and impairs the reproduction of the hepatitis-B virus.
- Interferon-alpha tablets are taken daily or three times a week for six months.
- Provide the patient with lamivudine and adenovir medication.
- Ask the patient to take adequate bed rest.
- Maintain the patient’s nutritional status properly.
- Provide the patient with adequate fluids.
- If the patient has a severe condition, consider liver transplantation.
Nursing Management:
-
- Maintain the patient’s skin integrity.
-
- Provide good skin care to the patient.
-
- To avoid irritating the patient’s skin Tell.
-
- Ask the patient to apply an emollient.
-
- Ask the patient to keep fingernails short.
-
- Assess the patient for any bleeding.
-
- If the patient is itching, provide medication to reduce it.
-
- Position the patient to prevent pressure ulcers Keep changing it frequently.
-
- Assess the patient for any neurological signs and symptoms.
-
- Provide the patient with a quiet and comfortable environment to work in.
-
- If the patient is experiencing any bleeding, ask him to report it immediately.
-
- Monitor the patient’s prothrombin time and bleeding time and administer vitamin K.
-
- Do not perform any procedure that may cause any trauma to the patient.
-
- Take proper care to avoid any needle stick injury to the patient.
Prevention:
- To prevent hepatitis B, take the hepatitis B vaccine properly.
- Properly screen the donated blood.
- Use disposable series – no needles.
- Instruct the patient to maintain good personal hygiene.
- Daily disinfection of the working area Do.
- Wear gloves when working with any body fluids.
- Advise health care personnel and high-risk individuals to get the hepatitis B vaccine.
- A total of three doses of hepatitis B are taken.
- A second dose (2nd dose) is taken one month after the first dose, and then a third dose of hepatitis B is taken six months after the first dose.
- If you have come into contact with hepatitis B virus due to any needle stick injury, get vaccinated immediately.
- Avoid sexual contact with a person who has acute or chronic hepatitis.
- Use a barrier method as a contraceptive during sexual activity.
- Avoid sharing personal items such as toothbrushes and razors.
- Do not use any needles or syringes that have not been disinfected and use disposable series and needles.
- Avoid contact with the body fluids of an infected person.
Hepatitis C During Pregnancy:
- Hepatitis C is an infection and inflammation of the liver and is mainly caused by the hepatitis C virus
- . Hepatitis C is a viral infection caused by the hepatitis C virus, an RNA virus that belongs to the Flaviviridae family of viruses. Hepatitis C was first identified in 1989. Hepatitis C is spread primarily through direct contact with the blood of an infected person. Hepatitis C ( C ) is different from hepatitis A ( A ) and B ( B ).
- The incubation period of hepatitis C
- is 15 -160 days.
Etiology:
- Because of the hepatitis C virus,
- Because of dialysis for a long time,
- Because of working with blood regularly.
- Because of unprotected sexual activity with a person who has hepatitis C infection.
- Because of coming into contact with any body fluid of a person who has hepatitis C infection Due to.
- Any needle stick injury.
- Blood transfusion.
- Tattooing with any infected instrument.
- Any accidental needle stick injury.
- Any organ transfusion.
- Sharing personal items such as toothbrushes and razors.
- Birthing of a child by a mother who has hepatitis C infection.
- In people who are sexually active.
- In people who have multiple partners.
Sign And Symptoms (signs and symptoms):
- Liver failure,
- Cirrhosis of the liver,
- Abdominal pain (right upper abdomen),
- Abdominal swelling.
- Jaundice,
- Dark urine and
- Pale and clay colored stools Passing stool.
- Gas build-up in the esophagus and stomach.
- Dark urine.
- Fatigue.
- Itching.
- Muscle and joint pain.
- Fever.
- Loss of appetite.
- Nausea.
- Vomiting.
- Liver cancer.
Diagnostic Evaluation:
- History taking,
- Physical examination,
- Liver function test,
- Assay EIA (enzyme immunoassay) to detect hepatitis C antibody.
- Hepatitis C genotypes.
- Assay the Albumin level.
- Assess the liver function test
- Assess the prothrombin time
- Liver biopsy.
Management:
- Advise the patient to take adequate rest.
- Keep the patient properly isolated.
- Use disposable syringes properly while handling the patient.
- Properly dispose of the patient’s excreta.
- Provide the patient with proper work and a comfortable environment. To do.
- Advise the patient to properly ingest safe drinking water.
- Properly check the patient’s vital signs.
- Provide the patient with antiviral medicine to treat hepatitis C virus
- Ex: pegylated interferon alpha and ribavirin
- Ask the patient to maintain good hand washing technique.
- Instruct the patient to follow strict aseptic technique.
- Follow strict aseptic technique when visiting a person who has an infection.
- Provide education to the patient not to scratch the area that is itching.
- If the patient has abdominal discomfort, extreme fatigue, skin rashes, and fever and vomiting, notify the doctor immediately.
- Provide education to the patient to Hepatitis B can also be transmitted through tattooing and skin piercing.
- Provide education to the patient that they should not donate blood after being infected with hepatitis C.
- Instruct the patient to take rest between activities.
- Instruct the patient to come for regular checkups.
- Advise the person to avoid sexual activity with someone who is infected with hepatitis C. Give.
- Instruct the patient to use a barrier method of contraception during sexual activity.
Hepatitis D During Pregnancy:

- Hepatitis D is also called the delta virus. Hepatitis D is an infection and inflammation of the liver that occurs mainly due to the hepatitis D virus. Hepatitis D is a viral infection that is caused by the hepatitis D virus. Hepatitis D is also called a satellite infection because hepatitis D is mainly found in people who have hepatitis B. Hepatitis D increases the severity of hepatitis B and causes more liver damage. It is mainly transmitted through contact with infected blood.
Etiology:
- Individuals who have hepatitis B In individuals.
- By sharing needles, syringes, and personal utensils such as toothbrushes and razors with an infected person.
- By engaging in sexual activity with an infected person.
- By engaging in unprotected sexual activity.
- By intravenous drug users.
- By exposure to the blood of an infected person. Due to direct contact.
- Due to the birth of a baby by an infected mother.
- Due to a past infection with Hepatitis B.
- Due to receiving a blood transfusion.
Sign And Symptoms :

- 1) Flu like Symptoms:
- Fatigue,
- Weakness,
- Muscle pain,
- Fever,
- 2) Jaundice:
- Yellowing of the skin, mucus due to the accumulation of bilirubin in the body Yellowish discoloration of the membranes and sclera is seen.
- 3) Abdominal pain:
- Pain and discomfort in the upper right quadrant of the abdomen occurs due to inflammation of the liver.
- 4) Dark urine:
- Due to the buildup of bilirubin in the body, the urine appears dark in color.
- 5) Pale or clay colored stool
- The stool appears pale and clay colored due to the lack of bilirubin being excreted from the body.
- 6) Nausea and vomiting:
- Many times, patients with hepatitis D experience nausea and vomiting.
- 7) Loss of appetite:
- A person does not feel hungry due to Hepatitis D.
- 8) Joint pain
- A person experiences joint pain due to the disease.
- 9) Confusion.
- 10) Itching.
- 11) Fever.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History Collection,
- Physical Examination,
- Liver Biopsy
- Blood Test
- Liver Function Test
- Liver Enzymes
- Abdominal Ultrasound
- Anti Delta Agent Antibody Test
Management:
Medical Management:
- Provide antiviral medication to the patient.
Ex:=tenoflovir,
Entecavir. - Provide interferon-alpha medication to the patient.
- Monitor the patient’s liver function test regularly.
- Advise the patient to take an adequate nutritional diet.
- Antiemetic if the patient has a condition of nausea and vomiting Provide medicine.
- If the patient’s condition is very severe, then liver transplantation should be done.
- Provide the patient with vaccines.
- Ask the patient to avoid drugs that alter liver function or damage liver cells.
- Ask the patient to eat high carbohydrate foods such as bread, jam, wheat, biscuits, rice, vegetables ,Potatoes, etc.
- Ask the patient not to share his personal equipment like toothbrush, razor etc.
- Advise to avoid sexual contact with an infected person.
Nursing Management:
Assessment:
Asking about the patient’s medical history and signs and symptoms of the disease.
Monitoring the patient’s vital signs.
Assessing the patient for jaundice, abdominal pain, and any other signs and symptoms.
Symptoms Management:
If the patient is experiencing nausea and vomiting, provide antiemetic medicine.
If the patient is experiencing pain, provide analgesic medicine.
Maintain the patient’s comfort level.
Advise the client to maintain their nutritional status
Advise the patient to follow a well-balanced diet Say that it contains adequate amounts of calories and vitamins so that the liver can function properly.
Monitor the patient for any signs and symptoms of malnutrition.
4) Maintain fluid balance properly:
Maintain the patient’s intake output chart.
Instruct the patient to take adequate amounts of fluids.
Maintain the patient’s hydration status.
If the patient has a condition of severe dehydration, provide intravenous fluids and maintain the patient’s hydration status.
5) Infection Control:
Provide education to the patient to maintain proper hygienic conditions.
Provide education to the patient to wash hands properly.
Ask the patient to maintain aseptic technique.
6) Rest and Activity:
Ask the patient to take adequate rest.
Ask the patient to do small amounts of physical activity.
Ask the patient to do small amounts of daily routine activity.
7) Psychological support:
Provide proper psychological support to the patient.
Clear all the doubts of the patient.
Give the patient complete information about the disease and its treatment.
8) Medication Administration:
Provide proper antiviral medicine to the patient.
Provide education to the patient for lifestyle modification.
Monitor the patient’s vital signs.
Test the patient’s liver function.
All the patient’s To perform laboratory investigations.
Provide education to the patient to get hepatitis B vaccination.
Ask the patient to have regular follow-up.
Hepatitis E (E) During Pregnancy
- Hepatitis E A viral Hepatitis E is an infection that is transmitted by the hepatitis E virus. Hepatitis E is an infection and inflammation of the liver and is mainly transmitted by the hepatitis E virus. Hepatitis E was mainly discovered in 1990. Hepatitis E is mainly transmitted through the feco-oral route, i.e. through contaminated/infected food and water.
- The incubation period of hepatitis E
- It ranges from two to nine weeks. Hepatitis E is self-limited but it affects pregnant women more severely. It can also cause abortion and intrauterine death in pregnant women.
Etiology:
- By hepatitis E virus.
- genotypes:=1,2,3,4
- Genotype := 1,2 are associated with the human infection.
- Due to contaminated food and water intake.
- Due to poor sanitation.
- Due to poor hygienic conditions.
- Due to low socio-economic conditions.
- During the third trimester of pregnancy.
- In international travelers.
- A person who lives in an area where there is an outbreak of hepatitis E.
- A person who has had sexual activity with an infected person.
- Due to unprotected sexual activity.
Sign And Symptoms (Signs And Symptoms):
- Weakness,
- Fatigue,
- Fever,
- Muscle pain,
- Nausea,
- Vomiting,
- Loss of appetite (anorexia),
- Abdominal pain,
- Pain in the right upper quadrant of the abdomen.
- Jaundice: Jaundice causes skin, mucus Yellowish discoloration of the membranes and sclera.
- Dark colored urine due to bilirubin.
- Pain and clay colored stool.
- Enlargement of the liver (hepatomegaly).
- Itching due to accumulation of bilirubin in the skin,
- Weakness,
- Malaise,
- Joint pain
- Muscle pain,
- Weight loss.
Diagnostic Evaluation :
- History taking,
- Physical examination
- Blood test
- Anti -HEV igM
- Antibody test.
- Liver function Tests
- Serological tests
- Stool examination
- Imaging studies
- assess the hepatitis A,
- hepatitis B,
- hepatitis c test.
Management:
- There is no specific treatment for Hepatitis E but it subsides on its own.
- The patient should be encouraged to take a nutritious diet.
- The patient should be given antiemetic medicine to treat the condition of nausea and vomiting.
- The patient should be provided with high carbohydrate foods such as bread, jam, wheat, biscuits, rice, vegetables, and potatoes. Provide.
- Ask the patient to maintain good hygienic conditions.
- Avoid eating uncooked food.
- Avoid drinking contaminated water.
- A complete health history and physical examination of the patient.
- Does the patient have any signs and symptoms of hepatitis? Ask about it.
- Ask the patient to take short breaks between activities.
- Assess the patient’s working ability.
- Provide the patient with a quiet environment to work in.
- Provide the patient with a high-calorie diet.
- Monitor the patient’s intake output chart.
- Serve food to the patient in an attractive manner.
- Provide a relaxing environment to the patient.
- Ask the patient to maintain oral hygiene.
- Ask the patient to avoid carbonated drinks.
- Ask the patient to adopt proper hand washing technique.
- Instruct the patient to maintain personal hygiene.
- Instruct the patient to avoid unprotected sexual activity.
- Avoid sexual activity with someone who is infected.
- Use a barrier method of contraception during sexual activities.
- Provide education to the patient on proper skin care Do.
- Ask the patient to bathe with warm water. Avoid using hot water as it increases skin dryness.
- Ask the patient to avoid using soaps containing alcohol.
- Ask the patient to apply emollient properly.
- Ask the patient to keep their fingernails short.
Urinary Track Infection
- Urinary tract infection is an infection and inflammation mainly in the part of the urinary system. The urinary system mainly includes the kidneys, ureters, bladder, and urethra. If infection and inflammation occurs in this system, it is called urinary tract infection. Infection in the urinary tract mainly arises due to pathogenic microorganisms. If urinary tract infection mainly affects the upper urinary tract, it is called pyelonephritis. If the urinary tract infection mainly affects the lower urinary tract, it is called simple cystitis.
Types of urinary tract infection:
There are two main types of urinary tract infection.
1)Upper urinary tract infection
2)Lower urinary tract infection
1)Upper urinary tract infection,
Upper urinary tract infection is mainly called pyelonephritis. Upper urinary tract infection mainly involves the kidneys and ureters. It causes fever, chills, nausea, vomiting and other symptoms.
2)Lower urinary tract infection.
Lower urinary tract infection is called simple cystitis.
Lower urinary tract infection mainly involves the bladder and urethra.
Etiology:
- Escherichia coli,
- Klebsiella,
- Enterococcus,
- Enterobacter,
- Pseudomonas,
- Proteus,
- Staphylococcus,
- Mycoplasma,
- Chlamydia,
Risk Factores (Risk Factores):
1)Female :
Short urethra,
due to structural abnormality line.
due to urethral stricture.
due to urethral vesical function abnormality.
due to obstruction
due to tumor presence.
due to calculi presence.
due to prostatic hypertrophy.
impaired bladder innervation:
due to multiple sclerosis.
due to urinary stasis. Due to neurogenic bladder.
Due to chronic diseases:
Immunosuppression,
Glomerulo
Nephritis,
Hypertension.
Due to sickle cell anemia.
Age:
Due to anemia.
Due to malnutrition.
Sign And Symptoms (Sign And Symptoms):
- Dysuria,
- Increased frequency of urination.
- Urgency to urinate.
- Hematuria (blood in urine).
- Cloudy and foul-smelling urination.
- Pelvic Pain.
- Flank pain.
- Fever
- Chills
- Nausea
- Vomiting
- Urinary incontinence.
- lower back pain
- Headache
- Pain during urination.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History collection,
- Physical Examination.
- Complete Blood Count.
- Urine Analysis.
- Urinary Microscopy.
- Urine Culture.
- Ultrasound.
- X ray.
- MRI.
- Cytoscopy.
Medical Management:
- Monitor the patient’s intake output chart.
- Assess the patient for any adverse reactions.
- Advise the patient to increase fluid intake.
- Provide antibiotic medicine to the patient.
Ex:=
ciprofloxacin ,
Norfloxacine,
Nitrofurantoin/trimethoprime. - If the patient is in pain, provide analgesic medicine.
Ex:=
Acetaminophen,
Ibuprofen - Advise the patient to avoid irritating foods such as alcohol, tea, coffee, spicy food, hot food.
- Advise the patient to maintain personal hygiene.
- Provide psychological support to the patient.
- Advise the patient to take proper medication.
- Nursing management of the patient:
- Properly assess the patient.
- Advise the patient to take proper fluid intake.
- Provide analgesic medicine if the patient is in pain.
- Keep the patient calm Provide diversional therapy.
- Assess the extent to which the patient’s medication is effective.
- Provide the patient with properly prescribed antibiotic medicine.
- Advise the patient to maintain proper personal hygiene.
- Advise the patient to get adequate rest.
- Assess the patient for any other complications.
- Advise the patient to follow up regularly.
- Properly document the patient’s information.
- Provide proper psychological support to the patient.
- Provide the patient with a comfortable and workable environment.
- Advise the patient to take a properly nutritious diet.
- Advise the patient to take regular follow-up.
- Provide psychological support to the patient.
- Clear all the doubts of the patient.
- Provide the patient with a comfortable and workable environment.
Upper urinary tract infection
- Upper urinary tract infection is called pyelonephritis. The upper urinary tract includes the kidneys and ureters. Pyelonephritis involves the kidneys, ureters, calyces, and renal pelvis. Pyelonephritis is mainly caused by bacterial infection. In pyelonephritis, bacteria travel primarily from the lower urinary tract (bladder and urethra) to the upper urinary tract (kidneys and ureters), creating infection and inflammation in the upper urinary tract.
Types of pyelonephritis:
There are two types of pyelonephritis.
1)Acute pyelonephritis
2)Chronic Pyelonephritis
1)Acute Pyelonephritis,
Acute pyelonephritis develops rapidly. And the symptoms have a sudden onset. Acute urinary tract infection is mainly seen from
24 to 48 hours to a week.
Etiology:
Causes of acute pyelonephritis:
Due to bacterial infection.
Escherichia coli.
Vesicourethral reflux
Due to urinary obstruction.
Due to impaired immune system.
Due to indwelling catheter.
Klebsiella.
Due to Enterobacter species.
2)Chronic pyelonephritis:
Chronic pyelonephritis develops gradually and is mainly caused by an extended Period
is seen up to.
Chronic pyelonephritis mainly results in chronic pyelonephritis due to repeated episodes of acute pyelonephritis infection.
Chronic pyelonephritis
Inflammation of the kidneys and fibrosis of the tubules and interstitial tissues occur in end-stage renal disease. Chronic pyelonephritis mainly occurs from 6 months to 1 year.
Chronic pyelonephritis is seen due to recurrent or persistent renal infection, vesico-urethral reflux, and urinary tract obstruction.
Causes of Chronic Pyelonephritis.
Due to bacterial infection.
Due to neurogenic bladder.
Due to hypertension.
Due to obstruction of urine flow.
Due to repeated infection.
Due to structural damage.
Kidney stones.
Due to urinary tract abnormality.
Sign And Symptoms::
- Fever.
- Feeling cold.
- Flank or back pain.
- Urinary frequency increases.
- Nausea and vomiting.
- Painful Urination.
- Urinary frequency increases.
- Costovertebral angle deformity.
- Hematuria.
- Fatigue.
- Flank tenderness.
- Malaysia.
- Back pain.
- Dysuria.
- Confusion.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History collection,
- Physical Examination,
- Urinalysis .
- Urine Culture.
- Sensitivity Test.
- Complete Blood Count Test.
- Blood Culture.
- Intravenous pyelography (IVP).
- Kidney ultrasound.
- CT Scan.
- Voiding cytourethrography
- Cytography
- Renal biopsy.
- MRI .
Medical Management.
- Provide antibiotic medicine to the patient.
- Ex:=
Tobramycine,
Gentamycine,
Vancomycine,
Ciprofloxacine ,
Norfloxacine, Trimethprim,
Sulfamethoxazole - Provide antipyretic medicine to the patient.
Ex:=Paracetamol. - Provide urinary antiinfective medicine to the patient To do.
Ex:=
Nitrofurantin,
Trimethoprime. - Provide Urinary Antiinfective Medicine to the patient.
Ex:=
Tab Phenazopyridine. - Surgical Management of Patients with Pyelonephritis:
- 1)Ureteroplasty:
- In this procedure, the stricture in the ureters is surgically removed or repaired.
- 2) Urethral reimplantation
- Urethral reimplantation is performed to completely cure vesicourethral reflux.
- 3) Urethral stent
- Urethral stents primarily increase urine flow.
- 4) Percutaneous ultrasonic Pyelolithotomy
- Percutaneous ultrasonic pyelolithotomy is mainly used to remove crush and stones.
Nursing Management:
- Properly assess the patient.
- Patient To properly assess the white sign of the patient.
- Advise the patient to take adequate fluid intake.
- Provide intravenous fluids to the patient.
- Provide proper medication to the patient.
- Provide analgesic medications to relieve the patient’s pain.
- Provide proper Advise on medication.
- Maintain proper intake output chart of patient.
- Advise patient to maintain aseptic technique.
- Advise patient to take proper follow-up.
- Advise patient to take adequate rest.
Lower Urinary tract Infection:
- Lower urinary tract infection is an infection and inflammation of the lower part of the urinary system, the bladder and urethra. Lower urinary tract infection occurs due to many reasons.
Like: - 1) Urethral vesico reflux.
2) Due to bacterial infection in the urinary tract. - Lower Urinary Tract Etiology:
- Due to bacterial infection.
Ex:
E.coli.
Klebsilla.
Enterococcus.
Staphylococcus saprophytucus. - Due to urinary tract abnormality.
Due to weakened immune system.
Urinary catheter.
Due to certain drugs.
Due to radiation.
Due to unhygienic conditions.
Due to congenital deformity in urinary system.
Unprotected sexual intercourse.
Any other infection Because of.
Sign And Symptoms (लक्षणो तथा चिन्हो (स्न्हो और सिंपटोम्स):
- Burning sensation during urination.
- Increase in urinary frequency.
- Urgency during urination.
- Passing small and frequent amounts of urine.
- Nocturia.
- Urinary incontinence.
- Foul-smelling urine.
- Hematuria.
- Discomfort in the pelvic area.
- Back pain.
- Pelvic pain.
- Low grade fever.
- Nausea.
- Vomiting.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History Collection,
- Physical Examination
- Urine Analysis.
- Cytoscopy.
- Ultrasound .
- X-ray.
- Intravenous urography
Medical Management :
- Provide antibiotic medication to the patient.
- If the patient is in pain, administer analgesic medicine.
- Advise the patient to exercise properly.
- Advise the patient to maintain personal hygiene.
- Advise the patient to drink plenty of water.
- Take a complete history of the patient.
- Take a proper history of what kind of signs and symptoms the patient has.
- Advise the patient to take proper medication.
- Provide antispasmodic medication to relieve the patient’s pain. To do.
- If the patient has a condition of inflammation, then provide aspirin medicine.
- Advise the patient to apply heat.
- Advise the patient to take plenty of fluid.
- Advise the patient to avoid irritating substances such as tea, coffee, cold drinks and spicy food.
- Advise the patient to maintain proper personal hygiene.
- Properly measure the patient’s vital signs.
- Advise the patient to have plenty of fluid intake.
- Provide psychological support to the patient.
- Provide the patient with complete information about his disease condition, its causes, its symptoms and signs.
Nursing Management:
Diabetes Mellitus :
- Diabetes is a chronic metabolic disorder in which carbohydrate, protein and lipid metabolism are impaired. Diabetes is a group of metabolic disorders in which a person’s blood has high blood sugar levels. This is mainly due to an impairment in insulin secretion and insulin action in the body, which leads to high blood sugar levels in the body.
- The ”3 P” syndrome is mainly seen in diabetes mellitus. Found.
- 1)P: Polyuria (frequent urination),
- 2)P: Polydipsia (increased thirst),
- 3)P: Polyphagia (increased hunger).
Types of diabetes mellitus (Diabetes type of malites) :
There are four main types of diabetes.
Type:1( IDDM) Insulin Dependent Diabetes Mellitus.
Type: 2 ( NIDDM ) Non Insulin Dependent Diabetes Mellitus.
Type: 3 Diabetes Mellitus Associated with Other Disease Conditions.
Type: 4 GDM Gestational Diabetes Mellitus.
Type:1(IDDM) Insulin Dependent Diabetes Mellitus:
- This is a type of diabetes mellitus in which the pancreatic beta cells in the body, which are responsible for producing insulin, are destroyed due to any autoimmune disease, resulting in a total deficiency of insulin. Due to the total deficiency of insulin, insulin is taken by injection. This type of diabetes is mainly seen before the age of 30.
type: 2 ( NIDDM ) Non-insulin dependent diabetes mellitus.
- Type 2 diabetes is mainly caused by insulin resistance or reduced insulin sensitivity, in which the pancreatic cells do not produce adequate amounts of insulin. This type of diabetes can be prevented by taking a proper diet, exercising, and making lifestyle changes and increasing physical activity. This type of diabetes is mainly seen after the age of 30. Therefore, it is Adult onset diabetes mellitus is also called. If diabetes is not treated in this way, then oral hypoglycemic agents are also taken.
Type: 3 Diabetes mellitus associated with other disease conditions.
- In this, diabetes is also seen due to any other disease in the body.
type:4 GDM Gestational Diabetes Mellitus
- This type of diabetes is mainly seen in women and even in those women, diabetes mellitus is seen during pregnancy due to glucose intolerance.
Etiology:
- Type:1( IDDM) Insulin Dependent Diabetes Mellitus:
- Inherited,
Environmental Factors
Due to certain viruses - Type: 2 ( NIDDM ) Non Insulin Dependent Diabetes Mellitus.
- Genetic Factors,
Environmental Factors,
Obesity, - Type: 3 Diabetes Mellitus Associated with Other Disease Conditions.
- During pregnancy due to hormonal imbalance. Due to insulin deficiency.
Despite insulin, due to cell resistance to insulin.
Due to excessive sugar intake.
Due to sedentary lifestyle.
Due to excessive cholesterol in the body.
Sign And Symptoms:
- P: Polyuria (frequent urination: passing urine frequently),
- P: Polydipsia (increased thirst),
- P: Polyphagia (increased hunger).
- Fatigue.
Weakness.
Visual impairment.
Tingling and numbness in hands and feet
Dry skin.
Sores that heal slowly
Frequent infections.
Nausea.
Vomiting.
Decreased wound healing
Weight loss.
Abdominal Pain.
Diagnostic Evaluation (Diagnostic Evaluation) :
History Collection,
Physical Examination,
1) Fasting Blood Sugar (FBS) This test is done without eating or drinking anything for at least eight hours. Its normal value should be less than 110 mg/dl milligrams per deciliter. And if the fasting blood glucose level is more than 125 mg/dl milligrams per deciliter, then it is diagnosed as diabetes.
2)Random blood sugar (RBS) In this, the sample is taken at any time and no preparation is required. If the random blood glucose is more than 200mg/dl milligrams per deciliter, then it is indicated as diabetes.
3)PP2bs (post prandial blood sugar) This test is done 2 hours after taking a full meal. Normally, the blood glucose level returns to the fasting glucose level two hours after a meal, but if any smoking or drinking of caffeine is done, then there is an alteration in it.
3) Glycosylated HB .
This test is done to assess the amount of glucose attached to the blood molecule.
4) Glycosylated Albumin: Normally, glucose is attached to albumin, so glycosylated albumin is used to assess the average glucose level.
5) Oral glucose tolerance test. In this, the patient is provided with 150 mg of carbohydrates for three days. Then the patient’s fasting blood glucose level is checked. Then the client is given 75 grams of glucose to drink, after which the patient’s glucose tolerance level is checked.
7) Ketonuria: If ketones are present in the urine, it indicates that the body is using fat as a source of energy.
8) Proteinuria: If protein is present in the urine, it indicates that protein is used as a major source of energy.
9)Serum lipid profile
10)Serum BUN.
11)Serum creatinine.
Management:
- Principles of Management
- To eliminate the symptoms of hyperglycemia.
- To reduce the microvascular and macrovascular complications of diabetes mellitus.
- To reduce the blood glucose level.
- The patient can achieve a normal life style as far as possible.
- The blood glucose level can be reduced by using patient education, dietary management, exercise and pharmacological therapy.
- Patient Education:
- Provide appropriate health education to the patient and his family members.
- In which, teach how to do self-monitoring of glucose.
- If there is type one diabetes mellitus, teach how to monitor urine ketones.
- Teach the patient how to administer insulin.
- Teach the management of hypoglycemia.
- Provide education to the patient about foot and skin care.
- Teach the management of diabetes before, during, and after exercise.
- Provide education to the patient about lifestyle modification.
- Dietary Management:
- Aim of Dietary Management:
- To reduce the symptoms of hyperglycemia.
- To reduce the symptoms of hypoglycemia if hyperglycemia is treated.
- To reduce the overall blood glucose level of the body.
- Avoid diets that increase blood glucose levels.
- If the patient is obese, ask him to lose weight.
- To ensure that the patient has a regular food intake.
- Telling the patient not to take sugar.
- Asking him to take a diet that contains adequate amounts of protein, carbohydrates and fat.
- Dietary Management:
- The main goal of dietary management is to improve metabolic control in a diabetic client.
- To improve the patient’s blood glucose level and lipid level.
- To make a daily food intake plan for the patient.
- To make a plan for the patient’s weight management.
- To provide adequate nutrition to the patient.
- A person’s lifestyle and habits play an important role in controlling and managing his disease.
- A balanced nutritional diet is very important for the patient.
- Ask the patient to take protein in his diet. Excessive protein intake increases renal function. And glomerular filtration rate increases.
- Maintain the level of fat in the patient’s diet. Maintain the daily cholesterol level in the diet and limit saturated fat and cholesterol.
- Provide carbohydrates according to the patient’s body requirement.
- Ask the patient to take carbohydrates in an adequate amount so that the energy requirement of the body can be maintained.
- For type :1 diabetes special diet management includes Breakfast should be taken 1 hour after taking the morning insulin dose.
- Then a small amount of carbohydrates should be taken after three hours.
- Lunch should be taken four to five hours after taking the morning insulin.
- Sugar should not be taken in the morning.
- Foods that are sweet and contain sugar should not be taken such as cakes, ice cream, jam etc.
- Check the patient’s blood glucose level regularly.
- Carbohydrates should be taken in small amounts before exercise.
- The patient should be asked to check the amount of glucose, ketones and albumin in the urine and all these substances are found during fasting.
- Calorie restriction should be done for the obese client.
- Exercise:
- Provide advice to the patient to do regular exercise to prevent his disease condition from getting worse.
- Ask him to do regular walking.
- Ask the patient to ride a bicycle regularly.
- Ask him to take adequate amount of carbohydrates before and after exercise.
- Pharmacological management:
- Pharmacological management is responsible for maintaining blood glucose levels.
- If insulin is given on the abdomen, its absorption is fast. When given on the arms and legs, its absorption decreases.
Time, Course:
1) Rapid acting insulin:
Ex:=Humalog.
Its onset is within 10 to 15 minutes.
2) Short acting insulin:
It is called regular insulin or R insulin or zinc crystelline zinc insulin ( czi ). Its onset is 30 minutes.
3) Intermediate acting insulin:
It is also called regular R insulin (R insulin) and its onset time is after three to four hours and the patient needs to take food during this period.
Long acting insulin:
Ultra lente insulin or Peakless insulin.
Its onset time is 6-8 hours and its duration of action is 20 to 30 hours. is.
Insulin dosage:
The starting dose of insulin is 0.5 units/kg/day.
Insulin is given in the morning in 2/3rd doses and in the evening in 1/3rd doses. This dose may be increased or decreased depending on food intake, exercise, and illness.
Insulin pump:
Insulin pump:
A small portable pump is used to administer insulin and its needle has to be changed daily.
Combination therapy:
The patient is provided with oral insulin.
Oral antidiabetic agents:
1)sulfonyle urea,
2)meglitinides,
3)thiazolidinediones,
4)bigunides,
5)alpha glucoside inhibitor.
This therapy is mainly used in patients with type 2 diabetes.
Nursing Management:
1)Impaired nutritional status more than body requirement related to intake inexcess of activity expenditure.
- The primary goal of a diet plan is to control glucose levels so that Assess the patient’s glucose level, and assess the patient’s lifestyle, cultural background, activity level, dietary habits, and food preferences.
- Instruct the patient to eat adequate amounts of food and to have snacks in between.
- Arrange extra meals before the patient engages in physical activity.
- Administer insulin as ordered by the doctor.
2)imbalance fluid volume related to increased stress hormone as evidenced by polyuria.
- Assess the patient’s intake output chart.
- Ask the patient to take fluids orally.
- Provide the patient with fluids intravenously.
- Check the patient’s serum electrolyte levels.
- To check the patient’s vital signs.
3)activity intolerance related to weakness as evidenced by limited activities.
- Assess the patient’s activity level.
- Plan the patient’s activity.
- Provide the patient with analgesic medicine before resuming activity.
- Assist the patient to rest between activities To tell.
- Provide the patient with prescribed medicine.
4) Knowledge deficit related to cause and disease as evidence by asking questions.
- Assess the patient’s knowledge level.
- Provide education to the patient about the diet for diabetes.
- Provide education to the patient about foot and nail care.
- Provide education to the patient to cover their feet with soft shoes.
5)fear related to insulin injection.
- Monitor the patient’s blood glucose level.
- Educate the patient about self-administration of insulin Provide education.
- Provide education to the patient about the complications of insulin therapy.
- Provide education to the patient about the signs and symptoms of hyperglycemia and hypoglycemia.
AIDS (Acquired Immunodeficiency Syndrome):
- Acquired Acquired Immunodeficiency Syndrome (AIDS) is a fatal illness. It is mainly transmitted by the human immunodeficiency virus (HIV). Once a person is infected with HIV, it remains for life. HIV weakens the immune system of a person, so any infection can easily get into the person’s body. Therefore, AIDS is not a single symptom but a group of many symptoms, hence it is called a syndrome. Its incubation period ranges from 2 months to 4 years.
Etiology:
- Human Immunodeficiency Virus,
- Hiv 1,
- Hiv 2,
- Sexual worker
- Health care worker,
- Any HIV infected person’s blood Due to contact with semen, cerebrospinal fluid, teachers, saliva, breast milk, cervical or vaginal secretions.
- Due to sexual activity with an HIV infected partner.
- Due to injecting with infected needles and syringes.
- Transmission can occur from an infected mother to her child.
- Due to contact/exposure to contaminated blood.
- Blood transfusion.
- Organ transfusion.
- A person who has already come into contact with someone who has syphilis or any other sexually transmitted disease.
Sign And Symptoms (Sign And Symptoms):
- Weight loss,
- Diarrhea,
- Arthralgia,
- Continuous cough for a month,
- Fever,
- Pharyngitis,
- Lymph node swelling,
- Weakening of the muscular system,
- Dyspnea,
- Headache,
- Enlargement of the liver.
- Headache.
- Sore Throat.
- Enlargement of the spleen.
- Mouth sore.
- Nausea and vomiting.
- Skin rashes.
- Fatigue.
- Oral ulcers.
- Loss of appetite.
- Weight loss.
- Night sweats.
- Swelling of lymph nodes.
- Diarrhea.
- Soreness in the mouth, anus, and genital area.
- Skin rashes. Neurological symptoms are seen.
Mode of transmission:
Spread:
1) Sexual Transmission: HIV and AIDS are transmitted through sexual contact.
2) Transmission through Blood:
AIDS is transmitted through the transmission of infected blood or direct contact with any infected blood.
3) Perinatal Transmission:
It can be transmitted from an infected mother to her child.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History Collection,
- Physical Examination.
- Recombinant DNA
- Technique
- PCR (Polymerase Chain Reaction).
- ELISA (Enzyme Linked Immuno Sorbent Assay).
- Viral Isolation in Culture.
- Lymphnode Biopsy.
- Rapid HIV Antibody Test.
- Western Blot Antibody Testing.
- Hiv viral load test.
- Complete Blood Count.
- CD4CELL Count.
Management:
1) Nucleoside Reverse Transcriptase Inhibitor( NRTI).
EX:= LAMIVUDINE
ZIDOVUDINE.
2)Non-nucleoside reverse transcriptase inhibitor (NNRTI):
EX:= EFAVIREN
( SUSTIVA).
ETRAVIRINE
( INTELENCE).
3)Protease Inhibitor:
Ex:= ataxanavir.
Duranavir.
4) Entry or Fusion Inhibitor
EX:=enfuvirtide
( fuzeon),
Maraviroc
( selzentry).
5) Integrase Inhibitor:
EX:=raltegravir
( isentress).
Nursing Management:
- Provide proper position to the patient.
- Advise the patient for deep breathing exercises.
- Provide proper oxygen to the patient.
- Maintain the patient’s hydration status.
- Assess the patient’s nutritional status.
- Provide the patient with a diet that is high in protein and high in calories.
- Provide the patient with fresh fruits, vegetables, whole grains, and protein.
- Provide the patient with easily digestible foods.
- Provide the patient with daily mouth care.
- Provide the patient with foods that the patient likes. To do.
- Maintain the patient’s social support.
- Spend time with the patient.
- Interact properly with the patient and their family members.
- Assess the patient’s skin integrity.
- Provide back care to the patient.
- Tell the patient about the importance of personal hygiene.
- Keep the patient away from anyone who has the infection.
- Have the patient use a barrier method of contraception.
- If the patient smokes, advise them to avoid smoking.
- Instruct the health care worker to maintain strict aseptic technique.
Prevention:
- Provide education to the patient to avoid unprotected sexual contact and to use barrier methods and contraceptives.
- Avoid pregnancy in a mother who has any sexually transmitted disease. Because the infection can also be transmitted to her child.
- Provide advertisements in mass media and television to create awareness about sexual health.
- A person who has HIV infection should not donate any type of blood or organ.
- Get properly tested before blood transfusion.
- Use strict sterilization practices in hospitals and clinics.
- Do not use used needles and syringes.
- Do not come into contact with the blood and body fluids of an infected person.
- Provide proper education to the patient about AIDS.
- Provide antiviral treatment to the patient.
- Provide psychological support to the patient.
- HIV is a sexually transmitted disease.
- Do not use used razors.
- Do not use used toothbrushes.
- Do not use used needles and syringes.
- Use disposable needles and syringes.
- If needles and syringes are to be reused, they should be used only after being properly autoclaved.
- If a woman has AIDS or an infection, she should avoid pregnancy because there are chances of AIDS and HIV being transmitted to the newborn baby.
- To educate the human being about the measures that can be taken for the prevention of Aid and Hiv.
- To create awareness among the individuals about the measures that can be taken for the prevention of HIV and AIDS by using all types of mass media and technology.
- To advise the individuals to avoid donating blood and other body organs from the individuals who are at high risk of HIV and AIDS.
- To get HIV and AIDS screening done when blood is to be transfused or blood is to be taken.
- To use sterilization techniques in hospitals and clinics.
- To use disposable needles and syringes as far as possible.
- If not possible, then use sterilized needles and syringes.
- Use zidovudine tablets as curative measures.
- Avoid contact with infected blood and body fluids.
- When coming into contact with blood and body fluids, medical personnel should observe universal precautions and use personal protective equipment (PPE) kits.
- Take extreme precautions when injecting and skin piercing.
- Use sterilization and disinfectant effectively.
- Provide education to the person about AIDS.
- Provide health education about A=Avoidable,
- I=Incurable,
- D=Disease,
- S=Syndrome.
- Explain AIDS diseases to the student properly.
- Also educate people that AIDS is not spread by any kind of flies or mosquitoes but is spread through unprotected sexual contact.
- Educate people that AIDS is not spread through clothes but through blood and body fluids.
- Proper precautions should be taken by staff working in hospitals who do not have HIV and AIDS.
- Provide antiretroviral therapy to people who have HIV and AIDS.
(STD: Sexually transmitted diseases)

Syphilis :
- Syphilis is a sexually transmitted disease.
- The causative organism of syphilis is the spirochete Treponema pallidum. The disease starts with syphilitic lesions in the genital tract and mainly occurs in the genitals, rectum and mouth. The disease is transmitted by direct contact with another person who has primary or secondary syphilitic lesions. Its incubation period is 9-90 days. Symptoms typically appear within nine days and last for up to three months.
Etiology:
- Spirochaete Treponema pallidum,
- Due to coming into contact with any infected person,
- Unprotected sexual activity ,
- Due to contact with infected blood or bloody fluid.
- Due to engaging in sexual activity with multiple partners.
- Due to contact with an infected partner.
Sign And Symptoms (लक्षनो तथा चिन्हो (सिन एंड Symptoms):
These symptoms depend on the stage of syphilis. Such as,
1)Primary stage
2)Secondary stage
3)Latent stage
4)Late stage
1) Primary syphilis:
- Primary syphilis occurs when the body comes into contact with the bacteria Then it is seen in two to eight weeks. It starts with a small round sore called a chancre which is painless but highly infectious.
- Small papules and lesions
The sore may be single or multiple,
The sore may also be present on the lips, tongue, hands, rectum and nipples.
Painless ulcers without any surrounding inflammatory reaction,
Inguinal glands may be enlarged.
2) Secondary Stage:
- The secondary stage starts two to four weeks after the appearance of the sore and lasts for two to four years.
- Low grade fever,
- Headache,
- Loss of appetite,
- Weight loss,
- Anemia,
- Sore throat,
- Hoarseness,
- Jaundice with or without hepatitis,
- Joint, muscle, long bone pain,
- Coarse, flat top, moist and necrotic lesions.
3) Latent Stage:
- This is the third stage of syphilis. This stage usually lasts for five to 20 years. This is mainly asymptomatic but affects multiple organs.
- In this, tumors occur in the skin, bones, and liver.
4) Late stage:
- This is the last stage of syphilis and about 15 to 30 percent of people who do not take treatment for syphilis enter this stage and its duration is very long. And this last stage is a life-threatening condition.
- A tumor-like mass is created in this.
- It damages the heart valves and blood vessels.
- Meningitis (infection and inflammation of the meninges layer of the brain),
- Paralysis.
- Coordination is lost No.
- Insomnia.
- Confusion.
- Impaired judgment.
- Slurred speech.
- Difficulty seeing.
- Deafness occurs.
- Mental illness.
- Memory declines.
Diagnostic Evaluation:
- History collection,
- Physical examination
- Blood Test:
- Blood test is done to see if any syphilis antibodies are present in the body
- Cerebrospinal fluid analysis.
- VDRL test.
- FTA-ABS (Fluorescent Treponemal Antibody Absorption) test is specific for Treponema palladium test.
Management:
- Treatment of syphilitic lesions is divided into three stages:
- 1.Early syphilis: (primary, secondary and early latent syphilis)
- a Benzathine penicillin G 2.4 mega units I/ M single dose every buttock. Half dose.
- b. Procaine penicillin G 600,000 units I/ M daily for 10-14 days.
- c. In penicillin hypersensitivity cases, tetracycline or erythromycin 500 mg orally 4 times a day for 14 days
- 2. Late syphilis: Benzathine penicillin G 2.4 mega units I/ M is given weekly for 3 weeks.
- 3) Follow-up:
- Serological tests are done after 1, 3, 6 and 12 months after treatment of early syphilis.
- Late symptomatic In cases, for life-sustaining surveillance, serological tests are performed annually.
Nursing Management:
- Treatment should be started as soon as the disease is detected.
- To control the disease, the patient should undergo examination at 3rd, 6th, and 12th months.
- Avoid coming into contact with a person who has syphilis infection.
Detailed examination of the person who is suspected should be done. - Provide education to the patient or use barrier method of contraception.
- Provide symptomatic treatment to the patient.
- Provide education to the patient and take proper treatment.
- Provide education to the patient and take proper treatment.
- Continuous abstinence until recovery from syphilis or any other sexually transmitted disease.
- Provide education to the patient on using a barrier method as a contraceptive.
- Maintain patient’s privacy and confidentiality.
- Instruct the patient to have regular follow-up.
- Educate the patient on sexual hygiene To provide.
Gonorrhea:
- Gonorrhea is a common sexually transmitted venereal disease. The causative organism of gonorrhea is Neisseria gonorrhoea. This infection is mainly transmitted in the genitourinary system, in which the genitals and rectum are involved. If this disease is not treated, then fever and arthritis can occur. If the hands are contaminated by this organism, then there is a possibility of this infection spreading to the eyes. Gonorrhea infection is mainly seen in the age group of 15 to 24 years. Gonorrhea is also known as “the clap” or “the drip”. Its incubation period is 3-7 days.
Etiology:
- Neisseria gonorrhoeae bacteria,
- Transmitted through vaginal, oral and anal sexual contact
- Any previous history of gonorrhea.
- Any other sexually transmitted infection.
- Not maintaining proper hygienic conditions of the genital area.
- If gonorrhea has already been diagnosed.
- If sexual activity started early.
- If there are multiple sex partners.
- If a pregnant mother has gonorrhea, she can transmit the infection to her baby.
Sign And Symptoms:
Male :
- Burning sensation occurs during urination.
- Purulent discharge comes out of the penis.
- Frequency of urination increases.
- Pain, redness and soreness occur.
- Urethral scarring.
- Enlarged scrotum.
- Pain and itching sensation during urination.
- Inflammation of the prostate gland and testicles.
- A thick yellow and green discharge comes out from the tip of the penis.
Female (Female) :
- Purulent discharge.
- Discomfort and pain in the abdomen.
- Burning sensation.
- Urgency and frequency in urination.
- Difficulty walking.
- ( Salpingitis: Infection and inflammation of the fallopian tubes).
- Fever,
- Vomiting,
- Low back pain,
- Pain during intercourse,
- Discharge and irritation from the anal area. Bleeding.
- Tenderness in the abdomen and pelvic area.
Diagnostic Evaluation:
- History taking,
- Physical examination,
- Swab test,
- Culture from the cervix, urethra, rectum or throat.
- Urine examination.
- Nucleic acid Test.
- Gram staining.
Management:
- Specific treatment for gonorrhea is a single dose of any of the following medications:
Ceftriaxone: 125 mg I/ M - Ciprofloxacin: 500 mg orally.
- Ofloxacin: 400 mg orally.
- Cefixime: 400 mg orally.
- Levofloxacin: 250 mg orally.
- Treatment of neonatal conjunctivitis is with a single dose of ceftriaxone (20-30 mg/kg) IM and gentamicin eye ointment (1%).
- Follow-up: Culture should be done 7 days after therapy. Repeat culture is done after 3 months at monthly interval.
Nursing Management:
- Take proper history of the patient.
- Provide proper antibiotic medicine to the patient.
- For syphilis Perform serum examination.
- Provide proper education to the patient about personal hygiene.
- Provide proper education to the patient about the disease condition.
- Advise the patient to avoid multiple sex partners.
- Educate the patient to use a contraceptive method, such as a barrier method.
- Provide proper psychological support to the patient.
- Provide antibiotic medicine to prevent infection.
- Ask the patient to maintain personal hygiene.
Complications (complications) :
- Pelvic Inflammatory Disease (PID),
- Infertility,
- Ectopic Pregnancy,
- Dyspareunia,
- Chronic Pelvic Pain, Tubo-Ovarian Mass,
- Bartholin Gland Abscess.
Tuberculosis during pregnancy:
- Tuberculosis is a serious infection caused by the bacterium Mycobacterium tuberculosis that mainly affects the lungs but can also spread to other areas of the body. Pulmonary tuberculosis is spread through the air, that is, by coming into contact with an infected person coughing or sneezing.
Etiology:
- Close contact with active tuberculosis patient
- Weak immune system (HIV, organ transplantation, cancer, corticosteroid therapy)
- Age
- Living in overcrowded area
- Malnutrition
- Chronic Health Conditions
Sign And Symptoms:
- Persistent cough (coughing for more than three weeks)
- Blood in sputum,
- Chest pain,
- Fever,
- Feeling cold,
- Swollen glands,
- Fatigue,
- Night sweats,
- Loss of appetite,
- Weight loss,
- Shortness of breath,
- Poor growth,
- Cuffing,
Diagnostic Evaluation:
- History Collection
- Physical Examination
- Tuberculin Skin Test
- X Ray
- Sputum Test
- Blood Test
Management:
- Antibiotic therapy is a combination of antibiotics given as a treatment for tuberculosis. In which isoniazid, rifampin, ethambutol and pyrazinamide medications are given. This medicine is given for a course of six to nine months.
- Directly Observed Treatment Short Course (DOTs)
In DOTs therapy, the TB patient is supervised by a health care provider. The patient takes the regular medicine exactly and its effectiveness is observed. So that it can be known whether the patient has completed the full course of treatment or not. - Isolation
TB positive patients are isolated. Because TB is a contagious disease and it spreads through the air. Therefore, the patient is isolated to prevent its spread. - Nutritional Support
Provide adequate nutritional support to the patient with TB so that his immune system can be improved and weight can be gained. - Education and Counseling
Provide education and counseling to the patient about tuberculosis. Explain infection control measures to the child and his family members.
- Management:
- Provide proper antipyretic medication to maintain the patient’s body temperature and if the child has a fever.
- Provide antibiotic drugs to treat bacterial infections.
- Provide expectorant drugs to expel phlegm.
- Provide nasal decongestants to relieve congestion.
- Get adequate rest and plenty of fluid intake.
- Avoid contact with irritants.
- Properly and completely assess the patient.
- Properly assess the patient’s respiratory status.
- To assess the patient’s vital signs completely.
- To properly assess the patient’s oxygen saturation.
- To properly assess the patient’s condition, continuously monitor the patient’s respiratory status and oxygen saturation.
- To continuously monitor the patient’s body temperature.
- To maintain the patient’s hydration status. And advise the patient to continuously ingest fluids to keep the mucus thin.
- Provide the patient with a properly comfortable position.
- Provide the patient with adequate oxygen to maintain the oxygen saturation of the patient’s body and to provide respiratory support.
- Provide the patient with properly prescribed medications.
- The patient and his/her Provide complete education to the family members about the child’s condition, its causes, symptoms and signs and its treatment.
- Provide proper work and comfortable environment to the patient.
- There is no need to terminate pregnancy in patients with tuberculosis.
- Provide proper care to the antenatal mother during the antenatal period itself so that maternal anemia and preeclampsia can be properly treated and managed.
- If the patient prefers hospital delivery, then he should be admitted to the hospital two weeks before the expected date of delivery.
- Advise the patient to take proper bed rest.
- Maintain the patient’s nutritional and hydration status properly.
- Advise the patient to do proper breathing exercises.
- Advise the patient to avoid fatty and spicy food.
- Advise the patient to take high protein.
- Advise the patient to keep her child properly separated after delivery and to contraindicate breastfeeding.
- If the mother is suffering from an active disease, then provide the baby with prophylactic T. Isoniazid 10-20mg/kg/day for 3 months.
- The child should be given isoniazid-resistant B.C.G. as soon as possible.
- Proper feeding should be provided to the baby. The baby’s temperature should be maintained regularly.
- The baby should be prevented from getting infected.
- The patient should avoid pregnancy for 2 years.
- The patient should be advised to avoid oral contraceptive medication while taking Rifampicin medicine.
- If the patient’s family is complete, then they should be advised for permanent sterilization method giving.
Multipara :
Definition:
- A woman who has more than one fetus reaching the stage of viability is called multipara.
Complications:
During Pregnancy:
- Abortion,
- Obstetrical hazards such as malpresentation,
- Multiple pregnancies,
- Placenta previa.
- Medical Disorders:
- Anemia,
- Hypertension,
- Cardiovascular complications .
- Prematurity,
During Labor:
- Cord prolapse,
- Cephalopelvic dishproportion (CPD),
- Obstructed labor,
- Rupture of the uterus,
- Postpartum hemorrhage,
- Shock,
- Precipitated labor,
- Prolapsed umbilical cord.
During puerperium:
- Increased morbidity rate due to intra-natal hazards.
- Subinvolution.
- Falling lactation.
Management:
- Multipara is considered in the highest category so the mother should be hospitalized immediately.
- Proper antenatal care should be provided to the mother.
- Delivery of a woman with multipara should be done in a hospital with a well-hospitalized facility.
- Presentation and position of the fetus should be checked properly at the time of delivery.
- After delivery, the mother should be given post The condition of Partum Hemorrhage (PPH) should be properly assessed.
Heart Disease During Pregnancy:
- Heart disease during pregnancy refers to any cardiovascular condition that affects the heart or blood vessels and occurs or worsens during pregnancy. This includes preexisting conditions, such as congenital heart disease or valvular heart disease, as well as conditions that develop during pregnancy, such as gestational hypertension or peripartum cardiomyopathy. These conditions can affect both the health of the mother and the developing fetus. The incidence of cardiac lesions in hospital deliveries is less than 1%. The mood in common cardiac listening is rheumatic.
Etiology:
- Advancing age,
- Cardiac arrhythmia,
- Left ventricular Hypertrophy,
- Previous heart failure,
- Due to the occurrence of risk factors such as infection, anemia, pre-eclampsia, severe weight gain, multiple pregnancy, inadequate supervision.
Classification of heart disease:
- Grade 1: Symptoms are not noticeable during physical activity and the state is uncompromised.
- Grade 2: Slightly compromised with some limitations in physical activity. The patient is comfortable at rest but uncomfortable with normal physical activity.
- Grade 3: Markedly compromised in which the patient is comfortable at rest but uncomfortable with less than normal physical activity.
- Grade 4: Severely compromised in which the patient is uncomfortable even at rest.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History Collection,
- Physical Examination,
- Chest X-ray,
- ECG,
- Echocardiography,
- Cardiac MRI,
- Doppler Flow Studies.
Sign And Symptoms:
Symptoms:
- Breathlessness,
- Nocturnal cough,
- Syncope,
- Chest pain.
Sign:
- Chest murmur,
- Cardiac enlargement,
- Arrhythmia,
- Chest radiography,
- Cardiomegaly,
- Pulmonary vascular markings increase,
- Enlargement of pulmonary veins,
- Dyspnea on exertion,
- Edema,
- Heart murmur,
- Palpitation,
- Bounding and collapsing pulse,
- Chest pain,
- Peripheral edema,
- Dilated jugular vein,
- Limitation of physical activity.
Aim of Management:
- The aim of management is to maintain and improve the physical and psychological well-being of the mother and fetus.
- To prevent major maternal complications.
- To detect high risk factors and prevent the development of cardiac failure.
Management:
- It is important to provide proper hospital care to patients with heart disease.
- Antenatal Care:
- Patients with heart disease should be supervised in a tertiary care hospital. Initial assessment should be done by a cardiologist.
- Intraperitoneal injection of Penidur LA 12 (benzathine penicillin) should be given at four-week intervals during pregnancy.
- Detect and provide proper treatment for each risk factor during antenatal visit.
- Properly assess the patient for dyspnea and cough.
- Properly auscultate for crepitus.
- Hospitalize the patient if the heart rate is more than 100/minute.
- Assess for anemia, weight and blood pressure.
- Re-evaluate the patient’s condition.
- Look for congenital abnormalities through sonography.
- Antenatal advice: Advise the patient to take adequate bed rest.
- Avoid excess excitement and stress.
- Avoid high calorie and spicy diet.
- Advise to avoid low salt diet intake in food.
- Advise the patient to take low carbohydrate diet intake.
- Antenatal advice: Advise to take adequate rest, advise to avoid excess excitement and strain, advise to avoid high calorie and spicy food. Advise to take low salt, less carbohydrate and fat but more protein in diet, correct anemia. Avoid cold and infection and take adequate dental care.
- Anticoagulant: Congenital heart disease, pulmonary hypertension, artificial valve replacement/atrial fibrillation, anticoagulant is given. Give heparin injection 5000 units twice daily subcutaneously as per instructions for 12 weeks of pregnancy, then give warfarin tablet 3mg daily at the same time till 36 weeks. Then give heparin injection till 7 days postpartum and then start warfarin tablet.
- Indications for surgery in pregnancy: Medical treatment fails, intolerance symptoms, cardiac failure.
- Admission/Hospitalization:
- Grade-1: Two weeks before expected date of delivery.
- Grade-2: Unfavorable social environment during 28 weeks.
- Grade-3&4: When pregnancy is diagnosed, keep the patient in the hospital throughout the pregnancy.
- Management of cardiac failure in pregnancy Proper care.
- Labor: Usually spontaneous labor and delivery occur without complications, and some obstetric indications are done with labor induction (vaginal PGE2).
- First stage:
- Position: Provide lateral recumbent position.
- Oxygen: 5-6 L/min.
- Analgesia: Epidural.
- Fluid: Provide not more than 75ml/hour.
- Watch carefully: Properly assess the patient’s pulse and respiration rate. If the pulse rate exceeds 110/min, provide intravenous digoxin 0.5 mg. Properly monitor vital signs through cardiac monitoring. Monitor central venous pressure if necessary.
- Provide antibiotics prophylactically.
- Second stage: Advise to avoid maternal pushing and ventouse delivery is preferred over forceps, and should be performed without lithotomy position. Intravenous ergometrine should not be given after delivery.
- Cesarean section is not required.
- Third stage: Slight blood loss is not a problem, if excessive, give oxytocin by infusion and frusemide.
- Puerperium: Keep patient under close observation for first 24 hours, record oxygen, pulse, BP and respiration, give diuretic if necessary. Breastfeeding is not contraindicated unless patient is in failure.
Teenage Pregnancy :
- Teenage pregnancy is defined as pregnancy in women between the ages of 13 and 19. It usually involves young women who are still in their adult years and as a result may face social, emotional, and health challenges. Teenage pregnancy can affect the mother’s educational, economic stability, and health, as well as the child’s health and development. Teenage mothers are at risk of complications such as gestational hypertension, cephalopelvic disproportion, anemia, and nutritional deficiencies. They also have a higher incidence of sexually transmitted diseases. Infants born to teenage mothers may suffer complications such as prematurity, birth asphyxia, and low birth weight.
Etiology:
- Fear of reporting sexual activity to parents.
- Limited use of contraceptives Use
- Low education level.
- Low knowledge of the ability to get pregnant.
- Due to early marriage.
- Low use of contraceptives.
- Due to rape.
- Sexual abuse Due to.
Diagnostic Evaluation:
- Positive pregnancy test, ultrasonography.
Management:
- Maintain adequate calorie intake in the diet, so that the growing adolescence and its fitness get adequate support.
- Educate the client on proper prenatal care and how to report possible problems to health care providers.
- Drugs: Give antibiotics if STD is present.
- Nursing Diagnosis:
- Deficient knowledge (maternal) about pregnancy and related responsibilities.
- Nutrition less than body requirements.
- Interrupted family processes.
- Planning and goals:
- Increase the patient’s knowledge about pregnancy and related responsibilities.
- Nutritional Advise on diet.
- Provide proper support to the patient and their family members.
- Implementation:
- Monitor nutritional deficiencies and monitor the amount of weight gain the patient is experiencing.
- Properly monitor blood pressure for gestational hypertension and glucose levels for gestational diabetes.
- Properly monitor the patient’s fundal height.
- Properly assess the patient’s knowledge.
- Properly conduct antenatal check-ups for the patient.
- Provide proper education to the patient about options such as pregnancy termination, continuation, etc.
- Allow the patient to explain his/her feelings and Promote mental and emotional well-being.
- Provide proper health education to the patient.
Osteomalacia:
- Bones need calcium and phosphorus to stay healthy and strong, but the body also needs vitamin D to absorb these two minerals. Without this vitamin, bones can become soft and flexible. This softening after the growth plate has closed is called osteomalacia. Osteomalacia is a softening of the bone usually caused by a deficiency of vitamin D. The affected bone is a soft bone. Osteomalacia is caused by a deficiency of vitamin D in the body, which can be caused by conditions that interfere with the absorption of vitamin D in the body, e.g. intestinal disorders.
Etiology:
- Due to vitamin D deficiency.
- Celiac disease,
- Kidney or liver disease,
- Certain types of surgery,
- Malnutrition during pregnancy,
- Certain types of drugs Cause.
Sign And Symptoms:
- Bone pain that spreads to the lower back, pelvis, hips, and ribs.
- Tenderness in the arms, legs, and spine.
- Low calcium levels cause muscle spasms and cramps.
- Low calcium in the body causes tingling and numbness sensation in the extremities or around the mouth.
- Bone fractures can occur very easily.
- Muscle weakness.
Diagnostic Evaluation:
- History collection,
Physical examination,
Diagnosis of osteomalacia is done through few blood investigations like:
Vitamin D level: This is assessed in the case of osteomalacia.
Calcium level: This is assessed in the case of osteomalacia.
Phosphorus level: This is assessed in the case of osteomalacia. - Alkaline phosphatase isoenzyme level: The level here is indicative of osteomalacia.
Parathyroid hormone level: An elevated level means that the body does not have adequate amounts of vitamin D.
X-rays and other imaging tests: These will show small cracks in the bone throughout the body (loose transformation zones).
Bone biopsy is rarely done.
Management:
- In cases of osteomalacia, early oral supplementation of vitamin D, calcium and phosphorus is prescribed by the doctor.
- In cases of absorption problems due to intestinal injury or surgery, intravenous vitamin D is prescribed.
- It is advisable to stay in the sun exposure. Antenatal check-ups are done periodically.
- The patient is properly prepared for delivery in a well-equipped hospital. Giving advice.
