ENGLISH-unit-12-neurological Disorder(part-1)(UPLOAD)
Nursing management of patients with the Neurological disorder and disease:
key terms:
1) Explain/Define Craniotomy. (Define Craniotomy)
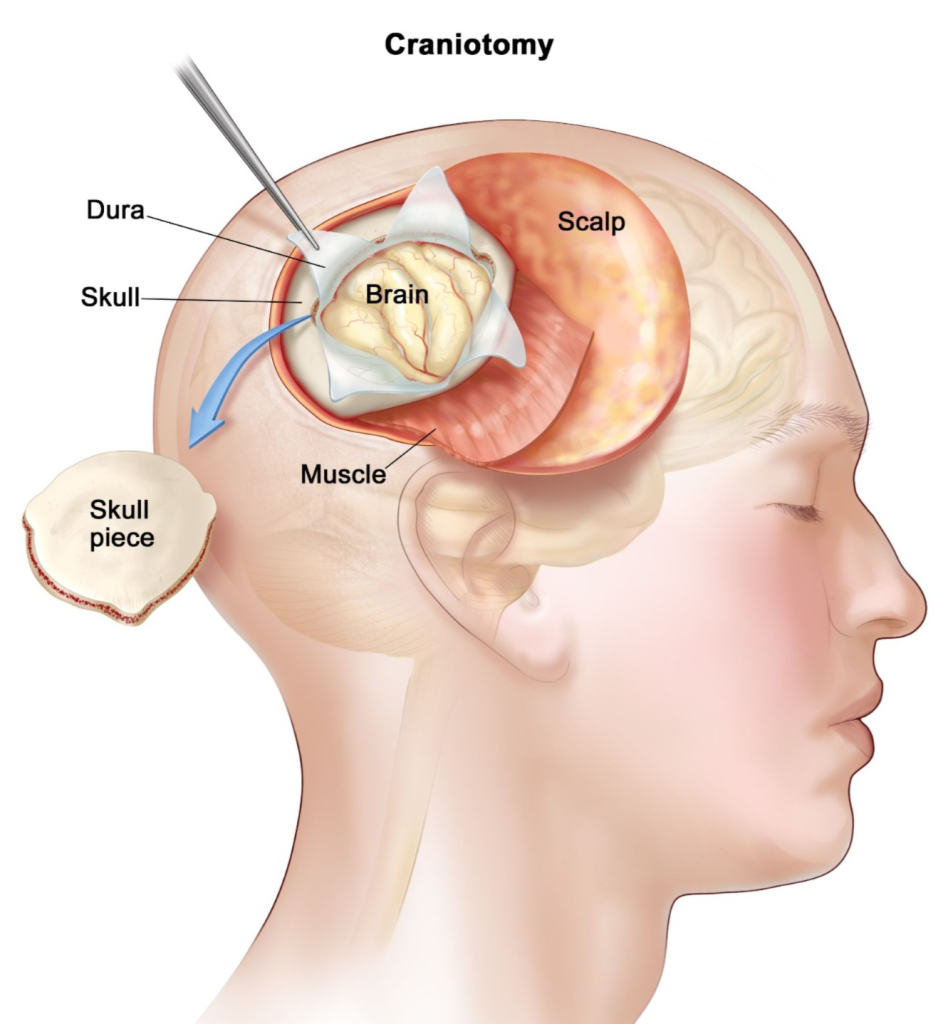
- A craniotomy is a surgical procedure in which A small hole (opening) is made in the skull bone to perform various types of medical procedures on the brain.
2) Explain/Define craniectomy.
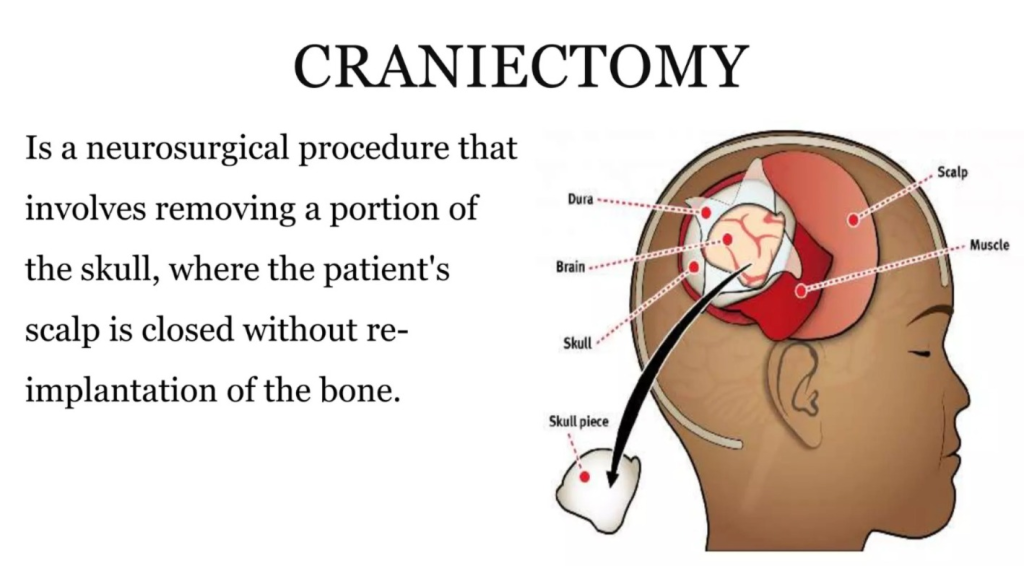
- Craniectomy is a surgical procedure in which a small portion of the skull bone is removed.
3) Explain/ Define Dysphagia. (Define Dysphagia)
- Swallowing difficulty is called Dysphagia.
4) Define/Explain photophobia. (Define Photophobia)
- Intolerance of light is called photophobia
- When a person has a condition of photophobia, even when exposed to minor light, they experience pain and discomfort in their eyes.
5) Explain/ define Agnosia. (Define agnosia)
- Agnosia is a type of neurological disorder in which a person is unable to recognize any things or objects through his sensory system. It is called agnosia.
6) Define/ Explain Ataxia. (Define ataxia)
- Ataxia is a condition in which a person’s muscle movements are not properly coordinated. The inability to coordinate leads to difficulty walking, speaking, and performing self-care activities.
7) Explain/ Define Tone. (Define Tone)

- The tension present in the muscles at rest is called tone.
8) Explain/ define the increased intracranial pressure. (Define Increased Intracranial Pressure)
- Intracranial pressure is the pressure that is present inside the skull. This pressure is mainly found between the brain tissue and the cerebrospinal fluid.
- Increased intracranial pressure means that the pressure of CSF increases above the normal pressure of cerebrospinal fluid. It is called increased intracranial pressure.
- Normal intra cranial pressure is 5 – 15 mmhg .
- In increase intracranial pressure the pressure of CSF is >15 mmhg .
9)Headache is also known as a:=Cephalalgia (cephalalgia)
10) Explain/Define concussion

- Concussion is a mild traumatic brain injury caused by a sudden traumatic impact or jolt to the brain, in which neural function is temporarily disturbed and symptoms such as confusion, headache, dizziness, and sometimes loss of consciousness are seen, while structural brain damage is usually not seen.
- Concussion is a temporary loss of neurological function and does not involve any structural damage to the brain. Not available. In concussion, the patient’s consciousness is lost for five minutes or less. In concussion, headache, dizziness, nausea, vomiting are mainly seen.
11) Explain/ Define Contusion. (Define contusion)
- Cerebral contusion is a bruising of brain tissue.
- Majority contusions are seen in the frontal and temporal lobes.
- These contusions are mainly seen due to any blunt trauma and injury to the brain.
12) Paraplegia : When there is impairment of sensory and motor function of any person’s lower extremities, what is it called?

paraplegia (paraplegia)
13)Quadriplegia ( Quadriplegia) : When a person has impaired motor and sensory function in their lower extremities and arms, what is it called?
Quadriplegia ( Quadriplegia)
14) Monoplegia: When the motor and sensory function of any one limb of a person is impaired, what is it called?
monoplegia (monoplegia)
15)Hemiplegia: What is it called when half of a person’s body is paralyzed?

Hemiplegia (Hemiplegia)
Explain the Neurological assessment. (Describe the neurological assessment)
- Neurological assessment mainly involves the assessment of the patient’s sensory and motor Response, especially the patient’s reflexes and any impairment in the nervous system are assessed to see if they are normal.
- A complete health history of the patient is taken in the neurological examination.
A) Present illness:=
- The patient is assessed to see if there are any signs and symptoms. Do.
- Ask the patient about the onset, duration, presentation, quality, quantity, precipitating and relieving factors of any signs and symptoms.
- If the patient is present with pain, ask about its location, intensity and whether the pain radiates.
- Ask the patient about his/her daily routine activities.
- Does the patient have any difficulty in speaking, seeing, hearing, tasting and smelling? Assess whether or not.
- Ask the patient about his/her sleep pattern.
- Ask the patient whether he/she is using any medication such as antihypertensive, antidiabetic, sedative, mood elevating drug and over the counter medication.
B) Past health history:=
- Assess the patient’s past history such as accident, fall down, any brain and spinal cord injury, and any chronic illness, seizures and any other neurological disorders.
C) Family health history :=
- Assess whether any family members have a chronic illness or not Ask.
- And ask family members about any other complications.
The neurological assessment is divided into five components.

- 1) level of consciousness and cognition ,
- 2) cranial nerve ,
- 3) motor function ,
- 4) Sensory function ,
- 5) Reflexes
1) level of consciousness and cognition
A) Mental status:=
- Mental status involves assessing the patient’s behavior, appearance, dress, grooming, movement, and facial expression.
B) Cognitive assessment:=
- In the cognitive assessment of the patient, the patient should be oriented to time, place, and person.
C) Assess the memory of patient:=
- In the memory of the patient, the patient should be 1) Recent, 2) Remote, and 3) Immediate Memory is assessed.
- 1)Recent:= In recent memory, the patient is asked what he ate for breakfast, lunch, and dinner.
- 2)Remote:= In remote memory, the patient’s birthday is assessed and any memorable events from childhood are assessed.
- 3) Immediate memory:= Provide five to six digits to the patient in immediate memory and then ask them to repeat them forward and backward.
D) Intellectual function:=
- In this, the patient’s IQ level is checked, which is mainly assessed through an interview.
E) thought content:=
- In this, the inside of the patient is checked through an interview.
- The thoughts that come to the patient’s mind are checked whether they are positive or negative.
F) Emotional status:=
- In this, whether the patient’s mood swings or not, whether the patient is irritable or not and whether he gets angry or not is assessed.
g) Language ability:=
- In language ability, ask which language the patient can understand and in which language he can write and speak.
H) impacts on lifestyle :=
- In this, if the patient has a neurological disorder, then it is assessed whether there is any kind of impact on his life.
I) level of consciousness assessed through the Glasgow coma scale ( GCS ).
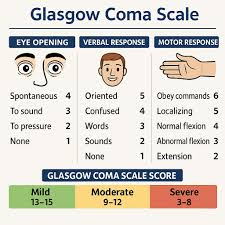
Glasgow coma scale Any type of stimulus is provided to the patient and the type of response the patient provides is assessed.
The patient’s level of consciousness is checked by the Glasgow Coma Scale.
In GCS, three components are mainly assessed.
1) Eye opening
2) Verbal Response
3) Motor Response
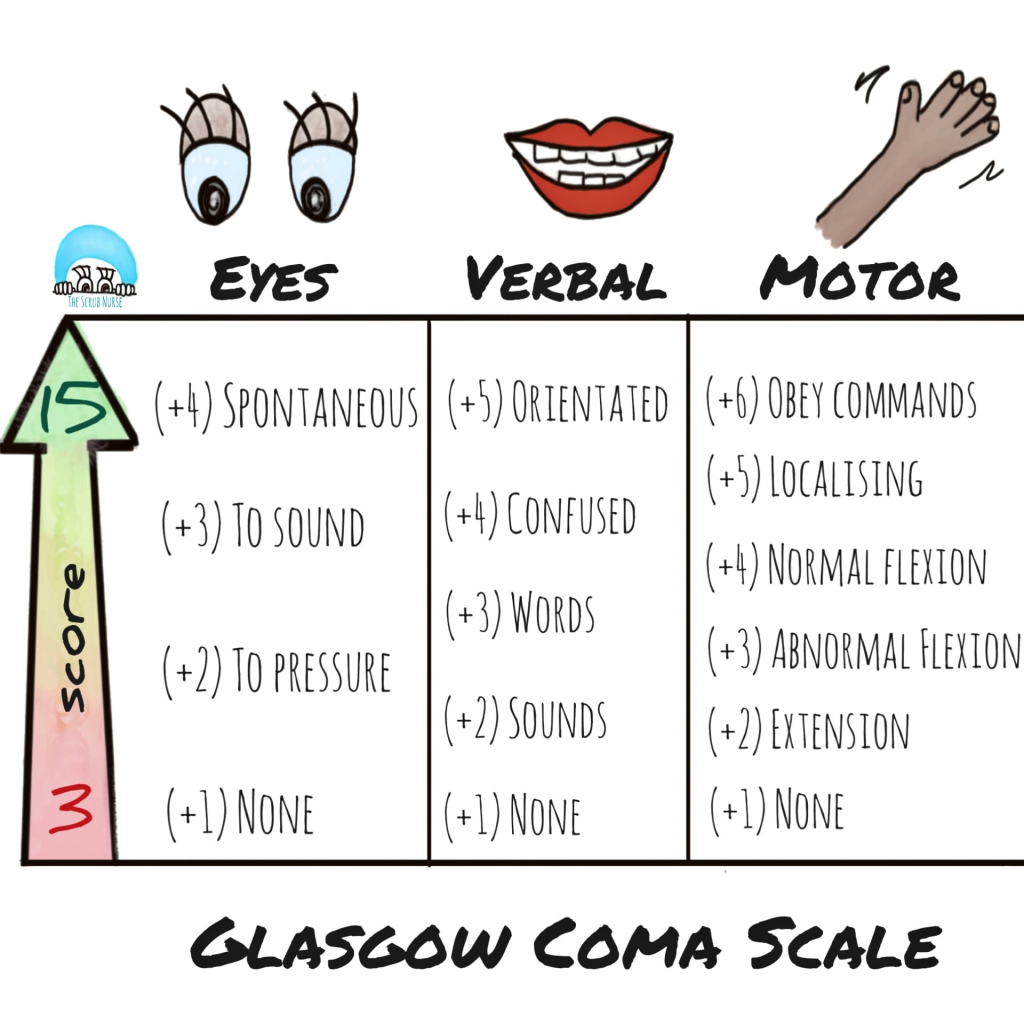
1) Eye opening
A total of four scores are given in eye opening.
1) Spontaneous (= In this, the patient opens and closes his eyes on his own) := { 4 }
2) To voice (= In this, the patient is asked to open and close his eyes and the patient follows) := { 3 } ,
3) To pain (= In this, the patient is pinched in the body and the patient makes an eye expression) := { 2 }
4) No response (No response := If there is no response from the patient) := { 1 }
2) Verbal Response
1) Oriented (Oriented:= If a person is asked about a time, place, and person and the person gives the correct answer) := { 5 } ,
2) Confused (= If the patient is asked about the time, place and person and the patient is confused):= { 4 } ,
3) Inappropriate word (= If we ask the patient a question and the patient gives a different answer) := { 3 },
4) Incomprehensible sound (= If the patient If any question is asked and he makes sound only through mouth, then) := { 2 } ,
5) No response (No response := If no response is given) := { 1 }
3) Motor Response (Motor Response)
Motor response mainly has six scores.
1) Obey command (Obey command) Command:= Whatever the patient is told to do if the patient follows it properly) := { 6 } ,
2) Localized pain ( Localized pain := If the patient is pinched and the patient provides a response) := { 5 } ,
3) Withdraw pain ( Withdraw pain := If the patient is pinched and the patient tries to withdraw his hand) := { 4 } ,
4) Flexion ( Flexion := When If any mid-area of the patient’s body is pressed and the patient’s body flexes):= { 3 } ,
5) Extension (Extension := If any stimulus is provided, the patient’s body is extended):= { 2 } ,
6) No response (No response := If the patient does not provide any response):= { 1 } is scored.
Thus, the Glasgow Coma Scale has a minimum score of 3 and a maximum score of 15.
result:=
{ 3 } score achieve:= then the patient has severe neurological damage.
{ 7 } score Achieve:= Then the patient is in a coma condition.
{ 8-12} score Achieve:= Then the patient has moderate neurological damage.
{ 13-14} score Achieve:= Then the patient has minor neurological damage.
{ 15 } score Achieve:= Then the patient is fully conscious and oriented.
Thus, the patient’s level of consciousness is assessed using the Glasgow Coma Scale.
2) Explain about cranial nerves (cranial nerve).
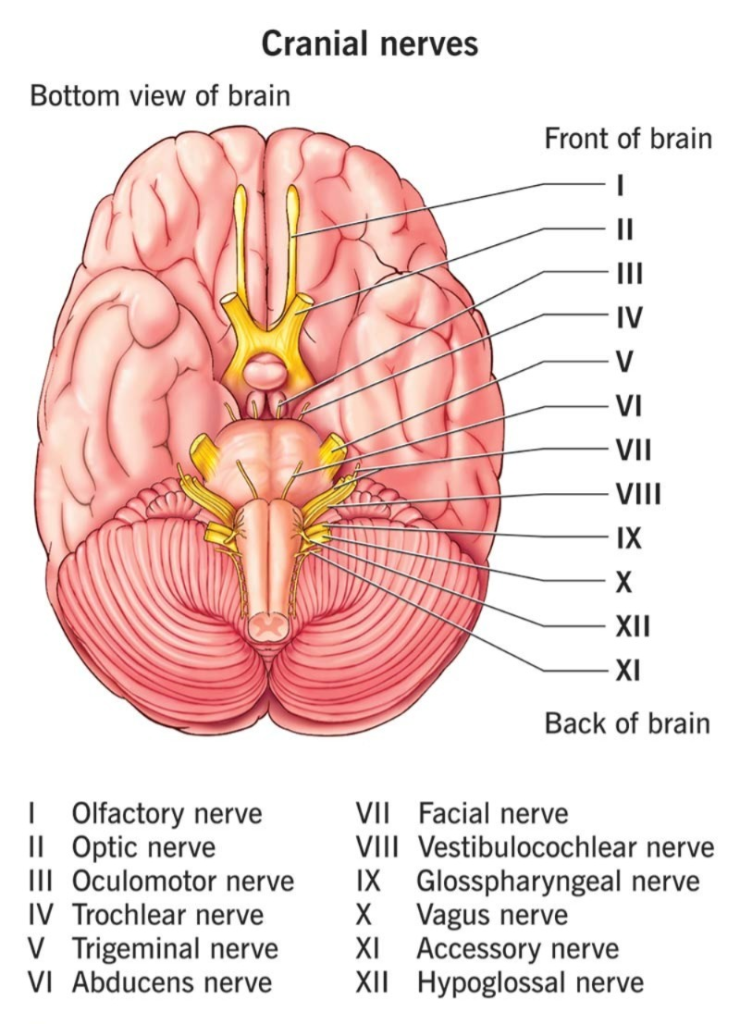
A cranial nerve examination assesses whether the patient’s cranial nerves are functioning properly.
There are total 12 cranial nerves.
Memory Trick: “Oh, Oh, Oh, To Touch And Feel Very Green Vegetables, AH!”
- O: Olfactory (I)
- O: Optic (II)
- O: Oculomotor (III)
- T: Trochlear (IV)
- T: Trigeminal (V)
- A: Abducens (VI)
- F: Facial (VII)
- V: Vestibulocochlear (VIII)
- G: Glossopharyngeal (IX)
- V: Vagus (X)
- A: Accessory (XI)
- H: Hypoglossal (XII).
Memory Tricks
1. To Remember the Names (Cranial Nerves in Order):
- Mnemonic: Heaven!
(Olfactory, Optic, Oculomotor, Trochlear, Trigeminal, Abducens, Facial, Vestibulocochlear, Glossopharyngeal, Vagus, Accessory, Hypoglossal).
To Identify the Type (Sensory, Motor, or Mixed):
- Mnemonic: Most.
(S = Sensory, M = Motor, B = Both/Mixed).
ASSESSMENT OF CRANIAL NERVES.

1) Olfactory nerve
- Type of nerve:= Sensory
- The olfactory nerve performs the function of recognizing smell.
- Assessment:=To assess the olfactory nerve, the patient is asked to close his eyes and hold any object like coffee, tea, orange near his nostril and smell it. If the patient can recognize the smell properly, then his olfactory nerve is functioning properly.
2) Optic nerve
- Type of nerve := Sensory
- The optic nerve functions for visual acuity.
- Assessment:= To assess visual acuity, the patient is assessed through a Snellen chart. In this, the patient is kept 20 feet away from the Snellen chart and then the printed material in it is read. The patient is asked to read.
3) Oculomotor nerve
- Type of nerve:= Motor nerve
- The oculomotor nerve functions to move the muscles of the eyelid, pupillary constriction, and accommodation of the lens.
- Assessment:= In the assessment of the oculomotor nerve, it is assessed whether the eyelid moves properly or not and whether it provides a proper reaction to any light.
4) Trochlear nerve
- Type of the nerve:= Motor nerve
- The trochlear nerve is responsible for the moment of the eye muscles.
- Assessment:= In this, the patient is asked to follow a letter drawn in the air with the eye. If the patient can follow it properly, then the moment of the eye muscles of the patient is said to be proper.
5) Trigeminal nerve
- Type of nerve:= (Mixed)
- The trigeminal nerve performs a mixed function of facial sensation, corneal reflex, and mastication.
- Assessment:= In this, the corneal reflex of the patient is assessed. Whether the patient has a sensation of pain or not is assessed. And advise the patient to assess their ability to clean their teeth.
6) Abducent nerve
- Type of nerve:= Motor nerve
- The abducent nerve functions to control the movement of the muscles of the eye.
- Assessment:= In this, the movement of the eye muscles is assessed.
7) Facial nerve:=
- Type of nerve:= Mixed nerve
- The facial nerve is responsible for facial expression, salivation, tearing, and Functions.
- Assessment:= In the assessment of the facial nerve, the patient is asked to smile, puff out the cheeks and raise the eyebrows. If the patient is able to do this properly, then his facial nerve is said to be functioning properly.
8) vestibulocochlear nerve
- Type of nerve:= Sensory nerve
- The vestibulocochlear nerve functions for hearing and equilibrium.
- Assessment:= To assess the vestibulocochlear nerve, the patient is assessed to see if he or she can properly hear the words spoken by a person.
9) Glossopharyngeal nerve
- Type of nerve:= Mixed nerve
- The glossopharyngeal nerve works for taste, sensation of the pharynx and tongue, and movement of the pharyngeal muscles.
- Assessment:= To assess the glossopharyngeal nerve, ask the patient to assess the taste of sour, salty, and sweet.
10) vagus nerve
- Type of the nerve:= Mixed nerve
- The vagus nerve functions to innervate the muscles of the pharynx, larynx, and soft palate, and to provide ear sensation.
- Assessment:= Vagus To assess the nerve, ask the patient to say “ah” and observe the patient’s palate and pharynx movements and assess whether any hoarseness is present in the patient’s speech.
11) Accessory nerve
- Type of nerve:= Motor nerve
- The accessory nerve innervates the sternocleidomastoid and trapezius muscles.
- Assessment:= Ask the patient to move the shoulder and assess the function of the accessory nerve. Do.
12) Hypoglossal nerve
- Type of nerve:=( motor nerve)
- The hypoglossal nerve plays an important role in the movement of the tongue.
- Assessment:= To assess the hypoglossal nerve, ask the patient to stick his tongue in the middle and assess the hypoglossal nerve.
- Thus, 12 cranial nerves are assessed.
3) Assessment about motor function,
In this, the patient’s motor ability, balance, and coordination and gait are assessed.
A) Motor ability
- In this, the size, tone, strength, coordination, balance, posture, symmetry of the muscles are assessed.
- The patient is assessed for any involuntary movements.
- Does the patient have rigidity and stiffness in the body? Otherwise, it is done.
B) Muscles strength :=
- In this, the patient’s muscle strength is assessed and the extent of weakness in the patient is assessed.
C) Co ordination (Coordination)
- In this, the coordination of the patient is checked.
D) Gait testing (Gait testing)
- In this, it is assessed whether the patient can walk properly or not.
4) Assessment about Sensory function,
1) Touch sensation
- To assess touch sensation, cotton is touched to a part of the body and then its sensation is assessed.
2) Pain sensation
- The sensation of pain is assessed by touching a sharp object to the patient’s body.
3) Temperature sensation
- In this, the patient is assessed to see if he or she has the sensation of hot and cold thoughts.
4) Vibration
- Vibration is mainly assessed using a low frequency tuning fork.
5) Position sense
- To assess position sense, ask the patient to close both eyes, then move the toes up and down, and then assess the moment.
5) Assessment about Reflexes
In reflex testing, five reflexes are mainly assessed.
1) Biceps reflex
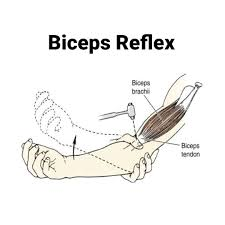
- In this test, the examiner holds the patient’s forearm, then places the thumb on the front part of the arm, then strikes the hammer on the thumb, then the elbow is properly flexed and the biceps muscles are properly contracted. If there is a contraction, the biceps reflex is a normal response.
2) Triceps Reflexes
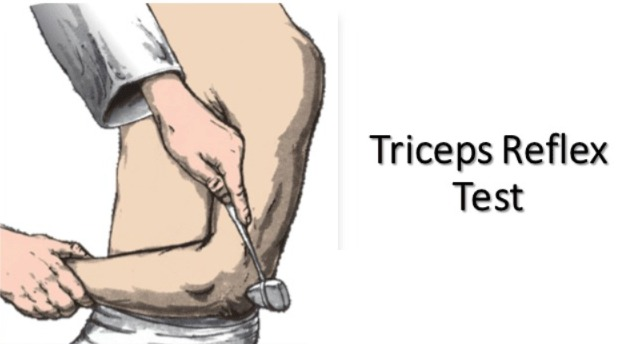
- In this test, the examiner provides support to the arm and then identifies the triceps tendon, which is present in the upper arm 2.5 to 5 centimeters above the elbow. It is flicked by the hammer. In this, the triceps muscles contract and the elbow extends, then the triceps reflex is said to be normal.
3) Brachio radial ( Brachioradialis)
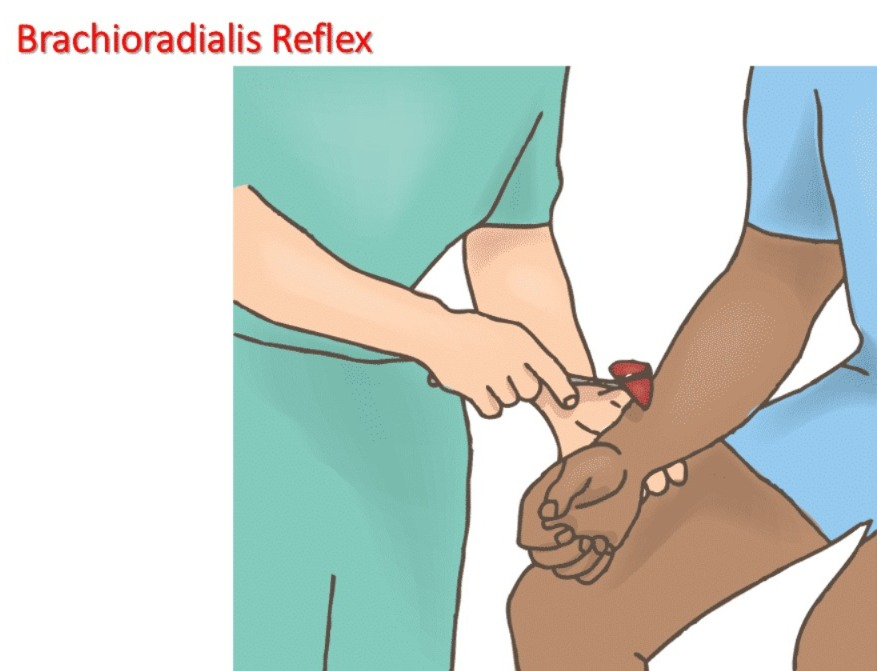
- In this procedure, a gentle strick is made with a hammer 2.5 to 5 centimeters above the wrist if the forearm is flexed. So brachio radialis reflux is normal.
4) patteler reflux

- In this, the patient is provided with a supine position, after which the examiner facilitates the leg, due to which the muscles relax. If the knee is extended, then patellar reflux is normal.
5) Achilles reflux testing
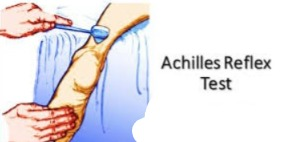
- In this, the patient is provided with a sitting position, after which the patient’s feet are kept slightly above the floor, after which the examiner’s first hand is placed under the toe of the patient’s foot, after which the back of the ankle is tapped with a hammer. If the patient’s foot is If it goes slightly downward, the patient’s Achilles reflex is said to be normal.
Thus, the patient’s reflexes are assessed.
Explain the Diagnostic evaluation of the patient with the neurological disease and disorder. Explain the diagnostic evaluation of a patient with neurological disease.
- Diagnostic evaluation is mainly used to assess any disease. is.
- The following diagnostic evaluations are performed to assess neurological disorders.
1) CSF (Cerebro Spinal Fluid) Analysis
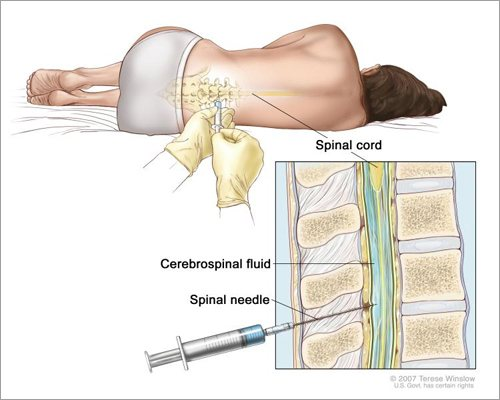
- In this test, the cerebrospinal fluid (CSF) is aspirated by inserting a spinal needle into the space between L3 – L4 and L4- L5.
- Then it is used to assess different types of diseases by aspirating.
- Like:=
- Meningitis,
- Alzheimer’s Disease,
- Cerebral Palsy,
- Epilepsy,
- Motor Neuron Disease,
- Multiple Sclerosis,
- This test is performed to diagnose.
2) Skull and Spinal X ray:=

- This is a simple X-ray that is used to detect fractures, bone erosion, calcification,
- To assess abnormal vascularity.
3) Cerebral Angiography:=

Blood vessels of the brain in cerebral angiography Examination is done to detect any abnormalities of blood vessels.
Ex:=
aneurysm,
artherosclerosis.
4)Computed Tomography (Ct scan):=
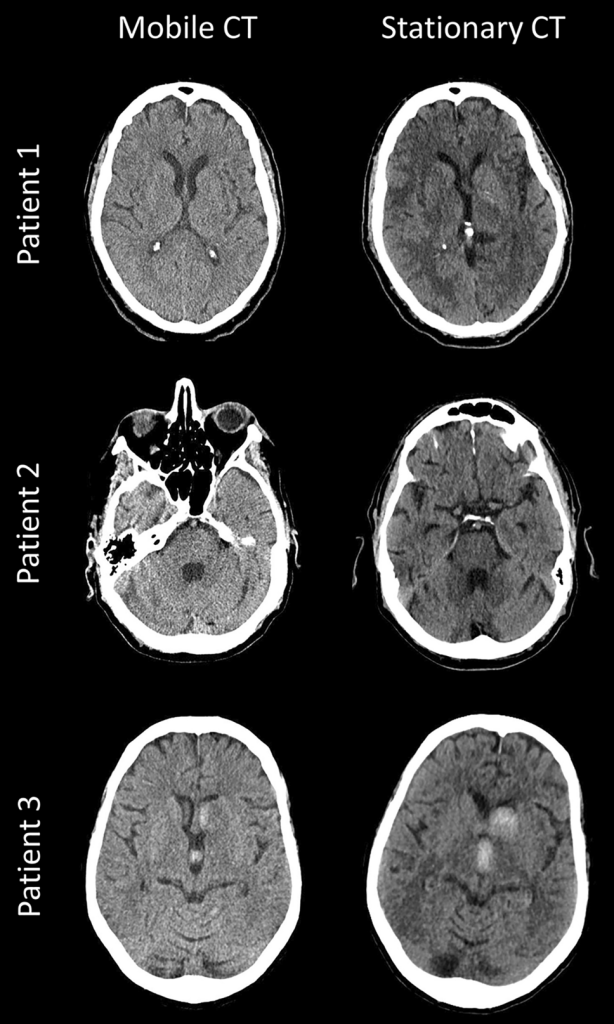
- This is a medical imaging technique in which multiple imaging of brain parts is taken.
- CT scan is mainly used to assess if there is haemorrhage, cyst, oedema, infraction, brain atrophy in the brain.
5) MRI (Magnetic resonance imaging)
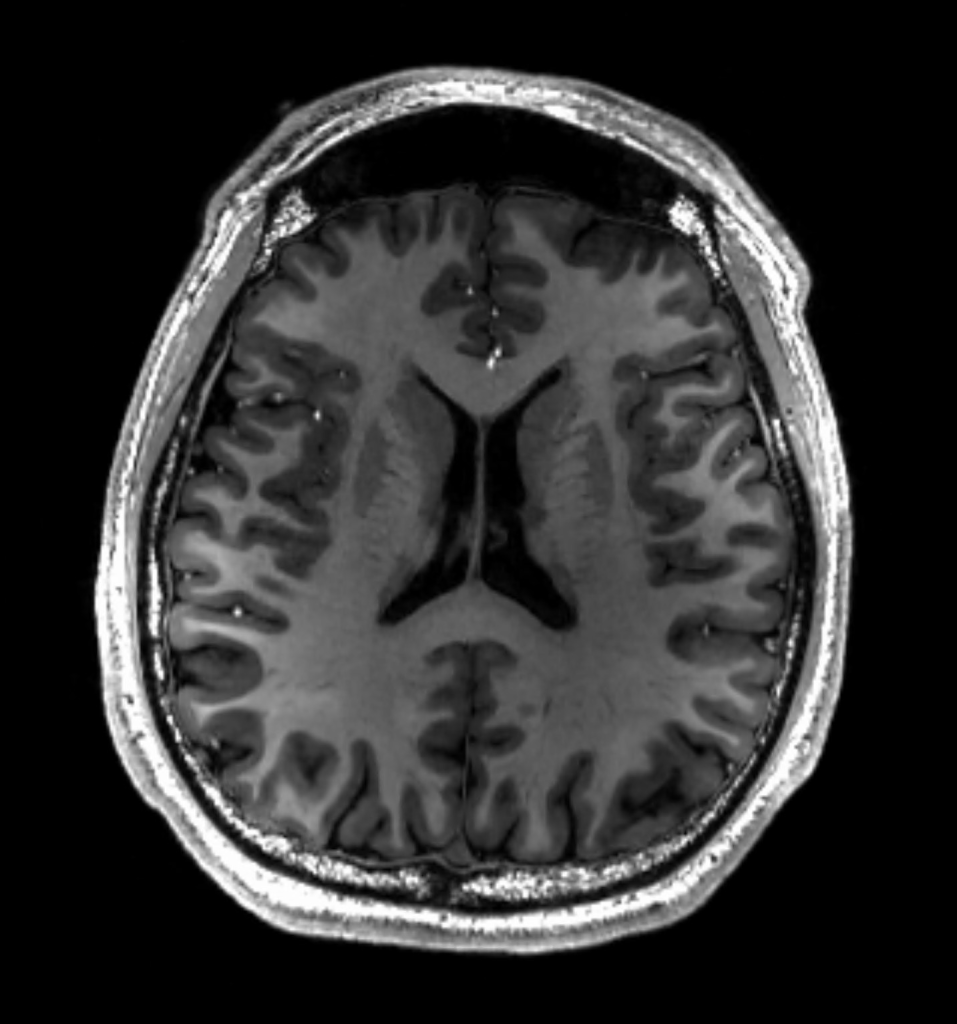
- MRI Scan is a medical imaging technique that uses radiology to detect any changes in the anatomy and physiology of the body.
- MRI uses a strong magnetic field, magnetic field gradient, and radiowaves to take images of the body.
- MRI is mainly used to detect stroke, multiple sclerosis, tumors, trauma, herniation, and seizures.
6) Magnetic Resonance Angiography :=
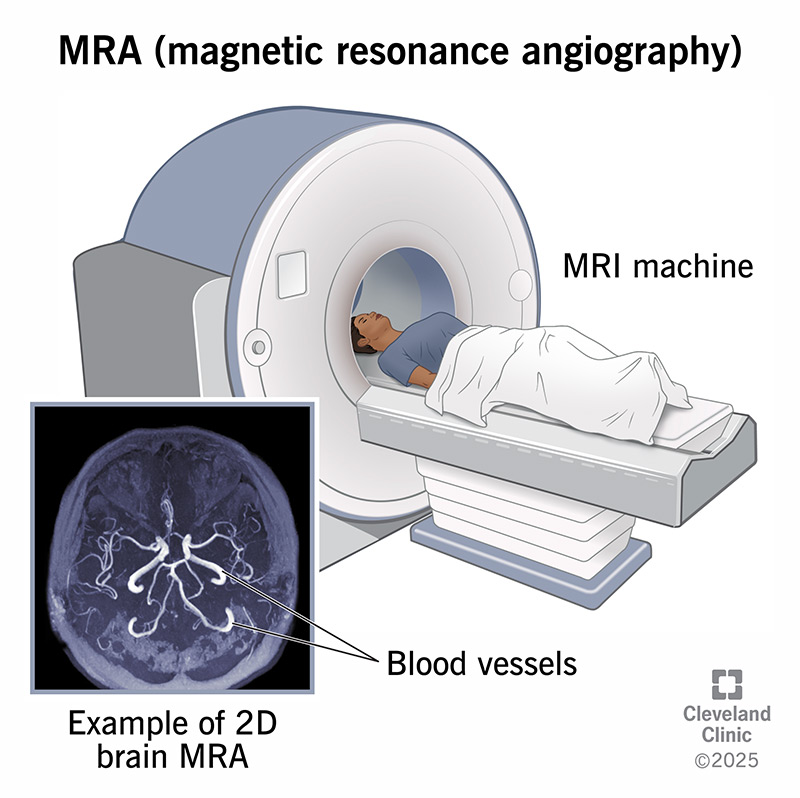
- This is a type of MRI procedure that is used to assess abnormalities of blood vessels.
- Magnetic Resonance Angiography is a less invasive procedure.
7) Magnetic Resonance Spectroscopy:=
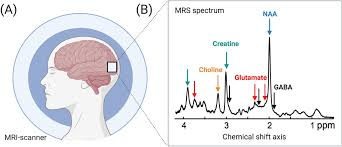
- Nuclear Magnetic Resonance Spectroscopy is a non-invasive ionizing radiation technique.
It is mainly used to assess changes in the brain. - It is mainly used to assess stroke, Alzheimer’s disease, seizure, sclerosis and other diseases. Used to do.
8) Myelography:=
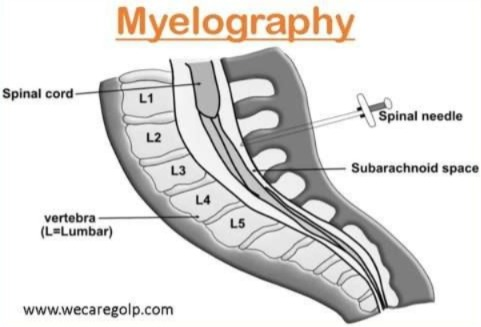
- Myelography is an imaging examination that involves inserting a spinal needle into the spinal canal and injecting a contractile medium around the spinal cord to detect any spinal lesions.
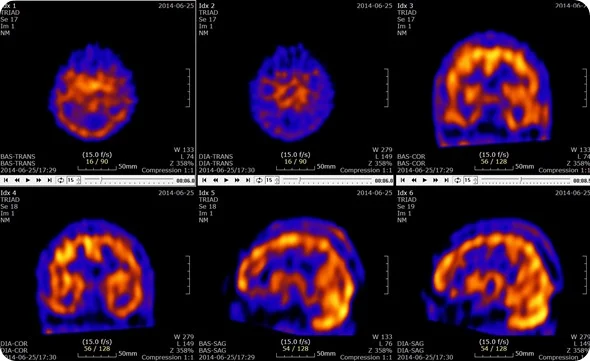
9) PET (Positron Emission Tomography)
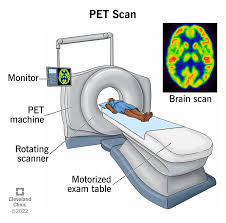
- This is an imaging study that uses radioactive materials to detect injury and damage to brain tissues.
- PET is mainly used to assess Parkinsonism, Tumors, Alzheimer’s and Seizures.
10) Single Photon Emission Computed Tomography ( SPECT )
- This test is mainly used to analyze the function of internal organs.
- This is a type of nuclear imaging in which a radioactive substance and a special camera are mainly used and a 3D picture is created and any abnormalities are detected.
11) EEG (Electroencephalogram)
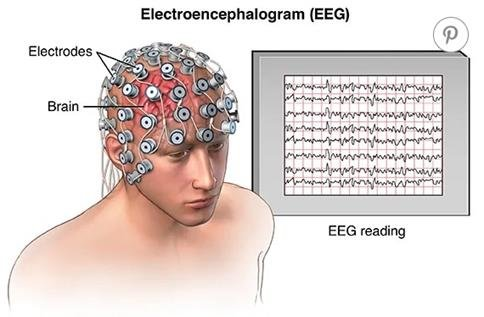
- EEG mainly involves placing electrodes and assessing the electrical activity of the brain.
- EEG mainly involves placing electrodes on the scalp Electrodes are placed and any abnormalities in the electrical activity of the brain are assessed. It is mainly used to assess seizures, CNS effects and brain death.
