ENGLISH-FON-GNM UNIT-2 NURSING PROCESS (Part : 3)

- The word nursing process was introduced by HALL in 1955. He gave 3 steps of nursing process: Observation, Administration of Care and Validation
- In 1961, Ida Jean Orlando gave 3 steps: Patient Behavior, Nurse Reaction, Nurse Action.
- In 1967, Lois Knowles discovered 5D: Discover, Develop, Decide, Do, Discriminate
- Then in 1973, Helen Yura and Mary Walsh gave the steps of nursing process: Assessing, Planning, Implementing and Evaluating.
- Then in 1991, the latest step of nursing process was given by the American Nurses Association, Nursing Diagnosis.
- The nursing process is a modified form of the scientific method used in the nursing profession. In which the patient’s needs and problems are identified, then related actions are taken and the patient’s problem is solved.
- The nursing process is a set of actions that are used to determine, plan, implement, and evaluate nursing care.
- The nursing process is a systematic problem-solving approach to providing comprehensive nursing care to individuals.
- The nursing process is a systematic method for assessing health status, diagnosing health problems, formulating a care plan, implementing the plan, and evaluating the effectiveness of the plan.
Write purpose of nursing process
- To identify the patient’s health status.
- To identify the patient’s needs.
- To identify the patient’s actual and potential problems.
- To identify nursing priorities.
- To restore, maintain, and promote the patient’s health.
- To provide specific nursing care and interventions.
- To evaluate the effectiveness of the nursing care provided.
Write characteristics of nursing process
- Nursing process is a kind of framework that helps nurses provide nursing care to individuals, families and communities.
- Nursing process is an interactive purposeful and systemic organization.
- Nursing process is universally applicable: that is, the nursing process is found everywhere and is applied everywhere.
- Nursing process is a dynamic and cyclical process: that is, the steps in the nursing process are interrelated, that is, they are related to each other. In which all the steps are followed one after the other. None of them can be skipped.
- Nursing process is patient-centered: that is, in the nursing process, the problem or need is identified and solved by keeping the patient in mind.
- The nursing process is goal-directed: that is, a goal is set in the nursing process and activities are performed to achieve that goal.
- The nursing process is outcome-oriented: that is, the outcome of the goal set during the nursing process is taken as to whether it is achieved or not, and how effective the interventions made to achieve this goal were is also evaluated.
- The nursing process is open and flexible: that is, information is collected through communication in the nursing process and nursing care is provided keeping in mind the nature, feelings, emotions, beliefs and values of the client.
- The nursing process can be used throughout life.
Write benefits of nursing process

- Nursing process is an orderly and systematic method for providing care.
- Nursing process is useful for providing comprehensive care to the patient.
- Nursing process helps in improving the quality of care.
- Nursing process is useful in solving and preventing the patient’s needs as well as current and potential problems.
- Nursing process is a type of legal document.
- Nursing process helps in providing continuity of care.
- In addition, nursing process also prevents duplication and omission.
- Nursing process is useful in making communication between nurses and other health care personnel effective.
Write steps of nursing process
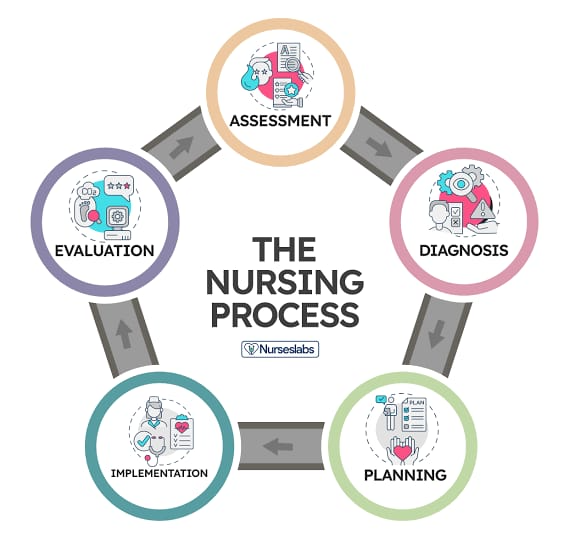
1) Assessment
2) Nursing diagnosis
3) Planning
4) Implemention
5) Evaluation
1) Assessment

- Assessment is the first step in the nursing process in which information or data about the patient is collected, organized, and analyzed. In which the patient’s physical, emotional, psychological, and sociocultural data are collected through observation, interview, and physical examination.
2) Nursing diagnosis

- Nursing diagnosis is the second step of the nursing process. In which the actual or potential problem of the patient is identified through assessment and a nursing diagnosis is made. Then, care is provided keeping this in mind.
3) Planning
- In this phase, we plan the activities or interventions we are going to do. We also set specific, measurable, achievable, and relevant goals and make a plan to achieve these goals.
4) Implemention

- In this phase, planned activities and interventions are implemented, i.e., they are brought into action mode. In which many types of care are provided, such as direct care, administering medicine, and providing education.
5) Evaluation

- Evaluation is the last step of the nursing process. In which the effectiveness of nursing interventions is assessed, that is, how effective the nursing care provided is is checked. Also, it is checked whether the set goals are fulfilled or not.
Assessment

- Assessment is the first step of the nursing process. In which the nurse systematically collects, organizes, verifies, analyzes, and documents patient data.
- Assessment is the collection and interpretation of clinical information.
- Assessment is an important step of the nursing process because the health status of the patient can be known due to assessment.
- During this step, the nurse collects data about the physiological, psychological, sociological, and spiritual status of the patient.
- This data can be collected through various techniques such as observation, interview, collection, and physical examination.
Purpose of assessment
- To establish a patient’s baseline information
- To obtain information about the patient’s health status
- To determine the patient’s normal function
- To identify the patient’s strengths
- To organize the information collected
- To provide a frame for nursing diagnosis
Types of assesment
1) Initial assessment
- Initial means initial. That is, the assessment done at the beginning. That is, in the initial assessment, the assessment is done within a certain period of time after admission to the health care agency. This is a type of comprehensive assessment in which the patient’s base line data and health history are collected in detail and a physical examination of the patient is also done.
2) Focus assessment:
- Focus assessment focuses on a specific problem. Focus assessment focuses on an already identified problem and collects related data. Focus assessment is done in depth than the initial assessment but is limited to a particular area. Therefore, focus assessment is performed to evaluate a specific problem or complaint. For example, performing the Glass Go Coma Scale in a case of head injury and performing a neurological examination.
3) Emergency assessment:
- Emergency assessment is conducted in an urgent or life-threatening situation. Critical issues can be identified and managed with the help of emergency assessment. For example, ABC assessment in an emergency condition. A – Airway, B – Breathing, C – Circulation.
4) Time lapsed assessment
- This assessment is done a few weeks or even months after the initial assessment. With the help of which the client’s current status is compared with the past base line data. So that the improvement in the patient’s health can be known. For example, when the patient comes for follow-up, his assessment is done.
5) Ongoing / shift assessment
- Ongoing assessment is performed at regular intervals during the patient’s care. In which the patient’s condition is continuously monitored and evaluated. For example, continuous vital sign monitoring.
Write down components of assessment
1) Collect data
2) Organize data
3) Validate data
4) Record / Document data
- 1) Collect data
- Data collection is the first step for assessment. In data collection, information is collected about the health status of the patient. This information is collected on the basis of history collection, interview, physical examination, laboratory data, diagnostic tests. In this data, from the patient’s chief complaint to past history is also collected.
- 2) Organize data
- Organize means to arrange. In this, the collected data is arranged, that is, the collected data is organized according to a framework. There are many types of frameworks to organize data. Mostly, different frameworks are seen in every nursing institute. That is, each institute follows its own framework. Due to this framework, omissions can be prevented.
- 3) Validate data
- Validation means cross-checking the collected data. In this step, the data collected is cross-verified whether it is correct or not, i.e. the accuracy of the collected data is checked. So that false diagnosis can be prevented.
- 4) Record / Document data
- Documentation or recording is a very important step. Therefore, to complete the assessment step of the nursing process, it is necessary to document that data. This documentation is done as per the hospital policy. In which the subjective data of the patient is written in his own words while the objective data is written in medical terms. This assessment is a form of documentation that can be used in future medico-legal cases.
Types of data
There are mainly two types of data:
1) Subjective data
2) Objective data
Subjective data

- Information provided verbally by the patient or their caregiver is known as ‘subjective data’.
- This includes symptoms, sensations, feelings, and perceptions.
- Subjective data relies on the patient’s interpretation because it cannot be measured or verified.
- For example, a patient’s feeling of pain is a type of symptom because it is reported by the patient and cannot be measured or observed.
Objective data

- Data that is obtained by direct observation by a health care worker is called ‘objective data’.
- Also known as ‘signs’.
- This data can be obtained through a physical examination, laboratory tests, or diagnostic procedures.
- Objective data is factual and can be verified.
- For example, elevated temperature, vomiting, which are signs. (If the patient says that he feels like he has a fever, we can measure the temperature with the help of a thermometer and observe it, and also measure the pulse, blood pressure.
two types of data based on its source) :
1) Primary data
2) Secondary data
- Primary data
- Information or data that is collected directly from a first-hand source (i.e., the patient or their caregiver) is known as primary data. Primary data can be collected through interviews, surveys, or experiments.
- Secondary data
- Data obtained from existing sources is known as secondary data. Such as data obtained from medical records, reports, literature, reviews, and databases.
Nursing diagnosis
- Nursing diagnosis is the second step in the nursing process. In which the nurse interprets the collected data using critical thinking and identifies the problem.
- Diagnosis is the clinical act of identifying the problem.
- Nursing diagnosis is the clinical judgment of the actual and potential health response of the individual, family, and community.
- Nursing diagnosis is the reasoning process or clinical act of identifying the problem.
- Nursing diagnosis provides a link between assessment and planning.
- A list of nursing diagnoses has been provided by the North American Nursing Diagnosis Association (NANDA), and all places use this NANDA nursing diagnosis.
Write purpose of nursing diagnosis
- To identify the client’s health status and actual and potential problems.
- To identify nursing priorities.
- To analyze the collected data.
- To provide direction for planning nursing interventions.
- To identify the client’s normal level of function.
Write down statment of nursing diagnosis
- Problem / Diagnostic label
- In nursing diagnosis, the patient’s actual or potential problem or diagnostic label is first written. This problem is written in a few words. This nursing diagnosis is taken from the list given by NANDA (North American Nursing Diagnosis Association). For example: Knowledge deficit, Anxiety, Ineffective airway clearance, Fluid volume deficit
- Etiology
- Etiology is the second statement of a nursing diagnosis. In which one or more causes of the problem are identified and written. Etiology gives directions for treating the problem. A problem can be seen in two patients, but it is not necessary that the etiology of both patients is the same. This problem and etiology are written with ‘related to’. For example, Anxiety related to hospitalization, Anxiety related disease condition. In which Anxiety is a problem or diagnostic label that is the same in all patients. Also, hospitalization and disease condition are the etiology that are different in all patients.
- Defining characteristic
- Defining characteristic shows how the problem in the patient is identified. Which can be subjective or objective data. This defining characteristic is written as ‘as evidenced by’ or ‘manifested’. For example, Altered body temperature related to inflammatory condition as evidenced by increasing body temperature, Acute pain related to surgical process manifestd by facial expression.
Write types of nursing diagnosis
1) Actual nursing diagnosis
2) Risk nursing diagnosis
3) Syndrome nursing diagnosis
4) Wellness diagnosis
- 1) Actual nursing diagnosis
- Actual nursing diagnosis includes current health problem or existing health problem. Which is present during the assessment and many characteristics are seen in it, i.e. many signs and symptoms are seen. Such as anxiety is characterized by fear, panic, sleep disturbance and ineffective airway clearance is characterized by cough, abnormal breathing. For example, Acute pain related to surgery, Anxiety related to hospitalization, Ineffective breathing pattern.
- 2) Risk nursing diagnosis
- Risk nursing diagnosis includes potential problem i.e. the problem that is seen due to actual (current) problem is included in risk nursing diagnosis. That is, the problem is not present now but may appear in the future. For example, Risk for infection related to immunospression, Risk for impaired skin integrity related to surgery
- 3) Syndrome nursing diagnosis
- Syndrome means a group of symptoms i.e. cluster of symptoms. In a syndrome nursing diagnosis, a cluster of current nursing diagnoses as well as high risk nursing diagnoses is seen i.e. more than one nursing diagnosis is seen and these nursing diagnoses are seen together and are addressed together. In addition, it requires similar i.e. the same intervention. For example, post-trauma syndrome, relocation stress syndrome, rape trauma syndrome
- 4) Wellness diagnosis
- A wellness diagnosis indicates how a person, family, or community can achieve a higher level of wellness. In which the Readiness for enhanced format is mainly used. For example, Readiness for enhanced family coping, Readiness for enhanced spiritual well being, Readiness for enhanced self-esteem.
- Write difference between nursing diagnosis and medical diagnosis
- Nursing diagnosis
- Nursing diagnosis identifies the patient’s needs as well as actual and potential problems.
- Nursing diagnosis is made by focusing on care. That is, nursing diagnosis identifies human responses.
- Nursing diagnosis identifies the patient’s risk factors and problems.
- Nursing diagnosis focuses on the signs and symptoms of a disease condition.
- Nursing diagnosis treats the problems caused by a disease condition.
- Nursing diagnosis can be for the patient as well as his family members and caregivers.
- For example, ineffective airway clearance
- Medical diagnosis
- In medical diagnosis, a disease condition is identified based on physical signs, symptoms, and diagnostic tests.
- Medical diagnosis is made by focusing on etiology. That is, medical diagnosis focuses on identifying the disease.
- In medical diagnosis, the specific cause of illness is identified.
- In medical diagnosis, the focus is on the pathology of the disease condition.
- In medical diagnosis, the disease condition is treated directly by a physician.
- Medical diagnosis is seen only for the patient.
- For example, pneumonia
List out nursing diagnosis
✓ Health promotion
Class 1 : Health awareness
- Decreased diversional activity engagement
- Readiness for enhanced health literacy
- Sedentary lifestyle
Class 2 : Health management
- Risk for elopement attempt
- Frail elderly syndrome
- Risk for frail elderly syndrome
- Readiness for enhanced exercise management
- Deficient community health
- Risk – prone health behaviour
- Ineffective health maintenance behaviours
- Ineffective health self management
- Readiness for enhanced health self management
- Ineffective family health self management
- Ineffective home maintenance behaviours
- Risk for home maintenance behaviours
- Readiness for enhanced home maintenance behaviours ineffective protection
✓ Nutrition
Class 1 : Ingestion
- Imbalance nutrition less than body requirement
- Readiness for enhanced nutrition
- Insufficient breast milk production
- Ineffective breast feeding
- Interrupted breast feeding
- Readiness for enhanced breast feeding
- Ineffective adolescent eating dynamics
- Ineffective child eating dynamics
- Ineffective infant feeding dynamics
- Obesity
- Overweight
- Risk for overweight
- Ineffective infant suck swallow response
Class 2 : Digestion
This class does not currently contains any diagnosis
Class 3 : Absorption
This class does not currently contains any diagnosis
Class 4 : Metabolism
- Risk for unstable blood glucose level
- Neonatal hyperbilirubinemia
- Risk for neonatal hyperbilirubinemia
- Risk for impaired liver function
- Risk for metabolic syndrome
Class 5 : Hydration
- Risk for electrolyte imbalance
- Risk for imbalance fluid volume
- Deficient fluid volume
- Risk for deficient fluid volume
- Excess fluid volume
✓ Elimination and exchange
Class 1 : Urinary function
- Disability associated with urinary incontinence
- Impaired urinary elimination
- Mixed urinary incontinence
- Strees urinary incontinence
- Urge urinary incontinence
- Risk for urge urinary incontinence
- Urinary retention
- Risk for urinary retention
Class 2 : Gastrointestinal function
- Constipation
- Risk for constipation
- Perceived constipation
- Chronic functional constipation
- Risk for chronic functional constipation
- Impaired bowel continence
- Diarrhea
- Dysfunctional gastrointestinal motility
- Risk for dysfunctional gastrointestinal motility
Class 3 : Integumentary function
This class does not currently contains any diagnosis
Class 4 : Respiratory function
- Impaired gas exchange
✓ Activity / Rest
Class 1 : Sleep / Rest
- Insomnia
- Sleep deprivation
- Readiness for enhanced sleep
- Disturbed sleep pattern
Class 2 : Activity / Exercise
- Decreased activity intolerance
- Risk for decrease activity intolerance
- Risk for disuse syndrome
- Impaired bed mobility
- Impaired physical mobility
- Impaired wheel chair
- Impaired sitting
- Impaired standing
- Impaired walking
- Impaired transfer ability
Class 3 : Energy balance
- Imbalance energy field
- Fatigue
- Wandering
Class 4 : Cardio vascular and pulmonary response
- Ineffective breathing pattern
- Decreased cardiac output
- Risk for decreased cardiac output
- Risk for impaired cardiovascular function
- Ineffective lymphedema self management
- Risk for ineffective lymphedema self management
- Impaired spontaneous ventilation
- Risk for unstable blood pressure
- Risk for thrombosis
- Risk for decrease cardiac tissue perfusion
- Risk for ineffective cerebral tissue perfusion
- Ineffective peripheral tissue perfusion
- Risk for ineffective peripheral tissue perfusion
- Dysfunctional ventilatory process
- Dysfunctional adult ventilatory weaning response
Class 5 : Self care
- Bathing self care deficit
- Dressing self care deficit
- Feeding self care deficit
- Toileting self care deficit
- Readiness for enhanced self care
- Self neglect
✓ Self perception
Class 1 : Self concept
- Hopelessness
- Readiness for enhanced hope
- Risk for compromised human dignity
- Disturbed personal identity
- Risk for disturbed personal identity
- Readiness for enhanced self concept
Class 2 : Self esteem
- Chronic low self esteem
- Risk for chronic low self-esteem
- Situational low self-esteem
- Risk for situational low self-esteem
Class 3 : Body image
Disturbed body image
✓ Role relationship
Class 1 : Caregiving roles
- Impaired parenting
- Risk for impaired parenting
- Readiness for enhanced parenting
- Caregiver role strain
- Risk for caregiver role strain
Class 2 : family relationship
- Risk for impaired attachment
- Disturbed family identity syndrome
- Risk for disturbed family identity syndrome
- Dysfunctional family process
- Interrupted family process
- Readiness for enhanced family process
Class 3 : Role performance
- Ineffective relationship
- Risk for ineffective relationship
- Readiness for enhanced relationship
- Parental role conflicts
- Ineffective role performance
- Impaired social interaction
✓ Sexuality
Class 1 : Sexual identity
This class does not currently contains any diagnosis
Class 2 : Sexual function
- Sexual dysfunction
- Ineffective sexuality pattern
Class 3 : Reproduction
- Ineffective child bearing process
- Risk for ineffective child bearing process
- Readiness for enhanced child bearing process
- Risk for disturbed maternal fetal dyad
✓ Coping / stress tolerance
Class 1 : Post truma response
- Risk for complicated immigration transition
- Post truma syndrome
- Risk for post trauma syndrome
- Rape truma syndrome
- Relocation stress syndrome
- Risk for relocation stress syndrome
Class 2 : Coping responses
- Ineffective activity planning
- Risk for ineffective activity planning
- Anxiety
- Defensive coping
- Ineffective coping
- Readiness for enhanced copping
- Readiness for enhanced community coping
- Compromise family coping
- Disabled family coping
- Readiness for enhanced
family coping - Death anxiety
- Ineffective denial
- Fear
- Maladaptive grieving
- Risk for maladaptive grieving
- Readiness for enhanced grieving
- Impaired mood regulation
- Powerlessness
- Risk for powerlessness
- Readiness for enhanced power
- Impaired resilience
- Risk for impaired resilience
- Readiness for enhanced resilience
- Chronic sorrow
- Stress overload
Class 3 : Neuro behavioural stress
- Acute substance withdrawal syndrome
- Risk for acute substance withdrawal syndrome
- Autonomic dysreflexia
- Neonatal abstinence syndrome
- Disorganised infant behaviour
- Risk for disorganised infant behaviour
- Readiness for enhanced organized infant behaviour
✓ Life principles
Class 1 : Values
This class does not currently contains any diagnosis
Class 2 : Beliefs
Readiness for enhanced spiritual well being
Class 3 : Values / Action congruence
- Readiness for enhanced descision making
- Descisional conflict
- Impaired emancipated descision making
- Risk for impaired emancipated descision making
- Readiness for enhanced emancipated descision making
- Moral distress
- Impaired religiosity
- Readiness for enhanced religiosity
- Spiritual distress
- Risk for spiritual distress
✓ Safety / protection
Class 1 : Infection
- Risk for infection
- Risk for surgical site infection
Class 2 : Physical injury
- Ineffective airway clearance
- Risk for aspiration
- Risk for bleeding
- Impaired dentition
- Risk for dry eye
- Ineffective dry eye self management
- Risk for dry mouth
- Risk for adult falls
- Risk for child falls
- Risk for injury
- Risk for corneal injury
- Nipples areolar complex injury
- Risk for nipples areolar complex injury
- Risk for urinary tract injury
- Impaired oral mucus membrane integrity
- Risk for impaired oral mucus membrane integrity
- Risk for peripheral neurovascular dysfunction
- Risk for physical truma
- Risk for vascular truma
- Adult pressure injury
- Risk for adult pressure injury
- Child pressure injury
- Risk for child pressure injury
- Neonatal pressure injury
- Risk for neonatal pressure injury
- Risk for shock
- Impaired skin integrity
- Risk for impaired skin integrity
- Risk for sudden infant death
- Risk for suffocation
- Delayed surgical recovery
- Risk for delayed surgical recovery
- Impaired tissue integrity
- Risk for impaired tissue integrity
Class 3 : Violence
- Risk for female genital mutilation
- Risk for other-directed violence
- Risk for self directed violence
- Self mutilation
- Risk for self mutilation
- Risk for suicidal behaviour
Class 4 : Environmental hazards
- Contamination
- Risk for contamination
- Risk for occupational injury
- Risk for poisoning
Class 5 : Defensive processes
- Risk for adverse reaction to iodinated contrast media
- Risk for allergic reaction
- Risk for lattex allergic reaction
Class 6 : Thermoregulation
- Hyperthermia
- Hypothermia
- Risk for hypothermia
- Neonatal hypothermia
- Risk for neonatal hypothermia
- Risk for perioprative hypothermia
- Ineffective thermoregulation
- Risk for ineffective thermoregulation
✓ Comfort
Class 1 : Physical comfort
- Impaired comfort
- Readiness for enhanced comfort
- Nausea
- Acute pain
- Chronic pain
- Chronic pain syndrome
- Labor pain
Class 2 : Environmental comfort
- Impaired comfort
- Readiness for enhanced comfort
Class 3 : Social comfort
- Impaired comfort
- Readiness for enhanced comfort
- Risk for loneliness
- Social isolation
✓ Growth / Development
Class 1 : Growth
This class does not currently contains any diagnosis
Class 2 : Development
- Delayed child development
- Risk for delayed child development
- Delayed infant motor development
- Risk for delayed infant motor development
Planning

- Planning is the third step of the nursing process. In which the entire framework of what activities are to be done is created. That is, in this framework, what activities are to be done, when to do them, where to do them, how to do them, who will do these activities, etc. are planned.
- Planning is a kind of selected and carried out action series to achieve a goal.
- Planning is a planned careframe for providing nursing care.
- Purpose of planning
- To give direction to client care activities.
- To reduce uncertainty
- To enhance continuity of care.
- To minimize impulsive and arbitrary decisions
- Write down types of planning
- There are mainly 3 types of planning:
- 1) Initial planning
- 2) Ongoing planning
- 3) Discharge planning
- 1) Initial planning
- Initial planning is the initial planning. Initial planning is done immediately after the initial assessment. This planning is done immediately after the assessment so that the length of stay in the hospital can be reduced. Initial planning is done by the nurse who does the admission assessment.
- 2) Ongoing planning
- Ongoing planning is done for continuous updating of the planned care of the patient. Ongoing planning is done by all the nurses who provide care to the patient. In which daily planning is carried out using the ongoing assessment.
- 3) Discharge planning
- Discharge planning is the planning of the patient after discharge, keeping in mind the patient’s needs. This is a curricular part of comprehensive health care.
Write down elements of planning
1) Prioritizing nursing diagnosis
2) Determining goal and expected outcomes
3) Select nursing
interventions
4) Developing nursing care plan
- 1) Prioritizing nursing diagnosis
- While planning, first prioritize the nursing diagnosis. That is, give first priority to the nursing diagnosis that requires immediate care. This priority is set according to Maslow’s hierarchy of needs. Give first priority to ineffective airway clearance. Give lower priority to nursing diagnoses like knowledge deficit.
- 2) Determining goal and expected outcomes
- After setting the priority of the nursing diagnosis, determine the goal of that diagnosis and determine the expected outcome. So that we know whether the nursing care provided is going in the right way or not. For example, set a goal like eliminating breathing difficulty in a patient with breathing difficulty.
- 3) Select nursing interventions
- After determining the goals and expected outcomes, select specific interventions according to the nursing diagnosis. So that the set goals can be achieved. For example, provide Fowler’s position in a patient with breathing difficulties, provide oxygen supplementation if necessary.
- 4) Developing nursing care plan
- After setting the priority of the nursing diagnosis, determining the goals and expected outcomes, and selecting specific nursing interventions, develop a nursing care plan. Which provides a framework for providing nursing care.
- Goal and expected outcome
- A goal is a statement of the expected outcome of a nursing intervention.
- A goal is a specific, measurable, achievable, relevant, and time-bound objective.
- It helps provide direction, motivation, and focus.
- Write down purpose of goal
- To evaluate the effectiveness of a nursing intervention
- To evaluate the client’s progress
- To evaluate whether changes are needed in a nursing intervention
- Write down types of goal
- There are mainly two types of goals:
- 1) Short term goal
- 2) Long term goal
- 1) Short term goal
- Short term goal is determined for a short time duration. Short term goal is to be achieved within a week. Short term goal is mainly set for immediate nursing care. For example, if a patient has breathing problem, then your short term goal is to relieve the patient from breathing difficulty.
- 2) Long term goal
- Long term goal is determined for a long duration. Long term goal is to be achieved from a week to a month. Long term goal is also applied after discharge. Such as the patient not getting any kind of infection after discharge.
- Expected outcome
- Expected outcome is a type of prediction. Which predicts the result of the action taken.
- The prediction of what kind of changes are seen in the health of the patient after providing nursing care is known as expected outcome.
- Write down principles for formulating the outcome
- The expected outcome should be patient centered.
- The expected outcome should be problem oriented.
- The expected outcome should be measurable and observable.
- The expected outcome should be clear and concise.
- Expected outcome should be time limited.
- Expected outcome should be realistic.
Implementation

- Implementation is the fourth step of the nursing process.
- In implementation, planned activities are converted into action.
- In implementation, planned activities and procedures are performed and documented.
- A nursing intervention is a type of action that is performed by a nurse to bring a patient out of the current health status and to achieve the expected outcome.
Write down purpose of implementation

- To provide therapeutic nursing care
- To provide technical nursing care
- To help the patient achieve optimal health
- Write activities of implementation
- Reassess the patient:
- The patient’s condition can change at any time, so reassess the patient’s condition even after interaction with the patient.
- Set priority:
- Priority also changes as the patient’s condition changes. Therefore, set priorities based on the reassessment and then implement nursing interventions.
- Organize resources:
- Arrange the equipment, articles, environment and health care personnel required to provide nursing care.
- Perform nursing interventions:
- Implement the planned nursing interventions according to the patient’s priorities.
- Documentation:
- Document everything in the patient’s health record as soon as possible after implementing the plan. Record it as per the institution’s policy.
- Write nursing skill required during implementation
- To successfully implement the nursing care plan, the nurse must have the following skills:
- Cognitive skill:
- The nurse must have cognitive skills to identify the patient’s needs and anticipate nursing knowledge. Cognitive skills include skills such as problem solving, decision making, and teaching.
- Interpersonal skills:
- A nurse needs to have the skills to develop interpersonal and intrapersonal relationships because she also needs other health care personnel to achieve goals. Apart from this, she also needs to have good communication skills.
- Technical skills:
- A nurse needs to have technical skills to perform procedures and use equipment and machines such as administering injections, calculating doses, and handling machines such as ventilators, phototherapy machines, infusion pumps, etc.
- Psychomotor skill:
- While providing nursing care, nurses need to have integration between cognitive and motor activities. For example, when giving intramuscular injections, nurses need to have knowledge of anatomy and physiology as well as the motor skills to administer the injection.
Evaluation

- Evaluation is the last or fifth step of the nursing process.
- Evaluation is a process in which the patient’s progress towards the expected outcome and the effectiveness of nursing care are determined.
- Evaluation is a type of judgment that judges how effective nursing was in achieving the set goals.
- This step determines the effectiveness and success of the entire nursing process.
- Evaluation also helps in making decisions about whether to continue, modify, or repeat the process.
- When documenting the evaluation phase, any one of the following three possible conclusions is written.
- The goal was met (This sentence is written when both goals have been achieved and the desired outcome is observed.)
- The goal was partially met (This sentence is written when the short-term goal has been achieved but the long-term goal has not been achieved)
Write purpose of evaluation
- To check effectiveness
- To monitor implementation
- To monitor the quality of nursing care
- To bring about improvements in the care plan
- To identify errors in the care plan
- To assess the collaboration of the client and health care team members
- To improve decision-making
Write activities during evaluation phase

- Review of Patient Goals and Outcome Criteria
- Data Collection
- Goal Measurement
- Documentation
- Revision and Modification of Nursing Care Plan