ENGLISH-ENT-EAR-DISORDER-PART-3
ENT-PART-3
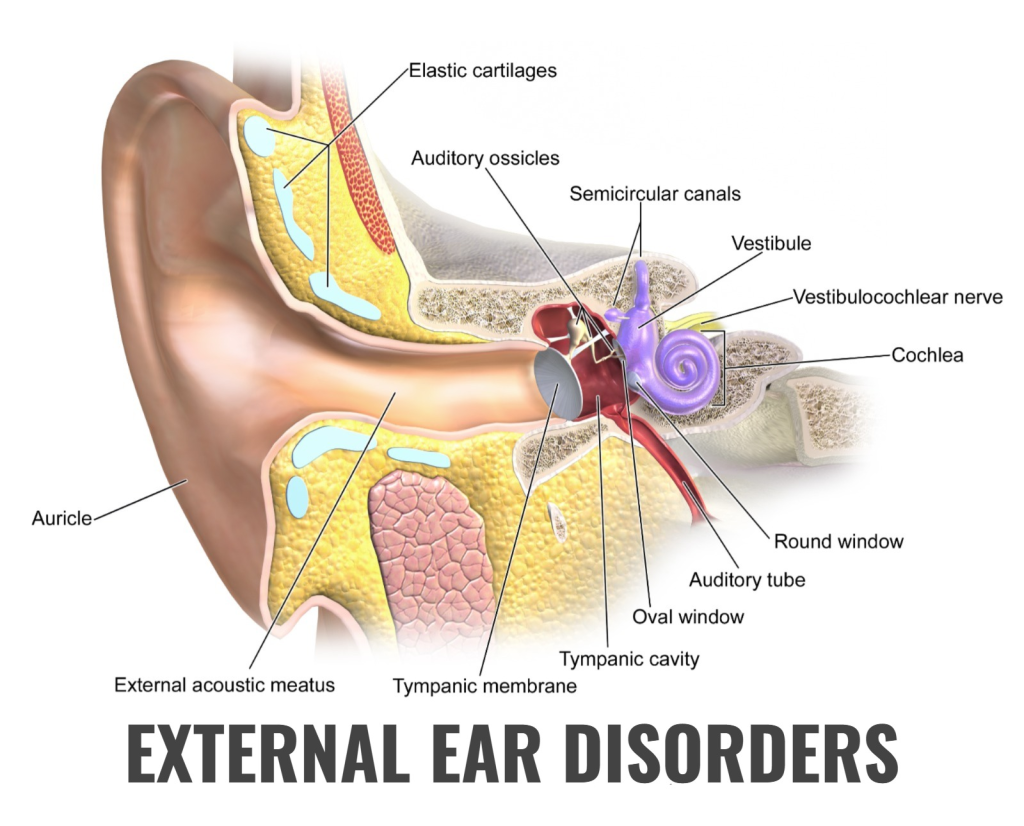
EXTERNAL EAR DISORDERS
👂OTITIS-EXTERNA ( Otitis externa)
🧡 DEFINE OTITIS-EXTERNA (Define Otitis Externa)
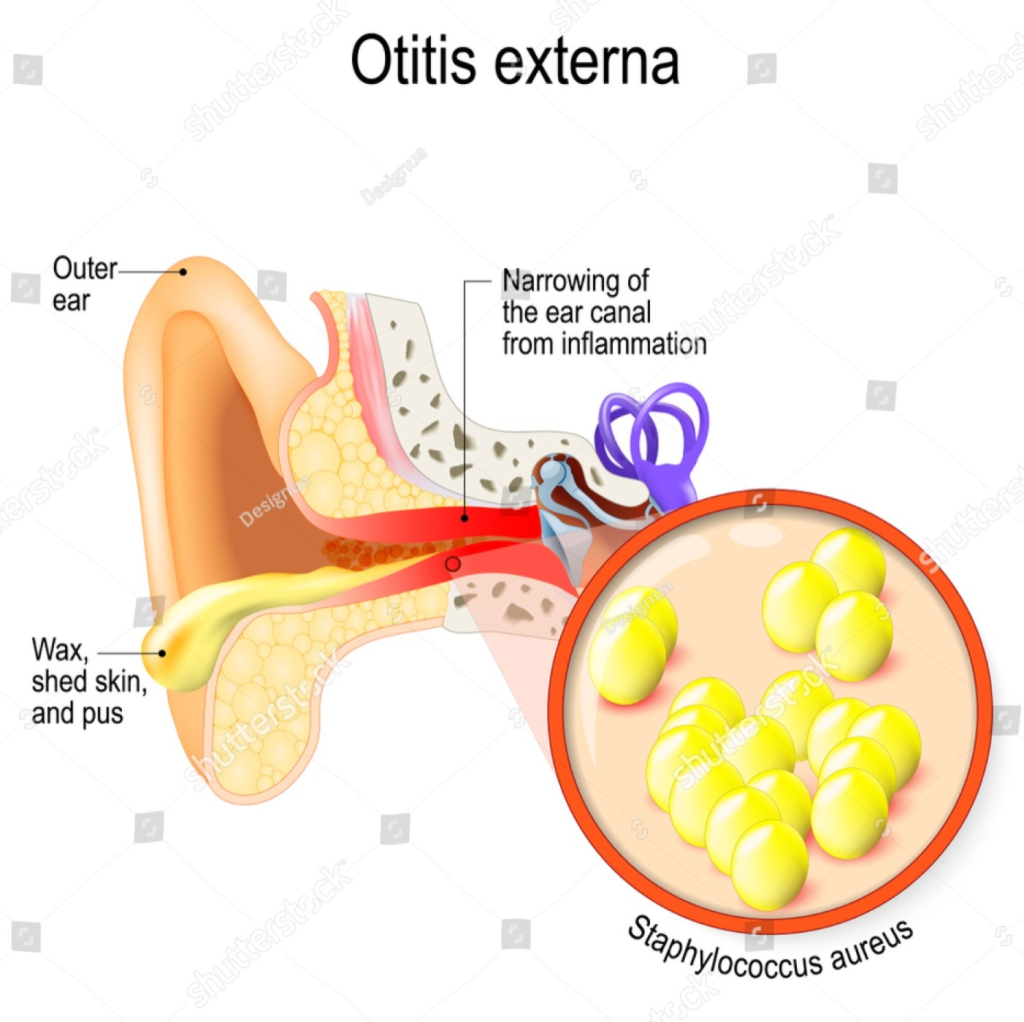
► Otitis externa is an infection and inflammation of the external Ear ( Ear lobe, external auditory canal ,Ear ).
► Otitis externa is also called swimmer’s ear( 🏊♀️ swimmers 👂 ear) . Because It is more common after swimming due to water getting into the ears, and otitis externa is more common in the summer than in the winter. (more common in summer than winter).
► It involves inflammation of the skin lining of the external auditory canal.
► It can be acute or chronic (Acute:= for a short time, chronic:= for a long time).
🧡 WRITE CAUSES OR ETIOLOGY OF OTITIS EXTERNA (Write the causes or etiology of Otitis Externa)
Water in the ear after swimming.
Any trauma to the external ear.
Bacterial infections such as Pseudomonas species,
Gram negative rods,
It is caused by Staphylococcus species (staphylococcus species).
Fungal infections such as Aspergillus species,
Candida species.
eczematous dermatitis.
Any skin infection of the face, neck or scalp.
Middle ear infection or inflammation Yes.
🧡 RISK FACTORS FOR OTITIS EXTERNA (Risk factors for Otitis Externa)
- Excessive Moisture: Prolonged exposure to water or moisture in the ear can create a favorable environment for the growth of bacteria or fungi. That is why otitis externa is often referred to as swimmer’s ear.
- Trauma to the Ear Canal: Scratching with objects such as cotton swabs or hairpins can damage the delicate SKIN, which becomes a PORTAL OF ENTRY for infection.
- Allergies: Allergic reactions can cause inflammation in the ear canal, making it more susceptible to infection.
- Immunosuppression: Conditions or medications that weaken the immune system, such as diabetes or certain medications, can increase the risk of infections, including otitis externa. Weakened immune system, such as diabetes or certain medications, can increase the risk of infections, including otitis externa.)
- Cuts or Abrasions: Any break in the skin of the ear canal, whether due to injury or irritation, can provide an entry point for bacteria or fungi.
- Swimming in Contaminated Water: Swimming in water that is contaminated with bacteria or fungi can introduce these microorganisms into the ear canal. a humid climate or regularly exposing the ears to high humidity can contribute to the development of otitis externa.
🧡 WRITE SIGN AND SYMPTOMS OF OTITIS EXTERNA (Write the signs and symptoms of otitis externa)
- Ear Pain (ear pain): One of the most common symptoms is pain, which can range from mild discomfort to severe, sharp pain. The pain is often exacerbated by movement of the outer ear or by pulling on the earlobe. (One of the most common symptoms is pain, which can range from mild discomfort to severe, sharp pain. The pain is often exacerbated by movement of the outer ear or by pulling on the earlobe.)
- Redness and Swelling : The ear canal may appear red and swollen, and the outer ear might be tender to the touch. The inflammation contributes to the discomfort associated with the condition. (itching)
- Swelling
- Watery discharge,
- Crusting, scaling,
- The skin becomes quite thick.
- The drainage from the ear is yellow, green, and foul-smelling.
- hearing loss occurs.
- fever.
🧡 WRITE DIAGNOSIS OF OTITIS EXTERNA (Write the diagnosis of otitis externa)
► History taking and physical examinationHistory taking and physical examination
► inspection of Ear-
► whisper test– whisper test
► otoscopic examination– otoscopic examination
🧡 WRITE MANAGEMENT OF OTITIS EXTERNA (Write Management of Otitis Externa)
★ Ear Cleaning/Irrigation: Ear irrigation is done to clean the external auditory canal and remove any debris, impacted wax, or foreign bodies.
★ Topical Medications: ► These include Antibiotics’ Ear drops Or corticosteroids are used to relieve ear inflammation. Ex:ciprofloxacin-dexamethasone,Neomycin,Hydrocortisone, Polymyxin B,etc
► Fungal infections are treated with topical antifungal agents such as nystatin.
► Topical corticosteroids creams or lotions are used.
★Pain Management : The patient’s pain is relieved by the use of painkillers. EX.NSAID-ACETAPHENOMEN
★ Prescription Medications : If the infection is severe, the doctor may prescribe oral antibiotics or antifungal medications.
★ Warm Compress: Applying a warm compress to the affected ear can help reduce pain and inflammation.
🧡 WRITE NURSING MANAGEMENT OF OTITIS EXTERNA (Write nursing management of otitis externa)
Assessment: ► Recent water exposure. ► Obtain a detailed medical history, including any ear injury or use of ear devices (headphones, hearing aids). ► Assess for signs and symptoms of otitis externa such as ear pain, itching, redness, swelling, discharge, and hearing loss. ► Assess the patient’s overall health, immune status, and any underlying conditions that may contribute to the infection. ► Apply any medicated ointments or powders to the patient for local treatment. ► Instill prescribed topical eardrops, which often contain antibiotics (e.g., neomycin, polymyxin B, hydrocortisone) ► Provide the patient with warm compresses.
► Apply cold applications to relieve inflammation and discomfort.
► Give the patient analgesics to relieve pain. Administering medications.
► Administer antibiotic medicine to the patient.
► Maintain aseptic technique to prevent any secondary infection.
Monitoring and Evaluation: Regularly assess the patient’s response to treatment, including changes in symptoms and signs of improvement. Monitor for any adverse drug reactions
- Advise the patient to take proper care and follow-up.
🧡 PREVENTION OF OTITIS EXTERNA (Prevention of Otitis Externa)
★ Avoid Irritants: Hair sprays, hair dyes and other chemicals that can worsen the condition Avoid contact with irritants that can cause irritation.
★ Keep the Ear Dry:
- Avoid swimming or submerging the affected ear in water until the infection has cleared.
- Use a water-resistant earplug or cotton ball coated with petroleum jelly when showering or bathing to prevent water from entering the ear.
- Tell the patient not to expose themselves to water.
- Tell the patient not to insert any instruments into the ear, such as cotton buds.
- Tell the patient not to allow any excessive accumulation of ear wax in the ear and to visit a doctor as per the proper procedure.
- If a patient has a previous ear infection or a hole in the ear drum or has had any type of ear surgery, consult a doctor before swimming or putting any other ear drops.
- Mineral Use oil Ear drops when there is any kind of dry crust in the ear to remove it.
- Do not put any kind of hair pins or ear buds in the ear.
- Get a proper ear examination by a doctor.
👂 FOREIGN BODY
Introduction
A foreign body in the ear is any small object that gets stuck in the ear. This is called a type of emergency. Foreign bodies accidentally get into the ear and the patient is not even aware of it.
► In adults (flies, mosquitoes, ants, cockroaches, etc. get into the ear), ► In children (chocolate, small pieces of any vegetable, beans, chewing gum, leaves, flowers, pieces of clothes, small toys, pencils erasers, etc. get into the ear of small children).
🧡 write clinical manifestation of foreign body in Ear ()
- Ear pain.
- Feeling uncomfortable in the ear.
- Tching in the ear.
- Vibrating sensation. in the ear.
- Reduced hearing in the affected ear.
- Suspected ear infection.
- Bleeding from the ear.
🧡 First aid (First Aid)
- Foreign objects cause pain in the ear and difficulty in hearing and if this object gets stuck in the ear, it causes a lot of damage but children are not aware of it.
- In this, when it seems that any foreign object has flowed into the ear, do not insert any kind of ear birds or hair pins into the ear, as doing so will cause the foreign body to flow further into the ear and it damages the middle ear.
- If any foreign body is visible outside, try to remove it slowly.
- Using the force of gravity means turning the affected ear towards that side and slowly Try to remove the foreign body.
- If any insect has flown into the ear, apply a little warm oil or olive oil so that if there is an insect, it comes out of the ear and if there is perforation in the ear drum, do not put oil in the ear and seek medical advice and go to the doctor.
🧡 Removal of foreign body (How to remove foreign body) )
- Removal of foreign bodies from the ear is very important in the emergency department.
- Before removing any foreign body, it should be killed with mineral oil or lidocaine (2%).
- Removal of foreign bodies includes mechanical extraction, irrigation, suction, and medication.
1)mechanical extraction:- (mechanical extraction)
- In this, the patient should be seated in a comfortable position.
- Repeatedly perform ear examination and check the depth of the foreign body.
- Then insert the lens of the otoscope and introduce the bayonet forceps from the other side.
- Insert the forceps slowly until the foreign body is grasped.
- Then, when the foreign body is grasped, remove the forceps slowly and take out the forceps slowly so as not to cause any injury to the auditory canal and ear drum.
- Check whether the foreign body has been completely removed or not.
- Also check whether there is any injury to the tympanic membrane.
2) Irrigation:-
- Irrigation is a simple method to remove any foreign body.
- Insert water slowly from the top or front of the ear.
- Ear irrigation is contraindicated for any soft object, organic matter, or seeds.
3)suctioning:-
- The tube is kept in contact with the foreign object and suction is done.
- Then any foreign object is caught by alligator forceps.
- Then the foreign object is removed.
- Thus, foreign objects are also removed by suction is.
Medication
There is no medicine for any foreign body, but if there is any kind of infection or abrasion, a combination of antibiotics and steroids is used.
Management
- Give Reassurance to the patient.
- Do not remove the foreign object with any sharp object as it can be ruptured by the panicked team member.
- If the foreign object is left inside the ear, lower the affected ear over the shoulder on that side and try to remove the foreign object slowly.
- War. Water And use fluid so that any insect floats and comes out.
- Put some oil inside the ear so that any insect floats and comes out.
- If it is difficult to get it out, consult a doctor.
- Do not put anything inside the ear such as earbud, hair pin, and any sharp objects in the ear.
- If the foreign body is visible from the outside, do not irrigate it because it will increase its size. It goes in and gets impacted in the ear.
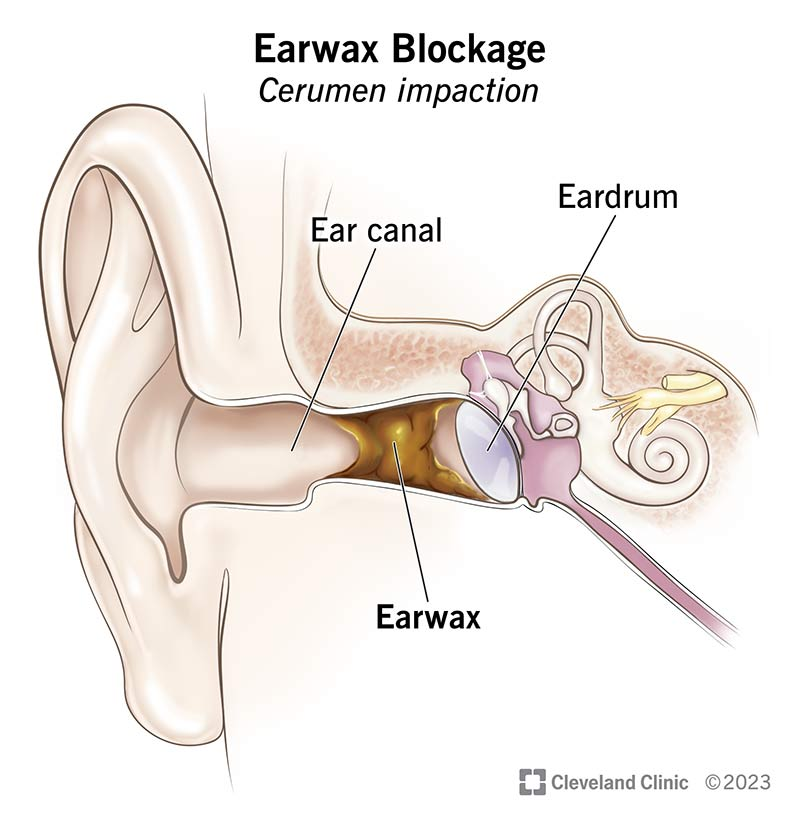
👂 Impacted cerumen (impacted cerumen)
introduction
Cerumen impaction is a condition in which Ear wax It is a blockage inside the titly external auditory canal.
This develops when ear wax gets blocked inside the ear canal and blocks the ear drum.
If ear wax gets blocked inside the ear canal, it causes problems.
Ear wax is also called cerumen .
Cerumen is a compound of cerumen and sebaceous It is a mixture of gland which Epithelium and dust particles are present.
Earwax protects the ear against infection and keeps the ear clean by trapping any dust particles.
Etiology
- A cerumen impaction occurs when earwax is pushed into the ear by cotton tips, hairpins, or other objects. A condition called cerumen occurs.
- In this, wax accumulates even when there is excessive production of wax by the ear gland.
- When the ear is not cleaned properly or is older age and there is a lot of hair in the ear, cerumen also becomes impacted.
Clinical manifestation
- Difficulty hearing,
- Itching
- Pain,
- Tinnitus-like sound in the ears
- Dizziness,
- Feeling of fullness in the ears,
- Discomfort in the ear,
- Pain in the ear,
- Hearing loss.
Treatment
- A) Irrigation of Ear
- B) Removal with curette
- C) Suctioning.
A) Irrigation of ear (irrigation):=
- Irrigation is the most common method to remove any impacted wax.
- In this, the ear canal is washed with water and a commercial irrigator syringe.
- The pressure and force of the water softens the earwax.
- The doctor adds a small amount of alcohol, hydrogen peroxide, and other antiseptics.
- After ear irrigation, the doctor applies antibiotic ear drops to protect against infection.
B)Removal with curette (curette):=
- A jobson Horne curette is used in a circular motion to break up the earwax.
- A cottoned tipped or applicators are used to remove the earwax.
C) Suctioning (Suction):=
- If ear wax causes too much occlusion If this is done, a large bore suctioning device is used to remove the earwax.
- The procedure for removing earwax through suction is very painful, so ask the patient to instill ear drops for two weeks after the suction.
Management
- Serum irrigation, suction , and is removed by instrumentation.
- If the earwax is not very tightly packed, then irrigation is done slowly and the impacted wax is removed.
- Earwax is removed with water.
- If irrigation is not successful, direct visual or mechanical removal is done.
- A few drops of glycerin and mineral oil and half a glass of hydrogen peroxide are placed in the ear canal. Leaving it for 30 minutes softens the earwax and makes it easier to remove.
- If the cerumen is not properly dislodged, instruments such as cerumen curette, aural suction, and binocular microscope are used.
- And ask the patient to follow up properly
👂Otalgia (Otalgia)

Introduction
- Otalgia is pain in the ear ( otalgia may be defined as a pain in the Ear or earache).
Etiology
- Due to bacterial contamination and insertion of any finger or toy.
- Any sharp Due to insertion of an object.
- Due to swimming in any polluted water,
- Any upper respiratory tract infection.
- Any foreign body infection such as any insect, grain, toy, etc. inserted.
Clinical manifestation
- Pain occurs.
- A sense of fullness.
- Itching occurs.
- Inflammation develops.
- Difficulty in hearing.
- Bleeding occurs.
- Severe pain in the ear.
Management
- Irrigate the ear.
- If any Do not irrigate if there are vegetables or insects as there is a possibility of swelling.
- Suction
- Instill mineral oil as it kills the insect and removes it from the ear.
- Many times it Even with anesthesia, there is a need to remove the foreign body.
👂Furenculosis ( Furenculosis)

introduction
- Furunculosis is an infection and inflammation of the hair follicles in the external auditory meatus is
- It is caused by an infection with staphylococcus bacteria.
Clinical manifestation
- Very painful,
- Has difficulty hearing for a while.
- Discomfort,
- Tenderness,
- Fever,
- Headache,
- Earache,
- Drainage comes out of the ear,
- Redness occurs,
- Swelling occurs
management
- Give the patient analgesics to relieve pain.
- Give the patient antibiotics,
- Give the patient warm Provide compression to reduce swelling.
- Provide warm compression to the patient to relieve discomfort.
- Make incision and drainage.
- Provide health education to the patient and their relatives to prevent ear infections and to take proper ear care.
- Instruct the patient to follow up properly.
Dieses and disorders of the middle 👂 Ear

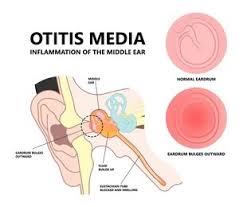
👂Otitis media
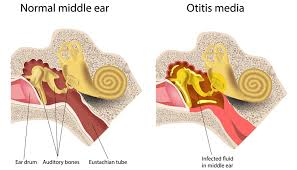
- Infection and inflammation of the middle ear is called otitis media. “Otitis” means:=inflammation*of the Ear. “Media” Means :=middle. This inflammation can cause a sore throat, (cold) cold or other It spreads from the upper respiratory tract infection to the middle ear and can be caused by viruses or bacteria and can be acute and chronic. It causes fluid accumulation in the middle ear and causes bulging and pain.
Types of otitis media
1. Acute Otitis Media (AOM)
- Definition: A rapid onset middle ear infection.
- Causes: Usually bacterial (e.g., Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis) or viral (e.g., RSV, influenza).
- Symptoms: Ear pain (otalgia)
- Fever
- Hearing loss
- Irritability in children
- Redness and bulging of the tympanic membrane.
- Complications: Tympanic membrane perforation, mastoiditis.
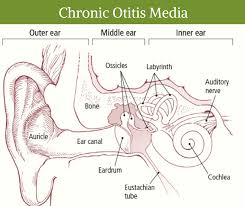
2. Chronic Otitis Media (COM)
- Definition: Persistent middle ear infection lasting more than 3 months, often with tympanic membrane perforation.
- Types:
- Chronic Suppurative Otitis Media (CSOM):
- Characterized by recurrent ear discharge (otorrhea).
- Associated with tympanic membrane perforation.
- Non-suppurative COM:
- Persistent inflammation without active infection.
- Often linked to Eustachian tube dysfunction.
- Chronic Suppurative Otitis Media (CSOM):
3. Otitis Media with Effusion (OME) (Serous Otitis Media)
- Definition: Presence of non-infected fluid in the middle ear.
- Causes:
- Eustachian tube dysfunction.
- Post-acute otitis media.
- Allergies or upper respiratory infections.
- Symptoms:
- Hearing loss or “fullness” in the ear.
- No significant pain or fever.
- Diagnosis:
- Fluid visible behind the tympanic membrane.
- Reduced tympanic membrane mobility.
4. Adhesive Otitis Media
- Definition: A chronic condition where the tympanic membrane becomes retracted and adheres to the ossicles or middle ear structures.
- Cause: Prolonged Eustachian tube dysfunction leading to negative middle ear pressure.
5. Recurrent Otitis Media
- Definition: Multiple episodes of acute otitis media (usually 3 or more episodes in 6 months or 4 or more in 12 months).
- Risk Factors:
- Young age.
- Frequent upper respiratory infections.
- Daycare attendance.
6. Bullous Myringitis
- Definition: A variant of otitis media characterized by blister formation on the tympanic membrane.
- Symptoms: Severe otalgia and possible bloody otorrhea.
Etiology
- Streptococcus bacteria,
- Haemophilus influenzae,
- upper respiratory tract infection,
- exposure to air with irritants such as tobacco smoke 🚬
- client with cleft palate or down syndrome.
Clinical manifestation
- Children who have otitis media are irritable,
- Children who have otitis media have problems in feeding and sleeping.
- Pain,
- A feeling of fullness in the ear,
- fever,
- sign of upper respiratory tract infection such as runny or stuffy nose 👃 or cough.
- Pus collects in the ear and causes pain.
- Rupture of the eardrum.
- Pus collects in the middle ear.
Management
- Antibiotics
- observation,
- Surgical management including myringotomy or tympanotomy.
Nursing management
Nursing assessment
- Patient should have upper respiratory Assess for infection of the tract.
- See if the patient complains of any numbness.
- See if the patient has ear pain.
- See if the patient hears a ringing sound in the ear.
- See if the patient feels uncomfortable.
- See if the patient has nausea and vomiting. See if it is or not.
Nursing Diagnosis
1) Anxiety related to unpredictability of sudden and severe attacks.
2) fear related to potential permanent hearing loss.
3) ineffective role performance related to impaired equilibrium.
4) Impaired social interaction related to communication barriers.
5)Risk for injury related to Impaired equilibrium.
6)fluid volume deficit related to 😵 and vomiting 🤢 .
Nursing interventions
- Assess the patient’s pain level.
- Check if the patient has any discharge from the ear.
- Properly drain the secretion from the ear. To do.
- Check the patient’s middle ear pressure.
- Treat the etiology of otitis media.
- Clean the ear by flushing with normal saline.
- Apply antibiotic ear drops to the patient.
- Provide complete bed rest to the patient.
Acute otitis media (Acute otitis media)
Introduction
Acute otitis media Acute suppurative otitis media or purulent otitis media.Acute otitis media is an acute infection and inflammation. It has an immediate onset and is short-lived. In this, the acute infection occurs in the middle ear and lasts for six weeks (6 week).
Etiology (causative organisam)
- most common cause upper respiratory tract infection.
- pneumococcus species,( Pneumococcus species),
- Haemophillus influenza ,( Haemophilus influenzae.),
- Morraxell catarhalis ( Moraxella catarrhalis),
- streptococcus pneumoniae ( Streptococcus pneumoniae).
Risk factors
- A baby is premature or has low birth weight,
- A family history,
- Altered immunity
- Craniofacial abnormality,
- Neuromuscular disease,
- Someone has seasonal allergies,
- Someone has tonsillitis,
- Someone has a deviated nasal septum,
- Someone has a tumor in the nose,
- Cleft palate or Down syndrome,
- Perforation of the tympanic membrane,
- Vitamin A, zinc, and iron deficiency,
- Measles, Diphtheria, and whooping cough,
- Frequent upper-airway infections,
- No children bottle-feeding Have,
- Have low socio-economic conditions,
- Exposure to tobacco or pollutants.
Clinical manifestation
- Earache,
- Blood vessels become engorged,
- Swelling of the mucous membrane,
- Serous exudate develops (fluid with fluid)
- Sensation of fullness,
- fever
- A ringing sound in the ears
- Drainage from the ear,
- Exudate from the ear Ear drum Due to rupture.
- Difficulty in hearing,
- Patient has irritability,
- Patient feels tenderness,
- Headache,
- Patient cannot sleep,
- Nausea, vomiting and diarrhea,
- Difficulty speaking,
- Pus-like collection in the ear.
Diagnostic evaluation
- History taking and physical examination
- Otoscopy examination,
- pure tone audiometry
- Whispered speech test,
- Weber test,
- Rinne test.
Management
Medical management
- Provide analgesia to relieve the patient’s pain,
- Give antipyretic medicine to relieve the patient’s fever,
- Give antibiotic medicine to the patient,
- Ask the patient to take complete bed rest,
- Instilling warm eardrops in the patient’s ear,
- Providing the patient with medicine as per his/her requirement.
Surgical management
- •Myringotomy:– If there is a collection of fluid in the middle ear, it is done by making an incision in the tympanic membrane. Or Tympanotomy is performed and the fluid is drained.
- Aspirate the fluid from the ear and send it to the laboratory for culture.
- Loosely place a cotton swab in the external ear and collect the drainage.
- Change the cotton swab frequently when it becomes wet with pus to prevent secondary infection.
- A cotton swab is There is an infection, so wash your hands frequently after changing it.
- When the discharge from the ear stops, apply antibiotics for a few days.
- If the patient’s body temperature increases, the patient complains of headache, he feels very sleepy, the patient is irritable and
- If he is disoriented, inform the doctor immediately.
- To prevent otitis media, all parents should Seek immediate medical attention or medication when experiencing pain.
- When signs and symptoms of otitis media occur, Continue antibiotics for a few days when symptoms subside.
Chronic otitis media
introduction
Chronic otitis media is also called chronic suppurative otitis media.Chronic suppurative otitis media is a long-term infection of the middle ear that causes ear tissue damage and chronic Otitis media is caused by repeated episodes of acute otitis media. Chronic otitis media is caused by the accumulation of fluid in the middle ear and the mastoid bone is also involved in the infection of the middle ear.
Etiology ( causes)
- Streptococcus ( Streptococcus ),
- stephylococcus
- pseudomonas organisam ( Pseudomonas infection),
- Perforation of eardrum,
- poor socio economic condition,
- overcrowding,
- poor nutrition,
- poor hygiene,
- chronic sinusitis,
- repeated episodes of acute otitis media.
Clinical manifestation
- Difficulty hearing,
- Pain,
- Dizziness,
- Foul smelling,
- Tenderness,
- Meningitis, (infection and inflammation of the meninges of the brain) to occur),
- Collection of abscesses in the brain,
- Facial paralysis,
- Fullness of Ear,
- Hearing loss,
- Balance problems,
- Dizziness,
- Headache,
- Facial weakness,
- Fever,
- Sleeplessness,
- Tenderness of mastoid process,
- Mucous membrane of ear red,
- Edematous and swollen.
Diagnostic evaluation
- History taking and physical examination,
- Otoscopic test,
- Whisper test,
- Weber test,
- Rinne test,
- Pure tone audiometry,
- Electronystegmography.
Management
- Antibiotics medicine,
- Analgesic medicine,
- antipyretic medicine,
Surgical management
Myringoplasty ( Myringoplasty ):=
- In this, the defect of the tympanic membrane is removed using an operating microscope.
Myringotomy ( Myringotomy):=
- In this, a small incision is made in the tympanic membrane and the fluid collected inside the tympanic membrane is drained.
Tympanoplasty ( Tympanoplastie):=
- Tympanoplastie is performed to repair a perforated ear drum and the middle ear bones such as the malleus, incus, and stapes.
Tympanocentesis ( Tympanosynthesis):=
- In this, a needle is inserted through the front of the tympanic membrane and the contents of the middle ear are aspirated and sent for culture.
Ossiculoplasty ( Ossiculoplasty):=
- Osciculoplasty involves surgical reconstruction of the middle ear bone. Laser surgery is also performed to restore hearing if there is a cholesteatoma in the stapes bone.
Mastoidectomy ( Mastoidectomy):=
- In this, if there is mastoiditis on the mastoid bone, then incision, drainage, and surgical repair of the mastoid process are done.
Simple mastoidectomy ( Simple Mastoidectomy):=
- In this, the surgeon makes an incision behind the ear and removes the infected area.
Radical mastoidectomy (Radical Mastoidectomy) :=
- In this, all the diseased conditions of the middle ear are removed. And its structure is removed. In this, the entire tympanic membrane and ossicles (mallus, incus, and stapes) bones are also removed and the opening of the eustachian tube is closed.
Cortical mastoidectomy Coltical mastoidectomy):=
- This operation is also called Schwartze operation.
Modified radical mastoidectomy (Modified Radical Mastoidectomy):=
- In this, the ossicles and tympanic membrane are preserved for hearing To perform reconstruction.
Nursing management
1) Pain related to inflammation and pressure on tympanic membrane.
Nursing interventions
- Relieving pain
- Assess the patient’s pain location, intensity, and frequency.
- Observe the ear canal for any inflammation or swelling.
- Assess the tympanic membrane for any redness, bulging, or bubbles.
- Provide the patient with analgesics.
- Analgesic ear Use drops.
- Tell the patient to sit up, rest their head and sleep on the unaffected area.
- Keep the head elevated.
- Apply a heating pad to the patient to increase blood supply and relieve discomfort.
2) Risk for infection*related to*euste
preventing infections:=
- Take a complete history from the patient, such as whether there was any ear infection before, whether there was any exposure to water or whether there was any exposure to allergies or whether there is any use of earphones i.e. hearing aids.
- Ask the patient about his symptoms, such as whether there is any pain in the ear, or difficulty in hearing, and whether there is any dizziness.
- Perform an otoscopic examination of the patient.
- Check the ear canal for any drainage or debris, and if so, its color.
- Check the appearance of the tympanic membrane and the amount of fluid draining.
- Administer antibiotic, antipyretic, and anti-inflammatory drugs to the patient. Provide to reduce infection and inflammation.
- Examine the ear 3 to 4 days after completing antibiotic treatment and check if any further treatment is needed.
- Remove any infectious agents or irritating materials such as tobacco, smoke, dust, allergens, etc.
- Advise the patient to take proper nutrition and also to rest and exercise.
- Educate family members to cover their mouth and nose when sneezing and coughing because good hygienic conditions are essential to prevent infection.
3) Impaired verbal communication related to hearing deficit.
Improving hearing and communication:=
- Check the patient’s hearing ability.
- Bring the patient to a well-lit area and ask him to keep his hands away from his mouth.
- Do not ask the patient to speak too loudly.
- Behave honestly with the patient.
- Tell the patient to speak in simple words and plain language and slowly.
- Use other methods of communication such as computer writing tools, etc.
- To prepare the patient for ear surgery.
- Tympanoplasty and Mastoidectomy This hearing Common surgical treatment for loss is.
4)fear and anxiety related to progression of disease .
- Education / *continuity of care.
- Teaching the patient or caregiver to administer medicine.
- Ear Administer the drops at room temperature.
- Do not allow the tip of the applicator or the tip of the drop to come into contact with the ear.
- Position the head in such a way that the flow of ear drops does not go properly into the ear canal. Keep them in this position for one to two minutes.
- Teach them how to clean their ears properly.
- A clean, soft cloth and finger are the best methods for cleaning the ears.
- Apply a cotton-tipped finger to the ear to clean the ears properly.
- Minimize the use of technology such as telephones, TVs, etc.
- Educate the patient to have routine ear examinations.
Mastoiditis
introduction
- mastoiditis It is an inflammation of the mastoid cellular system or the area behind the ear.
- Mastoiditis is an infection of the mastoid bone or the air-containing space.
- Mastoiditis occurs mainly as a complication of otitis media.
- Acute mastoiditis Acute otitis media Caused by .
- And chronic mastoiditis is mainly caused by chronic suppurative otitis media.
Etiology ( causes)
- Most common cause otitis media.
- Streptococcus pneumoniae ( Streptococcus pneumoniae),
- pseudomonas aeruginosa ( Pseudomonas Aeruginosa),
- haemophillus influenzae ( Haemophilus influenzae),
- moraxilla catarrhalis ( Moraxilla catarrhalis),
- mycobacterium species( Mycobacterium species),
- Pneumococcus ( Pneumococcus)
Clinical manifestation
- Pain behind the ear.
- Tenderness is felt in the mastoid region.
- Swelling occurs in the mastoid region.
- Ear pain,
- Mastoid process Redness occurs,
- Fever occurs,
- Headache occurs,
- Nausea and vomiting occur.
- Dizziness occurs,
- Hearing loss occurs.
- Discharge from the affected ear Is,
- Pus is formed.
- Abscess is formed,
- Only drainage comes out of the infected ear.
- Redness and swelling occur behind the ear.
Diagnostic evaluation
- History taking and physical examination.
- Computed tomography test (CT),
- Laboratory investigation
Medical management
- Antibiotics,
- Antipyretic
Surgical management
Mastoidectomy ( mastoidectomy)
- In this, the infected mastoid cell is surgically removed. In this, the surgeon makes an incision at the back of the ear, reaches the mastoid region, and removes the infected air cell.
Tympanostomy tube insertion ( Tympanotomy Tube Insertion)
- In this, a tube is inserted and pus is drained from the middle ear, which can treat the infection.
Nursing management
1) Anxiety related to Surgical procedure potential loss of hearing, potential taste disturbance, And potential loss *of facial *movements.
Reducing Anxiety:=
- Build a therapeutic relationship with the patient.
- Talk to the patient in a way that allows them to describe their Anxiety and their feelings.
- Ask the patient to avoid things that are causing them mental stress.
- Reassure the patient.
- Provide psychological support to the patient.
2) Acute pain related to mastoid surgery .
releving pain :=
- Assess the patient’s pain level.
- Give the patient the prescribed analgesic medication.
- Provide the patient with mind diversional therapy.
- Instruct the patient to take proper bed rest.
- Instruct the patient to drink plenty of fluids.
- Maintain the patient’s nutritional status.
3)Risk for infection related to mastoidectomy , surgical trauma to surrounding tissues and structures.
preventing infections:=
- Take immediate steps to prevent infection.
- Use antibiotic solution when placing packing in the external auditory canal.
- Instill antibiotic ear drops in the patient.
- Tell the patient to prevent water from entering the ear.
- Place a cotton ball loosely moistened with petroleum jelly in the ear.
- Check the patient for any infection.
- Maintain the patient’s hygienic condition.
- Wash hands properly before performing any procedure.
- Use aseptic technique while handling the patient. Maintain technique.
- Bring the patient to a well-lit environment.
Pre operative and post operative Nursing management:=
Pre operative Nursing management:=
- Preoperative audiogram and tympanogram should be performed to assess hearing acuity.
- Provide a comfortable position to the patient.
- Advise the patient to keep the ear dry.
- Tell the patient not to insert any objects such as earbuds or hair pins into the ear.
- Tell the patient not to make sudden movements.
- Tell the patient not to make sudden movements.
- Tell the patient not to Do not blow your nose as this can cause nasal secretions to reach the middle ear through the Eustachian tube.
- Provide local or systemic antibiotics to the patient.
- Provide analgesic medication to the patient.
- Give steroid nasal drops to the patient to prevent infection and inflammation.
- Provide psychological support to the patient to prepare you and him for surgery.
- Teaching the patient and his family members about the surgery and teaching them about post-operative care.
Post operative nursing care:=
- Providing complete bed rest to the patient for 24 to 48 hours after the operation.
- Check the dressing to make sure it is tight and proper to absorb the drainage.
- Change the dressing daily.
- Check if the patient has any facial paralysis.
- The patient should be given a Check for headache, vomiting, stuffy neck, dizziness, irritability, or disorientation.
- The patient is at risk of developing chronic purulent otitis media after surgery, so provide proper antibiotic medicine.
- Check the patient’s vital signs properly.
- Maintain the patient’s fluid level.
- Tell the patient and his relatives that the patient’s hygiene condition maintain.
- Administer antihistamine and analgesic medicine to the patient.
- Instruct the patient to follow up properly.
Perforation of Ear 👂 drum (perforation of ear drum)/ tympanic membrane perforation.
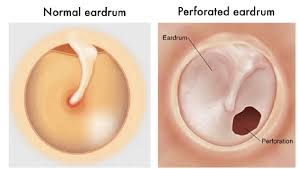
Introduction
A perforated eardrum is a hole (perforation) formed in the eardrum, and this hole is a passageway between the middle and inner ear. It damages and also causes infection. Conductive hearing loss can also occur due to perforation of the ear drum. Perforation of the ear drum causes hearing loss and also causes occlusive discharge.
Cause/Etiology
- Perforation can also occur due to direct injury to the ear drum.
- Any foreign object or anything that is completely damaged can also cause perforation in the ear drum.
- Insertion of any hair pin or ear birds.
- Even after a skull fracture.
- Due to exposure to very loud voices.
- Infection
- Due to not curating with a syringe properly.
- Due to trauma.
- Due to falling.
- Earache,
- Drainage from the ear comes out.
- Difficulty in hearing,
- Dizziness,
- Disoriented,
- Fullness of Ear 👂,
- Ringing in the ears What does it sound like?
- Bloody discharge from the ear.
- History tacking and physical examination
- Direct inspection with an otoscope.
- A perforated ear drum heals on its own within one to two months.
- Provide antibiotic therapy to the patient,
- Maintain aseptic technique to prevent further infection.
- Place packing in the ear drum.
- If the ear drum does not heal on its own, surgical correction is necessary.
- Ask the patient to maintain a hygienic condition of the ear.
- Provide the patient with analgesic medicine.
- If the perforated ear drum If it is due to foreign objects, do not try to remove it yourself and seek the help of a medical professional.
- In this, the perforated Ear drum is surgically corrected.
- In this, the perforated The eardrum is surgically closed.
Clinical manifestation
Diagnostic evaluation
Management
Surgical management
Some types of large and small holes require surgery. Surgery is performed under general anesthesia.
1) tympanoplasty (Tympanoplasti) :=
2)Myringoplasty (Myringoplasti):=
3)occiculoplasty ( ossiculo plasty):=
- This is a surgical procedure in which the ossicles are removed. Surgical reconstruction is performed.
Prevention
- Treat ear infections immediately.
- Do not insert any objects into the ear to clean the ear.
- Wear proper ear protection.
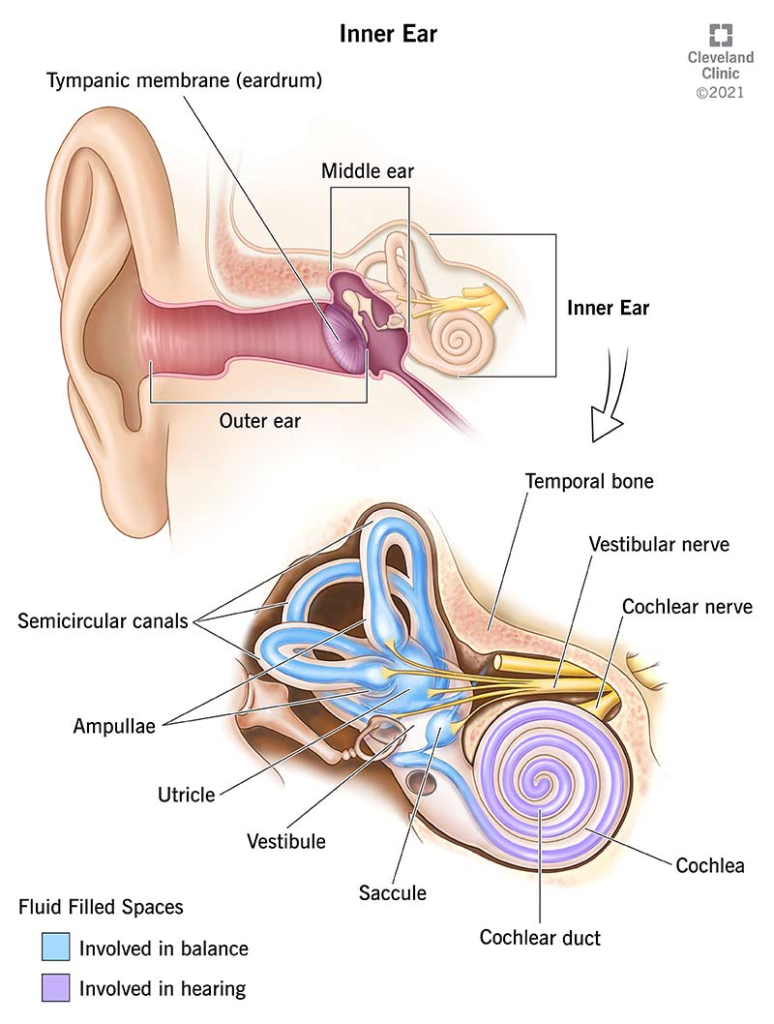
Disease and disorder of the internal ear 👂
Presbycusis (Presbycusis)
Introduction
In this age-related hearing loss, it is called presbycusis. We see presbycusis more in people over 65 years of age. It is a major age-related disorder.
Presbycusis occurs gradually and is seen in both ears, but many people are not aware of it.
Etiology/ cause
- Due to environmental noise.
- Due to damage to sensory receptors in the inner ear.
- Hereditary from generation to generation (Heredity)
- Due to age (Age)
- Due to certain health conditions such as diabetes and hypertension,
- Due to side effects of certain medications such as aspirin and some antibiotics.
Symptoms
- The person cannot hear properly,
- High pitch sounds such as “s” and “th” are difficult to distinguish.
- Conversations are difficult to understand when there is background noise.
- Men’s voices are easier to hear than women’s.
- A ringing sound in the ears, similar to tinnitus.
- Hearing becomes very difficult.
Treatment for presbycusis
- Avoid going to places with a lot of noise or being exposed to loud noise.
- Wearing ear plugs in the ears.
- Using hearing aids.
- Using telephone amplifiers,
- Training someone to understand what they are saying (lip reading training)
Labyrinthitis (Labyrinthitis)
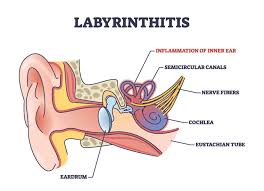
Introduction
Labyrinthitis is a disorder of the inner ear in which infection and inflammation occur in the inner ear. It is called labyrinthitis. In labyrinthitis, balance and hearing are affected. It can be found in one or both ears and its hallmark symptom is vertigo, meaning the person feels dizzy.
Etiology / cause
- Due to infection in another part of the body such as otitis media and meningitis.
- Due to some types of infection.
- Due to head injury Due to.
- Due to too much stress.
- Due to certain types of allergic conditions.
- Due to excessive alcohol consumption.
- Due to taking certain types of medications such as aspirin.
- Labyrinthitis can also be caused by an infection in the upper respiratory tract.
- It is also caused by viruses and bacteria.
Risk factors
- Drinking too much alcohol.
- Having any allergies.
- Having an upper respiratory tract infection (URTI)
- Smoking,
- Excessive stress,
- Taking certain types of prescription or non-prescription medications such as aspirin.
Types of Labytinthytis
1) DIFFUSE SEROUS LABYRINTHITIS (Diffuse Serous Labyrinthitis)
- This type of labyrinthitis is acute. And often occurs due to drinking alcohol. And due to some types of allergic conditions, the condition of diffuse serous labyrinthitis also occurs.
2) DIFFUSE SUPPURATIVE LABYRINTHITIS (Diffuse suppurative labyrinthitis)
- In this condition, due to repeated occurrence of labyrinthitis, purulent discharge comes out from the ear and due to this, destruction of the soft tissue structure of the ear occurs and due to this permanent hearing loss occurs.
3) CIRCUMSCRIBED LABYRINTHITIS (Circumscribed Labyrinthitis)
- In this, Bony Capsule Labyrinthitis also has involvement. That is, the bone also gets involved and a fistula is formed in the inner Ear. It is called Circumscribed Labyrinthitis It is said.
Clinical manifestation
- Very dizzy,
- Drainage comes out of the ear.
- Ear pain,
- Nausea 😵
- And vomiting 🤢
- Sensorineural Hearing loss occurs.
- aural fullness,
- 🤒 Fever,
- Facial weakness 😫,
- Neck pain,
- A ringing sound is heard in the ears,
- Difficulty focusing with the eyes.
- Upper respiratory track infection But there are symptoms.
- There are also problems with memory and thinking power,
- Depression and anxiety occur.
- Loss of balance.
Diagnostic evaluation
- History taking and physical examination,
- A complete physical and nervous system examination should be done,
- Electro encephalogram ( EEG)
- Electro encephalo gram,
- Electronystigmography
- Electronystigmography,
- Head CT scan,
- Hearing test( audiology/audiometry)
- M.R.I
- Warning or cooling the inner ear with air or water to test eye reflux.
Treatment
- Labyrinthitis usually goes away in a few weeks.
- Treatment involves removing the symptoms.
- Medication includes
- Antihistamine
- Medication used to treat nausea and vomiting,
- Medication to Relieving Dizziness such as meclizine, or scopolamine,
- Sedative hypnotonics such as valium.
Nursing Management
Nursing assessment
- Check whether the patient has involuntary eye movements.
- Check whether the patient is dizzy.
- Check whether the patient has hearing loss.
- Check the patient’s skin turgor.
- Check the patient’s hydration status Assess.
- See if the patient hears a sound like tinnitus.
Nursing diagnosis
- 1) Acute or severe headache related to disease condition .
- 2)Anxiety related to disease condition.
- 3)knowledge deficiency related to disease condition and its treatment and side effect .
- 4)Impaired social interaction related to communication barriers.
- 5)Risk for injury related to loss of balance.
Nursing management
- Early diagnosis of labyrinthitis.
- CT scan of the head to check for any injury.
- Neurological examination.
- Check the main cause of the disease.
- If the patient has hearing loss, consult a speech therapist. Send.
- Clean the ear with normal saline and antibiotics.
- Cover the eye with lotion.
- The patient and his family members should undergo all diagnostic Explain the test.
- Clear the earwax.
- Take care to prevent any other infection in the ear.
- Perform a hearing test on the patient.
- If the patient is dizzy, give him/her appropriate medicine.
- Provide sedative medicine to the patient to rest properly.
- Protect the patient from any further injury and take care to prevent hearing loss.
- Properly drain and clear the discharge.
- Provide emotional support to the patient.
- Treat the patient appropriately if he/she is dizzy.
- If the patient has a viral infection, provide him/her with proper bed rest and monitor his/her hydration status. Maintain.
- Give the patient antiviral medicine such as acyclovir,
- Famcyclovir, valacyclovir to reduce viral infection.
- If the patient has a bacterial infection, provide him with antibiotic medicine.
- If the patient has severe nausea, vomiting, give him IV fluid to maintain his hydration status.
- Provide the patient with corticosteroid medicine.
- Teach the patient how to coordinate head and eye movements.
- Improve the patient’s walking skills and balance.
- When the patient experiences any symptoms, take proper rest.
- Do not change the patient’s position suddenly.
- Tell the patient not to read when the symptoms are coming.
- Avoid going into very bright light.
- Avoid doing very heavy activities.
Meniere’s disease
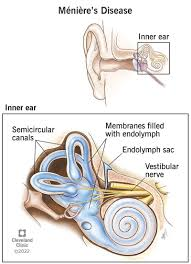
Introduction
Menieres’ disease is a disorder of the inner ear that affects the auditory system (hearing system) and the vestibular system (balance). It is characterized by sudden and recurrent episodes of dizziness and tinnitus, and progressive hearing loss, usually in one ear.
Menieres’ disease is named after the French physician Prosper Menieres, who described vertigo as a disorder of the inner ear in 1861.
Etiology/ cause
- Exact cause is not known,
- Most common cause dilatation of endolymphatic systems .
- Due to head injury.
- Due to middle ear infection.
- Due to syphilis.
- Due to allergic conditions. Due to alcohol use.
- Due to repeated viral infections.
- Due to respiratory tract infections.
- Due to smoking.
- Due to taking stress.
- Due to taking certain types of medicine.
- Genetic,
- Aspirin,
- Smocking cigarette,
- Drinking alcohol 🍸,
- Due to eating too much salt
- Due to low immunity.
Clinical manifestation
- Vertigo and tinnitus,
- Sweating,
- Nausea and vomiting,
- Fullness of both ears,
- Photophobia
- Headache,
- Nystegmus.
Diagnostic evaluation
- History taking and physical examination,
- Audiometric test
- MRI of Head.
Management
Medical management
- Ménière’s DCA cannot be cured but medicine is provided to relieve symptoms.
- Antihistamine,
- Anticholinergic ,
- Steroids,
- Diuretic,
- If the patient has dizziness and vertigo, then scopolamine is given.
- Sedative/ hypnotonics like diazepam,
- Antiemetics ( promethazine, chlorpromazine),
- Streptomycine Intramuscular,
- If the patient has severe hearing loss, provide a hearing aid.
- Tell the patient to eat something low in sugar to prevent fluid accumulation.
- Tell the patient to stop smoking.
- Exercise regularly.
surgical management
1) Endolymphatic sac decompression (endolympic shake decompression) :=
- In this operation, an incision is made behind the ear and the mastoid bone is exposed.
2) Labyrinthectomy
- In this, endolymphatic sac decompression As soon as an incision is made behind the ear and its labyrinth is exposed.
3) Vestibular neurectomy:
- The vestibular nerve is resected and the vertigo is relieved.
4) Cryosurgical method Method)
- In this method, a cryo probe is placed on the semicircular canal and a subnormal temperature is provided so that the labyrinth tissue is destroyed.
Nursing management
Assessment
- Ask the patient where the vertigo and dizziness started.
- Assess the extent of hearing loss.
- Assess the patient’s vital signs.
- Nutritional status of the patient Assess.
- Assess the patient’s hydration status.
- Patient’s weight. Assess.
- Weber and Riehne tests to check the amount of hearing loss.
- See if the patient has any other neurological symptoms such as visual changes, changes in mental status, and motor deficits.
- The patient To see if there is a condition of Nausea and Vomiting.
Nursing diagnosis
1) risk for injury related to sudden attacks of vertigo.
preventing injury:=
- Assess the patient for any conditions such as dizziness and vertigo.
- Instruct the patient to take adequate rest.
- Any conditions such as dizziness and vertigo should be treated. If episodes occur, ask the patient to lie down in a safe place.
- Seek medical advice when the patient starts to walk.
- Avoid activities such as driving, working in heavy machinery, climbing stairs, etc. for a week.
- Avoid excessive exercise.
- Avoid exposure to bright light, avoid watching TV and reading for a while.
2) fluid volume deficit related to vomiting and impaired intake.
Goals/Expected Outcomes:
- The patient will maintain adequate hydration as evidenced by:
- Normal skin turgor.
- Moist mucous membranes.
- Stable vital signs.
- The patient will verbalize understanding of measures to prevent dehydration.
- The patient will demonstrate improved fluid intake by the end of the care period.
Nursing Interventions and Rationales:
- Monitor Fluid and Electrolyte Status:
- Intervention: Assess intake and output (I&O), noting color, consistency, and volume of urine.
- Rationale: Helps evaluate fluid balance and detect early signs of dehydration or electrolyte imbalance.
- Assess Vital Signs:
- Intervention: Monitor blood pressure, pulse rate, and respiratory rate frequently.
- Rationale: Hypotension and tachycardia may indicate hypovolemia.
- Encourage Oral Fluid Intake:
- Intervention: Offer small sips of fluids like oral rehydration solutions (ORS), clear broth, or electrolyte drinks.
- Rationale: Helps replenish lost fluids and electrolytes without overwhelming the stomach.
- Administer IV Fluids as Prescribed:
- Intervention: Administer isotonic solutions (e.g., normal saline or lactated Ringer’s) as ordered by the physician.
- Rationale: Quickly restores circulating volume and corrects dehydration.
- Monitor for Signs of Electrolyte Imbalance:
- Intervention: Observe for symptoms like muscle cramps, weakness, or confusion.
- Rationale: Electrolyte imbalances (e.g., hyponatremia, hypokalemia) can result from vomiting and require prompt correction.
- Prevent Further Vomiting:
- Intervention: Administer antiemetic medications (e.g., ondansetron, metoclopramide) as prescribed.
- Rationale: Reduces nausea and vomiting, promoting fluid retention.
- Promote Nutritional Intake:
- Intervention: Gradually introduce bland foods once vomiting subsides (e.g., rice, bananas, toast).
- Rationale: Restores nutritional balance without irritating the gastrointestinal tract.
- Maintain Comfort:
- Intervention: Provide a calm environment, elevate the head of the bed, and encourage rest.
- Rationale: Reduces nausea and promotes comfort.
- Educate the Patient and Family:
- Intervention: Teach about the importance of hydration, recognizing signs of dehydration, and dietary modifications.
- Rationale: Encourages patient participation in recovery and prevention of future episodes.
Evaluation:
- The patient maintains stable vital signs within normal ranges.
- Improved hydration status evidenced by moist mucous membranes and adequate urine output.
- Patient verbalizes understanding of hydration and dietary measures.
- Resolution of nausea and vomiting, with gradual improvement in oral intake.
If more detailed or customized care is needed, let me know!
3) Altered nutrition less than body requirement related to nausea and vomiting .
Nursing interventions:=
- Ensuring adequate food and fluid .
- Patient’s intec output assess To do.
- When the patient feels better, ask him to take small amounts of fluids and small amounts of feeding.
- Ask him to take fresh meat, poultry, vegetables and fruits in the diet.
- Processed meat 🍖, canned products, salt 🧂 Avoid all these things.
- Tell the patient not to take caffeine, alcohol, tobacco, as well as chocolate, as these things aggravate the symptoms of Meniere’s disease.
- Avoid the patient from smoking.
- Smoking constricts the blood vessels which cause nerve The blood supply to the affected area is reduced.
- Advise the patient to eat less salty foods and to consume only one to two grams of salt throughout the day.
- olives,pickled food, Chips, some 🧀 cheeses should be taken in small quantities.
- Provide antiemetic medicine to treat the patient’s nausea and vomiting.
4) Anxiety related to*sudden onset of symptoms .
Goals/Expected Outcomes:
- The patient will verbalize a reduction in feelings of anxiety.
- The patient will demonstrate effective coping mechanisms.
- The patient will exhibit normalized physiological responses (e.g., regular breathing and heart rate).
Nursing Interventions and Rationales:
Establish a Therapeutic Relationship:
- Intervention: Remain calm, maintain a composed demeanor, and use a reassuring tone.
- Rationale: Helps build trust and reduces the patient’s perception of threat.
Assess the patient’s level of Anxiety:
- Intervention: Evaluate using an anxiety scale or by observing verbal and non-verbal cues.
- Rationale: Identifies severity to tailor interventions appropriately.
Provide Immediate Support:
- Intervention: Stay with the patient during acute episodes of anxiety.
- Rationale: Presence of a caregiver provides reassurance and prevents feelings of isolation.
Encourage Controlled Breathing:
- Intervention: Guide the patient in deep breathing exercises (e.g., inhale for 4 seconds, hold for 4 seconds, exhale for 4 seconds).
- Rationale: Reduces hyperventilation, stabilizes oxygen levels, and promotes relaxation.
Explain the Situation Clearly:
- Intervention: Provide information about the patient’s symptoms and the steps being taken for care.
- Rationale: Reduces uncertainty, which is a major cause of anxiety.
Create a Calm Environment:
- Intervention: Minimize noise, dim lights, and remove unnecessary stimuli.
- Rationale: Reduces environmental triggers that may exacerbate anxiety.
Empower the Patient:
- Intervention: Encourage the patient to express their fears and concerns.
- Rationale: Ventilation of feelings can help reduce internal tension.
Use Distraction Techniques:
- Intervention: Engage the patient in conversation, or suggest listening to calming music or using grounding techniques (e.g., focusing on surroundings).
- Rationale: Shifts the patient’s focus from anxious thoughts to neutral or pleasant stimuli.
Provide Pharmacological Support (if prescribed):
- Intervention: Administer anti-anxiety medications as ordered (e.g., benzodiazepines or SSRIs).
- Rationale: Helps manage physiological symptoms and provides immediate relief if non-pharmacological methods are insufficient.
Teach Coping Strategies:
- Intervention: Educate on relaxation techniques (e.g., progressive muscle relaxation or guided imagery) for long-term anxiety management.
- Rationale: Empowers the patient to manage future episodes of anxiety.
Involve Family (if appropriate):
- Intervention: Allow family members to be present for support, if the patient desires.
- Rationale: Familiar presence can provide comfort and reduce feelings of vulnerability.
5) self care deficit related to vertigo .
nursing interventions
minimise anxiety:=
- Explain all procedures to the patient.
- In the patient’s daily routine activities involves.
- Tell the patient to stop the activity when the dizziness is present and to continue the activity in small increments when the dizziness subsides.
- Tell the patient to reduce the amount of movement.
- If there is a significant amount of hearing loss, the patient should be given a hearing To provide aid.
- Ask the patient to take the proper medicine.
- Ask the patient to exercise adequately.
- Ask the patient to walk a little. To reduce the patient’s stress, provide exercise, speech exercises, and mind diversion therapy.
- The patient is not Ask to take safety measures when experiencing vertigo.
Otosclerosis ( otosclerosis)
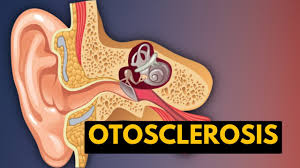
Introduction
Otosclerosis ” hardening of 👂 Ear ” ( Otosclerosis := Hardening of Ear) Otosclerosis is the abnormal growth of spongy bone, including the Stapes bone of the middle ear.
This involves the growth of new bone, causing the stapes bone to become immobile (i.e. unable to vibrate). And due to this, sound vibrations are not transmitted and due to this, conductive hearing loss occurs.
Otosclerosis affects both ears.
Otosclerosis or “hardening of bone” is caused by the formation of abnormal spongy bone and also includes the stapes bone of the middle ear, due to which conductive hearing loss also occurs.
Classification of otosclerosis
- 1)histological otosclerosis , ( histological oto*sclerosis)
- 2)clinical otosclerosis . ( clinical oto sclerosis)
- A)stepedial otosclerosis ( Stapedial Otosclerosis),
- B)cochlear Otosclerosis ( Cochlear Otosclerosis),
- C)mixed otosclerosis (Mix Otosclerosis)
1) Histological otosclerosis:=
Histological otosclerosis does not cause any symptoms during the life of the person but it is detected during post mortem.
2) Clinical otosclerosis:=
A) Stepedial otosclerosis:=
In this otosclerosis, a spongy bone is formed and it also includes the stapes bone of the middle ear, it is called stapedial otosclerosis. It causes conductive hearing loss.
B)Cochlear otosclerosis:=
In this, a spongy bone is formed on the cochlea and it also includes the membranous labyrinth, due to which sensorineural hearing loss occurs.
C)mixed otosclerosis:=
In this mixed condition, both the stapes bone and the membranous labyrinth develop spongy bone formations and hearing loss occurs, which is called mixed.
Etiology/ cause
- Due to metabolic disorders,
- Immune disorders,
- Vascular diseases,
- Infections such as measles
- Trauma,
- Temporal bone fractures Due to abnormality.
Clinical manifestation
- Difficulty in hearing.
- Dizziness and vertigo occur.
- Loss of balance.
- A sound similar to tinnitus is heard in the ears.
- A person cannot hear for a very long time.
Diagnostic evaluation
- History tacking and physical examination
- Otoscopic examination,
- Rinne test,
- Weber test,
- Audiogram,
- Tympanometery.
Management
Medical management
- Fluoride,
- Calcium or vitamin D,
- Analgesic ( ibruprofen, mornin, advil, oxycodone, acetaminophen, pydrocodone, acetaminophen),
- Hearing aid use to treat hearing loss,
Surgical management
- 1) Stapedectomy ( stapedectomy),
- 2) Stapedotomy ( stapedotomy).
1) stepedectomy : =
- In stapedectomy, the abnormal spongy stapes bone is removed and replaced with a prosthesis between the incus bone and the oval window.
2) stapedotomy ( stapedotomy) :=
- This is a modern surgery in which A hole is made in the foot plate of the stapes and a pistol-shaped prosthesis is placed in it.
Nursing management
Assessment
- Ask the patient about the onset and progression of symptoms.
- How much Assess the amount of conductive hearing loss.
- Assess the amount of conductive hearing loss through the Rayney test.
Post operative care
- Provide analgesic medicine to the patient according to the amount of pain after the operation.
- Post operative trauma and oedema For vertigo, provide dymenhydrinate 50 mg every six hours.
- Provide side rails on both sides of the bed to prevent the patient from falling.
- Provide antibiotic medicine to the patient to prevent infection after the operation.
- Tell the patient not to blow his nose because this can allow air and microorganisms to reach the eustachian tube.
- Sneeze as much as possible. Avoid.
- Do not lift any heavy objects until the surgeon gives permission.
- Advise the patient to avoid hair for two weeks. Do not wash the ear and do not let any water enter the ear for six (6) weeks.
- Remove the ear packing on the sixth day.
- Advise the patient to keep a sterile cotton swab in the ear for one week after the packing is removed when going out of the house.
- Change this cotton twice a day.
- After six weeks, advise the patient to do his daily routine activities in small amounts.
- Asking the patient to lie on the operation side may result in improper technique. Drainage can only be done.
- If the patient is asked to lie on the non-operated side, then the graft can be prevented from being displaced.
- Ask the patient if he/she is experiencing pain, headache, vertigo, or any unusual sensation in the ear.
- Provide the patient with anti-emetic medicine to prevent nausea.
- Provide the patient with antibiotic medicine.
Nursing management
Improving breathing pattern
- Ask the patient to take deep breaths.
- Ask the patient to do deep breathing and pursed lip breathing.
- Place the patient in a comfortable position provide.
improve communication related to deafness maintain hygiene .
- Ask the patient to maintain hygienic conditions.
- Provide a clean and neat environment to the patient.
- Ask the patient to wear clean and neat clothes.
- Observe the skin for any pressure ulcers.
- Involve family members in the client’s care.
Improve nutritionstatus
- Assess the nutritional status of the patient.
- Provide a safe and clean environment for the patient.
- Provide an attractive and easy Serve food in.
- Provide adequate water to the patient.
- Maintain the patient’s hydration status.
promote physical mobility
- Assist the patient in performing range of motion exercises.
- Involve the patient in daily routine activities.
relieve from fear and anxiety
- Explain the patient’s feelings to the patient and his family members To say for.
- Provide psychological support to the patient.
- Clarify all the patient’s doubts in simple language.
improve coping ability
- Give reassurance to the patient.
- Patient’s To clear all doubts.
- Provide education to the patient about the disease condition in a language that all patients and their family members can understand.
- Actively listen to the problems of the patient’s family members.
- Involve the patient’s family members in their care.
- Provide complete and accurate information to the patient’s family members and help them with their recovery and Giving proper information about progression.
Deafness ( Deffles )

- Deafness is a partial or complete hearing loss.
- Hearing Impairment is a mild difficulty in hearing and a total loss of hearing. Hearing impairment affects communication, social activity, and work activity. Deafness reduces a person’s quality of life. Elderly people mainly suffer from hearing loss. Age-related hearing loss affects 30 to 35% of people aged 65 to 75. It is found inside.
- 40% of cases occur in people over 70 to 75 years of age.
- Most hearing loss is caused by otitis media and mainly affects young children.
- Hearing loss can also be caused by noise, drugs and toxins, and centrineural Hearing loss is caused by a genetic condition.
qualification of hearing loss
The severity of hearing impairment is measured in terms of loudness and is measured in decibels.
- 1)mild:= between 25 and 40 dB.
- 2)moderate:=between 41 to 55 dB.
- 3)moderately severe:= between 56 to 70 dB.
- 4)severe:= between*71 and 90 dB .
- 5)profound:=91 dB or greater.
classification
- 1)conductive hearing loss, ( conductive hearing loss),
- 2)sensorineural hearing loss. ( Sensory Neural Hearing Loss)
- 3) mixed hearing loss. ( Mixed Hearing Loss)
1) Conductive Hearing Loss:=
Conductive hearing loss is an impairment in any of the normal mechanisms that transmit sound waves to the outer ear. Conductive hearing loss occurs when any of the mechanisms that transmit sound to the inner ear, such as the outer ear, ear drum, and middle ear bones, is impaired.
Etiology
••external ear :=
- Impacted cerumen.
- Otitis externa,
- Foreign body in the external auditory canal.
- Congenital atresia,
- Tumor in the ear canal.
•• middle ear:=
- Acute otitis media,
- Serous otitis media,
- Collection of fluid in the middle ear,
- Perforation of the tympanic membrane,
- Tympanosclerosis,
- Massage of the ossicular,
- Middle ear tumor,
- Temporal bone trauma,
••inner Ear :=
- Severe auto otosclerosis,
2)sensorineural hearing loss:=
Sensory neural hearing loss is caused by dysfunction of the inner ear.
Sensory neural hearing impairment is caused by any abnormality in the cochlea and the vestibulocochlear nerve that carries hearing to the brain. It can be mild, Moderate and severe and total deafness can also occur.
Etiology
- Sensory Neurals Hearing loss can be congenital or acquired,
- Due to the cochlea not developing properly,
- Due to any chromosomal abnormality,
- Due to genetic hearing loss,
- Due to age, for example, pressor cusps,
- Any benign or malignant tumor Due to,
- Certain types of drugs,
- Childhood infections such as measles, mumps, and meningitis,
- Any congenital infection such as
- Toxoplasmosis, rubella, cytomegalovirus, herpes, and syphilis,
- Premature birth,
- Alcohol syndrome,
- Due to poor nutrition during pregnancy,
- Due to any loud noise,
- Due to Meniere’s disease,
- Sudden pressure changes from flying, Diving and strenuous exercise,
- Due to any type of viral infection,
- Otosclerosis,
- Due to physical trauma such as a fracture of the temporal bone,
- Due to any type of autoimmune disease,
- Due to HIV or AIDS,
- chlamydia causes hearing loss of newborn,
- Due to exposure to chemicals.
3) mixed hearing loss:=
A type of hearing impairment in which both sensorineural hearing and conductive hearing loss are present There is a type of hearing loss.
Having both of these types of hearing loss is called mixed hearing loss.
clinical manifestation
- This is due to progressive hearing loss,
- Dizziness,
- Difficulty speaking,
- Difficulty understanding any kind of words,
- Difficulty speaking,
- To tell someone to speak very slowly, clearly and loudly,
- To have difficulty hearing,
management
1)Removing wax blockage:=
- Ear wax should be removed slowly using a scoop or suction.
2)hearing aid:=
- Hearing loss It is caused by damage to the inner ear, so it helps to make the sound stronger and easier to hear. Hearing aids deliver the sound to the inner ear very effectively.
3) cochlear implants:=
- A cochlear implant is a great option if you have very severe hearing loss.
- A cochlear implant involves an electrical device that is implanted in the cochlea that transmits sound to the inner ear and stimulates the cochlea, causing the patient to hear. hearing can.
4) aural rehabilitation:=
- Aural rehabilitation is the process in which hearing loss is identified and diagnosed and different types of treatment are provided to the aural Rehabilitation Therapy is provided to the patient to help the person hear up to the maximum amount.
type of aural rehabilitation therapies
- auditory training,
- speech reading (speech reading), (lip reading)
- hearing aid orientation,
- listening strategies,
- speech reading,
- auditory training,
- total communication,
- manual communication,.
surgical management
1) restore conductive hearing.
- myringotomy,
- stapedectomy.
2) assisted hearing in profound Deafness.
- cochlear implants,
- temporal bone stimulators (semi-implantable hearing device),
3)middle ear implants,
4)tumor excision.
communicating with hearing Impaired patients.
- Speak clearly and communicate in pure and simple language.
- Move closer to the speaker and try to hear clearly,
- Keep your mouth open Keep,
- Repeat the message.
prevention
- Protect your ears from any workplace,
- Watch how much you hear,
- Avoid loud noises of any kind.
Tumor of the ear and auditory nerve ( Tumor of the ear and auditory nerve.)
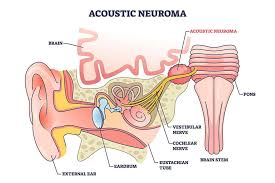
Acoustic neuroma
Introduction
- A vestibular schwannoma (also known as acoustic neuroma, acoustic neurinoma or acoustic neurilemoma)
- (also known as acoustic neuroma, acoustic neurinoma or acoustic neurilemoma) .
- Acoustic neuroma is a slow growing tumor of the nerve that connects the ear to the brain.
- This nerve is the vestibular cochlear is nerve.
- This The nerve is located behind the ear and inside the brain.
- Acoustic neuroma is not cancerous but a benign tumor.
- This means that this tumor does not spread to other parts of the body.
- However it can damage several important nerves as it grows.
Etiology
Age := most people develop acoustic neuroma between the age of 30 and 60.
neurofibromatosis
This is a type of inherited disorder in which acoustic neuromas are both auditory It develops in the nerve.
Due to exposure to radiation.
clinical manifestation
- Vertigo means dizziness.
- Hearing loss occurs.
- Ear pain. Tinnitus is a ringing sound.
- Difficulty understanding speech.
- Dizziness,
- Headache,
- Loss of balance,
- Numbness occurs.
- Pain,
- sleeplessness,
- vision problems,
- Weakness of the face.
Diagnostic evaluation
- History tacking and physical examination
- decrese feelings on one side of the face,
- drooping on one side of the face,
- unsteady walk,
- MRI of brain,
- audiology,
- est of equilibrium and balance ( electronysyagmography),
- test of hearing and brainstem function (brainstem auditory evoked response)
management
- observation,
- microsurgical removal,
- radiation therapy,
treatment
Treatment depends on the size of the tumor, its location, the person’s age, and their overall health.
The person and their health care provider observe the growth of the tumor and may provide radiation therapy to prevent its growth or remove the tumor.
Most acoustic neuromas are small and grow slowly.
When the tumor is small, it has few symptoms and is mainly seen in older patients, so regular MRI scans are necessary.
If it is treated If not, acoustic neuroma is a nerve Involves hearing and balance as well as movement.
If the tumor is very large, it can cause fluid to build up in the brain and cause the condition of hydrocephalus.
The condition of hydrocephalus is life-threatening.
In acoustic neuroma, it is removed if any of the following conditions are present:=
- 1) large tumor,
- 2)tumor that are causing symptoms,
- 3)tumor that are growing quickly,
- 4)tumor that. Are pressing on the brain.
Surgery is required to remove the tumor and further Surgery is also necessary to prevent damage to the nerve.
The patient is provided with radiotherapy.
Tumours that are difficult to remove through surgery are given radiation therapy to slow their growth.
When acoustic neuroma is removed, it damages the nerve as well as causes hearing loss and weakness on facial muscles and due to this Hearing problems occur
The damage is more severe when the tumor is very large.
Nursing assessment
- Ask the patient if they have any tinnitus sensation.
- How much headache is caused by a pain scale Ask.
- Ask whether there is any injury.
- Ask whether the patient feels tired and restless.
early detection of tumor by:=
C :=CHANGE IN BOWEL AND BLADDER HABIT,
A:=A SORE THAT DOES NOT CURE,
U:=UNUSUAL BLEEDING,
T:=THICKENIN OF*LUMP AND MASS ,
I:=INDIAGETION AND DIFFICULTY IN SWALLOWING ,
O:=OBVIOUS CHANGE IN MOLE ,
N:=NAGGING COUGH .
Nursing management
- Management depends on the size of the tumor and its location.
- Preventing metastasis of the tumor.
- The patient should be treated in any such situation To prepare the patient emotionally before accepting.
- To prepare the patient for chemotherapy and radiation therapy.
- To ensure that the side effects of chemotherapy are reduced and to provide treatment for them.
- If Alopecia If it is happening, that is, if his hair is losing a lot, prevent him from sunlight.
- Drink enough water to prevent dehydration.
- Apply emollients to the skin to prevent skin integrity.
- Provide the patient with proper sedatives to get enough sleep and rest.
Eustachian tube Insufflations
- The Eustachian tubes are small passages in the head that connect the ear to the back of the nose.
- These tubes become blocked due to colds and allergies.
- Mild to moderate cases can be treated at home with over-the-counter medications and prescription solutions.
1) Recognize the symptoms:= If there is swelling due to cold, allergy, infection, it prevents the Eustachian tube from opening and does not allow air to pass through. This results in a change in pressure and sometimes fluid accumulates in the ear. When this happens, the following symptoms are experienced.
- Earache,
- A ringing and popping sound is heard in the ear.
- A tinnitus-like sound is heard in the ear.
- Difficulty in hearing clearly It falls.
- Dizziness and difficulty maintaining balance.
2) Wriggle jaw:=
- This is known as a simple technique that attempts to restore airflow.
- This simply involves pushing the jaw forward and then rocking it back and forth from side to side. If the obstruction in the ear is minor, this action can open the Eustachian tube and restore normal airflow.
1) Vasalva Maneuver:=
This maneuver which attempts to force air through the blocked airway and restore airflow should always be done with this in mind. The air pressure in the body is affected when you try to get out of the blocked airway. The sudden drop in pressure when you exhale can cause rapid changes in blood pressure and heart rate.
- Take a deep breath and hold it. Close your mouth and close your nostrils.
- Try to blow air out of your blocked nostrils.
- If this maneuver is successful, you will hear a popping sound in your ears and your symptoms will be relieved.
2) Perform the Toynbee maneuver:
Like the Valsalva maneuver, the Toynbee maneuver aims to open the blocked Eustachian tube but Instead of changing the air pressure through each breath, it relies on adjusting the air pressure as you swallow. To perform this maneuver, do the following:=
- Pinch your nose,
- Take a sip of water,
- Swallow it,
Repeat this process until you feel your ears pop and open back up.
3) Blow up the balloon through the nose := This process may seem silly, but it is true.
- It can be effective in equalizing air pressure in the ear. This device is just a simple balloon with a nozzle that fits into the nostril. If you have a nozzle around the house that will open the balloon and fit securely into the nostril, you can make an autovalve balloon at home.
- Insert the nozzle into one nostril and pinch the other nostril closed with your finger.
- Inflate the balloon using your other nostril until Inflate it until it is the size of a fist.
- Try repeating the process on the nostrils. Repeat until you hear the popping sound of the fluid being released into the Eustachian tube.
4) Pinch your nose and swallow:
- Also called the Lowry Daw Page and it’s a little harder than it sounds. Before swallowing, you have to increase the air pressure in your body, as if you were trying to have a bowel movement. While you hold your breath and try to expel air, the increased pressure in your body makes it difficult for some people to swallow. Be patient, however, and keep at it. With enough practice, you can open your ears. is.
5) Place a heating pad or warm washcloth against your ear.
- This can ease any pain you may be experiencing and treat the blockage. The gentle heat of the warm compress can help to break up the congestion by closing the U-shaped tube. If you use a heating pad, you may need to place a cloth between the heating pad and your skin to prevent burns.
6)use nasal decongestant:=
- Ear drops cannot relieve your congestion because they are blocked.
- Because the ear and nose are connected by tubes
- Sprays are an effective way to treat Eustachian tube blockage.
- The spray bottle is held almost perpendicular to the face through the nostrils toward the back of the throat while you When spraying a decongestant, try to use a suction device that is hard enough to pull the liquid down the back of the throat but not so hard that it can be swallowed or sucked into the mouth. Try a stimulating maneuver after using a decongestant. They may be more effective at this time.
