ENGLISH-CHILD HEALTH NURSING (CHN) 16/09/2025 PAPER SOLUTION NO.13 (UPLOAD)
Q-1
a) Define diarrhea & List out its types. Define diarrhea and list its types. 03
Diarrhea is a condition in which liquid, loose and watery stools are passed more than three times in a day (in 24 hours). And the frequency of these loose, watery stools is also high. Due to diarrhea, excessive amounts of fluid and electrolytes are lost from the body, which leads to the condition of dehydration.
{Diarrhea is a disease in which passage of loose, liquid or watery stool more than three times per day}.
types of the Diarrhea:
There are four main types of diarrhea.
1) Acute Diarrhea
2) Chronic Diarrhea
3) Persistent Diarrhea
4) Dysentery
1) Acute Diarrhea: Acute diarrhea is a condition in which the onset of diarrhea is sudden and of short duration and is accompanied by two It lasts for less than a week. Acute diarrhea is mainly caused by any infection.
2) Chronic Diarrhea: Chronic diarrhea is a condition in which loose watery stools are present for more than 3 weeks, it is called chronic diarrhea. Chronic diarrhea is due to any organic disease.
3) Persistent Diarrhea: Persistent diarrhea is a condition in which attacks of acute diarrhea are seen for more than two weeks and that diarrhea is caused by infection.
4) Dysentery: Dysentery is a condition in which blood, mucus and pus are present in the stool and is accompanied by abdominal colic, fever, and tenesmus (a condition in which there is a need to pass stool even though the bowel is already empty).
b) Write causes, signs & symptoms of diarrhea. 04
Etiology/ cause of the Diarrhea. (Causes of diarrhea):
Due to unhygienic conditions.
Due to infection.
Viral infection:
- Rotavirus,
- Enterovirus,
- Adenovirus,
- Measles virus.
- Influenza virus.
Bacterial infection (Bacterial infection):
- E coli,
- Caused by Shigella bacteria,
- Caused by Salmonella bacteria.
- Caused by Staphylococcus bacteria.
- Caused by Vibrio cholerae.
Parasitic infections:
- Entamoeba histolytica,
- Giardia lamblia,
- Cryptosporidium,
- P. falciparum, P. vivax, P. ovale and P. malariae.
Fungal infection:
- Caused by Candida albicans,
- Infectious condition
- Upper respiratory tract infection,
- Otitis media,
- Tonsillitis,
- Pneumonia,
Urinary tract infection.
Dietic and nutritional factors:
- Overfeeding,
- Due to starvation,
- Due to food allergy and food poisoning.
- Due to other predisposing conditions
such as,
Age,
Season,
Artificial feeding
Clinical manifestation/ sign and symptoms of the child with the Diarrhea :
- Frequent passing of loose watery stools.
- Dehydration,
- Abdominal pain.
- Low grade fever.
- Loss of appetite.
- Abdominal distension to occur.
- Behavioral changes such as
- irritability,
- restlessness,
- weakness,
- fatigue,
- not sleeping properly,
- Physical changes such as
- weight loss,
- poor skin turgor,
- dry mucous membranes.
- dry lips,
- paleness,
- sunken eyes,
- depressed fontanelle,
- Changes in vital signs Such as,
- Low blood pressure,
- Tachycardia,
- Rapid respiration,
- Cold limbs,
- Decreased urinary output,
- Loss of consciousness,
- Dry mucous membranes
- Sunken eyes
- Decreased skin turgor and positive late test
- Absence of tears while crying
- Decreased urine output or Oliguria
- Increased pulse rate and weak pulse
- Increased capillary refill time Have
- The patient appears lethargic or irritable
- Patient feels depressed when palpating the fontanel in a pediatric patient
- Skin feels dry and cold
c) Explain nursing management of patient with diarrhea. Explain the nursing management of a patient with diarrhea.05
Nursing management of patient with diarrhea. Nursing management of a patient with diarrhea
- Provide rehydration therapy to the child.
- Provide oral rehydration solution (ORS) to maintain the child’s hydration status.
- Oral rehydration therapy is considered an effective treatment for mild to moderate dehydration.
- Provide intravenous fluid therapy to the child.
- If the child has a condition of dehydration and ORS therapy is not properly effective, then provide the child with intravenous fluid therapy.
- Provide the child with proper feeding along with intravenous therapy to prevent malnutrition.
- Provide easily digestible food to the child who can take food by mouth.
- Ex: Toast, rice, blanched food.
- Maintain adequate fluid and electrolyte levels in the child.
- Provide antibiotic medicine if the child has diarrheal disease due to any bacterial infection.
- Provide antidiarrheal medicine to the child
- Such as,
- Loperamide,
- Bismuth Subsalysilate.
- Properly assess the child.
- Assess the severity of the diarrheal disease.
- Assess the frequency, volume, and consistency of diarrhea.
- Assess the child for any symptoms of dehydration.
- Properly assess the child. Maintain fluid and electrolyte levels.
- Provide proper nutritional support to the child.
- Provide continuous breast-feeding to the child.
- Provide proper medication to the child.
- Provide antibiotic medication if the child has diarrhea due to any bacterial infection.
- If the child has any parasitic infection, provide antiparasitic medicine.
- Advise the child to practice proper hand hygiene techniques to prevent infection.
- Continuously monitor the child.
- Provide education to the child’s parents on safe water and food handling to prevent diarrheal conditions.
- Children’s Advise parents to provide regular medication to the child.
- Prevention care of the Diarrhea:
- Advise parents to provide adequate breast feeding to the child.
- Advise parents of the child to maintain proper hand hygiene.
- Advise parents of the child to properly use safe water and Prepare food hygienically.
- Provide proper hygienic bottle fitting to the child.
- Advise the child’s parents not to use any kind of pacifier.
- Advise the child’s parents to maintain strict personal hygiene.
- Advise the child to keep the child’s nails short and to keep the child’s hands and toys clean at all times. Giving advice.
- Providing adequate fluids to the child.
- Providing education to parents to provide easily digestible foods such as rice, dal, soup, coconut water to children.
- Advise parents to provide homemade ORS solution to the child, if necessary.
- Advise parents to provide regular medication to the child.
OR
a) Explain classification of congenital heart disease. Explain classification of congenital heart disease. 03
Classification of congenital heart disease:
Cyanotic and Acyanotic Condition
Introduction :
Congenital Heart Defects are mainly of two types: Cyanotic Condition and Acyanotic Condition. Both the conditions differ according to the level of blood flow and oxygenation in the cardiac field of the patient. The main difference depends on the amount of oxygen in the patient’s blood and the resulting cyanosis seen on the skin.
Cyanotic Condition:
Cyanotic condition is a condition in which deoxygenated blood mixes with oxygenated blood inside the patient’s heart and oxygen-depleted blood reaches various parts of the body. Due to this, a bluish color appears on the patient’s lips, nails and skin, which is called cyanosis.
This condition usually involves Right to Left Shunt, in which deoxygenated blood from the right side of the heart goes directly to the left side and is pumped through the body.
For example:
Tetralogy of Fallot, Transposition of Great Arteries, Tricuspid Atresia, Total Anomalous Pulmonary Venous Return, etc.
Symptoms:
- Lips, Nails and Skin appear blue (cyanosis)
- Oxygen saturation is less than 85%
- Patient gets tired quickly
- Increased respiratory rate
- Growth delay is observed
Acyanotic Condition:
In an acyanotic condition, the patient’s heart has abnormal blood flow but there is no direct effect on the oxygenation of the blood. That is, only oxygenated blood flows in the patient’s body and cyanosis is not observed.
In this condition, a Left to Right Shunt is usually seen, in which oxygenated blood from the left side turns to the right side and returns to the pulmonary circulation.
For example:
Atrial Septal Defect, Ventricular Septal Defect, Patent Ductus Arteriosus, Atrioventricular Canal Defect, etc.
Symptoms:
- No blue discoloration is visible in the skin
- Oxygen saturation is normal (≥ 95%)
- The patient has little respiratory distress
- Symptoms of pulmonary congestion and heart failure are seen Is
- Sometimes a gurgling sound and a murmur are heard
The main difference between Cyanotic and Acyanotic Cardiac Conditions is that in Cyanotic, the patient’s body has oxygen-depleted blood circulating in it, causing cyanosis, while in Acyanotic, there is a silent disorder within the heart despite having oxygenated blood. Both types of conditions can be severe for pediatric patients and require immediate medical and surgical intervention. As a nurse, it is a very important responsibility to understand this difference and provide proper observation and care to the patient.
b) Write clinical manifestation & diagnostic evaluation of tetralogy of fallot. Write the signs, symptoms and diagnostic evaluation of Tetralogy of Fallot.04
Tetralogy of Fallot is a congenital heart defect. In which four heart defects are found together in a child.
1) Ventricular septal defect,
2) Pulmonary stenosis,
3) Overriding aorta,
4) Right ventricular hypertrophy.
••>
1) Ventricular septal defect:
In ventricular septal defect, there is an abnormal opening in the septum separating the right and left ventricles.
2) Pulmonary stenosis:
In pulmonary stenosis, the pulmonary artery (the blood vessel that carries deoxygenated blood from the right ventricle to the lungs) narrows, which obstructs the blood flow from the right ventricle.
3) Overriding aorta aorta):
Overriding of aorta is a condition in which normally the aorta (the main blood vessel that carries oxygenated blood from the heart to the body) originates from the left ventricle of the heart, but in overriding of aorta, the aorta originates directly above the ventricular septal defect on the left ventricle.
4) Right ventricular hypertrophy:
When the pulmonary artery (A blood vessel that carries deoxygenated blood from the right ventricle and delivers blood to the lungs for oxygenation) narrowing and stenosis occurs, which requires the right ventricle of the heart to do extra work (pumping) to deliver blood from the right ventricle to the lungs. Due to this extra pumping, the muscles of the right ventricle of the heart thicken, which is called hypertrophy.
Clinical manifestation/ Sign and symptoms of the Tetralogy of Fallot (Tetralogy of Fallot for symptoms and signs).
- Cyanosis,
- Bluish discoloration of lips, skin, and nails,
- Shortness of breath,
- Clubing,
- Fatigue,
- Poor growth,
- Breathing difficulty,
- Abnormal murmur sound,
- Irritability,
- Dyspnea,
- Episodes of cyanotic spells (tat spells) including cyanosis, hypoxia and breathing difficulties in the child after feeding and any painful procedure,
- Polycythemia,
- Child’s skin becomes rough and clammy.
Diagnostic evaluation of the Tetralogy of Fallot.
- History tacking and physical examination, pulse oximetry, heart sound scultation,
- Electrocardiogram (ECG),
- Echocardiography,
- Chest X-ray,
- Cardiac Magnetic Resonance Imaging (MRI),
- Cardiac Catheterization.
c) Explain the management of patient with tetralogy of fallot. Explain the treatment of a patient with Tetralogy of Fallot.05
Medical management of the Tetralogy of Fallot.
- Provide proper oxygen to the child to treat his hypoxic condition and cyanosis.
- Provide proper sedative medicine to the child.
- Provide proper sedative medicine to the child.
- Provide proper intravenous fluids.
- Properly treat the child’s dehydration.
- Properly treat the child’s anemia.
- Properly position the child in the supine position to treat hypoxic spells.
- Administer intravenous vasopressors such as methoxamine to the child.
- If the child has a condition called severe technology of Fallot, provide the child with intravenous prostaglandin E1. This causes dilation of the ducts and increases pulmonary blood flow.
- If the child has a condition of acidosis, treat it properly.
Surgical management of the Tetralogy of Fallot.
- Surgical management of the Tetralogy of Fallot usually involves correcting the defect and providing palliative procedures. Performing this procedure increases blood flow to the lungs and treats the condition of cyanosis.
- The most common surgeries involve intracardiac repair and complete repair.
Complete Intracardiac Repair
- Complete intracardiac repair is the preferred surgical procedure to treat most of the conditions of Tetralogy of Fallot. In this procedure, the ventricular septal defect is treated with a patch. Then the obstruction of the pulmonary artery that has been stenosed is relieved so that blood can be properly transported from the right ventricle to the lungs, and then the overriding of the aorta is provided for repositioning. The aim of this procedure is to improve blood flow to the lungs and treat the child’s condition properly. 2. Blalock tossing or modified Blalock tossing stent.
- Blalock tossing stent is used in conditions where it is impossible to completely repair the condition of tetralogy of Fallot. In this procedure, a connection is made between the subclavian artery, innominate artery, and pulmonary artery, which can improve blood flow to the lungs.
Pulmonary valve stenosis
- In pulmonary valve stenosis, the stenosis of the valve is properly repaired.
Nursing management of the Tetralogy of Fallot
- Properly monitor the child.
- Properly assess the child’s vital signs.
- Properly assess the child’s cardiac function.
- Properly assess the child’s symptoms such as breathing difficulty, sweating, and fatigue.
- To the child’s parents Provide complete education about the child’s condition, its causes, symptoms and signs, its treatment and lifestyle modifications.
Preoperative Nursing Management
- Provide proper positioning of the child.
- Provide oxygen to the child.
- Properly position the child. Provide psychological support.
- Regularly monitor the child’s blood oxygen level.
- Provide proper protection to the child to prevent infection and trauma.
- Provide complete education to the child’s parents and caregivers about the child’s condition, its causes, symptoms, and signs.
- Proper aseptic technique for the child Provide maintenance care.
- Provide intravenous fluids to maintain the child’s nutritional status.
- Properly clothe the child to prevent hypothermia.
- Properly provide antibiotic medicine to prevent infection.
Postoperative Nursing Management
- Properly close monitoring of the child.
- Continuously monitor the child’s vital signs.
- Continuously monitor the child’s intake output chart.
- Provide adequate intravenous fluids to maintain the child’s nutritional status.
- Provide adequate respiratory support to the child.
- Properly administer oxygen to the child.
- Properly suction to keep the child’s airway clear.
- Continuously maintain the child’s body temperature and avoid exposing the child to the external environment.
- Provide a nutritious diet to the child.
- Maintain proper hygienic conditions to prevent the child from infection.
- Provide dressings by maintaining proper aseptic technique on the operative side.
- Monitor the child’s daily weight.
- Continuously monitor the child for any complications.
- The child Provide education to the parents to provide adequate care.
- Provide complete education to the parents about the child’s condition.
- Provide proper psychological support to reduce anxiety of the child and his family members.
- Advise the child’s parents to provide the prescribed medication to the child.
- Provide proper psychological support to the child’s parents.
- Advise the child’s parents to follow up regularly.
Q – 2
a) Define exclusive breast feeding and explain advantages of breast feeding. Define exclusive breast feeding and explain advantages of breast feeding. 08
Exclusive Breastfeeding:
Introduction:
Breastfeeding is the first and most important nutritional method of life for a newborn.When a baby is given only breast milk for the first 6 months after birth and no water or food of any kind is given. It is scientifically called “Exclusive Breastfeeding” Breastfeeding contains many important nutrients and immunological components.
Medical Benefits of Breastfeeding:
1.Benefits for the Infant:
Colostrum:
The thick yellow milk secreted in the first few hours and days after birth is called colostrum. This milk is rich in antibodies, which protect the infant from diseases like infection, diarrhea, and pneumonia.
Immunity:
The immunoglobulins, lactoferrin, lysozyme, etc. present in breast milk help in increasing the immunity of the infant.
Cognitive Development: Research shows that neurological development is better in breastfed babies.
Lower risk of obesity and diabetes:
Breastfed babies are at a lower risk of type 1 and type 2 diabetes and childhood obesity.
2. Benefits for the Mother:
Uterine Contraction:
A hormone called oxytocin is released during breastfeeding, which quickly returns the uterus to its original size and helps in the contraction of the uterus after delivery. Reduces Postpartum Hemorrhage.
Lower risk of breast and ovarian cancer: Females who breastfeed for a long time have a reduced chance of developing this type of cancer.
Calorie Burn:
During breastfeeding, the mother burns approximately 500 calories per day, which is helpful in reducing weight after pregnancy.
Important Medical Recommendations: World Health According to the World Health Organization (WHO), a baby should be given only breast milk for the first 6 months after birth.
Complementary feeding should be started after 6 months and breastfeeding should be continued for at least 2 years.
Breastfeeding is not just a nutrition method, but the beginning of a healthy lifestyle for both mother and child. The nutrients, antibodies and hormones it contains contribute significantly to the physical and mental development of both. Every mother should encourage breastfeeding under medical guidance.
b) Nurses responsibility in prevention of accidents in children. Explain the role of nurses in preventing accidents in children. 04
- Providing information about a safe environment to the child’s parents so that they can take special care of things that can harm children.
- Explaining to the parents that as the child grows older, his movement capacity will increase and he becomes high-risk for any accident.
- Convince the parents not to leave the child alone at any time and to supervise him constantly.
- Stay with the child during every activity of the child and assist him.
- Explain to ensure that electrical plugs and wiring in the house are not exposed.
- Explain to ensure that no small parts of the child’s toys are loose and that no other objects in the house are in a position that a small child can reach, so that the risk of foreign body aspiration can be reduced.
- Explain to ensure that no sharp objects are exposed or lying around in the house.
- Explain to ensure that hot items or cooking utensils are not within the child’s reach.
- Make sure that water containers around and inside the house are not full and that water tanks or reservoirs are not open.
- Encourage the child to play in an open space or field with supervision for sports. Explain to the child not to play games in the home environment.
- Keep any cord or long objects that can get entangled in the child’s neck out of his reach.
- Never put any inedible or poisonous items in the food container and keep all these items under lock and key out of the child’s reach.
- If any container contains inedible items, label it with a danger label and explain to the child.
- Mother and father should take steps to prevent accidents in children and be safe Special education should be given for the environment. So that mortality and morbidity due to accidental injuries in children can be reduced.
OR
a) Write down nursing management of acute respiratory infection. Write the nursing management of acute respiratory infection.08
Nursing Management of Acute Respiratory Infection:
Acute respiratory infection is a sudden infection of the respiratory system, affecting the nose, neck, trachea or lungs. These include diseases like common cold, bronchitis and pneumonia.
1.Assessment – Assessment:
- Checking vital signs — temperature, pulse, respiratory rate, blood pressure
Measuring oxygen saturation. - Checking for dyspnea (difficulty breathing).
- Auscultation for wheezing, crepitus Check.
- Observe the color and quantity of sputum.
- Check for the presence of cyanosis.
2.Airway Management Airway Management:
- Provide Semi-Fowler’s Position.
- Suction as needed.
- Do Deep Breathing and Coughing Exercise.
- Give Nebulization
3.Oxygen Therapy
- Give oxygen if oxygen saturation is less than 94%.
- Give oxygen through a nasal cannula or mask.
- Keep the Flow Rate as per the doctor’s orders.
- Give Humidified Oxygen.
4.Medication Administration – Medication Administration
- (Antibiotics)
- (Antipyretics)
- (Bronchodilators)
- (Mucolytics)
- (Antihistamines) Right patient, right Follow the rules of drug, right dose, right route, right time.
5.Fever Management – Fever Management.
- Measure temperature regularly (Lukewarm Sponging).
- Give adequate fluids.
- Give antipyretics on time.
6.Fluid and Nutritional Management – Fluid and Nutritional Management
- Give oral fluids.
- Give intravenous fluids if necessary.
- Give a nutritious and easily digestible diet.
- Give frequent small amounts of food.
7.Infection Control – Infection Control:
- Maintain Hand Hygiene.
- Wear a mask (follow Droplet Precautions).
- Teach Cough Etiquette.
8.Rest and Monitoring – Rest and Monitoring
- Provide adequate rest.
- Regular monitoring of respiratory rate and oxygen saturation to watch for complications such as respiratory failure.
9.Health Education – Health Education:
- Explain the importance of taking medicines on time.
- Explain the importance of adequate rest and nutrition.
- Avoid smoking.
- Provide education about vaccination.
Maintaining airway, providing adequate oxygen, administering medications on time, controlling transmission and preventing complications are the main objectives in the nursing management of Acute Respiratory Infection.
b) Write down causes, sign & symptoms of nephrotic syndrome. Write the causes, sign & symptoms of nephrotic syndrome.04
Nephrotic syndrome:
Nephrotic syndrome is a combination of two words.
-
- Nephron Meaning the basic structure of the kidney.
-
- Syndrome Meaning a group of symptoms.
Nephrotic syndrome in children is a kidney disorder in which the glomeruli, which are the filtering units of the kidneys, are damaged or the permeability of the glomeruli increases, leading to the excretion of protein from the body through urine, mainly albumin.
This excretion of protein from the body through urine leads to a decrease in the amount of protein in the blood, which causes swelling in the feet, particularly around the ankles and abdomen, causing a condition called edema. Due to which the lipid and cholesterol levels in the blood also increase.
Nephrotic symptoms are a collection of symptoms that are mainly seen due to damage to the glomeruli in the kidneys.
There are mainly four symptoms seen in nephrotic syndrome.
1) High levels of protein are excreted from the body in the urine (proteinuria).
2) Decreased amount of protein in the blood. (Hypoalbuminemia).
3) Increase in the amount of lipids in the blood (Hyperlipidemia).
4) Swelling in the body part (in the heel).
These four main symptoms are seen in nephrotic syndrome.
Nephrotic syndrome affects people of any age. It is mainly seen in children between the ages of 1 and 7 years.
Causes of Nephrotic Syndrome. Causes of Nephrotic Syndrome
- Due to glomerular disease,
- Due to hereditary conditions,
- Certain types of diseases such as cardiovascular disorders, damage to the small blood vessels of the kidneys,
- Certain types of disease conditions are more common in children, mainly
- Due to abnormal kidney function,
- Due to diabetic kidney disease,
- Due to certain types of infections,
- Due to medication,
- Focal segmental glomerulosclerosis (FSGS),
- Scattered scarring of Glomeruli,
- Membranous nephropathy,
- Caused by heart failure, certain diseases such as hepatitis B, hepatitis C, malaria, etc.
signs & symptoms of Nephrotic Syndrome. Nephrotic Syndrome Signs and Symptoms
- Swelling.
- Weight gain.
- Swelling is mainly seen in the lining of the eye socket and around the eye (in the periorbital area).
- Swelling is mainly seen in the feet and ankles due to sitting or standing for long periods of time.
- Face and puffiness.
- Proteinuria.
- Hypoalbuminemia.
- Hypercholesterolemia.
- Diarrhea.
- Vomiting.
- Anorexia.
- Liver Enlargement.
- Increase in blood pressure.
- Anemia.
- Infection of the respiratory tract, peritoneum and skin.
- Skin becomes pale.
- Skeletal muscles become wasting.
- Many times in the wall body also Swelling is seen which is called Anasarka.
- Ascites,
- Pitting edema,
- Oliguria (decreased urine output).
- Weight gain.
- Hematuria (blood in urine.)
- Respiratory Distress
- Increase in blood pressure.
- Kidney failure.
- Increase in cholesterol levels in the body.
- Fatigue.
- Immediate infection.
- Loss of appetite.
- Feeling tired.
Q-3 Write short answer (any two) Write a short answer. (Any two)6+6=12
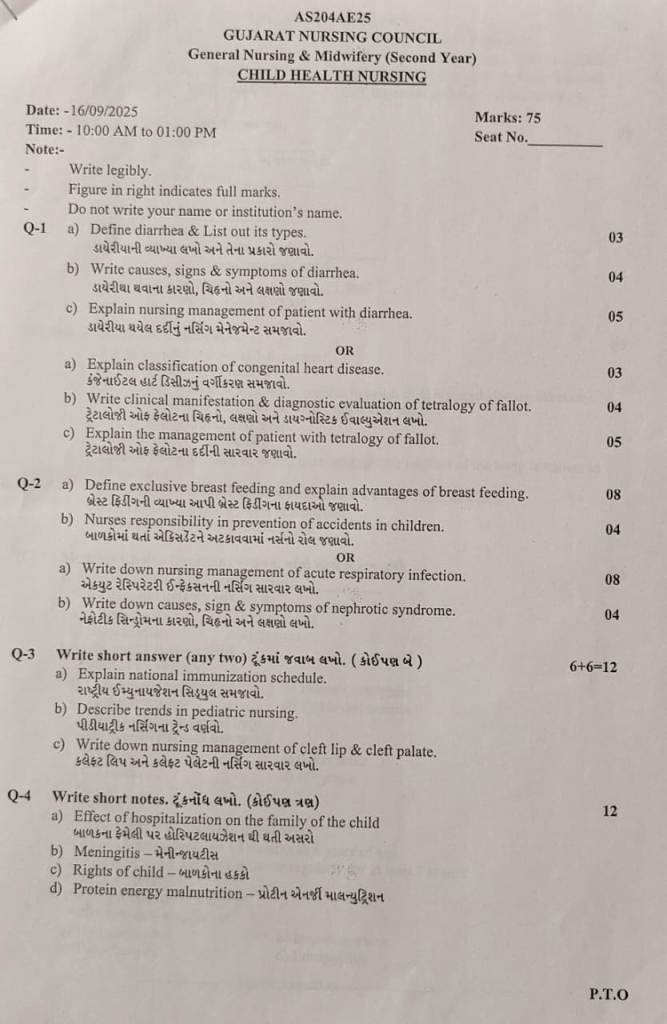
a) Explain national immunization schedule. Explain National Immunization Schedule.
b) Describe trends in pediatric nursing. Describe trends in pediatric nursing.
- In the past, adults and children were given the same treatment. But currently, due to the high mortality and morbidity seen in the pediatric age group, more importance has been given to children and child care.
- In addition, due to the development in the medical and surgical branches, the focus is on the special area of child health.
The following trends and practices are being seen in child health care in pediatrics. - Currently, pediatric care is provided by pediatricians and trained registered nurses.
A scientific treatment approach is maintained in care from infancy to adolescence period. is. - Special vaccines are administered for the prevention of diseases.
Regular assessment of the child’s growth and development is done. - Instead of curative care, emphasis is placed on preventive services and health promotion.
Advancement of technology and science is seen in the medical field. So that high quality care can be provided. - Evidence-based practice is seen in the care of children.
More emphasis is placed on institutional care instead of home care for any kind of care for children. This institute i.e. hospital which has been developed with changes that are liked by children through modernization. - Family-centered care is provided in every care of the child under the supervision of health care members with the support of parents and family members. Even during illness, the child is not separated from his parents and family members.
- Rooming in, that is, keeping the child with his mother as much as possible and keeping the mother with him in every care, is implemented.
- During the hospitalization of children, their visiting hours have been increased and flexible hours have been kept.
- There is a support group for parents, which helps in reducing the anxiety of the parents. And the play and recreational needs of children are taken into consideration.
- In the care of children, subspecialties of pediatric services such as pediatric neurology, cardiology, nephrology, etc. have developed.
c) Write down nursing management of cleft lip & cleft palate:
Airway clearance
- Provide proper upright position to the child. Provide proper hand support to the child’s head, which reduces the possibility of aspiration and ensures proper clearance of the child’s airway.
Feeding support
- Child has sucking problems due to conditions like cleft lip and left palate, due to which proper feeding should be provided. Use special cleft nipple to maintain the feeding condition of the child. Use special types of bottles and feeding devices.
Hearing Monitoring
- A child with a condition called cleft palate is more likely to develop middle ear infections. Therefore, assess the child’s hearing ability.
Speech therapy
- Children with cleft palate have speech difficulties, so provide proper speech therapy to the child.
Dental care
- If a child has a condition like cleft lip and left palate, there is a possibility of teeth malplacement, so the child should be provided with proper dental care.
Psychological Support
- If the parents of a child with a condition like left cleft palate and cleft palate are emotionally disturbed, then the parents should be provided with proper psychological support, counseling, emotional support and social support.
Monitoring and Follow-up
For proper care of the child, the parents should be provided with proper psychological support, counseling, emotional support and social support. Advise for regular follow-up.
Preoperative Nursing Management
- Follow the “Rule of Ten” before surgery for a child with a left cleft palate.
(10 weeks of age, 10 lbs of weight, 10 gm% of hb). - If the child has a cleft palate, then 12 months, weight is 9 kg (20 lbs) and 10 gm of Hb %.
- The child should be completely immunized before surgery.
- If the child has a habit of thumb shaking, then give advice to prevent thumb shaking.
- Advise the mother on sterile breastfeeding technique.
- Advise the mother to provide the best feeding to her child properly.
- Comfort of the child Provide proper positioning of the child for the level.
- Advise the child to provide proper love and affection to the child.
Post-operative Nursing Management
- Continuously monitor the child’s vital signs.
- Provide general post-operative care to the child To do.
- Provide proper side lining position to drain secretions and prevent aspiration of the child.
- Provide proper protection to the surgical site of the child.
- Use proper protective device on the sutured side.
- Provide proper supine position and position on the unaffected side.
- Provide proper elbow restraint to the child.
- Advise the child’s parents to provide proper love and affection to the child and advise the parents to provide support to the child.
- Advise the child to provide feedings through a medicine dropper properly.
- Advise the child’s parents to maintain proper upright position of the child after feedings. Keep.
- Advise the child to maintain aseptic technique to prevent infection in the child.
- Advise the parents to maintain proper hygiene while handling the child.
- Advise the parents to provide proper assistance when providing feeding for the child.
- If possible, advise the parents of the child to use special cleft palate nipples Give advice to parents to provide proper love and affection to their children.
- Advice to parents to provide proper love and affection to their children.
Q-4 Write short notes. Write short notes. (Any three) 12
a) Effect of hospitalization on the family of the child
Effect of hospitalization on the family of the child
Parents whose children are hospitalized not only feel separated from their children but also feel that other people are taking their place.
Furthermore, they feel a sense of inadequacy because other people are taking care of their children.
Family unity is also broken due to the child being hospitalized, and the parents experience anxiety and guilt over the child being separated from their parents.
If a child is hospitalized, the stress level of their parents and family members increases.
1) Mainly due to many factors, the stress level of parents increases. Such as,
A) Parents do not have proper information or knowledge about what kind of illness their child has.
B) Parents are also afraid of what kind of procedures their child will undergo in the hospital.
C) Parents are also afraid of what kind of treatment their child will be provided with. There will be.
D) Parents also fear what will happen to their child in the future, which increases their stress level.
E) When a child is hospitalized, the cost of his treatment can also be very high, due to which the financial burden on the parents comes, but the stress in the parents increases.
2) Many times, parents feel guilty that their child’s illness is due to the parents not taking proper care of him and any kind of defect in the care of the child.
3) Parents of a child who is hospitalized experience anxiety, fear, disappointment, and blame themselves.
4) When a child is treated, they are separated from their parents, which makes the parents feel helpless because they are unable to provide care for the child.
5) Often, parents of hospitalized children also become angry with the health care personnel.
6) Parents also experience anxiety due to certain causes such as the strange environment of the hospital. Separation of parents and child. Child’s illness. Different types of procedures performed in the hospital. Due to unknown events and outcomes. Due to the child suffering from any illness. Due to the parents not being able to take care of their child.
b) Meningitis – Meningitis
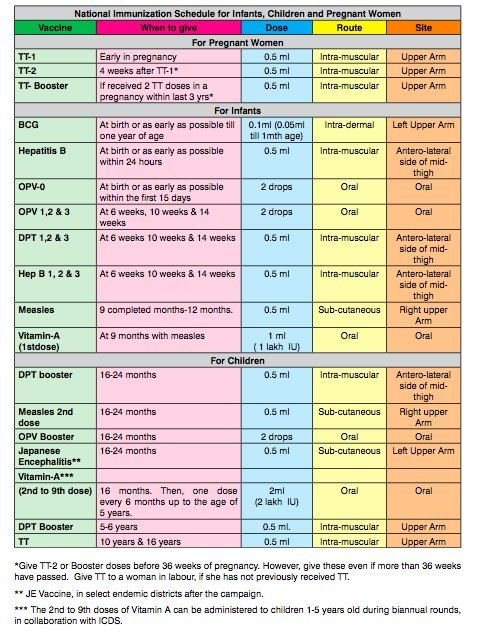
Meninges:= Meninges are the protective membranes of the brain and spinal cord that cover the brain and spinal cord.
These meninges have three other layers.
1) Duramater (outermost layer),
2) Arachnoid mater (intermediate layer),
3) Pia mater (innermost layer)
Thus, there are three layers of meninges that cover and protect the brain and spinal cord.
Meningitis:=
When the meninges, the layer of tissue that surrounds the brain and spinal cord, become infected and inflamed, the condition is called meningitis. This infection can be caused by bacteria, viruses, and microorganisms.
Etiology/ cause of the meningitis.
Due to bacterial infection.
Ex:=
- Mycobacterium Tuberculosis ,
- Streptococcus pneumoniae,
- Neisseria meningitidis,
- Haemophilus influenzae,
- Listeria monocytogenes.
Due to viral infection.
- Mumps,
- Herpes simplex viral,
- Epstain barr virous,
- Varicella-zoster viral ,
- Measles,
- Influenza.
Due to fungal infection.
- Candida,
- Due to systemic lupus erythematosus (SLE),
- Some types of medication Due to.
- Head injury.
- Head and spinal cord trauma.
- Cancer.
- Tobacco use.
- Immune system impairment.
- Overcrowding Due to.
- Due to brain surgery.
Clinical manifestation/ sign and symptoms of the patient with the Meningitis. (Meningitis symptoms and signs).
- Headache,
- Very high fever,
- Maintenance status altered. Confusion.
- Altered consciousness.
- Vomiting.
- Photophobia (an inability to tolerate light).
- Irritability.
- Drowsiness.
- Confusion Occur.
- Altered consciousness.
- Vomiting.
- Sign of meningeal irritation.
- Knuckle rigidity (neck stiffness).
- Headache.
- Altered mental status to occur.
- to be surprised.
- to have joint pain.
- to have muscle contraction.
Positive Brudzinski sign
In the Brudzinski sign, when the child is placed in a supine position and his neck is flexed towards the chest, his hip and ankle automatically The flexion is called the Brudzinski sign.
Kerning sign
In the Kerning sign, when the patient is provided with a supine position, after which the patient’s knee and hip are flexed, if the patient’s knee is extended again and he feels pain, it is called the Kerning sign.
K:= Knee,
E:= Extention
R:= Resistense
That is, when the knee is directly extended, the patient feels pain. It happens.
Diagnostic evaluation of the Child with the Meningitis. (Diagnostic evaluation of the child with meningitis).
- History taking and physical examination.
- Blood culture.
- Lumbar puncture.
- Chest X-ray.
- CSF examination.
- CT scan.
- Gram stain.
- CSF culture.
- MRI test.
Management of the Children with the Meningitis.
- Provide antibiotic medicine if the child has any bacterial infection.
- Ex:=
- Rifampicin ,
- Cefotaxime,
- Vancomycin.
- If the child has any viral infection, then provide antiviral medicine.
- If the child is in pain, then provide analgesic medicine.
- Ex:= Acetaminophen,
- NSAID ( Non steroidal anti inflammatory drug).
- Provide intravenous fluid to the child.
- If the child has fever, then provide antipyretic medicine To do.
- If the child has a fever, provide anticonvulsant medication.
- Continuously close monitor the child.
- Continuously close monitor the child’s vital signs.
- If the child has inflammation, provide corticosteroid medicine.
- If the child has If there is a condition of meningitis, keep it properly isolated.
- Properly monitor the hydration status of the child.
- Properly provide nutritional support to the child.
- Properly provide intravenous fluids to the child.
Nursing management of Children with the Meningitis.
- Properly assess the child.
- Continuously monitor the child’s vital signs.
- Properly assess the child’s hydration status.
- Maintain the child’s proper fluid and electrolyte levels.
- Give analgesics if the child is in pain Provide medicine.
- Properly assess the child’s neurological status.
- Provide anticonvulsant medicine if the child is having seizures.
- Provide proper nutritional support to the child.
- Provide proper psychological support to the child.
- Educate the child about his/her disease, the possible causes of his/her illness, and the possible consequences of his/her illness. Provide proper education about the cause, symptoms and signs.
- Continuously monitor the child’s intake output.
- Continuously monitor the child’s vital signs and neurological status.
- Continuously monitor the child’s level of consciousness.
- Advise the child to take medicine regularly.
- Advise the child to follow up regularly.
- Provide proper psychological support to the child.
c) Rights of child – Rights of children
- The United Nations declared the Rights of the Child on 20 November 1959. They were created with the aim of fulfilling the special needs of the child in mind.
These rights are as follows. - Right to free education.
Right to name and nationality.
Right to receive special care if the child is handicapped.
Right to receive affection, love and good understanding.
Right to receive adequate quality nutrition.
Right to receive first aid or relief in times of any disaster or distress.
Right to receive good medical care.
Right to play well and to have recreational facilities.
Ability to The right to develop and become a useful member of society. The right to be brought up in a peaceful and fraternal environment. The right to enjoy all the above rights equally without discrimination of religion, caste, creed, sex, color, etc. Children have also been given the right to exercise all the rights.
d) Protein energy malnutrition – Protein energy malnutrition
Protein energy malnutrition (PEM) is a nutritional problem in a child that is first diagnosed as protein calorie malnutrition. (PCM) which is caused by inadequate intake of protein and calories in the diet, resulting in impairment in the child’s growth, development and overall health.
There are two main types of PEM.
1) Marasmus
2) Kwashiorkor
1) Marasmus
The Marasmus of PEM is caused by severe calorie deficiency, which results in weakness, loss of muscle mass, and wasting of body tissues.
Children with Marasmus usually look very thin and have a “starved” appearance.
2) Kwashiorkor
Kwashiorkor is a form of PEM that occurs due to severe protein deficiency despite adequate calorie intake.
Children with kwashiorkor have a swollen abdomen (edema) due to water retention, fatty liver, skin lesions, and stunted growth. And a child with quasi-seroconstriction is normal but has a higher body weight than marasmus.
Classification of the child with the Protein energy Malnutrition. (Classification of Protein Energy Malnutrition)
A) Syndromal Classification
There are a total of five types of syndromal classification.
1) Nutritional Marasmus,
2) Kwashiorkor,
3) Nutritional Dwarfing,
4) Marasmic Kwashiorkor,
5) Pre Kwashiorkor
1) Nutritional Marasmus
Nutritional Marasmus is a severe form of protein energy malnutrition.
In which chronic starvation is observed and the intake of both protein and calories is inadequate.
The condition of nutritional Marasmus is mainly seen when there is extreme poverty, food insecurity, and access to nutritious food is low.
2) Kwashiorkor,
Kwashiorkor is a form of PEM It is caused by severe protein deficiency despite adequate calorie intake.
Children with kwashiorkor have water retention, which causes a swollen abdomen (edema), fatty liver, skin lesions, and stunted growth. And children with quasi-serocorticism are normal but have a higher body weight than those with marasmus.
3) Nutritional dwarfing,
Nutritional dwarfing is also called stunted growth and growth retardation.
Nutritional dwarfing is a manifestation of protein allergy malnutrition (PEM) in children. It is a condition where children fail to achieve their expected growth due to inadequate intake of essential nutrients including protein and calories.
Nutritional dwarfing is mainly seen during the period of growth and development of a child such as infancy and early childhood.
It causes skeletal growth delay of the child, short stature,
delayed puberty, cognitive deficit,
etc.
4) Marasmic Kwashiorkor,
Marasmic Kwashiorkor is a severe form of protein energy malnutrition. It has combined features of marasmus and kwashiorkor. This condition of marasmic kwashiorkor is mainly seen in children when there is prolonged and severe malnutrition.
And is mainly seen due to extreme poverty and food insecurity.
5) Pre-kwashiorkor
“Pre-kwashiorkor” involves the early stage or warning sign of kwashiorkor, which is a severe form of protein-energy malnutrition (PEM). It is an early sign of kwashiorkor. In prekwashiorkor, children may show signs of moderate to severe malnutrition.
B) Indian Academy for Pediatric (IAP) Classification .
Indian Academy for Pediatric Classification is mainly based on the weight of the child.
Grade:=1 (Mild Malnutrition)The child’s weight is 70-80% of the expected weight.
Grade:=2 (Moderate Malnutrition) The child weighs 70-60% of the expected weight.
Grade:=3 (Severe Malnutrition) The child weighs 60-50% of the expected weight.
Grade:=4 (Superior) The child weighs 50% less than the expected weight.
When the weight of a child is more than 80% of the expected weight for his age, he is said to be normal.
C) Gomez Classification
The Gomez classification is based on the weight of the child according to his age. In Gomez classification, when the expected weight is more than 90% according to age, it is called normal.
First degree: – Weight between 90 – 75% of expected.
Second degree: – Weight between 75-60% of expected.
Third degree: – Weight less than 60% of expected.
D) International classification
Expected weight is between 80 and 60%.
With AD:- Kwashiorkor,
Without AD:=Undernutrition,
If weight is below 60% of expected weight with AD:= Marashmic Kwashiorkor
If weight is below 60% of expected weight and Without AD := Nutritional Marasmus .
E) Arnold Classification
Arnold Classification is mainly based on Mid Arm Circumference.
Mild to Moderate := If Mid Arm Circumference is between 12.5-13.5 cm.
Severe:= If Mid Arm Circumference is Less than 12.5 centimeters.
Marasmus
Marasmus is a word derived from the Greek word “marasmos” meaning wasting.
In PEM (Protien Energy Malnutrition), marasmus is caused by severe calorie deficiency, which results in weakness, loss of muscle mass, and wasting of body tissues and subcutaneous fat. Loss occurs.
Children with Marasmus are usually very thin and have a
” Starved “ appearance.
In Marasmus, the child loses more than 50% of their expected weight for their age.
Etiology / cause of the Marasmus
- Due to an inadequate diet,
- Calories in the diet are inadequate Due to taking in large amounts,
- Due to poor feeding,
- Due to certain medical conditions,
- Such as chronic vomiting,
- Due to chronic infections,
- Ex := syphilis, tuberculosis, upper respiratory infections,
- Due to certain types of environmental factors,
- Due to poverty,
- Marasmus is most commonly seen in infants,
- Due to congenital diseases such as cleft palate hydrocephalus, Hisprung’s disease, etc.,
- Due to certain types of metabolic disorders such as galactosemia.
Classification of the Marasmus. (Classification of Marasmus)
There are a total of 4 classifications of Marasmus according to the grade.
1) Grade-1 :=
In this grade, there is loss of fat from the axilla and groin area.
2) Grade-2 :=
In this grade, there is loss of fat from the axilla and groin area Fat loss occurs from. Along with this, fat loss also occurs from the abdominal and gluteal regions.
3) Grade-3 :=
In this grade, fat loss occurs from the axilla and groin area. Along with this, fat loss also occurs from the abdominal and gluteal regions. Along with this, the fat of the chest and spine also gets involved.
4) Grade-4 := In this grade, there is involvement of the first three grades along with loss of the fat of the bucklepad.
Clinical manifestation / sign and symptoms of the child with the Marasmus. (Symptoms and signs of Marasmus)
- Severe wasting of body tissues,
- Loss of subcutaneous fat,
- The child becomes very thin,
- Facial features become shrunken,
- Child’s growth Retardation,
- Developmental delay in the child,
- Subcutaneous fat loss from the child’s buttocks, abdomen, thighs.
- Face looks aged.
- Fat loss from the child’s cheeks.
- Child becomes irritable.
- Severe malnutrition in the child.
- Electrolyte imbalance in the child.
- Neurological in the child
- Symptoms seen,
- The child becomes less active,
- The child’s spleen, Gonads,
- And the size of the liver is reduced,
- The child feels weak, tired, and exhausted.
- Changes in the child’s behavior are seen,
- Physical activity decreases,
- Extreme weight loss in the child,
Diagnostic evaluation of the child with the Marasmus. (Diagnostic Evaluation of Marasmus Vada Child)
- History taking and physical examination,
- X ray,
- Anthropometric measurement of the child,
- Laboratory investigation of the child,
- Complete blood count,
- Assess serum electrolyte and serum albumin tests,
- Properly perform imaging testing of the child,
Management of the child with the Marasmus. (Management of a child with marasmus)
- Provide adequate nutritional supplements to the child,
- Provide adequate high calorie feeding to the child.
- Advise the child to consume nutritious food.
- Maintain adequate fluid and electrolyte levels of the child To do.
- Provide adequate iron supplements to the child.
- Advise the child to gradually increase their diet.
- Provide adequate antibiotic medicine if the child has any infection.
- Provide adequate psychological support to the child.
- The child’s Record weight daily.
- Advise the child to provide adequate breastfeeding.
- Provide nutritious food like green leafy vegetables, soup, banana, pulses, cereals, milk etc.
- Provide the child with small and frequent amounts of diet.
- Provide adequate work and comfortable environment for the child To do.
kwashiorkor. (kwashiorkor )
Kwashiorkor is a form of severe protein energy malnutriment (PEM). Kwashiorkor is a form of PEM. Which is caused by severe protein deficiency despite adequate calorie intake.
Children with kwashiorkor have a swollen abdomen (edema) due to water retention, fatty liver, skin lesions, and stunted growth. Unlike marasmus, children with kwashiorkor are normal but have a higher body weight.
Kwashiorkor is also called “ Red Hairy Boy ” .
Kwashiorkor was first described by British physician Dr. Cicely Williams in 1933. But the specific term kwashiorkor was described in 1935.
The condition of kwashiorkor is mainly seen in preschool children.
The main symptoms of kwashiorkor are edema in the body due to fluid retention.
Etiology / cause of kwashiorkor (cause of kwashiorkor.)
- Due to poverty,
- Providing the child with the best fitting in an inadequate amount,
- Intake of protein rich food in an inadequate amount,
- Non-availability of protein rich food,
- Low socio-economic status Due to,
- Due to faulty feeding habits,
- Due to an unbalanced diet,
- Due to not consuming an adequate amount of nutritious diet,
- Due to certain medical conditions such as chronic infections,
- Gastro intestinal disorders, etc.,
- Due to some types of metabolic disorders,
- Due to environmental factors,
- Due to not providing the child with an adequate winning diet,
- Due to taking essential vitamins and minerals in inadequate amounts,
Clinical manifestation/ sign and symptoms of the child with the Kwashiorkor.
- Oedema (pitting edema) in the body is seen mainly in the lower extremities, upper extremities, abdomen, face etc.,
- The condition of bloated stomach is seen due to the collection of fluid in the abdomen,
- The skin becomes dry and scaly,
- Muscle wasting and muscle atrophy,
- Skin changes such as pigmentation,
- Hyperpigmentation, roughening of the skin, discoloration, etc.,
- Hepatomegaly (liver enlargement) in a child,
- Child’s appetite
- Decrease ,
- Behavioral changes in the child,
- Growth and development of the child being delayed,
- Skeletal growth of the child being impeded,
- Condition of anemia being observed in the child,
- Changes in the child’s hair,
- The child is not interested in any activity,
- Muscular wasting is seen in the child,
- The child’s face is swollen due to edema
- “moon face” is seen.
- Psychomotor changes are seen in the child,
- Intellectual impairment in the child,
Diagnostic evaluation of the child with the Kwashiorkor .
- History tacking and physical examination,
- Anthropometric measurements,
- Laboratory Test,
- Complete Blood Count Test,
- Serum Albumin Test,
- Serum Electrolyte Test,
- Arterial Blood Gas Analysis,
Medical management of the child with Kwashiorkor.
- Provide the child with an adequate protein-rich diet.
- Advise the child to have adequate calorie intake.
- Advise the child to have adequate nutrient-rich food intake.
- Provide adequate glucose solution if the child has a condition of hypoglycemia.
- If the child has a condition of anemia, treat it properly through blood transfusion.
- Advise the child to take proper skin care.
- Provide proper play therapy and recreation therapy to the child.
- Advise the parents of the child to provide nutritious rich food to the child.
- Provide adequate vitamin A supplements to the child Provide.
- If kwashiorkor is in an advanced stage, immediately hospitalize the child.
- Properly assess the child’s fluid and electrolyte levels.
- Assess the child’s height, weight, and nutritional status.
- Properly provide psychological support to the child.
Nursing management of the child with the Kwashiorkor.
(Nursing management of the child with the Kwashiorkor)
- Properly assess the child’s nutritional status.
Q-5 Define following (any six) Write the following definition. (Any six)12
a) Pediatric nursing
- Pediatric nursing is a branch of nursing and the art and science of providing comprehensive nursing care, i.e. preventive, promotive, curative and rehabilitative care, to a child from conception to adolescence for his/her physical growth, mental, emotional, spiritual and psychosocial development. is provided.
- The aim of pediatric nursing is to ensure that the child’s growth and development is appropriate and that the child can develop holistically, that is, physically, mentally, socially, spiritually, intellectually and emotionally properly.
b) Development
- Development is the process of physiological maturation and maturation of the functional capacity of the body. The progressive increase in the child’s skills and capacity to perform any task is called development. The main reason for development is the maturation of the nervous system. This is a qualitative aspect of the body. It is a little difficult to measure development, but it can definitely be measured in a child. Development is measured according to different activities through physiological, psychological, social, intellectual and emotional changes. The child learns to speak, learns to walk, etc. show development.
c) Cryptorchidism
- Cryptorchidism, also known as “undescended testicles”, is a condition in which one or both testicles fail to move down from the abdomen into the scrotum before they are born.
- This condition can affect the development and function of the testicles. This condition is more common in premature infants.
- Usually the testicles are present in the abdominal area of the fetus until 7 months of intrauterine life and these testicles descend into the scrotum during the period between 8 and 9 months of intrauterine life. However, due to some factors, these testicles do not descend into the scrotum and the testicles remain present in the abdominal area of the newborn. This condition is called cryptorchidism (undescended testicles). Which can increase the risk of infertility, inguinal hernia and testicular cancer in the future. is.
d) Spina Bifida
- Spina bifida is a congenital neural tube defect. The neural tube is normally responsible for the formation and closure of the spinal cord and brain during early embryonic development. When the spinal cord forms, it does not close completely, leaving a gap between the vertebrae. This incomplete spinal cord closure causes the spinal cord and There are different types of spinal column malformations.
- When there is a defect in the closure of the vertebral column and a space is left between them, tissue is exposed from this bony space and a sac-like structure protrudes outwards, which is called spina bifida.
There are three main types of spina bifida.
1) Spina bifida occulta.
2) Spina bifida meningocele.
3) Spina bifida meningomyelocele.
••>
1) Spina bifida occulta.
- Spina bifida occulta is the mildest and most common form of spina bifida, where the spinal cord and nerves are usually unaffected. In spina bifida occulta, there is a small gap or opening in the spinal cord, but it is covered by a layer of skin, so there is no visible protrusion of the spinal cord or meninges. Most often, there are no symptoms in this form of spina bifida.
2) Spina bifida meningocele:
- In this form, the protective layer around the spinal cord (the meninges) herniates (protrudes) outward from the lower back area through a gap or opening in the spinal cord, creating a sac or cyst filled with the meninges layer and cerebrospinal fluid. Unlike myelomeningocele, the spinal cord itself is not involved, and the neurological deficit is less severe.
3) Spina bifida meningomyelocele.
- Meningomyelocele is the most severe form of spina bifida, where the spinal cord, meninges, and nerves protrude (protrude) through a gap or opening in the spinal cord, forming a sac or cyst in the lower back area covered by a thin layer of skin. Meningomyelocele often causes neurological deficits and functional impairment. People with meningomyeloceles may experience paralysis, muscle weakness, sensory loss, bowel and bladder dysfunction, and other complications such as hydrocephalus (fluid accumulation in the brain), Chiari malformations, and other malformations.
e) Intussusception
- Intussusception is when the wall of the intestine telescopes into itself, which is called intussusception. In this, a part of the intestine gets trapped inside.
- This is a condition of intestinal obstruction seen in children. This is a type of medical emergency. It is usually seen near the ileocecal region.
- Due to this obstruction, blockage of gas and secretions occurs and edema i.e. swelling is seen due to improper blood circulation. Sometimes necrosis and gangrene can also develop due to this.
f) Neonatal mortality rate. Neonatal Mortality Rate
- Neonatal Mortality Rate is an important public health indicator that shows the total number of deaths of neonates within the first 28 days of life out of all live births in a given area and year. In other words, the number of deaths of children under 28 days of age per 1000 live births in the same area and during the same year is called neonatal mortality rate.
NMR (Neonatal Mortality Rate) =
Total deaths of children under 28 days of age in an area during a year
————————————————————- × 1000
Total live births in the same area and during the same year
g) Juvenile Delinquency – Juvenile Delinquency
Juvenile delinquency is one of the most common problems of society.‘Juvenile’ means childhood and ‘delinquency’ means antisocial behavior or criminal behavior
Juvenile delinquency is a type of criminal act that is usually committed by children and teenagers who are below 18 years of age. Juvenile delinquency is illegal or antisocial repetitive behavior by a child, usually committed by individuals under the age of 18. This juvenile delinquency can range from relatively minor crimes such as vandalism, shoplifting to more serious crimes including assault, drug offenses, and property crimes. This juvenile delinquency behavior involves lying, stealing, stealing from home, running away from school, running away from home, disobeying someone, fighting, looting, sexual assault, etc.
h) Congenital clubfoot – Congenital clubfoot
- Club foot is a congenital anomaly of the musculoskeletal system. In which a non-traumatic deformity is seen in the foot. It is also called talipes. These words are derived from the Latin words talus meaning ankle and pes meaning foot. This terminology was given in 1839.
- Club foot is a complex foot deformity. In which it is seen due to deformity of the bones, ligaments and muscles of the foot.
- In this, the part of the foot is seen twisted from its normal position.
In this problem, the deviation of the foot is seen in all different directions, and it is classified differently. - In this problem, the main thing is that the foot is not in the normal anatomical position, it is seen bent in different angles and directions.
Q-6(A) Fill in the blanks – Fill in the blanks. 05
1.Koplik spot is seen in …… Koplik spot is seen in ……. Answer: Measles
2.Age group of toddler is …… . The age group of toddler is ……. Answer: 1–3 years
3.BFHI stands for …… BFHI’s full name is …… Answer: Baby Friendly Hospital Initiative
4.Child weight doubles at the age of …… . …… The weight of a child doubles at the age of 5 months. Answer:5 months
5.R.C.H phase II is started in …… year. ….. Answer: 2005
(B) True or False – Tell me which is true or false. 05
1. Cleft lip surgery is done at 3-6 months. Cleft lip is operated after 3-6 months. ✅ True
2.Trendelenburg is the most appropriate position in which child is placed after tonsillectomy. ❌ False Appropriate position: Side-lying or prone position (to prevent bleeding aspiration)
3.Enuresis means urination is sleep. Enuresis is called urination in the sleep. ✅ True
4.Leg heels being elevated & turned outward from the midline of the body is known as Talipus varus. The heel of the foot is elevated from the midline of the body and turned outward is called talipus varus. ❌ False Correcr Answer : Talipes varus = foot turned inward (inversion)
5.Umbilical cord contains 1 vein & 2 arteries. The umbilical cord has 1 vein and 2 arteries.✅ True
(C) Multiple Choice Questions – Write the correct option from the following.05
1. Who is known as father of pediatric …… . Who is known as the father of pediatrics? Correct Answer: a) Abraham Jacob
a) Abram Jacob
b) Kashyapa
c) Hippocrates
d) Susruta
2.Trisomy 21 is also called …… Another name for Trisomy 21 …… Correct Answer: b) Down’s syndrome
a) Klinefelter’s syndrome
b) Down’s syndrome
c) Turner syndrome
d) Sickle cell anemia
3.Early neonate is a period from …. Early Neonatal Period The period of …… is. Correct Answer: a) 0–7 days
a) 0-7 days
b) 0-7 months
c) 0-7 weeks
d) 0-7 years
4.Pica is …… Correct Answer: c) Eating of non-nutritive substance regularly for at least 1 month
a) Associated with parasitic infestation
b) Most common between 18 months to 6 years of age
c) Eating of non-nutritive substance regularly for at least 1 month
d) All are correct
5.Bulging fontanelle is a sign of……. Correct Answer: a) Hydrocephalus
a) Hydrocephalus
b) Intussusception
c) Dehydration
d) Encephalitis
