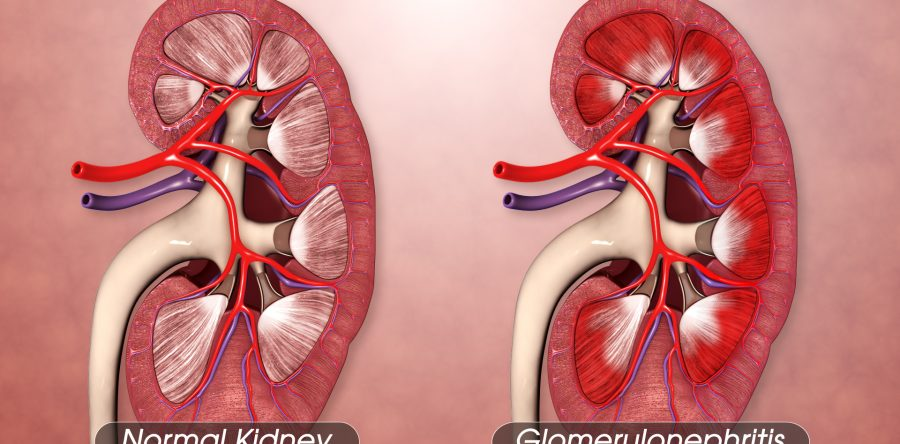
Glomerulonephritis refers to a group of kidney diseases that cause inflammation of the glomeruli, the tiny filtering units in the kidneys. The pathological changes vary depending on whether the condition is acute, chronic, or rapidly progressive, but some common mechanisms underlie all types.
Pathophysiological Mechanisms:
Immune Complex Deposition
Antigen-antibody complexes (from infections, autoimmune disorders) deposit in the glomerular basement membrane (GBM).
These immune complexes activate the complement system, attracting neutrophils and macrophages, causing inflammation and damage.
Cellular Proliferation
Mesangial cells, endothelial cells, and epithelial cells proliferate in response to injury.
This causes glomerular enlargement and reduced filtration surface area.
Increased Glomerular Permeability
Damage to the podocytes and GBM leads to leakage of proteins (proteinuria) and red blood cells (hematuria) into the urine.
Thickening of Basement Membrane
Chronic inflammation causes fibrosis and scarring of the GBM, further impairing filtration.
Crescent Formation (in Rapidly Progressive GN)
Severe injury leads to leakage of fibrin and inflammatory cells into Bowman’s space.
Forms crescents that compress the glomerulus and rapidly destroy renal function.
Glomerulosclerosis
Over time, persistent inflammation and ischemia lead to hardening and scarring of the glomeruli (glomerulosclerosis), reducing kidney function.
Tubulointerstitial Changes
As glomerular damage progresses, tubular atrophy, interstitial inflammation, and fibrosis occur, contributing to chronic kidney disease (CKD).
Clinical Correlation:
Hematuria (tea-colored or cola-colored urine)
Proteinuria
Edema (especially around eyes and ankles)
Hypertension
Reduced glomerular filtration rate (GFR)
Histological Findings:
Hypercellular glomeruli (due to proliferation/infiltration)
Thickened capillary walls
Immune deposits (seen on immunofluorescence microscopy)
Crescents in Bowman’s space (in rapidly progressive types)
Fibrosis and glomerulosclerosis in chronic stages
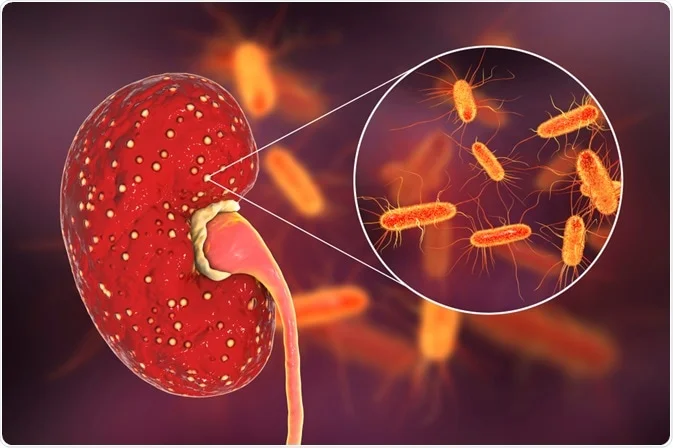
Pyelonephritis – Pathological Changes
Pyelonephritis is an inflammation of the renal pelvis and the renal parenchyma, typically due to a bacterial infection. It may be acute or chronic, with distinct pathological features.
Pathophysiological Mechanisms:
Acute Pyelonephritis
Bacterial Infection
Most commonly caused by Escherichia coli (E. coli).
Bacteria ascend from the lower urinary tract (bladder) to the kidney via the ureter.
Inflammatory Response
Neutrophils infiltrate the renal interstitium and tubules.
Formation of pus (suppuration) and abscesses in the renal tissue.
Tubular Damage
Infection leads to necrosis of tubular epithelium, causing tubular dysfunction.
Cast formation and shedding of epithelial cells seen in urine.
Edema and Hyperemia
Kidneys become swollen, red, and congested due to vascular dilation and inflammatory exudate.
Chronic Pyelonephritis
Repeated or Persistent Infection
Often associated with urinary tract obstruction, vesicoureteral reflux, or neurogenic bladder.
Leads to progressive renal damage.
Interstitial Fibrosis and Tubular Atrophy
Ongoing inflammation causes scarring and fibrosis of the interstitial tissue.
Loss and atrophy of nephrons, especially tubules.
Irregular Renal Scarring
Patchy, asymmetric scarring with cortical thinning.
Seen especially at upper and lower poles of the kidney.
Glomerulosclerosis and Hyalinization
Chronic inflammation may lead to sclerosed glomeruli and hyalinized arterioles.
May progress to chronic kidney disease (CKD).
Clinical Correlation:
Acute Pyelonephritis
Chronic Pyelonephritis
Sudden fever, chills, flank pain
Often asymptomatic or mild symptoms
Dysuria, urgency, frequency
Polyuria, nocturia, hypertension
Tenderness at costovertebral angle
Progressive renal failure
Pus cells and bacteria in urine
Small, shrunken, scarred kidneys on imaging
Histological Findings:
Acute:
Neutrophilic infiltration in interstitium and tubules
Microabscess formation
Chronic:
Interstitial fibrosis
Tubular atrophy and thyroidization (tubules resemble thyroid tissue)
Glomerulosclerosis
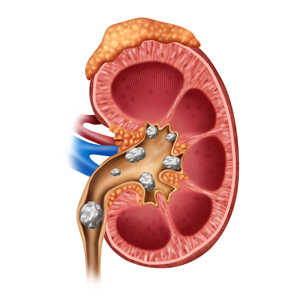
Renal Calculi – Pathological Changes
Renal calculi, also known as kidney stones, are solid crystalline masses formed in the kidneys from minerals and salts. These can obstruct urinary flow and cause tissue damage.
Types of Renal Calculi:
Calcium oxalate/calcium phosphate (most common)
Struvite stones (infection-related)
Uric acid stones
Cystine stones (rare, genetic)
Pathophysiological Changes:
1. Supersaturation of Urine
High concentrations of stone-forming substances (e.g., calcium, oxalate, uric acid) in urine.
Leads to crystallization when these exceed their solubility.
2. Nucleation and Crystal Growth
Crystals start to form around a nucleus (tiny particle or existing damage).
Grow larger over time to form calculi.
3. Aggregation and Retention in Kidney
Crystals aggregate and get trapped in the renal tubules or calyces.
They attach to damaged epithelium or Randall’s plaques (calcium deposits at papillary tips).
4. Obstruction of Urinary Tract
Stone can block ureter, renal pelvis, or urethra.
Causes urinary stasis, hydronephrosis (dilation of renal pelvis), and increased pressure in kidneys.
5. Inflammation and Mucosal Injury
Stones cause irritation and erosion of the urinary tract lining.
Leads to hematuria (blood in urine), pain, and infection risk.
6. Secondary Infection (Especially in Struvite Stones)
Stones may harbor bacteria.
Promotes recurrent urinary tract infections (UTIs) and stone enlargement (staghorn calculi).
7. Ischemia and Renal Damage
Long-standing obstruction causes:
Compression of renal vasculature
Decreased blood flow (ischemia)
Atrophy and fibrosis of kidney tissue
Can lead to renal failure if untreated
Histological Findings:
Damaged tubular epithelium
Inflammatory cell infiltration
Calcium deposits within tubules
Areas of fibrosis and scarring
Clinical Correlation:
Symptoms
Findings
Severe flank pain (renal colic)
Hematuria (microscopic or visible)
Nausea, vomiting
Crystals in urine (crystalluria)
Urinary urgency/frequency
Imaging: X-ray, Ultrasound, CT scan
Fever (if infection present)
Hydronephrosis on imaging
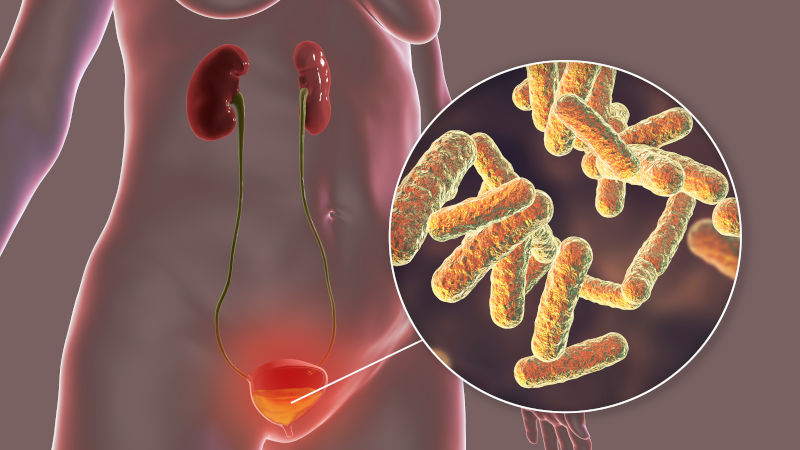
Cystitis – Pathological Changes
Cystitis refers to inflammation of the urinary bladder, most commonly due to a bacterial infection. It can be acute or chronic, and the pathological changes differ depending on the stage and cause of the condition.
Etiology (Common Causes):
Bacterial infection – most common cause (e.g., E. coli, Klebsiella, Proteus)
Chemical irritants (e.g., drugs, radiation, chemotherapy)
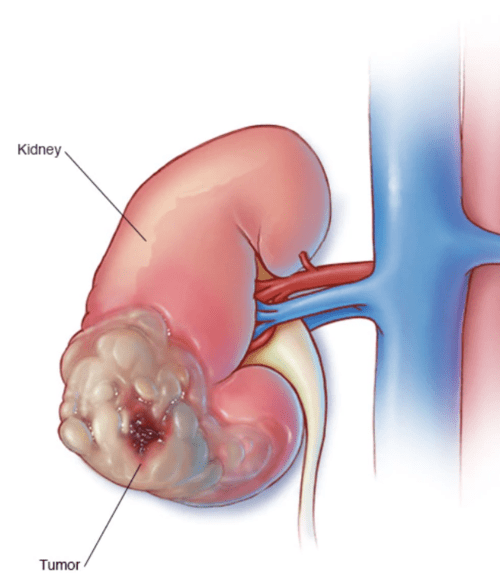
Renal Cell Carcinoma (RCC) is the most common malignant tumor of the kidney in adults, originating from the renal tubular epithelium. It is also called hypernephroma or adenocarcinoma of the kidney.
Etiology / Risk Factors:
Smoking
Obesity
Hypertension
Chronic kidney disease
Genetic syndromes (e.g., von Hippel-Lindau disease)
Male gender, typically between 50–70 years of age
Pathological Changes (Gross & Microscopic)
1. Origin and Growth
RCC arises from proximal convoluted tubule epithelial cells.
The tumor usually grows unilaterally (one kidney) and is solitary.
Located in the cortex of the kidney.
2. Gross Appearance
Golden-yellow color due to high lipid content.
Often has areas of:
Hemorrhage
Necrosis
Cystic degeneration
Calcification
3. Histological Types (Subtypes of RCC)
Type
Features
Clear Cell RCC (most common)
Cells have clear cytoplasm due to lipid and glycogen. Highly vascular.
Papillary RCC
Papillary or tubular structures with foamy macrophages. Associated with trisomy 7, 17.
Chromophobe RCC
Pale eosinophilic cells with perinuclear halo. Better prognosis.
4. Invasion and Spread
RCC is known for early vascular invasion, especially into:
Renal vein
Inferior vena cava
Can also invade the pelvis and ureter, spreading via hematogenous route.
5. Metastasis
Common sites:
Lungs
Bones
Liver
Brain
Metastasis may occur before primary tumor is detected due to silent progression.
Microscopic Features (Clear Cell RCC):
Cells arranged in nests or tubules
Clear cytoplasm with distinct borders
Rich capillary network
Atypical nuclei, mitotic figures may be seen
Clinical Correlation – Classic Triad (seen in <10% cases):
Symptom
Explanation
Hematuria
Due to tumor invading renal vessels
Flank pain
From tumor mass or hemorrhage
Palpable mass
Large or advanced tumor
Other features:
Fever
Weight loss
Hypertension (due to increased renin)
Polycythemia (due to ectopic erythropoietin production)
Paraneoplastic syndromes
Imaging and Diagnosis:
Ultrasound, CT scan, MRI
Confirmed by histopathology after nephrectomy or biopsy
Acute Renal Failure (ARF) or AKI is a sudden and rapid decline in kidney function, leading to the accumulation of waste products, fluid, and electrolyte imbalances. It develops over hours to days.
Types of AKI (based on the location of the cause):
Type
Cause Origin
Prerenal
Due to reduced blood flow to kidneys
Intrarenal (Intrinsic)
Due to direct kidney tissue damage
Postrenal
Due to obstruction of urine flow
Pathological Changes by Type
1. Prerenal AKI – Before the kidney
Cause: Hypoperfusion due to dehydration, shock, heart failure, blood loss.
Changes:
No structural damage initially
Prolonged hypoperfusion → ischemic injury to tubules
Can progress to acute tubular necrosis (ATN) if not corrected
2. Intrarenal AKI – Within the kidney
Most common type = Acute Tubular Necrosis (ATN)
a. Ischemic ATN
Caused by prolonged hypotension or shock
Patchy necrosis of tubular epithelium (especially in proximal tubules & thick ascending limb)
Tubular basement membrane may remain intact
b. Nephrotoxic ATN
Caused by toxins (e.g., aminoglycosides, contrast dye, heavy metals)
Diffuse necrosis of proximal tubular cells
May see cellular debris and casts in tubules
Other Intrarenal Causes:
Glomerulonephritis – inflammation & damage to glomeruli
Interstitial nephritis – allergic/infective inflammation of interstitium
Chronic Renal Failure is a progressive, irreversible decline in kidney function lasting more than 3 months. It leads to the accumulation of waste products, electrolyte imbalance, fluid overload, and hormonal dysfunction.
Pathological Changes in CRF
1. Nephron Loss
Primary event: Continuous damage to nephrons due to underlying disease (e.g., diabetes, hypertension, glomerulonephritis).
Remaining nephrons undergo hypertrophy and hyperfiltration to compensate → over time, they burn out too.
2. Glomerular Changes
Glomerulosclerosis – scarring of glomeruli.
Reduced filtration surface → ↓ GFR (Glomerular Filtration Rate).
Progressive loss of glomerular capillaries.
3. Tubulointerstitial Changes
Tubular atrophy – degeneration and loss of tubule structure.
Interstitial fibrosis – accumulation of extracellular matrix (scar tissue).
Inflammatory cell infiltration – especially lymphocytes and macrophages.
Leads to impaired reabsorption and secretion.
4. Vascular Changes
Arteriosclerosis – thickening of arterial walls → ↓ blood flow.
Ischemia → further tubular and glomerular damage.
Hyalinization of small vessels.
5. Systemic Effects (Multisystem Involvement)
System Affected
Pathological Effects
Hematologic
Anemia (↓ Erythropoietin), Platelet dysfunction
Skeletal
Renal osteodystrophy (↓ Vitamin D, ↑ PTH)
Cardiovascular
Hypertension, LVH, Uremic pericarditis
Neurological
Uremic encephalopathy, peripheral neuropathy
Gastrointestinal
Nausea, vomiting, uremic breath
Skin
Uremic frost, pruritus, dry skin
Stages of CRF (Based on GFR):
Stage
GFR (ml/min/1.73m²)
Description
1
>90
Normal GFR, kidney damage present
2
60–89
Mild reduction
3
30–59
Moderate reduction
4
15–29
Severe reduction
5
<15
Kidney failure (End-stage renal disease – ESRD
Histological Findings:
Glomerulosclerosis
Tubular atrophy
Interstitial fibrosis
Arterial narrowing and hyalinization
Inflammatory infiltrates
Clinical Features:
Manifestation
Cause
Fatigue, weakness
Anemia, uremia
Edema
Salt & water retention
Hypertension
RAAS activation, fluid overload
Bone pain
Renal osteodystrophy
Nausea, vomiting
Uremic toxins
Itching (pruritus)
Accumulation of uremic waste in skin
Confusion, seizures
Uremic encephalopathy (late stage)
Summary:
Chronic Renal Failure involves progressive nephron loss, fibrosis, and inflammation, eventually leading to end-stage renal disease (ESRD), where the kidneys can no longer sustain life without dialysis or transplantation.
MALE GENITAL SYSTEM
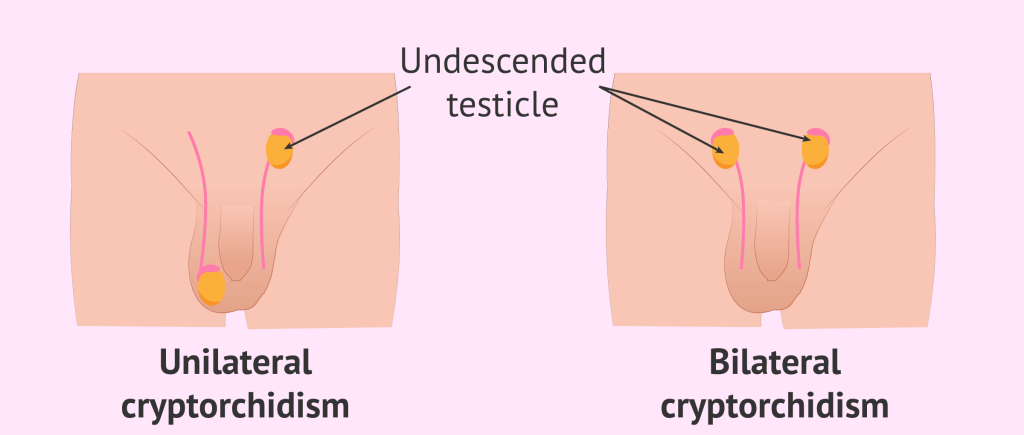
Cryptorchidism – Pathological Changes
Cryptorchidism is a condition in which one or both testes fail to descend into the scrotal sac. Normally, the testes descend from the abdomen to the scrotum during fetal development, usually before birth. When this process is incomplete, the testes may remain in the abdomen, inguinal canal, or upper scrotum.
Sites of Undescended Testes:
Abdominal cavity (most severe)
Inguinal canal (most common)
Pre-scrotal or high scrotal position
Pathological Changes in Cryptorchidism
1. Histological Changes in the Undescended Testis:
Change
Description
Germ cell atrophy
Early loss of germ cells due to abnormal temperature
Sertoli cell-only tubules
Seminiferous tubules lack germ cells
Thickened basement membrane
Degenerative changes in tubules
Fibrosis of interstitium
Scarring replaces normal parenchyma
Leydig cell hyperplasia
Increased Leydig cells due to disrupted hormonal feedback
2. Functional Impairment
Impaired spermatogenesis due to high intra-abdominal temperature (which is ~2–3°C higher than scrotal temperature)
Infertility especially if both testes are undescended and untreated
Endocrine function may be preserved in mild/unilateral cases
3. Risk of Malignancy
Increased risk (up to 4–10 times) of developing testicular cancer, especially seminoma
Risk remains even after surgical correction, but is reduced if corrected early (before 1–2 years of age)
4. Testicular Torsion & Trauma
Undescended testes are more prone to torsion (twisting of the spermatic cord) and trauma, particularly when located in the inguinal canal
5. Atrophy and Hypoplasia
Affected testis is usually smaller, softer, and atrophic compared to normal
May remain non-functional if not surgically corrected in time
Microscopic Features:
Loss of germinal epithelium
Small, hyalinized seminiferous tubules
Increased interstitial fibrosis
Few or absent spermatogonia
Prominent Leydig cells
Clinical Correlation:
Feature
Explanation
Empty scrotal sac
Most obvious sign of cryptorchidism
Infertility
Due to impaired spermatogenesis
Increased cancer risk
Especially seminoma in abdominal testis
Testicular torsion/trauma
Due to abnormal position
Management Note:
Orchiopexy (surgical correction) recommended before 12–18 months of age
Early intervention preserves fertility and reduces cancer risk
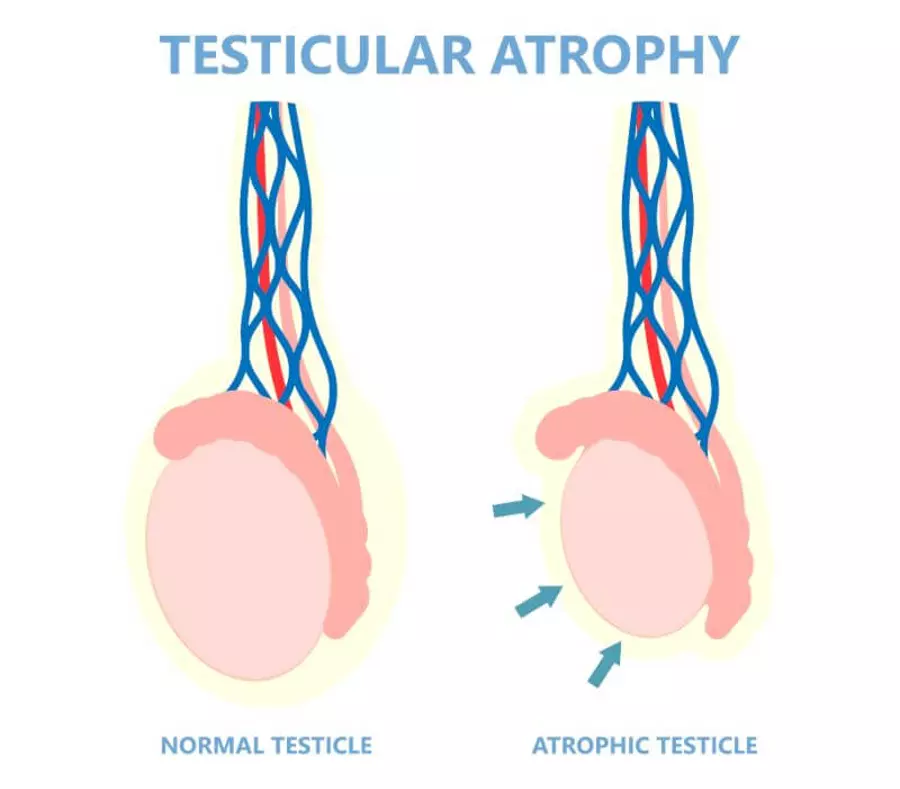
Testicular Atrophy – Pathological Changes
Testicular atrophy refers to the shrinkage and loss of function of the testes. It can be unilateral or bilateral, and is often associated with reduced fertility or hormonal imbalance.
Causes of Testicular Atrophy:
Category
Examples
Inflammatory
Mumps orchitis, chronic epididymo-orchitis
Hormonal
Hypogonadism (primary or secondary), low FSH/LH
Drugs/Toxins
Alcohol, chemotherapy, steroids
Vascular
Testicular torsion, varicocele
Congenital/Genetic
Klinefelter syndrome, cryptorchidism
Infectious
HIV, tuberculosis
Trauma/Radiation
Testicular injury or irradiation
Pathological Changes in Testicular Atrophy:
1. Shrinkage of Testicular Parenchyma
The testis becomes smaller, softer, and lighter in weight.
2. Tubular Changes (Seminiferous Tubules)
Pathological Feature
Explanation
Tubular atrophy
Thinning and collapse of seminiferous tubules
Germ cell loss
Early and progressive disappearance of spermatogenic cells
Sertoli cell-only pattern
Only Sertoli cells remain in the tubules
Thickened basement membrane
Due to fibrosis and degeneration
3. Interstitial Changes
Fibrosis of interstitial tissue
Loss of Leydig cells (↓ testosterone production)
In some cases: Leydig cell hyperplasia (compensatory)
4. Sclerosis and Hyalinization
Tubular walls become hyalinized (glassy appearance)
Peritubular fibrosis – collagen deposition around tubules
Loss of normal vascularity
5. Secondary Changes
Infertility due to loss of spermatogenesis
Hypogonadism (↓ testosterone) → reduced libido, muscle mass, energy
Elevated FSH/LH in primary testicular failure (feedback response)
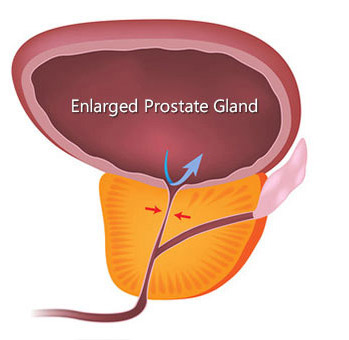
Prostatic Hyperplasia is a non-cancerous enlargement of the prostate gland, commonly seen in older men, especially over age 50. It primarily affects the transition zone of the prostate (around the urethra) and can obstruct urine flow.
Etiology & Risk Factors:
Hormonal imbalance: Increased dihydrotestosterone (DHT) and estrogen
Aging
Genetic predisposition
Androgen sensitivity
Pathological Changes in BPH
1. Glandular and Stromal Hyperplasia
Proliferation of both epithelial (glandular) and stromal (fibromuscular) cells
Results in formation of nodules, especially in the periurethral region (transition zone)
2. Nodular Enlargement
Multiple nodules of varying sizes compress the prostatic urethra
Leads to urinary outflow obstruction
3. Glandular Changes
Glands become dilated and lined by two layers:
Inner columnar epithelial cells
Outer basal cells
May contain corpora amylacea (proteinaceous concretions)
4. Stromal Changes
Increased smooth muscle and fibrous tissue
Fibromuscular nodules form due to proliferation of stromal elements
5. Compression of Urethra
Leads to narrowing of the prostatic urethra
Causes difficulty in urination (lower urinary tract symptoms)
6. Secondary Changes in Bladder and Kidneys
Bladder wall hypertrophy
Trabeculated bladder (due to chronic obstruction)
Hydronephrosis and renal damage in severe, untreated cases
Surgical: TURP (Transurethral Resection of Prostate) in severe cases
Summary:
BPH is caused by hormonal-induced proliferation of glandular and stromal tissue in the prostate, leading to nodular enlargement and urinary outflow obstruction, but not a precancerous condition.
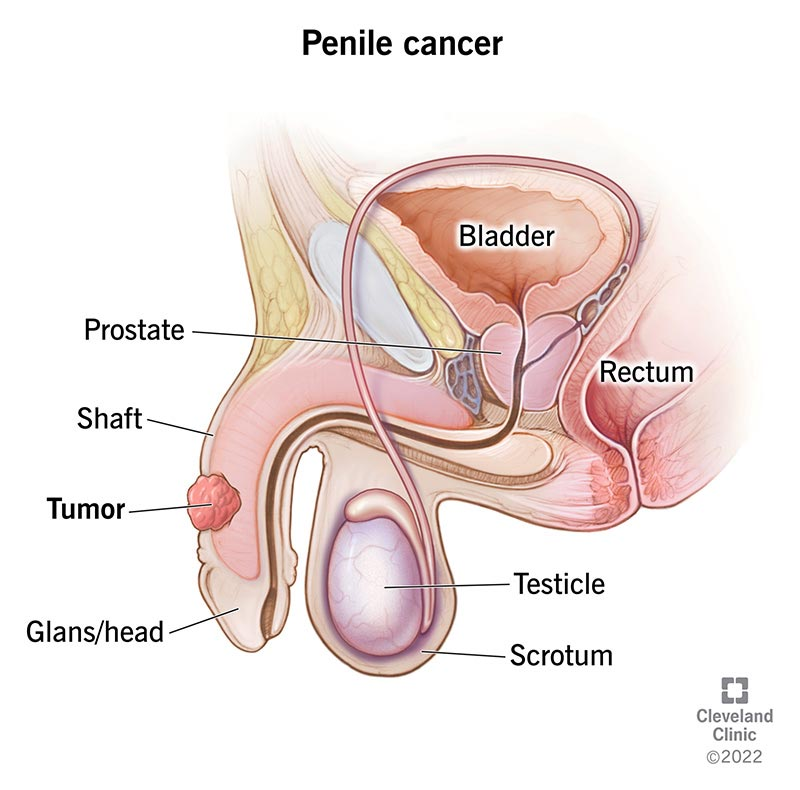
Carcinoma Penis – Pathological Changes
Penile carcinoma is a malignant tumor of the skin and mucosa of the penis, most commonly affecting the glans penis, prepuce (foreskin), or coronal sulcus. It is most often a squamous cell carcinoma (SCC).
Risk Factors:
Poor hygiene
Phimosis (tight foreskin)
Chronic inflammation or smegma accumulation
Human papillomavirus (HPV) – especially types 16, 18
Smoking
Multiple sexual partners
Lack of circumcision
Pathological Changes
1. Origin
Arises from squamous epithelium of the glans, prepuce, or penile shaft.
Often begins as a precancerous lesion like leukoplakia, erythroplasia of Queyrat (in situ carcinoma), or Bowen’s disease.
2. Macroscopic Appearance
Ulcerative, exophytic (fungating), or nodular mass
Rounded eosinophilic structures seen in well-differentiated SCC
Cellular atypia
Enlarged, pleomorphic, hyperchromatic nuclei
Invasion
Tumor invades dermis, corpus spongiosum, corpus cavernosum
Lymphovascular invasion
May be present in aggressive tumors
Inflammatory infiltrate
Lymphocytes, plasma cells in stroma
4. Lymph Node Spread
Commonly spreads to inguinal lymph nodes
Later may spread to pelvic lymph nodes
Lymph node involvement is an important prognostic factor
Clinical Features:
Symptom/Sign
Cause/Explanation
Penile lump or ulcer
Primary tumor
Foul-smelling discharge
Secondary infection or necrosis
Bleeding or pain
Tumor invasion
Inguinal lymphadenopathy
Regional metastasis
Difficulty retracting foreskin
Due to phimosis or tumor mass
Precancerous Lesions:
Condition
Description
Leukoplakia
White plaque-like lesion
Bowen’s Disease
SCC in situ on shaft or scrotum
Erythroplasia of Queyrat
SCC in situ on glans/prepuce
Management:
Surgical excision (partial or total penectomy)
Inguinal lymph node dissection (if nodes are involved)
Radiotherapy or chemotherapy in selected cases
Early detection = better prognosis
Prognosis:
Good if detected early and limited to glans/prepuce
Poorer if there is deep invasion or lymph node metastasis
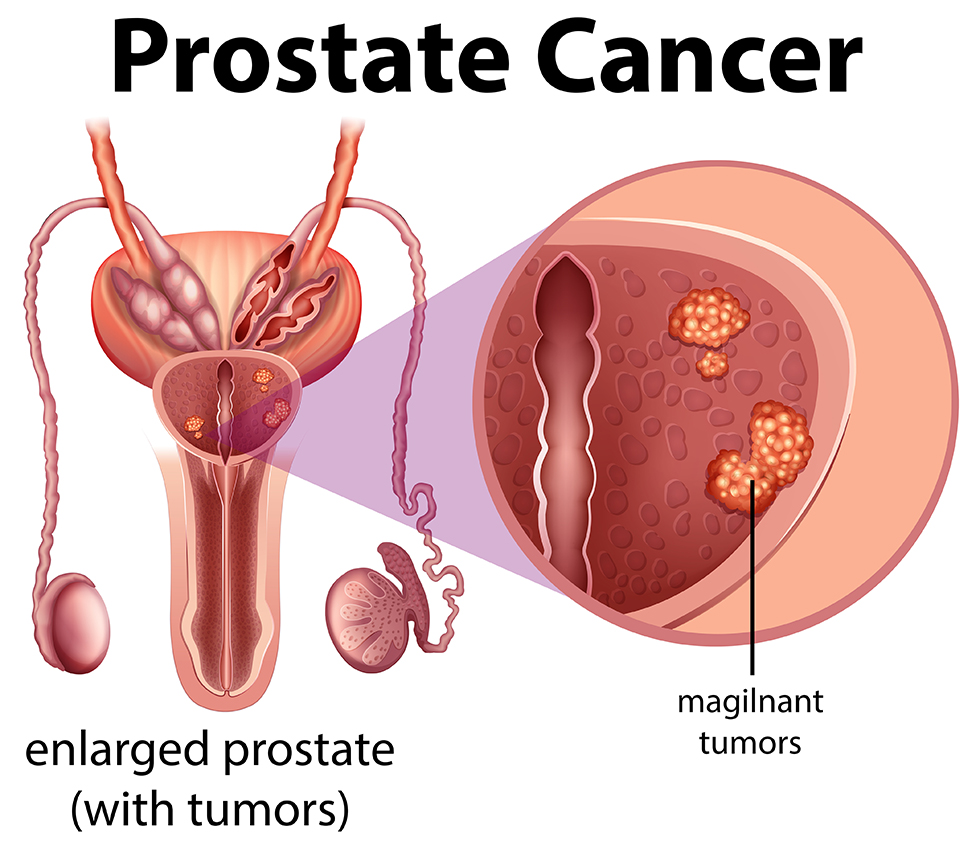
Carcinoma Prostate – Pathological Changes
Prostate carcinoma is a malignant tumor that arises most commonly from the glandular epithelium of the prostate. It is typically an adenocarcinoma and is the most common cancer in elderly men.
Risk Factors:
Age > 50 years
Family history of prostate cancer
High-fat diet
Hormonal imbalance (androgens like testosterone)
African descent
Genetic mutations (BRCA2, HOXB13, etc.)
Pathological Changes in Prostate Cancer
1. Origin and Site
Arises from the posterior peripheral zone of the prostate (unlike BPH, which affects the central/transitional zone).
Often multifocal and asymmetrical.
2. Gross Pathology
Hard, irregular, gritty nodule in the posterior prostate.
In advanced stages, the prostate becomes enlarged, firm, and distorted.
3. Microscopic (Histological) Features
Feature
Description
Adenocarcinoma
Most common type (95%)
Small, crowded glands
Lined by single layer of malignant cuboidal/columnar cells
Loss of basal cell layer
Important diagnostic clue
Perineural invasion
Cancer cells invade around nerves – common finding
Prominent nucleoli
Within malignant nuclei
Cribriform patterns
Fused glandular structures (in high-grade tumors)
4. Gleason Grading System
Used to assess tumor differentiation and prognosis.
Ranges from Grade 1 (well-differentiated) to Grade 5 (poorly differentiated).
Gleason Score = Sum of the two most common patterns (2–10).
Prostate cancer is a slow-growing adenocarcinoma that starts in the peripheral zone.
Shows microscopic glandular patterns, loss of basal layer, and may show perineural invasion.
Commonly metastasizes to bones and is monitored using PSA levels.
FEMALE GENITAL SYSTEM
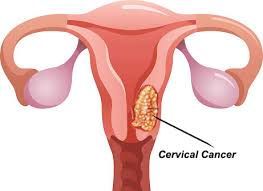
Carcinoma Cervix – Pathological Changes
Carcinoma of the cervix is a malignant tumor arising from the epithelial lining of the cervix, most commonly the squamocolumnar junction (transformation zone). It is one of the most common cancers in women, especially in developing countries.
Cervical carcinoma is caused primarily by high-risk HPV infection. It progresses from dysplasia (CIN) to invasive cancer, showing clear histological features like basement membrane invasion, keratin pearls, or glandular patterns, with local and distant spread if untreated.
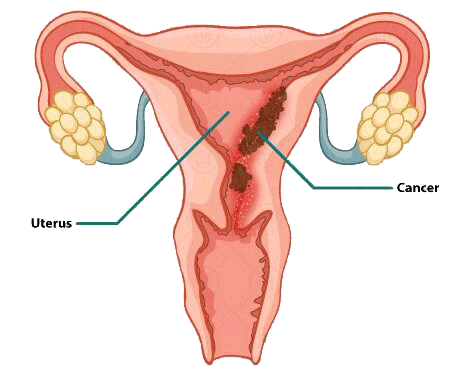
Carcinoma of Endometrium – Pathological Changes
Endometrial carcinoma is a malignant tumor arising from the lining of the uterus (endometrium). It is the most common gynecological cancer in postmenopausal women.
Risk Factors (Mainly due to unopposed estrogen exposure):
Obesity
Early menarche / late menopause
Nulliparity (no childbirth)
Estrogen therapy (without progesterone)
Polycystic ovarian syndrome (PCOS)
Endometrial hyperplasia
Diabetes mellitus, hypertension
Tamoxifen therapy
Lynch syndrome (hereditary non-polyposis colorectal cancer – HNPCC)
Types of Endometrial Carcinoma
Type
Description
Type I (Endometrioid type)
Most common (~80%), estrogen-dependent, usually arises from endometrial hyperplasia, seen in perimenopausal/postmenopausal women, better prognosis
Type II (Non-endometrioid/serous type)
Estrogen-independent, arises from atrophic endometrium, usually in older women, aggressive, poor prognosis
Pathological Changes
1. Gross Appearance:
Polypoid, fungating, or diffuse thickening of the endometrium
May fill the uterine cavity and invade the myometrium
2. Microscopic (Histological) Features
a. Type I (Endometrioid Adenocarcinoma):
Glandular pattern resembling normal endometrium
Crowded back-to-back glands
Minimal to moderate nuclear atypia
Invasion into myometrium is key feature of malignancy
Often associated with endometrial hyperplasia
b. Type II (Serous Papillary / Clear Cell Carcinoma):
Papillary or solid growth patterns
High-grade nuclei, marked atypia
Psammoma bodies may be present
Frequent myometrial invasion and lymphovascular spread
3. Myometrial Invasion
Depth of invasion into the myometrium is a key prognostic factor
Deep invasion → higher risk of metastasis
4. Lymphovascular Spread
Tumor may invade lymphatic vessels
Spreads to pelvic and para-aortic lymph nodes
Hematogenous spread to lungs, liver, bones in advanced cases
Clinical Features
Symptom
Explanation
Postmenopausal bleeding
Most common early sign
Pelvic pain or pressure
In advanced disease
Watery or bloody vaginal discharge
Due to tumor breakdown
Enlarged uterus
In large or advanced tumors
Diagnosis
Transvaginal ultrasound: Thickened endometrium (>4 mm in postmenopausal women)
Endometrial biopsy / D&C: For histological confirmation
Progestin therapy (for fertility preservation or recurrence)
Summary
Endometrial carcinoma arises from the endometrial lining, often due to unopposed estrogen. It shows glandular proliferation, nuclear atypia, and myometrial invasion. Early detection via postmenopausal bleeding can lead to excellent prognosis, especially in Type I cancers.
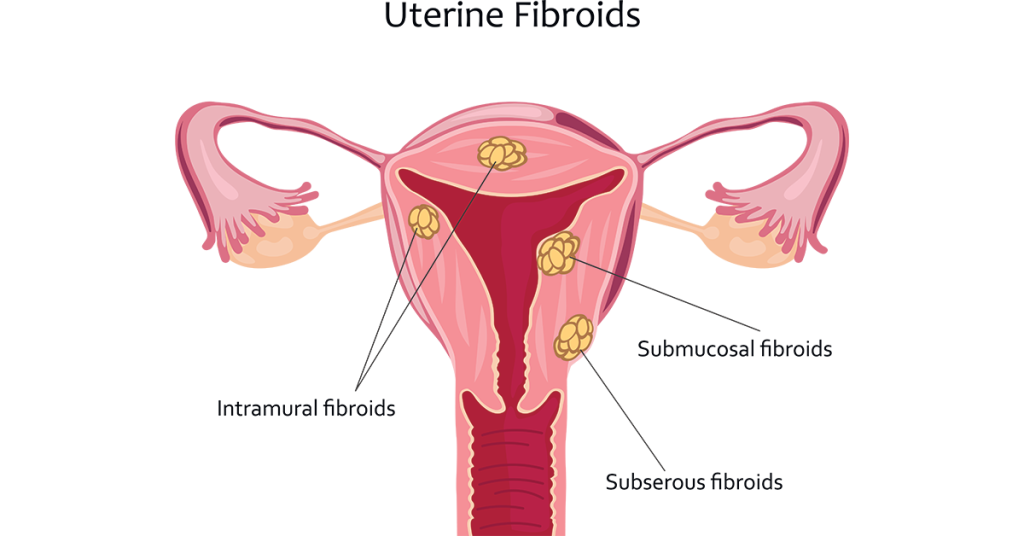
Uterine fibroids are benign (non-cancerous) tumors of the smooth muscle of the uterus (myometrium). They are the most common tumor of the female reproductive tract, especially during reproductive years.
Risk Factors:
Women of reproductive age (30–50 years)
Estrogen and progesterone sensitive – grow during pregnancy, shrink after menopause
Early menarche, obesity, nulliparity
Family history of fibroids
African descent (higher risk)
Types of Uterine Fibroids (by location):
Type
Location
Intramural
Within the muscular wall of the uterus
Submucosal
Beneath the endometrial lining, projecting into the cavity
Subserosal
Beneath the outer uterine layer, projecting outward
Pedunculated
Attached to the uterus by a stalk (can be submucosal or subserosal)
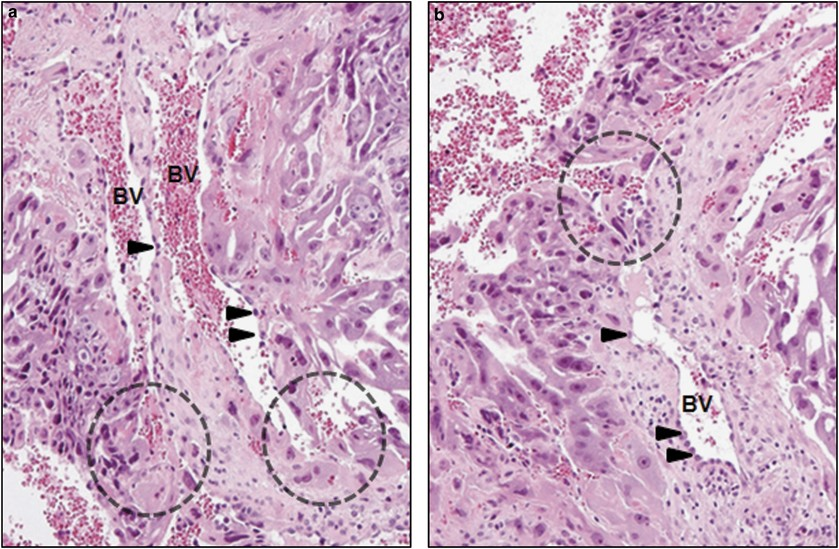
Pathological Changes
1. Gross Appearance
Well-circumscribed, round, firm nodules
White or gray cut surface with whorled (spiral) pattern
May be single or multiple
Degenerative changes occur in large or long-standing fibroids
2. Histological Features
Feature
Description
Smooth muscle cells
Uniform spindle-shaped cells arranged in fascicles
No nuclear atypia
Cells look benign (no malignant features)
Low mitotic activity
Cell division is minimal
Dense collagen
Interspersed between muscle bundles
Whorled architecture
Characteristic pattern seen under microscope
3. Degenerative Changes (Common in large fibroids):
Type
Description
Hyaline degeneration
Most common; glassy, pink appearance
Cystic degeneration
Fluid-filled spaces form
Red (carneous) degeneration
Hemorrhagic infarction (often in pregnancy)
Calcification
Common in postmenopausal women
Fatty or myxoid change
Rare
Clinical Features
Symptom
Explanation
Menorrhagia (heavy bleeding)
Especially in submucosal fibroids
Pelvic pain or pressure
Due to mass effect or degeneration
Urinary frequency
Pressure on bladder
Constipation
Pressure on rectum
Infertility or miscarriage
Interference with implantation or fetal growth
Abdominal mass
Firm, irregular enlargement
Diagnosis
Pelvic examination: Enlarged, irregular uterus
Ultrasound: Confirms size, number, and location
MRI: Used in complex or large cases
Hysteroscopy: For submucosal fibroids
Management
Treatment Option
Indication
Observation
Asymptomatic, small fibroids
Hormonal therapy
GnRH agonists (to shrink fibroids temporarily)
Myomectomy
Surgical removal (preserves uterus – good for fertility)
Hysterectomy
Definitive treatment in symptomatic women not desiring future pregnancy
A vesicular mole is an abnormal pregnancy caused by proliferation of trophoblastic tissue and swelling (hydropic degeneration) of chorionic villi. It is classified under gestational trophoblastic diseases (GTD) and can be either benign (molar pregnancy) or premalignant.
Types of Vesicular Mole:
Type
Features
Complete Mole
No fetal tissue, all villi are swollen, 46,XX or 46,XY (paternal origin only)
Partial Mole
Some fetal tissue present, mixed normal and abnormal villi, triploid (69,XXY or 69,XXX)
In some cases, invasion into myometrium (invasive mole)
Risk of progression to choriocarcinoma (especially with complete mole)
Clinical Features:
Symptom/Sign
Explanation
Vaginal bleeding
Due to abnormal trophoblast invasion
Uterus larger than gestational age
Excessive villous growth
Hyperemesis gravidarum
Elevated hCG levels
Early-onset preeclampsia
Before 20 weeks – suspicious for mole
Absence of fetal heart sounds
In complete mole
Passage of grape-like vesicles
Characteristic of molar pregnancy
Laboratory Findings:
Very high β-hCG levels (much higher than normal pregnancy)
Ultrasound: “Snowstorm” or “cluster of grapes” appearance
No gestational sac or fetus (in complete mole)
Management:
Uterine evacuation by suction curettage
Monitor β-hCG levels post-evacuation weekly until undetectable
Avoid pregnancy for 6–12 months
Chemotherapy (e.g., methotrexate) if persistent GTD or choriocarcinoma develops
Complications:
Persistent gestational trophoblastic disease
Invasive mole
Choriocarcinoma
Uterine rupture (rare)
Anemia, hyperthyroidism (due to cross-reactivity with TSH receptors)
Choriocarcinoma – Pathological Changes
Choriocarcinoma is a highly malignant tumor arising from the trophoblastic tissue of the placenta. It can occur after a molar pregnancy, normal pregnancy, abortion, or ectopic pregnancy.
Key Characteristics:
Aggressive and rapidly spreading
Produces very high levels of β-hCG
Highly vascular and hemorrhagic
Tends to metastasize early—especially to lungs and brain
Pathological Changes
1. Gross Appearance
Soft, bulky, and hemorrhagic mass
Often with areas of necrosis and blood clots
Usually found in the uterus, but can also appear at metastatic sites (lung, liver, brain)
Pelvic ultrasound: May show intrauterine mass, but no fetus
Histopathology: Confirms diagnosis with absence of chorionic villi and presence of two trophoblast cell types
Management
Treatment
Notes
Chemotherapy
Highly effective – Methotrexate or multi-drug regimen (e.g., EMA-CO)
Surgery (rare)
Hysterectomy for resistant or non-responsive cases
Monitor β-hCG
Until undetectable and then for 6–12 months
Avoid pregnancy
During follow-up to ensure accurate β-hCG tracking
Prognosis
Type
Prognosis
Gestational choriocarcinoma
Excellent with chemo
Non-gestational (germ cell origin)
Poorer prognosis
Summary
Choriocarcinoma is a highly malignant tumor of trophoblastic origin, usually following a molar or normal pregnancy, characterized by absence of chorionic villi, high β-hCG levels, trophoblastic cell proliferation, hemorrhage, and early widespread metastasis, but is often curable with chemotherapy.
Breast
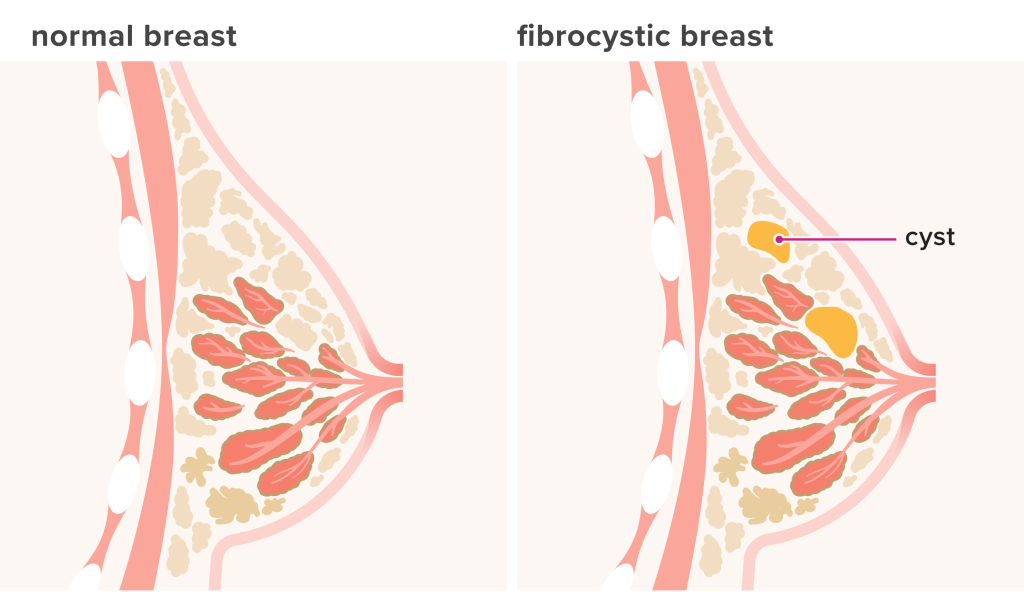
Fibrocystic Changes – Pathological Changes
Fibrocystic changes (also called fibrocystic breast disease or fibrocystic condition) are non-cancerous (benign) changes in the breast tissue. They are the most common breast condition in women of reproductive age, especially between 30–50 years.
These changes are hormone-related (estrogen and progesterone) and often fluctuate with the menstrual cycle.
Overview of the Condition:
Not a true disease but a collection of benign histological changes
May involve fibrosis, cyst formation, ductal hyperplasia, or epithelial changes
Usually bilateral and associated with pain, tenderness, and lumpiness, especially before menstruation
Pathological Changes in Fibrocystic Disease
1. Cyst Formation
Dilatation of breast ducts → formation of fluid-filled cysts
Cysts may be small (microcysts) or large (macrocysts)
Lined by flattened or apocrine metaplastic epithelium
Contents may be blue-green (“blue-dome cysts” on gross examination)
2. Fibrosis
Rupture of cysts → leakage of fluid into surrounding stroma
Leads to chronic inflammation and fibrosis
Makes the breast feel firm, nodular, or rope-like
3. Epithelial Hyperplasia
Proliferation of ductal epithelial cells
Can be:
Usual (simple) hyperplasia: Benign, no atypia
Atypical hyperplasia: Cells show mild nuclear atypia, increased risk of developing breast cancer
Proliferative without atypia (usual hyperplasia, sclerosing adenosis)
Slight increase
Proliferative with atypia (atypical ductal/lobular hyperplasia)
Moderate to high risk (~4–5x)
Diagnosis:
Breast examination
Ultrasound/mammography: May show dense, cystic, or fibrotic areas
Fine-needle aspiration or biopsy: To rule out malignancy
Cyst fluid analysis (if needed)
Management:
Approach
Indication
Reassurance
In simple, non-suspicious cases
Supportive therapy
Pain relief, proper bra support
Hormonal modulation
For severe symptoms (e.g., OCPs)
Cyst aspiration
If large, painful cyst
Biopsy/surgical removal
If atypia or suspicious lesion
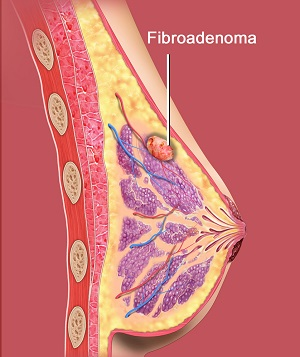
Fibroadenoma – Pathological Changes
Fibroadenoma is a benign (non-cancerous), solid breast tumor that most commonly occurs in young women, typically between 15–35 years of age. It arises from the stromal (connective) and epithelial (ductal) elements of the breast, hence the name fibro- (fibrous tissue) + adenoma (glandular tumor).
Pathogenesis
Hormone-sensitive tumor (especially estrogen)
Commonly enlarges during pregnancy or menstrual cycle, and may regress after menopause
Arises from terminal duct-lobular unit of the breast
Pathological Features
1. Gross Appearance
Well-circumscribed, oval or round, rubbery, mobile mass (“breast mouse”)
Non-tender, usually painless
Size typically ranges from 1–3 cm, but may be larger (giant fibroadenoma)
2. Microscopic (Histological) Features
Fibroadenoma is a biphasic tumor (has two components):
Component
Features
Stromal (fibrous)
Proliferation of fibrous connective tissue
Epithelial (glandular)
Proliferation of ducts and glandular epithelium
There are two growth patterns:
a. Pericanalicular Pattern:
Fibrous tissue surrounds and compresses the ducts
Ducts remain round or oval
b. Intracanalicular Pattern:
Fibrous tissue invades and distorts ducts, creating slit-like spaces
Most fibroadenomas show a mixture of both patterns.
3. Cellular Details:
Ducts lined by two layers: inner epithelial and outer myoepithelial cells (important to distinguish from malignancy)
No cellular atypia or mitosis
Stroma may be myxoid or hyalinized
Clinical Features
Feature
Description
Painless breast lump
Firm, mobile, well-defined
Common in young women
Ages 15–35 years
Increases with estrogen
May grow during pregnancy or hormone therapy
Regresses postmenopause
Hormone-dependent
Variants of Fibroadenoma
Variant
Feature
Giant fibroadenoma
Very large (>5 cm), common in adolescents
Juvenile fibroadenoma
Rapidly growing, seen in teenagers
Complex fibroadenoma
Contains cysts, sclerosing adenosis, or epithelial hyperplasia; slightly ↑ cancer risk
Diagnosis
Clinical examination
Ultrasound (especially in young women)
Mammography (in older women)
Fine-needle aspiration (FNA) or core biopsy to confirm diagnosis
Management
Approach
Indication
Observation
Small, asymptomatic fibroadenoma
Surgical excision
Large, symptomatic, or growing mass
Cryoablation or laser therapy
Minimally invasive alternatives
Regular follow-up
To monitor any changes or growth
Prognosis
Excellent – benign tumor
No risk of metastasis
Slight increase in cancer risk only in complex fibroadenomas
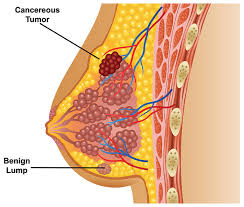
Carcinoma of the Breast – Pathological Changes
Breast carcinoma is a malignant tumor that arises most commonly from the epithelial lining of the ducts or lobules of the breast. It is the most common cancer in women worldwide and a leading cause of cancer-related deaths.
Risk Factors:
Female sex, increasing age
Family history (BRCA1, BRCA2 mutations)
Early menarche / late menopause
Nulliparity, late first pregnancy
Hormone replacement therapy
Obesity, alcohol, radiation exposure
Prolonged estrogen exposure
Types of Breast Carcinoma
A. Non-Invasive (In Situ) Carcinomas
Confined within the ducts or lobules; no stromal invasion
Type
Features
Ductal Carcinoma in Situ (DCIS)
Arises in ducts, may show comedo necrosis, calcifications, or cribriform patterns
Lobular Carcinoma in Situ (LCIS)
Arises in lobules, often multifocal and bilateral, marker for future invasive cancer
B. Invasive (Infiltrating) Carcinomas
Invade surrounding stroma, fat, lymphatics, and may metastasize.
Type
Features
Invasive Ductal Carcinoma (IDC)
Most common (~70–80%), hard, irregular mass, desmoplastic stroma
Invasive Lobular Carcinoma
~10%, single-file pattern of tumor cells, bilateral/multifocal tendency
Hard, irregular mass, often in the upper outer quadrant
May be fixed to skin or chest wall
Retraction of nipple or skin dimpling
Inflammatory type → swollen, red breast with peau d’orange
2. Microscopic Features
Feature
Description
Malignant epithelial cells
Irregular, pleomorphic nuclei, high N/C ratio
Invasion of stroma
Breaks through basement membrane
Desmoplasia
Dense fibrous tissue reaction (firm feel)
Mitotic figures
Increased cell division
Lymphovascular invasion
Common in aggressive types
Single-file cells (in lobular type)
Classic feature of lobular carcinoma
Molecular Subtypes (Based on Receptor Status)
Subtype
Receptors
Prognosis
Luminal A
ER+/PR+, HER2–
Best prognosis
Luminal B
ER+/PR+, HER2+
Moderate prognosis
HER2-enriched
ER–, PR–, HER2+
Aggressive
Triple-negative
ER–, PR–, HER2–
Poor prognosis, aggressive
Clinical Features
Feature
Explanation
Painless, hard breast lump
Most common presentation
Skin dimpling, nipple retraction
Tumor invasion of Cooper’s ligaments
Nipple discharge or eczema
In Paget’s disease
Peau d’orange
Lymphatic blockage by tumor cells
Axillary lymphadenopathy
Common first site of metastasis
Spread of Tumor
Route
Sites Affected
Lymphatic
Axillary → supraclavicular nodes
Hematogenous
Bones, lungs, liver, brain
Local invasion
Skin, muscle, chest wall
Investigations
Mammography: Detects microcalcifications
Ultrasound/MRI
FNAC / Core biopsy: Histological diagnosis
IHC for receptor status: ER, PR, HER2
Staging: TNM system (Tumor, Node, Metastasis)
Management
Treatment Modality
Used For
Surgery
Lumpectomy or mastectomy
Radiotherapy
After breast-conserving surgery
Chemotherapy
For high-grade or advanced tumors
Hormonal therapy
Tamoxifen (ER+), Aromatase inhibitors
Targeted therapy
Trastuzumab (HER2+ tumors)
Prognostic Factors
Good Prognosis
Poor Prognosis
Small tumor size
Large tumor
Negative lymph nodes
Node involvement
ER/PR positive
Triple negative
Low-grade tumor
High mitotic index, necrosis
CENTRAL NERVOUS SYSTEM (CNS)
Meningitis – Pathological Changes
Meningitis is an inflammation of the meninges, the protective membranes covering the brain and spinal cord. It can be acute or chronic, and is usually caused by bacteria, viruses, fungi, or tuberculosis.
Types of Meningitis and Their Causes
Type
Common Causes
Acute Bacterial Meningitis
Streptococcus pneumoniae, Neisseria meningitidis, Haemophilus influenzae, E. coli
Viral (Aseptic) Meningitis
Enteroviruses, HSV, mumps virus
Tuberculous Meningitis
Mycobacterium tuberculosis
Fungal Meningitis
Cryptococcus neoformans (especially in immunocompromised)
Pathological Changes in Meningitis (by type)
1. Acute Pyogenic (Bacterial) Meningitis
a. Gross Changes
Cloudy, opaque meninges
Purulent exudate on surface of brain, especially over convexities and base
Congested blood vessels
b. Microscopic Features
Neutrophilic infiltration in the subarachnoid space
Inflammation of leptomeninges (pia + arachnoid mater)
Fibrinous exudate, bacteria seen on Gram stain
Vasculitis, thrombosis of vessels → infarction
May involve ventricles (ventriculitis)
c. Complications
Hydrocephalus (due to blocked CSF flow)
Cerebral edema
Seizures, cranial nerve palsies
Abscess formation
2. Viral (Aseptic) Meningitis
a. Gross Changes
Meninges appear normal or slightly congested
b. Microscopic Features
Lymphocytic infiltration of meninges
Mild edema of brain tissue
No pus formation
No fibrin deposition
c. Prognosis
Generally self-limiting with full recovery
3. Tuberculous Meningitis
a. Gross Changes
Thick gelatinous exudate at the base of the brain
Involves cranial nerves and blood vessels
b. Microscopic Features
Granulomatous inflammation with:
Epithelioid cells
Langhans giant cells
Caseous necrosis
Lymphocytes and plasma cells in CSF
Vasculitis of arteries → infarction
May lead to hydrocephalus
c. Complications
Fibrosis, adhesions, hydrocephalus
Cranial nerve damage
4. Fungal Meningitis (e.g., Cryptococcal)
a. Seen in immunocompromised (HIV/AIDS)
Minimal inflammation
Clear gelatinous appearance of meninges
b. Microscopy
Capsulated yeast cells (e.g., Cryptococcus) in CSF
May be seen with India Ink stain
Mild mononuclear infiltration
CSF Findings (Key for Diagnosis)
Type
Appearance
Cells
Protein
Glucose
Pressure
Bacterial
Turbid
Neutrophils ↑
↑↑
↓↓
↑
Viral
Clear
Lymphocytes ↑
Normal/↑
Normal
Normal/↑
TB
Cobweb clot
Lymphocytes ↑
↑
↓
↑
Fungal
Clear/slightly hazy
Lymphocytes ↑
↑
↓/Normal
↑
Clinical Features of Meningitis
Sign/Symptom
Cause
Headache, fever
Inflammatory response
Neck stiffness (nuchal rigidity)
Meningeal irritation
Vomiting, photophobia
Raised intracranial pressure
Seizures, altered sensorium
Cerebral irritation or inflammation
Kernig’s/Brudzinski’s sign
Specific signs of meningeal irritation
Complications (Especially in bacterial/TB meningitis)
Hydrocephalus
Seizures
Hearing loss (CN VIII involvement)
Brain abscess
Death, if untreated
Summary
Meningitis is an inflammatory condition of the meninges caused by various pathogens.
Bacterial: Acute, neutrophilic response with pus and high fatality
Viral: Lymphocytic, milder course
Tuberculous: Chronic granulomatous inflammation
Fungal: Subtle, seen in immunocompromised patients Early diagnosis via CSF analysis, and prompt treatment are crucial.
Encephalitis – Pathological Changes
Encephalitis is an inflammation of the brain parenchyma, usually caused by viral infections. It is a potentially life-threatening condition that affects the neurons, glial cells, and blood vessels of the brain.
Common Causes of Encephalitis
Cause Type
Examples
Viral (most common)
Herpes Simplex Virus (HSV-1), Enteroviruses, Japanese Encephalitis virus, Rabies virus, Cytomegalovirus (CMV), Epstein-Barr Virus (EBV), HIV
Swollen brain with flattening of gyri and narrowing of sulci
Edematous and congested brain tissue
Petechial hemorrhages in severe cases
Softening of brain tissue (malacia)
2. Microscopic (Histological) Features
Feature
Description
Perivascular cuffing
Lymphocytes and plasma cells accumulate around blood vessels
Neuronal degeneration
Neurons show swelling, shrinkage, or necrosis
Microglial nodules
Small clusters of activated microglia around damaged neurons
Neuronophagia
Phagocytosis of injured neurons by microglia
Edema
Swelling of brain tissue, leading to increased intracranial pressure
Glial reaction (gliosis)
Proliferation of astrocytes in response to injury
3. Virus-Specific Features
Virus
Unique Pathological Features
Herpes Simplex Virus (HSV-1)
Necrosis and hemorrhage in temporal lobes, Cowdry type A inclusion bodies
Rabies virus
Negri bodies in neurons (esp. hippocampus, Purkinje cells)
Japanese Encephalitis
Inflammation, microglial nodules, neuronophagia in thalamus and basal ganglia
HIV
HIV encephalitis, multinucleated giant cells, microglial activation
Clinical Features of Encephalitis
Feature
Explanation
High-grade fever
Due to infection/inflammation
Altered mental status
Drowsiness, confusion, disorientation
Seizures
Due to neuronal irritation or cortical involvement
Headache, vomiting
Due to raised intracranial pressure
Focal neurological signs
Paralysis, speech issues, visual disturbances
Neck stiffness
Sometimes present (may mimic meningitis)
Behavioral changes
Especially in HSV encephalitis (affecting temporal lobes)
Diagnosis
Investigation
Finding
CSF analysis
Clear fluid, lymphocytic pleocytosis, ↑ protein, normal glucose
MRI/CT Brain
Edema, hemorrhage, especially in temporal lobes (HSV)
EEG
Abnormal electrical activity
PCR for viral DNA/RNA
Confirms viral cause (e.g., HSV, JE virus)
Serological tests
Antibodies to specific viruses
Management
Approach
Details
Antiviral therapy
Acyclovir for HSV encephalitis
Supportive care
Fluids, fever control, oxygen, seizure management
Corticosteroids
In autoimmune encephalitis or severe inflammation
Management of complications
E.g., cerebral edema, respiratory failure
Summary
Encephalitis is an inflammatory condition of the brain, often viral in origin, showing perivascular inflammation, neuronal destruction, microglial activation, and cerebral edema. It presents with fever, altered consciousness, seizures, and may lead to coma or death if untreated. Prompt diagnosis and antiviral therapy are critical.
Stroke – Pathological Changes
A stroke (also known as cerebrovascular accident – CVA) is a sudden loss of brain function caused by interruption of blood supply to the brain. This leads to neuronal injury, inflammation, and tissue death. Strokes can be ischemic or hemorrhagic, and the pathological changes vary accordingly.
Types of Stroke
Type
Description
Ischemic Stroke
Caused by blockage of a cerebral artery (80–85% of all strokes)
Hemorrhagic Stroke
Caused by rupture of a blood vessel leading to bleeding into brain tissue (15–20%)
Pathological Changes in Stroke
1. Ischemic Stroke (Cerebral Infarction)
Caused by thrombosis or embolism → reduced oxygen and glucose → cell death
a. Gross Pathology:
Affected area becomes pale and soft in early stages
Over time, it becomes edematous, then liquefies (liquefactive necrosis)
Later, cystic cavities form due to tissue breakdown
CT Scan: To differentiate ischemic vs. hemorrhagic stroke (bleeding appears bright)
MRI: More sensitive for early ischemic changes
Angiography: For aneurysms or vessel occlusion
Blood tests, ECG, carotid Doppler: For underlying causes
Summary
A stroke leads to tissue damage due to interrupted blood flow or bleeding.
In ischemic stroke, the brain undergoes liquefactive necrosis, inflammatory infiltration, and later gliosis.
In hemorrhagic stroke, blood accumulation causes neuronal destruction, pressure effects, and edema.
Time is brain – early diagnosis and treatment can limit permanent damage.
Tumors of the Central Nervous System (CNS) – Pathological Changes
CNS tumors are abnormal growths within the brain or spinal cord. They can be benign or malignant, primary or secondary (metastatic), and may arise from neurons, glial cells, meninges, or other components.
Classification of CNS Tumors
(Based on WHO & tissue origin)
I. Glial Cell Tumors (Gliomas)
(Arise from supporting glial cells)
Type
Cell of Origin
Features
Astrocytoma
Astrocytes
Most common glioma; graded I–IV
Glioblastoma multiforme (GBM)
High-grade astrocytoma (Grade IV)
Aggressive, necrosis, hemorrhage
Oligodendroglioma
Oligodendrocytes
Slow-growing, calcifications, “fried-egg” cells
Ependymoma
Ependymal cells
Common in 4th ventricle (kids), spinal cord (adults)
“Fried-egg” appearance of cells, delicate capillary network
Prognosis
Relatively better than GBM
4. Ependymoma
Feature
Description
Location
4th ventricle (children), spinal canal (adults)
Microscopy
Perivascular pseudorosettes, true rosettes
CSF spread possible
May block CSF → hydrocephalus
5. Medulloblastoma
Feature
Description
Population
Children, cerebellum
Microscopy
Small round blue cells, Homer-Wright rosettes
Aggressive
Spreads via CSF – drop metastases in spinal cord
General Pathological Features of CNS Tumors
Mass effect: Pressure on adjacent brain tissue → headache, vomiting, papilledema
Edema: Due to disrupted blood-brain barrier
Necrosis & hemorrhage: Common in high-grade tumors (e.g., GBM)
Infiltration vs. compression:
Malignant tumors (gliomas) infiltrate
Benign tumors (meningioma) compress
Diagnosis Tools
MRI with contrast – gold standard
CT scan – quick for hemorrhage or calcification
Biopsy – definitive diagnosis
CSF analysis – for medulloblastoma or ependymoma (if spinal spread suspected)
Treatment Options
Method
Used For
Surgical excision
First-line for accessible tumors
Radiotherapy
Especially for malignant/inoperable tumors
Chemotherapy
Used in GBM, medulloblastoma
Targeted therapies
Based on genetic mutations (e.g., IDH, MGMT status in gliomas)
Summary
CNS tumors include a wide range of benign and malignant neoplasms. Gliomas (especially glioblastoma) are the most common malignant primary brain tumors. Meningiomas and schwannomas are usually benign. Pathological changes include cellular atypia, necrosis, vascular proliferation, and infiltrative growth, depending on the tumor type.
FOR UNLOCK 🔓 FULL COURSE NOW. MORE DETAILS CALL US OR WATSAPP ON- 8485976407