Proteins are large biomolecules composed of amino acids linked by peptide bonds. They are essential macromolecules that perform a vast range of functions in biological systems, including enzymatic catalysis, structural support, transport, communication, and immune responses.
I. Structure of Proteins
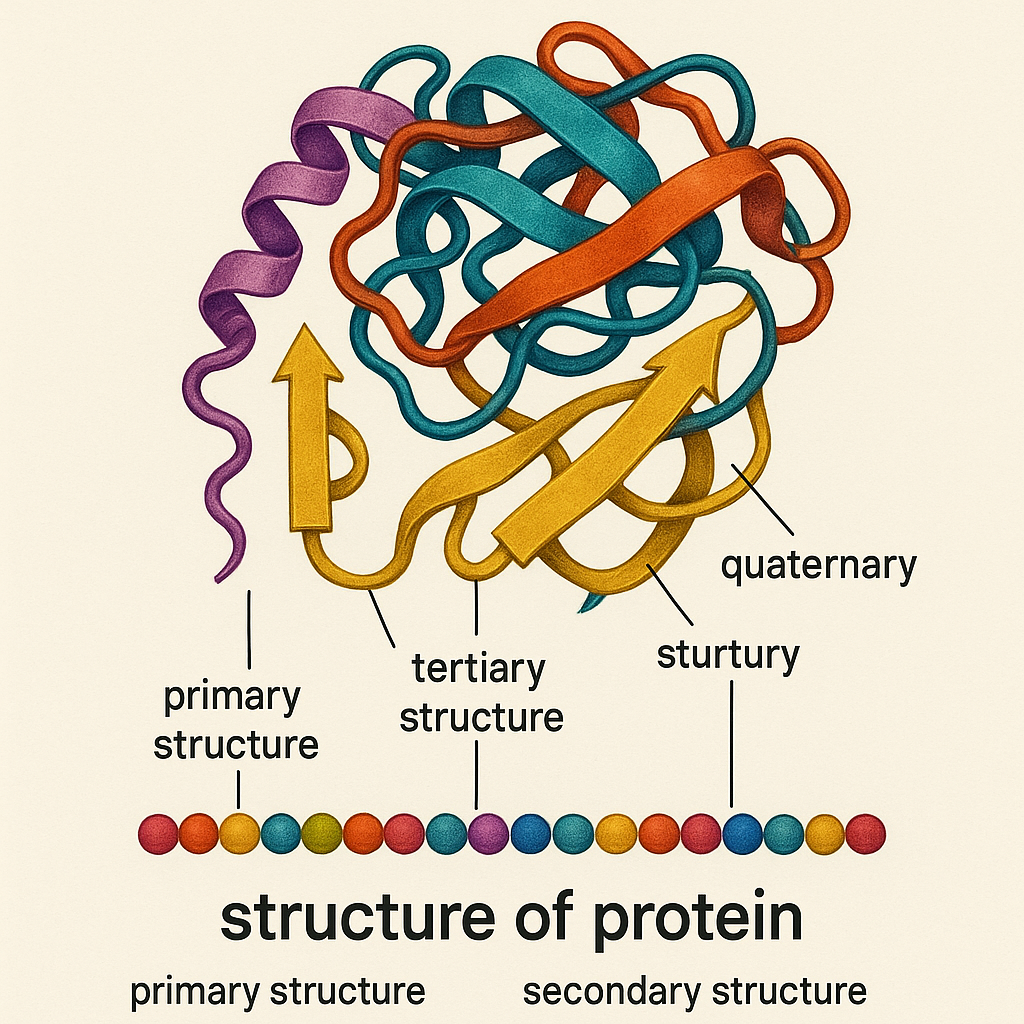
Proteins have four levels of structural organization:
1. Primary Structure
Refers to the linear sequence of amino acids in a polypeptide chain.
Determined by the genetic code.
Peptide bonds hold amino acids together.
2. Secondary Structure
Refers to local folding patterns within the polypeptide chain.
Common secondary structures:
Alpha-helix (α-helix): A right-handed coil stabilized by hydrogen bonds.
Beta-pleated sheet (β-sheet): Formed by hydrogen bonds between strands.
Random coil: Unstructured regions connecting helices and sheets.
3. Tertiary Structure
The 3D structure of a protein due to interactions among R-groups of amino acids.
Stabilized by:
Hydrogen bonds
Disulfide bonds (covalent bonds between cysteine residues)
Hydrophobic interactions
Ionic bonds
Van der Waals forces
4. Quaternary Structure
Formed when two or more polypeptide chains (subunits) interact to form a functional protein.
Examples: Hemoglobin (four subunits), DNA polymerase (multiple subunits).
II. Classification of Proteins
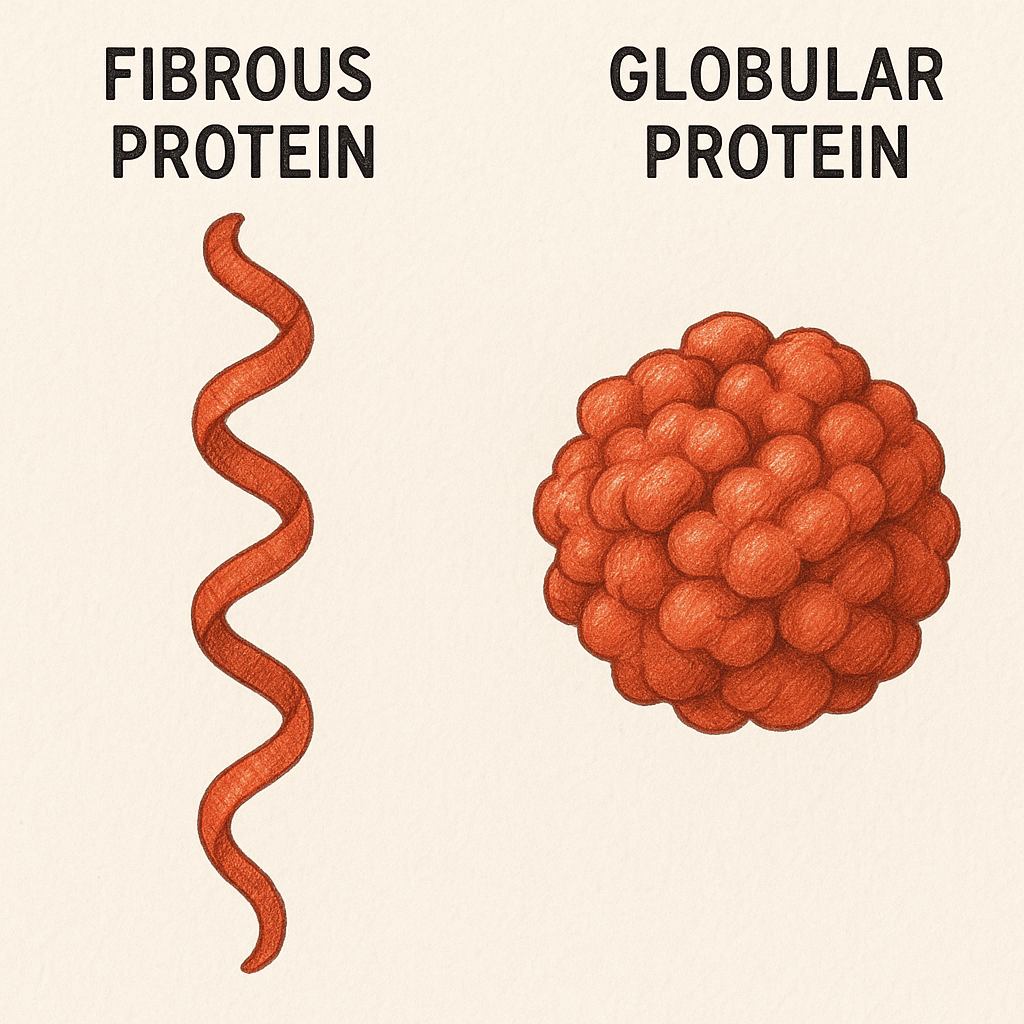
A. Based on Structure
Fibrous Proteins – Insoluble, provide structural support.
Examples: Collagen, Keratin, Myosin
Globular Proteins – Soluble, functional proteins.
Examples: Hemoglobin, Enzymes, Antibodies
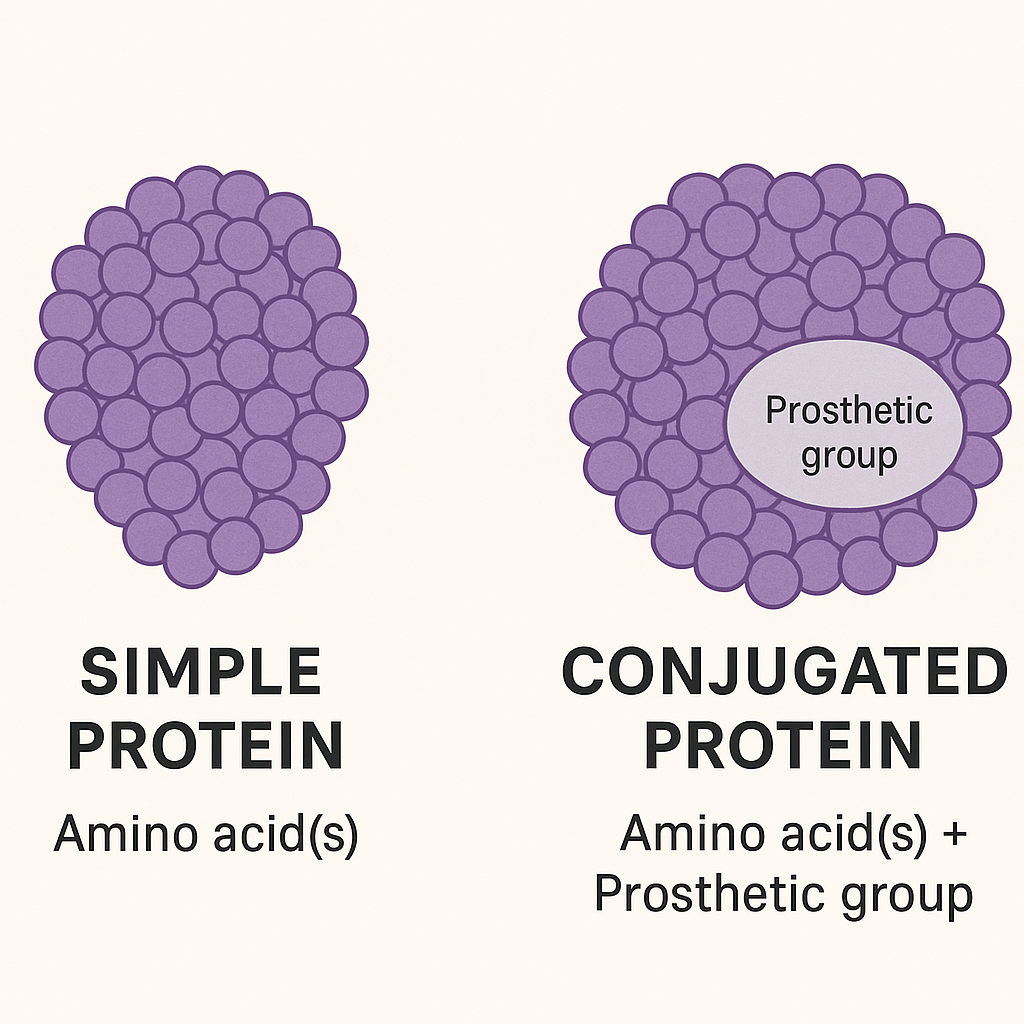
B. Based on Composition
Simple Proteins – Contain only amino acids.
Examples: Albumin, Globulin
Conjugated Proteins – Contain a non-protein component (prosthetic group).
Bradford Assay: Protein quantification using Coomassie dye.
Western Blot: Detects specific proteins in a sample.
Urea and Creatinine Levels: Assess protein metabolism in kidney function.
VIII. Dietary Sources of Protein
High-Quality (Complete) Proteins:
Animal sources: Eggs, Meat, Fish, Dairy
Plant sources: Soybeans, Quinoa
Low-Quality (Incomplete) Proteins:
Legumes, Grains, Nuts (can be combined to form complete proteins, e.g., rice + beans).
Classification of Amino Acids Based on Nutrition
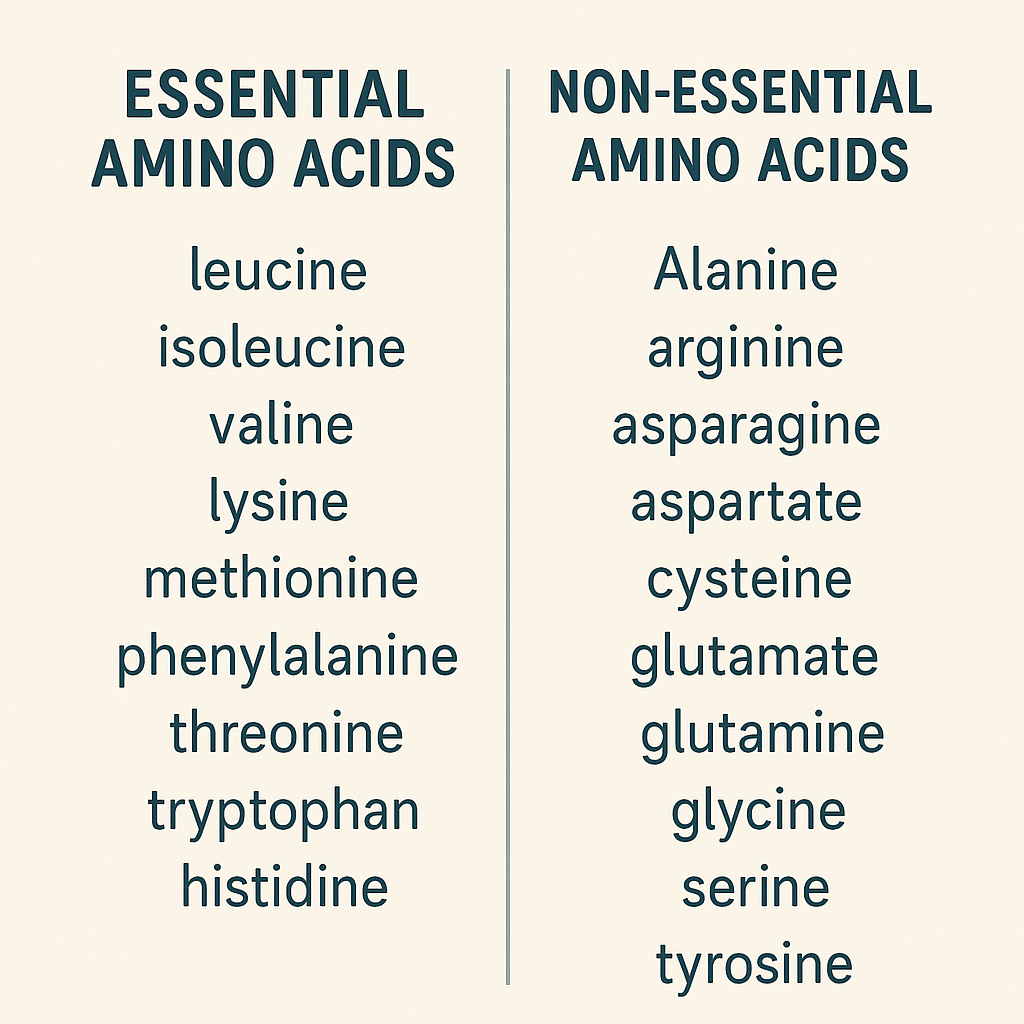
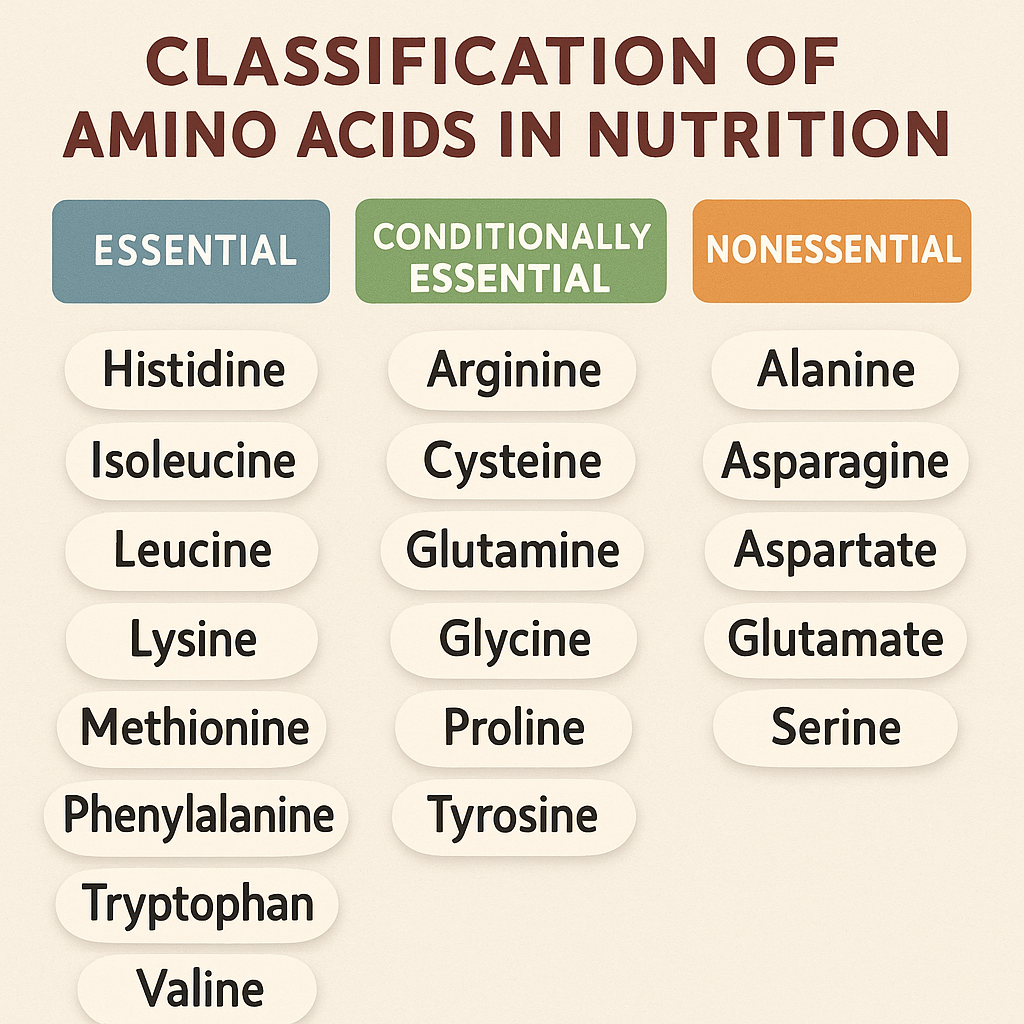
Amino acids are the building blocks of proteins and are classified based on various criteria, including their nutritional importance. Based on nutrition, amino acids are classified into Essential, Non-Essential, and Conditionally Essential amino acids.
I. Classification of Amino Acids Based on Nutrition
Amino acids can be categorized based on whether they can be synthesized in the body or need to be obtained from the diet.
These amino acids are normally non-essential, but become essential under specific conditions such as stress, illness, or rapid growth (infants, children, critically ill patients).
The body may not produce them in sufficient amounts during such times.
List of Conditionally Essential Amino Acids:
Arginine (Essential in infants, trauma, sepsis)
Cysteine (Precursor for glutathione, important in detoxification)
Glutamine (Most abundant amino acid; crucial for gut and immune function)
Glycine (Plays a role in collagen formation and neurotransmission)
Proline (Important for wound healing and collagen synthesis)
Tyrosine (Synthesized from phenylalanine; precursor for dopamine, thyroid hormones)
Ornithine (Involved in the urea cycle, essential during stress conditions)
Functions of Conditionally Essential Amino Acids:
Arginine: Supports nitric oxide production (vasodilation).
Cysteine: Precursor for antioxidant glutathione.
Glutamine: Helps in intestinal and immune health.
Glycine: Component of collagen, supports neurotransmission.
Proline: Involved in wound healing and connective tissue repair.
Tyrosine: Precursor for neurotransmitters and thyroid hormones.
Used in neurotransmitter and thyroid hormone production.
Arginine
Used for vasodilation (cardiovascular health).
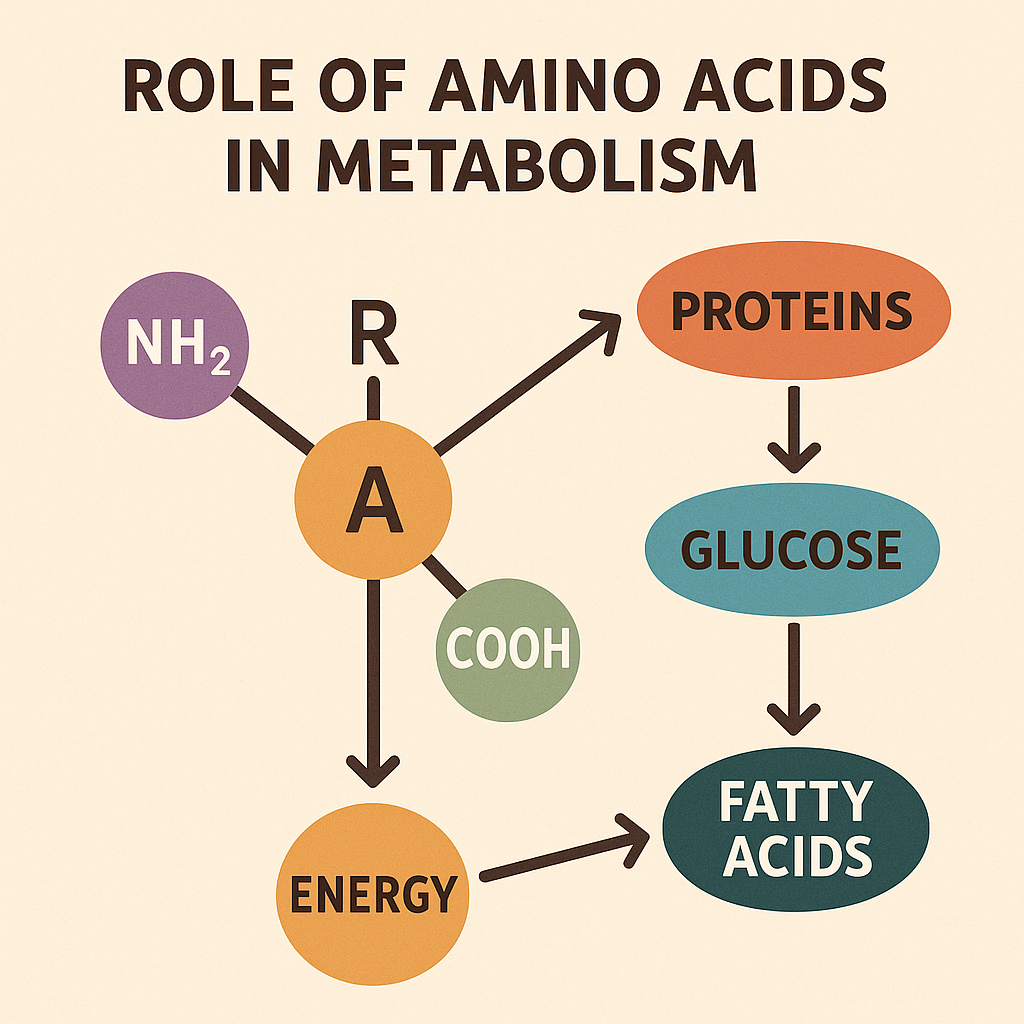
Classification of Amino Acids Based on Metabolic Rate
Amino acids can be classified based on their metabolic fate into three main categories:
Glucogenic Amino Acids
Ketogenic Amino Acids
Both Glucogenic and Ketogenic Amino Acids
This classification is based on whether the amino acid is metabolized to form glucose, ketone bodies, or both.
I. Glucogenic Amino Acids
Definition: Amino acids that are metabolized to pyruvate or TCA cycle intermediates (e.g., oxaloacetate, α-ketoglutarate, succinyl-CoA, fumarate) which can be used for gluconeogenesis to produce glucose.
Function: Important for energy production, especially during fasting or starvation.
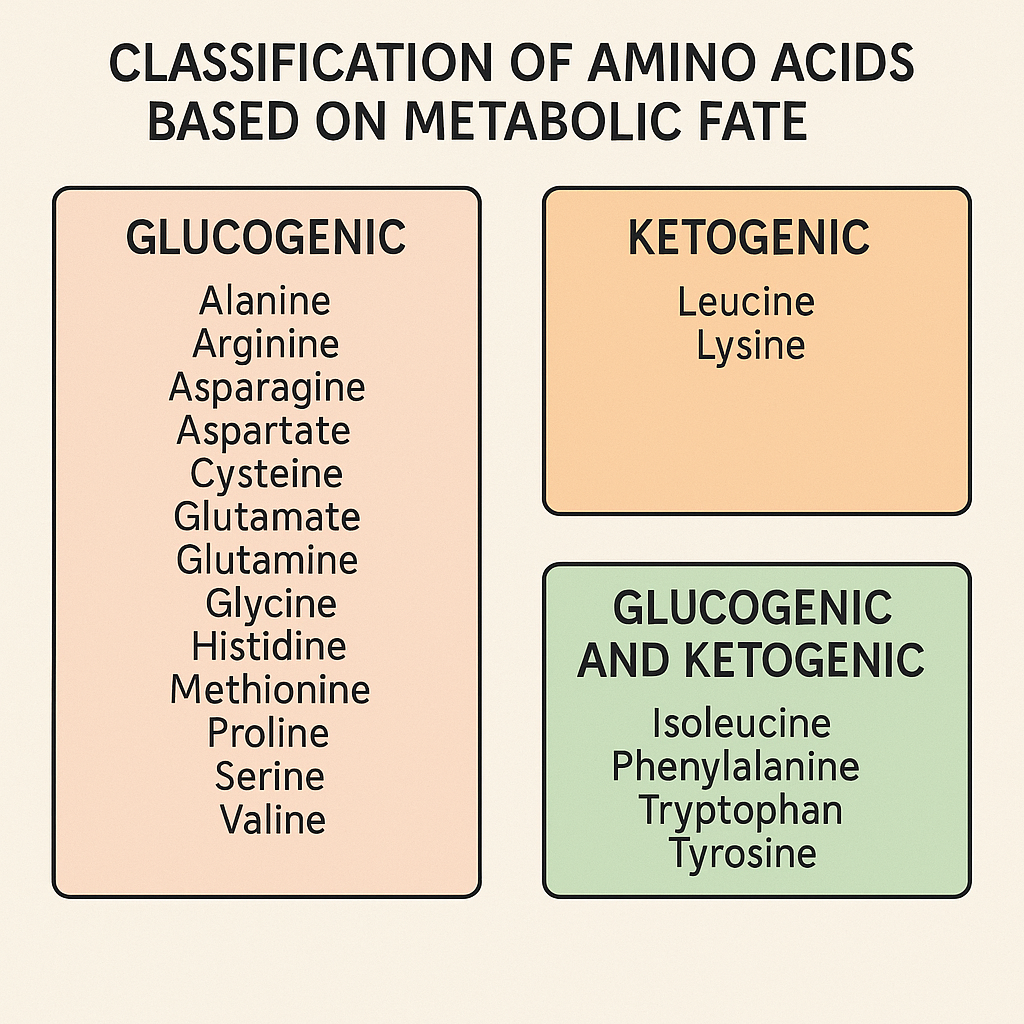
Examples of Glucogenic Amino Acids
Alanine → Pyruvate
Aspartate → Oxaloacetate
Glutamate → α-Ketoglutarate
Serine → Pyruvate
Methionine → Succinyl-CoA
Arginine → α-Ketoglutarate
Histidine → α-Ketoglutarate
Proline → α-Ketoglutarate
Valine → Succinyl-CoA
Cysteine → Pyruvate
Glycine → Serine → Pyruvate
Mnemonic for Glucogenic Amino Acids:
“All His Army Soldiers March Past Very Quickly” (Alanine, Histidine, Aspartate, Serine, Methionine, Proline, Valine, QGlutamine)
II. Ketogenic Amino Acids
Definition: Amino acids that are metabolized into acetyl-CoA or acetoacetyl-CoA, which can be converted into ketone bodies (acetoacetate, β-hydroxybutyrate) or used in fatty acid synthesis.
Function: Used for energy during prolonged fasting, starvation, or low-carbohydrate diets.
Examples of Ketogenic Amino Acids
Leucine → Acetyl-CoA & Acetoacetate
Lysine → Acetyl-CoA
Mnemonic for Ketogenic Amino Acids:
“L-K for Keto” (Leucine and Kysine are purely ketogenic.)
III. Both Glucogenic and Ketogenic Amino Acids
Definition: Amino acids that have metabolic pathways leading to both gluconeogenesis and ketogenesis.
Function: Can be converted into either glucose (for energy) or ketone bodies (for alternative fuel).
Examples of Both Glucogenic & Ketogenic Amino Acids
Phenylalanine → Fumarate + Acetoacetate
Isoleucine → Succinyl-CoA + Acetyl-CoA
Tryptophan → Pyruvate + Acetoacetate
Tyrosine → Fumarate + Acetoacetate
Threonine → Succinyl-CoA + Acetyl-CoA
Mnemonic for Both Glucogenic & Ketogenic Amino Acids:
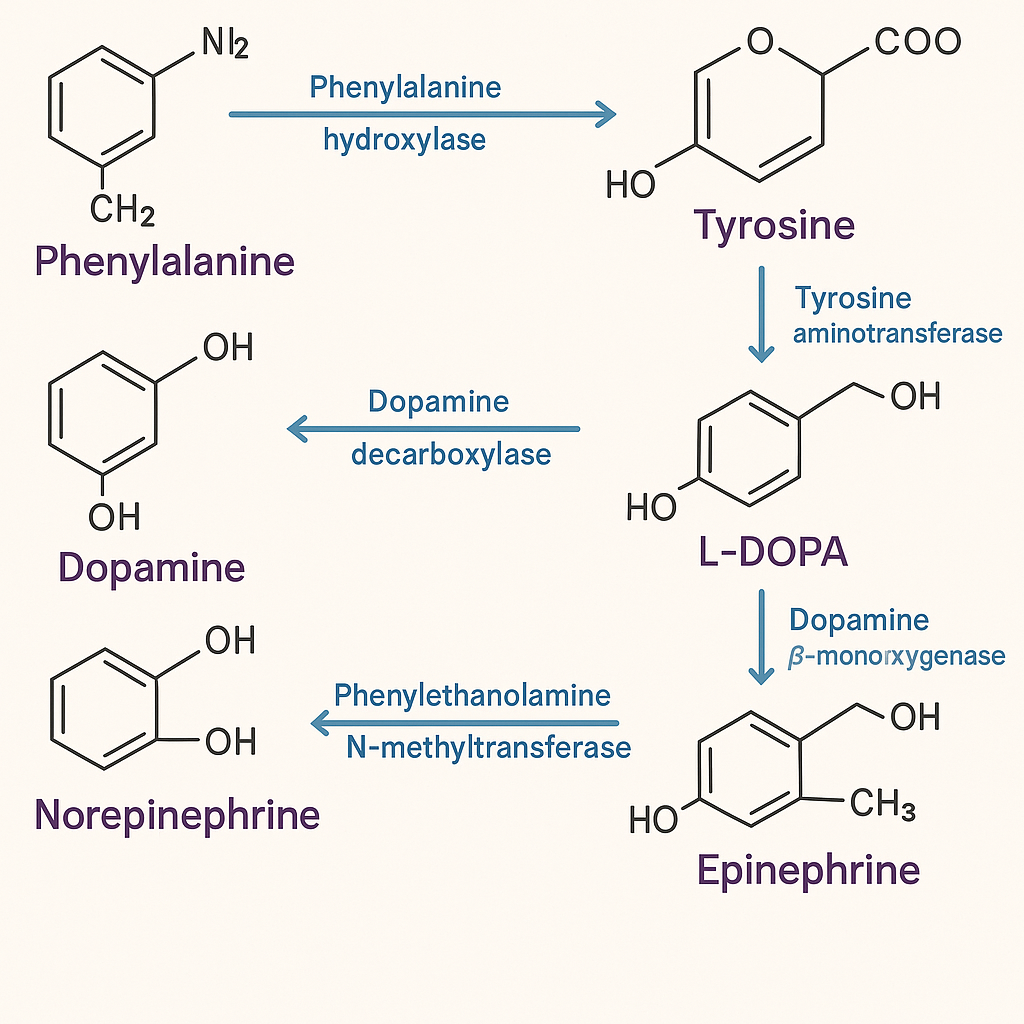
Phenylketonuria (PKU): Phenylalanine cannot be converted into tyrosine due to deficiency of phenylalanine hydroxylase.
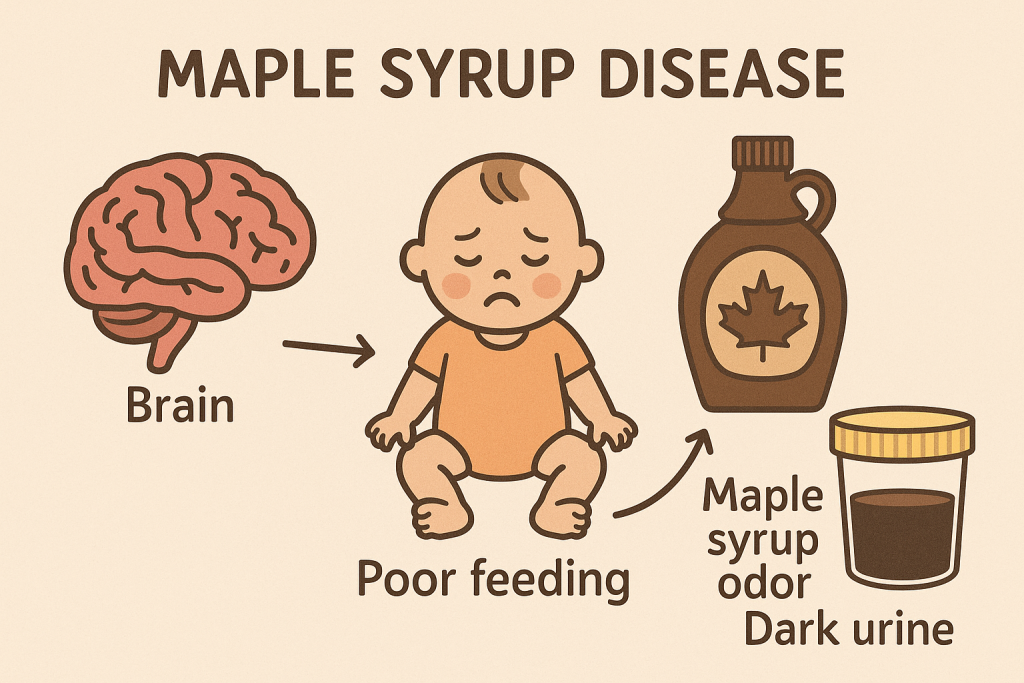
Maple Syrup Urine Disease (MSUD): Deficiency in branched-chain ketoacid dehydrogenase affecting valine, leucine, and isoleucine metabolism.
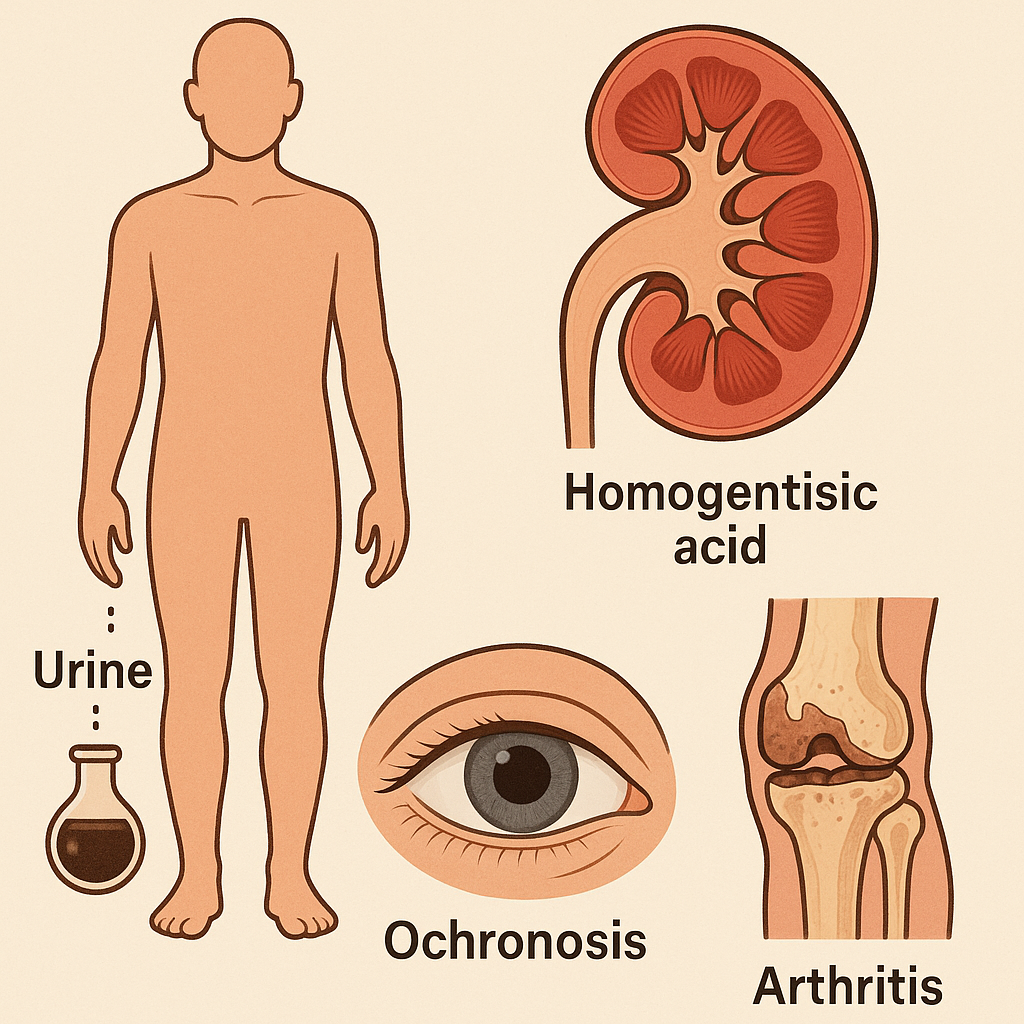
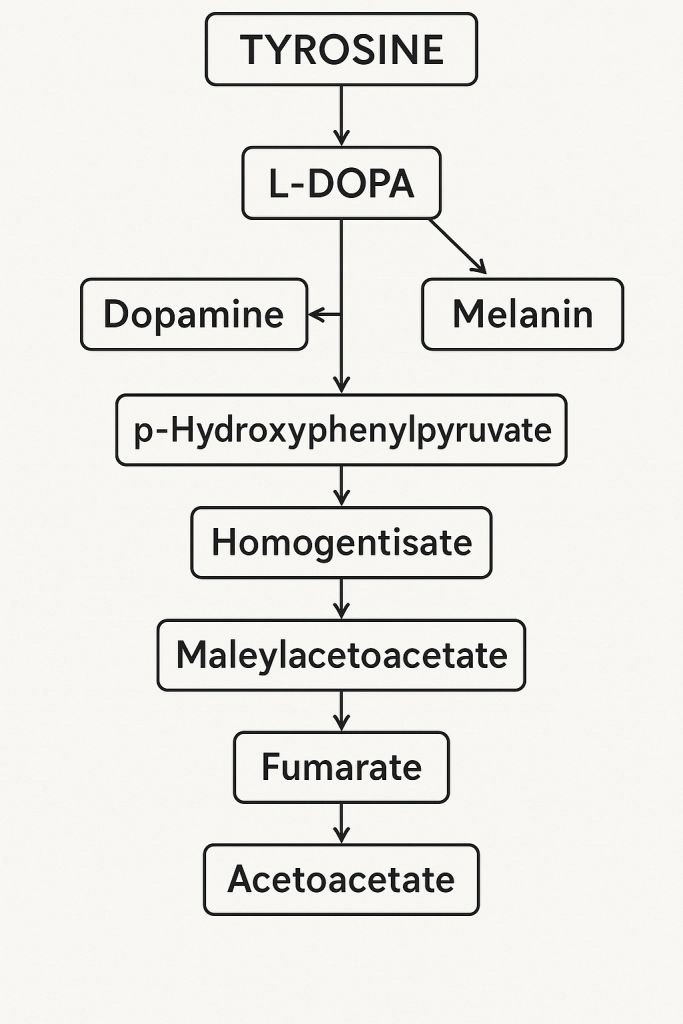
Alkaptonuria: Accumulation of homogentisic acid due to a defect in tyrosine metabolism.
Relevance in Diet and Nutrition
Ketogenic amino acids are important for people on ketogenic diets.
Glucogenic amino acids are crucial for maintaining blood glucose levels during fasting.
Amino Acids in Starvation
During fasting, glucogenic amino acids provide glucose via gluconeogenesis.
During prolonged starvation, ketogenic amino acids contribute to ketone body formation for brain energy.
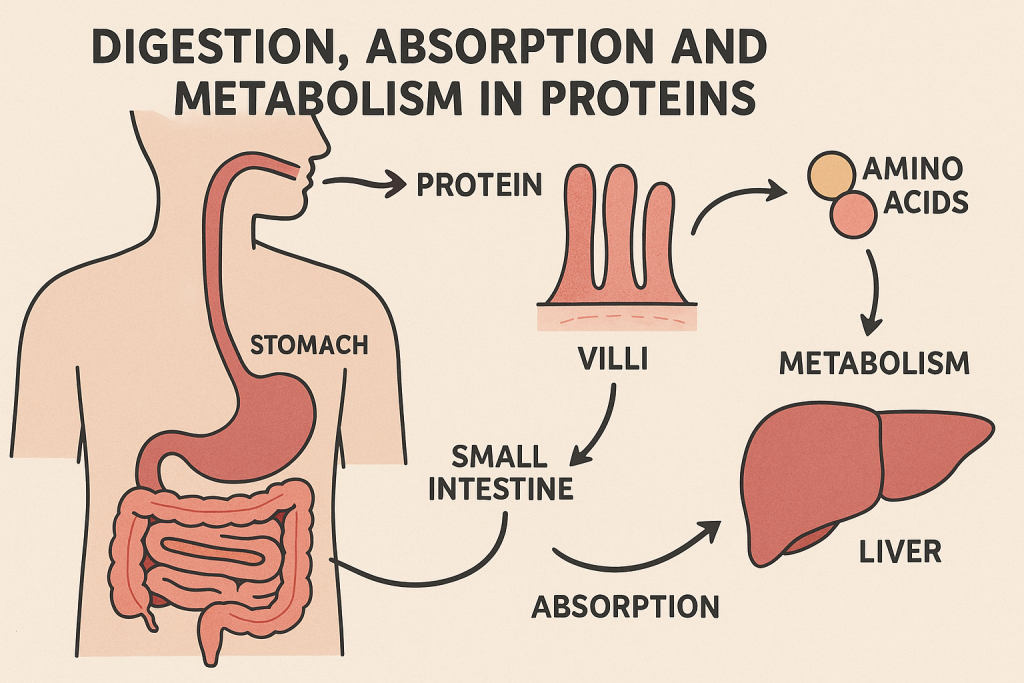
Digestion, Absorption, and Metabolism of Proteins
Proteins are essential macromolecules that play a vital role in the body’s structure, function, and metabolism. The digestion, absorption, and metabolism of proteins involve several biochemical processes that convert dietary proteins into amino acids, which are then utilized for various physiological functions.
I. Digestion of Proteins
Protein digestion involves the breakdown of complex protein molecules into amino acids through the action of enzymes in different parts of the digestive system.
1. Digestion in the Mouth
No enzymatic digestion of protein occurs in the mouth.
Mechanical digestion (chewing) helps break down protein-rich foods into smaller pieces, increasing the surface area for enzyme action.
2. Digestion in the Stomach
Gastric juice is secreted, containing hydrochloric acid (HCl) and pepsinogen.
Hydrochloric acid (HCl):
Denatures proteins (unfolds their structure).
Activates pepsinogen into pepsin.
Pepsin: A protease that breaks down proteins into smaller peptides and polypeptides.
End Products: Large polypeptides, some oligopeptides.
3. Digestion in the Small Intestine
Pancreatic enzymes complete the digestion process:
Trypsin (activated from trypsinogen by enterokinase) → Breaks down polypeptides.
Chymotrypsin (activated from chymotrypsinogen) → Breaks down larger peptides.
Carboxypeptidase → Removes terminal amino acids from polypeptides.
Elastase → Breaks down elastin proteins.
Brush Border Enzymes (Intestinal Enzymes):
Aminopeptidase: Removes amino acids from the N-terminal.
Dipeptidase: Breaks down dipeptides into free amino acids.
End Products of Digestion: Free amino acids, dipeptides, and tripeptides.
II. Absorption of Amino Acids
Absorption occurs mainly in the jejunum and ileum of the small intestine.
Amino acids are absorbed via active transport and facilitated diffusion.
1. Transport Mechanisms
Sodium-Dependent Transport: Amino acids are absorbed along with Na⁺ ions using energy.
Sodium-Independent Transport: Facilitated diffusion via carrier proteins.
Peptide Transport (PepT1): Dipeptides and tripeptides are absorbed faster than free amino acids.
2. Absorption of Special Amino Acids
Branched-chain amino acids (Leucine, Isoleucine, Valine) are absorbed preferentially by muscles.
Glutamine is used by enterocytes for energy.
Cysteine and Methionine require active transport.
After absorption, amino acids enter the portal circulation and are transported to the liver for metabolism.
III. Metabolism of Proteins
Protein metabolism includes the utilization, breakdown, and excretion of amino acids.
1. Amino Acid Pool
The body maintains a free amino acid pool for protein synthesis, energy production, and conversion to other compounds.
Sources:
Dietary proteins.
Breakdown of body proteins (proteolysis).
De novo synthesis of non-essential amino acids.
2. Protein Anabolism (Synthesis of Proteins)
Transcription (DNA → mRNA) and Translation (mRNA → Protein) occur in ribosomes.
Amino acids are linked by peptide bonds to form functional proteins.
3. Catabolism of Proteins (Amino Acid Degradation)
When proteins are broken down, their amino acids undergo deamination, transamination, and urea cycle processing.
A. Transamination (Transfer of Amino Group)
Transfer of an amino group (-NH₂) from one amino acid to a keto acid.
Disorders Related to Protein Digestion, Absorption, and Metabolism
Protein metabolism disorders occur due to enzyme deficiencies, genetic mutations, or malabsorption issues. These disorders affect digestion, absorption, amino acid metabolism, or nitrogen excretion, leading to severe physiological complications.
I. Disorders Related to Protein Digestion and Absorption
These disorders arise due to deficiencies in digestive enzymes or problems in intestinal absorption.
1. Protein-Energy Malnutrition (PEM)
Cause: Insufficient protein intake.
Types:
Kwashiorkor
Occurs with adequate calorie intake but low protein intake.
Biologically Important Compounds Synthesized from Various Amino Acids
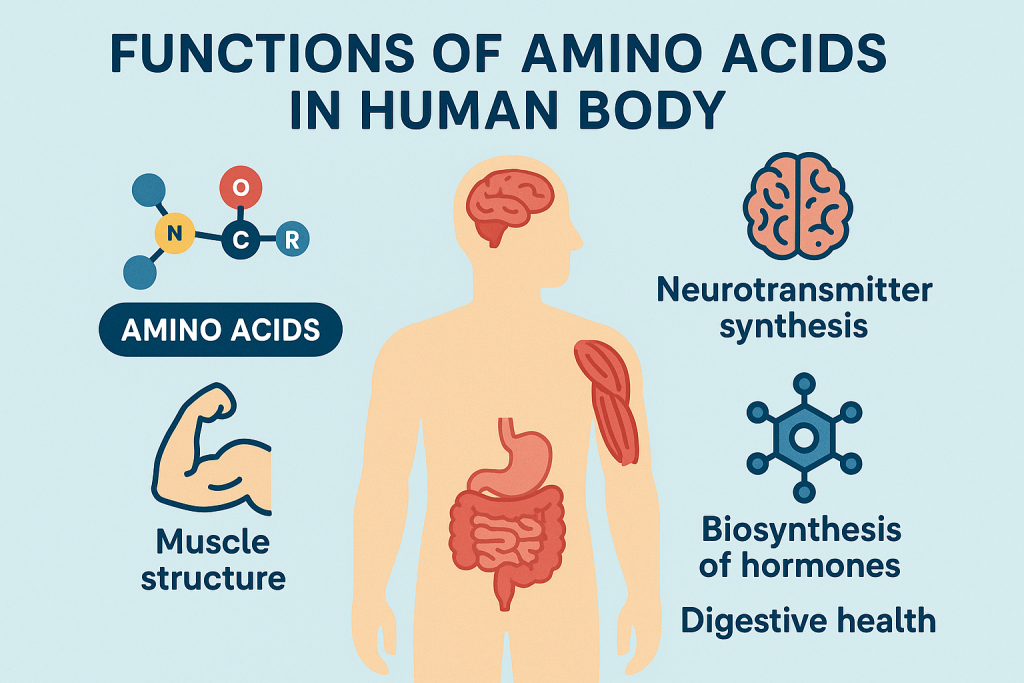
Amino acids serve as precursors for many biologically important compounds in the body. These compounds are essential for metabolism, neurotransmission, detoxification, and cellular function.
I. Biologically Important Compounds and Their Amino Acid Precursors
Amino acids are involved in the biosynthesis of neurotransmitters, hormones, nucleotides, and other biomolecules.
1. Neurotransmitters and Hormones
Biologically Important Compound
Precursor Amino Acid
Function
Dopamine
Tyrosine
Neurotransmitter, mood regulation
Norepinephrine (Noradrenaline)
Tyrosine
Fight-or-flight response
Epinephrine (Adrenaline)
Tyrosine
Increases heart rate, stress response
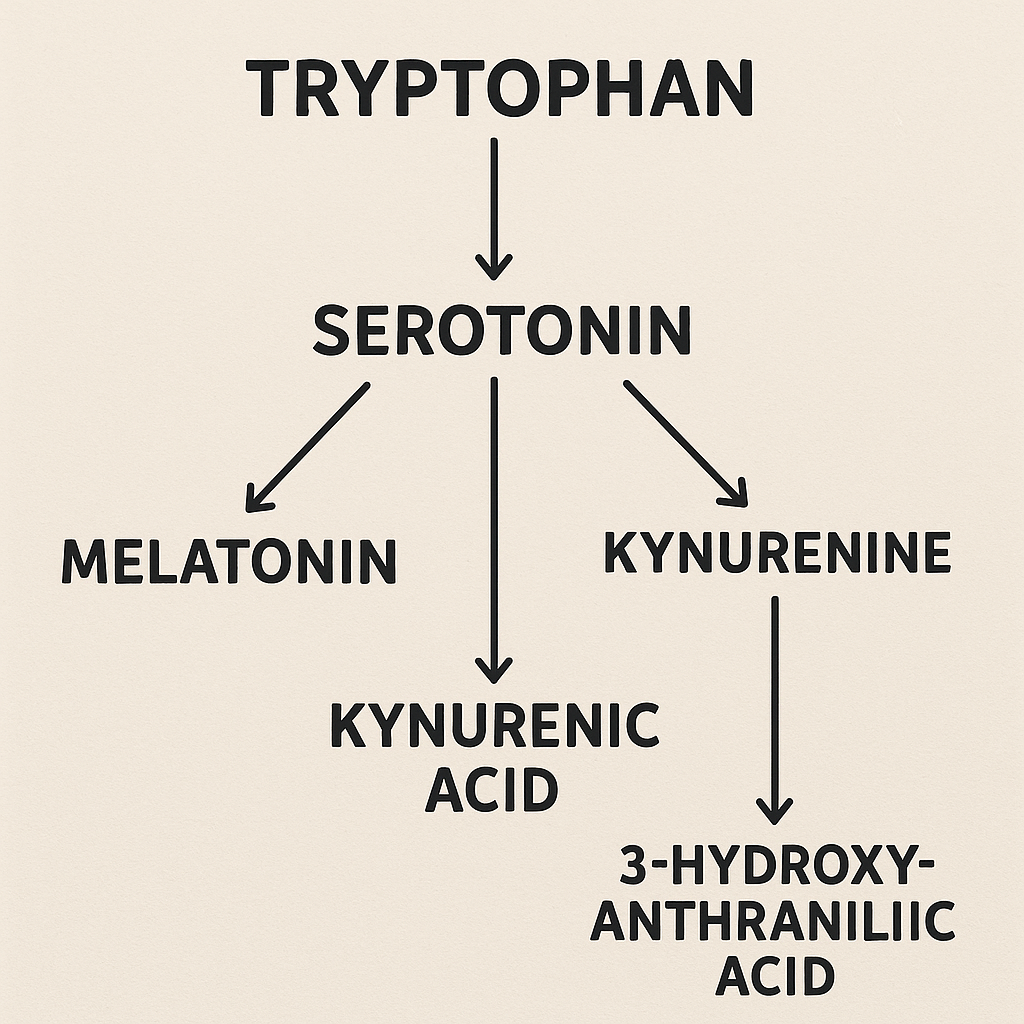
Serotonin
Tryptophan
Mood regulation, sleep-wake cycle
Melatonin
Tryptophan
Regulates circadian rhythm
Histamine
Histidine
Inflammatory response, allergic reactions
γ-Aminobutyric acid (GABA)
Glutamate
Inhibitory neurotransmitter
Acetylcholine
Serine
Muscle contraction, memory function
Thyroid Hormones (T3, T4)
Tyrosine
Regulates metabolism
2. Energy Metabolism and Antioxidants
Biologically Important Compound
Precursor Amino Acid
Function
Creatine
Arginine + Glycine + Methionine
Energy storage in muscles
Glutathione
Glutamate + Cysteine + Glycine
Antioxidant, detoxification
Carnitine
Lysine + Methionine
Fatty acid transport into mitochondria
Coenzyme A
Cysteine
Energy metabolism
3. Nucleotide Synthesis (DNA & RNA Precursors)
Biologically Important Compound
Precursor Amino Acid
Function
Purines (Adenine, Guanine)
Glycine, Aspartate, Glutamine
DNA and RNA synthesis
Pyrimidines (Cytosine, Thymine, Uracil)
Aspartate, Glutamine
DNA and RNA synthesis
SAM (S-Adenosyl Methionine)
Methionine
Methylation reactions
4. Structural and Functional Proteins
Biologically Important Compound
Precursor Amino Acid
Function
Collagen
Glycine + Proline + Hydroxyproline
Connective tissue strength
Keratin
Cysteine
Hair, nails, skin structure
Elastin
Glycine + Valine + Alanine
Elastic properties of tissues
5. Other Biologically Important Compounds
Biologically Important Compound
Precursor Amino Acid
Function
Heme (Hemoglobin, Myoglobin, Cytochromes)
Glycine
Oxygen transport, electron transport chain
Nitric Oxide (NO)
Arginine
Vasodilation, immune response
Urea (End Product of Protein Metabolism)
Arginine (via Urea Cycle)
Excretion of nitrogen waste
II. Summary of Amino Acids and Their Biologically Important Derivatives
Inborn errors of amino acid metabolism are genetic disorders caused by enzyme deficiencies affecting the breakdown, synthesis, or transport of amino acids. These disorders result in the accumulation or deficiency of specific amino acids and their metabolites, leading to neurological, developmental, and metabolic complications.
I. Classification of Inborn Errors of Amino Acid Metabolism
These disorders can be classified based on the affected metabolic pathway:
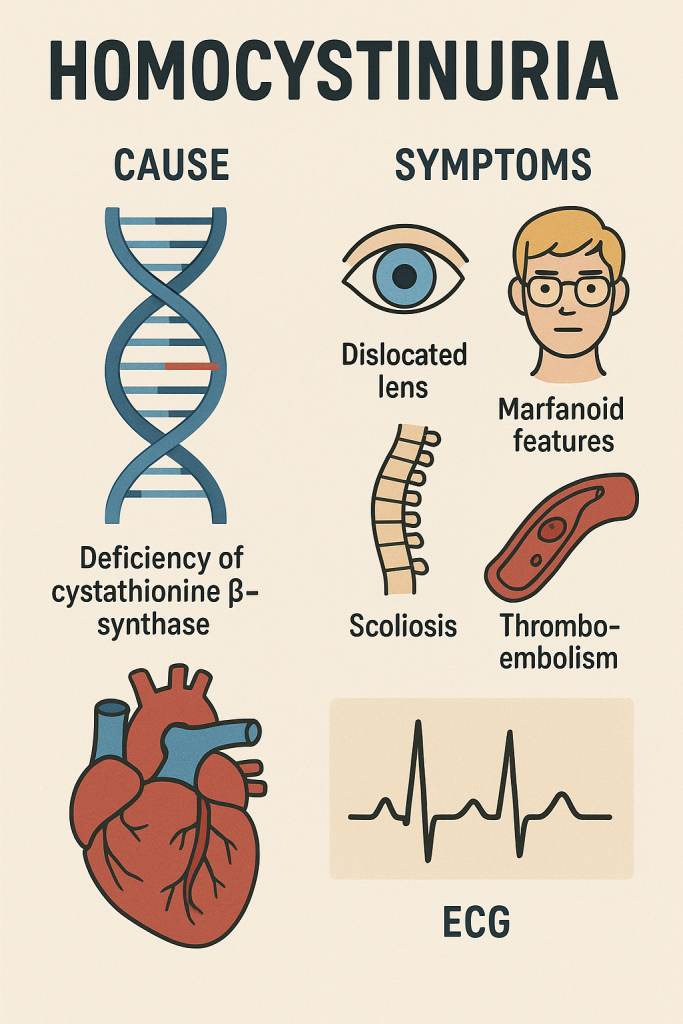
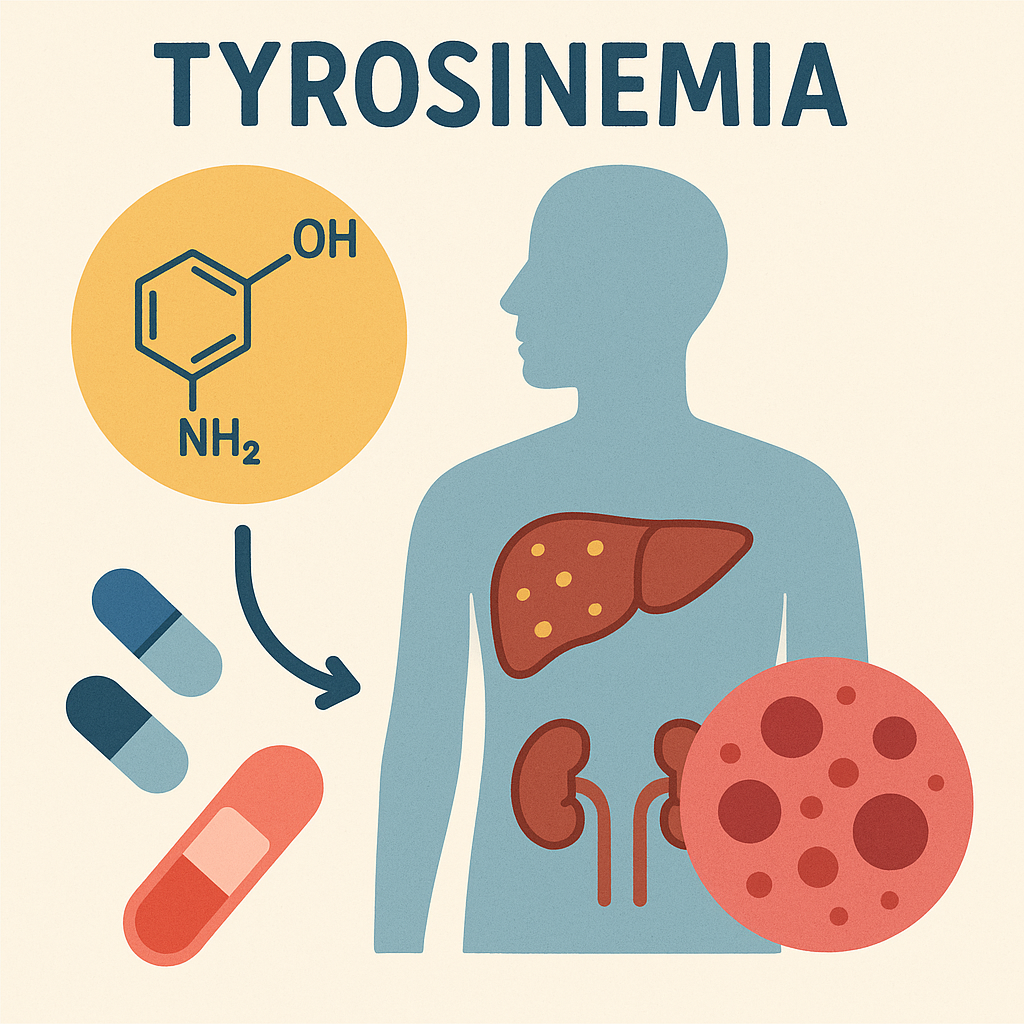
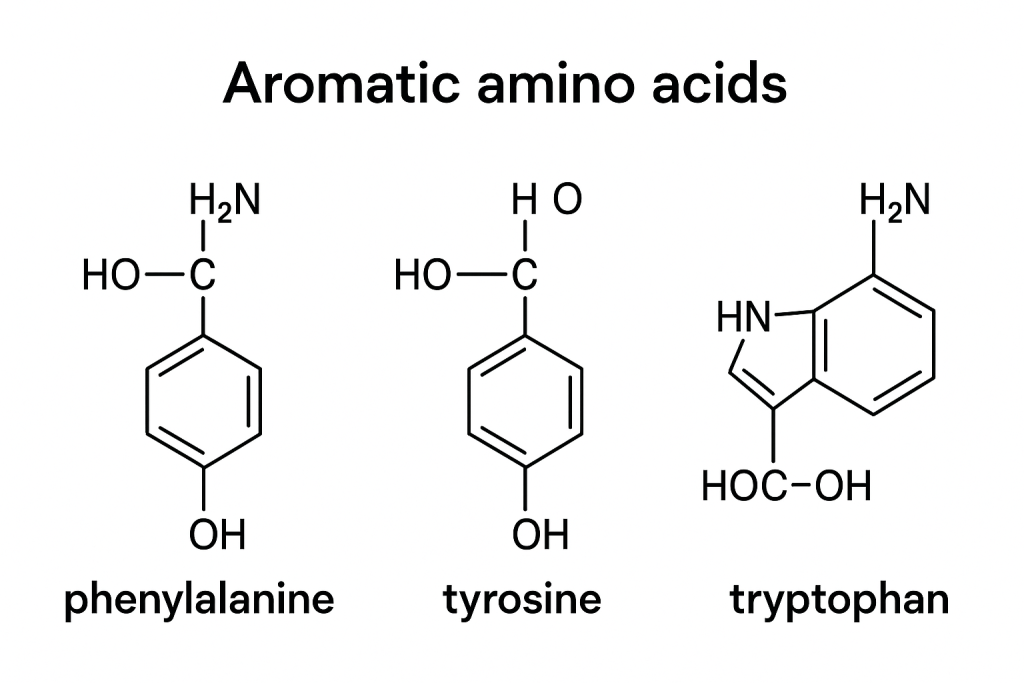
Disorders of Phenylalanine and Tyrosine Metabolism
Disorders of Branched-Chain Amino Acid Metabolism
Disorders of Sulfur-Containing Amino Acid Metabolism
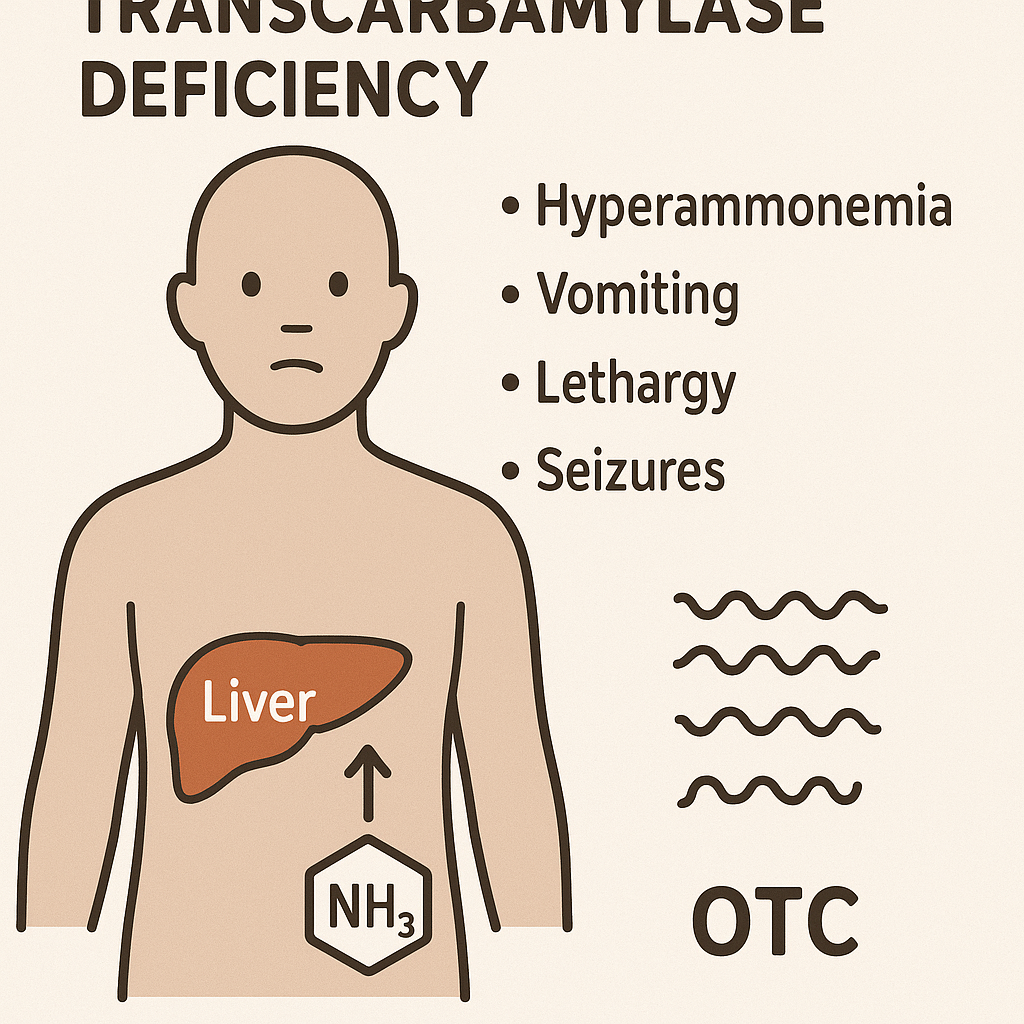
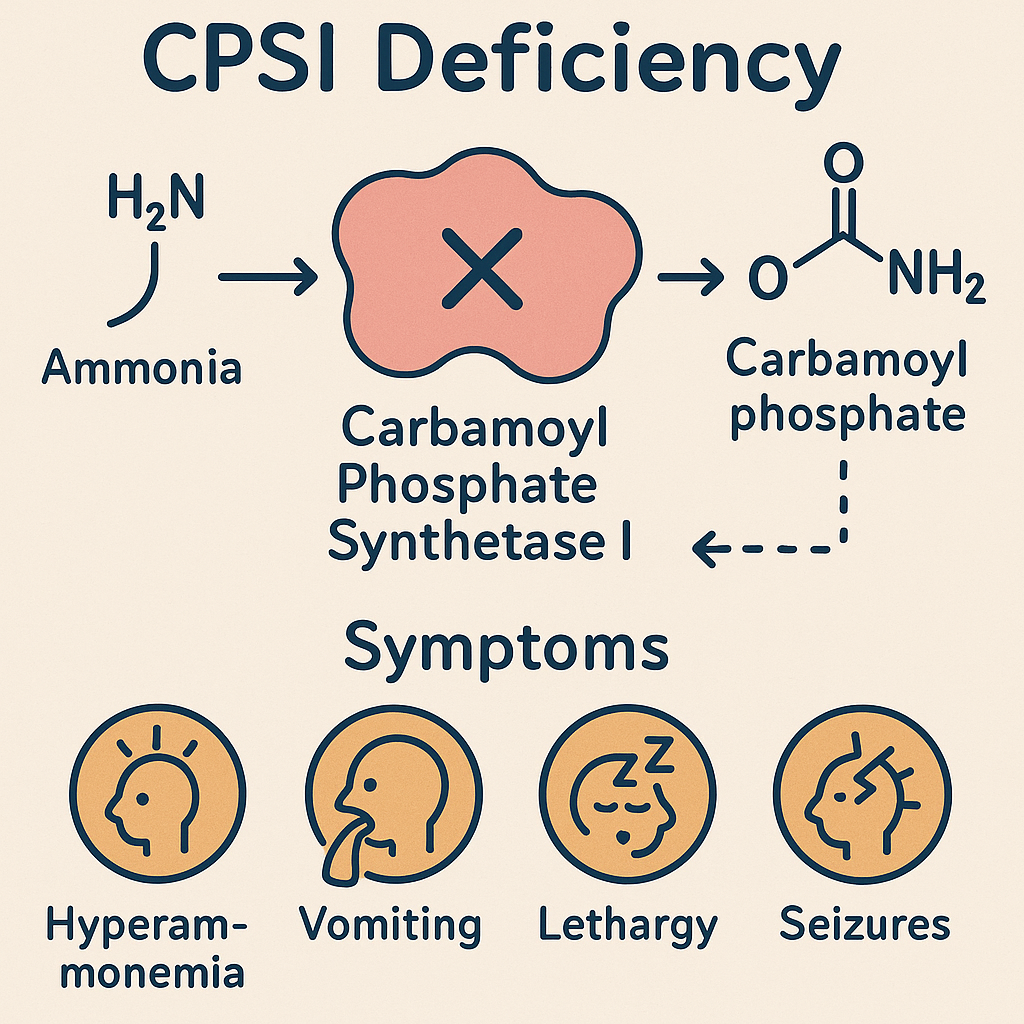
Disorders of Urea Cycle Metabolism
Disorders of Tryptophan Metabolism
Disorders of Histidine Metabolism
Disorders of Glycine and Serine Metabolism
Disorders of Proline and Hydroxyproline Metabolism
II. Major Inborn Errors of Amino Acid Metabolism
1. Disorders of Phenylalanine and Tyrosine Metabolism
Precursor for tyrosine, dopamine, norepinephrine, epinephrine
Phenylketonuria (PKU), Alkaptonuria
Tyrosine
Precursor for catecholamines, thyroid hormones, melanin
Tyrosinemia, Albinism
Tryptophan
Precursor for serotonin, melatonin, niacin
Hartnup Disease, Carcinoid Syndrome
Plasma Proteins:
Plasma proteins are proteins present in blood plasma, essential for maintaining osmotic pressure, immunity, transport, and clotting functions. These proteins are primarily synthesized in the liver and play a vital role in homeostasis.
I. Types of Plasma Proteins
Plasma proteins are classified into three major groups:
Albumin
Globulins
Fibrinogen
Other Plasma Proteins (Complement proteins, Enzymes, Hormones, Transport proteins, etc.)
II. Normal Values of Plasma Proteins
Plasma Protein
Normal Value (g/dL)
Percentage (%)
Total Plasma Proteins
6.0 – 8.0 g/dL
100%
Albumin
3.5 – 5.0 g/dL
55 – 60%
Globulins (α, β, γ)
2.0 – 3.5 g/dL
35 – 40%
Fibrinogen
200 – 400 mg/dL
4 – 6%
III. Detailed Classification and Functions of Plasma Proteins
Transport Proteins (Albumin, Transferrin, Haptoglobin, Ceruloplasmin, Thyroid-binding globulin)
Transport of metals, hormones, and nutrients
IV. Functions of Plasma Proteins
Function
Plasma Protein Involved
Maintaining Osmotic Pressure
Albumin
Transport of Substances
Albumin, Transferrin, Haptoglobin
Blood Clotting
Fibrinogen, Prothrombin
Immunity
Immunoglobulins, Complement proteins
Inflammatory Response
CRP, α1-Antitrypsin
Enzyme Regulation
α2-Macroglobulin
Lipid Transport
Lipoproteins (HDL, LDL)
V. Clinical Significance of Plasma Proteins
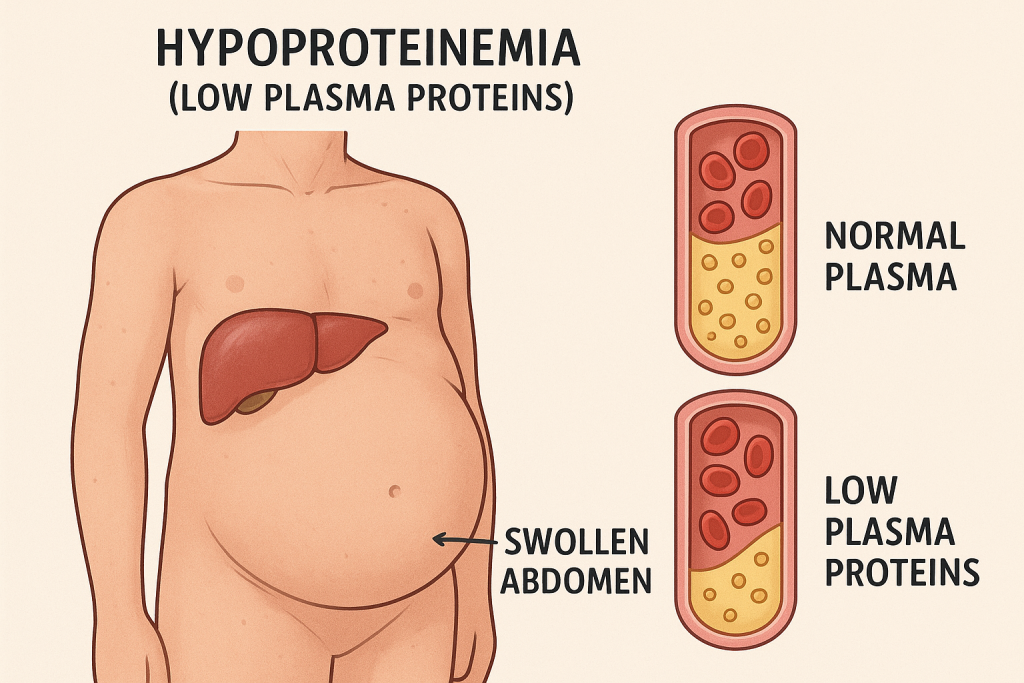
1. Hypoproteinemia (Low Plasma Proteins)
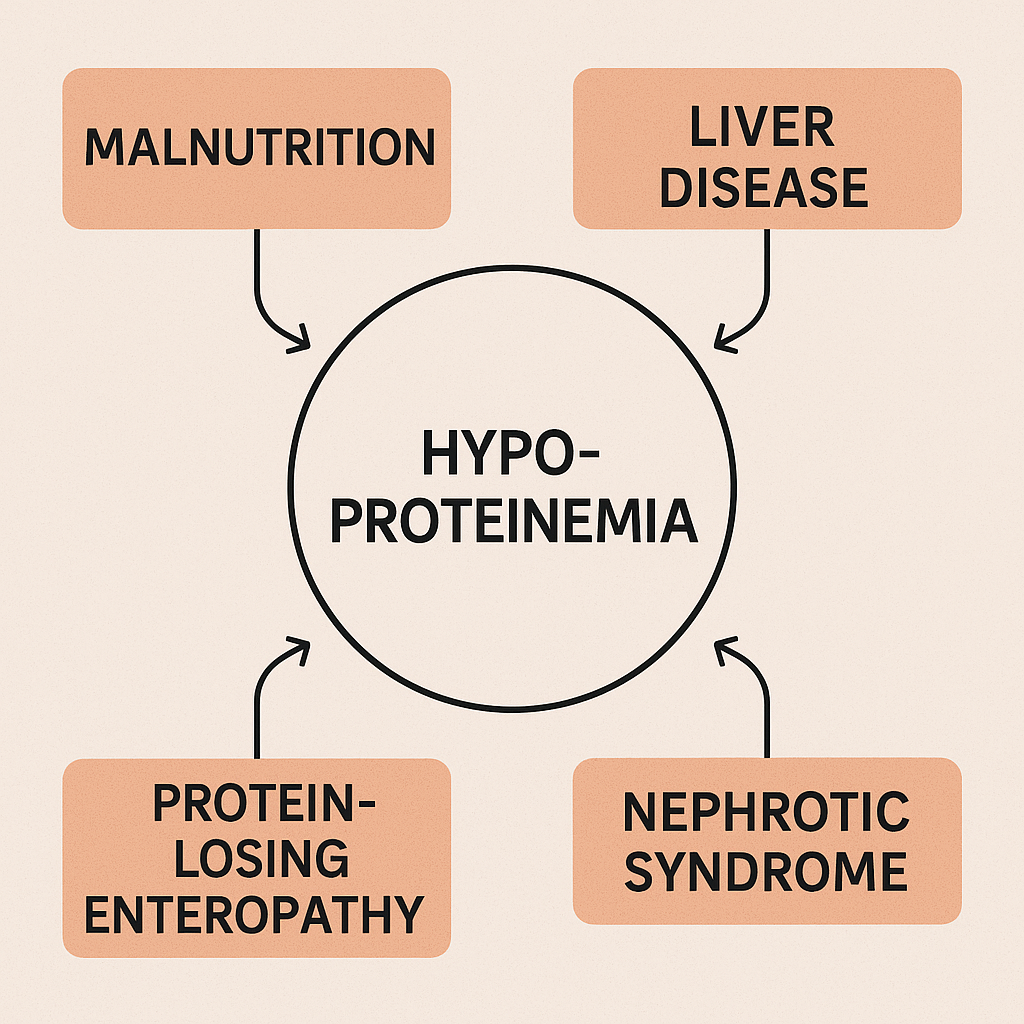
Causes:
Liver disease (reduced synthesis)
Kidney disease (protein loss in urine)
Malnutrition (low protein intake)
Severe burns or hemorrhage
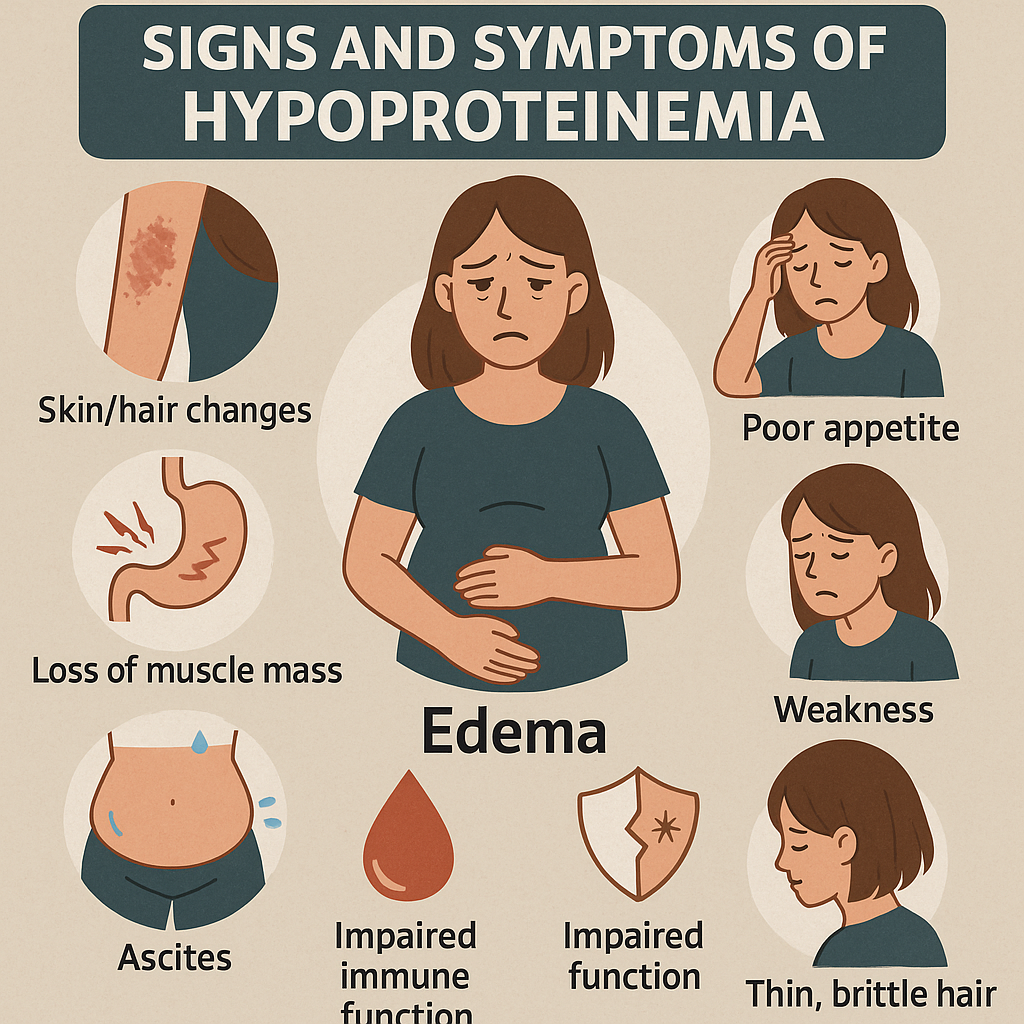
Effects:
Edema (low albumin → low oncotic pressure)
Immune deficiency (low globulins)
Poor clotting (low fibrinogen)
2. Hyperproteinemia (High Plasma Proteins)
Causes:
Dehydration (increased concentration)
Chronic infections (increased globulins)
Multiple myeloma (excess Ig production)
Effects:
Increased blood viscosity
Kidney damage due to excess IgG (Bence-Jones proteins)
3. Specific Disorders of Plasma Proteins
Disorder
Affected Protein
Clinical Findings
Liver Cirrhosis
↓ Albumin, ↓ Clotting Factors
Ascites, bleeding tendency
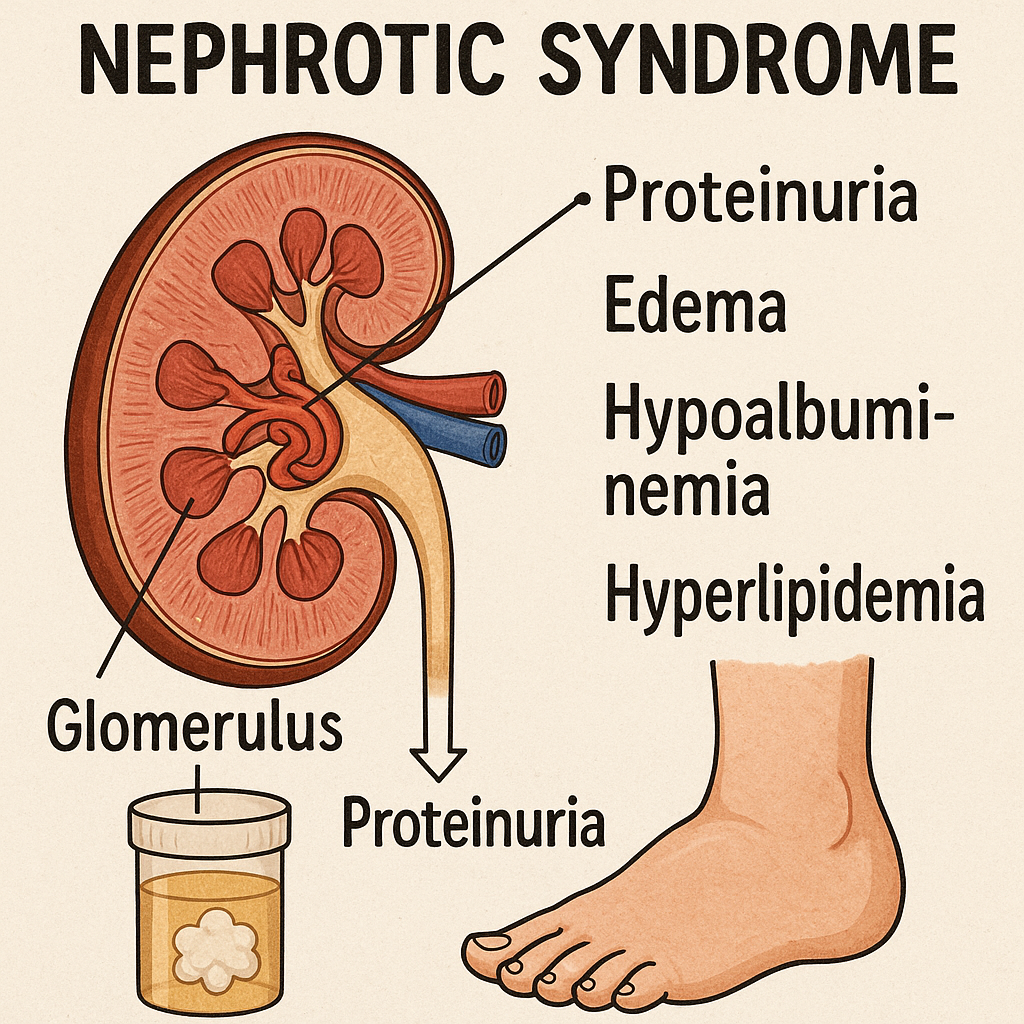
Nephrotic Syndrome
↓ Albumin, ↑ α2-Globulins
Severe edema, proteinuria
Multiple Myeloma
↑ IgG or IgA
Bone pain, hypercalcemia
Wilson’s Disease
↓ Ceruloplasmin
Copper accumulation, liver failure
Iron Deficiency Anemia
↓ Transferrin saturation
Microcytic anemia
VI. Summary of Plasma Proteins
Type
Major Proteins
Normal Value
Function
Albumin
Albumin
3.5 – 5.0 g/dL
Osmotic balance, transport
Globulins
α1, α2, β, γ Globulins
2.0 – 3.5 g/dL
Immunity, transport, inflammation
Fibrinogen
Fibrinogen
200 – 400 mg/dL
Blood clotting
Functions of Plasma Proteins
Plasma proteins are essential biomolecules present in blood plasma that perform a variety of physiological roles, including maintaining osmotic balance, immune defense, blood clotting, and transport of biomolecules. These proteins are primarily synthesized in the liver except for immunoglobulins, which are produced by B lymphocytes.
I. Major Functions of Plasma Proteins
Plasma proteins can be grouped based on their primary functions:
Maintenance of Osmotic Pressure
Transport Function
Blood Clotting and Hemostasis
Immune Defense
Enzymatic and Regulatory Functions
Inflammatory and Acute Phase Response
Buffering and pH Regulation
Nutritional and Structural Functions
II. Detailed Functions of Plasma Proteins
1. Maintenance of Colloid Osmotic Pressure
Protein Involved:Albumin
Function:
Maintains oncotic (colloid osmotic) pressure, preventing fluid leakage from blood vessels into tissues.
Low albumin levels result in edema (fluid accumulation in tissues), seen in liver disease, nephrotic syndrome, and malnutrition.
Metabolic Acidosis: Excess acid in the blood due to kidney failure.
Respiratory Acidosis: Increased CO₂ retention in chronic lung diseases.
8. Nutritional and Structural Functions
Plasma Protein
Function
Albumin
Acts as a protein reserve for tissue repair
Collagen precursors
Essential for connective tissue strength
Fibrinogen & Fibronectin
Wound healing
Clinical Significance:
Low albumin levels in malnutrition can cause muscle wasting and weakness.
Collagen deficiency in scurvy (Vitamin C deficiency) leads to poor wound healing.
III. Summary Table: Major Functions of Plasma Proteins
Function
Major Plasma Proteins Involved
Colloid Osmotic Pressure
Albumin
Transport Function
Albumin, Transferrin, Haptoglobin, Lipoproteins
Blood Clotting
Fibrinogen, Prothrombin, Clotting Factors
Immune Defense
Immunoglobulins, Complement Proteins, CRP
Enzymatic Regulation
α1-Antitrypsin, Cholinesterase, Angiotensinogen
Inflammatory Response
CRP, Haptoglobin, Fibrinogen
pH Buffering
Albumin, Hemoglobin
Nutritional Function
Albumin, Collagen Precursors
IV. Clinical Importance of Plasma Proteins
Disorder
Affected Plasma Protein
Clinical Effects
Liver Cirrhosis
↓ Albumin, ↓ Clotting Factors
Edema, bleeding tendency
Nephrotic Syndrome
↓ Albumin, ↑ α2-Globulins
Severe edema, proteinuria
Multiple Myeloma
↑ Immunoglobulins (IgG, IgA)
Bone pain, hypercalcemia
Wilson’s Disease
↓ Ceruloplasmin
Copper accumulation, liver failure
Iron Deficiency Anemia
↓ Transferrin saturation
Microcytic anemia
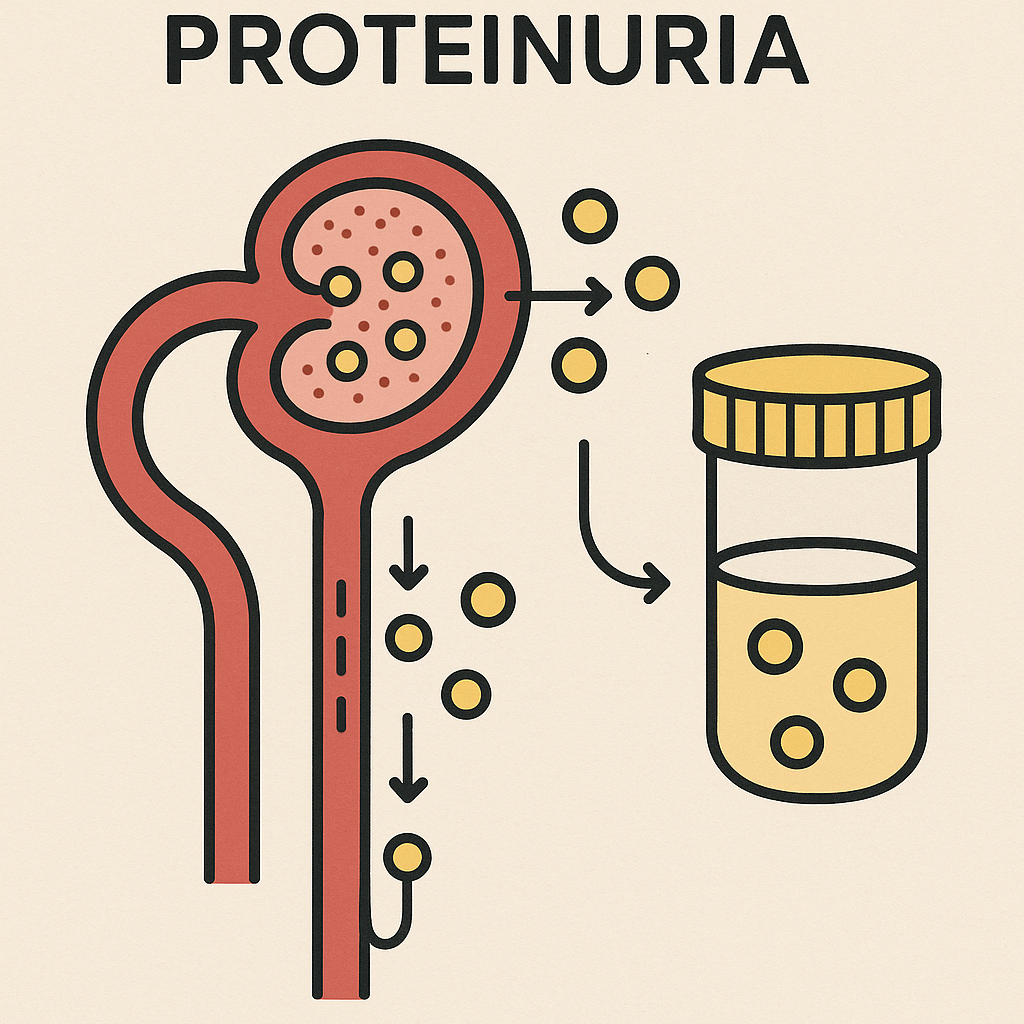
Proteinuria:
I. Introduction
Proteinuria is the presence of excess protein in the urine, indicating kidney dysfunction or damage to the glomerular filtration barrier. Under normal conditions, only small amounts of protein (<150 mg/day) are excreted in the urine. When the filtration system is compromised, larger proteins such as albumin, immunoglobulins, and fibrinogen pass into the urine, leading to proteinuria.
II. Normal Urinary Protein Excretion
Total protein in urine: <150 mg/day
Albumin excretion: <30 mg/day
Nephrotic range proteinuria: >3.5 g/day (Severe loss of protein)
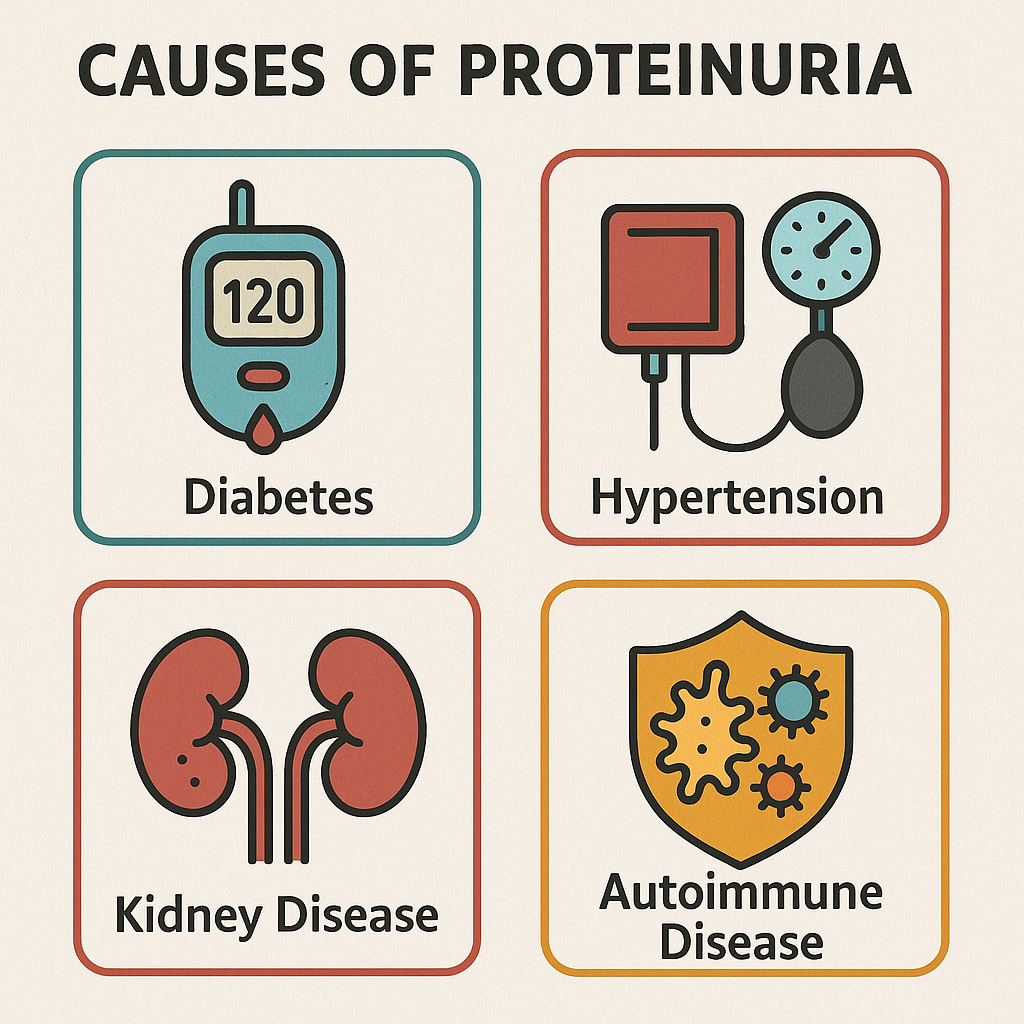
III. Causes of Proteinuria
Proteinuria can be classified based on its cause:
1. Physiological (Benign) Proteinuria
Occurs temporarily without underlying kidney disease.
Causes:
Strenuous exercise
Fever or stress
Dehydration
Cold exposure
Pregnancy-related proteinuria (Mild protein loss in urine)
2. Pathological Proteinuria
Occurs due to kidney disease or systemic disorders affecting the glomerulus or tubules.
A. Glomerular Proteinuria (Most Common)
Damage to the glomerular filtration barrier leads to leakage of large proteins.
Causes:
Glomerulonephritis (Inflammation of the kidney glomeruli)
Diabetic nephropathy (Protein leakage due to high blood sugar)
Hypertension (Hypertensive nephropathy)
Nephrotic Syndrome (Heavy protein loss, edema, hyperlipidemia)
ACE inhibitors, steroids, diuretics, antibiotics, dialysis if severe
Nursing Management
Monitor urine output, control BP, diet management, patient education
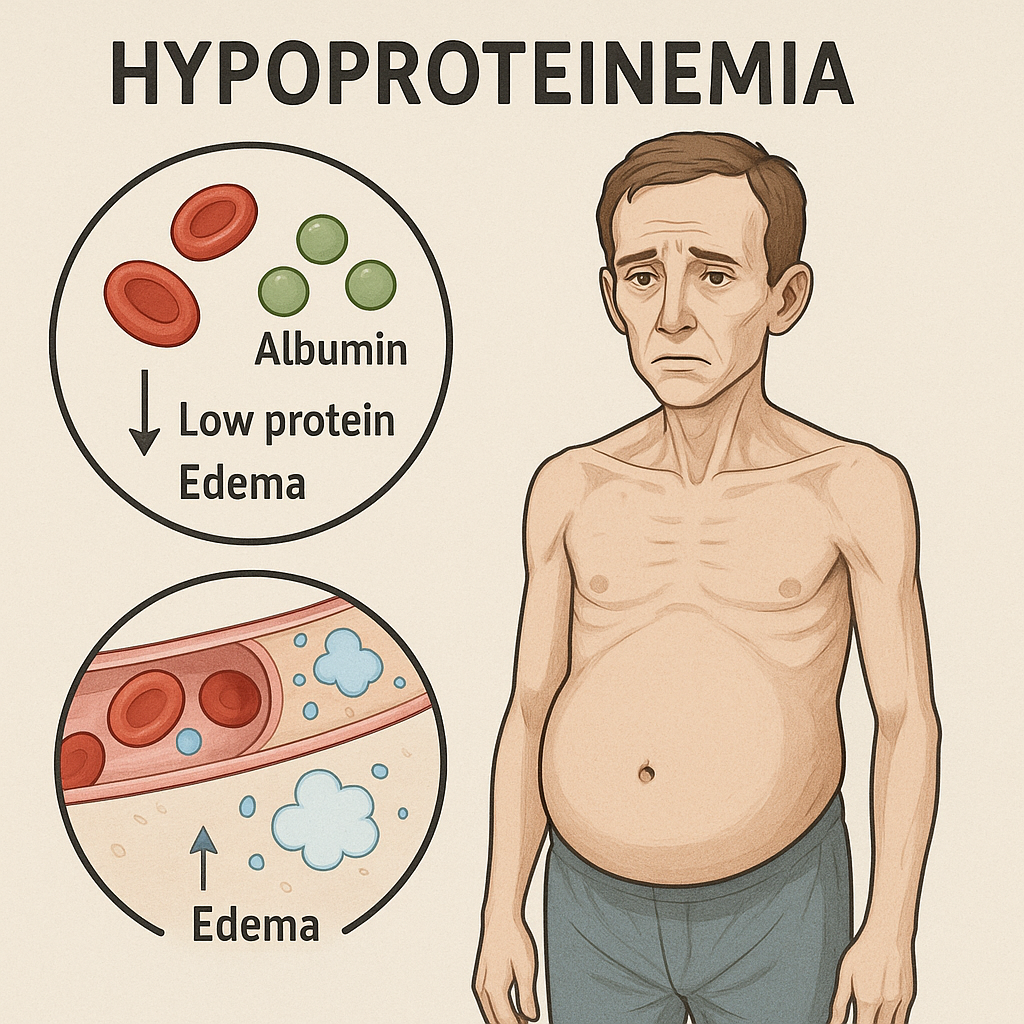
Hypoproteinemia:
I. Introduction
Hypoproteinemia is a condition characterized by low levels of total protein in the blood, specifically albumin and globulins. Plasma proteins play a critical role in osmotic balance, immunity, transport, and clotting. A decrease in these proteins can lead to edema, impaired immune function, and metabolic disturbances.
Normal Plasma Protein Levels
Plasma Protein
Normal Range
Total Protein
6.0 – 8.0 g/dL
Albumin
3.5 – 5.0 g/dL
Globulins
2.0 – 3.5 g/dL
Fibrinogen
200 – 400 mg/dL
Hypoproteinemia is diagnosed when total protein falls below 6.0 g/dL.
Severe hypoproteinemia occurs when albumin is <2.5 g/dL, leading to edema and severe complications.
II. Causes of Hypoproteinemia
Hypoproteinemia can result from decreased protein synthesis, increased protein loss, or increased protein breakdown.
1. Decreased Protein Synthesis
Occurs when the liver fails to produce adequate proteins.
Serum protein tests, urine tests, liver/kidney function tests
Medical Management
Treat underlying disease, albumin infusions, diuretics, steroids
Nursing Management
Monitor edema, maintain high-protein diet, educate on prevention
Hypergammaglobulinemia:
I. Introduction
Hypergammaglobulinemia is a condition characterized by increased levels of gamma globulins (immunoglobulins/antibodies) in the blood. Gamma globulins, mainly composed of immunoglobulins (IgG, IgA, IgM, IgE, IgD), play a crucial role in immune defense. Elevated levels of these proteins suggest chronic infections, autoimmune diseases, or hematologic malignancies.
Normal Serum Gamma Globulin Levels
Immunoglobulin (Ig)
Normal Range (mg/dL)
IgG
700 – 1600 mg/dL
IgA
70 – 400 mg/dL
IgM
50 – 300 mg/dL
IgE
<100 IU/mL
IgD
<10 mg/dL
Hypergammaglobulinemia is defined as gamma globulin levels exceeding the normal range, with IgG > 1600 mg/dL.
Monoclonal vs. Polyclonal Hypergammaglobulinemia:
Monoclonal: Overproduction of a single type of immunoglobulin (e.g., multiple myeloma).
Monitor for infections, prevent complications, patient education
Principle of Electrophoresis: Definition, Mechanism, Types, and Applications
I. Introduction
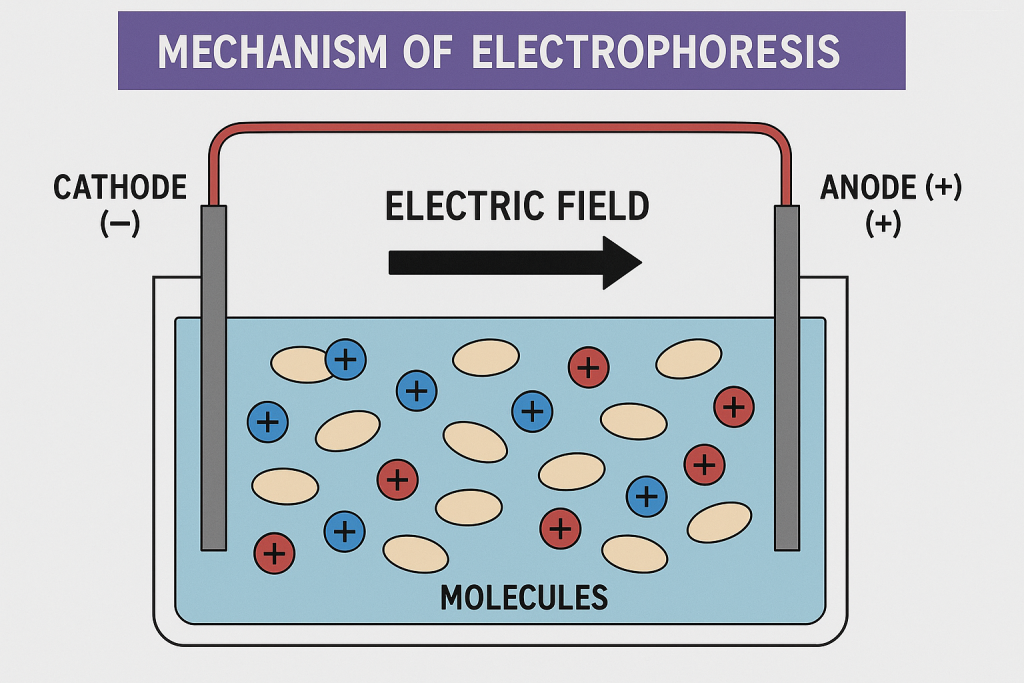
Electrophoresis is a laboratory technique used to separate charged molecules (proteins, DNA, RNA) in an electric field based on their size, charge, and mobility. It is widely used in clinical diagnostics, molecular biology, genetics, and protein analysis.
II. Principle of Electrophoresis
Electrophoresis is based on the movement of charged particles (anions and cations) through a medium (gel or liquid) under the influence of an electric field.
Positively charged molecules (cations) move toward the negative electrode (cathode).
Negatively charged molecules (anions) move toward the positive electrode (anode).
Larger molecules move slower, while smaller molecules move faster.
Key Factors Influencing Electrophoretic Mobility
Factor
Effect on Electrophoresis
Charge of the molecule
Higher charge → Faster movement
Size of the molecule
Larger molecules → Move slower
Shape of the molecule
Spherical molecules move faster than elongated molecules
Electric field strength
Higher voltage → Faster migration
Type of buffer and pH
Affects charge and migration speed
Gel matrix or medium
Determines separation resolution (Agarose vs. Polyacrylamide)
III. Types of Electrophoresis
Electrophoresis is classified based on the medium used, separation principle, and application.
1. Based on Medium Used
Type
Description
Application
Agarose Gel Electrophoresis
Uses agarose gel, suitable for DNA and RNA
DNA fingerprinting, PCR product analysis
Polyacrylamide Gel Electrophoresis (PAGE)
Uses polyacrylamide gel, high-resolution
Protein separation, SDS-PAGE for protein analysis
Capillary Electrophoresis
Uses narrow capillaries with high-voltage
Drug analysis, small molecule separation
2. Based on Separation Principle
Type
Principle
Application
Zone Electrophoresis
Molecules separate into distinct bands/zones
Serum protein electrophoresis (SPEP)
Isoelectric Focusing (IEF)
Separation based on isoelectric point (pI)
Protein and enzyme characterization
Two-Dimensional Electrophoresis (2D-PAGE)
Combines IEF and SDS-PAGE for better resolution
Proteomics and protein identification
3. Based on Application
Type
Purpose
Example
Serum Protein Electrophoresis (SPEP)
Detects abnormal proteins
Multiple Myeloma diagnosis
Hemoglobin Electrophoresis
Identifies hemoglobin variants
Sickle Cell Disease detection
Western Blotting
Identifies specific proteins using antibodies
HIV, COVID-19 detection
Southern & Northern Blotting
DNA (Southern) and RNA (Northern) analysis
Genetic mutation studies
IV. Mechanism of Electrophoresis
Sample Preparation
DNA, RNA, or protein is mixed with a loading dye to visualize movement.
Loading the Sample
The sample is placed in wells of the gel.
Application of Electric Field
Electric current is applied, and charged molecules migrate.
Separation of Molecules
Molecules separate based on size and charge.
Staining & Visualization
Ethidium Bromide (for DNA/RNA) or Coomassie Blue (for proteins) is used to stain the gel.
Analysis of Results
The band pattern is analyzed to interpret molecular weight or charge.
V. Applications of Electrophoresis
Electrophoresis is widely used in medicine, research, forensics, and biotechnology.
Confirms HIV infection, protein analysis in diseases
DNA Electrophoresis
Identifies genetic mutations and disorders
2. Research Applications
DNA sequencing
Protein-protein interaction studies
Gene expression analysis
3. Forensic Applications
DNA fingerprinting (Crime scene investigations, paternity testing)
Blood protein analysis in forensic toxicology
VI. Advantages & Limitations of Electrophoresis
Advantages
✅ Highly accurate and reliable ✅ Separates complex mixtures ✅ Used for diagnostic and genetic studies ✅ Rapid and cost-effective
Limitations
❌ Time-consuming for large samples ❌ Requires specialized equipment and staining ❌ Cannot be used for non-charged molecules ❌ Some techniques require hazardous chemicals (e.g., Ethidium Bromide in DNA analysis)
VII. Summary of Electrophoresis
Aspect
Details
Principle
Separation of molecules based on charge and size under an electric field
Types
Agarose gel electrophoresis, PAGE, Capillary electrophoresis
Mechanism
Sample loading → Electric field application → Separation → Staining → Analysis
Applications
Medical diagnostics, forensic DNA analysis, molecular biology research
Normal & Abnormal Electrophoretic Patterns: Interpretation & Clinical Significance
I. Introduction
Electrophoresis is a laboratory technique used to separate plasma proteins, hemoglobin, DNA, or RNA based on their charge and size in an electric field.
Normal electrophoretic patterns show expected distribution and proportions of proteins or hemoglobin.
Abnormal electrophoretic patterns indicate disease conditions such as multiple myeloma, nephrotic syndrome, autoimmune diseases, or hemoglobinopathies.
Common Types of Electrophoresis Used in Medical Diagnostics
Type of Electrophoresis
Used For
Serum Protein Electrophoresis (SPEP)
Evaluating plasma proteins
Urine Protein Electrophoresis (UPEP)
Detecting protein loss in urine
Hemoglobin Electrophoresis
Identifying hemoglobin variants
Lipoprotein Electrophoresis
Analyzing lipoprotein disorders
Immunoelectrophoresis
Detecting abnormal immunoglobulin production
II. Normal Electrophoretic Patterns
A normal electrophoretic pattern consists of five major protein fractions:
1. Normal Serum Protein Electrophoresis (SPEP) Pattern
Albumin (55-60% of total proteins)
Alpha-1 globulins (α1) (2-5%)
Alpha-2 globulins (α2) (6-10%)
Beta globulins (β) (8-15%)
Gamma globulins (γ) (10-20%)
Graph Representation of Normal Serum Electrophoresis
The albumin band appears as the largest peak, followed by smaller peaks for globulin fractions.
Protein Fraction
Function
Normal Serum Levels
Albumin
Maintains osmotic pressure, transports substances
3.5 – 5.0 g/dL
α1-globulins
Transport proteins, protease inhibitors
0.2 – 0.4 g/dL
α2-globulins
Haptoglobin, ceruloplasmin
0.5 – 1.0 g/dL
β-globulins
Transferrin, complement proteins
0.7 – 1.2 g/dL
γ-globulins
Immunoglobulins (IgG, IgA, IgM)
0.6 – 1.5 g/dL
III. Abnormal Electrophoretic Patterns
Abnormal electrophoretic patterns indicate protein imbalances due to disease conditions.
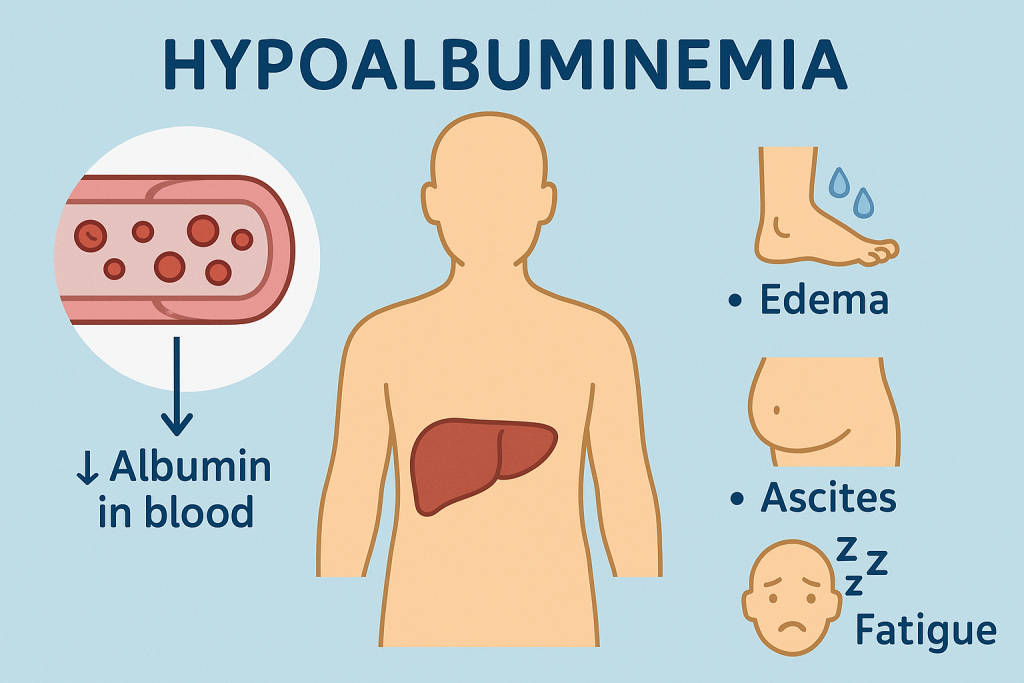
1. Hypoalbuminemia (Low Albumin)
Electrophoresis Pattern:Decreased albumin band.
Causes:
Liver disease (Cirrhosis, Hepatitis)
Nephrotic Syndrome (Loss of albumin in urine)
Malnutrition (Protein deficiency)
Chronic inflammation (Protein loss)
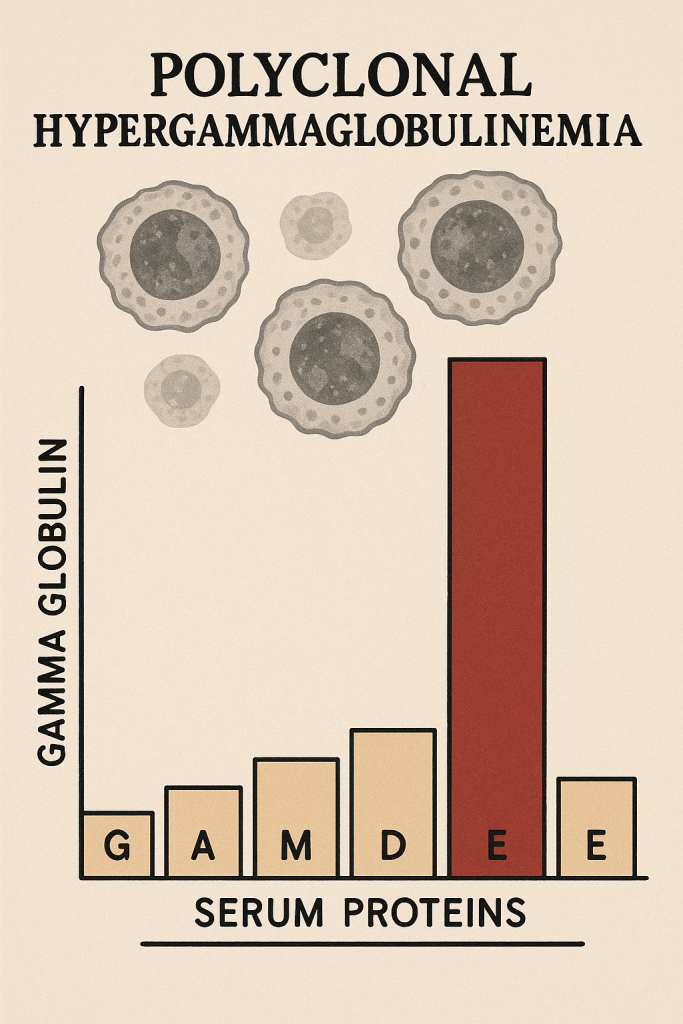
2. Polyclonal Hypergammaglobulinemia
Electrophoresis Pattern:Broad, diffuse increase in gamma-globulin band.
Causes:
Chronic infections (HIV, Tuberculosis, Hepatitis)
Autoimmune diseases (SLE, Rheumatoid Arthritis)
Liver disease (Chronic hepatitis, Cirrhosis)
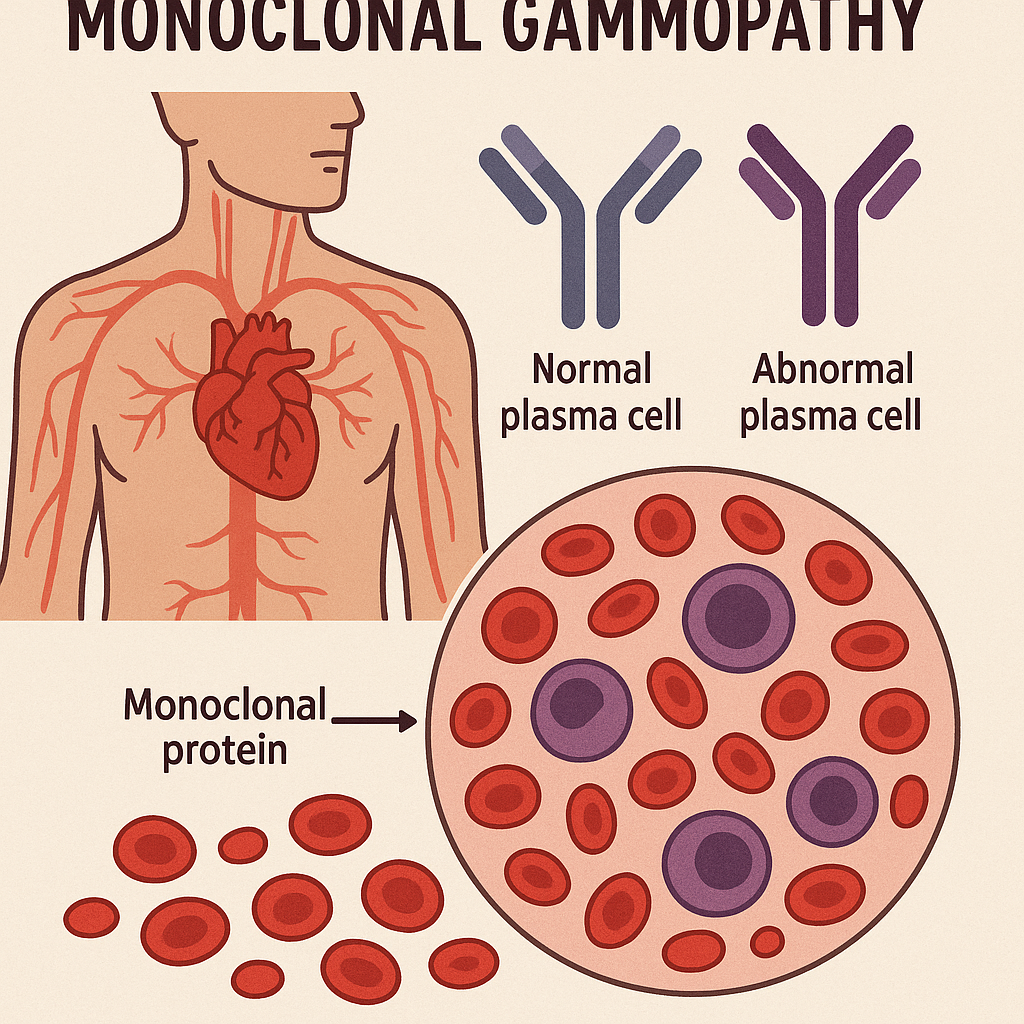
3. Monoclonal Gammopathy (M-spike)
Electrophoresis Pattern:Sharp, narrow peak in gamma region (M-spike).
Causes:
Multiple Myeloma (Excess monoclonal IgG or IgA)
Waldenström’s Macroglobulinemia (Excess IgM)
MGUS (Monoclonal Gammopathy of Undetermined Significance) (Pre-cancerous stage)
Distinguishing Features:
Multiple Myeloma: High M-spike, increased plasma cells in bone marrow.
Waldenström’s Macroglobulinemia: High IgM levels, hyperviscosity symptoms.
4. Nephrotic Syndrome
Electrophoresis Pattern:
Low albumin band
Increased α2-globulin band (due to haptoglobin, ceruloplasmin)
Causes:
Glomerular kidney disease (Protein loss via urine)
Minimal Change Disease (MCD)
Diabetic Nephropathy
5. Acute Inflammatory Response
Electrophoresis Pattern:
Increased α1 and α2-globulin bands (Acute phase proteins)