BSC SEM 4 UNIT 3 ADULT HEALTH NURSING 2
UNIT 3 Nursing management of patient with Kidney and Urinary problems
🔍 Anatomy & Physiology of the Genitourinary System
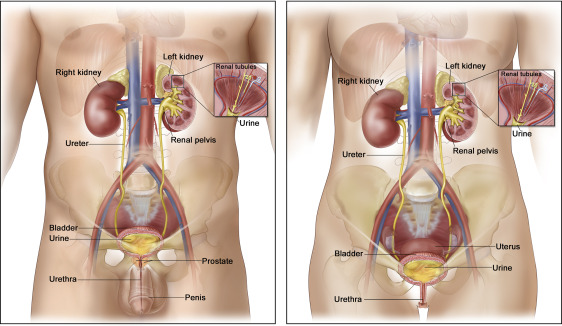
🧠 Main Components: The Genitourinary system = Urinary system + Reproductive system
🚽 I. Urinary System Anatomy & Physiology
🧩 Major Organs
- 👂 Kidneys (2)
- 🧪 Ureters (2)
- 🚰 Urinary Bladder (1)
- 🚿 Urethra (1)
🧠 Functions of the Urinary System
🔹 Removes metabolic waste products (urea, creatinine)
🔹 Maintains fluid & electrolyte balance
🔹 Regulates acid-base balance (pH)
🔹 Secretes hormones:
- Erythropoietin – stimulates RBC production
- Renin – controls blood pressure
- Calcitriol – active form of vitamin D for calcium absorption
🧬 Organ-Wise Structure & Function
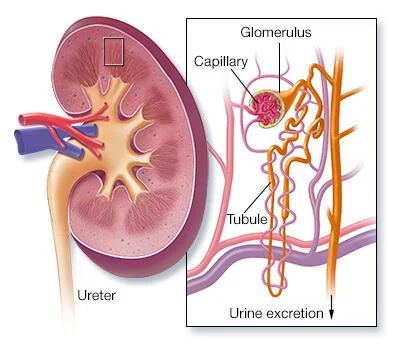
🔹 1. Kidneys (👂)
- Bean-shaped organs located retroperitoneally.
- Contains nephrons – the functional units.
- Each nephron includes:
- Glomerulus: filtration of blood
- Bowman’s capsule: collects filtrate
- Tubules (PCT, Loop of Henle, DCT): reabsorption and secretion
- Function:
✅ Filtration
✅ Reabsorption
✅ Secretion
✅ Urine formation
🔹 2. Ureters (🧪)
- Muscular tubes (~25-30 cm long)
- Connect kidneys to bladder
- Peristalsis pushes urine downward
🔹 3. Urinary Bladder (🚰)
- Hollow, muscular organ
- Lined by transitional epithelium
- Stores urine (capacity ~400–600 mL)
- Detrusor muscle contracts during urination
🔹 4. Urethra (🚿)
- Transports urine out of the body
- Female urethra: ~4 cm
- Male urethra: ~20 cm (also part of reproductive tract)
🍒 II. Reproductive System Anatomy & Physiology
🚺 A. Female Reproductive System
🧩 Organs
- Ovaries (🥚)
- Fallopian Tubes (🌀)
- Uterus (🏰)
- Vagina (🕳️)
- External genitalia (🌸)
- Mammary glands (🍼)
🧠 Functions
🔹 Production of ova (eggs)
🔹 Secretion of hormones (estrogen, progesterone)
🔹 Menstruation, Fertilization, Pregnancy, Lactation
🔹 1. Ovaries (🥚)
- Almond-shaped glands
- Produce ova and hormones
- Hormones: Estrogen, Progesterone
🔹 2. Fallopian Tubes (🌀)
- Site of fertilization
- Lined with cilia to move egg
- Connect ovaries to uterus
🔹 3. Uterus (🏰)
- Pear-shaped muscular organ
- Layers: Endometrium, Myometrium, Perimetrium
- Site of implantation and fetal growth
🔹 4. Vagina (🕳️)
- Muscular canal
- Functions: intercourse, birth canal, and menstrual flow exit
🔹 5. Mammary Glands (🍼)
- Modified sweat glands
- Produce milk for infant feeding under prolactin and oxytocin
🚹 B. Male Reproductive System
🧩 Organs
- Testes (⚽)
- Epididymis (🐛)
- Vas deferens (🧵)
- Seminal vesicles, Prostate (🧴)
- Penis (🍆)
- Urethra (🚿) – Shared with urinary system
🧠 Functions
🔹 Production of sperm
🔹 Secretion of testosterone
🔹 Fertilization via ejaculation
🔹 1. Testes (⚽)
- Located in scrotum
- Produce sperm and testosterone
- Contain seminiferous tubules
🔹 2. Epididymis (🐛)
- Site of sperm maturation and storage
🔹 3. Vas Deferens (🧵)
- Transports sperm from epididymis to ejaculatory duct
🔹 4. Seminal Vesicles & Prostate (🧴)
- Secrete seminal fluid for sperm motility and nourishment
🔹 5. Penis (🍆)
- Erectile organ
- Conducts urine and semen via urethra
🔄 Interconnection of Urinary & Reproductive Systems
| Feature | Male | Female |
|---|---|---|
| Shared Urethra | ✅ (urine & semen) | ❌ (urine only) |
| Reproductive Glands | Seminal vesicles, Prostate | Ovaries |
| Urinary Bladder | Same in both | Same in both |
⚙️ Physiological Control Mechanisms
- 💧 Urinary Regulation:
- ADH (vasopressin) – water reabsorption
- Aldosterone – Na⁺ reabsorption
- 🍳 Reproductive Hormone Axis:
- Hypothalamus (GnRH) → Pituitary (FSH, LH) → Gonads (sex hormones)
✅ Key Takeaways
🔹 The urinary system maintains internal homeostasis
🔹 The reproductive system ensures species continuation
🔹 Hormonal control is central to both systems
🔹 Sex differences exist in anatomy and hormonal function
🧾 HISTORY-RELATED MANAGEMENT OF PATIENT WITH KIDNEY AND URINARY PROBLEMS
🩺 I. Importance of History-Taking in Renal & Urinary Disorders
History-taking is the foundation of clinical assessment in nephrology and urology. It helps to:
✅ Identify underlying causes of renal/urinary issues
✅ Recognize progression or chronicity of disease
✅ Guide focused examination, investigations & treatment
✅ Detect risk factors and comorbid conditions
📋 II. Key Components of History-Taking
🔹 A. Chief Complaints (presenting symptoms)
Ask specifically about:
- 🔸 Dysuria (painful urination)
- 🔸 Frequency or urgency
- 🔸 Oliguria / Anuria (low or no urine output)
- 🔸 Hematuria (blood in urine)
- 🔸 Nocturia (night-time urination)
- 🔸 Incontinence
- 🔸 Lower abdominal or flank pain
- 🔸 Swelling / Edema
- 🔸 Fever / Chills (in UTI or pyelonephritis)
🔹 B. History of Present Illness (HPI)
- 📆 Onset, duration, and pattern of symptoms
- 🕒 Aggravating/relieving factors (e.g., position, fluids)
- 📈 Progression of symptoms
- 💊 Any self-treatment or medications taken?
🔹 C. Past Medical History
- 🔍 Any previous kidney disorders:
- UTI, Nephritis, Kidney stones, Glomerulonephritis, CKD, Dialysis
- 🫀 Coexisting conditions:
- Diabetes Mellitus
- Hypertension
- Autoimmune diseases
- Recurrent infections
🔹 D. Surgical History
- Past surgeries involving:
- Kidneys (nephrectomy)
- Bladder or prostate (e.g., TURP)
- Catheterization history
🔹 E. Medication History
- Use of nephrotoxic drugs (NSAIDs, aminoglycosides, contrast media)
- Diuretics, antihypertensives, antibiotics
🔹 F. Family History
- Genetic kidney conditions:
- Polycystic kidney disease
- Alport syndrome
- Renal stones
🔹 G. Dietary and Fluid History
- 💧 Daily fluid intake
- 🧂 High salt/protein consumption?
- 🍹 Alcohol/caffeine intake?
- 🚰 Type of drinking water (hard/contaminated)?
🔹 H. Psychosocial & Lifestyle Factors
- 🚬 Smoking
- 🏋️♂️ Occupation (chemical exposure, dehydration)
- 🌡️ Recent travel (for endemic infections)
🧠 III. Clinical Management Based on History
🧪 1. Investigations Ordered Based on History
- 🔬 Urinalysis (for protein, blood, WBCs, bacteria)
- 💉 Blood urea, serum creatinine, eGFR
- 🧬 Urine culture
- 🔍 Ultrasound / CT scan of kidneys or bladder
- 🧪 Electrolytes, ABG (acid-base balance)
- 🧬 Creatinine clearance or 24-hr urine collection
🩹 2. Medical Management Plan
Tailored to diagnosis suggested by history:
| Condition | Management Based on History |
|---|---|
| UTI | Antibiotics, fluids, hygiene education |
| Nephrolithiasis | Pain relief, hydration, possible lithotripsy |
| Glomerulonephritis | Steroids, BP control, protein restriction |
| CKD | Diet modification, dialysis prep, erythropoietin |
| Acute Renal Failure | Treat cause, fluid balance, renal replacement therapy |
👩⚕️ IV. Nursing Management Guided by History
✅ Assessment
- Monitor urine output (I/O charting)
- Check for edema, BP, weight, electrolyte changes
- Daily weight for fluid retention
💉 Nursing Interventions
- Educate on fluid intake/output
- Ensure proper catheter care (if history of retention or surgery)
- Promote comfort during painful urination
- Dietary advice (low sodium, protein if needed)
- Monitor drug side effects (nephrotoxicity)
🍽️ V. Nutritional Advice Based on History
| If History Indicates… | Suggested Nutritional Approach |
|---|---|
| Proteinuria | Moderate protein intake |
| Hyperkalemia | Avoid potassium-rich foods |
| Fluid overload | Restrict fluid intake |
| Recurrent stones | Avoid oxalate, high protein, increase fluids |
| CKD/ESRD | Low sodium, phosphorus, protein, potassium |
🚨 VI. Red Flag History Findings That Need Immediate Attention
- 🚫 Anuria (<100 mL/day)
- 🩸 Visible hematuria
- 💣 Sudden hypertension with no cause
- 😰 Severe flank pain + fever
- ⚠️ Confusion + uremic symptoms (CKD)
🧷 VII. Documentation Tips
- Record history clearly & systematically
- Include all medications, allergies, and past episodes
- Ensure follow-up and education notes are updated
📌 KEY POINTS
🔹 Comprehensive history = cornerstone of renal care
🔹 Guides investigations, treatment, and nursing planning
🔹 Red flag symptoms = require urgent action
🔹 Nutritional and lifestyle history influences long-term outcomes
🩺 PHYSICAL ASSESSMENT & RELATED MANAGEMENT
🔍 For Patients with Kidney & Urinary Problems
🧠 I. Purpose of Physical Assessment
✅ Identify signs of renal/urinary dysfunction
✅ Correlate findings with history
✅ Detect complications (e.g., edema, hypertension)
✅ Plan targeted nursing care and medical interventions
👀 II. General Observation (Initial Inspection)
🔹 Look for:
- 🏥 Pallor (anemia due to chronic kidney disease)
- 🧊 Edema (periorbital, pedal)
- 💦 Signs of dehydration or fluid overload
- 😰 Restlessness (uremia, infection)
- 🍞 Uremic frost (rare but indicative of severe CKD)
- 🧴 Skin dryness, itching (due to toxin retention)
- 📉 Weight loss (chronic illness)
💪 III. Vital Signs Assessment
| Vital Sign | Significance in Renal/Urological Disease |
|---|---|
| 🌡️ Temperature | Raised in infections (UTI, pyelonephritis) |
| 🩸 Blood Pressure | Elevated in CKD or glomerulonephritis |
| ❤️ Heart Rate | Tachycardia in hypovolemia or sepsis |
| 🫁 Respiratory Rate | Increased in acidosis or pulmonary edema |
🤲 IV. Focused Physical Assessment – Head to Toe
🔹 A. Skin and Mucosa
- Dryness, itching, pallor (anemia)
- Signs of fluid imbalance
- Uremic frost (advanced CKD)
🔹 B. Eyes
- Periorbital edema = nephrotic syndrome
- Pale conjunctiva = anemia
🔹 C. Neck
- Jugular venous distension (JVD) in fluid overload
- Enlarged lymph nodes in infection
🔹 D. Abdomen
- 🔍 Inspection: distension, visible masses
- 🖐️ Palpation: tenderness over kidney region (CVA tenderness → pyelonephritis)
- 🪗 Percussion: bladder distension (full bladder = dullness in suprapubic area)
- 🎧 Auscultation: renal artery bruit (renal artery stenosis)
🔹 E. Flank Region
- Perform costovertebral angle (CVA) tenderness test
📌 Positive in pyelonephritis or renal stone
🔹 F. Lower Limbs
- 🧦 Check for:
- Pedal edema (protein loss or fluid retention)
- Capillary refill and pulses (vascular perfusion)
🔹 G. Urinary System Specific Assessment
- Bladder palpation: check for retention
- Urine characteristics:
- Color (blood, tea-colored, cloudy)
- Odor
- Amount (oliguria, anuria)
- Stream (weak, interrupted)
📝 V. Related Nursing & Clinical Management Based on Assessment
🔹 1. Edema Noted
- 💉 Monitor daily weight and intake/output (I/O)
- 🍽️ Implement low-sodium diet
- 💊 Administer diuretics as prescribed
- 🛏️ Elevate legs to reduce swelling
🔹 2. High BP or Fluid Overload
- 🩸 Monitor BP every 4 hrs
- 🚰 Fluid restriction
- 🧂 Sodium restriction
- 💊 Administer antihypertensives
🔹 3. Pain Over Kidney/Flank
- 🧊 Cold compress for mild pain
- 💊 Administer prescribed analgesics
- 🧪 Prepare for imaging (ultrasound, CT)
🔹 4. Bladder Distension / Retention
- 🧪 Perform bladder scan
- 🚽 Encourage timed voiding
- 🧼 Ensure aseptic catheterization if indicated
- 🗓️ Record urinary patterns
🔹 5. Signs of Infection (Fever, CVA tenderness, burning urine)
- 🧪 Send urine culture
- 💉 Administer antibiotics as per culture
- 🚰 Encourage fluid intake (if not contraindicated)
📊 VI. Monitor Parameters
| Parameter | Normal | Kidney/Urinary Disorder |
|---|---|---|
| Urine Output | 1–2 L/day | ↓ in AKI, ↑ in diabetes insipidus |
| Serum Creatinine | 0.6–1.2 mg/dL | ↑ in renal dysfunction |
| BUN | 10–20 mg/dL | ↑ in renal failure |
| BP | 120/80 mmHg | ↑ in CKD or glomerulonephritis |
| Daily Weight | Stable | ↑ in edema/fluid retention |
🧷 VII. Nursing Interventions Summary
🔹 Maintain fluid and electrolyte balance
🔹 Educate about signs of UTI and CKD
🔹 Promote rest and hygiene
🔹 Maintain catheter care (if present)
🔹 Encourage low-sodium/protein diet if indicated
🔹 Monitor labs and report critical changes
📌 Key Points
✔ Physical assessment must always correlate with history and labs
✔ Detect early complications like fluid overload, infection, or renal shutdown
✔ Use findings to direct specific nursing care and collaborative interventions
✔ Document findings accurately and timely
🧪 DIAGNOSTIC TESTS & RELATED MANAGEMENT
📌 For Patients with Kidney and Urinary Problems
🔬 I. Purpose of Diagnostic Testing
✔ Confirm clinical diagnosis
✔ Monitor severity and progression of kidney/urinary disorders
✔ Detect complications (e.g., electrolyte imbalance, infection)
✔ Guide treatment and nursing interventions
✔ Evaluate response to therapy
🧾 II. Common Diagnostic Tests & Interpretation
🔹 A. Urine Tests
| 🧪 Test | 🔍 Purpose | 🔬 Abnormal Findings |
|---|---|---|
| Urinalysis (R/M) | General urine assessment | Proteinuria, hematuria, pyuria, ketones |
| Urine Culture & Sensitivity (C/S) | Identify infecting organism | Positive for bacteria in UTI |
| 24-Hour Urine Collection | Assess creatinine clearance, protein loss | ↑ Protein = Nephrotic syndrome |
| Urine Specific Gravity | Concentration ability of kidneys | Low in renal failure |
🔹 B. Blood Tests
| 🩸 Test | 🔍 Purpose | 🔬 Interpretation |
|---|---|---|
| Serum Creatinine | Kidney function marker | ↑ in renal dysfunction |
| Blood Urea Nitrogen (BUN) | Waste product from protein | ↑ in CKD, dehydration |
| Electrolytes (Na⁺, K⁺, Ca²⁺, P) | Fluid/electrolyte imbalance | ↑ K⁺ in AKI, ↓ Ca²⁺ in CKD |
| GFR (Glomerular Filtration Rate) | Kidney filtration ability | ↓ in chronic kidney disease |
| Complete Blood Count (CBC) | Check for anemia or infection | ↓ Hb in CKD, ↑ WBC in UTI |
| Arterial Blood Gas (ABG) | Acid-base balance | Metabolic acidosis in ESRD |
🔹 C. Imaging Studies
| 🖼️ Test | 🔍 Purpose | 🔬 Findings |
|---|---|---|
| Ultrasound Abdomen/KUB | Kidney size, obstruction, stones | Hydronephrosis, stones, small kidneys |
| CT Scan (KUB) | Detailed kidney/bladder structure | Stones, tumors, obstruction |
| IVP (Intravenous Pyelogram) | Evaluate urinary tract flow | Delayed excretion = obstruction |
| MRI / MR Urography | Tumor detection or soft tissue analysis | Detects structural anomalies |
| X-ray KUB | Detect radio-opaque stones | Visible stones in renal/ureteral area |
🔹 D. Special Tests
| 🧫 Test | 🔍 Use |
|---|---|
| Renal Biopsy | Microscopic diagnosis of nephritis, nephrotic syndrome |
| Cystoscopy | Visualize bladder & urethra; remove small tumors |
| PSA (Prostate-Specific Antigen) | Screen for BPH or prostate cancer in males |
🧠 III. Nursing Role in Diagnostic Test Management
✅ Before Test (Pre-Procedure Care)
- 🔹 Explain the purpose and procedure to patient
- 💧 Maintain hydration (esp. before CT with contrast)
- 🛑 NPO if required (e.g., before IVP or biopsy)
- 🩸 Check for allergy to contrast media (iodine)
- 💊 Hold nephrotoxic drugs (e.g., metformin before CT scan)
✅ During the Test
- 🧤 Maintain aseptic technique (urine collection, catheterization)
- 🧘♂️ Ensure patient is calm and positioned properly
- 🧑⚕️ Assist the doctor or technician as needed
✅ After Test (Post-Procedure Care)
- 💦 Encourage fluids (to flush contrast material)
- 🩹 Monitor for complications (e.g., hematuria post-biopsy)
- 🌡️ Observe for signs of infection or allergic reactions
- 📋 Document findings and report critical values
🩺 IV. Medical Management Based on Test Results
| 🧪 Test Result | 🚑 Related Medical Action |
|---|---|
| ↑ Creatinine & ↓ GFR | Prepare for dialysis, restrict nephrotoxic drugs |
| ↑ WBC in urine | Start antibiotics for UTI |
| ↑ Potassium (hyperkalemia) | Administer kayexalate, restrict K⁺ intake |
| ↓ Hemoglobin (anemia of CKD) | Start erythropoietin, iron supplements |
| Obstruction seen on imaging | Refer for urological intervention/surgery |
| Massive proteinuria | Start steroids, ACE inhibitors |
🧷 V. Nursing Management Based on Test Findings
🌊 1. Fluid & Electrolyte Balance
- Monitor I/O
- Maintain IV fluids if dehydrated
- Educate on fluid restriction if overloaded
🛌 2. Infection Control
- Maintain hygiene
- Monitor temp, WBC
- Administer prescribed antibiotics
📖 3. Patient Education
- Importance of follow-up labs
- Drug compliance (e.g., antihypertensives, diuretics)
- Diet counseling based on lab results (e.g., low Na⁺, K⁺, protein)
📌 VI. Key Points to Remember
✔ Diagnostic tests confirm type, cause, and severity of kidney/urinary disease
✔ Interpretation must guide clinical and nursing decisions
✔ Monitor for complications of procedures
✔ Provide emotional support and education to the patient
✔ Regular follow-up tests are crucial in CKD/ESRD management
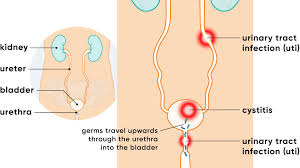
🚽 Urinary Tract Infection (UTI).

🧾 Definition
A Urinary Tract Infection (UTI) is an infection that occurs in any part of the urinary system, including:
- Kidneys (pyelonephritis)
- Ureters
- Bladder (cystitis)
- Urethra (urethritis)
🦠 Causative Organisms
🔹 Bacteria (most common)
- Escherichia coli (E. coli) – 💯 most common
- Klebsiella, Proteus, Enterococcus, Pseudomonas
🔹 Fungi – Candida (in immunocompromised)
🔹 Viruses – Rare, often in children or immunocompromised
📊 Types of UTI
| Type | Involved Organ | Common Name |
|---|---|---|
| 🟡 Lower UTI | Bladder & urethra | Cystitis, Urethritis |
| 🔴 Upper UTI | Kidneys | Pyelonephritis |
| 🟠 Recurrent UTI | ≥2 in 6 months or ≥3 in 12 months | Chronic/recurrent |
| 🟣 Complicated UTI | In patients with structural/functional abnormalities or catheter use | Hospital-acquired |
🧠 Etiology / Causes
🔹 Poor perineal hygiene
🔹 Catheterization or instrumentation
🔹 Urinary retention or obstruction (e.g., BPH, stones)
🔹 Short urethra in females
🔹 Diabetes mellitus (glucose in urine encourages bacteria)
🔹 Immunosuppression
🔹 Pregnancy (hormonal & anatomical changes)
🧬 Pathophysiology
- Bacteria ascend through the urethra
- Multiply and invade the bladder → Cystitis
- If untreated, may ascend to ureters/kidneys → Pyelonephritis
- Triggers inflammation, mucosal edema, and immune response
- Can lead to systemic infection (urosepsis) if severe
🚨 Signs & Symptoms
🔹 Lower UTI (Cystitis)
- 🩸 Burning sensation during urination (dysuria)
- 🔁 Increased frequency and urgency
- 🌙 Nocturia
- 🔍 Cloudy, foul-smelling urine
- 🩸 Hematuria (blood in urine)
- ⚡ Suprapubic discomfort
🔹 Upper UTI (Pyelonephritis)
- 🌡️ Fever, chills
- 😣 Flank pain (costovertebral angle tenderness)
- 🤮 Nausea, vomiting
- 🔁 Frequency, dysuria (may still be present)
🧪 Diagnostic Tests
| Test | Purpose |
|---|---|
| Urinalysis (R/M) | Detects WBCs, RBCs, nitrites, bacteria |
| Urine Culture & Sensitivity (C/S) | Identifies organism and best antibiotic |
| CBC | Shows ↑ WBC count in infection |
| Blood cultures | If urosepsis is suspected |
| Ultrasound / KUB | Detect structural causes, obstruction |
| Cystoscopy | In recurrent UTIs to evaluate anatomy |
💊 Medical Management
✅ Antibiotics (based on C/S)
- Nitrofurantoin (common in simple UTI)
- Trimethoprim-sulfamethoxazole (TMP-SMX)
- Ciprofloxacin, Levofloxacin (complicated UTI)
- Cephalosporins
- Amoxicillin-clavulanic acid
- Antifungals if fungal UTI
✅ Supportive Treatment
- 💧 Adequate hydration (2–3 liters/day)
- 💊 Analgesics (e.g., phenazopyridine – for burning)
- 🛌 Rest for pyelonephritis
- ⛔ Avoid caffeine, alcohol, spicy foods
👩⚕️ Nursing Management
🩺 Assessment
- Monitor urinary output, color, odor
- Assess for signs of systemic infection
- Monitor temperature and vital signs
- Check for flank or suprapubic pain
🧷 Nursing Interventions
- Encourage increased fluid intake
- Educate on perineal hygiene (front to back wiping)
- Administer medications as prescribed
- Monitor response to antibiotics
- Educate on completing full antibiotic course
- Prevent catheter-associated UTI (CAUTI) – aseptic technique, early removal
- Encourage voiding every 2–3 hours
🍽️ Nutritional Considerations
- 🚱 Avoid bladder irritants: caffeine, citrus, spicy food, alcohol
- 🍒 Include cranberry juice (evidence mixed but sometimes helpful)
- 🧂 Low sodium if fluid retention
- 💧 Maintain good hydration unless contraindicated
⚠️ Complications
- 🔺 Pyelonephritis
- ⚠️ Urosepsis (life-threatening)
- 🧱 Renal scarring (in recurrent UTI)
- 🧫 Chronic kidney disease
- 👶 Pregnancy complications (preterm labor, low birth weight)
🧠 Prevention Tips
- 🔄 Empty bladder completely during voiding
- 🚽 Urinate before and after intercourse
- 🧻 Wipe front to back
- 🚫 Avoid irritant soaps or sprays
- 🩲 Wear cotton underwear
- 🚱 Limit use of public baths or douches
📌 Key Points
✔ UTI is common, especially in women
✔ Early detection & proper antibiotic treatment = key
✔ Prevent recurrence by addressing risk factors
✔ Educate patient on hygiene and hydration
✔ Watch for signs of complication (fever, back pain, low urine output)
🚽 CYSTITIS
(Bladder Inflammation / Lower Urinary Tract Infection)
🧾 Definition
Cystitis is the inflammation of the urinary bladder, most commonly caused by bacterial infection, but may also be due to chemical irritants, medications, or radiation. It is a type of lower urinary tract infection (UTI).
🦠 Causes of Cystitis
🔹 Infectious Causes (most common)
- Bacterial (especially Escherichia coli – 80–90% of cases)
- Klebsiella, Proteus, Enterococcus, Staphylococcus saprophyticus
- Fungal – Candida albicans (in immunocompromised)
- Viral (rare)
🔹 Non-Infectious Causes
- Chemical irritants (e.g., hygiene sprays, bubble baths)
- Radiation (post-radiotherapy bladder inflammation)
- Interstitial cystitis (chronic, non-infective)
- Drug-induced (e.g., cyclophosphamide)
📊 Types of Cystitis
| Type | Description |
|---|---|
| Acute Cystitis | Sudden onset, bacterial infection |
| Chronic Cystitis | Recurrent or persistent bladder inflammation |
| Interstitial Cystitis | Non-infectious, chronic, painful bladder syndrome |
| Radiation Cystitis | Due to pelvic radiotherapy |
| Hemorrhagic Cystitis | Blood in urine due to infection or drugs |
| Catheter-associated Cystitis | Occurs with long-term catheterization |
🧬 Pathophysiology of Cystitis
- Microorganisms (usually ascending from the urethra) enter the bladder
- Adhere to bladder mucosa and multiply
- Trigger an inflammatory response → WBC infiltration
- Causes edema, mucosal irritation, pain, and dysuria
- If untreated, may spread to kidneys → pyelonephritis
🚨 Signs and Symptoms
| Symptom | Description |
|---|---|
| 🔥 Dysuria | Burning sensation while urinating |
| 💦 Urinary frequency | Frequent urge to urinate |
| 🧻 Urinary urgency | Sudden, strong need to urinate |
| 🌙 Nocturia | Night-time urination |
| ⚡ Suprapubic discomfort | Pain/pressure in lower abdomen |
| 🩸 Hematuria | Blood in urine (may appear pink/red) |
| 🌫️ Cloudy, foul-smelling urine | Due to pus or bacteria |
| 🌡️ Low-grade fever | (if infection spreads) |
🧪 Diagnosis
🧫 Laboratory Tests
- Urinalysis (R/M) – WBCs, RBCs, nitrites, leukocyte esterase
- Urine Culture & Sensitivity (C/S) – Identifies bacteria & appropriate antibiotic
- CBC – Elevated WBC count if systemic response
- CRP/ESR – Elevated in inflammation (chronic or interstitial)
🖥️ Imaging (if recurrent or complicated)
- Ultrasound KUB – To rule out stones or obstruction
- CT scan – In severe, chronic, or atypical cases
- Cystoscopy – For chronic or interstitial cystitis
💊 Medical Management
✅ Antibiotic Therapy (based on C/S report)
- Uncomplicated cystitis:
- Nitrofurantoin
- Trimethoprim-sulfamethoxazole (TMP-SMX)
- Fosfomycin
- Cephalexin
- Complicated/recurrent cases:
- Ciprofloxacin or Levofloxacin
- Amoxicillin-clavulanic acid
✅ Supportive Therapy
- Analgesics (e.g., Phenazopyridine) – for dysuria
- Antispasmodics – to relieve bladder spasms
- Hydration – increase fluid intake to flush bacteria
- Avoid bladder irritants (alcohol, caffeine, spicy food)
✅ Chronic/Interstitial Cystitis
- Amitriptyline or antihistamines
- Bladder instillations (e.g., DMSO, heparin)
- Pelvic floor physical therapy
🏥 Surgical Management
➡ Usually not required for simple cystitis, but may be considered in:
✅ Indications for Surgical Intervention:
- Recurrent infections due to anatomical abnormality
- Obstructive causes (e.g., strictures, stones)
- Non-resolving interstitial cystitis
- Bladder augmentation or cystectomy (very rare, last resort)
🛠️ Surgical Procedures:
- Cystoscopy + fulguration of Hunner’s ulcers (in interstitial cystitis)
- Urethral dilation or urethroplasty if obstruction
- Removal of bladder stones or tumors
- Suprapubic catheterization for chronic retention
📌 Key Points
✔ Cystitis is mostly bacterial, especially in women
✔ Prompt treatment with appropriate antibiotics prevents complications
✔ Encourage hydration and hygiene to prevent recurrence
✔ Chronic or interstitial cystitis needs long-term multidisciplinary care
✔ Surgical options are rarely needed, reserved for complicated or resistant cases
👩⚕️ NURSING MANAGEMENT OF CYSTITIS
(Inflammation of the Urinary Bladder)
🧠 I. Nursing Assessment
✅ Subjective Data
- Patient complaints of:
- 🔥 Burning sensation while urinating (dysuria)
- 🔁 Increased frequency and urgency
- ⚡ Suprapubic discomfort
- 🌡️ Fever or chills (if infection ascends)
✅ Objective Data
- Observe:
- 💦 Cloudy, foul-smelling, or bloody urine
- 🧴 Signs of perineal redness or irritation
- 🌡️ Elevated temperature
- 📋 Urine test reports (WBCs, bacteria, nitrites)
- 🧫 Positive urine culture
- 🧍 Restlessness or discomfort on voiding
🎯 II. Nursing Diagnoses
- 🔥 Acute pain related to bladder inflammation and infection
- 💦 Impaired urinary elimination related to urgency, frequency, and dysuria
- 🦠 Risk for infection (spread) related to ascending bacteria
- 🧠 Deficient knowledge related to disease condition, hygiene, and prevention
- 😖 Anxiety related to discomfort and altered urinary patterns
📝 III. Nursing Goals / Planning
✅ Relieve dysuria and suprapubic pain
✅ Promote normal urinary elimination pattern
✅ Prevent complications like pyelonephritis or recurrent infection
✅ Educate patient about hygiene and medication compliance
✅ Reduce anxiety and provide emotional support
🩺 IV. Nursing Interventions
🔹 1. Pain Management
- 💊 Administer prescribed analgesics (e.g., phenazopyridine)
- 🧊 Encourage warm sitz baths for comfort
- 📈 Monitor pain intensity and duration regularly
- 🛌 Provide rest and relaxation
🔹 2. Infection Control
- 💧 Encourage 2–3 liters of fluid intake/day (unless contraindicated)
- 💉 Administer prescribed antibiotics on time
- 🧪 Monitor urine output, color, and clarity
- 🌡️ Monitor temperature and signs of systemic infection
- 🧴 Maintain perineal hygiene (front to back cleaning)
- ⛔ Avoid use of strong soaps, sprays, or bubble baths
🔹 3. Promote Urinary Elimination
- 🚽 Encourage frequent voiding (every 2–3 hrs)
- 🧼 Clean the perineal area after each void
- 🛏️ Ensure comfortable toilet access
- 🧍 Assist mobility if patient is weak or elderly
🔹 4. Patient Education
- 📖 Teach importance of completing full course of antibiotics
- ❌ Avoid bladder irritants: caffeine, alcohol, spicy foods
- 🧴 Practice proper perineal hygiene
- 👖 Wear loose, cotton underwear
- 🧊 Teach early signs of recurrence to report
- 👩⚕️ Educate catheterized patients/families on catheter care
🔹 5. Psychosocial Support
- 🗣️ Provide reassurance and therapeutic communication
- 🧘 Encourage stress-reducing activities
- 🧍 Maintain privacy during procedures and toileting
- 📋 Answer all queries to reduce anxiety
📊 V. Evaluation Criteria
✅ Pain reduced within 24–48 hours
✅ Clear urine with no foul smell or hematuria
✅ Patient completes antibiotics as prescribed
✅ Temperature remains normal
✅ Patient verbalizes understanding of hygiene and recurrence prevention
✅ Patient maintains normal voiding pattern
📌 Key Points
✔ Prompt nursing interventions relieve discomfort and prevent complications
✔ Hygiene education is key to preventing recurrence
✔ Ensure fluid intake and early reporting of symptoms
✔ Monitor response to antibiotics closely
✔ Provide emotional support and patient-centered care
🥗 NUTRITIONAL CONSIDERATION in CYSTITIS
Proper diet and hydration play a supportive role in recovery and prevention of recurrent infections.
✅ Encouraged:
- 💧 Increase fluid intake (2–3 liters/day unless contraindicated) – helps flush out bacteria
- 🍒 Cranberry juice – may help prevent bacterial adhesion to bladder walls (evidence mixed but commonly recommended)
- 🍉 Water-rich fruits and vegetables – cucumber, watermelon, oranges, carrots
- 🫗 Warm fluids (soups, herbal teas) – soothing and hydrating
- 🍚 Easily digestible, low-fat diet during acute infection
❌ Avoid:
- ☕ Caffeine (coffee, cola, chocolate) – bladder irritant
- 🌶️ Spicy and acidic foods (tomatoes, vinegar, citrus) – worsen burning
- 🍺 Alcohol – irritates bladder lining and dehydrates
- 🧂 Excess salt – can aggravate inflammation
- ❄️ Cold carbonated drinks – worsen urinary irritation
⚠️ COMPLICATIONS of CYSTITIS
If untreated or recurrent, cystitis can lead to several short- and long-term complications:
| Complication | Description |
|---|---|
| 🔼 Pyelonephritis | Infection ascending to kidneys; can become life-threatening |
| 🧫 Urosepsis | Systemic infection from urinary tract → septicemia |
| 🧱 Bladder scarring | From chronic inflammation; may reduce bladder elasticity |
| 🔁 Recurrent UTIs | Frequent infections → impact quality of life |
| 🚻 Urinary retention | Due to inflammation/swelling |
| 💊 Antibiotic resistance | Due to inappropriate or repeated antibiotic use |
| 👶 Pregnancy complications | In pregnant women: preterm labor, low birth weight |
📌 KEY POINTS on CYSTITIS
✅ Cystitis = inflammation of the bladder, most commonly bacterial (E. coli)
✅ Women are more affected due to shorter urethra
✅ Signs: dysuria, urgency, frequency, cloudy/foul urine, suprapubic pain
✅ Diagnosis: Urinalysis, urine culture, and sometimes imaging
✅ Treatment: Antibiotics + fluids + symptom relief
✅ Nursing care focuses on pain relief, hydration, hygiene, and prevention
✅ Diet should support healing – no caffeine, alcohol, spicy food
✅ Prevent recurrence with good hygiene, fluid intake, and complete antibiotic course
✅ Monitor for signs of complications like fever, flank pain, or hematuria
✅ Education and early reporting of symptoms are essential for recovery and prevention
🔥 PYELONEPHRITIS
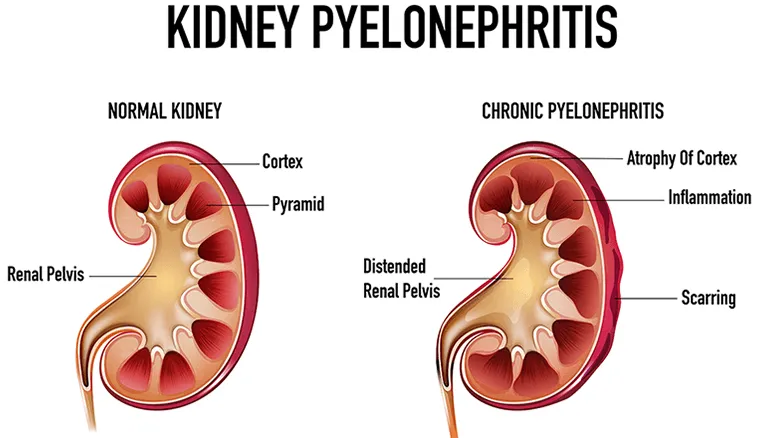
(Kidney Infection – Upper Urinary Tract Infection)
🧾 Definition
Pyelonephritis is an inflammation and infection of the kidney tissue, calyces, and renal pelvis, typically caused by bacterial invasion from the lower urinary tract (bladder/urethra) or the bloodstream.
It is a serious upper urinary tract infection (UTI) that can lead to kidney damage if not treated promptly.
🦠 Causes of Pyelonephritis
✅ Infectious Causes (Most Common)
- Ascending infection from bladder (most frequent pathway)
- Hematogenous spread (from bloodstream in sepsis)
🔍 Common Pathogens:
- 🦠 Escherichia coli – most common (85–90%)
- Proteus mirabilis
- Klebsiella pneumoniae
- Enterococcus faecalis
- Pseudomonas aeruginosa
🧬 Predisposing/Risk Factors
- 🔁 Recurrent lower UTIs (cystitis)
- 🧱 Urinary tract obstruction (e.g., renal stones, enlarged prostate)
- 🧪 Vesicoureteral reflux (VUR) – backward flow of urine from bladder to kidneys
- 💉 Diabetes mellitus (poor immunity and glucose in urine)
- 🚻 Pregnancy (hormonal and anatomical changes)
- 🚿 Indwelling urinary catheters
- 😷 Immunosuppression
- 🧒 Children with structural defects of urinary tract
📊 Types of Pyelonephritis
| 🧾 Type | 🔍 Description |
|---|---|
| ✅ Acute Pyelonephritis | Sudden-onset bacterial infection of kidneys; often following cystitis |
| ♻️ Chronic Pyelonephritis | Recurrent or persistent infection that causes renal scarring and progressive loss of kidney function |
| 🧫 Emphysematous Pyelonephritis | Severe necrotizing infection of kidney with gas-forming organisms; common in diabetics |
| 🧪 Xanthogranulomatous Pyelonephritis (XGP) | Rare, chronic form with destruction of kidney tissue; often associated with staghorn calculi |
| 🩸 Pyonephrosis | Accumulation of pus in renal pelvis due to obstructed and infected kidney; urological emergency |
🧬 PATHOPHYSIOLOGY OF PYELONEPHRITIS
- Entry of pathogens (usually bacteria like E. coli) into the lower urinary tract (bladder/urethra)
- Bacteria ascend via the ureters to reach the renal pelvis and kidney parenchyma
- The pathogens invade renal interstitial tissue, leading to:
- Inflammatory response (WBC infiltration)
- Interstitial edema and congestion
- Tubular necrosis in severe cases
- Kidney function is impaired temporarily or permanently (especially in chronic cases)
- If untreated, infection may:
- Spread into bloodstream → urosepsis
- Cause renal scarring → chronic kidney damage
🚨 SIGNS AND SYMPTOMS OF PYELONEPHRITIS
| System | Clinical Features |
|---|---|
| 🌡️ General | Sudden high-grade fever, chills, fatigue, malaise |
| 🩺 Renal/Urinary | Flank pain or costovertebral angle (CVA) tenderness, lower abdominal pain |
| 🚽 Urinary | Dysuria (burning), frequency, urgency, cloudy/foul-smelling urine, hematuria |
| 🤢 Gastrointestinal | Nausea, vomiting, anorexia |
| 🫀 Severe Cases | Hypotension, tachycardia (signs of sepsis), confusion (especially in elderly) |
🔍 CVA Tenderness Test: Positive when gentle tapping at the costovertebral angle elicits pain → indicates renal inflammation
🧪 DIAGNOSIS OF PYELONEPHRITIS
🔬 1. Laboratory Investigations
| Test | Findings |
|---|---|
| Urinalysis (R/M) | Pyuria (↑ WBCs), bacteriuria, hematuria, positive leukocyte esterase & nitrites |
| Urine Culture & Sensitivity (C/S) | Confirms the organism and guides antibiotic choice |
| CBC (Complete Blood Count) | ↑ Total WBC count, ↑ neutrophils |
| CRP / ESR | Elevated inflammatory markers |
| Blood cultures | To rule out bacteremia/sepsis in severe cases |
| Renal function tests (BUN, creatinine) | Elevated in severe or chronic cases |
| Procalcitonin | May be elevated in bacterial systemic infection (urosepsis) |
🖥️ 2. Imaging Studies
| Imaging | Purpose |
|---|---|
| Ultrasound (KUB) | Detects hydronephrosis, abscess, obstruction (especially in pregnancy or stones) |
| CT scan (abdomen/pelvis with contrast) | Gold standard for detecting complications (e.g., abscess, emphysematous pyelonephritis) |
| IVP (Intravenous Pyelogram) | Rarely used; shows delayed excretion or obstruction |
| DMSA Renal Scan | Detects renal scarring (used in pediatric or recurrent cases) |
💊 I. MEDICAL MANAGEMENT
🧠 Goal: Eliminate infection, relieve symptoms, prevent complications, and preserve kidney function.
✅ 1. Antibiotic Therapy
Initiated promptly, often before culture results (empiric), and adjusted later based on C/S report.
| Severity | Common Antibiotics |
|---|---|
| Mild to Moderate (oral) | – Ciprofloxacin |
- Levofloxacin
- Trimethoprim-sulfamethoxazole (TMP-SMX)
- Amoxicillin-clavulanate | |
- Severe (IV) | – Ceftriaxone
- Piperacillin-tazobactam
- Meropenem (if ESBL-producing bacteria)
- Gentamicin (caution in renal impairment) |
🔁 Duration:
- 7–14 days for uncomplicated cases
- Longer in complicated/recurrent infections
✅ 2. Supportive Therapy
- 💧 IV Fluids – maintain hydration and renal perfusion
- 💊 Antipyretics & Analgesics – Paracetamol for fever and pain
- 🚫 Avoid nephrotoxic drugs (NSAIDs, aminoglycosides – unless closely monitored)
- 🛌 Rest – during febrile period
- ⏱️ Monitor vitals – especially temperature, BP, HR for signs of sepsis
- 🚽 Encourage frequent voiding – to prevent urinary stasis
✅ 3. Management of Underlying Cause (if present)
- Diabetes: Control blood sugar
- Obstruction: Relieve with stent or catheter
- Stones: Refer for stone management
🔪 II. SURGICAL MANAGEMENT
👨⚕️ Indicated in complications, obstructive uropathy, or recurrent non-resolving infections.
✅ 1. Indications for Surgical Intervention
- 🔄 Recurrent pyelonephritis due to anatomical obstruction
- 🧱 Ureteral obstruction or stones
- 💉 Abscess not responding to antibiotics
- 🧫 Emphysematous pyelonephritis
- 🧪 Pyonephrosis (pus in kidney pelvis)
- ☠️ Life-threatening urosepsis due to obstruction
✅ 2. Common Surgical Procedures
| Procedure | Purpose |
|---|---|
| Percutaneous Nephrostomy | Temporary drainage of infected urine from obstructed kidney |
| Ureteric Stenting | Bypass obstruction to allow drainage |
| Ureterolithotomy / Lithotripsy | Stone removal from ureters/kidneys |
| Drainage of Renal Abscess | Via percutaneous or surgical approach |
| Nephrectomy (rare) | Removal of a severely damaged or non-functioning kidney in chronic or severe cases |
📌 KEY GOALS OF MANAGEMENT
✔ Prompt and effective antibiotic therapy
✔ Maintain hydration and electrolyte balance
✔ Identify and correct obstruction or anatomical abnormalities
✔ Prevent renal scarring and chronic kidney disease
✔ Monitor for and treat urosepsis or systemic complications
👩⚕️ NURSING MANAGEMENT OF PYELONEPHRITIS
(Kidney Infection – Upper Urinary Tract Infection)
🧠 I. Nursing Assessment
✅ Subjective Data
- Complaint of flank pain, burning urination, fever, or nausea
- History of recurrent UTIs or urinary obstruction
- Feelings of fatigue, chills, or urinary urgency
✅ Objective Data
- 🌡️ Fever, ↑ HR, ↑ RR (sepsis signs)
- 🔍 Costovertebral angle (CVA) tenderness
- 📋 Abnormal urinalysis/culture reports (bacteria, WBCs)
- 💧 Decreased urine output (oliguria)
- 🩺 Elevated WBC count or serum creatinine
🎯 II. Nursing Diagnoses
- 🦠 Risk for infection (spread/sepsis) related to bacterial invasion of kidneys
- 🔥 Acute pain related to renal inflammation
- 💦 Impaired urinary elimination related to infection or obstruction
- 💧 Fluid volume deficit related to fever, vomiting, and decreased intake
- 🧠 Deficient knowledge related to disease process, medication, and prevention
- 😓 Fatigue related to systemic infection and inflammation
📝 III. Nursing Goals / Expected Outcomes
✅ Patient will report reduced pain within 48–72 hours
✅ Maintain adequate urine output and clear urine
✅ Demonstrate understanding of medication regimen
✅ Maintain normal body temperature
✅ Prevent complications such as urosepsis or renal damage
🩺 IV. Nursing Interventions
🔹 1. Pain and Fever Management
- 💊 Administer prescribed analgesics and antipyretics (e.g., paracetamol)
- 🛌 Provide rest in a comfortable position (semi-Fowler’s or supine with knees flexed)
- 🧊 Offer warm compresses on the flank area for pain relief
- 🌡️ Monitor and document temperature regularly
🔹 2. Infection Control
- 💉 Administer antibiotics as prescribed, on schedule
- 🧫 Monitor lab results (WBCs, cultures, CRP) for effectiveness
- 🧼 Emphasize hand hygiene and perineal hygiene
- 🔍 Watch for signs of urosepsis (hypotension, confusion, tachycardia)
🔹 3. Urinary Elimination Monitoring
- 📋 Monitor intake and output (I/O) – hourly in severe cases
- 🚽 Encourage frequent voiding (every 2–3 hours)
- 💦 Observe urine color, clarity, volume, and odor
- ⛔ Monitor for signs of urinary retention or obstruction
🔹 4. Fluid Balance and Hydration
- 💧 Encourage oral fluid intake (2–3 liters/day unless restricted)
- 💉 Provide IV fluids in case of vomiting, dehydration, or severe infection
- 🩺 Monitor vital signs, BP, and daily weight
- ⚠️ Watch for signs of fluid overload in patients with reduced renal function
🔹 5. Patient and Family Education
- 📖 Educate about the importance of completing antibiotics
- 🚿 Teach proper perineal hygiene (front to back cleaning)
- ☕ Advise to avoid bladder irritants (caffeine, alcohol, spicy food)
- 🧼 Educate about urinary tract health: voiding after intercourse, avoiding tight clothing
- 📞 Teach early warning signs of recurrence to report promptly
📊 V. Evaluation
| Goal | Evaluation Criteria |
|---|---|
| Pain relief | Patient reports ↓ pain and fever |
| Infection control | Normal WBC count, afebrile state |
| Hydration | Normal urine output & clear urine |
| Learning | Patient verbalizes understanding of meds and prevention |
| Complication prevention | No signs of urosepsis or renal failure |
📌 KEY NURSING TIPS
✔ Monitor for fever, flank pain, CVA tenderness
✔ Administer fluids + antibiotics as prescribed
✔ Promote urinary drainage and hygiene
✔ Educate to prevent recurrence or progression to chronic pyelonephritis
✔ Be vigilant for signs of urosepsis or worsening renal function.
🥗 NUTRITIONAL CONSIDERATION IN PYELONEPHRITIS
Proper nutrition supports healing, improves immune response, and helps flush out toxins from the kidneys.
✅ Recommended Diet:
- 💧 Increase fluid intake (2–3 liters/day unless contraindicated) – promotes urine flow and bacterial elimination
- 🥬 Alkaline-forming foods – leafy greens, carrots, pumpkin, bananas
- 🧂 Low-sodium diet – prevents fluid retention and reduces kidney workload
- 🥛 Protein moderation – especially in chronic or recurring pyelonephritis
- 🍉 Water-rich fruits – watermelon, oranges, cucumber for hydration
- 🍵 Warm fluids – herbal teas, clear soups to soothe and hydrate
- 🍯 Foods rich in Vitamin C – boosts immunity (e.g., amla, citrus fruits)
❌ Foods to Avoid:
- ☕ Caffeine and cola drinks – bladder irritants
- 🍋 Citrus juices (in acute stage) – may irritate bladder in some cases
- 🍟 Processed foods and salty snacks – high sodium content
- 🍺 Alcohol – irritates urinary tract and dehydrates
- 🌶️ Spicy and acidic foods – may aggravate urinary symptoms
⚠️ COMPLICATIONS OF PYELONEPHRITIS
Untreated or poorly managed pyelonephritis can result in severe, even life-threatening complications.
🔥 Acute Complications
- Renal abscess formation
- Pyonephrosis (pus in renal pelvis)
- Emphysematous pyelonephritis – gas-forming infection, mostly in diabetics
- Urosepsis – bacteria spread into bloodstream, leading to septic shock
♻️ Chronic Complications
- Chronic pyelonephritis – persistent infection leads to fibrosis and scarring
- Hypertension – due to renal scarring and fluid imbalance
- Renal insufficiency or Chronic Kidney Disease (CKD)
- Recurrent UTIs – especially in patients with structural abnormalities
- End-stage renal disease (ESRD) – rare but possible with repeated damage
📌 KEY POINTS TO REMEMBER
✔ Pyelonephritis is a serious infection of the kidneys, usually from an ascending UTI
✔ Caused mainly by E. coli and associated with fever, flank pain, dysuria, and CVA tenderness
✔ Early diagnosis and appropriate antibiotics prevent complications
✔ Encourage fluids, proper hygiene, and urinary habits
✔ Monitor for signs of urosepsis, renal failure, or recurrence
✔ Dietary modifications support kidney healing and immune function
✔ In severe cases, surgical drainage or nephrostomy may be required
✔ Nursing care involves close monitoring, medication administration, pain control, and patient education.
🧠 NEPHRITIS

(Inflammation of the Nephrons – the functional units of the kidneys)
🧾 DEFINITION
Nephritis is the inflammation of the nephrons (functional units of the kidneys), primarily involving the glomeruli, tubules, or interstitial tissues, which can impair the kidney’s ability to filter and eliminate waste products, electrolytes, and fluids effectively.
Nephritis may be acute or chronic, and can result in proteinuria, hematuria, oliguria, and hypertension.
🧬 CAUSES OF NEPHRITIS
🔹 Infectious Causes
- Post-streptococcal infection (commonly after throat or skin infection)
- Bacterial or viral infections (e.g., hepatitis B/C, HIV)
🔹 Autoimmune Disorders
- Systemic lupus erythematosus (SLE)
- Goodpasture’s syndrome
- IgA nephropathy (Berger’s disease)
🔹 Toxins and Drugs
- NSAIDs, certain antibiotics
- Chemotherapeutic agents
- Heavy metals
🔹 Metabolic and Other Conditions
- Diabetes mellitus (can lead to diabetic nephropathy)
- Hypertension (can cause secondary nephritic changes)
- Genetic conditions (e.g., Alport syndrome)
📊 TYPES OF NEPHRITIS
| Type | Description |
|---|---|
| Glomerulonephritis | Inflammation of the glomeruli, often immune-mediated |
| Interstitial Nephritis | Inflammation of renal interstitium and tubules, often drug-induced |
| Pyelonephritis | Infection and inflammation of renal pelvis and tissue, usually bacterial |
| Lupus Nephritis | Kidney inflammation caused by systemic lupus erythematosus |
| Hereditary Nephritis (Alport Syndrome) | Genetic condition affecting glomeruli and basement membrane |
| Membranoproliferative Nephritis | Immune complex deposition causes thickening of glomerular basement membrane |
| Mesangiocapillary Nephritis | Inflammation with mesangial and capillary involvement (variant of MPGN) |
🔬 PATHOPHYSIOLOGY OF NEPHRITIS
(Example: Glomerulonephritis – most common form)
- Trigger (infection, autoimmune, drug) activates the immune system
- Immune complexes deposit in the glomerular basement membrane
- Triggers complement activation and leukocyte infiltration
- Leads to inflammation, swelling, and damage to glomeruli
- Results in:
- 🩸 Hematuria (RBCs leak into urine)
- 💧 Fluid retention (due to reduced filtration)
- 🧂 Hypertension (salt & water retention)
- ⚖️ Oliguria and azotemia (reduced urine output and nitrogenous waste buildup)
- 🧬 Proteinuria (due to glomerular damage)
🚨 SIGNS AND SYMPTOMS OF NEPHRITIS
| Symptom | Description |
|---|---|
| 🩸 Hematuria | Cola-colored or pink urine due to RBCs |
| 💦 Oliguria | Reduced urine output |
| 🌊 Edema | Puffy eyes, facial swelling, pedal edema (due to fluid retention) |
| 🧂 Hypertension | Resulting from sodium & water retention |
| 🔥 Fever | If infection is present |
| 🥱 Fatigue & Malaise | From uremia and anemia |
| 🧠 Headache or confusion | In severe cases with high BP or uremia |
| 🩺 Proteinuria | Frothy urine (protein leakage) |
🧪 DIAGNOSIS OF NEPHRITIS
🧫 Laboratory Tests
| Test | Findings |
|---|---|
| Urinalysis (R/M) | Hematuria, proteinuria, RBC casts, WBCs |
| Urine Culture | Rule out infection (e.g., in pyelonephritis) |
| Blood Tests | ↑ Serum creatinine, ↑ BUN, ↓ GFR |
| Electrolytes | Imbalance (↑ K⁺, ↓ Na⁺ in some cases) |
| CBC | Anemia (↓ Hb), leukocytosis in infection |
| ASO Titer | Positive in post-streptococcal GN |
| ANA / Anti-dsDNA / Complement levels | For lupus nephritis |
| Anti-GBM Antibodies | In Goodpasture’s syndrome |
🖥️ Imaging Studies
- Renal Ultrasound – to assess kidney size, structure, swelling, or obstruction
- CT Scan (KUB) – if abscess or structural abnormality suspected
- DMSA Renal Scan – for functional assessment in chronic cases
🔬 Renal Biopsy
- Essential for diagnosis in lupus nephritis, interstitial nephritis, or chronic GN
- Helps determine the type, severity, and prognosis
💊 I. MEDICAL MANAGEMENT
Goals: Control inflammation, relieve symptoms, treat underlying cause, and prevent complications like renal failure.
✅ 1. General Supportive Therapy
- 💧 Fluid balance monitoring – strict input/output charting
- 🛌 Rest during acute phase to reduce metabolic demand
- 🧂 Sodium restriction – especially in edema and hypertension
- 💧 Fluid restriction – if oliguria or fluid overload
- 🚫 Protein restriction – in moderate to severe renal dysfunction
- 📈 Monitor weight, BP, serum electrolytes, creatinine daily
✅ 2. Antibiotic Therapy
- For infection-related nephritis (e.g., post-streptococcal):
- Penicillin, cephalosporins, or other culture-sensitive antibiotics
- Early treatment of pharyngitis or skin infection to prevent GN
✅ 3. Anti-inflammatory and Immunosuppressive Therapy
- In autoimmune nephritis (e.g., lupus nephritis, IgA nephropathy):
- Corticosteroids (e.g., Prednisolone) – reduce inflammation
- Immunosuppressants: Cyclophosphamide, Azathioprine, Mycophenolate mofetil
- Biologics: Rituximab (in resistant lupus nephritis)
✅ 4. Antihypertensives
- To control renal hypertension and reduce proteinuria:
- ACE inhibitors (e.g., Enalapril, Lisinopril)
- ARBs (e.g., Losartan)
- Diuretics (e.g., Furosemide) if edema is present
✅ 5. Diuretics
- For edema management:
- Loop diuretics (e.g., furosemide) for fluid overload
- Watch for hypokalemia or volume depletion
✅ 6. Renal Replacement Therapy
- For severe or end-stage renal failure due to chronic nephritis:
- Hemodialysis
- Peritoneal dialysis
🔪 II. SURGICAL MANAGEMENT
🧠 Surgical intervention is rare in typical nephritis but may be required in specific or complicated cases.
🔹 1. Renal Biopsy
- Not therapeutic but diagnostic
- Helps determine:
- Type of nephritis (e.g., lupus nephritis, IgA nephropathy)
- Disease severity and prognosis
- Treatment plan (steroid responsiveness, immunosuppressants)
🔹 2. Surgical or Interventional Management (if complications arise)
| Procedure | Indication |
|---|---|
| Nephrostomy tube | Relief of urinary obstruction causing hydronephrosis |
| Nephrectomy | Non-functioning kidney due to end-stage scarring or severe infection |
| Dialysis access (AV fistula/peritoneal catheter) | For patients progressing to ESRD |
| Kidney transplantation | For end-stage renal disease from chronic nephritis |
📌 Summary Table
| Treatment Type | Used For |
|---|---|
| Antibiotics | Infection-triggered nephritis |
| Steroids/Immunosuppressants | Autoimmune nephritis (e.g., lupus nephritis) |
| ACE inhibitors/ARBs | Hypertension and proteinuria control |
| Diuretics | Fluid overload/edema |
| Dialysis | AKI or CKD due to nephritis |
| Surgery (rare) | Structural correction or ESRD (transplant) |
👩⚕️ NURSING MANAGEMENT OF NEPHRITIS
(Inflammation of the Nephrons – Kidney Units)
🧠 I. Nursing Assessment
✅ Subjective Data
- Complaints of:
- 🩸 Cola-colored or bloody urine (hematuria)
- 💦 Decreased urine output (oliguria)
- 😫 Generalized weakness, fatigue
- 🤕 Headache (due to hypertension)
- 😰 Swelling of face or legs (edema)
✅ Objective Data
- 🌡️ Low-grade fever (infection-related)
- 🧂 Facial/periorbital or pedal edema
- 🩺 Elevated BP
- 🔬 Lab reports: proteinuria, hematuria, ↑ BUN/creatinine
- 💧 Decreased urine output with frothy or dark urine
🎯 II. Nursing Diagnoses
- 💦 Fluid volume excess related to decreased kidney function
- 🧂 Impaired urinary elimination related to glomerular inflammation
- 🔥 Acute pain (flank or generalized) related to tissue inflammation
- 🧠 Risk for impaired skin integrity due to edema
- 📚 Deficient knowledge related to disease process and self-care
- 🧴 Risk for infection related to decreased immunity or immunosuppressive therapy
- 🥱 Activity intolerance related to fatigue and anemia
📝 III. Nursing Goals
✅ Maintain fluid-electrolyte balance
✅ Promote effective urinary elimination
✅ Reduce edema and hypertension
✅ Prevent complications like infection or renal failure
✅ Enhance knowledge about condition and self-care
✅ Promote rest and support recovery
🩺 IV. Nursing Interventions
🔹 1. Fluid Balance Monitoring
- 💧 Strict intake and output (I/O) charting
- ⚖️ Daily weight monitoring (same time each day)
- ⛔ Fluid restriction as prescribed in oliguria/edema
- 💉 Monitor IV fluids carefully if given
🔹 2. Monitor Vital Signs
- 🩺 Check BP every 4 hours – report elevation
- 📉 Monitor for hypotension (esp. in diuretic/dialysis therapy)
- 🌡️ Monitor temperature for infection
🔹 3. Manage Edema
- 🛌 Elevate legs to reduce dependent edema
- 🧦 Avoid tight clothing or shoes
- 🧂 Maintain low-sodium diet
- 💊 Administer diuretics as prescribed
🔹 4. Enhance Urinary Elimination
- 🚽 Encourage timed voiding if retention suspected
- 🧼 Maintain perineal hygiene to prevent UTI
- 🔍 Observe urine color, clarity, volume
- 🧫 Send samples for R/M and C/S as ordered
🔹 5. Pain and Comfort Measures
- 💊 Administer prescribed analgesics or antipyretics
- 🛌 Encourage rest in comfortable position
- 🌙 Limit physical activity during acute phase
🔹 6. Prevent Skin Breakdown
- 🧴 Inspect skin daily, especially over bony prominences
- 🧽 Provide gentle skin care
- 🛌 Reposition every 2 hours if patient is bed-bound
- Use pressure-relieving devices if needed
🔹 7. Patient & Family Education
- 📖 Explain disease condition in simple terms
- 💊 Teach importance of completing medications (steroids, antibiotics)
- 🧂 Educate on low-salt/protein diet (as prescribed)
- 🧼 Teach hygiene and infection prevention (if immunosuppressed)
- ☎️ Instruct on signs of recurrence or complication (e.g., reduced urine, swelling, high BP)
📊 V. Evaluation Criteria
| Goal | Expected Outcome |
|---|---|
| Fluid balance maintained | Stable weight, normal I/O |
| Pain relief achieved | Patient reports less discomfort |
| Normal BP maintained | BP within target range |
| Reduced edema | Visible decrease in swelling |
| Urine output improves | ≥0.5 mL/kg/hr urine production |
| Patient understanding | Demonstrates knowledge of care and meds |
📌 KEY POINTS TO REMEMBER
✔ Early nursing interventions prevent progression to chronic kidney disease
✔ Maintain fluid, electrolyte, and BP control
✔ Hygiene, rest, and diet are critical in the recovery phase
✔ Patient education is essential for long-term self-care
✔ Monitor for complications like renal failure, infection, or hypertensive crisis.
🥗 NUTRITIONAL CONSIDERATION IN NEPHRITIS
Diet plays a vital role in supporting kidney function, managing symptoms, and preventing complications in patients with nephritis.
✅ Recommended Diet
| Focus | Dietary Advice |
|---|---|
| 💧 Fluids | Monitor or restrict fluids in case of oliguria or edema |
| 🧂 Sodium | Low-sodium diet to control fluid retention and hypertension |
| 🥩 Protein | Moderate protein intake – reduce urea load, especially in chronic cases |
| 🍌 Potassium | Limit potassium-rich foods if serum K⁺ is elevated (e.g., banana, orange, potato) |
| 🥛 Phosphorus | Restrict phosphorus (milk, cheese, nuts) in chronic renal involvement |
| 🥗 Vitamins | Supplement with B-complex and iron in anemia; limit fat-soluble vitamins if renal failure present |
| 🧃 Small, frequent meals | Easily digestible foods, especially in uremic patients with poor appetite |
❌ Foods to Avoid
- 🧂 Pickles, chips, processed foods (high sodium)
- ☕ Caffeinated drinks
- 🍺 Alcohol
- 🍗 High-protein diets (esp. red meat in renal impairment)
- 🍦 Dairy in large amounts (for phosphorus control)
⚠️ COMPLICATIONS OF NEPHRITIS
If untreated or poorly managed, nephritis may progress to serious or irreversible conditions.
| Category | Complication |
|---|---|
| 🧠 Renal | – Acute kidney injury (AKI) |
- Chronic kidney disease (CKD)
- End-stage renal disease (ESRD) | | 🩺 Cardiovascular | – Hypertension
- Left ventricular hypertrophy
- Heart failure due to fluid overload | | 🧫 Infectious | – Urinary tract infections
- Sepsis in severe or immunosuppressed patients | | 🧍 Hematologic | – Anemia of chronic disease
- Hyperkalemia (life-threatening arrhythmia) | | 💊 Therapy-related | – Steroid side effects: moon face, hyperglycemia, infection risk
- Immunosuppression complications |
📌 KEY POINTS TO REMEMBER ABOUT NEPHRITIS
✔ Nephritis = inflammation of kidney structures, mostly glomeruli
✔ Caused by infection, autoimmune conditions, toxins, or genetic disorders
✔ Characterized by hematuria, proteinuria, edema, oliguria, and hypertension
✔ Diagnosis confirmed by urinalysis, renal function tests, and biopsy
✔ Medical treatment involves antibiotics, steroids, immunosuppressants, and diuretics
✔ Surgical options are rare but include renal biopsy, nephrostomy, or transplant in ESRD
✔ Nursing care focuses on fluid balance, BP control, infection prevention, skin care, and patient education
✔ Diet modification is essential – limit sodium, protein, and potassium as needed
✔ Monitor for complications like renal failure, sepsis, or hypertensive crisis
✔ Early recognition and multidisciplinary care can preserve kidney function and improve prognosis.
🧠 NEPHROTIC SYNDROME
📖 DEFINITION
Nephrotic Syndrome is a clinical condition characterized by a group of signs and symptoms resulting from increased permeability of the glomerular basement membrane, leading to excessive loss of protein in the urine (proteinuria).
It is defined by the classic tetrad:
- Massive proteinuria (>3.5 g/day)
- Hypoalbuminemia (<3.0 g/dL)
- Edema (generalized – anasarca)
- Hyperlipidemia (↑ cholesterol, ↑ triglycerides)
🦠 CAUSES OF NEPHROTIC SYNDROME
Nephrotic syndrome can be:
✅ Primary (Idiopathic) Glomerular Diseases
- Disease limited to the kidney
- Most common in children
| Cause | Description |
|---|---|
| Minimal Change Disease (MCD) | Most common in children; normal glomeruli on light microscopy |
| Focal Segmental Glomerulosclerosis (FSGS) | Common in adults; segmental scarring in some glomeruli |
| Membranous Nephropathy | Thickened glomerular basement membrane, seen in adults |
| Mesangioproliferative GN | Mesangial cell proliferation with immune deposits |
❎ Secondary Causes (Systemic Conditions or External Agents)
| Category | Examples |
|---|---|
| Infections | Hepatitis B & C, HIV, malaria, syphilis |
| Autoimmune Disorders | Systemic lupus erythematosus (SLE), rheumatoid arthritis |
| Drugs & Toxins | NSAIDs, penicillamine, gold, heroin |
| Malignancy | Lymphoma, leukemia, solid tumors |
| Metabolic Disorders | Diabetes mellitus (diabetic nephropathy), amyloidosis |
📊 TYPES OF NEPHROTIC SYNDROME
| Type | Characteristics |
|---|---|
| Congenital Nephrotic Syndrome | Rare, genetic; appears in infants (e.g., Finnish type) |
| Primary (Idiopathic) Nephrotic Syndrome | Most common in children (especially MCD) |
| Secondary Nephrotic Syndrome | Occurs due to systemic disease (e.g., diabetes, lupus) |
| Steroid-Responsive Nephrotic Syndrome (SRNS) | Responds well to corticosteroids (mostly in children) |
| Steroid-Resistant Nephrotic Syndrome (SRNS) | Poor response to steroids; may need immunosuppressants |
| Relapsing Nephrotic Syndrome | Repeated episodes after remission |
| Frequent Relapser | More than 2 relapses in 6 months or ≥4 in a year |
🧬 PATHOPHYSIOLOGY OF NEPHROTIC SYNDROME
- Damage to the glomerular basement membrane (especially the podocytes) due to immune complexes, toxins, genetic factors, or systemic diseases.
- This leads to increased permeability of the glomeruli to large plasma proteins (especially albumin).
- Massive proteinuria results — >3.5 g/day.
- Loss of albumin causes:
- ↓ Plasma oncotic pressure → fluid shifts to interstitial space → edema
- Hypoalbuminemia triggers hepatic lipoprotein synthesis → hyperlipidemia
- Liver also increases clotting factors → hypercoagulability
- The kidney retains sodium and water in response to low circulating volume → further edema
- Immune defense is weakened due to urinary loss of immunoglobulins and proteins → risk of infection
🔍 SIGNS AND SYMPTOMS
| System | Clinical Manifestations |
|---|---|
| 💧 Fluid Balance | – Generalized edema (anasarca) |
- Periorbital puffiness (first sign)
- Ascites, pleural effusion, weight gain | | 🧪 Urinary Changes | – Frothy urine
- Massive proteinuria
- Decreased urine output (oliguria) | | 🩺 Cardiovascular | – Hypertension (not always present)
- Tachycardia in hypovolemia | | 🧫 Metabolic | – Hyperlipidemia → xanthelasma (fat deposits on eyelids) | | 🔥 Immune System | – Increased risk of infections (cellulitis, peritonitis) | | 🧱 Clotting System | – Increased risk of thrombosis (renal vein thrombosis, DVT) | | 🥱 General | – Fatigue
- Irritability (esp. in children)
- Loss of appetite
✨ Classic Triad of Nephrotic Syndrome:
✔ Massive proteinuria
✔ Hypoalbuminemia
✔ Generalized edema
🧪 DIAGNOSIS OF NEPHROTIC SYNDROME
✅ 1. Urine Tests
| Test | Findings |
|---|---|
| Urinalysis (R/M) | Massive proteinuria, lipiduria, fatty casts (“Maltese cross” under microscope) |
| 24-Hour Urine Protein | >3.5 g/day confirms nephrotic-range proteinuria |
| Urine Albumin-to-Creatinine Ratio (ACR) | Elevated levels indicate protein loss |
✅ 2. Blood Tests
| Test | Findings |
|---|---|
| Serum Albumin | Low (<3.0 g/dL) – due to protein loss |
| Serum Cholesterol, Triglycerides | Elevated – due to liver compensation |
| BUN, Creatinine | May be elevated in renal impairment |
| Electrolytes | Na⁺ may be low due to dilution; K⁺ usually normal |
| CBC | May show anemia or leukocytosis (if infection present) |
| Clotting Profile | Altered – risk of thrombosis |
✅ 3. Imaging
- Renal ultrasound – shows enlarged kidneys in some types
- Doppler ultrasound – to rule out renal vein thrombosis in complicated cases
✅ 4. Special Tests
- Renal Biopsy – gold standard to identify specific glomerular pathology (e.g., MCD, FSGS, membranous nephropathy)
- Autoimmune Screening – ANA, dsDNA, complement levels (if lupus suspected)
- Viral Markers – for HBV, HCV, HIV (in secondary nephrotic syndrome)
💊 I. MEDICAL MANAGEMENT
🎯 Goals: Control proteinuria, reduce edema, treat underlying cause, prevent complications.
✅ 1. Corticosteroids
- Prednisolone is the drug of choice in Minimal Change Disease (MCD) (especially in children)
- Dose and duration:
- Initial dose: 2 mg/kg/day (children), taper based on response
- 80–90% of children respond within 4–6 weeks
- Monitor for side effects: weight gain, hyperglycemia, growth retardation, infections
✅ 2. Immunosuppressive Agents (used when steroid-resistant or dependent)
- Cyclophosphamide – used in frequently relapsing nephrotic syndrome
- Calcineurin inhibitors (e.g., Cyclosporine, Tacrolimus) – effective in FSGS
- Mycophenolate mofetil (MMF) – alternative to cyclophosphamide in some cases
- Rituximab – in resistant or frequently relapsing cases
✅ 3. Diuretics
- To reduce edema and fluid overload
- Commonly used:
- Furosemide (Lasix)
- Spironolactone (potassium-sparing)
- Monitor for electrolyte imbalance (especially K⁺)
✅ 4. Antihypertensive Drugs
- Used to control blood pressure and reduce proteinuria
- Preferred drugs:
- ACE inhibitors (e.g., Enalapril, Lisinopril)
- ARBs (e.g., Losartan)
- These also reduce intraglomerular pressure
✅ 5. Albumin Infusion + Diuretic
- In cases of severe hypoalbuminemia with edema
- Administer IV albumin + furosemide to mobilize fluid
- Monitor for signs of fluid overload (e.g., pulmonary edema)
✅ 6. Lipid-Lowering Agents
- For hyperlipidemia associated with nephrotic syndrome
- Use statins (e.g., Atorvastatin), especially in adults
✅ 7. Anticoagulation (if needed)
- In high-risk patients (e.g., with renal vein thrombosis, DVT, severe hypoalbuminemia)
- Use Heparin, followed by Warfarin
✅ 8. Antibiotics / Vaccinations
- Treat infections early due to low immunity
- Vaccination against:
- Pneumococcus
- Influenza
- Hepatitis B
- Avoid live vaccines while on immunosuppressants
🔪 II. SURGICAL MANAGEMENT
✳️ Surgery is rare and not a first-line treatment. It is considered only in specific complications.
✅ Indications for Surgical Intervention
| Indication | Surgical Procedure |
|---|---|
| Renal vein thrombosis | Thrombectomy or vascular intervention |
| End-stage renal disease (ESRD) | Kidney transplantation |
| Severe ascites or pleural effusion not responding to medical therapy | Paracentesis or thoracentesis (drainage procedures) |
| Biopsy requirement | Renal biopsy (diagnostic, not therapeutic) |
⚠️ Kidney Transplantation
- Reserved for end-stage renal failure caused by progressive nephrotic syndrome (esp. FSGS)
- Lifelong immunosuppression required post-transplant
📌 Summary Table
| Management Component | Purpose |
|---|---|
| Steroids | Control inflammation, reduce proteinuria |
| Immunosuppressants | For steroid-resistant or frequent relapsers |
| Diuretics | Control edema |
| ACEi/ARBs | Lower BP and reduce protein loss |
| Albumin infusion | Temporarily correct hypoalbuminemia |
| Statins | Treat hyperlipidemia |
| Anticoagulants | Prevent/treat thrombosis |
| Vaccines/Antibiotics | Infection prevention and control |
| Surgery/Transplant | For rare complications or ESRD |
👩⚕️ NURSING MANAGEMENT OF NEPHROTIC SYNDROME
🧠 I. Nursing Assessment
✅ Subjective Data
- Complaints of:
- Swelling of face, feet, or abdomen
- Frothy urine
- Fatigue or weakness
- Decreased urine output
- Loss of appetite or irritability (esp. in children)
✅ Objective Data
- Periorbital and pedal edema
- Frothy urine on observation
- BP may be mildly elevated
- Weight gain due to fluid retention
- Lab reports showing:
- ↓ Serum albumin
- ↑ Proteinuria
- ↑ Serum cholesterol/triglycerides
🎯 II. Nursing Diagnoses
- 💦 Excess fluid volume related to altered kidney function
- 🍽️ Imbalanced nutrition: less than body requirements related to anorexia, protein loss
- 🧴 Risk for infection related to immunosuppression and protein loss
- 🧠 Activity intolerance related to fatigue and edema
- 📚 Deficient knowledge related to disease condition, medications, and prevention of relapse
- 😰 Body image disturbance (especially in children/adolescents) due to facial swelling and weight gain
📝 III. Nursing Goals / Planning
✅ Reduce edema and maintain fluid balance
✅ Prevent complications such as infections and thrombosis
✅ Ensure adequate nutritional intake
✅ Promote normal activity as tolerated
✅ Educate patient/family for long-term management
✅ Provide emotional support
🩺 IV. Nursing Interventions
🔹 1. Monitor Fluid Balance
- 📋 Record accurate intake and output (I/O)
- ⚖️ Daily weight measurement (same time, same scale)
- 💧 Monitor urine color, volume, and consistency
- ⛔ Administer diuretics as prescribed and observe response
- 🛏️ Position the patient in semi-Fowler’s with elevated limbs to reduce edema
🔹 2. Edema and Skin Care
- 🌬️ Turn and reposition the patient every 2 hours
- 🧼 Provide gentle skin care to prevent skin breakdown
- 🧦 Use soft, non-restrictive clothing
- 🛌 Avoid prolonged sitting/standing in one position
🔹 3. Infection Prevention
- 🧼 Practice and teach hand hygiene
- 🧫 Monitor temperature and signs of infection (respiratory, peritoneal, skin)
- 💉 Ensure vaccinations are updated (e.g., pneumococcal, flu)
- 🛑 Restrict visitors during immunosuppressive therapy
- 📋 Monitor WBC count and educate on infection risks
🔹 4. Nutritional Support
- 🍲 Encourage a low-sodium, moderate-protein diet (as per doctor’s advice)
- 🥛 Encourage small, frequent, high-calorie meals
- 💊 Administer vitamin and mineral supplements as prescribed
- 🍉 Ensure adequate hydration unless restricted
🔹 5. Emotional and Psychological Support
- 🧠 Explain the disease process and reassure recovery
- 🎓 Involve family in care, especially for pediatric cases
- 💬 Address body image concerns, particularly in adolescents
- 🤝 Refer for psychological counseling if needed
🔹 6. Medication Education
- 📅 Teach proper use of corticosteroids and side effects
- ⚠️ Warn about immunosuppressant precautions
- 🛡️ Educate on avoiding abrupt withdrawal of steroids
- 🚫 Teach the importance of avoiding NSAIDs and nephrotoxic drugs
📊 V. Evaluation Criteria
| Goal | Expected Outcome |
|---|---|
| Fluid balance maintained | Edema reduced, normal I/O, weight stabilized |
| Infection prevented | Afebrile, no signs of new infection |
| Adequate nutrition | Maintains appetite and dietary intake |
| Understanding improved | Patient/family verbalizes knowledge of care |
| Activity tolerance improved | Participates in mild activities without fatigue |
📌 KEY NURSING POINTS
✔ Close monitoring of fluid status is crucial
✔ Prevent infections – major risk due to protein loss and immunosuppression
✔ Promote nutritional recovery and medication compliance
✔ Address emotional and psychological needs, especially in children
✔ Educate family about early signs of relapse (swelling, frothy urine)
✔ Encourage follow-up and long-term lifestyle adjustments;
🥗 NUTRITIONAL CONSIDERATION IN NEPHROTIC SYNDROME
Proper nutrition helps: ✔ Manage edema
✔ Prevent nutritional deficiencies
✔ Support immune function
✔ Minimize renal damage progression
✅ Recommended Diet
| Component | Advice |
|---|---|
| 💦 Fluids | Moderate to restricted intake if oliguria or severe edema present |
| 🧂 Sodium | Strict sodium restriction (1–2 g/day) to manage edema and hypertension |
| 🥩 Protein | Moderate protein intake (0.8–1 g/kg/day) |
| → high-protein diet is not advised unless protein loss is excessive and renal function is stable | |
| 🍚 Calories | Adequate calorie intake to prevent protein breakdown (use carbs and fats) |
| 🍌 Potassium | Monitor serum levels – restrict if hyperkalemia develops (especially with diuretics) |
| 🥛 Phosphorus | May need restriction in prolonged or chronic cases |
| 🍓 Vitamins & Minerals | Supplement B-complex, iron, and zinc if anemia or poor intake |
| 🍱 Meals | Small, frequent meals with soft, bland, easily digestible food recommended during edema or fatigue phases |
❌ Avoid:
- 🧂 Pickled, canned, and processed foods
- 🧀 High-fat dairy (if lipid levels are high)
- 🍔 Junk food high in salt and cholesterol
- 🍫 Excessive chocolate, nuts (high potassium/phosphorus)
- 🍺 Alcohol and caffeine
⚠️ COMPLICATIONS OF NEPHROTIC SYNDROME
If untreated or poorly managed, nephrotic syndrome can lead to serious complications:
| Category | Complications |
|---|---|
| 💉 Hematologic | – Thrombosis (renal vein thrombosis, DVT, PE) |
- Hypercoagulability due to increased clotting factors | | 🧫 Infectious | – Increased susceptibility to infection (e.g., peritonitis, cellulitis, pneumonia)
→ due to loss of immunoglobulins | | 💧 Fluid/Electrolyte Imbalance | – Severe edema, ascites, pleural effusion - Hypovolemia (despite edema) | | 🩺 Renal | – Acute kidney injury (AKI)
- Chronic kidney disease (CKD)
- End-stage renal disease (ESRD) in progressive cases | | 🍳 Metabolic | – Hyperlipidemia → early atherosclerosis
- Malnutrition from protein and calorie loss | | 🧠 Psychological | – Depression, body image issues, especially in children/adolescents
📌 KEY POINTS TO REMEMBER – NEPHROTIC SYNDROME
✔ Characterized by:
🔹 Massive proteinuria
🔹 Hypoalbuminemia
🔹 Generalized edema
🔹 Hyperlipidemia
✔ Common in children – most often due to Minimal Change Disease (MCD)
✔ Managed with:
🔸 Corticosteroids (first-line)
🔸 Immunosuppressants if steroid-resistant
🔸 Diuretics and ACE inhibitors to control edema and proteinuria
🔸 Statins for lipid control
🔸 Antibiotics/Vaccines to prevent infection
✔ Nursing care focuses on:
✅ Monitoring fluid balance
✅ Preventing infection
✅ Ensuring nutritional support
✅ Educating patient/family on early relapse signs
✔ Complications include:
🔺 Thrombosis
🔺 Infections
🔺 Renal failure
🔺 Growth retardation in children (with long-term steroid use)
✔ Lifelong follow-up may be necessary in relapsing or chronic cases.
🪨 RENAL CALCULI
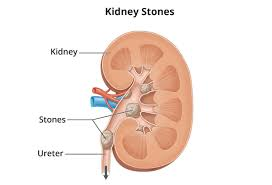
(Kidney Stones / Nephrolithiasis / Urolithiasis)
📖 DEFINITION
Renal calculi are hard, crystalline mineral and salt deposits that form inside the kidneys or anywhere along the urinary tract (ureters, bladder, urethra).
They develop when urine becomes concentrated, allowing minerals to crystallize and stick together, forming stones of varying size and composition.
🔍 CAUSES / RISK FACTORS
Renal calculi form due to multiple contributing factors:
✅ 1. Metabolic Factors
- Hypercalciuria – high calcium in urine
- Hyperoxaluria – high oxalate in urine
- Hyperuricosuria – excess uric acid
- Cystinuria – genetic defect in amino acid metabolism
- Low citrate levels – citrate inhibits stone formation
✅ 2. Dehydration / Low Fluid Intake
- Concentrated urine promotes crystal formation
✅ 3. Dietary Factors
- High intake of:
- Sodium
- Animal protein
- Oxalate-rich foods (e.g., spinach, nuts, chocolate)
- Sugary drinks
- Low intake of:
- Water
- Calcium (counterintuitive: low calcium increases oxalate absorption)
✅ 4. Urinary Tract Infections (UTIs)
- Especially with urease-producing bacteria (e.g., Proteus, Klebsiella) → promote struvite stones
✅ 5. Obstruction or Stasis of Urine
- e.g., Enlarged prostate, congenital abnormalities
✅ 6. Medical Conditions
- Gout
- Hyperparathyroidism
- Renal tubular acidosis
- Inflammatory bowel disease
- Bariatric surgery (malabsorption increases oxalate)
✅ 7. Genetic / Family History
- Higher risk if first-degree relatives have had stones
📊 TYPES OF RENAL CALCULI
| Type | Description | Common Causes |
|---|---|---|
| 🟡 Calcium Oxalate Stones | Most common (~70–80%) | High oxalate, low fluid, low citrate |
| ⚪ Calcium Phosphate Stones | Can occur alone or with oxalate | High urine pH, hyperparathyroidism |
| ⚙️ Struvite Stones (Infection stones) | Made of magnesium ammonium phosphate | Recurrent UTIs with urease-producing bacteria |
| 🔴 Uric Acid Stones | Radiolucent on X-ray | Acidic urine, gout, high purine diet |
| 🧬 Cystine Stones | Rare, genetic condition (cystinuria) | Inherited metabolic disorder of amino acids |
🧪 Note: Some patients may form mixed-type stones
🧬 PATHOPHYSIOLOGY OF RENAL CALCULI
- Supersaturation of urine: When the concentration of crystal-forming substances (e.g., calcium, oxalate, uric acid) exceeds their solubility in urine.
- Nucleation: These substances begin to precipitate and form tiny crystals.
- Crystal growth and aggregation: Crystals grow and join together, forming a larger mass (stone).
- Impaired inhibitors: Normally, substances like citrate and magnesium prevent stone formation. When these are low, stones form more easily.
- Adherence to urothelium: Crystals stick to the renal papilla or tubular epithelium, forming nidus.
- Obstruction & irritation: Stones may remain silent or migrate into the ureter, causing obstruction, stretching, and colicky pain. This may also lead to hydronephrosis and secondary infection.
🚨 SIGNS & SYMPTOMS OF RENAL CALCULI
Symptoms vary depending on size, location, and mobility of the stone:
🔹 Renal Pelvis (Non-obstructive)
- May be asymptomatic
- Dull flank pain
- Microscopic hematuria
🔹 Ureter (Obstructive)
- Renal colic (sudden, severe, crampy flank pain radiating to groin/genitals)
- Hematuria – gross or microscopic
- Nausea and vomiting – due to severe pain
- Urgency/frequency – especially if stone is in lower ureter or near bladder
- Painful urination (dysuria) – with lower tract involvement
- Fever/chills – if complicated by infection (urgent condition)
🧪 DIAGNOSIS OF RENAL CALCULI
✅ 1. Urine Tests
| Test | Purpose |
|---|---|
| Urinalysis (R/M) | Hematuria, crystals, WBCs (if infection), pH levels |
| 24-Hour Urine Collection | Measures calcium, oxalate, citrate, uric acid |
| Urine Culture | Rule out infection (struvite stones) |
| Urine pH | Acidic in uric acid stones, alkaline in struvite stones |
✅ 2. Blood Tests
| Test | Purpose |
|---|---|
| Serum Calcium, Phosphate | Detect hyperparathyroidism, hypercalcemia |
| Serum Uric Acid | Elevated in gout or uric acid stones |
| Creatinine, BUN | Assess renal function |
| PTH levels | If hyperparathyroidism suspected |
✅ 3. Imaging Studies
| Imaging | Purpose |
|---|---|
| Non-contrast CT scan (KUB) | Gold standard for detecting stones (including radiolucent uric acid stones) |
| Ultrasound (USG KUB) | Preferred in pregnancy and children; detects hydronephrosis and larger stones |
| X-ray KUB | Detects radiopaque stones (calcium-containing) |
| IVP (Intravenous Pyelogram) | Older test – used for anatomical visualization |
| MRI | Rarely used; not ideal for stone detection |
💊 I. MEDICAL MANAGEMENT
🎯 Goals: Relieve pain, promote stone passage, prevent recurrence, and treat complications like infection or renal failure.
✅ 1. Pain Management (Renal Colic Relief)
- 💉 NSAIDs – Diclofenac, Ketorolac (first-line for renal colic)
- 💊 Opioids – Tramadol, Morphine (for severe or unresponsive pain)
- 🧊 Hydration – IV fluids to support perfusion and flushing
✅ 2. Medical Expulsive Therapy (MET)
- Given to facilitate spontaneous passage of small stones (≤5–10 mm), especially in the ureter:
- Alpha-blockers (e.g., Tamsulosin) – relax ureter smooth muscle
- Calcium channel blockers (e.g., Nifedipine) – reduce ureteric spasm
- Duration: up to 4 weeks with monitoring
✅ 3. Antibiotics
- Used when infection is present (fever, pyuria, positive culture)
- Broad-spectrum IV antibiotics initially, e.g., Ceftriaxone, Piperacillin-Tazobactam
✅ 4. Hydration Therapy
- Encourage high fluid intake (2.5–3 liters/day)
- Aims to dilute urine and prevent crystal formation
✅ 5. Dietary and Preventive Therapy
- Based on stone composition:
- Calcium stones: Limit sodium, oxalate-rich foods; maintain normal dietary calcium
- Uric acid stones: Limit purine-rich food (meat, seafood); alkalinize urine with potassium citrate
- Cystine stones: Increase fluid, alkalinize urine
- Struvite stones: Treat underlying UTI aggressively
- Use of Thiazide diuretics (e.g., Hydrochlorothiazide) in recurrent calcium stone formers
- Allopurinol: for hyperuricemia or uric acid stones
🔪 II. SURGICAL MANAGEMENT
🧠 Indicated when stone is too large, impacted, infected, or causing obstruction or renal damage.
✅ 1. Extracorporeal Shock Wave Lithotripsy (ESWL)
- Non-invasive
- Uses ultrasound-guided shock waves to break stones into fragments
- Best for stones <2 cm, located in kidney or upper ureter
- Not suitable for: pregnant women, bleeding disorders, obesity
✅ 2. Ureteroscopy (URS)
- Endoscopic procedure via urethra → bladder → ureter
- Uses laser (Holmium:YAG) to fragment stones
- Suitable for mid to lower ureteral stones
✅ 3. Percutaneous Nephrolithotomy (PCNL)
- Invasive
- Used for large (>2 cm), complex, or staghorn stones
- A small incision is made in the back → nephroscope inserted → stone removed/broken
- Requires anesthesia and post-op monitoring
✅ 4. Open or Laparoscopic Stone Removal (Nephrolithotomy/Ureterolithotomy)
- Rarely used today
- Reserved for anatomic abnormalities, failed other methods, or very large stones
✅ 5. Nephrostomy Tube Placement
- For temporary drainage of obstructed/infected kidney
- Used when infection and hydronephrosis are present
- Inserted under ultrasound/fluoroscopy
🩺 Summary Table
| Procedure | Best For | Notes |
|---|---|---|
| ESWL | Stones <2 cm, renal or upper ureter | Non-invasive, outpatient |
| URS with laser | Mid/lower ureter stones | Endoscopic, effective |
| PCNL | Large or staghorn stones | Invasive, hospital stay |
| Open Surgery | Rare, complex cases | Last resort |
| Nephrostomy | Infection + obstruction | Temporary drainage |
👩⚕️ NURSING MANAGEMENT OF RENAL CALCULI
(Kidney Stones – Nephrolithiasis / Urolithiasis)
🧠 I. Nursing Assessment
✅ Subjective Data
- Patient reports:
- Severe flank pain (radiating to groin or genitalia)
- Nausea, vomiting
- Burning or difficulty urinating
- Sense of urgency and frequency
- History of stone passage or previous renal calculi
✅ Objective Data
- Observed:
- Hematuria (visible or microscopic)
- Restlessness due to colicky pain
- Fever/chills (if infection present)
- Decreased or concentrated urine output
- Lab reports: ↑ BUN/Creatinine, positive urinalysis, imaging evidence of calculi
📝 II. Nursing Diagnoses
- 🔥 Acute pain related to ureteric spasm or stone movement
- 💧 Fluid volume deficit related to vomiting and reduced intake
- 💦 Impaired urinary elimination related to obstruction
- 🦠 Risk for infection related to urinary stasis and obstruction
- 📚 Deficient knowledge regarding dietary modifications, fluid intake, and recurrence prevention
- ⚠️ Anxiety related to pain and diagnostic procedures
🎯 III. Nursing Goals / Expected Outcomes
✅ Relieve pain and discomfort
✅ Maintain adequate fluid balance and urine output
✅ Prevent infection and complications
✅ Educate patient on prevention and lifestyle modifications
✅ Prepare patient for and assist during diagnostic or surgical procedures
🩺 IV. Nursing Interventions
🔹 1. Pain Management
- 💊 Administer prescribed analgesics (NSAIDs or opioids)
- 🛌 Provide rest and a comfortable position (side-lying or fetal)
- ❄️ Apply warm compresses on flank (if ordered)
- 🌡️ Monitor pain intensity and response to treatment
🔹 2. Monitor Urinary Elimination
- 📋 Record intake and output accurately
- 🚽 Encourage frequent voiding to prevent stasis
- 📦 Strain all urine to catch passed stones for analysis
- 📉 Observe for hematuria, oliguria, or signs of obstruction
🔹 3. Hydration and Fluid Balance
- 💧 Encourage 2.5–3 liters/day oral fluids if not contraindicated
- 💉 Administer IV fluids to maintain hydration in vomiting/dehydrated patients
- ⚠️ Monitor for signs of fluid overload (in renal impairment)
🔹 4. Infection Prevention
- 🌡️ Monitor for fever, chills, pyuria, leukocytosis
- 💊 Administer antibiotics if prescribed
- 🧼 Maintain strict perineal hygiene
- 🚫 Avoid unnecessary catheterization
🔹 5. Patient Education
- 📚 Educate on:
- Hydration (importance of 2–3 L/day intake)
- Dietary modifications based on stone type
- Avoiding high-oxalate, high-sodium, and purine-rich foods
- Recognizing early signs of recurrence (flank pain, hematuria)
- 🧪 Teach the purpose of urine straining and stone analysis
🔹 6. Pre- and Post-Procedure Care
- 📋 Prepare patient for diagnostic tests (USG, CT, IVP)
- 🧑⚕️ Assist during ESWL, URS, PCNL as required
- 🛏️ Provide post-op care: pain relief, monitoring for bleeding, infection, or obstruction
- 🚫 Observe for complications like urosepsis or hemorrhage
📊 V. Evaluation Criteria
| Nursing Goal | Expected Outcome |
|---|---|
| Pain control | Patient reports relief within 30–60 mins post-analgesia |
| Fluid balance maintained | Adequate urine output, normal vitals |
| Urinary elimination improved | Clear urine passage, no obstruction |
| Knowledge improved | Patient verbalizes lifestyle changes |
| No infection | Normal temperature, WBCs, no dysuria |
📌 KEY NURSING POINTS
✔ Renal calculi cause acute, severe pain → prioritize analgesia
✔ Encourage fluid intake and urine monitoring
✔ Educate patient on stone type-specific dietary modifications
✔ Prevent complications like obstruction, infection, or renal damage
✔ Support patient pre/post procedure and reduce anxiety through education
🥗 NUTRITIONAL CONSIDERATION IN RENAL CALCULI
Diet plays a crucial role in the prevention of stone recurrence and managing metabolic risk factors.
✅ General Dietary Guidelines:
- 💧 Increase fluid intake: 2.5–3 liters/day (unless contraindicated)
→ Dilutes urine and prevents stone formation - 🧂 Restrict sodium intake: High salt increases calcium excretion
- 🍽️ Eat regular meals: Avoid starvation or dehydration
🍋 Stone Type-Specific Dietary Recommendations:
| Stone Type | Dietary Modifications |
|---|---|
| Calcium Oxalate | ↓ Oxalate-rich foods (spinach, beets, nuts, chocolate) |
| Maintain normal calcium intake (not excessive) | |
| ↓ Sodium and animal protein | |
| Calcium Phosphate | ↓ Sodium and animal protein |
| Avoid excessive dairy (too much phosphate) | |
| Maintain moderate calcium | |
| Uric Acid | ↓ Purine-rich foods (organ meats, red meat, seafood, legumes) |
| Alkalinize urine with potassium citrate, lemon water | |
| Encourage high fluid intake | |
| Struvite (Infection stones) | Prevent UTIs |
| Encourage hygiene and hydration | |
| May need antibiotics | |
| Cystine | High fluid intake (even at night) |
| Alkalinize urine (citrate, lemon juice) | |
| Moderate protein restriction |
⚠️ COMPLICATIONS OF RENAL CALCULI
If left untreated or if recurrent, renal stones may cause:
| Category | Complications |
|---|---|
| 💧 Obstructive | – Hydronephrosis |
- Acute urinary retention
- Renal colic | | 🧫 Infectious | – Recurrent UTIs
- Pyelonephritis
- Urosepsis | | 🧱 Renal Damage | – Acute Kidney Injury (AKI)
- Chronic Kidney Disease (CKD)
- Renal scarring or atrophy | | 🩸 Bleeding | – Hematuria
- Ureteral trauma post-stone passage | | ⚖️ Electrolyte imbalance | – Hypokalemia/hyperkalemia from diuretics or obstruction | | 🧠 Psychosocial | – Anxiety from pain, fear of recurrence
- Disruption of daily activities |
📌 KEY POINTS – RENAL CALCULI
✔ Renal calculi are mineral deposits formed due to supersaturation of urine with crystal-forming substances
✔ Most common types: Calcium oxalate > Uric acid > Struvite > Cystine
✔ Classic symptom: Sudden, severe flank pain radiating to the groin (renal colic)
✔ Diagnosis: Urinalysis, CT KUB (gold standard), ultrasound, X-ray
✔ Treatment includes:
- Pain relief
- Medical expulsive therapy
- ESWL, URS, or PCNL for larger stones
✔ Nursing care focuses on: - Pain management
- Hydration
- Monitoring urine output
- Infection prevention
✔ Diet modification and hydration are key to prevent recurrence
✔ Teach patients to strain urine, identify stone type, and follow up regularly.
🚨 ACUTE RENAL FAILURE (ARF)

(Also called Acute Kidney Injury – AKI)
📖 DEFINITION
Acute Renal Failure (ARF) or Acute Kidney Injury (AKI) is a sudden and rapid decline in kidney function that occurs within hours to days, leading to:
✔ Inability to excrete waste products
✔ Impaired fluid and electrolyte balance
✔ Inability to regulate acid–base balance
✔ Possible oliguria or anuria
🔍 It is reversible if identified and treated early.
🦠 CAUSES OF ACUTE RENAL FAILURE
Causes of ARF are typically classified into three major categories:
✅ 1. Prerenal Causes (Before the kidneys – due to decreased blood flow)
| Cause | Explanation |
|---|---|
| 🚱 Dehydration | Loss of fluid volume (vomiting, diarrhea, bleeding) |
| ❤️ Heart failure / shock | Decreased cardiac output → poor renal perfusion |
| 🩸 Hypovolemia | Hemorrhage, burns |
| 🔁 Renal artery stenosis or thrombosis | Obstruction of renal blood supply |
✅ 2. Intrarenal (Intrinsic) Causes (Damage to kidney tissues)
| Cause | Explanation |
|---|---|
| 🔬 Acute tubular necrosis (ATN) | Ischemia or nephrotoxins damaging renal tubules |
| 💊 Nephrotoxic drugs | Aminoglycosides, NSAIDs, contrast dye |
| 🧫 Infections | Glomerulonephritis, pyelonephritis |
| 🧪 Autoimmune diseases | Lupus nephritis, vasculitis |
✅ 3. Postrenal Causes (Obstruction after the kidneys – affects urine flow)
| Cause | Explanation |
|---|---|
| 🔒 Ureteral obstruction | Kidney stones, blood clots |
| ⛔ Bladder outlet obstruction | Prostatic hypertrophy (BPH), tumors, strictures |
| ⚠️ Urethral obstruction | Trauma, congenital narrowing |
📊 TYPES OF ACUTE RENAL FAILURE / AKI
| Type | Description |
|---|---|
| Oliguric AKI | Urine output <400 mL/day |
| More severe, higher risk of complications | |
| Non-oliguric AKI | Normal urine output but poor filtration |
| Often due to nephrotoxins | |
| Anuric AKI | Urine output <100 mL/day |
| Suggests complete obstruction or severe ischemia | |
| Acute-on-Chronic Renal Failure | Acute worsening of pre-existing chronic kidney disease |
🧬 PATHOPHYSIOLOGY OF ACUTE RENAL FAILURE
- Initial insult (prerenal, intrarenal, or postrenal) causes sudden reduction in renal perfusion or direct damage to kidney tissue.
- ↓ Glomerular filtration rate (GFR) → accumulation of nitrogenous wastes in the blood (azotemia).
- Tubular dysfunction results in:
- Impaired reabsorption and secretion
- Electrolyte imbalances (e.g., ↑ K⁺, ↓ Na⁺)
- Metabolic acidosis due to retained hydrogen ions
- Oliguria or anuria may occur due to poor filtration or obstruction.
- If untreated, can lead to:
- Volume overload
- Uremia
- Multiorgan dysfunction
- Potential progression to chronic kidney disease
🌀 Phases of ARF (AKI)
| Phase | Description |
|---|---|
| 1. Initiation | Time between injury and onset of symptoms |
| 2. Oliguric Phase | Urine output <400 mL/day; BUN/creatinine rise; electrolyte imbalance |
| 3. Diuretic Phase | Gradual return of renal function; urine output increases but may cause dehydration and electrolyte loss |
| 4. Recovery Phase | Gradual normalization of BUN, creatinine, and GFR over weeks to months |
🚨 SIGNS AND SYMPTOMS OF ACUTE RENAL FAILURE
Symptoms may vary depending on the cause, stage, and rate of progression:
🔹 General/Systemic
- 🥱 Fatigue, malaise
- 🤢 Nausea, vomiting
- 😰 Confusion, drowsiness (due to uremia)
- 🥵 Fever (if infection present)
🔹 Renal
- 💦 Oliguria or anuria
- 💧 Fluid overload: edema, ascites, weight gain
- 🩸 Hematuria or proteinuria
- 🚽 Changes in urine color, clarity, volume
🔹 Cardiovascular
- 🧂 Hypertension (volume retention)
- ❤️ Arrhythmias (due to hyperkalemia)
- 🫁 Pulmonary edema (in severe cases)
🔹 Neurological
- 😵 Altered mental status (uremic encephalopathy)
- Muscle twitching or seizures in severe electrolyte imbalance
🧪 DIAGNOSIS OF ACUTE RENAL FAILURE
✅ 1. Blood Tests
| Test | Findings |
|---|---|
| Serum Creatinine | ↑ indicates impaired filtration |
| Blood Urea Nitrogen (BUN) | ↑ due to azotemia |
| Electrolytes | ↑ K⁺, ↓ Na⁺, ↑ phosphate, ↓ calcium |
| Arterial Blood Gas (ABG) | Metabolic acidosis (low pH, low bicarbonate) |
✅ 2. Urine Tests
| Test | Purpose |
|---|---|
| Urinalysis (R/M) | Proteinuria, hematuria, casts (e.g., muddy brown casts in ATN) |
| Urine Output Monitoring | Oliguria <400 mL/day or Anuria <100 mL/day |
| Urine Electrolytes | To differentiate prerenal vs. intrarenal AKI |
✅ 3. Imaging Studies
| Test | Use |
|---|---|
| Ultrasound (KUB) | Detect obstruction, kidney size, hydronephrosis |
| CT Scan | Detailed assessment if ultrasound is inconclusive |
| Doppler studies | Evaluate renal blood flow (renal artery stenosis) |
✅ 4. Additional Tests
- Renal biopsy – if glomerular or autoimmune cause suspected
- ECG – to monitor for arrhythmias from hyperkalemia
- Cultures – if infection is suspected
💊 I. MEDICAL MANAGEMENT
🎯 Goal: Restore renal function, correct fluid/electrolyte imbalance, treat the underlying cause, and prevent complications.
✅ 1. Treat Underlying Cause
| Cause Type | Treatment |
|---|---|
| Prerenal | Restore perfusion: IV fluids for dehydration, vasopressors in shock |
| Intrarenal | Remove nephrotoxins, manage glomerulonephritis or ATN |
| Postrenal | Relieve obstruction (e.g., catheterization, stenting) |
✅ 2. Fluid and Electrolyte Management
- 💧 IV fluids (e.g., isotonic saline) for volume depletion (prerenal AKI)
- 🚫 Fluid restriction in cases of oliguria and volume overload
- ⚖️ Monitor weight, I/O, central venous pressure (CVP)
🔋 Electrolyte Corrections:
| Electrolyte | Management |
|---|---|
| Hyperkalemia | IV calcium gluconate, insulin + glucose, sodium bicarbonate, kayexalate |
| Hyponatremia | Fluid restriction or slow correction with hypertonic saline |
| Metabolic Acidosis | Sodium bicarbonate IV (if severe) |
| Hyperphosphatemia / Hypocalcemia | Phosphate binders, calcium supplementation if needed |
✅ 3. Nutritional Support
- 🍽️ High-calorie, low-protein diet (until dialysis initiated)
- 🚱 Fluid restriction based on urine output + insensible loss
- 🧂 Sodium and potassium restriction in oliguria/hyperkalemia
✅ 4. Diuretics (with caution)
- Used to convert oliguric to non-oliguric AKI
- Drugs: Furosemide, Mannitol
- Monitor for response; discontinue if ineffective
✅ 5. Renal Replacement Therapy (RRT) / Dialysis
Indicated when:
- 📉 Severe uremia (confusion, pericarditis)
- 💦 Fluid overload unresponsive to diuretics
- ⚠️ Life-threatening electrolyte imbalance (e.g., K⁺ > 6.5)
- 🌡️ Severe acidosis (pH <7.1)
- 🧠 Neurological symptoms (seizures, altered sensorium)
🔪 II. SURGICAL MANAGEMENT
Surgical treatment is not first-line but may be necessary in specific causes of AKI, particularly postrenal obstruction or renal artery issues.
✅ Surgical Interventions (Indication-Based)
| Procedure | Indication |
|---|---|
| Urinary catheterization | Immediate relief of bladder outlet obstruction (BPH, neurogenic bladder) |
| Percutaneous Nephrostomy | Relief of upper tract obstruction (e.g., hydronephrosis) |
| Ureteric Stenting | Bypass obstruction due to stones, tumors |
| Surgical Removal of Obstruction | Tumors, strictures, impacted stones |
| Renal artery stenting or bypass | Renal artery stenosis causing prerenal AKI |
| Kidney transplantation (long-term) | For patients progressing to end-stage renal disease (ESRD) post-AKI |
🩺 Summary: Management Priorities
| Priority | Action |
|---|---|
| ⚠️ Life-threatening issues | Dialysis for electrolyte or fluid overload crisis |
| 🧬 Identify cause | Treat reversible causes (shock, obstruction, nephrotoxins) |
| 🔋 Electrolyte balance | Monitor Na⁺, K⁺, Ca²⁺, PO₄³⁻ |
| 💧 Fluid management | Prevent overload or dehydration |
| 🍱 Nutrition | Restrict protein, potassium, sodium as needed |
| 🧪 Monitor labs | Serial BUN, creatinine, ABG, urinalysis |
| ⛑️ Prevent complications | Infection, sepsis, pressure ulcers, bleeding |
👩⚕️ NURSING MANAGEMENT OF ACUTE RENAL FAILURE (ARF) / ACUTE KIDNEY INJURY (AKI)
🧠 I. Nursing Assessment
✅ Subjective Data
- Complaints of:
- Fatigue, dizziness
- Reduced urine output (oliguria/anuria)
- Nausea, headache, confusion
- Shortness of breath or swelling (if fluid overloaded)
✅ Objective Data
- Urine output <400 mL/day
- Weight gain due to fluid retention
- Peripheral or facial edema
- Elevated BP
- Lab findings: ↑ creatinine, BUN, K⁺; ↓ GFR
- Abnormal ECG (from hyperkalemia: peaked T-waves)
📝 II. Common Nursing Diagnoses
- 💧 Fluid volume excess related to decreased renal function
- 🔥 Risk for electrolyte imbalance (e.g., hyperkalemia, hyponatremia)
- 🥱 Fatigue related to anemia and toxin accumulation
- 🧴 Risk for impaired skin integrity due to edema and immobility
- 🦠 Risk for infection related to invasive devices (catheter, IV) or immunosuppression
- 😰 Anxiety related to sudden illness, hospitalization, and possible dialysis
- 📚 Deficient knowledge regarding condition, diet, fluid management
🎯 III. Nursing Goals
✅ Maintain fluid and electrolyte balance
✅ Support kidney function and monitor response
✅ Prevent complications (e.g., infection, skin breakdown, arrhythmias)
✅ Educate patient and family
✅ Promote comfort and emotional support
🩺 IV. Nursing Interventions
🔹 1. Monitor and Maintain Fluid Balance
- 📋 Strict I/O charting – hourly if on IV fluids
- ⚖️ Daily weights – same time and scale each day
- 🛑 Fluid restriction as per doctor’s orders
- 💉 Administer diuretics cautiously if indicated
🔹 2. Electrolyte and Lab Monitoring
- 🧪 Check serum K⁺, Na⁺, Ca²⁺, PO₄³⁻, BUN, creatinine regularly
- ⚠️ Monitor for signs of hyperkalemia: muscle weakness, ECG changes
- 📉 Administer medications like kayexalate, calcium gluconate, or insulin with glucose as prescribed for high K⁺
🔹 3. Prevent Infection
- 🧼 Practice and teach strict hand hygiene
- 🌡️ Monitor for signs of infection (fever, WBC count)
- 🧫 Maintain aseptic technique with catheters, IV lines, or during dialysis
- 💊 Administer antibiotics as ordered
🔹 4. Skin and Pressure Area Care
- 🛌 Turn and reposition patient every 2 hours
- 🧴 Keep skin clean and dry
- 🧦 Use pressure-relieving devices (mattress, cushions)
- Monitor for signs of uremic frost or itching in uremia
🔹 5. Diet and Nutrition Education
- 🚱 Enforce fluid restriction if ordered
- 🍲 Encourage low-protein, low-potassium, low-sodium diet
- 🥗 Provide small, frequent meals to reduce nausea
- Collaborate with a dietitian if needed
🔹 6. Emotional and Psychological Support
- 🗣️ Provide reassurance and explain treatments in simple terms
- 👨👩👧 Include family in education and care plan
- ☎️ Refer to social worker or counselor if chronic dialysis or transplant is anticipated
📊 V. Evaluation Criteria
| Nursing Goal | Expected Outcome |
|---|---|
| Fluid balance maintained | Stable weight, normal BP, no edema |
| Electrolyte levels normalized | Serum values within normal range |
| No infection | Afebrile, clean catheter sites, stable WBC |
| Skin remains intact | No pressure sores or rashes |
| Patient understands condition | Explains diet/fluid restrictions and follow-up plan |
📌 KEY NURSING POINTS FOR ARF
✔ Monitor urine output hourly in critical cases
✔ Maintain strict fluid and electrolyte monitoring
✔ Prevent complications: hyperkalemia, infection, skin breakdown, pulmonary edema
✔ Educate on dietary changes and fluid restrictions
✔ Provide support for possible dialysis initiation
✔ Identify early signs of deterioration and report promptly..
🥗 NUTRITIONAL CONSIDERATION IN ACUTE RENAL FAILURE (ARF / AKI)
Nutrition plays a vital role in supporting renal recovery, maintaining electrolyte balance, and preventing catabolism.
✅ Goals of Nutrition in ARF:
✔ Provide adequate calories
✔ Prevent protein-energy malnutrition
✔ Control fluid, sodium, potassium, and phosphate intake
✔ Avoid accumulation of nitrogenous waste
🍽️ Dietary Guidelines:
| Nutrient | Considerations |
|---|---|
| 🥩 Protein | – Restrict during oliguric phase: 0.6–0.8 g/kg/day |
- Increase in dialysis phase: up to 1.2–1.5 g/kg/day | | 🔋 Calories | – 30–35 kcal/kg/day from carbohydrates & fats to avoid protein breakdown | | 💧 Fluids | – Restricted to output + 500 mL/day in oliguric patients | | 🧂 Sodium | – Limit to 1–2 g/day to control hypertension and fluid retention | | 🍌 Potassium | – Restrict to 1.5–2 g/day
- Avoid bananas, oranges, tomatoes, potatoes | | 🧀 Phosphorus | – Limit dairy, meat, nuts (if elevated) | | 💊 Vitamins & Minerals | – Supplement water-soluble vitamins (B-complex, C)
- Use phosphate binders if needed |
❌ Avoid:
- High-potassium foods: coconut water, spinach, dry fruits
- High-protein diets (in early phases)
- Processed foods high in sodium and phosphate
- Excess fluid or free water intake
⚠️ COMPLICATIONS OF ACUTE RENAL FAILURE
If not managed promptly, ARF can result in serious, life-threatening complications:
| System | Complications |
|---|---|
| ⚖️ Fluid-Electrolyte | – Hyperkalemia |
- Hyponatremia
- Fluid overload → pulmonary edema, hypertension | | 💉 Metabolic | – Metabolic acidosis
- Uremia → encephalopathy, pericarditis | | 🧠 Neurological | – Confusion, drowsiness, seizures (from toxins or electrolyte imbalance) | | 🫀 Cardiovascular | – Arrhythmias from hyperkalemia
- Heart failure (fluid overload) | | 🧫 Infectious | – Increased risk due to invasive devices, poor immunity | | 🧴 Skin & GI | – Pruritus, uremic frost
- Nausea, vomiting, GI bleeding (uremic gastritis) | | 🧬 Progression to CKD or ESRD | – Especially in prolonged or untreated ARF |
📌 KEY POINTS TO REMEMBER – ACUTE RENAL FAILURE (ARF / AKI)
✔ ARF = sudden loss of kidney function over hours to days
✔ Three types:
- Prerenal – perfusion problem
- Intrarenal – kidney tissue damage
- Postrenal – obstruction
✔ Major clinical signs:
- Oliguria or anuria
- Fluid retention (edema, weight gain)
- Rising BUN, creatinine
- Electrolyte imbalance (↑K⁺, ↓Na⁺, ↓Ca²⁺)
✔ Early diagnosis = better prognosis
- Urinalysis, BUN/Creatinine, electrolyte panels, renal ultrasound/CT
✔ Management includes:
- Fluid and electrolyte control
- Remove underlying cause
- Dialysis if indicated
✔ Nursing priorities:
- Monitor I/O, weight, BP, ECG
- Prevent complications
- Support nutrition
- Educate patient and family
✔ Diet: Fluid-restricted, low protein (unless on dialysis), low sodium/potassium
✔ Early treatment may reverse ARF, but delayed care may progress to chronic kidney disease (CKD) or end-stage renal disease (ESRD)..
🧠 CHRONIC RENAL FAILURE (CRF)
(Also called Chronic Kidney Disease – CKD)
📖 DEFINITION
Chronic Renal Failure (CRF) or Chronic Kidney Disease (CKD) is a progressive, irreversible loss of kidney function that occurs over months to years. It leads to the accumulation of metabolic waste products, disturbances in fluid and electrolyte balance, acid-base imbalance, and hormonal dysregulation (e.g., erythropoietin, vitamin D).
🧪 Defined as:
- GFR <60 mL/min/1.73 m² for ≥3 months, with or without kidney damage
OR - Evidence of kidney damage (e.g., albuminuria, structural abnormality) for ≥3 months
🦠 CAUSES OF CHRONIC RENAL FAILURE
✅ 1. Diabetic Nephropathy
- Most common cause
- Chronic hyperglycemia → glomerular damage → proteinuria → nephron loss
✅ 2. Hypertensive Nephrosclerosis
- Long-standing uncontrolled hypertension → arteriosclerosis of renal arterioles
✅ 3. Glomerulonephritis
- Repeated or chronic glomerular inflammation → scarring and nephron destruction
✅ 4. Polycystic Kidney Disease (PKD)
- Genetic disorder leading to cyst formation and renal tissue destruction
✅ 5. Chronic Pyelonephritis or Reflux Nephropathy
- Recurrent infections or vesicoureteral reflux → renal scarring
✅ 6. Obstructive Uropathy
- Prolonged obstruction (e.g., kidney stones, BPH, tumors) → back pressure and damage
✅ 7. Autoimmune Diseases
- Lupus nephritis, vasculitis
✅ 8. Drug-Induced Nephrotoxicity
- Long-term use of NSAIDs, aminoglycosides, contrast dyes
✅ 9. Other Causes
- HIV nephropathy
- Amyloidosis
- Chronic interstitial nephritis
- Congenital anomalies
📊 TYPES / STAGES OF CHRONIC RENAL FAILURE (CKD)
CKD is classified into 5 stages based on glomerular filtration rate (GFR):
| Stage | Description | GFR (mL/min/1.73 m²) |
|---|---|---|
| Stage 1 | Kidney damage with normal or ↑ GFR | ≥90 |
| Stage 2 | Mild ↓ in GFR | 60–89 |
| Stage 3a | Mild-moderate ↓ | 45–59 |
| Stage 3b | Moderate-severe ↓ | 30–44 |
| Stage 4 | Severe ↓ in GFR | 15–29 |
| Stage 5 (ESRD) | Kidney failure, dialysis needed | <15 |
🛑 Stage 5 CKD = End-Stage Renal Disease (ESRD)
➡ Patient usually requires dialysis or renal transplantation
🧬 PATHOPHYSIOLOGY OF CHRONIC RENAL FAILURE
- Initial kidney damage (from diabetes, hypertension, glomerulonephritis, etc.) leads to loss of functioning nephrons.
- Remaining nephrons hyperfunction to compensate → glomerular hyperfiltration.
- Over time, this causes increased intraglomerular pressure and progressive glomerulosclerosis.
- Leads to:
- ↓ GFR
- ↓ Ability to excrete nitrogenous waste → azotemia & uremia
- ↓ Excretion of sodium and water → volume overload & hypertension
- ↓ Potassium excretion → hyperkalemia
- ↓ Phosphate excretion + ↓ vitamin D activation → hypocalcemia & renal osteodystrophy
- ↓ Erythropoietin production → anemia
- Eventually leads to end-stage renal disease (ESRD) if untreated.
🚨 SIGNS & SYMPTOMS OF CHRONIC RENAL FAILURE
Symptoms develop gradually and worsen as GFR declines.
🔹 General
- 🥱 Fatigue, weakness, lethargy
- 😵 Headache, drowsiness
- 🤢 Nausea, vomiting, metallic taste
- 👄 Uremic fetor (ammonia odor in breath)
- 🧊 Intolerance to cold
🔹 Renal/Urinary
- 💧 Oliguria or polyuria (early) → oliguria (later)
- 🩸 Hematuria or proteinuria
- ⚖️ Nocturia
🔹 Cardiovascular
- 🧂 Hypertension
- 🫀 Heart failure, pericarditis
- 🫁 Pulmonary edema (in advanced stages)
🔹 Gastrointestinal
- ⚡ Nausea, anorexia, weight loss
- 💨 Constipation or diarrhea
- 🩸 GI bleeding (uremic gastritis)
🔹 Musculoskeletal
- 🦴 Bone pain, fractures (renal osteodystrophy)
- 🌙 Muscle cramps
🔹 Neurological
- 💭 Confusion, poor concentration
- 🧠 Seizures, tremors (late uremia)
- 🔥 Peripheral neuropathy (burning, numbness)
🔹 Integumentary
- 🧴 Dry, itchy skin (uremic pruritus)
- ❄️ Pallor (anemia), yellow-gray skin tone
- ❄️ Uremic frost (late-stage crystal deposition on skin)
🔹 Hematologic
- 🩸 Anemia (normocytic, normochromic)
- 🧫 Increased infection risk
- 🩹 Increased bleeding tendency (platelet dysfunction)
🧪 DIAGNOSIS OF CHRONIC RENAL FAILURE
✅ 1. Blood Tests
| Test | Finding |
|---|---|
| Serum Creatinine | ↑ (late indicator) |
| BUN (Blood Urea Nitrogen) | ↑ |
| GFR (Glomerular Filtration Rate) | ↓ — calculated using eGFR formulas (MDRD or CKD-EPI) |
| Electrolytes | ↑ K⁺, ↑ PO₄³⁻, ↓ Ca²⁺, metabolic acidosis |
| Hemoglobin (Hb) | ↓ (anemia of chronic disease) |
| Parathyroid Hormone (PTH) | ↑ due to secondary hyperparathyroidism |
| Vitamin D | ↓ (due to reduced activation in kidneys) |
✅ 2. Urine Tests
| Test | Finding |
|---|---|
| Urinalysis | Proteinuria, hematuria, casts |
| 24-hour urine protein | Measures protein loss (>150 mg/day = abnormal) |
| Urine albumin-to-creatinine ratio (ACR) | Detects microalbuminuria (early CKD) |
✅ 3. Imaging Studies
- Renal Ultrasound (KUB): Small, shrunken kidneys in chronic cases
- CT Scan / MRI: To detect structural anomalies or obstructions
- Renal Doppler: If vascular cause suspected
✅ 4. Renal Biopsy
- Indicated if diagnosis is unclear or to assess type/severity of glomerular disease (especially in young or non-diabetic patients)
💊 I. MEDICAL MANAGEMENT
🎯 Goals: Slow disease progression, manage symptoms, prevent complications, and prepare for renal replacement therapy (RRT) if needed.
✅ 1. Control of Underlying Cause
- Diabetes control:
- HbA1c <7%
- Use insulin or oral hypoglycemics (e.g., glipizide — safer in CKD)
- Hypertension management:
- Target BP <130/80 mmHg
- Use ACE inhibitors (e.g., Enalapril) or ARBs (e.g., Losartan) to reduce proteinuria and preserve GFR
✅ 2. Anemia Management
- 🧪 Monitor hemoglobin regularly (target Hb: 10–11.5 g/dL)
- Administer:
- Erythropoietin-stimulating agents (ESAs) – e.g., Epoetin alfa
- Iron supplements – oral or IV (e.g., ferrous sulfate, iron sucrose)
- Folic acid and Vitamin B12 if deficient
✅ 3. Electrolyte and Bone Metabolism Control
| Problem | Management |
|---|---|
| Hyperphosphatemia | Phosphate binders – calcium carbonate, sevelamer |
| Hypocalcemia | Calcium supplements, active vitamin D (calcitriol) |
| Secondary hyperparathyroidism | Vitamin D analogs, calcimimetics (cinacalcet) |
| Metabolic acidosis | Oral sodium bicarbonate to maintain serum HCO₃ >22 mmol/L |
✅ 4. Fluid and Electrolyte Balance
- 🧂 Sodium and fluid restriction in edema or hypertension
- 🍌 Potassium restriction if hyperkalemia present
- 💉 Diuretics (loop diuretics like furosemide) if fluid overloaded
✅ 5. Proteinuria Control
- Use ACE inhibitors or ARBs to reduce intraglomerular pressure
- Encourage dietary protein moderation based on GFR
✅ 6. Management of Dyslipidemia
- Statins (e.g., Atorvastatin) to lower LDL and reduce cardiovascular risk
✅ 7. Infection Prevention
- Annual influenza vaccine
- Pneumococcal vaccine
- Hepatitis B vaccine (especially before starting dialysis)
✅ 8. Patient Education
- Disease progression awareness
- Diet, fluid restrictions
- Medication adherence
- Signs of complications or when to seek help
🔪 II. SURGICAL MANAGEMENT
Surgery is not routine for CKD itself, but may be necessary for:
✅ 1. Arteriovenous (AV) Fistula or Graft Creation
- Required for hemodialysis access
- Done well before dialysis initiation (GFR <15 or symptomatic)
✅ 2. Peritoneal Dialysis Catheter Insertion
- For patients opting for Continuous Ambulatory Peritoneal Dialysis (CAPD)
- Surgically placed into the peritoneal cavity
✅ 3. Kidney Transplantation
- Indicated in End-Stage Renal Disease (ESRD)
- Preferred over lifelong dialysis in eligible patients
- Requires pre-transplant workup and lifelong immunosuppressive therapy (e.g., tacrolimus, mycophenolate, steroids)
✅ 4. Surgical Management of Complications
| Complication | Surgery |
|---|---|
| Obstructive uropathy | Relief via stent, nephrostomy, or surgery |
| Polycystic kidney | Nephrectomy in symptomatic cases |
| Parathyroid hyperplasia | Parathyroidectomy in resistant secondary hyperparathyroidism |
📌 KEY GOALS OF MANAGEMENT
✔ Delay disease progression
✔ Treat reversible causes (e.g., infections, obstruction)
✔ Control complications (anemia, bone disease, hyperkalemia)
✔ Prepare for and initiate renal replacement therapy when needed
👩⚕️ NURSING MANAGEMENT OF CHRONIC RENAL FAILURE (CRF) / CKD
🧠 I. Nursing Assessment
✅ Subjective Data
- Fatigue, weakness
- Nausea, poor appetite
- Muscle cramps or itching
- Changes in urination (polyuria, nocturia, or oliguria)
- Shortness of breath
✅ Objective Data
- Edema (facial, pedal, periorbital)
- High blood pressure
- Pale, dry, itchy skin
- Confusion or altered sensorium
- Abnormal lab values (↑BUN, creatinine, ↓Hb, ↑K⁺, ↓Ca²⁺)
📝 II. Nursing Diagnoses
- 💧 Excess fluid volume related to impaired renal excretion
- 🩸 Imbalanced nutrition: less than body requirements related to anorexia and dietary restrictions
- ⚡ Risk for electrolyte imbalance (hyperkalemia, hypocalcemia)
- 🧠 Activity intolerance related to fatigue, anemia, and toxin accumulation
- 🧴 Risk for impaired skin integrity due to uremic pruritus and edema
- 😰 Anxiety related to disease progression and dialysis dependency
- 📚 Deficient knowledge related to disease process, medications, diet, and self-care
🎯 III. Nursing Goals
✅ Maintain fluid and electrolyte balance
✅ Prevent complications (infection, skin breakdown, hyperkalemia)
✅ Promote adequate nutrition and energy
✅ Enhance knowledge about disease and management
✅ Provide emotional and psychosocial support
🩺 IV. Nursing Interventions
🔹 1. Monitor and Manage Fluid Balance
- 📋 Monitor intake and output (I/O) strictly
- ⚖️ Record daily weight
- 🛑 Enforce fluid restriction as prescribed
- 🧂 Limit sodium to control BP and fluid retention
- 💧 Assess for signs of fluid overload: crackles, dyspnea, edema
🔹 2. Monitor Electrolyte and Lab Values
- 🧪 Monitor:
- Serum potassium, sodium, calcium, phosphate
- BUN, creatinine
- Hemoglobin levels
- ⚠️ Observe for signs of:
- Hyperkalemia: muscle weakness, ECG changes
- Hypocalcemia: tetany, numbness
- Uremia: drowsiness, confusion
🔹 3. Provide Nutritional Support
- 🍲 Encourage low-protein, low-sodium, low-potassium, low-phosphorus diet
- 🚱 Limit fluid intake as prescribed
- 💊 Administer vitamins and phosphate binders as ordered
- 🥣 Collaborate with a dietitian
🔹 4. Skin Care and Comfort
- 🧼 Provide gentle skin care with emollients for dryness/itching
- 🔁 Reposition patient frequently to prevent pressure ulcers
- ❄️ Use cool compresses or prescribed medications for uremic pruritus
🔹 5. Manage Anemia and Fatigue
- 💉 Administer erythropoietin and iron supplements as prescribed
- 🛌 Encourage rest periods between activities
- 👨⚕️ Monitor for signs of severe anemia or dyspnea
🔹 6. Educate Patient and Family
- 📚 Teach about:
- Importance of medication adherence
- Dietary restrictions
- Fluid control
- Signs of complications (e.g., hyperkalemia, infection)
- ⏰ Stress the need for regular follow-up and lab monitoring
🔹 7. Psychosocial and Emotional Support
- 🧠 Provide reassurance regarding treatment options
- 🗣️ Allow the patient to express fears about dialysis or transplant
- 👨👩👧 Include family in decision-making
- ☎️ Refer for counseling or social work as needed
📊 V. Evaluation Criteria
| Goal | Expected Outcome |
|---|---|
| Fluid balance | Stable weight, no edema or pulmonary symptoms |
| Electrolytes | Serum values within normal limits |
| Nutrition | Maintains adequate dietary intake and albumin levels |
| Skin integrity | No rashes or breakdown |
| Anemia control | Hemoglobin maintained at target level |
| Knowledge | Patient verbalizes understanding of disease and care plan |
| Psychosocial support | Expresses reduced anxiety and increased coping ability |
📌 KEY NURSING TAKEAWAYS FOR CRF/CKD
✔ Monitor fluid and electrolyte status continuously
✔ Prevent complications like hyperkalemia, infections, anemia
✔ Promote adherence to renal diet and medication schedule
✔ Provide education on disease progression, dialysis, and transplant
✔ Offer emotional and psychosocial support to the patient and family
✔ Collaborate with a multidisciplinary team for optimal care..
🥗 NUTRITIONAL CONSIDERATION IN CHRONIC RENAL FAILURE (CRF / CKD)
Nutrition in CRF aims to prevent uremia, delay disease progression, and reduce metabolic complications.
✅ General Goals:
✔ Maintain nutritional status
✔ Prevent electrolyte imbalances
✔ Reduce nitrogenous waste
✔ Control fluid overload and hypertension
✔ Minimize complications like hyperkalemia, hyperphosphatemia
🍽️ Dietary Guidelines by Stage (Non-dialysis patients)
| Nutrient | Recommendations |
|---|---|
| 🥩 Protein | – Moderate intake: 0.6–0.8 g/kg/day (to reduce urea buildup) |
- ↑ Protein (1.2–1.5 g/kg/day) if patient is on dialysis | | 🍚 Calories | 30–35 kcal/kg/day (to prevent protein breakdown) | | 💧 Fluids | Restrict as per urine output + 500 mL/day if oliguric | | 🧂 Sodium | Limit to 1.5–2 g/day to reduce fluid retention and BP | | 🍌 Potassium | Restrict if levels are high – avoid bananas, oranges, potatoes, spinach | | 🧀 Phosphorus | Restrict dairy, nuts, chocolate, colas – may require phosphate binders | | 🥬 Calcium & Vitamin D | Supplement if serum calcium is low and phosphorus is high | | 💊 Supplements | B-complex, folic acid, iron (to treat anemia)
❌ Avoid:
- Salt substitutes (contain potassium)
- Processed foods (high sodium & phosphorus)
- Canned soups, fast food
- Excess animal protein
- Cola drinks and chocolate (high phosphate)
⚠️ COMPLICATIONS OF CHRONIC RENAL FAILURE
If not well-managed, CRF leads to multiple systemic and life-threatening complications:
| System | Complications |
|---|---|
| 🧫 Hematologic | – Anemia (↓ erythropoietin) |
- Bleeding tendencies (platelet dysfunction) | | 💧 Fluid & Electrolyte | – Hyperkalemia
- Hyponatremia, fluid overload
- Metabolic acidosis | | 🧠 Neurological | – Uremic encephalopathy
- Peripheral neuropathy | | 🦴 Skeletal | – Renal osteodystrophy
- Osteomalacia, bone fractures | | 🫀 Cardiovascular | – Hypertension
- Heart failure
- Pericarditis
- Accelerated atherosclerosis | | 🧴 Integumentary | – Uremic pruritus
- Uremic frost (late stage) | | 🧠 Psychosocial | – Anxiety, depression, fear of dialysis or death | | 🧬 End-stage | – Progression to ESRD, requiring dialysis or transplantation
📌 KEY POINTS – CHRONIC RENAL FAILURE / CKD
✔ CKD is a progressive, irreversible loss of renal function over months or years
✔ Common causes:
- Diabetes mellitus (most common)
- Hypertension
- Glomerulonephritis
- Polycystic kidney disease
✔ Classified in 5 stages based on GFR
- Stage 5 = End-Stage Renal Disease (ESRD)
✔ Signs/Symptoms:
- Fatigue, edema, oliguria
- Nausea, uremic breath, pruritus, bone pain, anemia
✔ Management includes:
- Controlling underlying causes
- Managing anemia, fluid & electrolyte imbalance
- Diet therapy
- Preparing for dialysis or transplant
✔ Nursing care focuses on:
- Monitoring labs, BP, weight
- Educating on diet, fluid, and medications
- Preventing infections and complications
- Supporting psychosocial needs
✔ Early diagnosis and adherence to treatment may slow progression and improve quality of life.
🌟 Disorders of Ureter 🌟
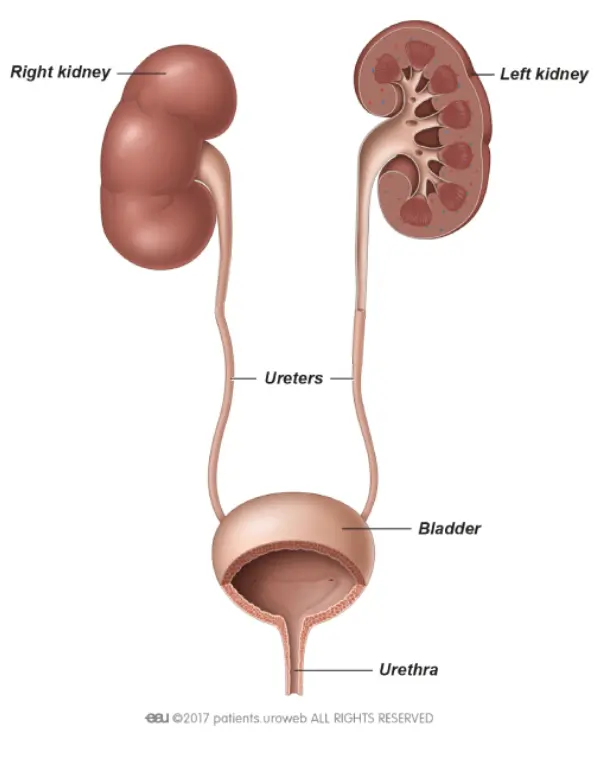
📘 Definition:
Disorders of the ureter refer to a group of conditions affecting the structure or function of one or both ureters, the muscular tubes that carry urine from the kidneys to the bladder.
⚠️ Causes:
🔹 Congenital anomalies – e.g., ureteropelvic junction obstruction
🔹 Obstructive conditions – e.g., stones, tumors
🔹 Infections – e.g., ureteritis
🔹 Trauma or injury – surgical, accidental
🔹 Neurological dysfunction – neurogenic bladder affecting ureter function
🔹 Vesicoureteral reflux (VUR) – backflow of urine into ureters
🧬 Types of Ureteral Disorders:
- 🟢 Ureteral Obstruction (due to stones, tumors, strictures)
- 🔵 Ureterocele (cystic dilation of the distal ureter)
- 🟡 Vesicoureteral Reflux (VUR)
- 🟠 Ureteral Stricture or Stenosis
- 🟣 Ectopic Ureter (abnormal opening outside the bladder)
- 🔴 Ureteritis (inflammation of the ureter)
🔄 Pathophysiology:
Disorders interfere with normal urine flow, leading to:
🔹 Urinary stasis
🔹 Hydroureter (dilated ureter)
🔹 Hydronephrosis (kidney swelling)
🔹 Increased pressure → renal tissue damage
🔹 Risk of infections and renal failure if left untreated
🔍 Signs and Symptoms:
🔸 Flank pain or lower abdominal pain
🔸 Hematuria (blood in urine)
🔸 Dysuria or burning sensation during urination
🔸 Frequent urinary tract infections (UTIs)
🔸 Nausea, vomiting
🔸 Fever (in case of infection)
🔸 Oliguria (low urine output)
🔸 Urinary incontinence (in ectopic ureter/VUR)
🧪 Diagnosis:
🧫 Urinalysis – detects infection, blood
🧬 Urine culture – identifies pathogens
🖥️ Ultrasound (KUB) – identifies hydronephrosis, ureteral dilation
🩻 Intravenous Pyelogram (IVP) – contrast imaging of ureter
🩻 CT scan or MRI – detailed anatomy
📈 Voiding Cystourethrogram (VCUG) – for VUR
🔎 Cystoscopy or Ureteroscopy – direct visualization
💊 Medical Management:
✔️ Antibiotics – for infections
✔️ Analgesics/NSAIDs – for pain
✔️ Alpha-blockers – to help stone passage
✔️ Hydration therapy – flush small stones
✔️ Anticholinergics or bladder relaxants – for VUR or reflux symptoms
🏥 Surgical Management:
🔧 Ureteral stenting – to relieve obstruction
🔧 Ureteral reimplantation – in VUR
🔧 Endoscopic dilation or laser – for strictures
🔧 Ureterolithotomy – removal of large stones
🔧 Nephroureterectomy – removal of kidney and ureter (in cancer cases)
🔧 Ureteroureterostomy – segmental ureter removal and reconnection
🧑⚕️ Nursing Management:
🩺 Assessment & Monitoring
▪ Monitor urine output, color, and clarity
▪ Monitor for signs of infection or hematuria
▪ Assess pain and vital signs regularly
💉 Pre & Post-operative Care
▪ Pre-op: Consent, NPO status, bowel prep if ordered
▪ Post-op: Monitor catheter, drains, IV fluids, and pain relief
🧼 Infection Prevention
▪ Strict asepsis in catheter care
▪ Educate on hygiene and hydration
📚 Patient Education
▪ Importance of fluid intake
▪ Medication adherence
▪ Signs of recurrence or complications
▪ Post-surgical precautions
🥗 Nutritional Consideration:
🍀 Encourage:
✅ High fluid intake (2.5–3L/day)
✅ Citrus juices (alkalinize urine)
✅ Low sodium diet (if hypertension/renal involvement)
✅ Cranberry juice (for UTIs)
🚫 Avoid:
❌ Excess protein (in stricture/cancer cases)
❌ Oxalate-rich foods if stone-prone (spinach, nuts)
❌ Caffeine and alcohol (irritate urinary tract)
⚠️ Complications:
❗ Hydronephrosis
❗ Recurrent urinary tract infections
❗ Kidney damage or failure
❗ Sepsis (from ascending infection)
❗ Renal calculi formation
❗ Urinary incontinence (esp. with ectopic ureter)
✅ Key Points:
🔹 Ureter disorders can be congenital or acquired
🔹 Early detection prevents renal complications
🔹 Management involves both medical and surgical interventions
🔹 Nursing role includes monitoring, educating, and preventing infections
🔹 Adequate fluid intake and hygiene are essential
🔹 Lifelong follow-up may be needed for chronic conditions
🚫🟡 URETERAL OBSTRUCTION
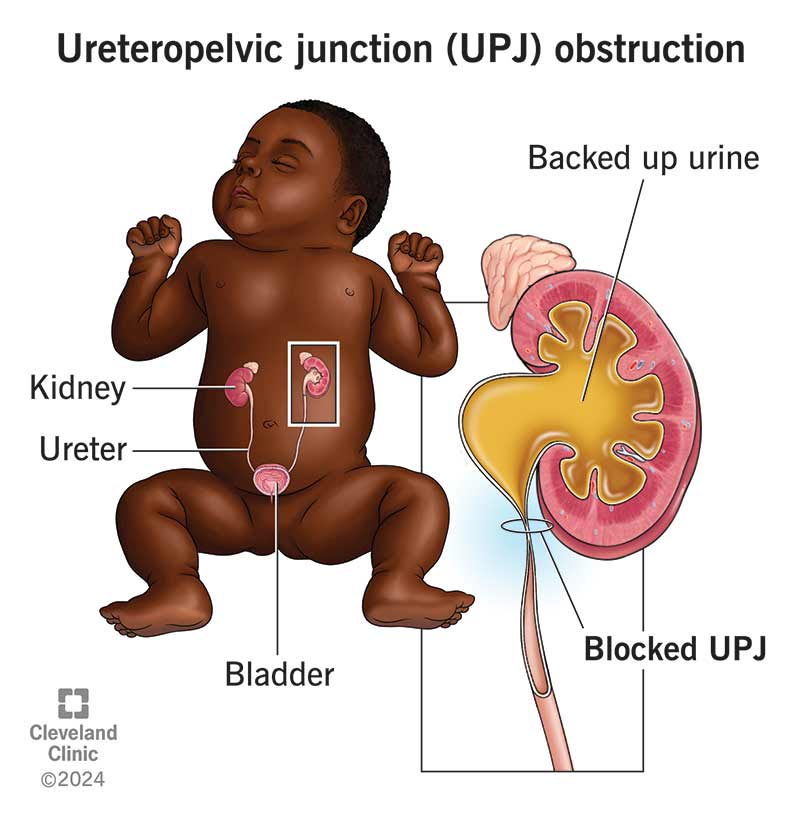
📘 Definition:
Ureteral Obstruction refers to a blockage in one or both ureters (tubes that carry urine from kidneys to bladder), causing partial or complete obstruction of urine flow, which can lead to hydronephrosis, infection, and renal damage.
⚠️ Causes:
🔹 Kidney or ureteral stones (calculi)
🔹 Ureteral strictures (narrowing due to scarring or injury)
🔹 Ureteral tumors (benign or malignant)
🔹 External compression (from enlarged lymph nodes, tumors, or pregnancy)
🔹 Congenital abnormalities (e.g., ureteropelvic junction obstruction)
🔹 Ureterocele (dilated distal ureter)
🔹 Post-surgical adhesions or fibrosis
🔹 Neurogenic bladder with reflux
🧬 Types:
- 🟢 Unilateral Obstruction – affects one ureter only
- 🔵 Bilateral Obstruction – affects both ureters
- 🟡 Acute Obstruction – sudden onset, e.g., stone
- 🔴 Chronic Obstruction – develops slowly, e.g., tumors or fibrosis
- 🟠 Partial Obstruction – allows some urine to pass
- 🟣 Complete Obstruction – blocks all urine flow
🔄 Pathophysiology:
🔸 Obstruction → ↓ Urine flow
🔸 ↑ Pressure in ureter and renal pelvis
🔸 Dilation of ureter (hydroureter) and kidney pelvis (hydronephrosis)
🔸 Compression of renal parenchyma
🔸 ↓ Renal perfusion → ↓ GFR (glomerular filtration rate)
🔸 Accumulation of toxins → acute kidney injury (if bilateral)
🔸 Risk of urinary tract infection (UTI) and pyelonephritis
🔍 Signs and Symptoms:
🔸 Flank or abdominal pain (sharp or dull)
🔸 Hematuria (blood in urine)
🔸 Dysuria or urgency (if infection)
🔸 Nausea and vomiting (in acute cases)
🔸 Fever and chills (if infected)
🔸 Decreased urine output
🔸 Bladder distension or urinary retention
🔸 Signs of uremia in bilateral obstruction (fatigue, confusion, itching)
🧪 Diagnosis:
🧫 Urinalysis – check for infection, hematuria
🧬 Urine culture – for infection
🖥️ Ultrasound (KUB) – shows hydronephrosis, hydroureter
🩻 Intravenous Pyelogram (IVP) – detects site of blockage
🧲 CT scan / MRI – identifies stones, tumors
📊 Renal Function Tests – ↑ BUN, ↑ creatinine
🔎 Cystoscopy / Ureteroscopy – direct visualization of ureter
💊 Medical Management:
✅ Pain relief: NSAIDs, opioids
✅ Antibiotics: if infection present
✅ Alpha-blockers (e.g., tamsulosin): to facilitate stone passage
✅ IV fluids: to flush out small stones
✅ Diuretics (cautiously): if indicated
✅ Management of underlying cause: tumor, fibrosis, etc.
🏥 Surgical Management:
🔧 Ureteral Stent Insertion: keeps ureter open
🔧 Percutaneous Nephrostomy: for temporary urine diversion
🔧 Ureteroscopy with laser lithotripsy: for stone removal
🔧 Balloon Dilation: for strictures
🔧 Ureterolysis: to remove fibrotic tissue
🔧 Ureteroureterostomy / Reimplantation: reconstruct damaged segments
🔧 Nephroureterectomy: for malignant causes
🧑⚕️ Nursing Management:
🩺 Assessment:
▪ Monitor urinary output and character
▪ Assess for pain, fever, signs of infection
▪ Monitor renal function reports (BUN, creatinine)
💉 Pre/Post-op Care:
▪ Prepare patient for imaging or surgical intervention
▪ Maintain catheter/nephrostomy tube care
▪ Provide post-op pain management
📚 Patient Education:
▪ Hydration importance
▪ Avoidance of stone-promoting diet (if applicable)
▪ Medication adherence
▪ Recognize early signs of recurrence
🥗 Nutritional Consideration:
✅ Increase Fluid Intake: 2.5–3 L/day
✅ Citrate-rich foods (lemon, oranges): prevent stones
✅ Low-sodium diet: reduces calcium excretion
✅ Low-oxalate diet: avoid spinach, chocolate, nuts (in stone-prone cases)
✅ Adequate calcium (not excess): prevents stone formation
❌ Avoid excess protein, caffeine, soft drinks (increase stone risk)
⚠️ Complications:
❗ Hydronephrosis
❗ Recurrent UTI / pyelonephritis
❗ Renal scarring and chronic kidney disease (CKD)
❗ Acute renal failure (in bilateral obstruction)
❗ Sepsis (if infection spreads)
❗ Electrolyte imbalance and metabolic acidosis
✅ Key Points:
🔹 Ureteral obstruction can be acute or chronic, partial or complete
🔹 Early diagnosis prevents permanent kidney damage
🔹 Hydronephrosis is a key consequence
🔹 Imaging and renal function tests guide treatment
🔹 Surgical intervention is often required
🔹 Nurses play a vital role in monitoring, infection control, and education
🔹 Nutrition and hydration are crucial in prevention and recovery
🎈 URETEROCELE
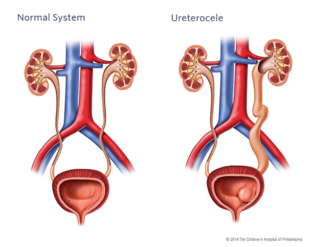
📘 Definition:
A ureterocele is a cystic dilation (ballooning) of the distal end of the ureter as it enters the bladder. It results in a sac-like outpouching that may block urine flow and lead to urinary tract complications.
🧠 It can occur in one or both ureters and is more common in females and infants.
⚠️ Causes:
🔹 Congenital defect – failure of the ureteric orifice to develop normally
🔹 Ectopic ureter – ureter drains below bladder sphincter or in abnormal location
🔹 Obstruction at the ureterovesical junction
🔹 Ureteral valve malfunction
🔹 Associated with duplicated urinary systems (more than one ureter per kidney)
🧬 Types of Ureterocele:
- 🟢 Orthotopic (Intravesical):
▪ Located entirely within the bladder
▪ Less severe - 🔵 Ectopic (Extravesical):
▪ Partly located outside the bladder
▪ Common in duplicated collecting systems
▪ Often causes obstruction or reflux
🔄 Pathophysiology:
- Distal ureteral narrowing → urine buildup
- Ballooning/dilation of ureteral end → ureterocele formation
- Obstruction of urine flow from kidney → hydronephrosis
- Stasis of urine → increased infection risk
- In severe cases → renal parenchymal damage and loss of function
🔍 Signs and Symptoms:
👶 In Infants/Children:
🔸 Recurrent urinary tract infections (UTIs)
🔸 Abdominal mass or distension
🔸 Poor urinary stream
🔸 Fever, vomiting
🔸 Foul-smelling urine
🧑 In Adults:
🔸 Flank pain or lower abdominal pain
🔸 Hematuria (blood in urine)
🔸 Frequent urination or urgency
🔸 Urinary retention or incontinence
🔸 Sometimes asymptomatic (found incidentally)
🧪 Diagnosis:
🩻 Ultrasound (KUB): Shows ureterocele, hydronephrosis
🧲 Voiding Cystourethrogram (VCUG): Detects reflux and ureterocele prolapse
📷 Intravenous Pyelogram (IVP): Outline of ureterocele in contrast
🧬 MRI / CT scan: More detailed anatomy
🔍 Cystoscopy: Direct visualization of ureterocele bulging into bladder
💊 Medical Management:
✅ Antibiotics: If UTI is present
✅ Antispasmodics or analgesics for pain relief
✅ Observation: For small, asymptomatic ureteroceles
✅ Regular monitoring of renal function, growth, and development in children
🏥 Surgical Management:
🔧 Endoscopic Puncture/Incision:
▪ Common initial treatment
▪ Minimally invasive
▪ Helps decompress ureterocele
🔧 Ureteral Reimplantation:
▪ Relocates ureter to normal bladder position
▪ Done for ectopic or recurrent cases
🔧 Partial Nephrectomy:
▪ If severe kidney damage in duplex systems
🔧 Excision of ureterocele with reconstruction:
▪ In complex or non-responsive cases
🧑⚕️ Nursing Management:
🩺 Pre-operative care:
▪ Educate parents/patients about surgery
▪ Prepare for imaging/surgical procedure
▪ Monitor UTI signs
💉 Post-operative care:
▪ Monitor urine output, hematuria
▪ Maintain catheter care
▪ Watch for signs of infection or urinary retention
📚 Patient/Parent Education:
▪ Importance of follow-up
▪ Medication compliance
▪ Report fever, pain, or foul urine
🥗 Nutritional Consideration:
✅ Encourage:
🍀 High fluid intake – prevents infection and flushes system
🥣 Balanced diet to promote growth in children
🧃 Vitamin C–rich foods (cranberry juice, oranges) – reduce UTI risk
❌ Avoid:
⚠️ Caffeine, carbonated beverages, spicy food – irritants to urinary tract
⚠️ Excessive protein in kidney damage
⚠️ Complications:
❗ Recurrent UTIs
❗ Hydronephrosis
❗ Renal damage or loss of kidney function
❗ Vesicoureteral reflux (VUR)
❗ Urinary retention or incontinence
❗ Bladder outlet obstruction
✅ Key Points:
🔹 Ureterocele is a congenital dilation of the distal ureter
🔹 Can be orthotopic or ectopic – severity depends on type
🔹 Early diagnosis is critical in children to prevent kidney damage
🔹 Commonly managed with endoscopic surgery
🔹 Long-term follow-up is essential to monitor renal function
🔹 Nurses play a key role in infection control, education, and post-op care
🔄💦 VESICOURETERAL REFLUX (VUR)
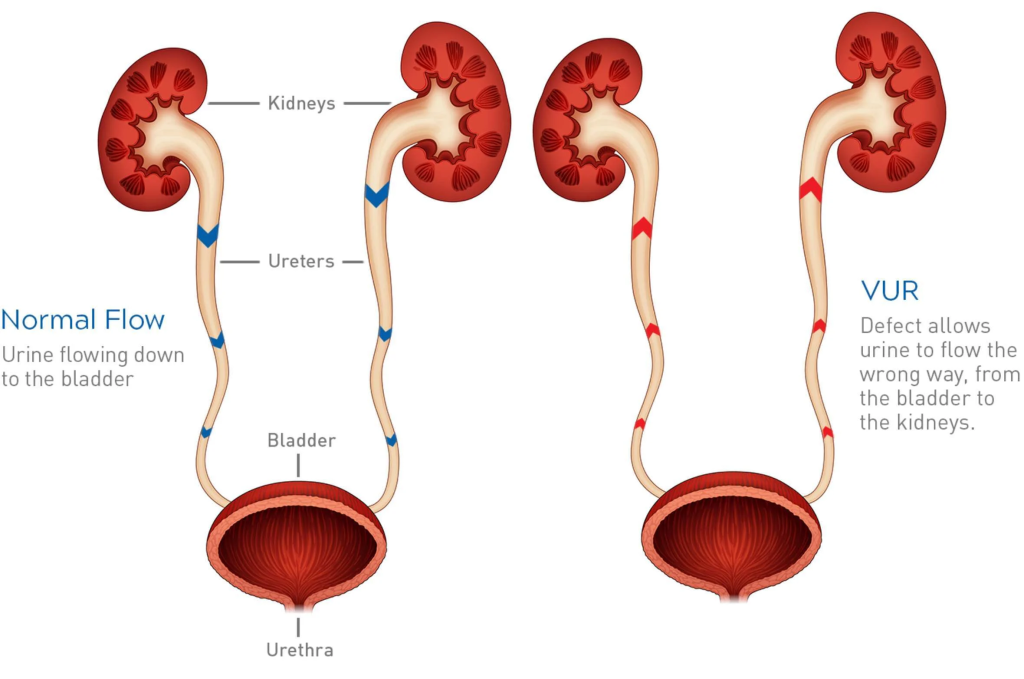
📘 Definition:
Vesicoureteral Reflux (VUR) is a condition where urine flows backward from the bladder up into one or both ureters and sometimes into the kidneys.
🧠 This reverse flow can lead to kidney infections, hydronephrosis, and even renal scarring if left untreated.
⚠️ Causes:
🔹 Primary VUR (congenital):
▪ Due to improper formation of the ureterovesical junction (UVJ)
▪ Valve mechanism fails to prevent backflow
🔹 Secondary VUR (acquired):
▪ Due to bladder dysfunction, obstruction, or neurogenic bladder
▪ Pressure buildup forces urine back into the ureters
▪ Often associated with posterior urethral valves, spina bifida, etc.
🧬 Types / Grades of VUR:
🟢 Grade I: Urine refluxes into ureter only
🔵 Grade II: Urine reaches renal pelvis without dilation
🟡 Grade III: Mild dilation of ureter and renal pelvis
🟠 Grade IV: Moderate dilation and tortuosity of ureter
🔴 Grade V: Severe dilation and loss of ureteral contour
👉 Grades I–III = mild to moderate
👉 Grades IV–V = severe, often need surgery
🔄 Pathophysiology:
- Defective UVJ valve or high bladder pressure
- Urine flows retrograde into ureters/kidneys
- Stasis of urine → bacterial growth → UTI
- Repeated infections → pyelonephritis & renal scarring
- Long-term → chronic kidney disease if untreated
🔍 Signs and Symptoms:
👶 In Infants/Children:
🔸 Recurrent febrile UTIs
🔸 Poor weight gain or growth
🔸 Irritability, feeding problems
🔸 Abdominal mass (hydronephrosis)
🧒 In Older Children:
🔸 Burning during urination
🔸 Frequent urination or bedwetting
🔸 Flank or abdominal pain
🔸 High fever during UTI
🔸 Hematuria
🧑 Sometimes asymptomatic and detected during investigation of UTI
🧪 Diagnosis:
🧫 Urinalysis & Urine Culture: Confirm UTI
🖥️ Ultrasound (KUB): Detects hydronephrosis or scarring
📉 Voiding Cystourethrogram (VCUG): Gold standard
🔎 Radionuclide Cystogram (RNC): Measures reflux, less radiation
🧬 DMSA Scan: Detects renal scarring or cortical damage
🧪 Renal function tests – BUN, creatinine
💊 Medical Management:
✅ Low-dose prophylactic antibiotics – to prevent recurrent UTIs
✅ Frequent monitoring – urine cultures, ultrasounds
✅ Bladder training and timed voiding in older children
✅ Treat constipation – reduces bladder pressure
✅ Anticholinergics for bladder spasms in secondary VUR
🏥 Surgical Management:
🔧 Endoscopic Deflux Injection:
▪ Minimally invasive
▪ Bulking agent injected near UVJ
▪ For Grades II–IV
🔧 Ureteral Reimplantation Surgery (Cohen’s):
▪ Ureter is repositioned in bladder wall
▪ Prevents backflow
▪ For high-grade VUR or failed medical therapy
🔧 Bladder augmentation or reconstruction (rare):
▪ In cases of neurogenic bladder or complex abnormalities
🧑⚕️ Nursing Management:
🩺 Monitor for UTIs:
▪ Fever, urgency, frequency, cloudy/foul-smelling urine
▪ Educate parents on signs of infection
💊 Medication Compliance:
▪ Administer prophylactic antibiotics on schedule
▪ Encourage regular follow-ups and urine tests
💧 Encourage Fluids:
▪ Promote frequent urination to prevent stasis
📚 Patient/Parent Education:
▪ Importance of hygiene and proper wiping (front to back in girls)
▪ Avoid holding urine
▪ Dietary fiber to avoid constipation
▪ Explain procedures like VCUG, surgery
🥗 Nutritional Consideration:
✅ Encourage:
🥤 Adequate hydration – 2–3 L/day (based on age)
🍊 Cranberry juice – may reduce UTI risk
🥦 Fiber-rich diet – to prevent constipation
🍱 Balanced meals for growth in children
❌ Avoid:
⚠️ Caffeine, spicy foods (bladder irritants)
⚠️ Processed foods with high sodium (fluid retention)
⚠️ Complications:
❗ Recurrent pyelonephritis
❗ Renal scarring
❗ Hypertension
❗ Proteinuria
❗ Chronic kidney disease (CKD)
❗ Growth retardation (in children)
❗ Vesicoureteral obstruction post-surgery (rare)
✅ Key Points:
🔹 VUR is backflow of urine from bladder to ureters/kidneys
🔹 Can be congenital (primary) or secondary to bladder dysfunction
🔹 Diagnosis confirmed by VCUG
🔹 Low grades often resolve with time and antibiotics
🔹 Higher grades may require surgical correction
🔹 Nurses play a critical role in UTI prevention, parent education, and post-op care
🔹 Long-term follow-up is crucial for renal health monitoring
🔻🧵 URETERAL STENOSIS
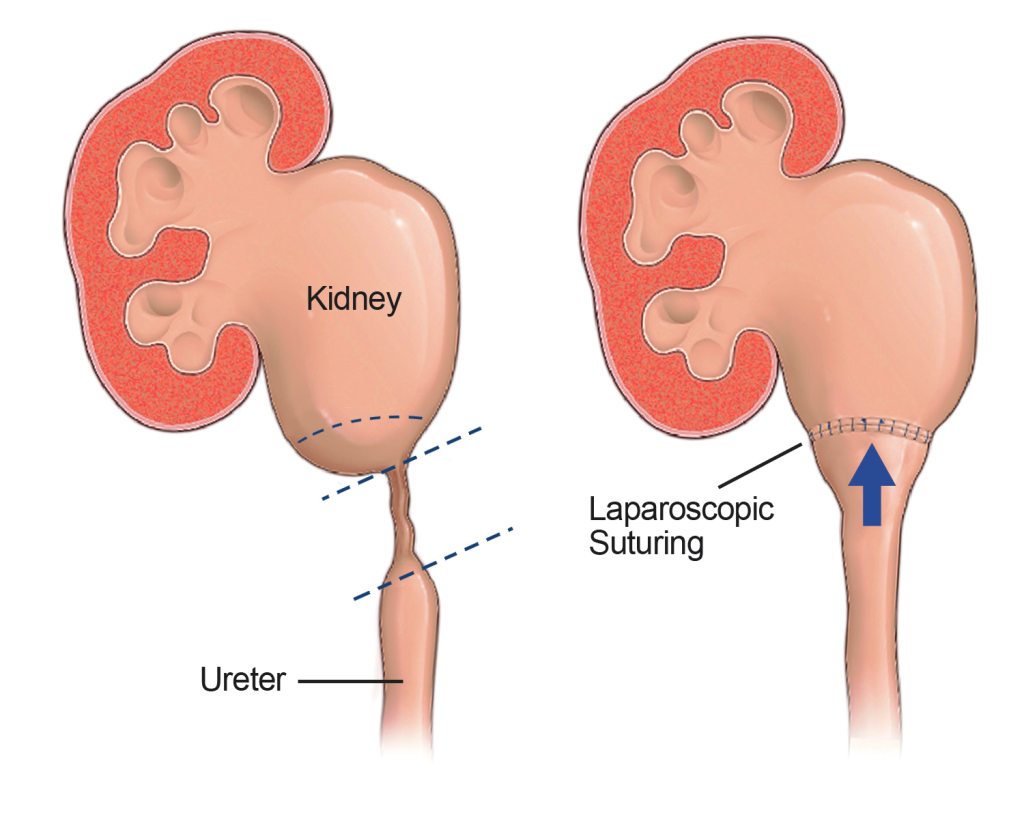
📘 Definition:
Ureteral stenosis is a narrowing (stricture) of the ureter, the tube that carries urine from the kidney to the bladder. This narrowing restricts urine flow, leading to hydronephrosis, urinary stasis, and potentially renal damage.
⚠️ Causes:
🔹 Congenital Defect – abnormal ureter development (often at the ureteropelvic junction – UPJ)
🔹 Post-surgical Injury – e.g., from pelvic or ureteral surgery
🔹 Radiation Therapy – fibrosis causing strictures
🔹 Infection – chronic inflammation (e.g., TB, schistosomiasis)
🔹 Ureteric Stones – inflammation and scarring post-passage
🔹 Tumors or External Compression – pelvic mass pressing ureter
🔹 Retroperitoneal fibrosis
🧬 Types of Ureteral Stenosis:
- 🟢 Intrinsic Stenosis – due to scarring or narrowing of the ureteral wall
- 🔵 Extrinsic Stenosis – due to external compression (tumors, fibrosis)
- 🟡 Unilateral – affects one ureter (common)
- 🔴 Bilateral – both ureters affected (rare, but serious)
🔄 Pathophysiology:
- Narrowing of ureter → obstruction of urine flow
- Urine backs up → hydroureter and hydronephrosis
- Pressure on renal pelvis → decreased GFR and renal perfusion
- Prolonged obstruction → tissue damage, renal atrophy
- Urine stagnation → risk of infection
🔍 Signs and Symptoms:
🔸 Flank pain or abdominal discomfort
🔸 Hematuria (blood in urine)
🔸 Nausea and vomiting (acute obstruction)
🔸 Recurrent urinary tract infections
🔸 Decreased urine output (if bilateral or severe)
🔸 Hypertension (in prolonged renal involvement)
🔸 Fever and chills (if infection present)
🧪 Diagnosis:
🧫 Urinalysis & Urine Culture – detect hematuria or infection
🖥️ Ultrasound (KUB) – hydronephrosis or hydroureter
📷 Intravenous Pyelogram (IVP) – identifies site of narrowing
🧲 CT Urography or MRI – detailed view of obstruction
🔬 Renal Function Tests – BUN, creatinine, GFR
🔎 Cystoscopy / Retrograde Pyelography – direct view of ureter
🧬 Nuclear Scan (DTPA/MAG3) – evaluates renal drainage
💊 Medical Management:
✅ Antibiotics – for infection
✅ Pain relief – NSAIDs or opioids
✅ Hydration therapy – maintain renal perfusion
✅ Monitoring – small or partial strictures may be monitored regularly
✅ Treat underlying cause – e.g., fibrosis, infection
🏥 Surgical Management:
🔧 Balloon Dilation:
▪ Minimally invasive
▪ Used to stretch narrowed area
🔧 Ureteral Stenting:
▪ Stent placed across stenosis to keep ureter open
🔧 Endoureterotomy:
▪ Internal cutting of the narrowed ureter using a scope
🔧 Ureteroureterostomy:
▪ Surgical removal of the narrowed segment and reconnection of ureter ends
🔧 Ureteral Reimplantation:
▪ Repositioning the ureter into the bladder (especially in lower ureteral stenosis)
🔧 Nephrostomy Tube:
▪ Used temporarily if obstruction is severe to divert urine directly from kidney
🧑⚕️ Nursing Management:
🩺 Pre-operative Care:
▪ Prepare for imaging or surgical procedures
▪ Explain procedures to patient/family
▪ Assess renal function, pain, and infection signs
💉 Post-operative Care:
▪ Monitor urinary output and color
▪ Catheter or nephrostomy care
▪ Pain and infection control
▪ Monitor for hematuria, fever
📚 Patient Education:
▪ Hydration importance
▪ Infection prevention
▪ Follow-up imaging and labs
▪ Lifestyle and diet if recurrent stones are the cause
🥗 Nutritional Consideration:
✅ Encourage:
💧 Adequate hydration – 2–3 L/day
🍊 Citrate-rich foods – prevent stone recurrence
🥦 Balanced diet – support healing
❌ Avoid:
⚠️ High sodium intake – increases calcium excretion
⚠️ Oxalate-rich foods (in stone-formers)
⚠️ Caffeine, alcohol – can irritate the bladder
⚠️ Complications:
❗ Recurrent UTIs
❗ Hydronephrosis and renal atrophy
❗ Renal failure (if bilateral or severe)
❗ Electrolyte imbalance
❗ Sepsis (from untreated infection)
❗ Persistent pain and hypertension
✅ Key Points:
🔹 Ureteral stenosis is narrowing of ureter that obstructs urine flow
🔹 It can be congenital or acquired, intrinsic or extrinsic
🔹 Imaging and renal function tests are key for diagnosis
🔹 Minimally invasive and open surgical options exist
🔹 Nurses must focus on infection prevention, renal monitoring, and education
🔹 Hydration and follow-up are critical to prevent recurrence
💦🧫 URINARY BLADDER DISORDERS
📘 Definition:
Urinary bladder disorders refer to a variety of conditions affecting the structure and function of the bladder, which is responsible for storing and expelling urine. These disorders can lead to problems like urinary retention, incontinence, infections, or pain.
⚠️ Causes:
🔹 Infections – especially E. coli, leading to cystitis
🔹 Neurological disorders – spinal cord injury, Parkinson’s, stroke
🔹 Bladder outlet obstruction – due to prostate enlargement, tumors, or strictures
🔹 Congenital anomalies – e.g., exstrophy, neurogenic bladder
🔹 Trauma or surgery – affecting bladder control
🔹 Medications – anticholinergics, opioids
🔹 Radiation therapy – bladder tissue damage
🧬 Types of Bladder Disorders:
- 🔴 Urinary Incontinence – involuntary leakage of urine
- 🔵 Urinary Retention – incomplete emptying of the bladder
- 🟡 Neurogenic Bladder – loss of normal bladder control due to nerve damage
- 🟢 Cystitis – bladder infection/inflammation
- 🟣 Bladder Stones – hard masses of minerals
- 🟠 Bladder Cancer – malignant growth in bladder lining
- ⚫ Overactive Bladder (OAB) – frequent, urgent need to urinate
- ⚪ Bladder Prolapse (Cystocele) – bladder drops into vaginal wall in women
🔄 Pathophysiology:
The normal bladder function depends on the coordination between the bladder muscles (detrusor), urethral sphincter, and the nervous system.
🩻 In bladder disorders, either:
▪ The muscle function is impaired (too weak or overactive)
▪ Nerve control is lost (neurogenic)
▪ Obstruction causes overdistension
▪ Or infection/inflammation disrupts bladder lining integrity
This leads to symptoms such as urgency, retention, frequency, pain, or incontinence.
🔍 Signs and Symptoms:
🔸 Urgency to urinate
🔸 Frequent urination (polyuria)
🔸 Burning during urination (dysuria)
🔸 Pain in lower abdomen or pelvis
🔸 Urine leakage (incontinence)
🔸 Difficulty initiating urination
🔸 Incomplete bladder emptying
🔸 Nocturia (urinating at night)
🔸 Hematuria (blood in urine)
🔸 Cloudy or foul-smelling urine
🧪 Diagnosis:
🧫 Urinalysis & Culture: Detect infection, hematuria, proteinuria
🖥️ Ultrasound (KUB): Evaluate post-void residual volume, stones, tumors
🔍 Cystoscopy: Direct visualization of bladder wall
📈 Urodynamic Tests: Assess bladder pressure, capacity, and flow
📷 CT / MRI: Detect tumors, anatomical issues
🧪 Bladder diary or frequency-volume chart
💊 Medical Management:
✅ Antibiotics: For bladder infections (e.g., nitrofurantoin, ciprofloxacin)
✅ Anticholinergics / Beta-3 agonists: For overactive bladder
✅ Alpha-blockers: To improve urine flow
✅ Analgesics: For pain relief (e.g., phenazopyridine)
✅ Botulinum toxin (Botox): For OAB
✅ Hormone therapy: For postmenopausal women with atrophy
✅ Bladder training, pelvic floor exercises (Kegel)
🏥 Surgical Management:
🔧 Transurethral Resection of Bladder Tumor (TURBT): For bladder cancer
🔧 Urethral dilation or stenting: For obstruction
🔧 Bladder augmentation (augmentation cystoplasty): In severe neurogenic bladder
🔧 Catheterization (intermittent or indwelling): For retention
🔧 Urinary diversion (e.g., ileal conduit): In cases of bladder removal
🔧 Sling procedures / bladder suspension: For incontinence
🔧 Stone removal surgery
🧑⚕️ Nursing Management:
🩺 Assessment:
▪ Monitor urinary output, bladder distension
▪ Assess signs of UTI, retention, or leakage
▪ Evaluate pain level and voiding patterns
💉 Interventions:
▪ Assist with catheterization
▪ Promote adequate fluid intake
▪ Encourage timed voiding or double voiding
▪ Provide perineal hygiene
▪ Administer prescribed medications
📚 Patient Education:
▪ Hydration and bladder-friendly diet
▪ Toilet scheduling for urgency or incontinence
▪ Pelvic floor exercises
▪ Recognizing signs of infection or retention
▪ Catheter care (if applicable)
🥗 Nutritional Consideration:
✅ Encourage:
🍀 Fluids: 2–3 L/day (unless restricted)
🍊 Vitamin C-rich foods: May acidify urine and help prevent UTIs
🥣 High-fiber diet: Prevent constipation that affects bladder function
❌ Avoid:
⚠️ Caffeine, alcohol, spicy foods, citrus fruits – bladder irritants
⚠️ Carbonated beverages – may worsen urgency
⚠️ High-sodium foods – cause fluid retention
⚠️ Complications:
❗ Chronic urinary tract infections
❗ Hydronephrosis (from retention)
❗ Renal failure (if obstructive uropathy is not treated)
❗ Bladder rupture (rare)
❗ Bladder fibrosis or thickening
❗ Urinary incontinence → social isolation
❗ Sepsis (if infection spreads)
✅ Key Points:
🔹 Bladder disorders affect both storage and emptying of urine
🔹 Common types include incontinence, retention, cystitis, and OAB
🔹 Early diagnosis is essential to prevent renal damage and infections
🔹 Urodynamic studies and cystoscopy are key diagnostic tools
🔹 Medical and surgical treatments are tailored to type and severity
🔹 Nurses play a vital role in monitoring, hygiene, patient education, and catheter care
🔹 Hydration and lifestyle changes are important for prevention and management
💧🔓 URINARY INCONTINENCE

📘 Definition:
Urinary Incontinence (UI) is the involuntary loss of urine that is objectively demonstrable and causes social or hygienic problems.
🧠 It can range from occasional leaks to complete loss of bladder control, affecting people of all ages, especially elderly women.
⚠️ Causes:
🔹 Weak pelvic floor muscles (post childbirth, aging)
🔹 Overactive bladder muscle (detrusor instability)
🔹 Neurological disorders (stroke, Parkinson’s, spinal injury)
🔹 Bladder outlet obstruction (e.g., enlarged prostate)
🔹 Urinary tract infections (UTIs)
🔹 Constipation
🔹 Medications (diuretics, sedatives, antipsychotics)
🔹 Obesity or chronic cough (↑ intra-abdominal pressure)
🔹 Hormonal changes (e.g., menopause)
🧬 Types of Urinary Incontinence:
- 🟢 Stress Incontinence:
▪ Leakage with activities that ↑ abdominal pressure (e.g., coughing, sneezing, lifting)
▪ Due to weak pelvic floor or urethral sphincter - 🔵 Urge Incontinence (Overactive Bladder):
▪ Sudden, intense urge to urinate followed by leakage
▪ Caused by detrusor muscle overactivity - 🟡 Overflow Incontinence:
▪ Bladder doesn’t empty completely → constant dribbling
▪ Caused by bladder outlet obstruction or weak detrusor - 🟠 Functional Incontinence:
▪ Normal bladder function, but mobility/cognitive issues prevent timely toileting
▪ Common in elderly or dementia patients - 🔴 Mixed Incontinence:
▪ Combination of stress + urge incontinence
▪ Very common in women
🔄 Pathophysiology:
Normal continence depends on:
▪ Proper bladder contraction
▪ Adequate urethral sphincter tone
▪ Neurological control
In incontinence:
🔁 Imbalance in detrusor activity, sphincter tone, or nerve signaling
🔁 Bladder pressure exceeds urethral pressure
🔁 → Leakage of urine
🔍 Signs and Symptoms:
🔸 Involuntary leakage of urine
🔸 Sudden urge to urinate
🔸 Frequent urination (polyuria)
🔸 Nocturia (night-time urination)
🔸 Difficulty in initiating urination
🔸 Constant dribbling (in overflow)
🔸 Wet clothes, odor, social withdrawal
🧪 Diagnosis:
🧫 Urinalysis and Culture: Rule out UTI
🧲 Bladder Diary: Record fluid intake and voiding patterns
🔍 Post-void residual (PVR): Measures incomplete bladder emptying
📈 Urodynamic Studies: Evaluate bladder pressure and function
🖥️ Pelvic Ultrasound: Checks for obstruction or residual urine
🔬 Cystoscopy: Visualize bladder lining if indicated
💊 Medical Management:
✅ Anticholinergics (e.g., oxybutynin, tolterodine) – reduce bladder contractions
✅ Beta-3 agonists (e.g., mirabegron) – relax detrusor muscle
✅ Topical estrogen – for postmenopausal women
✅ Alpha-blockers (e.g., tamsulosin) – for overflow due to prostate
✅ Imipramine – dual effect: sphincter tone + bladder relaxation
✅ Botulinum toxin (Botox) – for urge incontinence
✅ Medications to treat constipation
🏥 Surgical Management:
🔧 Mid-urethral sling (MUS):
▪ Common surgery for stress incontinence in women
▪ Supports the urethra
🔧 Artificial urinary sphincter:
▪ Mostly for men post-prostate surgery
🔧 Bladder neck suspension (Burch procedure):
▪ Lifts bladder neck to improve closure
🔧 Urethral bulking agents:
▪ For mild incontinence; injected into urethra
🔧 Sacral nerve stimulation:
▪ For urge incontinence not responsive to meds
🧑⚕️ Nursing Management:
🩺 Assessment:
▪ Identify type and severity of incontinence
▪ Maintain bladder diary
▪ Assess for UTIs, skin breakdown
💧 Interventions:
▪ Encourage scheduled toileting (bladder training)
▪ Promote Kegel exercises
▪ Maintain hygiene and dry bedding
▪ Educate on fluid intake (not to restrict excessively)
▪ Use of absorbent pads/briefs
▪ Assist with mobility and accessibility to toilets
📚 Patient Education:
▪ Explain the condition and reassure
▪ Importance of pelvic floor exercises
▪ Avoid bladder irritants (caffeine, alcohol)
▪ Emphasize regular bowel habits
▪ Encourage hydration
🥗 Nutritional Consideration:
✅ Encourage:
💧 Fluid intake: 1.5–2L/day (unless restricted)
🥬 High-fiber diet: Prevent constipation
🍊 Cranberry juice/Vitamin C: Prevent UTIs
❌ Avoid:
⚠️ Caffeine, alcohol, spicy foods – bladder irritants
⚠️ Carbonated drinks
⚠️ Excessive fluid restriction (worsens concentration and irritates bladder)
⚠️ Complications:
❗ Skin breakdown (incontinence-associated dermatitis)
❗ Recurrent UTIs
❗ Social isolation, depression
❗ Sleep disturbances
❗ Falls (from rushing to the bathroom)
❗ Dehydration (from limiting fluids)
✅ Key Points:
🔹 UI is common but treatable – especially in older adults
🔹 Types include stress, urge, overflow, functional, and mixed
🔹 Kegel exercises, bladder training, and medications are first-line treatments
🔹 Surgery is effective in selected patients
🔹 Nurses play a critical role in monitoring, education, hygiene, and continence promotion
🔹 Lifestyle modifications and dietary changes enhance outcomes
🚫💧 URINARY RETENTION
📘 Definition:
Urinary Retention is the inability to completely or partially empty the bladder, despite a strong urge to urinate.
🧠 It can be acute (sudden and painful) or chronic (gradual and painless).
⚠️ Causes:
🔸 Obstructive Causes:
▪ Benign prostatic hyperplasia (BPH)
▪ Urethral stricture
▪ Bladder stones or tumors
▪ Constipation compressing urethra
🔹 Neurogenic Causes:
▪ Spinal cord injury
▪ Multiple sclerosis
▪ Diabetic neuropathy
▪ Parkinson’s disease
🔸 Infectious/Inflammatory Causes:
▪ Severe urinary tract infections
▪ Prostatitis
▪ Urethritis
🔹 Medication-Induced:
▪ Anticholinergics
▪ Opioids
▪ Anesthetics
▪ Antidepressants
🔸 Post-surgical or Postpartum:
▪ Pelvic surgery
▪ Epidural/spinal anesthesia
▪ Bladder muscle dysfunction after delivery
🧬 Types:
- 🟥 Acute Urinary Retention
▪ Sudden, painful inability to pass urine
▪ Requires emergency intervention - 🟦 Chronic Urinary Retention
▪ Gradual loss of bladder emptying ability
▪ May have no symptoms until advanced - 🟨 Incomplete Urinary Retention
▪ Bladder empties partially; high post-void residual urine
🔄 Pathophysiology:
- Obstruction or impaired nerve control → urine accumulates
- Bladder overdistension → ↑ pressure
- Detrusor muscle overstretches → loss of contractility
- Urine stagnation → infection and hydronephrosis (in chronic cases)
🔍 Signs and Symptoms:
🔴 Acute Retention:
▪ Severe suprapubic pain
▪ Inability to void despite urge
▪ Bladder distension
▪ Restlessness, sweating
🔵 Chronic Retention:
▪ Frequent urination with small volumes
▪ Weak urine stream
▪ Post-void dribbling
▪ Feeling of incomplete emptying
▪ Nocturia
▪ Recurrent urinary tract infections
🧪 Diagnosis:
🧫 Urinalysis & Culture – to detect UTI
🖥️ Bladder Ultrasound / Bladder Scan – post-void residual volume
📈 Uroflowmetry – assesses urine flow rate
🔎 Cystoscopy – visualizes urethral or bladder obstruction
🧬 Urodynamic studies – measure bladder pressure and function
📷 MRI/CT Scan – if neurogenic or structural cause is suspected
💊 Medical Management:
✅ Alpha-blockers (e.g., tamsulosin) – relax bladder neck (esp. in BPH)
✅ Cholinergic drugs (e.g., bethanechol) – stimulate bladder contraction
✅ Antibiotics – for infection
✅ Analgesics – relieve discomfort
✅ Discontinuation or adjustment of causative medications
🏥 Surgical/Procedural Management:
🔧 Immediate catheterization (intermittent or indwelling) – for acute relief
🔧 Suprapubic catheterization – if urethral catheter fails
🔧 Urethral dilation – for strictures
🔧 Transurethral Resection of Prostate (TURP) – for BPH
🔧 Bladder neck incision or surgery – to relieve outlet obstruction
🔧 Sacral nerve stimulation or urinary diversion – in neurogenic causes
🧑⚕️ Nursing Management:
🩺 Assessment:
▪ Monitor urinary output and bladder distension
▪ Assess pain, restlessness, or signs of infection
▪ Observe post-void residuals
💉 Interventions:
▪ Assist with catheterization
▪ Ensure aseptic catheter care
▪ Maintain fluid balance
▪ Apply heat to lower abdomen (relaxes bladder)
▪ Promote privacy and relaxed environment for voiding
▪ Encourage ambulation and upright posture
📚 Patient Education:
▪ Avoid delaying urination
▪ Bladder training and timed voiding
▪ Pelvic floor and relaxation exercises
▪ Medication compliance
▪ Signs of recurrence or infection
🥗 Nutritional Consideration:
✅ Encourage:
💧 Adequate fluid intake – to keep urine flowing
🥗 High-fiber diet – to avoid constipation (which worsens retention)
🍊 Cranberry juice – may reduce UTI risk
❌ Avoid:
⚠️ Alcohol and caffeine – bladder irritants
⚠️ Spicy or acidic foods – can worsen urgency or retention
⚠️ Complications:
❗ Recurrent UTIs
❗ Bladder overdistension
❗ Hydronephrosis
❗ Acute kidney injury
❗ Bladder rupture (rare, in severe acute retention)
❗ Social embarrassment or isolation
❗ Long-term catheter dependence
✅ Key Points:
🔹 Urinary retention is a common urological emergency, especially in men with BPH
🔹 Can be acute, chronic, or incomplete
🔹 Diagnosis involves ultrasound, urodynamic studies, and physical exam
🔹 Treatment includes catheterization, medications, or surgical procedures
🔹 Nurses play a vital role in catheter care, fluid monitoring, and patient education
🔹 Preventable factors include timely voiding, hydration, and avoiding causative drugs
🧠💦 NEUROGENIC BLADDER
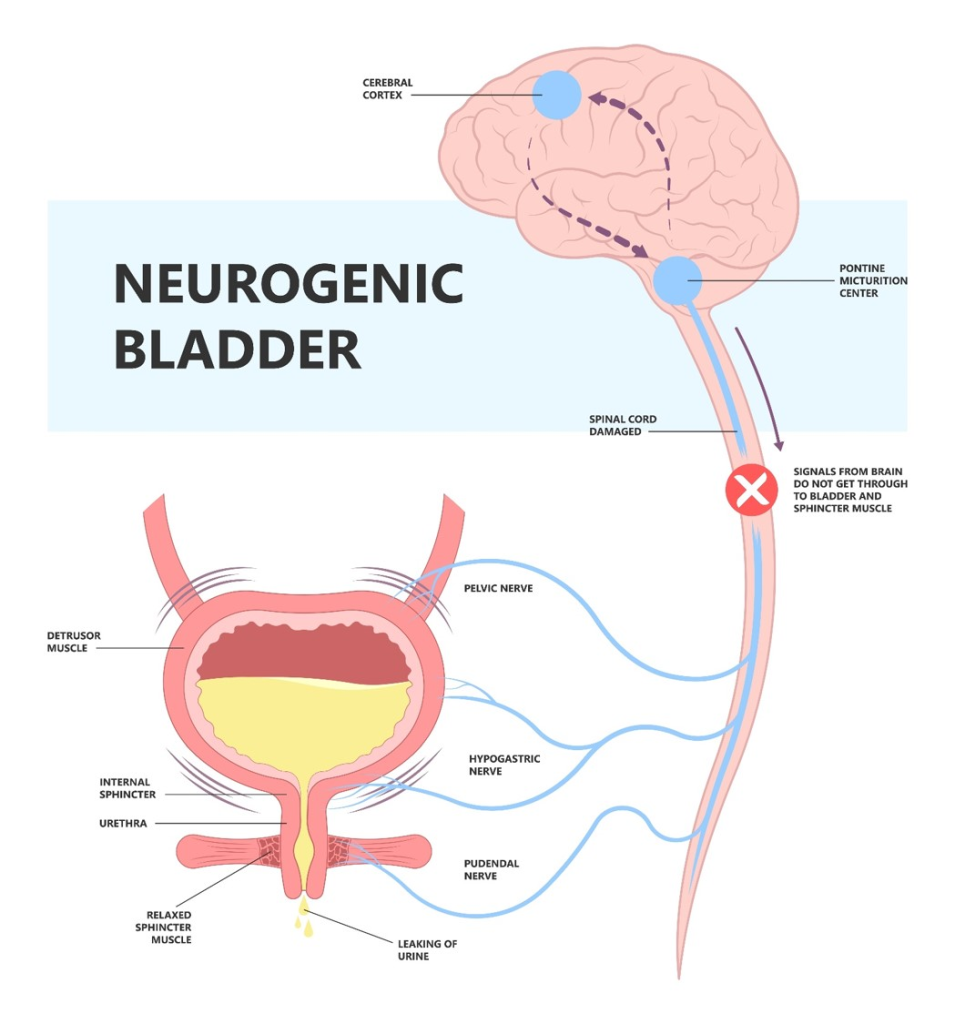
📘 Definition:
Neurogenic bladder is a dysfunction of the urinary bladder caused by damage to the nerves that control bladder storage and voiding.
🧠 This condition disrupts the communication between the bladder muscles and the brain/spinal cord, leading to incontinence, retention, or both.
⚠️ Causes:
🔸 Central Nervous System (CNS) Disorders:
▪ Stroke
▪ Parkinson’s disease
▪ Brain tumors
▪ Multiple sclerosis
🔹 Spinal Cord Disorders:
▪ Spinal cord injury
▪ Spina bifida / Myelomeningocele
▪ Herniated disc
▪ Tumors affecting spinal cord
🔸 Peripheral Nerve Disorders:
▪ Diabetic neuropathy
▪ Pelvic surgery-induced nerve damage
▪ Chronic alcoholism
▪ Guillain-Barre Syndrome
🔹 Congenital Defects:
▪ Sacral agenesis
▪ Tethered cord syndrome
🧬 Types of Neurogenic Bladder:
- 🟥 Spastic (Hyperreflexic/Overactive) Bladder:
▪ Due to upper motor neuron lesion
▪ Involuntary bladder contractions
▪ Small capacity, frequent urination, urgency - 🟦 Flaccid (Areflexic/Underactive) Bladder:
▪ Due to lower motor neuron lesion
▪ Bladder fails to contract
▪ Retention and overflow incontinence - 🟩 Mixed Neurogenic Bladder:
▪ Features of both spastic and flaccid types
▪ Unpredictable voiding pattern
🔄 Pathophysiology:
- Nerve injury or dysfunction → loss of voluntary or involuntary bladder control
- Impaired coordination between detrusor muscle and sphincter
- Results in either:
- Overactive bladder (↑ contraction → urgency/incontinence)
- Underactive bladder (↓ contraction → retention)
- Long-term → bladder hypertrophy, infection, vesicoureteral reflux, and renal damage
🔍 Signs and Symptoms:
🟢 Spastic Bladder: 🔸 Urinary urgency and frequency
🔸 Incontinence (urge type)
🔸 No sensation of fullness
🔸 Nocturia
🔵 Flaccid Bladder: 🔸 Urinary retention
🔸 Overflow incontinence (dribbling)
🔸 Sensation of incomplete voiding
🔸 Increased risk of infection
🟡 Common to Both: 🔸 Recurrent UTIs
🔸 Suprapubic pain or fullness
🔸 Constipation (common comorbidity)
🔸 Kidney dysfunction (late sign)
🧪 Diagnosis:
🧫 Urinalysis & Culture: To detect infections
🧲 Bladder Scan/Ultrasound: For post-void residual urine
📈 Urodynamic Studies:
▪ Evaluate detrusor activity, capacity, compliance
▪ Identify detrusor-sphincter dyssynergia
🔎 Cystoscopy: To assess bladder lining
🧬 Renal Function Tests: BUN, creatinine
🧠 MRI/CT scan of spine or brain: To detect neurological pathology
💊 Medical Management:
✅ Anticholinergic drugs (e.g., oxybutynin, tolterodine) – for overactive bladder
✅ Beta-3 agonists (mirabegron) – relax bladder muscle
✅ Cholinergic agents (bethanechol) – stimulate bladder contraction in flaccid type
✅ Alpha-blockers – help relax urethral sphincter in retention
✅ Botulinum toxin injections – relax overactive bladder
✅ Antibiotics – for recurrent UTIs
🏥 Surgical/Procedural Management:
🔧 Clean Intermittent Catheterization (CIC):
▪ First-line for retention and flaccid bladder
🔧 Indwelling catheterization or suprapubic catheter – if CIC is not feasible
🔧 Bladder augmentation (augmentation cystoplasty):
▪ Used when bladder capacity is low
🔧 Urinary diversion (e.g., ileal conduit):
▪ For severe bladder damage
🔧 Sphincterotomy or stent placement:
▪ For detrusor-sphincter dyssynergia
🔧 Sacral nerve modulation (e.g., InterStim):
▪ Stimulates bladder nerves to restore control
🧑⚕️ Nursing Management:
🩺 Assessment:
▪ Monitor urinary output, bladder fullness
▪ Assess for UTI signs: fever, cloudy urine, dysuria
▪ Maintain intake-output chart
💉 Interventions:
▪ Teach clean intermittent catheterization
▪ Maintain catheter care if indwelling
▪ Encourage scheduled toileting (bladder training)
▪ Maintain perineal hygiene
▪ Promote bowel regularity (avoid constipation)
📚 Patient Education:
▪ Recognize symptoms of UTI
▪ Importance of catheter care and hand hygiene
▪ Fluid intake – neither excess nor restriction
▪ Avoid bladder irritants
▪ Long-term follow-up with urologist or neurologist
🥗 Nutritional Consideration:
✅ Encourage:
💧 Adequate hydration – 1.5–2.5 L/day (as advised)
🍊 Cranberry juice or Vitamin C-rich foods – reduce UTI risk
🥦 High-fiber diet – to prevent constipation
🥣 Balanced nutrition – for healing and strength
❌ Avoid:
⚠️ Caffeine, alcohol, carbonated drinks – bladder irritants
⚠️ Spicy and acidic foods – worsen urgency and frequency
⚠️ High-sugar diet – increases UTI risk in diabetic patients
⚠️ Complications:
❗ Recurrent UTIs
❗ Bladder stones
❗ Vesicoureteral reflux
❗ Renal damage/failure
❗ Incontinence-associated dermatitis
❗ Autonomic dysreflexia (in spinal cord injury)
❗ Social isolation, depression
✅ Key Points:
🔹 Neurogenic bladder results from neurological damage to bladder control mechanisms
🔹 Can be spastic (overactive) or flaccid (underactive)
🔹 Requires lifelong management and monitoring
🔹 Early intervention helps prevent renal complications
🔹 Nursing care includes catheterization, infection prevention, and patient education
🔹 Diet, hydration, and hygiene are crucial in management
🟣🚻 URETHRAL DISORDERS
📘 Definition:
Urethral disorders are a group of medical conditions that affect the urethra, the tube responsible for carrying urine from the bladder to the outside of the body. These disorders can lead to pain, obstruction, incontinence, or infection.
⚠️ Causes:
🔹 Infections – bacterial urethritis (e.g., E. coli, Neisseria gonorrhoeae, Chlamydia)
🔹 Trauma – catheterization, pelvic fracture, sexual injury
🔹 Congenital anomalies – posterior urethral valves, hypospadias
🔹 Inflammatory conditions – autoimmune (e.g., Reiter’s syndrome)
🔹 Tumors – benign or malignant
🔹 Strictures – due to fibrosis from injury, surgery, or infection
🔹 Hormonal changes – postmenopausal thinning in females
🔹 Neurological conditions – affecting urethral sphincter tone
🧬 Types of Urethral Disorders:
- 🔴 Urethritis – Inflammation of the urethra (infectious or non-infectious)
- 🟠 Urethral Stricture – Narrowing due to scarring or fibrosis
- 🟡 Urethral Diverticulum – Outpouching of urethral wall, more common in females
- 🟢 Urethral Syndrome – UTI-like symptoms without proven infection
- 🔵 Urethral Prolapse – Mucosal protrusion through the urethral opening (common in elderly women or young girls)
- 🟣 Urethral Carcinoma – Rare malignant tumor of urethral lining
- ⚪ Congenital Defects – Hypospadias, epispadias, posterior urethral valves
🔄 Pathophysiology:
▪ Inflammation, trauma, infection, or fibrosis causes narrowing or dysfunction of the urethra
▪ Leads to impaired urine flow, stasis, and increased risk of infection or retention
▪ In diverticula, urine collects in the pouch → causes infection and dribbling
▪ In strictures, resistance to flow causes backpressure on the bladder and kidneys
🔍 Signs and Symptoms:
🔸 Burning or pain during urination (dysuria)
🔸 Urinary frequency and urgency
🔸 Weak urine stream or interrupted flow
🔸 Urinary retention
🔸 Dribbling after urination
🔸 Blood in urine (hematuria)
🔸 Urethral discharge (in infections)
🔸 Palpable mass in urethral diverticulum
🔸 Pelvic pain or pressure
🔸 Incontinence (if sphincter involved)
🧪 Diagnosis:
🧫 Urinalysis & Culture – Detect infection
🧪 Urethral swab and STD screening – In suspected gonorrhea/chlamydia
🖥️ Ultrasound or Bladder scan – Assess post-void residual
🔎 Urethroscopy / Cystoscopy – Direct visualization of urethra
📈 Uroflowmetry – Assess urine flow pattern and obstruction
📷 Retrograde urethrogram (RUG) – Gold standard for strictures
🧬 Biopsy – If malignancy suspected
💊 Medical Management:
✅ Antibiotics – for infectious urethritis (e.g., ceftriaxone + doxycycline)
✅ Anti-inflammatories – NSAIDs for pain and inflammation
✅ Topical estrogen cream – for atrophic urethritis in postmenopausal women
✅ Alpha-blockers – help with urine flow in mild stricture
✅ Sitz baths and local soothing agents – for prolapse or irritation
✅ Behavioral therapy or pelvic floor rehab – in urethral syndrome
🏥 Surgical Management:
🔧 Urethral Dilation:
▪ Stretching of narrowed segment (temporary relief)
🔧 Internal Urethrotomy:
▪ Endoscopic incision of stricture
🔧 Urethroplasty:
▪ Surgical reconstruction for long or recurrent strictures
🔧 Diverticulectomy:
▪ Surgical excision of urethral diverticulum
🔧 Urethral Sling or Suspension Procedures:
▪ For incontinence related to urethral weakness
🔧 Excision and Reconstruction:
▪ For urethral tumors or prolapse
🧑⚕️ Nursing Management:
🩺 Assessment:
▪ Monitor for urinary flow, pain, and infection signs
▪ Record intake/output and assess for retention
▪ Examine perineal area for discharge, mass, or prolapse
💉 Interventions:
▪ Administer prescribed antibiotics/analgesics
▪ Provide perineal hygiene and comfort measures
▪ Educate on avoiding irritants (perfumed soaps, tight clothing)
▪ Assist in post-op catheter care and wound care
▪ Promote adequate fluid intake
📚 Patient Education:
▪ Complete full antibiotic course
▪ Avoid sexual contact until infection clears (if STD)
▪ Encourage timed voiding and pelvic floor exercises
▪ Follow-up care and when to report recurrence
🥗 Nutritional Consideration:
✅ Encourage:
💧 Adequate hydration – flush out bacteria
🍊 Vitamin C / cranberry juice – maintain urinary acidity
🥣 Fiber-rich diet – prevent constipation (which worsens urethral pressure)
❌ Avoid:
⚠️ Caffeine, spicy foods, alcohol – bladder and urethral irritants
⚠️ Carbonated drinks – can worsen symptoms
⚠️ Complications:
❗ Recurrent UTIs
❗ Urinary retention
❗ Hydronephrosis (if chronic obstruction)
❗ Renal damage
❗ Sepsis (from untreated infections)
❗ Urethral abscess
❗ Fistula formation (in severe inflammation or malignancy)
❗ Social embarrassment due to incontinence
✅ Key Points:
🔹 Urethral disorders include infective, structural, functional, and congenital types
🔹 Early symptoms include dysuria, dribbling, or weak stream
🔹 Diagnosis involves urine tests, imaging, urethroscopy, and flow studies
🔹 Strictures and diverticula often need surgical correction
🔹 Nurses play a critical role in infection control, catheter care, and patient education
🔹 Diet, hygiene, and hydration are essential in both treatment and prevention
🔥🧫 URETHRITIS
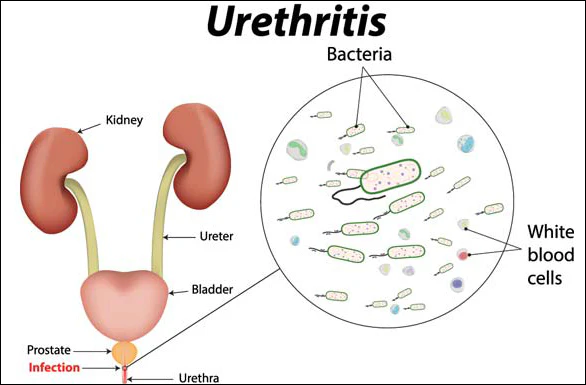
📘 Definition:
Urethritis is the inflammation of the urethra, the tube that carries urine from the bladder to the outside of the body.
It is commonly caused by bacterial infections (especially sexually transmitted infections), but may also result from chemical irritation or trauma.
⚠️ Causes:
🔹 Infectious Causes:
- Sexually transmitted infections (STIs):
▪ Neisseria gonorrhoeae → Gonococcal urethritis
▪ Chlamydia trachomatis → Nongonococcal urethritis
▪ Mycoplasma genitalium
▪ Trichomonas vaginalis
▪ Herpes simplex virus - Bacterial infections (non-STD):
▪ E. coli, Klebsiella, Proteus (commonly in females or catheterized patients)
🔸 Non-infectious Causes:
- Chemical irritants (e.g., soaps, spermicides, bubble bath)
- Urinary catheterization trauma
- Radiation therapy
- Autoimmune diseases (e.g., Reiter’s syndrome)
🧬 Types:
- 🟥 Gonococcal Urethritis (GU):
▪ Caused by Neisseria gonorrhoeae
▪ More purulent and acute presentation - 🟦 Nongonococcal Urethritis (NGU):
▪ Most often caused by Chlamydia trachomatis
▪ Less discharge, often subclinical - 🟨 Nonspecific Urethritis:
▪ No clear bacterial cause identified
▪ May be due to irritation, allergic reaction, or autoimmune disorder
🔄 Pathophysiology:
- Pathogens or irritants invade the urethral mucosa
- Trigger inflammatory response
- Mucosal edema, infiltration of immune cells
- Results in pain, discharge, and urinary symptoms
- Can ascend → prostatitis, epididymitis, or pelvic inflammatory disease (PID)
🔍 Signs and Symptoms:
🔸 Burning or pain during urination (dysuria)
🔸 Urethral discharge (clear, white, yellow, or green)
🔸 Urinary frequency and urgency
🔸 Itching or irritation at urethral opening
🔸 Hematuria (rare)
🔸 Pain during intercourse (in females)
🔸 In men: testicular pain or scrotal swelling (if infection spreads)
🚨 Some cases may be asymptomatic, especially in women
🧪 Diagnosis:
🧫 Urinalysis: Pyuria (WBCs), no significant bacteria in NGU
🧪 Urethral swab or first-void urine test:
▪ NAAT (Nucleic Acid Amplification Test) for Chlamydia, Gonorrhea
🔬 Gram stain of urethral discharge:
▪ Intracellular gram-negative diplococci = gonorrhea
🩺 STD panel: Test for Trichomonas, HSV, HIV, Syphilis
🩻 Cystoscopy (rare): If symptoms persist without infection
💊 Medical Management:
✅ Antibiotics (based on cause):
- 🔸 Gonococcal Urethritis:
▪ Ceftriaxone 500–1000 mg IM + Doxycycline 100 mg BID × 7 days - 🔹 Nongonococcal Urethritis:
▪ Doxycycline 100 mg BID × 7 days or
▪ Azithromycin 1g single dose - 🔸 Trichomonas infection:
▪ Metronidazole 2g single dose
✅ Pain Relief: NSAIDs, warm sitz baths
✅ Hydration: Encourage fluids to flush urethra
✅ Avoid sexual activity until treatment is completed and symptoms resolve
🏥 Surgical/Procedural Management:
🔧 Not usually required, but in complicated or chronic cases:
▪ Urethral dilation – for post-inflammatory stricture
▪ Cystoscopy – for persistent symptoms
▪ Abscess drainage – if any periurethral abscess forms
🧑⚕️ Nursing Management:
🩺 Assessment:
▪ Record symptoms: pain, discharge, urinary flow
▪ Check for fever, tenderness, signs of complications
▪ Assess sexual history sensitively and confidentially
💉 Interventions:
▪ Administer antibiotics as prescribed
▪ Encourage fluid intake
▪ Provide genital hygiene education
▪ Apply warm compress for local discomfort
📚 Patient Education:
▪ Importance of completing full antibiotic course
▪ Abstain from sexual activity until treatment completion
▪ Use of condoms to prevent reinfection
▪ Inform and treat sexual partners
▪ Return for follow-up testing
🥗 Nutritional Consideration:
✅ Encourage:
💧 Fluids (2–3 L/day) – helps clear infection
🍊 Vitamin C-rich diet – helps acidify urine
🥗 Balanced diet – supports immune function
❌ Avoid:
⚠️ Caffeine, spicy foods, alcohol – may irritate urinary tract
⚠️ Artificial sweeteners – bladder irritants
⚠️ Complications:
❗ Ascending infection → Prostatitis, Epididymitis (in men)
❗ Pelvic Inflammatory Disease (PID) → infertility (in women)
❗ Chronic urethral strictures
❗ Urethral abscess formation
❗ Recurrent infections
❗ Increased risk of HIV transmission if untreated
✅ Key Points:
🔹 Urethritis is most commonly infectious and may be sexually transmitted
🔹 Gonorrhea and Chlamydia are the most frequent causes
🔹 Prompt diagnosis and treatment prevent complications
🔹 Education on safe sex practices and partner notification is essential
🔹 Nurses play a vital role in assessment, treatment adherence, hygiene, and counseling.
🔵🔬 DISORDERS OF THE PROSTATE
📘 Definition:
Prostatic disorders refer to any disease condition affecting the prostate gland, a small gland located below the bladder in males that helps produce seminal fluid. These disorders can be benign or malignant, and may affect urinary and sexual function.
⚠️ Causes:
🔹 Hormonal changes with aging
🔹 Bacterial infections
🔹 Family history of prostate cancer
🔹 Autoimmune responses
🔹 Chronic inflammation
🔹 Lifestyle factors – smoking, obesity, high-fat diet
🔹 Sexually transmitted infections
🧬 Types of Prostatic Disorders:
- 🟢 Benign Prostatic Hyperplasia (BPH):
▪ Non-cancerous enlargement of the prostate, common in older men - 🔴 Prostatitis:
▪ Inflammation of the prostate
▪ Can be acute, chronic bacterial, chronic non-bacterial, or asymptomatic - ⚫ Prostate Cancer:
▪ Malignant tumor of prostate tissue
▪ Most common cancer in men over 50 years
🔄 Pathophysiology:
➤ BPH:
▪ Age-related hormonal imbalance (↑ estrogen/androgen ratio)
▪ Leads to glandular hyperplasia
▪ Enlarged prostate compresses urethra → urinary outflow obstruction
➤ Prostatitis:
▪ Invasion of prostate tissue by pathogens (bacteria/STIs)
▪ Inflammation → edema, pain, and urinary symptoms
➤ Prostate Cancer:
▪ Genetic mutations in prostate cells
▪ Uncontrolled growth → tumor formation
▪ May invade surrounding tissues or metastasize (especially to bones)
🔍 Signs and Symptoms:
🔸 Common to All:
▪ Weak urine stream
▪ Urgency and frequency
▪ Nocturia
▪ Incomplete bladder emptying
▪ Hesitancy in starting urination
▪ Dribbling after urination
🔵 Prostatitis-specific:
▪ Painful urination (dysuria)
▪ Lower abdominal, pelvic, or perineal pain
▪ Fever, chills (acute)
▪ Painful ejaculation
▪ Hematospermia (blood in semen)
🔴 Prostate cancer-specific:
▪ Often asymptomatic in early stages
▪ Bone pain (in metastasis)
▪ Erectile dysfunction
▪ Hematuria
▪ Weight loss, fatigue (late signs)
🧪 Diagnosis:
🧬 Digital Rectal Examination (DRE):
▪ Palpate size, shape, and consistency of the prostate
🩺 Prostate-Specific Antigen (PSA) blood test:
▪ Elevated in cancer, BPH, and prostatitis
📸 Transrectal Ultrasound (TRUS):
▪ Imaging of prostate structure
📈 Urine flow studies:
▪ Assess degree of obstruction
🔬 Prostate biopsy:
▪ Confirm cancer diagnosis
🧫 Urine culture / semen analysis:
▪ For prostatitis
🧲 MRI, Bone scan, CT scan:
▪ Staging of prostate cancer
💊 Medical Management:
✅ For BPH:
▪ Alpha-blockers (e.g., tamsulosin) – relax prostate muscles
▪ 5-alpha-reductase inhibitors (e.g., finasteride) – shrink prostate
▪ Combination therapy
▪ Herbal therapy (e.g., saw palmetto – with caution)
✅ For Prostatitis:
▪ Antibiotics (fluoroquinolones, doxycycline)
▪ NSAIDs for pain and inflammation
▪ Muscle relaxants
▪ Warm sitz baths
▪ Hydration and sexual abstinence (during acute phase)
✅ For Prostate Cancer:
▪ Watchful waiting/active surveillance (for early-stage cancer)
▪ Hormonal therapy (androgen deprivation)
▪ Radiation therapy
▪ Chemotherapy
▪ Immunotherapy
▪ Targeted therapy
🏥 Surgical Management:
🔧 Transurethral Resection of the Prostate (TURP):
▪ Most common for BPH
▪ Removes obstructing part of the prostate
🔧 Open prostatectomy:
▪ For very large prostates
🔧 Prostatectomy (radical):
▪ For prostate cancer (removal of entire prostate)
🔧 Laser therapy or microwave therapy:
▪ Minimally invasive options
🔧 Cryosurgery or HIFU (High-Intensity Focused Ultrasound):
▪ For localized prostate cancer
🧑⚕️ Nursing Management:
🩺 Assessment:
▪ Monitor urinary output
▪ Pain assessment
▪ Observe for hematuria or infection signs post-surgery
💉 Post-op Care (TURP/prostatectomy):
▪ Maintain continuous bladder irrigation (CBI)
▪ Monitor for clot retention
▪ Teach catheter care
▪ Manage incontinence and dribbling post-catheter removal
📚 Patient Education:
▪ Limit fluids before bedtime
▪ Avoid caffeine/alcohol
▪ Practice timed voiding
▪ Teach about PSA monitoring and follow-up
▪ Avoid heavy lifting or straining post-surgery
▪ Teach early signs of complications
🥗 Nutritional Consideration:
✅ Encourage:
🥦 High-fiber diet – prevent constipation
🍅 Lycopene-rich foods (tomatoes) – prostate-protective
🥬 Cruciferous vegetables (broccoli, cauliflower)
💧 Adequate hydration
❌ Avoid:
⚠️ Caffeine and alcohol – may worsen symptoms
⚠️ High-fat red meats – associated with increased prostate cancer risk
⚠️ Spicy foods – may irritate bladder
⚠️ Complications:
❗ Urinary retention
❗ Recurrent UTIs
❗ Hematuria
❗ Erectile dysfunction (especially post-surgery)
❗ Incontinence
❗ Bladder or kidney damage
❗ Metastasis (in prostate cancer)
✅ Key Points:
🔹 Prostate disorders include BPH, prostatitis, and prostate cancer
🔹 Symptoms often overlap → diagnosis requires PSA, DRE, and imaging
🔹 BPH is benign but can affect quality of life
🔹 Prostate cancer may be asymptomatic early, but treatable if caught early
🔹 Nurses play a vital role in monitoring, catheter care, patient education, and post-op recovery
🔹 Diet, lifestyle changes, and regular screening improve outcomes
🔴🧬 PROSTATITIS
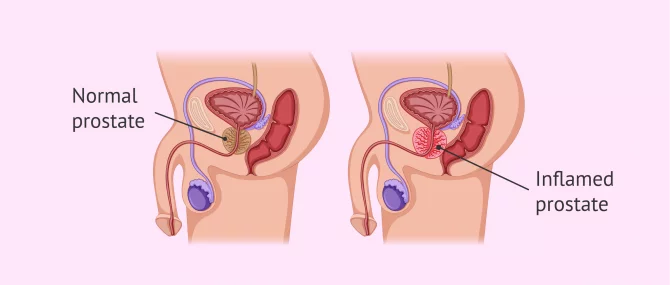
📘 Definition:
Prostatitis is the inflammation of the prostate gland, which may be acute or chronic, and caused by infectious or non-infectious factors.
🧠 It affects men of all ages but is most common in men aged 30–50 years.
⚠️ Causes:
🔹 Infectious Causes:
- Bacterial infections (most common in acute prostatitis):
▪ Escherichia coli (E. coli)
▪ Klebsiella
▪ Proteus
▪ Pseudomonas aeruginosa
▪ Enterococcus faecalis - Sexually transmitted infections (STIs):
▪ Neisseria gonorrhoeae
▪ Chlamydia trachomatis
▪ Mycoplasma genitalium - Recurrent urinary tract infections
- Urethral catheterization or instrumentation (e.g., cystoscopy)
🔸 Non-Infectious / Inflammatory Causes:
- Autoimmune response
- Pelvic floor muscle dysfunction
- Stress or anxiety
- Trauma to the perineum (e.g., cycling, horseback riding)
- Urine reflux into prostatic ducts
🧬 Types of Prostatitis (Based on NIH Classification):
1. 🟥 Acute Bacterial Prostatitis (ABP):
- Sudden onset caused by bacterial infection
- Severe symptoms: fever, chills, dysuria, pelvic pain
- Often associated with UTI or catheter use
2. 🟦 Chronic Bacterial Prostatitis (CBP):
- Low-grade infection persisting >3 months
- Recurrent UTIs with the same pathogen
- Symptoms may be mild or intermittent
3. 🟨 Chronic Prostatitis / Chronic Pelvic Pain Syndrome (CP/CPPS):
- Most common type (~90% of cases)
- Unknown cause (non-bacterial)
- Pelvic or perineal pain >3 months
- No identifiable bacteria in cultures
- Subtypes:
🔹 Inflammatory (WBCs present)
🔹 Non-inflammatory (no WBCs)
4. 🟩 Asymptomatic Inflammatory Prostatitis:
- No symptoms
- Inflammation detected incidentally (e.g., during fertility testing or prostate biopsy)
- No treatment usually required
🔄🧠 PATHOPHYSIOLOGY OF PROSTATITIS
🧬 1. Acute Bacterial Prostatitis (ABP):
▪ Bacteria ascend from the urethra, bladder, or rectum → enter prostatic ducts
▪ Infection triggers inflammation → edema, hyperemia of the prostate
▪ Obstruction of ducts and prostatic swelling → urinary retention, pain, and systemic symptoms
▪ Can extend to surrounding tissues if not treated → abscess or sepsis
🧬 2. Chronic Bacterial Prostatitis (CBP):
▪ Occurs when bacteria persist in prostatic tissue despite treatment
▪ Prostate acts as a reservoir for recurrent UTIs
▪ Inflammation becomes chronic, often with subtle or no systemic symptoms
▪ Associated with fibrosis and scarring
🧬 3. Chronic Prostatitis/Chronic Pelvic Pain Syndrome (CP/CPPS):
▪ Exact mechanism unknown
▪ May involve:
🔹 Autoimmune response
🔹 Pelvic floor muscle spasm
🔹 Nerve hypersensitivity
🔹 Psychological stress
▪ No identifiable pathogen, but inflammation or pain persists
🚨🧍♂️ SIGNS AND SYMPTOMS OF PROSTATITIS
🟥 Acute Bacterial Prostatitis:
🔸 High fever, chills
🔸 Painful urination (dysuria)
🔸 Pelvic or perineal pain
🔸 Suprapubic or lower back pain
🔸 Painful ejaculation
🔸 Difficulty in urination / urinary retention
🔸 Tender, swollen prostate on rectal exam
🔸 Nausea, malaise (systemic infection signs)
🔸 Cloudy or foul-smelling urine
🟦 Chronic Bacterial Prostatitis:
🔸 Recurrent UTI symptoms
🔸 Mild pelvic or perineal discomfort
🔸 Pain in scrotum, penis, or rectum
🔸 Ejaculatory pain or sexual dysfunction
🔸 Low-grade fever (occasional)
🔸 Symptoms lasting >3 months
🟨 Chronic Prostatitis/CPPS:
🔸 Chronic pelvic pain (>3 months)
🔸 Perineal pressure or burning
🔸 Discomfort during or after urination
🔸 Pain with ejaculation
🔸 Fatigue, irritability
🔸 No identifiable infection
🟩 Asymptomatic Inflammatory Prostatitis:
🔸 No symptoms
🔸 Inflammation discovered incidentally (e.g., infertility work-up)
🔍🧪 DIAGNOSIS OF PROSTATITIS
🧫 Laboratory Tests:
✅ Urinalysis and Urine Culture:
▪ Check for pyuria (WBCs), bacteriuria, and identify pathogens
✅ Prostate-Specific Antigen (PSA):
▪ May be elevated in acute prostatitis
▪ Used with caution (not specific for cancer here)
✅ Expressed Prostatic Secretion (EPS) Test (4-glass test):
▪ Collects urine before and after prostate massage
▪ Helps differentiate between types of prostatitis
✅ Semen Analysis:
▪ Check for WBCs, infection, and sperm motility (in infertility cases)
🧬 Imaging & Examination:
📈 Digital Rectal Exam (DRE):
▪ Prostate may feel tender, swollen, or boggy in acute cases
🖥️ Transrectal Ultrasound (TRUS):
▪ Detect abscesses or prostate enlargement
🧲 MRI Pelvis (if needed):
▪ For chronic cases or to rule out complications
💊🩺 MEDICAL MANAGEMENT OF PROSTATITIS
🟥 1. Acute Bacterial Prostatitis (ABP):
✅ Hospitalization may be required if severe
✅ Empirical Antibiotic Therapy (adjust after culture report):
▪ Fluoroquinolones (Ciprofloxacin, Levofloxacin)
▪ Trimethoprim-Sulfamethoxazole (TMP-SMX)
▪ Cephalosporins or Aminoglycosides in resistant cases
⏳ Duration: Usually 2–4 weeks
✅ Supportive Care:
▪ NSAIDs for pain (e.g., ibuprofen)
▪ Antipyretics for fever
▪ Bed rest during acute phase
▪ Increased fluid intake
▪ Stool softeners (to avoid straining)
🟦 2. Chronic Bacterial Prostatitis (CBP):
✅ Long-term Antibiotic Therapy (at least 4–6 weeks):
▪ Fluoroquinolones (most effective due to prostatic penetration)
▪ Tetracyclines (e.g., doxycycline) as alternatives
✅ Alpha-blockers (e.g., tamsulosin) – relieve urinary obstruction
✅ Anti-inflammatory drugs – reduce chronic pelvic pain
✅ Prostatic massage therapy (sometimes used with antibiotics)
✅ Management of recurrent UTIs and patient education
🟨 3. Chronic Prostatitis / Chronic Pelvic Pain Syndrome (CP/CPPS):
✅ Multimodal approach needed:
▪ Alpha-blockers – for voiding symptoms
▪ NSAIDs or COX-2 inhibitors – for inflammation and pain
▪ Neuropathic pain agents (e.g., amitriptyline, gabapentin)
▪ Muscle relaxants – for pelvic floor tension
▪ Biofeedback, pelvic floor physiotherapy
▪ Stress reduction techniques – mindfulness, relaxation
▪ Antibiotics trial – only if infection suspected
▪ Botulinum toxin injections (in selected refractory cases)
🟩 4. Asymptomatic Inflammatory Prostatitis:
❗ No specific treatment required
☑️ Manage if associated with infertility
☑️ Monitor PSA if elevated
🏥🔧 SURGICAL / PROCEDURAL MANAGEMENT OF PROSTATITIS
🛠️ 1. Indications for Surgical Intervention:
🔸 Recurrent, chronic, or refractory cases
🔸 Prostatic abscess formation
🔸 Severe bladder outlet obstruction
🔸 Suspected structural abnormalities or complications
🔧 2. Common Surgical or Procedural Options:
✅ Transurethral Resection of the Prostate (TURP):
▪ Indicated in patients with significant urinary obstruction due to chronic prostatitis
▪ Removes prostatic tissue causing blockage
▪ Relieves symptoms but not used routinely
✅ Prostatic Abscess Drainage:
▪ Done via Transrectal or Transperineal ultrasound-guided aspiration
▪ Required in acute prostatitis not responding to antibiotics
✅ Suprapubic Catheterization:
▪ In acute retention when urethral catheter is not safe due to inflamed prostate
✅ Surgical Prostatectomy (rare):
▪ Used only in severe, non-resolving, or complicated cases
▪ Not a first-line option
🧑⚕️💼 NURSING MANAGEMENT OF PROSTATITIS
🩺 1. Assessment:
🔍 Conduct thorough history and physical assessment:
▪ Urinary symptoms – frequency, urgency, dysuria, hesitancy
▪ Pain – location (perineal, lower back, suprapubic, rectal)
▪ Fever, chills (in acute cases)
▪ Sexual function (painful ejaculation, libido changes)
▪ Past history of UTIs, STIs, or catheter use
🔍 Digital Rectal Examination (DRE) – gently assess for tenderness and swelling (by physician)
💉 2. Symptom Management and Interventions:
🩹 For Acute Prostatitis (ABP):
✅ Administer prescribed antibiotics on time
✅ Monitor for fever, sepsis, and retention
✅ Pain management: NSAIDs as prescribed
✅ Encourage bed rest during the acute phase
✅ Apply warm compresses or sitz baths for perineal discomfort
✅ Monitor and record vital signs regularly
🧻 For Urinary Symptoms:
✅ Encourage frequent voiding – don’t delay urination
✅ Monitor urine output and characteristics (color, smell, volume)
✅ Assist with catheter care if retention occurs
✅ Educate on double voiding technique to reduce retention
📚 3. Education and Psychosocial Support:
🧠 Educate the patient on:
▪ Disease process and treatment duration
▪ Importance of completing full antibiotic course
▪ Avoid alcohol, caffeine, and spicy foods – bladder irritants
▪ Avoid prolonged sitting or activities that put pressure on perineum (e.g., cycling)
▪ Safe sexual practices (if STI is the cause)
▪ Use of condoms and partner notification
💬 Provide emotional support:
▪ Address concerns about sexual health and fertility
▪ Provide privacy, maintain non-judgmental communication
▪ Refer for psychological counseling or pelvic floor therapy in chronic CPPS
💧 4. Fluid and Nutritional Support:
▪ Encourage adequate fluid intake (2–3 liters/day if not contraindicated)
▪ Maintain nutritionally balanced diet to support immune response
▪ Advise high-fiber intake to prevent constipation (which increases pelvic pressure)
🩺 5. Monitoring and Follow-up:
📅 Schedule follow-up for:
▪ PSA levels (if initially elevated)
▪ Urine culture/sensitivity to assess antibiotic response
▪ Recheck for symptom resolution or progression to chronic prostatitis
▪ Educate on the importance of early reporting of new or recurring symptoms
⚠️ 6. Emergency Management (for Acute Retention or Sepsis):
🚨 Recognize and report:
▪ Sudden urinary retention
▪ Fever > 101°F, hypotension
▪ Confusion or lethargy (signs of sepsis)
▪ Prepare for catheterization or surgical intervention
🥗🍽️ NUTRITIONAL CONSIDERATION IN PROSTATITIS
✅ Encouraged:
💧 Plenty of fluids (2–3 liters/day unless restricted)
▪ Helps flush bacteria from urinary tract
▪ Reduces urinary stasis and discomfort
🥦 Anti-inflammatory diet:
▪ Rich in green leafy vegetables, berries, tomatoes, and fish (omega-3s)
🍅 Lycopene-rich foods:
▪ Tomatoes, watermelon – support prostate health
🍊 Vitamin C-rich fruits (oranges, guavas, berries):
▪ Helps boost immunity and maintain urinary tract health
🥣 High-fiber foods:
▪ Whole grains, legumes, vegetables – prevent constipation (which worsens perineal pressure)
❌ Avoided:
⚠️ Caffeine (coffee, cola, energy drinks)
▪ Can irritate bladder and worsen urinary urgency
⚠️ Spicy foods (chili, black pepper)
▪ May increase pelvic discomfort and inflammation
⚠️ Alcohol
▪ Can irritate the bladder and decrease immune response
⚠️ Acidic and carbonated drinks
▪ Can worsen burning sensations during urination
⚠️🧨 COMPLICATIONS OF PROSTATITIS
🟥 Acute Bacterial Prostatitis:
❗ Urinary retention
❗ Prostatic abscess
❗ Urosepsis (systemic infection)
❗ Bladder outlet obstruction
❗ Epididymitis or orchitis (spread of infection)
❗ Chronic prostatitis if not completely treated
🟦 Chronic Bacterial Prostatitis / CPPS:
❗ Recurrent urinary tract infections
❗ Infertility (due to inflammation in semen)
❗ Chronic pelvic pain syndrome
❗ Sexual dysfunction (painful ejaculation, erectile difficulties)
❗ Depression and psychological distress due to long-standing symptoms
❗ Urethral stricture (rare, from scarring)
✅📌 KEY POINTS ON PROSTATITIS
🔹 Prostatitis is inflammation of the prostate, either infectious or non-infectious
🔹 Most common in men aged 30–50 years
🔹 Four types: Acute bacterial, Chronic bacterial, Chronic pelvic pain syndrome, Asymptomatic
🔹 Symptoms include pelvic pain, dysuria, painful ejaculation, and urinary difficulties
🔹 Diagnosis involves urinalysis, PSA, prostate exam, and cultures
🔹 Management includes antibiotics, alpha-blockers, anti-inflammatories, and sometimes surgery
🔹 Nursing care includes monitoring, catheter care, hygiene, pain relief, and patient education
🔹 Diet, hydration, stress reduction, and sexual health counseling are essential in chronic cases
🔹 Untreated prostatitis can lead to severe complications including infertility and sepsis
🔵💥 BENIGN PROSTATIC HYPERPLASIA (BPH)
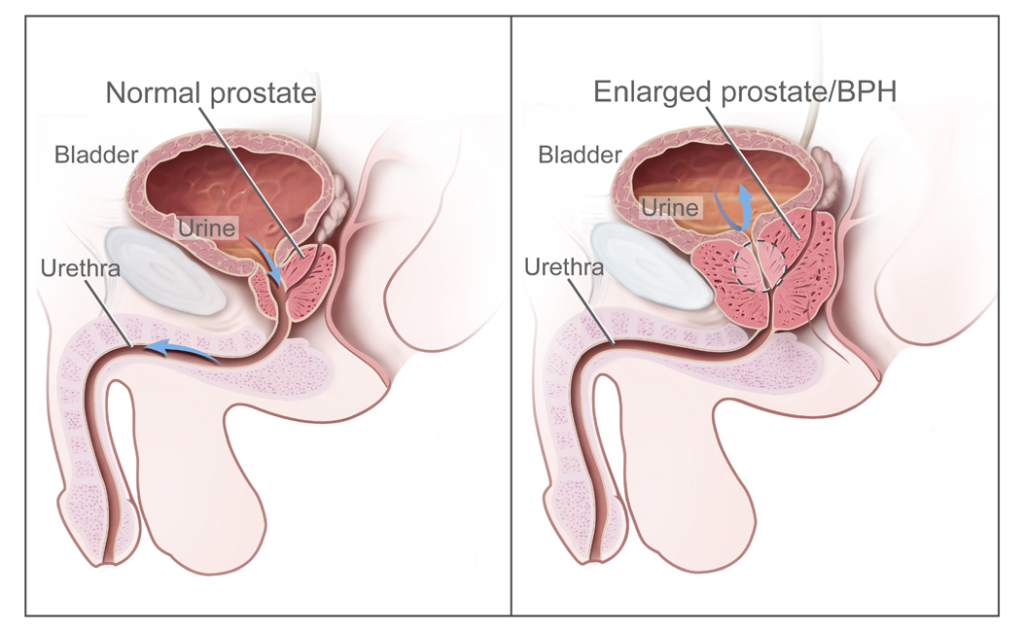
📘 Definition:
Benign Prostatic Hyperplasia (BPH) is a non-cancerous enlargement of the prostate gland, commonly seen in aging men, that causes compression of the urethra and results in lower urinary tract symptoms (LUTS).
🧠 Although benign, BPH can significantly impact quality of life due to urinary difficulties, bladder dysfunction, and even renal issues if untreated.
⚠️ Causes / Risk Factors:
🔹 Primary (Natural Aging Process):
▪ Hormonal changes, especially an increase in the estrogen:testosterone ratio
▪ Accumulation of dihydrotestosterone (DHT) in prostate tissues, stimulating growth
🔸 Other Contributing Risk Factors:
▪ Age > 50 years (main risk factor)
▪ Family history of BPH
▪ Obesity and metabolic syndrome
▪ Sedentary lifestyle
▪ Chronic inflammation of the prostate
▪ Diabetes mellitus and cardiovascular disease
▪ Excessive alcohol or caffeine intake
🧬 Types / Classification of BPH:
🟢 1. Histological Classification:
▪ Based on tissue overgrowth seen microscopically
▪ Involves proliferation of:
- Glandular tissue
- Fibrous tissue
- Smooth muscle components
🔵 2. Anatomical Classification:
▪ Based on zone of enlargement in the prostate
| Zone Affected | Effect |
|---|---|
| Transition Zone | Most commonly involved in BPH |
| Periurethral Region | Causes direct urethral compression |
| Central Zone | Less commonly involved |
🟡 3. Clinical Classification:
- Static (Mechanical) Component:
▪ Due to enlarged prostate physically obstructing the urethra - Dynamic (Functional) Component:
▪ Due to increased smooth muscle tone of the bladder neck and prostate under sympathetic control
🔸 Both components often coexist and contribute to Lower Urinary Tract Symptoms (LUTS) in BPH
🔄🧠 PATHOPHYSIOLOGY OF BPH
🔬 Hormonal Influence:
- Aging leads to ↓ testosterone and relatively ↑ estrogen
- ↑ Estrogen promotes activity of 5-alpha reductase, which converts testosterone → Dihydrotestosterone (DHT)
- DHT stimulates proliferation of prostate stromal and epithelial cells
- Leads to gradual enlargement of the prostate gland, especially in the transition zone
🔄 Obstruction Mechanism:
- The enlarged prostate compresses the urethra
- ↑ bladder outlet resistance → incomplete emptying
- Detrusor muscle hypertrophy develops to compensate
- Long-term pressure → bladder decompensation, residual urine, and even hydronephrosis
🚨🧍♂️ SIGNS AND SYMPTOMS OF BPH
🔵 Lower Urinary Tract Symptoms (LUTS) – divided into Obstructive & Irritative:
🔸 Obstructive (Voiding) Symptoms:
▪ Weak urine stream
▪ Hesitancy (delay in starting urination)
▪ Intermittency (stopping and starting)
▪ Straining to void
▪ Incomplete bladder emptying
▪ Post-void dribbling
🔹 Irritative (Storage) Symptoms:
▪ Increased frequency of urination
▪ Nocturia (waking up at night to urinate)
▪ Urgency
▪ Urge incontinence
▪ Dysuria (rare in BPH, usually infection)
⚠️ Advanced/Complicated Symptoms:
▪ Acute urinary retention
▪ Recurrent urinary tract infections (UTIs)
▪ Bladder stones
▪ Hematuria (in some cases)
▪ Hydronephrosis and renal dysfunction (in severe, neglected cases)
🔍🧪 DIAGNOSIS OF BPH
🧫 Laboratory Tests:
✅ Urinalysis:
▪ To rule out infection or hematuria
✅ Serum PSA (Prostate-Specific Antigen):
▪ May be mildly elevated in BPH
▪ Helps differentiate from prostate cancer (but not diagnostic alone)
🩺 Clinical Assessment:
✅ Digital Rectal Examination (DRE):
▪ Prostate is enlarged, smooth, firm, and non-tender
🖥️ Imaging & Functional Tests:
✅ Ultrasound (KUB or TRUS – transrectal ultrasound):
▪ Measures prostate volume, residual urine, and bladder wall thickness
✅ Post-Void Residual (PVR) Volume Measurement:
▪ Assesses incomplete bladder emptying
✅ Uroflowmetry:
▪ Measures flow rate (reduced in BPH)
✅ Cystoscopy:
▪ Used in complex cases to evaluate obstruction or hematuria
✅ Urodynamic Studies:
▪ To assess bladder pressure, especially in patients with inconclusive symptoms
💊🩺 MEDICAL MANAGEMENT OF BPH
✅ 1. Watchful Waiting (for Mild Symptoms):
▪ Regular monitoring of symptoms
▪ Lifestyle changes:
🔹 Timed voiding
🔹 Avoid fluids before bedtime
🔹 Limit caffeine and alcohol
🔹 Reduce constipation
💊 2. Pharmacological Therapy:
🔹 Alpha-1 Adrenergic Blockers (Relax prostate and bladder neck smooth muscles):
▪ Tamsulosin, Alfuzosin, Doxazosin, Terazosin
▪ Quick symptom relief (within days to weeks)
📝 Side Effects: Dizziness, orthostatic hypotension, retrograde ejaculation
🔸 5-Alpha-Reductase Inhibitors (Shrink prostate size by blocking DHT formation):
▪ Finasteride, Dutasteride
▪ Effective in large prostates
🕒 Takes 3–6 months for effect
📝 Side Effects: Decreased libido, erectile dysfunction, gynecomastia
🔹 Combination Therapy:
▪ Alpha-blocker + 5-alpha-reductase inhibitor
▪ More effective in moderate to severe cases
🔸 Phosphodiesterase-5 Inhibitors:
▪ Tadalafil (Cialis) – useful for men with both BPH and erectile dysfunction
🔹 Anticholinergics / Beta-3 Agonists:
▪ For overactive bladder symptoms (frequency/urgency)
▪ Used cautiously in those with high residual urine
⚠️ Avoid Medications That Can Worsen BPH Symptoms:
❌ Antihistamines
❌ Decongestants
❌ Tricyclic antidepressants
🏥🔧 SURGICAL MANAGEMENT OF BPH
🛠️ 1. Minimally Invasive Procedures:
🔧 Transurethral Microwave Thermotherapy (TUMT):
▪ Uses heat to destroy excess prostate tissue
▪ Office-based, done under local anesthesia
🔧 Transurethral Needle Ablation (TUNA):
▪ Radiofrequency energy destroys tissue
▪ Less bleeding, faster recovery
🔧 Prostatic Urethral Lift (UroLift):
▪ Mechanical retraction of prostate lobes
▪ Preserves sexual function
▪ Office-based procedure
🔧 Water Vapor Thermal Therapy (Rezūm):
▪ Injects steam into prostate → tissue necrosis
▪ Short procedure time, preserves ejaculatory function
🏥 2. Standard Surgical Procedures:
🧰 Transurethral Resection of the Prostate (TURP):
▪ Gold standard for moderate to severe BPH
▪ Removes obstructing prostate tissue via endoscope
📝 Complications: Bleeding, retrograde ejaculation, TUR syndrome
🧰 Transurethral Incision of the Prostate (TUIP):
▪ Incisions made in prostate to relieve pressure
▪ Suitable for small prostates
🧰 Open Prostatectomy (Retropubic/Suprapubic):
▪ For very large prostates (>80–100g) or with bladder stones
▪ Invasive; longer recovery time
📝 Complications: Incontinence, impotence, bleeding
🧑⚕️📋 NURSING MANAGEMENT OF BPH
🩺 1. Assessment:
🔍 Collect thorough health history: ▪ Onset, duration, and severity of urinary symptoms
▪ Frequency, urgency, hesitancy, nocturia
▪ Incomplete voiding, dribbling, straining
▪ History of urinary tract infections, retention, hematuria
▪ Impact on quality of life (e.g., sleep disruption, social embarrassment)
🔍 Physical assessment:
▪ Monitor abdominal distension (bladder enlargement)
▪ Assist physician with Digital Rectal Exam (DRE)
▪ Observe for signs of urinary retention or infection
💉 2. Monitor and Manage Symptoms:
✅ Observe urinary patterns: ▪ Keep intake-output chart
▪ Monitor for post-void residual using bladder scanner
▪ Encourage timed voiding and double voiding
✅ Administer medications as prescribed: ▪ Alpha-blockers, 5-alpha-reductase inhibitors
▪ Monitor for side effects (hypotension, dizziness, sexual dysfunction)
✅ Pain management: ▪ Administer analgesics if needed (especially after procedures like TURP)
💧 3. Promote Effective Urination:
🚽 Encourage: ▪ Privacy and relaxed environment for urination
▪ Sitting or standing positions (whichever facilitates urination)
▪ Warm compress over suprapubic area for relaxation
▪ Timed voiding (every 2–3 hours) to avoid retention
💧 Maintain adequate hydration
▪ Encourage 2–3 L/day (unless contraindicated)
▪ Limit fluid intake before bedtime to reduce nocturia
🛏️ 4. Post-operative Care (e.g., after TURP):
🔹 Maintain Continuous Bladder Irrigation (CBI): ▪ Monitor for clots, bleeding, catheter blockage
▪ Ensure urine output is light pink
▪ Adjust flow rate to maintain clear urine
▪ Secure catheter to avoid tension
▪ Record input vs output (irrigation fluid vs drainage)
🔹 Monitor for TURP Syndrome (water intoxication):
▪ Watch for: confusion, bradycardia, hypotension, nausea
🔹 Provide perineal hygiene and catheter care
▪ Prevent infection and skin breakdown
📚 5. Patient Education:
🧠 Educate patient and family on: ▪ Importance of medication adherence
▪ Avoiding bladder irritants (caffeine, alcohol, spicy foods)
▪ Bladder training techniques
▪ Signs of UTI or acute retention
▪ Avoid straining during bowel movements – use stool softeners
▪ Avoid heavy lifting or prolonged standing post-op
▪ Pelvic floor exercises to improve urinary control
📅 6. Follow-up and Emotional Support:
🤝 Provide: ▪ Psychological support regarding sexual concerns or anxiety
▪ Information on follow-up appointments, PSA monitoring
▪ Support groups if chronic symptoms impact mental well-being
🥗🍽️ NUTRITIONAL CONSIDERATION IN BPH
✅ Recommended Diet for Prostate Health:
🔹 Fluids:
💧 Encourage 2–3 L/day of water intake (unless contraindicated)
▪ Helps flush the bladder
▪ Reduce UTI risk and prevent urinary stasis
▪ Limit fluids 2 hours before bedtime to reduce nocturia
🔹 Anti-inflammatory Foods:
🥦 Green leafy vegetables
🍓 Berries, turmeric, garlic
🥑 Healthy fats (olive oil, flaxseeds)
🔹 Lycopene-Rich Foods:
🍅 Tomatoes, watermelon, pink grapefruit
▪ May help reduce prostate enlargement risk
🔹 Zinc and Selenium:
▪ Found in pumpkin seeds, legumes, and fish
▪ Important for prostate function and immune support
❌ Foods to Avoid or Limit:
⚠️ Caffeine (tea, coffee, energy drinks):
▪ Increases bladder irritability and frequency
⚠️ Alcohol:
▪ Acts as a diuretic and bladder stimulant
▪ May worsen urinary urgency
⚠️ Spicy and acidic foods:
▪ Trigger bladder irritation in some men
⚠️ High-fat red meat and processed foods:
▪ Associated with increased risk of prostate inflammation and possibly cancer
⚠️🧨 COMPLICATIONS OF BPH
🔸 Acute Urinary Retention (AUR):
▪ Sudden, painful inability to urinate – medical emergency
🔸 Chronic Urinary Retention:
▪ Incomplete bladder emptying over time
🔸 Urinary Tract Infections (UTIs):
▪ Due to stasis of urine in bladder
🔸 Bladder Stones:
▪ Form due to stagnant urine and debris buildup
🔸 Hematuria:
▪ Blood in urine from engorged vessels
🔸 Hydronephrosis & Kidney Damage:
▪ Backpressure on ureters and kidneys from prolonged retention
🔸 Bladder Diverticula:
▪ Outpouching of bladder wall due to overdistension
✅📌 KEY POINTS ON BPH
🔹 BPH is a non-cancerous enlargement of the prostate that affects most men after age 50
🔹 Results from hormonal changes, especially involving DHT
🔹 Causes lower urinary tract symptoms (LUTS): hesitancy, weak stream, frequency, urgency
🔹 Diagnosis includes DRE, PSA, ultrasound, uroflowmetry, and PVR measurement
🔹 Medical treatment involves alpha-blockers, 5-alpha-reductase inhibitors, and combination therapy
🔹 Surgical options like TURP are used for moderate to severe or complicated cases
🔹 Nursing care includes symptom monitoring, catheter management, patient education, and post-op support
🔹 Nutrition plays a supportive role — fluids, anti-inflammatory foods, and prostate-healthy nutrients are encouraged
🔹 Complications include retention, infection, renal damage, and impact on quality of life
🔹 Early recognition and consistent follow-up are key to preventing complications
🔵🧬 PROSTATIC STRICTURE
📘 Definition:
A Prostatic Stricture is a narrowing of the prostatic urethra, the portion of the urethra that passes through the prostate gland.
This condition results in obstructed urine flow, commonly due to fibrosis or scarring following infection, inflammation, trauma, or surgery.
🧠 It is a subset of urethral strictures, but located specifically in the prostatic segment of the urethra.
⚠️ Causes:
🔹 Iatrogenic (most common):
▪ Post-surgical complications (especially after TURP – Transurethral Resection of the Prostate)
▪ Post-catheterization trauma
▪ Radiation therapy for prostate cancer
▪ Endoscopic instrumentation or prostate biopsy
🔸 Infectious:
▪ Chronic prostatitis
▪ STIs – gonorrhea, chlamydia
▪ Tuberculosis of the genitourinary tract
🔹 Inflammatory / Autoimmune:
▪ Long-standing prostatic inflammation → fibrosis and narrowing
🔸 Congenital (rare):
▪ Developmental narrowing of the prostatic urethra from birth
🧬 Types / Classification:
🟢 Based on Etiology:
- Iatrogenic Stricture – due to medical intervention
- Infectious Stricture – chronic infections/inflammation
- Congenital Stricture – developmental defect
🔵 Based on Location:
▪ Prostatic Urethra (within the prostate gland)
▪ Can be isolated or extend to membranous urethra
🟡 Based on Severity:
▪ Partial Stricture – mild to moderate narrowing
▪ Complete Stricture – no urine passage (may lead to retention)
🔄🧠 PATHOPHYSIOLOGY OF PROSTATIC STRICTURE
- Initial insult (e.g., surgery, infection, catheter trauma) damages the prostatic urethral lining
- Healing response triggers fibrosis and collagen deposition
- Formation of a dense scar → luminal narrowing
- Increased urethral resistance to urine flow
- Bladder compensates by increasing detrusor pressure
- Over time, results in urinary retention, detrusor hypertrophy, and possibly hydroureter/hydronephrosis
🚨🧍♂️ SIGNS AND SYMPTOMS OF PROSTATIC STRICTURE
🔸 Weak or reduced urinary stream
🔸 Hesitancy or straining during urination
🔸 Intermittent urine flow
🔸 Incomplete bladder emptying
🔸 Dribbling after urination
🔸 Urinary frequency and urgency
🔸 Nocturia
🔸 Painful urination (dysuria)
🔸 Urinary retention (in severe cases)
🔸 Recurrent UTIs
🔸 In rare cases: hematuria or pelvic/perineal discomfort
🔍🧪 DIAGNOSIS OF PROSTATIC STRICTURE
🧫 Urinalysis & Culture:
▪ To rule out UTIs or underlying prostatitis
🩺 Physical Examination:
▪ Digital Rectal Examination (DRE):
🔹 May reveal enlarged or firm prostate
🔹 Tenderness in prostatitis-related cases
📈 Uroflowmetry:
▪ Measures urine flow rate
▪ Decreased peak flow rate and prolonged voiding time
🖥️ Post-Void Residual (PVR) Volume Measurement:
▪ Assesses amount of urine left after voiding
▪ Often elevated in strictures
🔬 Retrograde Urethrogram (RUG):
▪ Gold standard for stricture localization and length
▪ Uses contrast dye under X-ray to visualize narrowing
📷 Cystoscopy (Endoscopy):
▪ Direct visualization of the prostatic urethra
▪ Can assess stricture severity, location, and plan for treatment
🧲 Ultrasound (TRUS) or MRI (if needed):
▪ For complex cases or to assess prostatic tissue and surrounding structures
💊🩺 MEDICAL MANAGEMENT OF PROSTATIC STRICTURE
⚠️ Note: Since prostatic strictures are structural, medical treatment alone is often not curative, but it is used to manage symptoms, prevent infections, and prepare for surgical intervention.
✅ 1. Symptomatic Treatment:
🔹 Alpha-1 Adrenergic Blockers (e.g., Tamsulosin, Alfuzosin):
▪ Reduce smooth muscle tone of prostate and bladder neck
▪ Improve urine flow and decrease voiding pressure
▪ Often used pre-operatively or in mild cases
🔹 Analgesics / NSAIDs:
▪ For pain relief, especially if inflammation is present
▪ Helps with perineal or pelvic discomfort
🔹 Antibiotics:
▪ Used if stricture is associated with chronic or recurrent UTI
▪ E.g., fluoroquinolones or culture-specific antibiotics
🔹 Stool softeners:
▪ Prevent straining during bowel movements, which can worsen urinary symptoms
✅ 2. Monitoring and Lifestyle Support:
💧 Encourage hydration to maintain urine flow
🧻 Promote timed voiding to prevent retention
🚫 Avoid bladder irritants (caffeine, alcohol, spicy foods)
🏥🔧 SURGICAL MANAGEMENT OF PROSTATIC STRICTURE
Surgery is the mainstay of treatment for prostatic stricture, especially when urine flow is significantly obstructed.
🛠️ 1. Urethral Dilation:
🔹 Gradual insertion of increasingly larger dilators to stretch the stricture
🔹 Minimally invasive and outpatient procedure
🔹 Temporary solution — high recurrence rate
🔹 Often used for short, simple strictures
🛠️ 2. Visual Internal Urethrotomy (VIU):
🔹 Endoscopic procedure where the stricture is cut internally using a cold knife or laser
🔹 Performed under local or spinal anesthesia
🔹 Suitable for short strictures (<1.5 cm)
🔹 Quicker recovery, but recurrence is possible
🛠️ 3. Transurethral Resection of Stricture Tissue:
🔹 Used when stricture is associated with TURP scarring or obstructive tissue in the prostatic urethra
🔹 Often performed during follow-up TURP procedures
🔹 Removes fibrotic tissue causing obstruction
🛠️ 4. Urethroplasty (Open Reconstruction):
🔹 Reserved for recurrent or long strictures
🔹 Involves surgical excision of fibrotic tissue and anastomosis of healthy urethral ends
🔹 May use buccal mucosal grafts if needed
🔹 Longer recovery, but higher long-term success rate
🛠️ 5. Perineal Urethrostomy (for severe or failed cases):
🔹 Creating a new urinary opening in the perineum
🔹 Used in complex, recurrent, or multi-level strictures
🔹 Allows bypassing of diseased segment
🔹 Last resort in elderly or debilitated patients
🔧 6. Suprapubic Cystostomy (Temporary Diversion):
🔹 Used in acute urinary retention
🔹 Provides temporary bladder drainage
🔹 Allows stabilization before definitive repair
🧑⚕️📋 NURSING MANAGEMENT OF PROSTATIC STRICTURE
🩺 1. Comprehensive Assessment:
🔍 Take a detailed history:
- Duration and severity of urinary symptoms
- History of prostatitis, catheterization, or surgery
- Frequency of urinary tract infections
- Any history of urinary retention or hematuria
🔍 Physical assessment:
- Observe for bladder distension
- Assist physician with Digital Rectal Examination (DRE)
- Assess for pain, fever, or signs of infection
💧 2. Monitor Urinary Function:
📊 Maintain Intake-Output Chart (I/O):
- Monitor urine flow, color, and frequency
- Record post-void residual volume (PVR) if using bladder scan
💦 Encourage hydration (unless contraindicated)
- Promotes smooth urine flow
- Reduces risk of infection
🧻 Promote timed voiding or double voiding to prevent retention
💊 3. Medication Administration & Monitoring:
💊 Administer:
- Alpha-blockers (e.g., tamsulosin) for urinary relaxation
- Antibiotics if infection is present
- Analgesics/NSAIDs for pain or inflammation
- Stool softeners to avoid straining
👀 Monitor:
- Side effects of medications
- Effectiveness in relieving symptoms
- Signs of worsening obstruction or retention
🛏️ 4. Pre- and Post-operative Care:
🔹 Pre-operative Nursing Responsibilities:
- Prepare patient physically and emotionally for urethrotomy, TURP, or urethroplasty
- Ensure NPO status, consent, and pre-op labs
- Explain procedure and post-op expectations (e.g., catheter use)
🔹 Post-operative Care:
- Monitor for bleeding, infection, catheter patency
- Provide catheter care (especially after TURP or urethrotomy)
- Irrigate catheter gently if ordered (e.g., in CBI – continuous bladder irrigation)
- Encourage early ambulation and deep breathing exercises
📚 5. Patient Education and Counseling:
🧠 Educate patient on:
- Disease process and treatment plan
- Importance of medication compliance
- Signs of complications (e.g., retention, fever, hematuria)
- Catheter care and hygiene (if discharged with catheter)
💬 Provide emotional support:
- Address anxiety related to voiding difficulty or surgery
- Reassure regarding recovery and long-term outcomes
- Discuss sexual concerns if needed (e.g., ejaculation issues after TURP)
🧼 6. Infection Prevention & Hygiene:
✅ Encourage:
- Hand hygiene
- Proper perineal care
- Catheter hygiene (indwelling or suprapubic)
✅ Monitor:
- Fever, chills, cloudy/foul-smelling urine
- Local redness or swelling at catheter insertion site
🥗🍽️ NUTRITIONAL CONSIDERATION IN PROSTATIC STRICTURE
✅ Recommended:
💧 Increased fluid intake:
▪ 2–3 liters/day unless contraindicated
▪ Helps flush bacteria and reduce risk of infection and urinary stasis
🥣 High-fiber diet:
▪ Whole grains, fruits, vegetables
▪ Prevents constipation, which can increase abdominal pressure and worsen symptoms
🍅 Anti-inflammatory foods:
▪ Tomatoes (lycopene), berries, green leafy vegetables
▪ Support prostate health and reduce inflammation
🐟 Omega-3 rich foods:
▪ Salmon, walnuts, flaxseeds
▪ Beneficial in reducing prostatic inflammation
❌ To Avoid:
⚠️ Caffeine and alcohol:
▪ Act as bladder irritants
▪ May worsen urgency, frequency, or retention
⚠️ Spicy and acidic foods:
▪ Can irritate the urinary tract lining
⚠️ Low fluid intake or dehydration:
▪ Increases risk of urinary tract infections and stone formation
⚠️🧨 COMPLICATIONS OF PROSTATIC STRICTURE
🔸 Urinary Complications:
❗ Chronic urinary retention
❗ Recurrent urinary tract infections (UTIs)
❗ Bladder stones
❗ Overflow incontinence (due to distended bladder)
❗ Hematuria (blood in urine)
🔸 Kidney-Related Complications:
❗ Hydronephrosis – backflow of urine into kidneys
❗ Renal damage or failure – if obstruction is prolonged
🔸 Post-treatment/Surgical Complications:
❗ Stricture recurrence – common after dilation or internal urethrotomy
❗ Infection at catheter or surgical site
❗ Bleeding post-procedure
❗ Urethral fistula or diverticulum (in rare or complex cases)
✅📌 KEY POINTS ON PROSTATIC STRICTURE
🔹 Prostatic stricture is a narrowing of the prostatic urethra, usually due to surgical trauma, infection, or inflammation
🔹 Common in men after TURP, catheterization, or recurrent prostatitis
🔹 Leads to lower urinary tract symptoms (LUTS) like weak stream, retention, and frequency
🔹 Diagnosis includes uroflowmetry, RUG, cystoscopy, and post-void residual measurement
🔹 Medical management helps control symptoms, but surgery is the definitive treatment
🔹 Common procedures: Urethrotomy, TURP, urethroplasty, and suprapubic cystostomy
🔹 Nurses play a crucial role in monitoring, catheter care, infection prevention, and patient education
🔹 Proper nutrition, hydration, and lifestyle modification support recovery and prevent complications
🔹 Long-term follow-up is essential to detect recurrence or renal involvement early.
🔴🚫 PROSTATIC OBSTRUCTION
📘 Definition:
Prostatic obstruction refers to a blockage of urinary flow through the prostatic urethra due to enlargement or pathological changes in the prostate gland.
🧠 It is a form of bladder outlet obstruction (BOO) and is most commonly seen in elderly males due to Benign Prostatic Hyperplasia (BPH) or prostate cancer.
⚠️ Causes:
🔹 Benign Prostatic Causes:
▪ Benign Prostatic Hyperplasia (BPH) – most common
▪ Prostatic strictures – from post-TURP scarring or infection
▪ Prostatic calculi (stones in prostatic ducts)
▪ Prostatitis – inflammation/swelling narrows the urethral lumen
🔸 Malignant Causes:
▪ Prostate cancer – mass compresses urethra from within or outside
🔹 Other/Secondary Causes:
▪ Bladder neck obstruction due to prostatic hyperplasia
▪ Neurogenic bladder dysfunction coexisting with prostatic enlargement
▪ Trauma or post-radiation fibrosis causing prostatic urethral narrowing
🧬 Types of Prostatic Obstruction:
🟢 1. Partial Obstruction:
▪ Some urine flow is maintained
▪ Often seen in early or moderate BPH
🔴 2. Complete Obstruction:
▪ No urine can pass
▪ May cause acute urinary retention — a urological emergency
🔵 3. Chronic Obstruction:
▪ Develops slowly
▪ May cause bladder decompensation and renal effects over time
🟡 4. Acute Obstruction:
▪ Sudden onset, often with severe pain and inability to void
▪ Usually triggered by infection, cold exposure, medications, or alcohol intake
🔄🧠 PATHOPHYSIOLOGY OF PROSTATIC OBSTRUCTION
- Prostatic enlargement or fibrosis compresses the prostatic urethra
- Causes resistance to urine flow from bladder → urethra
- Increased detrusor pressure needed to overcome resistance
- Leads to bladder muscle hypertrophy initially
- Over time, bladder compliance decreases → residual urine, retention, UTIs
- Chronic back pressure → ureteral dilation → hydronephrosis → renal impairment
🚨🧍♂️ SIGNS AND SYMPTOMS OF PROSTATIC OBSTRUCTION
🔸 Voiding (Obstructive) Symptoms:
▪ Weak or interrupted urinary stream
▪ Hesitancy in starting urination
▪ Straining during urination
▪ Dribbling after urination
▪ Feeling of incomplete bladder emptying
▪ Prolonged urination time
🔹 Storage (Irritative) Symptoms:
▪ Increased urinary frequency
▪ Nocturia
▪ Urgency
▪ Urge incontinence (in severe cases)
🔺 Advanced Symptoms:
▪ Acute urinary retention (painful, complete inability to void)
▪ Recurrent UTIs
▪ Hematuria (due to vessel congestion)
▪ Suprapubic pain or bladder distension
▪ Signs of renal dysfunction (elevated urea/creatinine, fatigue)
🔍🧪 DIAGNOSIS OF PROSTATIC OBSTRUCTION
🧫 Lab Investigations:
▪ Urinalysis – detect infection, hematuria
▪ Urine culture – if UTI suspected
▪ Serum PSA – to assess for prostate cancer or inflammation
▪ Renal function tests (BUN, Creatinine) – to detect kidney involvement
📈 Functional & Imaging Studies:
✅ Post-void residual volume (PVR) using bladder scan:
▪ Increased residual urine suggests incomplete emptying
✅ Uroflowmetry:
▪ Reduced flow rate is a key diagnostic sign
✅ Ultrasound KUB (Kidney, Ureter, Bladder):
▪ Evaluates bladder wall thickness, prostate size, and hydronephrosis
✅ Transrectal Ultrasound (TRUS):
▪ Visualizes prostate and assesses for nodules or cancer
✅ Cystoscopy:
▪ Direct visualization of urethra and prostate
▪ Helpful in diagnosing strictures or bladder neck obstruction
✅ MRI Pelvis (if needed):
▪ For prostate cancer staging or complex anatomy
💊🩺 MEDICAL MANAGEMENT OF PROSTATIC OBSTRUCTION
Medical management is primarily useful in Benign Prostatic Hyperplasia (BPH)-induced obstruction or early/mild cases. It aims to relieve obstruction, improve urine flow, and reduce prostate size or inflammation.
✅ 1. Alpha-1 Adrenergic Blockers:
▪ Tamsulosin, Alfuzosin, Doxazosin, Terazosin
🧠 Mechanism: Relax smooth muscle in prostate and bladder neck
🕒 Rapid symptom relief (within days to weeks)
📝 Side Effects: Dizziness, orthostatic hypotension, retrograde ejaculation
✅ 2. 5-Alpha-Reductase Inhibitors:
▪ Finasteride, Dutasteride
🧠 Mechanism: Inhibit conversion of testosterone to dihydrotestosterone (DHT)
🔻 Gradually shrink prostate size (esp. in large prostates)
🕒 Takes 3–6 months for clinical effect
📝 Side Effects: Decreased libido, erectile dysfunction, gynecomastia
✅ 3. Combination Therapy:
▪ Alpha-blocker + 5-alpha-reductase inhibitor
▪ Superior to monotherapy in patients with moderate-to-severe symptoms
✅ 4. Anticholinergics / Beta-3 Agonists:
▪ Used for storage symptoms (urgency/frequency)
▪ Prescribed with caution to avoid urinary retention
✅ 5. Antibiotics (if associated UTI or prostatitis):
▪ Ciprofloxacin, Levofloxacin, Doxycycline (culture-sensitive)
✅ 6. Catheterization (for Acute Retention):
▪ Urethral catheterization (immediate relief)
▪ Suprapubic catheterization if urethral route fails
🏥🔧 SURGICAL MANAGEMENT OF PROSTATIC OBSTRUCTION
Surgery is indicated when: ▪ Symptoms are severe or progressive
▪ Urinary retention, recurrent UTIs, hematuria, or renal impairment occurs
▪ Failure of medical therapy
🛠️ 1. Transurethral Resection of the Prostate (TURP):
▪ Gold standard for BPH-related obstruction
▪ Removes obstructing prostate tissue via endoscope
▪ Rapid symptom relief and urine flow improvement
📝 Complications: Bleeding, retrograde ejaculation, TURP syndrome
🛠️ 2. Transurethral Incision of the Prostate (TUIP):
▪ For smaller prostates (<30g)
▪ Involves making one or two small cuts to relieve pressure
▪ Less invasive than TURP
🛠️ 3. Open Prostatectomy:
▪ For very large prostates (>80–100g) or coexisting bladder stones
▪ Involves removal of inner portion of prostate
▪ Higher risk and longer recovery than TURP
🛠️ 4. Laser Surgery (HoLEP, GreenLight):
▪ Laser vaporization or enucleation of prostate tissue
▪ Less bleeding and quicker recovery
▪ Suitable for patients on anticoagulants
🛠️ 5. Prostatic Urethral Lift (UroLift):
▪ For mild-to-moderate obstruction
▪ Uses implants to lift and hold enlarged prostate tissue away from urethra
▪ Preserves ejaculation function
🛠️ 6. Water Vapor Therapy (Rezūm):
▪ Injects steam to ablate prostatic tissue
▪ Minimally invasive with fewer side effects
▪ Suitable for early BPH with LUTS
🛠️ 7. Suprapubic Cystostomy:
▪ Temporary diversion in complete retention
▪ Often used preoperatively or when catheterization fails.
🧑⚕️📋 NURSING MANAGEMENT OF PROSTATIC OBSTRUCTION
🩺 1. Assessment and Monitoring:
🔍 Collect comprehensive history:
- Onset and progression of urinary symptoms
- Frequency, urgency, nocturia, weak stream, straining
- History of UTIs, prostate problems, or surgery
🔍 Physical Examination Support:
- Assist physician with Digital Rectal Examination (DRE)
- Monitor for bladder distension (palpation or percussion)
- Assess for pain, fever, hematuria, or retention
📊 Vital Signs Monitoring:
- Especially if infection, retention, or TURP syndrome is suspected
💧 2. Promote Effective Urination:
✅ Encourage:
- Timed voiding every 2–3 hours
- Double voiding technique (urinate → pause → try again)
- Adequate fluid intake (unless restricted) to prevent urinary stasis
⚠️ Avoid:
- Delaying urination
- Dehydration or excess fluid intake at bedtime (reduces nocturia)
💉 3. Medication Administration and Monitoring:
💊 Administer prescribed:
- Alpha-blockers, 5-alpha-reductase inhibitors
- Antibiotics for UTI or prostatitis
- NSAIDs for pain or inflammation
👀 Monitor for:
- Side effects: hypotension, dizziness, retrograde ejaculation
- Effectiveness of therapy (improved stream, decreased retention)
🛏️ 4. Pre-operative and Post-operative Care (e.g., TURP):
📌 Pre-operative Care:
- Explain procedure (TURP, TUIP, etc.) and obtain informed consent
- Ensure NPO status as ordered
- Prepare for possible bladder irrigation post-op
📌 Post-operative Care:
- Maintain Continuous Bladder Irrigation (CBI)
🔹 Monitor flow rate, color of urine (should be pink-clear)
🔹 Report bright red bleeding or large clots
🔹 Monitor input vs output to detect fluid absorption/TURP syndrome - Secure catheter to prevent urethral trauma
- Observe for bladder spasms, treat as per protocol
- Promote early ambulation to prevent complications
🧼 5. Infection Prevention:
✅ Perform and teach:
- Catheter care and hygiene
- Perineal care post-op
- Hand hygiene before/after catheter management
🧪 Monitor for:
- Signs of UTI: fever, cloudy urine, foul odor, dysuria
📚 6. Patient and Family Education:
🧠 Teach patient to:
- Recognize symptoms of obstruction, retention, or infection
- Take medications as prescribed
- Avoid caffeine, alcohol, and spicy foods
- Maintain a high-fiber diet to avoid straining during bowel movements
- Return for follow-up visits, PSA testing, or catheter removal
💬 Provide emotional support for:
- Anxiety, concerns about urination or sexual function
- Reassurance about recovery and long-term management
🥗🍽️ NUTRITIONAL CONSIDERATION IN PROSTATIC OBSTRUCTION
✅ Recommended Diet:
💧 Adequate hydration (2–3 liters/day, unless restricted):
▪ Helps flush the urinary system
▪ Prevents urinary stasis and infection
▪ Reduces risk of bladder stone formation
🥗 High-fiber diet:
▪ Whole grains, green leafy vegetables, fruits
▪ Prevents constipation, which increases intra-abdominal pressure and worsens obstruction
🍅 Lycopene-rich foods:
▪ Tomatoes, pink grapefruit, watermelon
▪ May support prostate health and reduce inflammation
🥒 Anti-inflammatory foods:
▪ Berries, turmeric, omega-3s (from flaxseed, fish)
❌ Foods to Avoid:
⚠️ Caffeine (tea, coffee, cola)
▪ Irritates the bladder and increases frequency/urgency
⚠️ Alcohol
▪ Acts as a diuretic and irritant
▪ May worsen symptoms or cause acute retention in some
⚠️ Spicy or acidic foods
▪ Can irritate the bladder lining and worsen LUTS
⚠️ Highly processed and fatty meats
▪ Associated with increased inflammation and prostate enlargement
⚠️🧨 COMPLICATIONS OF PROSTATIC OBSTRUCTION
🔸 Urinary System Complications:
❗ Acute Urinary Retention (AUR) – painful inability to urinate
❗ Chronic Retention – progressive bladder distension
❗ Recurrent Urinary Tract Infections (UTIs)
❗ Bladder stones – due to stagnant urine
❗ Hematuria – blood in urine due to vessel congestion
❗ Overflow incontinence – due to bladder overdistension
🔹 Renal Complications:
❗ Hydroureter and Hydronephrosis
▪ Backpressure on ureters and kidneys
❗ Renal insufficiency or failure
▪ If untreated, long-standing obstruction can impair kidney function
🔺 Post-surgical Complications:
❗ Bleeding (esp. post-TURP)
❗ TURP syndrome – hyponatremia due to irrigation fluid absorption
❗ Retrograde ejaculation
❗ Urinary incontinence
❗ Urethral stricture or bladder neck contracture
✅📌 KEY POINTS ON PROSTATIC OBSTRUCTION
🔹 Prostatic obstruction occurs due to BPH, strictures, cancer, or prostatitis, leading to bladder outlet blockage
🔹 Common in older men, and a major cause of lower urinary tract symptoms (LUTS)
🔹 Symptoms include weak stream, hesitancy, frequency, urgency, and retention
🔹 Diagnosis: Urinalysis, PSA, PVR, uroflowmetry, TRUS, and cystoscopy
🔹 Medical management includes alpha-blockers, 5-alpha-reductase inhibitors, and antibiotics
🔹 Surgical options include TURP, TUIP, laser surgery, or prostatectomy depending on severity
🔹 Nursing care focuses on monitoring, catheter care, infection prevention, and patient education
🔹 Nutrition and hydration play a supportive role in managing symptoms and preventing complications
🔹 Long-standing untreated obstruction may lead to renal damage, UTIs, incontinence, or stone formation.
🧠🔬 UPPER URINARY TRACT TUMORS
📘 Definition:
Upper urinary tract tumors are abnormal growths or cancers that originate in the renal pelvis or ureters, which are lined with urothelial (transitional) epithelium.
🔺 These tumors are relatively rare, accounting for about 5–10% of all urothelial cancers.
⚠️ Causes / Risk Factors:
🔹 Smoking – major risk factor
🔹 Occupational exposure to chemicals (aromatic amines, dyes, solvents)
🔹 Chronic inflammation or infection (e.g., recurrent UTIs)
🔹 Analgesic abuse (e.g., phenacetin-containing drugs)
🔹 Long-term use of aristolochic acid (herbal medicines)
🔹 History of bladder cancer (field cancerization of urothelium)
🔹 Genetic predisposition – Lynch syndrome (HNPCC)
🔹 Radiation therapy to pelvic area
🧬 Types of Upper Urinary Tract Tumors:
- 🟠 Urothelial (Transitional Cell) Carcinoma (TCC) – Most common
- 🔴 Squamous Cell Carcinoma – Rare, associated with chronic irritation
- 🟣 Adenocarcinoma – Extremely rare
- 🟡 Benign tumors (e.g., fibroepithelial polyps, papillomas) – uncommon
🔄🧠 PATHOPHYSIOLOGY:
- Carcinogens (e.g., tobacco, chemicals) irritate and mutate the urothelial lining
- Leads to cellular dysplasia, followed by carcinoma in situ or papillary growth
- Tumor may grow in an exophytic (into lumen) or infiltrative pattern
- Tumor can obstruct urine flow, cause hydronephrosis, and invade renal parenchyma or surrounding structures
- Metastasis may occur via lymphatics, blood vessels, or direct invasion
🚨🧍♂️ SIGNS AND SYMPTOMS:
🔸 Painless gross hematuria (most common presenting symptom)
🔸 Flank pain or dull ache (if obstruction present)
🔸 Recurrent urinary tract infections
🔸 Palpable abdominal/flank mass (rare)
🔸 Fatigue and weight loss (in advanced cases)
🔸 Obstructive uropathy symptoms (hydronephrosis, decreased urine output)
🔸 Fever (if associated infection)
🔍🧪 DIAGNOSIS:
🧫 Laboratory Investigations:
▪ Urinalysis – shows hematuria
▪ Urine cytology – detects malignant cells
▪ Blood tests – CBC, renal function (urea, creatinine), electrolytes
🖥️ Imaging Studies:
✅ Ultrasound KUB – first-line for hydronephrosis or mass detection
✅ CT Urography – gold standard for visualizing upper tract tumors
✅ MRI – alternative in contrast-allergic patients
✅ Intravenous Urogram (IVU) – older method, now replaced by CT
✅ Retrograde Pyelography – outlines ureter/pelvis during cystoscopy
✅ PET-CT – for metastatic workup
🔬 Endoscopic Evaluation:
▪ Ureteroscopy – allows direct visualization and biopsy
▪ Cystoscopy – to assess for concurrent bladder tumors
💊🩺 MEDICAL MANAGEMENT:
🔹 Chemotherapy:
▪ Systemic: Cisplatin-based regimens (e.g., Gemcitabine + Cisplatin)
▪ Neoadjuvant (before surgery) or adjuvant (after surgery)
🔸 Immunotherapy:
▪ For advanced or metastatic urothelial carcinoma
▪ Agents: Atezolizumab, Nivolumab, Pembrolizumab
🔹 Intracavitary Therapy:
▪ In selected patients via ureteric catheter or percutaneous approach (BCG or mitomycin)
🔸 Targeted Therapy (in advanced cases):
▪ FGFR inhibitors (if FGFR mutation present)
🏥🔧 SURGICAL MANAGEMENT:
✅ Nephroureterectomy:
▪ Gold standard for high-grade or invasive tumors
▪ Complete removal of kidney, ureter, and bladder cuff
✅ Segmental Ureterectomy:
▪ For low-grade, localized ureteric tumors
✅ Endoscopic Tumor Ablation:
▪ Laser or electrocautery via ureteroscopy
▪ For small, low-grade, superficial tumors
✅ Partial Nephrectomy:
▪ In patients with solitary kidney or poor renal function
🧑⚕️📋 NURSING MANAGEMENT:
🩺 Pre-operative:
▪ Assess urinary symptoms, hematuria, and pain
▪ Monitor labs: renal function, clotting profile
▪ Educate patient on surgical procedures and potential outcomes
▪ Prepare patient for nephroureterectomy or endoscopic surgery
💉 Post-operative Care:
▪ Monitor vital signs, urine output, surgical site
▪ Care for catheters, stents, or drains
▪ Watch for signs of bleeding, infection, urinary leak
▪ Administer medications (antibiotics, analgesics, chemotherapy)
▪ Encourage early ambulation and pulmonary exercises
📚 Patient Education:
▪ Instructions on catheter care
▪ Warning signs of recurrence or infection
▪ Importance of follow-up cystoscopy (due to recurrence risk)
▪ Support for psychological effects and body image (esp. post-nephrectomy)
🥗🍎 NUTRITIONAL CONSIDERATION:
✅ Encourage:
💧 Hydration – maintain urinary flow and flush residual carcinogens
🥦 Antioxidant-rich foods – fruits, vegetables, berries
🥣 High-fiber diet – prevent constipation post-surgery
🧂 Low-sodium if renal function is compromised
🐟 Adequate protein for healing (in moderation in renal dysfunction)
❌ Avoid:
⚠️ High-oxalate foods (if stones are coexisting)
⚠️ Processed meats, smoking, and alcohol
⚠️ Over-the-counter herbal remedies (nephrotoxic risk)
⚠️🧨 COMPLICATIONS:
❗ Hematuria and clot retention
❗ Hydronephrosis → renal failure
❗ Local or distant metastasis (lungs, bones, liver)
❗ Postoperative infection or bleeding
❗ Urinary fistula or ureteral stricture
❗ Psychosocial issues — body image, anxiety, depression
❗ Reduced renal function (especially after nephrectomy)
✅📌 KEY POINTS:
🔹 Upper urinary tract tumors are rare and most commonly urothelial carcinomas
🔹 Smoking and chemical exposure are key risk factors
🔹 Hematuria is the hallmark symptom
🔹 Diagnosis requires CT urography, urine cytology, and ureteroscopy
🔹 Nephroureterectomy is the gold-standard treatment for high-grade disease
🔹 Minimally invasive options available for low-grade tumors
🔹 Nurses play a critical role in pre/post-op care, education, and follow-up
🔹 Long-term monitoring is essential due to risk of recurrence or bladder tumors
🔹 Nutritional support and hydration improve outcomes and protect kidney function
🟡🔬 LOWER URINARY TRACT TUMORS
📘 Definition:
Lower urinary tract tumors are abnormal growths or malignancies that arise in the urinary bladder, urethra, and sometimes the bladder neck and trigone. The bladder is the most common site.
🔺 The majority are urothelial (transitional cell) carcinomas.
⚠️ Causes / Risk Factors:
🔹 Smoking – most significant risk factor
🔹 Occupational exposure – rubber, leather, paint, dye industries (aromatic amines)
🔹 Chronic cystitis or bladder irritation
🔹 Radiation therapy
🔹 Bladder schistosomiasis infection (linked to squamous cell carcinoma)
🔹 Indwelling catheters (long-term use)
🔹 Cyclophosphamide chemotherapy
🔹 Genetic predisposition – Lynch syndrome
🧬 Types of Lower Urinary Tract Tumors:
- 🔴 Urothelial (Transitional Cell) Carcinoma – ~90%
- 🟣 Squamous Cell Carcinoma – linked to schistosomiasis or chronic inflammation
- 🟡 Adenocarcinoma – rare, aggressive
- 🟢 Benign tumors – papilloma, inverted papilloma, leiomyoma (rare)
🔄🧠 Pathophysiology:
- Chronic exposure to carcinogens (e.g., tobacco, toxins)
- → Mutation in urothelial cells lining the bladder or urethra
- → Cellular dysplasia → carcinoma in situ → invasive tumor
- Tumors may be papillary (superficial) or flat and invasive
- Invasion into bladder wall or spread via lymphatics or blood
🚨🧍♂️ SIGNS AND SYMPTOMS:
🔸 Painless gross hematuria (most common presenting sign)
🔸 Frequency and urgency
🔸 Dysuria (burning or painful urination)
🔸 Urinary retention (if obstruction occurs)
🔸 Pelvic pain or suprapubic discomfort (advanced cases)
🔸 Weight loss, fatigue (late-stage disease)
🔸 Incontinence (in urethral tumors)
🔍🧪 DIAGNOSIS:
🧫 Lab Investigations:
▪ Urinalysis – detect hematuria, pyuria
▪ Urine cytology – detect cancerous cells
▪ Renal function tests – BUN, creatinine
▪ Tumor markers (e.g., NMP22, BTA, UroVysion FISH – optional)
🖥️ Imaging & Endoscopy:
✅ Ultrasound (KUB) – detect mass, wall thickening
✅ CT Urography / IVP – visualize tumor and upper tract
✅ MRI – staging and local invasion
✅ Cystoscopy with biopsy – gold standard for diagnosis
✅ Urethroscopy – for urethral tumor localization
💊🩺 MEDICAL MANAGEMENT:
✅ Intravesical Therapy:
- BCG (Bacillus Calmette-Guérin) – for superficial bladder cancer
- Mitomycin C / Doxorubicin – chemotherapy agents delivered directly into the bladder
✅ Systemic Chemotherapy:
- For muscle-invasive or metastatic disease
- Cisplatin + Gemcitabine regimen is commonly used
✅ Immunotherapy:
- Checkpoint inhibitors: Atezolizumab, Nivolumab, Pembrolizumab (advanced or resistant cases)
🏥🔧 SURGICAL MANAGEMENT:
🔧 Transurethral Resection of Bladder Tumor (TURBT):
▪ First-line for diagnosis and treatment of non-muscle invasive bladder cancer
🔧 Partial Cystectomy:
▪ For isolated tumor in bladder dome
🔧 Radical Cystectomy:
▪ For muscle-invasive bladder cancer
▪ Removal of bladder, nearby lymph nodes, and surrounding organs (e.g., prostate, uterus)
🔧 Urinary Diversion Procedures:
▪ Ileal conduit
▪ Neobladder
▪ Continent cutaneous reservoir
🔧 Urethrectomy:
▪ For urethral tumors, often along with cystectomy
🧑⚕️📋 NURSING MANAGEMENT:
🩺 Pre-operative:
▪ Monitor for hematuria, anemia, and urinary symptoms
▪ Prepare patient emotionally and physically for cystectomy
▪ Explain potential need for urostomy or neobladder
💉 Post-operative:
▪ Monitor urine output, stoma site, signs of infection
▪ Provide stoma care and education
▪ Manage pain and prevent DVT/pulmonary complications
▪ Administer intravesical medications if ordered
▪ Encourage ambulation and breathing exercises
📚 Patient Education:
▪ Stoma or neobladder management
▪ Infection prevention
▪ Signs of recurrence or metastasis
▪ Psychosocial support and counseling
🥗🍎 NUTRITIONAL CONSIDERATION:
✅ Encourage:
▪ High-protein diet (for healing)
▪ High-fiber diet (prevent straining post-surgery)
▪ Hydration (unless contraindicated)
▪ Vitamin-rich foods for immune support
❌ Avoid:
▪ Caffeine, alcohol, acidic foods
▪ Processed meats (carcinogenic potential)
⚠️🧨 COMPLICATIONS:
❗ Hematuria and anemia
❗ Urethral or bladder obstruction
❗ Tumor recurrence or metastasis
❗ Urinary incontinence
❗ Electrolyte imbalance (post-diversion)
❗ Infection (UTI, surgical site, peritonitis)
❗ Body image issues and depression
✅📌 KEY POINTS:
🔹 Bladder tumors are the most common lower urinary tract tumors
🔹 Hematuria is the primary symptom
🔹 Cystoscopy with biopsy confirms diagnosis
🔹 TURBT and intravesical therapy for superficial tumors
🔹 Cystectomy + chemo for invasive tumors
🔹 Nursing care involves stoma management, hydration, and emotional support
🔹 Long-term surveillance is essential due to high recurrence rate