🧬 Common Terms Used in Pathology – Understanding the Language of Disease
Pathology is the branch of medical science that deals with the study of disease, including its causes, development, effects on the body, and outcomes. To navigate this complex field, one must first be fluent in its specialized vocabulary. The terms used in pathology help health professionals describe disease processes accurately, communicate findings, and understand the underlying mechanisms of illness.
Whether you’re examining a biopsy slide, reviewing lab results, or explaining a diagnosis, these terms are the foundation of understanding disease.
🧠 1. Pathology
Definition: The scientific study of the nature, causes, development, and consequences of diseases.
Definition: A regulated form of necrosis, combining aspects of both apoptosis and necrosis — often occurs during viral infections or immune responses.
🧠 Emerging interest in targeted therapies that influence necroptotic pathways.
🧬 44. Paraneoplastic Syndrome
Definition: A group of symptoms that occur in cancer patients due to substances secreted by tumors, not by local tumor presence.
🧠 Examples: Hypercalcemia, Cushing’s syndrome, SIADH in lung cancer.
Nurses should monitor for unusual systemic effects in cancer patients.
🧬 45. Cachexia
Definition: A syndrome of weight loss, muscle wasting, and fatigue seen in advanced chronic diseases (e.g., cancer, AIDS).
🧠 Nutritional support, psychosocial care, and palliative measures are crucial.
🧪 46. Pyemia
Definition: A type of septicemia characterized by widespread pus-forming (pyogenic) bacteria in the bloodstream, leading to multiple abscesses in various organs.
🧠 Example: Untreated boils or infected wounds can lead to pyemia with lung and brain abscesses.
Nursing Implication: Monitor for high-grade fever, chills, and organ dysfunction in septic patients.
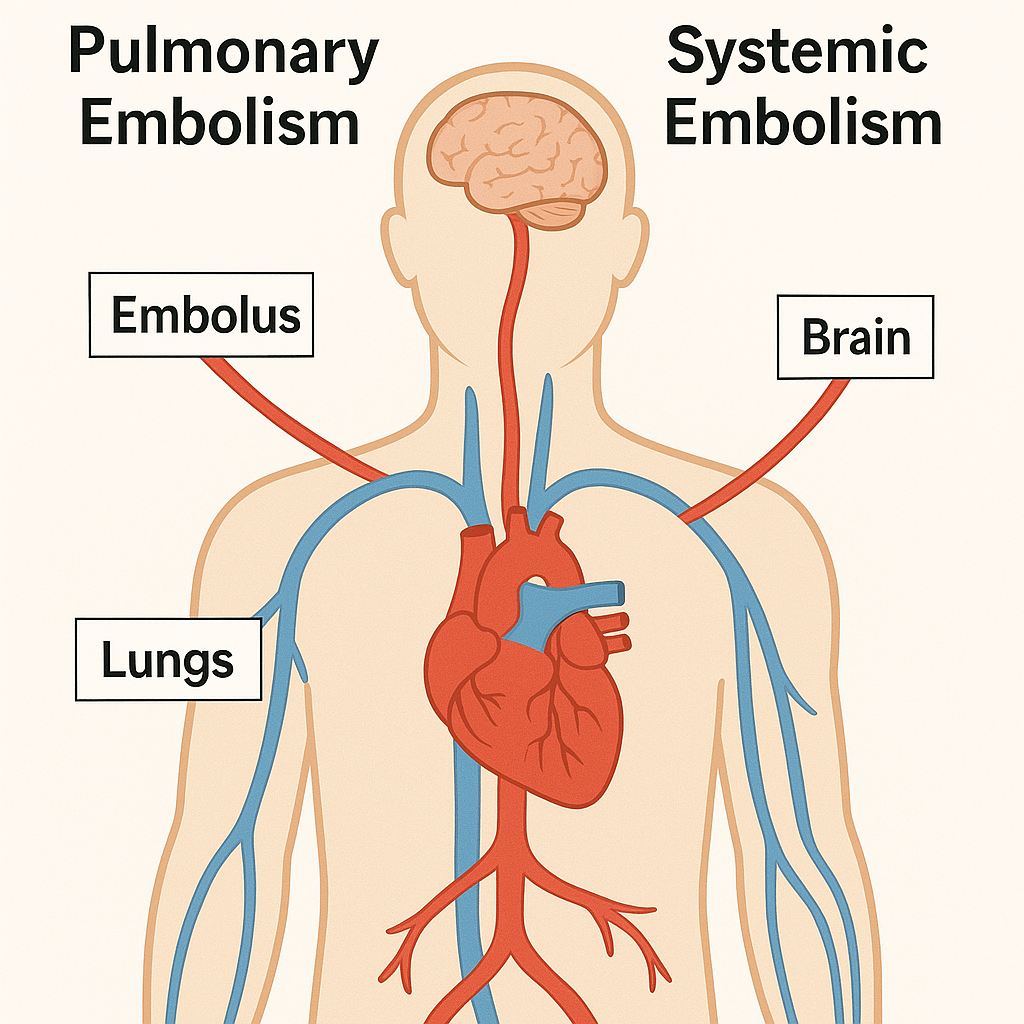
💥 47. Shock Organ
Definition: The organ most commonly or severely affected during anaphylaxis or systemic shock.
🧠 In humans:
Lungs are the shock organ in anaphylactic shock
Kidneys in hypovolemic shock
Heart in cardiogenic shock
Nursing Role: Early recognition of organ-specific signs helps in timely resuscitation.
🧫 48. Serositis
Definition: Inflammation of a serous membrane, such as the pleura, pericardium, or peritoneum.
🧠 Common in autoimmune diseases like lupus (SLE).
Nurses should assess for chest pain, ascites, or pericardial rubs.
⚠️ 49. Amyloidosis
Definition: A condition characterized by abnormal deposition of amyloid proteins in tissues and organs, leading to dysfunction.
🧠 Affects kidneys, liver, heart, and nervous system.
Watch for unexplained weight loss, edema, neuropathy.
🦴 50. Osteomyelitis
Definition: A bone infection, most commonly caused by Staphylococcus aureus.
🧠 Can be acute or chronic, and is painful, with fever, swelling, and warmth.
Early detection prevents permanent deformity.
🧬 51. Oncogene
Definition: A gene that has the potential to cause cancer when mutated or overexpressed.
🧠 Example: HER2 gene in breast cancer.
Knowing oncogene status helps determine targeted therapy.
🩸 52. Hematuria
Definition: Presence of blood in urine, which may appear grossly red or be microscopic.
🧠 Could indicate UTI, trauma, kidney disease, or cancer.
Nurses should report any hematuria promptly and monitor renal function.
💉 53. Hemoptysis
Definition: Coughing up blood from the respiratory tract.
🧠 Seen in conditions like tuberculosis, lung cancer, pulmonary embolism.
Nursing priority: Position patient, assess respiratory status, notify physician.
🔍 54. Morphology
Definition: The form and structure of cells, tissues, or organs — especially how they change in disease.
🧠 Example: Cancer cells show abnormal morphology under the microscope — large nuclei, irregular shape, increased mitosis.
🧠 55. Myelopathy
Definition: A disease or disorder of the spinal cord.
🧠 Causes include trauma, tumors, infection, or degenerative changes.
Symptoms include motor/sensory deficits, spasticity, or bowel/bladder dysfunction.
🔬 56. Gliosis
Definition: A reactive change of glial cells (astrocytes) in response to CNS damage.
🧠 It forms a scar-like barrier in the brain after trauma, stroke, or infection.
Not directly harmful but can affect brain signal transmission.
🧪 57. Paraproteinemia
Definition: Presence of abnormal immunoglobulins in the blood, commonly seen in multiple myeloma.
🧠 May lead to hyperviscosity syndrome, kidney failure, or anemia.
Nurses must monitor for bone pain, fatigue, or renal signs in at-risk patients.
🔥 58. Cytokine Storm
Definition: A severe immune reaction where the body releases too many pro-inflammatory cytokines into the blood too quickly.
🧠 Seen in COVID-19, sepsis, and CAR-T cell therapy.
Requires ICU-level care — monitor oxygen saturation, fever, and organ failure signs.
🔄 59. Recurrence
Definition: The return of a disease after a period of improvement or remission.
🧠 Seen in cancer, autoimmune disorders, infections.
Nurses play a role in patient education, follow-up care, and early detection.
📉 60. Regression
Definition: Shrinkage or reduction of disease severity or tumor size, often after treatment.
🧠 Not a cure — may be temporary. Clinical improvement in patients should be monitored regularly to confirm ongoing response.
💢 61. Flare-up
Definition: A sudden worsening of symptoms in a chronic disease (e.g., asthma, psoriasis, rheumatoid arthritis).
🧠 Nurses help manage trigger avoidance, medication compliance, and supportive therapy.
📘 62. Desquamation
Definition: Peeling or shedding of skin, often following inflammation, burns, or certain infections.
🧠 Seen in scarlet fever, Kawasaki disease, or chemical burns.
Nurses must monitor for secondary infections and provide wound care.
⚠️ 63. Toxidrome
Definition: A set of symptoms associated with a specific class of toxins.
Recognizing toxidromes aids in early poisoning diagnosis.
🧠 Nursing is both an art and a science — and pathology is the science that sharpens clinical judgment.
🧬 Importance of the Study of Pathology – The Science Behind Clinical Excellence
Pathology is the foundation of modern medicine — the study of disease in its most complete sense. It explains the why, how, and what of every abnormal process in the human body. From a swollen lymph node to a failing organ, from a microscopic cell mutation to a full-blown clinical syndrome — pathology provides the framework to understand it all.
For healthcare professionals, especially nurses, doctors, and technicians, pathology is not just theory; it is practical knowledge that guides decision-making, enhances communication, and improves patient outcomes.
🧠 Why is the Study of Pathology Important?
🔍 1. Understanding the Cause and Nature of Diseases (Etiology & Pathogenesis)
Pathology helps identify the root cause (etiology) and the mechanism (pathogenesis) behind every disease.
🧠 Example: Knowing that diabetes mellitus results from insulin dysfunction allows healthcare workers to understand complications like neuropathy, nephropathy, and retinopathy.
👉 Application: Enables nurses and clinicians to not just treat symptoms, but understand what’s happening at the cellular and systemic level.
⚙️ 2. Connecting Clinical Signs and Symptoms with Underlying Pathology
Studying pathology sharpens the ability to correlate clinical presentations (e.g., fever, pain, swelling, fatigue) with tissue-level changes.
🧠 Example: A patient with right lower abdominal pain, fever, and rebound tenderness may be suffering from appendicitis — a diagnosis that is rooted in understanding the inflammatory pathology of the appendix.
👉 Nurses can more confidently monitor, assess, and escalate care when they understand what’s occurring inside the body.
🧬 3. Improving Diagnosis and Treatment Planning
Pathology provides the basis for:
Histopathological examination
Biochemical and hematological lab reports
Radiological findings and tumor grading
🧠 Example: A biopsy report confirming malignant cells helps tailor the stage-specific cancer treatment.
👉 Nursing application: Helps nurses understand lab and diagnostic reports, educate patients, and reinforce the medical plan of care.
⚕️ 4. Enhancing Evidence-Based and Personalized Care
Understanding how diseases progress, what complications arise, and which interventions are proven effective ensures that care is scientifically sound.
🧠 Example: Recognizing early signs of shock in trauma patients leads to faster resuscitation and better survival rates.
👉 Pathology empowers nurses to deliver accurate, timely, and prioritized care.
🧪 5. Mastering Laboratory Interpretation and Communication
Many nursing actions are based on lab values (e.g., CBC, LFTs, urinalysis, cultures). Without pathology, these numbers lack meaning.
🧠 Example: A drop in hemoglobin along with elevated bilirubin may suggest hemolytic anemia.
👉 Nurses can interpret lab results, advocate for patients, and alert the team to dangerous trends.
👨⚕️ 6. Critical for Emergency and ICU Situations
In acute care, understanding disease mechanisms is essential for recognizing life-threatening conditions early.
🧠 Example: In sepsis, knowing the systemic inflammatory response allows early detection through vitals, urine output, and mental status.
👉 In ICU, nurses act as the first responders — and pathology knowledge sharpens their clinical judgment.
🧬 7. Forms the Basis of Public Health and Preventive Medicine
Understanding the causative factors of disease (e.g., infection, lifestyle, environment) guides prevention strategies like:
Vaccination
Screening programs
Health education
🧠 Example: Pathology helped define the link between HPV and cervical cancer, leading to vaccines and Pap smear screening.
👉 Nurses in community and school settings use this knowledge to educate, screen, and refer patients.
🧾 8. Supports Interdisciplinary Collaboration
Pathology bridges knowledge between:
Doctors (diagnosis)
Nurses (patient care)
Pharmacists (medication planning)
Technologists (diagnostic testing)
👉 Shared understanding of pathology enables smooth communication and coordinated care.
📚 In Summary – Why Study Pathology?
✅ It deepens your understanding of what disease is ✅ It strengthens your ability to assess and act quickly ✅ It connects clinical symptoms to root causes ✅ It improves the quality and accuracy of nursing care ✅ It supports critical thinking in complex patient scenarios ✅ It empowers you to educate, explain, and advocate
🔑 Conclusion: To care for a disease, you must first understand it — and that’s exactly what pathology offers.
🧬 Cell Injury – Etiology (Causes)
Cells are the basic units of life, each designed to perform specific functions vital to the survival of tissues and organs. While cells possess remarkable mechanisms for adaptation and repair, they are not indestructible. When the intensity or duration of a stressor exceeds the cell’s adaptive capacity, the result is cell injury — the first step in disease development.
Understanding the etiology (causes) of cell injury is foundational in pathology because nearly every disease begins with some form of cellular disturbance.
🧠 What is Cell Injury?
Cell injury is defined as any change that impairs the normal structure or function of a cell. If the injury is mild or short-lived, it may be reversible. But if severe or persistent, it may lead to irreversible damage and ultimately cell death — either by necrosis or apoptosis.
🧪 Etiology of Cell Injury – What Causes Cells to Become Injured?
The causes of cell injury can be classified into external (exogenous) and internal (endogenous) factors. They include physical, chemical, infectious, genetic, and nutritional insults.
Let’s explore each in detail:
🔥 1. Physical Agents (Mechanical and Environmental Trauma)
These include a wide range of environmental forces that can physically damage cells and tissues.
🧠 Mechanism: Cytokines and immune cells may cause inflammatory cell injury, tissue necrosis, or fibrosis.
🧪 8. Free Radical Injury (Oxidative Stress)
Free radicals are unstable molecules that can damage lipids, proteins, and DNA.
Generated during metabolism, radiation, inflammation, and chemical exposure
Normally neutralized by antioxidants (e.g., vitamins C and E, catalase)
🧠 Excess free radicals = oxidative stress, leading to cell injury.
🧫 9. Aging
With age, cells undergo:
Reduced repair capacity
Decreased mitochondrial function
Telomere shortening
Accumulation of DNA damage
🧠 Result: Increased vulnerability to cell injury and chronic disease.
📚 In Summary
✅ Major Etiological Factors of Cell Injury:
Physical agents
Chemical agents and drugs
Infectious agents
Genetic abnormalities
Nutritional imbalances
Hypoxia and ischemia
Immune reactions
Free radical damage
Aging
🔑 Key Concept: The nature, severity, and duration of the injury — along with the type of cell affected — determine whether the damage is reversible or irreversible.
👩⚕️ Why Is This Important for Nurses and Clinicians?
Understanding the causes of cell injury helps nurses:
Anticipate complications
Identify early warning signs
Prioritize care (e.g., oxygenation in hypoxia)
Educate patients about risk factors
Interpret lab results and imaging
🧠 Knowledge of cellular injury bridges the gap between basic science and clinical care — making it essential for every healthcare provider.
🧬 Cell Injury: Pathogenesis of Reversible and Irreversible Damage
Cells are resilient, dynamic structures designed to adapt to changing environments. But when the stress exceeds a cell’s ability to adapt, it undergoes injury. This injury may be reversible if the stimulus is mild or short-lived — allowing the cell to recover. However, if the stress is severe or prolonged, the injury becomes irreversible, leading to cell death.
Understanding the pathogenesis (sequence of events) of reversible and irreversible cell injury is essential for diagnosing and managing acute and chronic diseases.
🧠 I. Reversible Cell Injury – Early and Potentially Repairable
🔄 Definition:
A mild to moderate injury where the cell’s structural and functional integrity is disturbed but not permanently damaged. If the stress is removed, the cell returns to normal.
⚙️ Pathogenesis of Reversible Injury:
🔹 Trigger (e.g., hypoxia, toxins) ⬇ 🔹 ATP depletion due to impaired mitochondrial function ⬇ 🔹 Failure of Na⁺/K⁺ pumps on cell membrane → Na⁺ accumulates inside the cell ⬇ 🔹 Water influx → cellular swelling (hydropic change) ⬇ 🔹 Detachment of ribosomes from rough ER → ↓ protein synthesis ⬇ 🔹 Mild chromatin clumping in the nucleus ⬇ 🔹 Accumulation of fatty vacuoles in some cells (e.g., liver)
✅ Key Morphological Features:
Cell swelling
Blebbing of plasma membrane
Dilated endoplasmic reticulum
Fatty change in organs like liver, heart
🧠 Outcome: If the injury is corrected (e.g., oxygen restored), cell recovers and resumes normal function.
☠️ II. Irreversible Cell Injury – The Point of No Return
🛑 Definition:
An injury so severe that cell recovery is impossible, even if the stressor is removed. This leads to cell death by necrosis or apoptosis.
⚠️ Pathogenesis of Irreversible Injury:
🔹 Persistent or severe damage (e.g., prolonged ischemia) ⬇ 🔹 Severe ATP depletion → failure of energy-dependent processes ⬇ 🔹 Mitochondrial dysfunction becomes irreversible → no ATP production ⬇ 🔹 Massive calcium influx into the cell ⬇ 🔹 Activation of:
Karyolysis: fading and dissolution ⬇ 🔹 Inflammatory reaction (especially in necrosis)
❌ Key Morphological Features:
Severe mitochondrial damage with dense deposits
Disruption of membranes
Nuclear destruction
Leakage of enzymes (e.g., cardiac troponins in MI)
🧠 Outcome: Irreversible damage → cell death, which may lead to tissue necrosis or apoptosis depending on the mechanism.
🔬 Comparison Table: Reversible vs. Irreversible Cell Injury
Feature
Reversible Injury
Irreversible Injury
ATP depletion
Mild to moderate
Severe and prolonged
Cell swelling
Present
Exaggerated, leads to rupture
Membrane integrity
Maintained
Lost, contents leak out
Nuclear damage
Minimal (chromatin clumping)
Pyknosis, karyorrhexis, karyolysis
Mitochondrial damage
Swelling, but reversible
Membrane rupture and calcium deposits
Outcome
Recovery if cause is removed
Cell death (necrosis or apoptosis)
👩⚕️ Nursing and Clinical Implications
Understanding the pathogenesis of cell injury allows nurses and healthcare professionals to:
✅ Recognize early signs of organ dysfunction ✅ Understand the critical window for intervention ✅ Interpret biochemical markers (e.g., troponins, AST/ALT) ✅ Support recovery strategies (oxygenation, fluid therapy) ✅ Educate patients on prevention of further injury (e.g., diabetes control, toxin avoidance)
🔍 Example: In myocardial infarction, restoring blood flow within minutes may reverse injury. Delay beyond a few hours leads to irreversible cell death and heart muscle necrosis.
📚 In Summary
Reversible injury: Early, mild, recoverable; involves swelling, ATP drop, and biochemical disruption.
The transition point is when mitochondrial and membrane damage becomes irreversible.
🧠 The study of cell injury pathogenesis bridges molecular understanding and bedside decision-making — making it essential for every nurse and clinician.
Certainly! Here is a detailed, academic, and well-structured narrative explanation of Necrosis — a type of cell death — presented in an attractive and engaging format, ideal for nursing, medical, and paramedical education.
☠️ Necrosis – The Pathological Death of Cells
Necrosis is a dramatic and destructive event in the life of a cell — a point where damage becomes irreversible, and the cell dies prematurely in a chaotic and inflammatory fashion. Unlike programmed cell death (apoptosis), necrosis is uncontrolled, accidental, and always pathological, resulting from overwhelming injury that disrupts cellular architecture and triggers surrounding tissue inflammation.
It is a hallmark of many acute diseases, including infarctions, infections, trauma, and toxic exposures — making it essential for clinicians and nurses to recognize its implications in practice.
🧠 What is Necrosis?
Definition: Necrosis is unregulated cell death caused by external injury, characterized by:
Loss of membrane integrity
Enzymatic digestion of cell components
Leakage of cellular contents
Inflammatory response in surrounding tissues
Necrosis affects groups of cells or tissues, unlike apoptosis which is individual and non-inflammatory.
🧪 Pathogenesis of Necrosis – How Does It Occur?
Necrosis begins when a cell suffers irreversible damage, commonly due to:
🔍 The released enzymes and cellular debris trigger an inflammatory response — leading to pain, swelling, and fever.
🔬 Morphological Changes in Necrosis
Under the microscope, necrotic cells show:
Eosinophilia (bright pink cytoplasm due to protein denaturation)
Nuclear changes:
Pyknosis: Nuclear shrinkage
Karyorrhexis: Nuclear fragmentation
Karyolysis: Fading/dissolution of nucleus
Disruption of plasma and organelle membranes
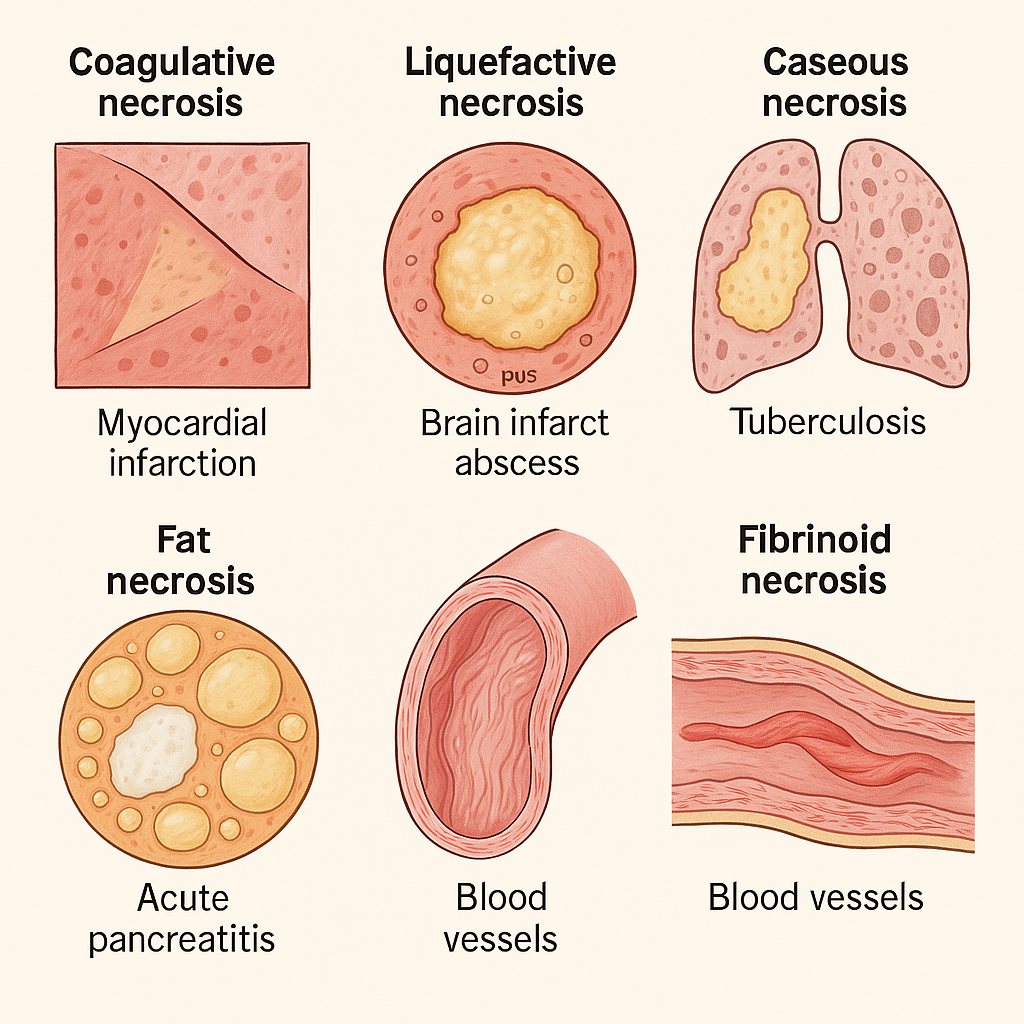
🧩 Types of Necrosis – Based on Tissue and Cause
Different tissues show different patterns of necrosis:
🔹 1. Coagulative Necrosis
Most common type
Seen in: Myocardial infarction, kidney infarction
Tissue appears firm, pale, and preserved for a few days
Architecture is maintained, but cells are dead
🧠 Caused by: Ischemia (except in the brain)
🔹 2. Liquefactive Necrosis
Tissue is completely digested → liquid, pus-like mass
Seen in: Brain infarcts, abscesses
Due to release of lysosomal enzymes from neutrophils
🧠 Common in bacterial infections and CNS tissue
🔹 3. Caseous Necrosis
Combination of coagulative and liquefactive
Appears cheese-like, soft, white, granular
Seen in: Tuberculosis (especially lungs), fungal infections
🧠 Microscopically: Granulomas with central necrosis surrounded by immune cells
🔹 4. Fat Necrosis
Enzymatic destruction of fat cells
Seen in: Acute pancreatitis, breast trauma
Results in chalky white areas (saponification: fat + calcium)
🧠 Calcium deposits may appear on X-ray or during surgery.
🔹 5. Fibrinoid Necrosis
Occurs in blood vessel walls
Seen in: Vasculitis, immune reactions (autoimmune diseases)
🧠 Appears as bright pink amorphous material due to antigen-antibody complex deposition
⚠️ Clinical Consequences of Necrosis
Triggers inflammation and swelling
May lead to tissue destruction or scarring
May cause organ dysfunction or failure
Acts as a marker of disease severity
🧠 Example: Release of cardiac enzymes (like troponin) after myocardial necrosis helps in diagnosing a heart attack.
👩⚕️ Nursing and Clinical Relevance
Understanding necrosis helps nurses to:
✅ Recognize signs of acute injury or infarction ✅ Interpret lab markers of tissue necrosis (e.g., CK-MB, AST, LDH) ✅ Understand wound healing phases and complications ✅ Monitor for secondary infections in necrotic tissue ✅ Educate patients on prevention and early reporting (e.g., diabetic foot ulcers)
📚 In Summary
Necrosis is unregulated cell death resulting from severe injury
It is always pathological, causing inflammation and tissue breakdown
There are different types of necrosis, depending on tissue and cause
Recognizing necrosis is vital in diagnosing, treating, and preventing complications in many diseases
🔑 Necrosis marks the breakdown of cells — and understanding it helps healthcare providers intervene before entire organs fail.
☠️ Gangrene – When Cell Death Takes Over Entire Tissues
Gangrene is a dramatic and often devastating consequence of severe and progressive cell death, where large areas of tissue undergo necrosis, leading to loss of function, infection, and potentially life-threatening complications. It represents massive irreversible tissue damage, commonly seen in limbs, toes, and intestines — particularly in people with vascular disease, diabetes, or infections.
Understanding gangrene is crucial in clinical practice, especially for early detection, nursing care, and prevention of complications.
🧠 What is Gangrene?
Definition: Gangrene is a condition involving massive necrosis of body tissues, typically due to loss of blood supply, bacterial infection, or both. It leads to tissue death, discoloration, foul smell, and, if untreated, sepsis or death.
Gangrene is not a type of necrosis itself, but a gross manifestation of it, especially coagulative or liquefactive necrosis, often combined with infection.
⚠️ Etiology (Causes) of Gangrene
Gangrene usually occurs when blood flow to a tissue is blocked (ischemia), and bacteria invade the necrotic, oxygen-deprived environment. Common causes include:
Arterial occlusion (atherosclerosis, embolism)
Severe trauma or crush injuries
Infections (e.g., Clostridium perfringens)
Burns, frostbite
Diabetes mellitus (especially in the lower limbs)
Surgery or tight bandaging
Intestinal volvulus or strangulation
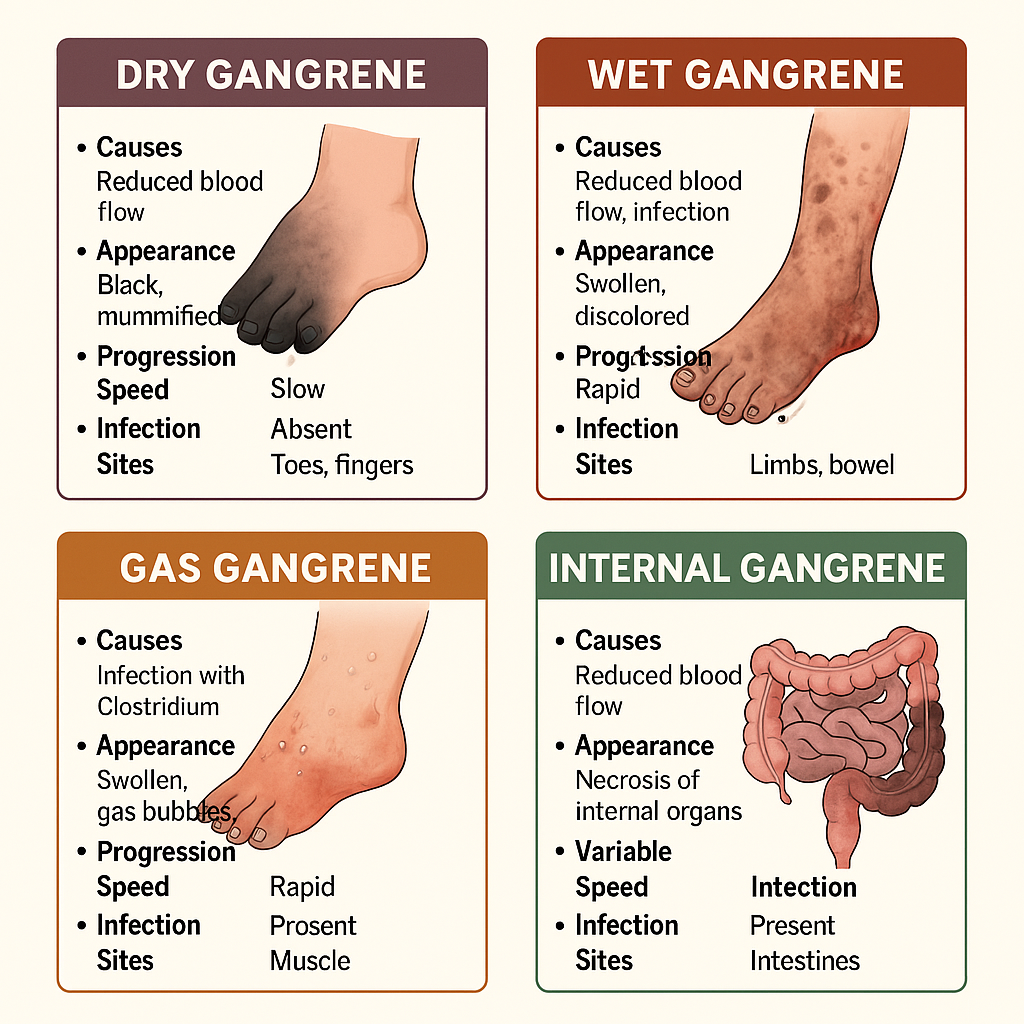
🧩 Types of Gangrene – Based on Clinical and Pathological Features
🔴 1. Dry Gangrene (Ischemic Type)
🧠 Pathophysiology:
Caused by gradual arterial obstruction (e.g., atherosclerosis)
Leads to coagulative necrosis without bacterial infection
🩺 Clinical features:
Dry, shriveled, and black tissue
Clear line of demarcation between dead and living tissue
Monitor color, warmth, and sensation in extremities
Observe for swelling, pain, odor, discharge
Check for fever or signs of sepsis
✅ Prevention:
Educate diabetic patients on foot care
Ensure proper wound hygiene and dressings
Promote early mobilization in immobile patients
Avoid tight bandaging or casts
✅ Interventions:
Assist in wound debridement and dressing changes
Administer prescribed antibiotics and fluids
Prepare for surgical interventions if needed
Provide psychological support for patients facing amputation
📚 In Summary
Gangrene is a severe form of tissue necrosis, often due to ischemia and infection
Types include:
Dry gangrene: non-infective, slow
Wet gangrene: infective, rapid
Gas gangrene: bacterial, emergency
Internal gangrene: affects internal organs
Early diagnosis and intervention can be life-saving
Nursing care focuses on early detection, prevention, infection control, and emotional support
🧠 Gangrene is a visible reminder of invisible dangers — hypoxia, bacteria, and delayed care. Understanding it saves limbs, and sometimes lives.
Certainly! Here’s a detailed, academic, and well-structured narrative explanation of Atrophy, a key concept under cellular adaptations, presented in an engaging and clinical-friendly style — ideal for nursing, medical, and allied health learners.
🔬 Cellular Adaptation: Atrophy – When Cells Choose to Shrink to Survive
In the ever-changing environment of the human body, cells must constantly adapt to stress in order to survive. When faced with a decrease in demand or supply, cells often respond by reducing their size and activity — a process known as atrophy. Think of it as a survival mechanism: rather than die, the cell shrinks its operations, like a business scaling down to avoid shutting down.
Atrophy is one of the major forms of cellular adaptation alongside hypertrophy, hyperplasia, metaplasia, and dysplasia — but uniquely, it represents a regressive, energy-saving change.
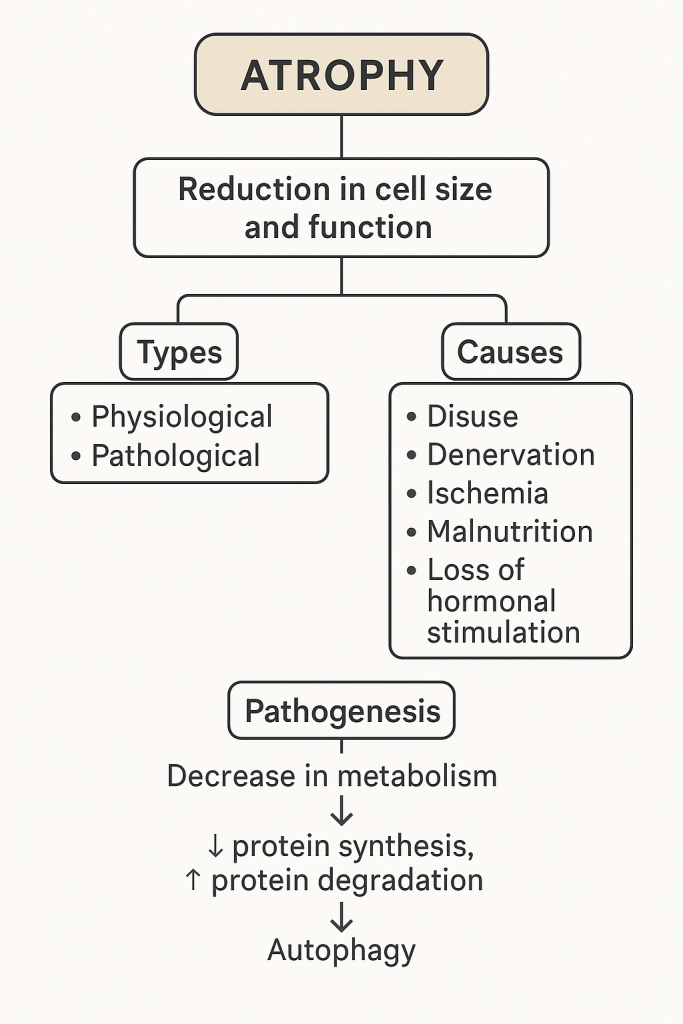
📖 What is Atrophy?
Definition: Atrophy is the reduction in cell size and function — and sometimes in cell number — in response to decreased workload, nutrition, blood flow, or hormonal stimulation. When many cells in a tissue atrophy, the entire organ or tissue shrinks.
🧠 Key Insight: It is often reversible, especially if the underlying cause is corrected early.
🧪 Types of Atrophy
🔹 1. Physiological Atrophy
A normal, programmed process that occurs during development or aging.
🧠 Examples:
Thymic atrophy after puberty
Uterine atrophy post-menopause
Muscle atrophy with aging (sarcopenia)
🔹 2. Pathological Atrophy
Occurs due to disease, injury, or adverse conditions.
🧠 Common examples:
Disuse atrophy: After immobilization (e.g., limb in a cast)
Denervation atrophy: Following nerve injury (e.g., poliomyelitis)
Ischemic atrophy: Due to reduced blood supply (e.g., renal artery stenosis)
Malnutrition or cachexia: Seen in cancer or chronic illness
Endocrine atrophy: Due to decreased hormonal stimulation (e.g., adrenal atrophy after steroid therapy)
🧩 Mechanism/Pathogenesis of Atrophy
The cellular shrinkage seen in atrophy is not random — it involves highly regulated metabolic processes that help cells conserve energy and survive.
🔄 Step-by-step Pathogenesis:
Decrease in functional demand or supply (e.g., less oxygen, nutrients, or nerve signals) ↓
Cellular metabolic activity reduces to match the new environment ↓
Protein synthesis decreases and protein degradation increases ↓
Activation of ubiquitin-proteasome pathway (a system for degrading proteins) ↓
Autophagy may occur — the cell digests its own components using lysosomes ↓
Result: Cell shrinkage, decreased organelle number, and reduction in overall tissue/organ size
🧬 Microscopic and Gross Appearance
Microscopically:
Cells are smaller in size
Decreased cytoplasm and organelles
Nucleus may appear condensed
Macroscopically (gross):
Organ or tissue appears smaller, lighter, and shrunken
In severe cases, may have fibrotic or fatty replacement
🏥 Clinical Examples of Atrophy
Type
Example
Nursing Relevance
Disuse Atrophy
Muscle shrinkage in bedbound patients
Encourage early ambulation & ROM exercises
Denervation Atrophy
Paralysis after spinal cord injury
Monitor for pressure sores, use splints
Vascular Atrophy
Kidney shrinkage in renal artery stenosis
Assess for hypertension & renal function
Hormonal Atrophy
Endometrial thinning post-menopause
Monitor postmenopausal bleeding
Nutritional Atrophy
Wasting in malnourished patients
Nutritional assessment, refer to dietician
👩⚕️ Nursing & Clinical Implications
Understanding atrophy allows nurses to:
Recognize signs of tissue wasting early (muscle weakness, size reduction)
Educate patients on the importance of mobility and activity
Prevent complications such as pressure ulcers, contractures, and malnutrition
Support rehabilitation and nutritional interventions
Collaborate with physiotherapists and dietitians for recovery plans
🧠 Atrophy is often a silent warning — identifying it early can prevent disability and improve quality of life.
📚 In Summary
Atrophy is a reversible reduction in cell size and function
It may be physiological (normal) or pathological (disease-related)
Causes include disuse, denervation, ischemia, malnutrition, and hormonal loss
It involves reduced protein synthesis, increased degradation, and autophagy
Nurses play a key role in preventing and managing the consequences of atrophy
🔑 Cells shrink to survive — and your care can help them thrive again.
Would you like a flowchart or visual diagram summarizing types, causes, and pathogenesis of atrophy for easy revision or presentation use?
💪 Cellular Adaptation: Hypertrophy – Growth Without Multiplication
Cells, like individuals, adapt to survive — and sometimes they do this by growing in size, not number. This cellular adaptation is called hypertrophy. When a tissue or organ is placed under increased demand, it may respond by enlarging its individual cells, leading to an overall increase in organ size and functional capacity. Unlike hyperplasia (increase in cell number), hypertrophy is all about bigger cells, not more cells.
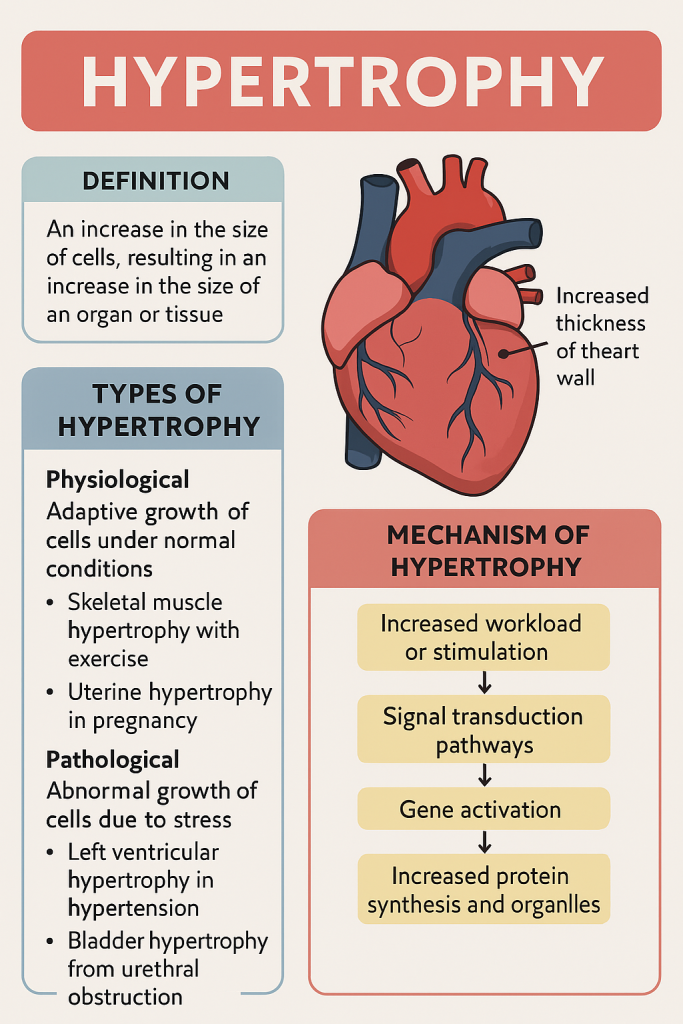
📖 What is Hypertrophy?
Definition: Hypertrophy is the increase in the size of individual cells, leading to enlargement of the affected organ or tissue, without an increase in cell number.
🧠 This occurs in tissues composed of non-dividing cells (e.g., cardiac muscle, skeletal muscle) that cannot replicate but can synthesize more structural components.
🧪 Types of Hypertrophy
🔹 1. Physiological Hypertrophy
A normal adaptation to increased functional demand or hormonal stimulation.
🧠 Examples:
Skeletal muscle hypertrophy in athletes due to resistance training
Uterine hypertrophy during pregnancy under the influence of estrogen
Breast hypertrophy during lactation
🔹 2. Pathological Hypertrophy
Occurs as a compensatory response to chronic stress or disease, often leading to dysfunction if the stress persists.
🧠 Examples:
Left ventricular hypertrophy due to hypertension or aortic valve stenosis
Bladder wall hypertrophy due to urethral obstruction (e.g., prostate enlargement)
🔍 Although initially adaptive, pathological hypertrophy can progress to organ failure.
🧩 Mechanism / Pathogenesis of Hypertrophy
Cells undergo hypertrophy through increased protein synthesis and organelle production — especially in muscle fibers.
⚙️ Step-by-Step Pathogenesis:
Increased workload or hormonal signal ↓
Activation of signal transduction pathways (mechanical stretch, growth factors like IGF-1) ↓
Gene activation for structural proteins and enzymes ↓
Synthesis of more actin, myosin, mitochondria, etc. ↓
Enlargement of cell size ↓
Organ/tissue enlargement
🔬 Microscopic and Macroscopic Features
Microscopically:
Enlarged cells with abundant cytoplasm
Larger nuclei due to increased DNA content
Normal cell architecture usually preserved (in early stages)
Macroscopically:
Organs appear enlarged, firm, and heavy
🧠 Example: In cardiac hypertrophy, the heart wall thickens, especially the left ventricle.
🧠 Hypertrophy vs. Hyperplasia
Feature
Hypertrophy
Hyperplasia
Definition
Increase in cell size
Increase in cell number
Cell types
Occurs in non-dividing cells
Occurs in dividing cells
Examples
Cardiac hypertrophy, muscle growth
Endometrial hyperplasia, goiter
✅ Both may coexist (e.g., in uterus during pregnancy: hypertrophy + hyperplasia)
🏥 Clinical Relevance of Hypertrophy
Common Conditions:
Cardiac hypertrophy → leads to arrhythmias, heart failure
Skeletal muscle hypertrophy → fitness or compensatory adaptation
Prostate hypertrophy (BPH) → leads to urinary symptoms
Renal hypertrophy → one kidney enlarges if the other is removed
👩⚕️ Nursing and Practical Implications
Nurses should be aware of hypertrophy in the following ways:
✅ Assessment:
Monitor organ function (e.g., ECG in cardiac hypertrophy)
Check for functional limitations (e.g., reduced exercise tolerance)
✅ Education:
Teach patients about lifestyle factors (e.g., blood pressure control to prevent cardiac hypertrophy)
Explain the difference between adaptive and harmful growth
✅ Care Planning:
Adjust care for patients with enlarged hearts, prostates, or other affected organs
Collaborate with physicians to monitor hypertrophic progression using imaging or lab tests
📚 In Summary
Hypertrophy is the increase in cell size, leading to enlarged tissue/organ
It is an adaptive response to increased workload or hormonal signals
May be physiological (normal) or pathological (disease-related)
Reversible if the underlying cause is removed early
Common in muscles, heart, uterus, and kidneys
🔑 In the body’s silent language of survival, hypertrophy is how cells say, “Let me grow stronger to endure.”
🧬 Cellular Adaptation: Hyperplasia – When Cells Multiply to Meet Demand
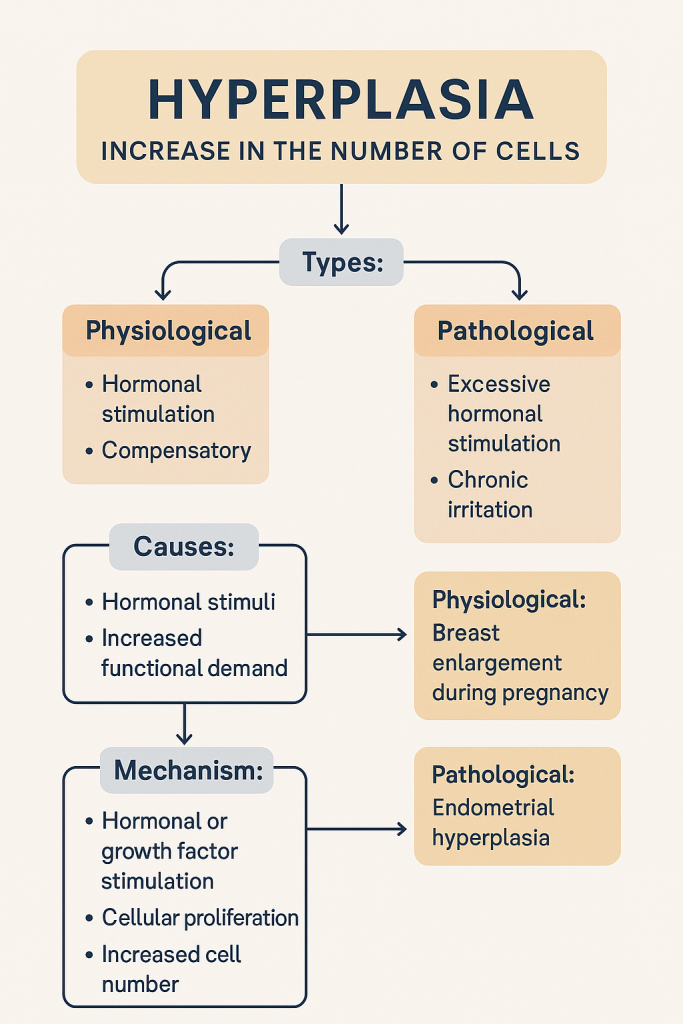
In the dynamic environment of the human body, when an organ or tissue is faced with increased demand or stimulation, one of the most elegant responses is hyperplasia — the increase in the number of cells, leading to tissue enlargement. Unlike hypertrophy (which increases cell size), hyperplasia results from cell proliferation, often in cells capable of mitosis.
This process can be physiological, helping the body adapt or heal, or pathological, contributing to disease. It is a cornerstone concept in understanding regenerative growth, hormonal responses, and tumor biology.
📖 What is Hyperplasia?
Definition: Hyperplasia is the increase in the number of cells in an organ or tissue, usually resulting in an increase in the volume of the organ, due to increased cell division (mitosis).
🧠 It occurs only in cells capable of proliferation — such as epithelial cells, glandular tissues, and connective tissues.
🧪 Types of Hyperplasia
🔹 1. Physiological Hyperplasia
A normal and controlled cell proliferation in response to a specific stimulus.
🧠 Examples:
Hormonal hyperplasia: → Endometrial growth during the menstrual cycle → Breast tissue enlargement during puberty/pregnancy
Compensatory hyperplasia: → Liver regeneration after partial hepatectomy → Skin regeneration after wound healing
🔹 2. Pathological Hyperplasia
An excessive and often uncontrolled proliferation that can lead to dysfunction or progress to cancer.
🧠 Examples:
Endometrial hyperplasia due to estrogen dominance (risk for carcinoma)
Benign prostatic hyperplasia (BPH) in older men → urinary issues
Viral-induced hyperplasia (e.g., warts caused by HPV)
⚠️ Pathological hyperplasia can be reversible if the stimulus is removed.
🧩 Mechanism / Pathogenesis of Hyperplasia
Hyperplasia results from activation of growth-promoting genes and cell signaling pathways that stimulate DNA replication and mitosis.
🧬 Step-by-Step Pathogenesis:
Hormonal or compensatory stimulus (e.g., estrogen, tissue loss) ↓
Binding to cell surface receptors ↓
Signal transduction pathways activated ↓
Transcription of growth-related genes ↓
DNA replication → mitosis ↓
Increased cell number in tissue
🧠 The process is highly regulated in physiological hyperplasia, but may become dysregulated in pathological states.
🔬 Microscopic and Macroscopic Features
Microscopically:
Increased number of normal-looking cells
Preserved architecture (in benign hyperplasia)
May show nuclear crowding or mild atypia in pathological cases
Macroscopically:
Organs appear enlarged and firm
May form nodules (e.g., prostate in BPH)
🧠 Hyperplasia vs. Hypertrophy
Feature
Hyperplasia
Hypertrophy
Cell change
Increase in number of cells
Increase in size of cells
Cell type
Occurs in dividing cells
Occurs in non-dividing cells
Examples
Endometrium, liver, prostate
Skeletal muscle, cardiac muscle
Coexistence
Can occur together
Yes — e.g., in pregnant uterus
🏥 Clinical Relevance of Hyperplasia
Condition
Clinical Significance
BPH (Benign Prostatic Hyperplasia)
Urinary retention, urgency, nocturia
Endometrial Hyperplasia
Abnormal uterine bleeding, risk of cancer
Psoriasis
Epidermal hyperplasia
Warts (HPV)
Viral-induced epithelial hyperplasia
📌 Understanding hyperplasia helps identify and treat early changes that may progress to malignancy.
Teach about risk factors (e.g., obesity and estrogen dominance)
Promote screening (e.g., Pap smear for cervical hyperplasia)
✅ Interventions:
Support treatment (e.g., hormonal therapy in endometrial hyperplasia)
Assist in monitoring regrowth or recurrence post-surgery (e.g., TURP in BPH)
📚 In Summary
Hyperplasia = Increase in cell number → enlarged organ/tissue
Can be physiological (hormonal, compensatory) or pathological
Mechanism involves growth factors, gene activation, and mitosis
Occurs in dividing cells (unlike hypertrophy)
Nurses play a role in early detection, management, and patient education
🔑 Hyperplasia is the body’s way of saying, “More hands are needed.” Sometimes it helps — and sometimes it goes too far.
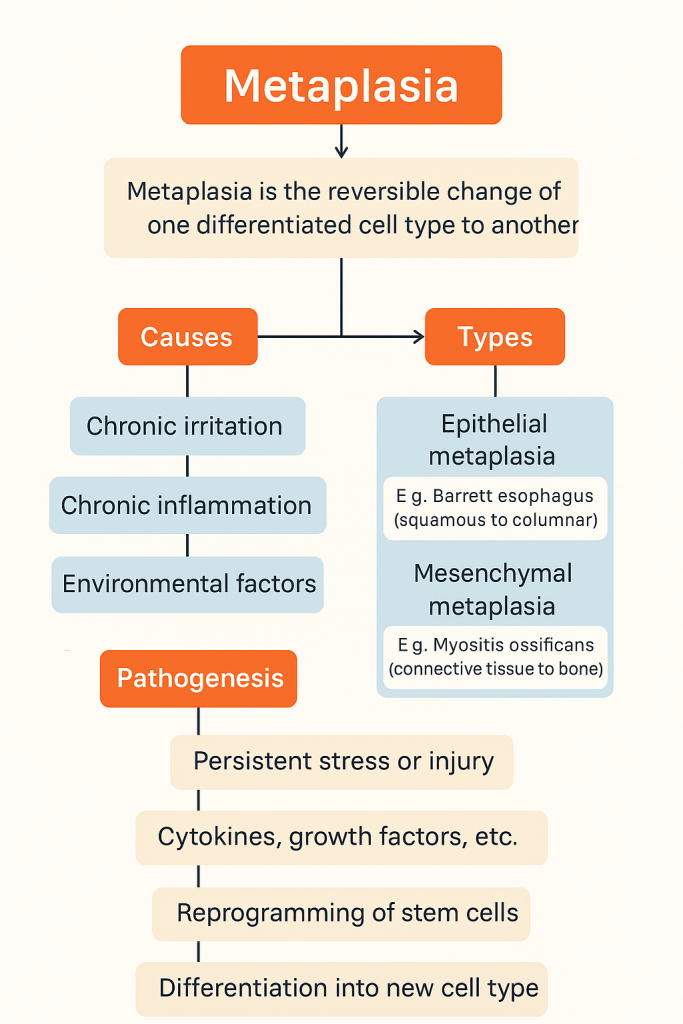
🔄 Cellular Adaptation: Metaplasia – A Change for Survival
In the face of chronic stress or irritation, some cells opt not to shrink or die, but to transform. This fascinating adaptive process is called metaplasia — where one mature cell type is replaced by another mature cell type that is better suited to endure the new environment. It’s like swapping one profession for another under pressure — an engineer becoming a firefighter during a disaster.
Metaplasia is a reversible, protective cellular response, but if the underlying stimulus persists, it may lay the groundwork for dysplasia and malignancy.
📖 What is Metaplasia?
Definition: Metaplasia is a reversible change in which one differentiated (mature) cell type is replaced by another differentiated cell type of the same germ layer, often as an adaptive response to chronic irritation or environmental stress.
🧠 Usually involves epithelial or mesenchymal cells (connective tissue).
⚠️ It is not a change in the existing cells, but a reprogramming of stem cells to produce a different lineage.
🧠 Why Does Metaplasia Occur?
Metaplasia occurs when cells adapt to a hostile or damaging environment. The new cell type is often more resistant, but less specialized, which can affect function.
🧠 Example: In chronic smokers, the normal ciliated columnar epithelium in the trachea is replaced by stratified squamous epithelium to better withstand chemical injury — but at the cost of lost mucociliary function.
Cytokines, growth factors, and extracellular matrix signals released ↓
Reprogramming of stem cells or undifferentiated mesenchymal cells ↓
Cells begin to differentiate into a new cell type ↓
New tissue better resists injury, but may compromise function ↓
If stress persists → dysplasia → potential neoplasia
🔬 Types of Metaplasia
🔹 Epithelial Metaplasia (Most Common)
Original Cell Type
Replaced With
Example
Ciliated columnar epithelium
Stratified squamous epithelium
Respiratory tract of smokers
Stratified squamous epithelium
Columnar epithelium (intestinal type)
Barrett’s esophagus (due to acid reflux)
Transitional epithelium (bladder)
Squamous epithelium
Chronic cystitis
🔹 Mesenchymal (Connective Tissue) Metaplasia
Original Cell Type
Replaced With
Example
Connective tissue
Cartilage or bone
Myositis ossificans in injured muscle
🧬 Is Metaplasia Harmful or Helpful?
✅ Protective in the short term — reduces vulnerability to stress. ❌ Potentially harmful if the stimulus persists — may lead to dysplasia and cancer.
🧠 Example:
Barrett’s esophagus → metaplasia from squamous to columnar epithelium → risk of esophageal adenocarcinoma if untreated
🧾 Microscopic Features
Mature, differentiated cells of an abnormal type for that location
No atypia or uncontrolled proliferation (unless it progresses to dysplasia)
No inflammation, unless due to underlying cause (e.g., chronic infection)
🏥 Clinical Examples of Metaplasia
Condition
Cellular Change
Cause
Smoker’s airway
Columnar → Squamous
Chronic smoke exposure
Barrett’s esophagus
Squamous → Columnar (intestinal type)
Chronic GERD
Chronic cervicitis
Columnar → Squamous
Chronic infection/injury
Bladder in chronic infection
Transitional → Squamous
Recurrent UTIs
Myositis ossificans
Muscle → Bone (connective tissue metaplasia)
Trauma or inflammation
👩⚕️ Nursing & Clinical Implications
Nurses and clinicians must:
✅ Recognize symptoms of chronic irritation (e.g., heartburn, cough, infections) ✅ Educate patients on lifestyle risks (e.g., smoking, acid reflux) ✅ Encourage screening for conditions like Barrett’s esophagus ✅ Monitor for signs of progression to dysplasia or cancer ✅ Support care for biopsy, imaging, or medication therapy
📚 In Summary
Metaplasia is a reversible cellular adaptation involving replacement of one mature cell type by another
It occurs due to chronic irritation or inflammation
Common in epithelial and connective tissues
It may protect temporarily but can progress to dysplasia and cancer
Nurses play a key role in identifying risks, promoting prevention, and supporting early treatment
🔑 When cells change their identity to survive, we must change our care to prevent disease progression.
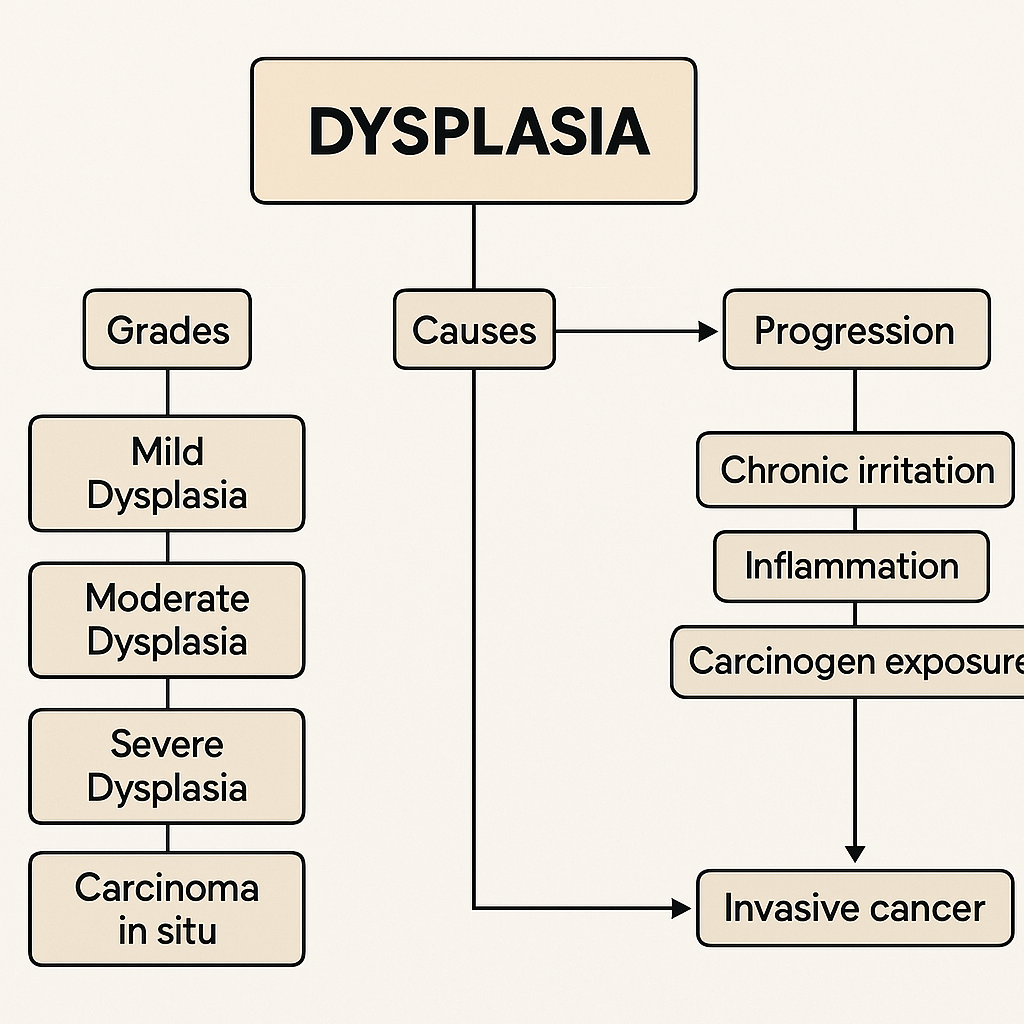
🧬 Cellular Adaptation: Dysplasia – The Warning Sign Before Cancer
Among all cellular adaptations, dysplasia stands out as a red flag — a warning that cells are beginning to lose their normal structure, function, and control. Unlike the more orderly adaptations like hypertrophy or metaplasia, dysplasia is disorganized, erratic, and potentially dangerous.
Though still reversible in its early stages, dysplasia is considered a precursor to cancer, especially when seen in epithelial tissues. Understanding it is crucial in clinical diagnosis, screening, and cancer prevention.
📖 What is Dysplasia?
Definition: Dysplasia is a disordered and abnormal development of cells, characterized by:
Loss of cellular uniformity
Disturbed architecture
Nuclear atypia and increased mitosis
It often affects epithelial tissues and reflects pre-malignant changes. If the abnormal stimulus persists, dysplasia can progress to carcinoma in situ, and ultimately to invasive cancer.
🧠 Key Concept: Dysplasia = Disorganized but non-invasive growth.
🧠 Is Dysplasia an Adaptation or a Disease?
While earlier adaptations (like hyperplasia or metaplasia) are controlled and purposeful, dysplasia is considered a pathological deviation — not an adaptation. It reflects a failure of normal maturation and control mechanisms in cell replication.
🧩 Causes of Dysplasia
Dysplasia arises due to chronic irritation, inflammation, or exposure to carcinogens, which disrupt normal cell regulation.
🔹 Common Causes:
Persistent infections (e.g., HPV in the cervix)
Chronic inflammation (e.g., gastritis in H. pylori infection)
Exposure to toxins or carcinogens (e.g., tobacco smoke)
Untreated metaplasia
Radiation or chemical injury
🔬 Pathological Features of Dysplasia
🔍 Microscopic Changes:
Pleomorphism: Variability in cell and nuclear size/shape
Hyperchromatism: Dark, densely staining nuclei
Increased mitotic figures, some abnormal
Loss of polarity: Disrupted alignment of cells
Disorganized epithelial layering
⚠️ Despite these changes, in dysplasia the basement membrane is intact — there is no invasion, distinguishing it from cancer.
🧪 Classification of Dysplasia
Grade
Extent of Abnormality
Clinical Relevance
Mild Dysplasia
Lower 1/3 of epithelium affected
May regress with treatment
Moderate Dysplasia
Up to 2/3 affected
Needs monitoring and intervention
Severe Dysplasia
More than 2/3 but not full thickness
Pre-cancerous; high risk
Carcinoma in situ
Full thickness dysplasia, non-invasive
Immediate treatment required
📘 Common Sites of Dysplasia
Tissue
Condition / Example
Cervix
Cervical intraepithelial neoplasia (CIN)
Respiratory tract
Squamous dysplasia in smokers
Esophagus
Dysplasia in Barrett’s esophagus
Colon
Adenomatous polyps showing dysplastic changes
Skin
Actinic keratosis (sun-induced dysplasia)
🏥 Clinical Importance of Dysplasia
Premalignant: A strong predictor of cancer development if untreated
Screenable: Can be detected by Pap smears, endoscopy, skin exams
Reversible: If the cause is removed early (e.g., HPV treatment, smoking cessation)
Monitorable: Requires biopsy, grading, and sometimes removal
Educate patients about screening programs (Pap test, colonoscopy)
✅ Prevention:
Promote vaccinations (e.g., HPV vaccine)
Support smoking cessation and lifestyle modification
✅ Follow-Up:
Monitor biopsy reports and histology findings
Encourage adherence to follow-up screening
Support emotional and psychological care in patients with pre-cancerous diagnoses
📚 In Summary
Dysplasia is a precancerous cellular abnormality, marked by disorganized cell growth, nuclear changes, and architectural loss
It is not cancer, but may become cancer if left untreated
Graded based on severity (mild → carcinoma in situ)
Found commonly in epithelial tissues exposed to chronic injury or infection
Nurses play a vital role in education, screening, prevention, and early intervention
🔑 Dysplasia is a crossroad — early detection means we can turn back before reaching cancer.
Certainly! Here’s a detailed, academic, and engaging explanation of Apoptosis — a crucial physiological process — presented in a structured and attractive format ideal for nursing, medical, and paramedical learners.
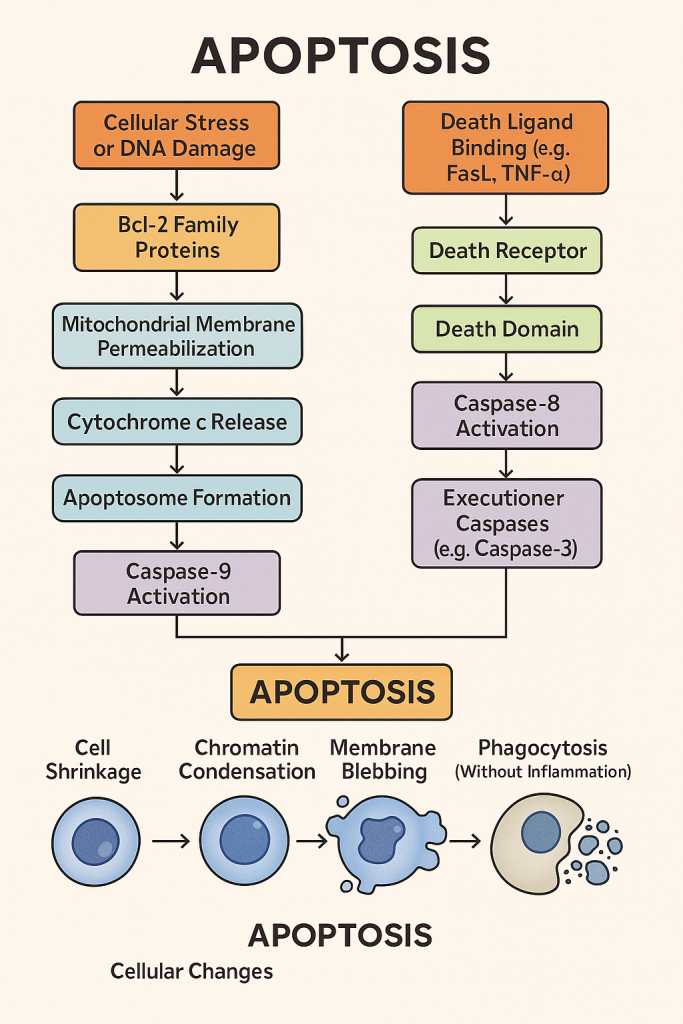
🌱 Apoptosis – The Art of Cellular Self-Destruction
Not all cell deaths are chaotic or damaging. Some are carefully planned and beneficial, like a leaf falling in autumn to make room for new growth. This process is known as apoptosis, or programmed cell death — an elegant, tightly regulated cellular event that shapes the body during development, maintains tissue health, and protects against disease.
Unlike necrosis, which is accidental and inflammatory, apoptosis is controlled, clean, and quiet, ensuring the cell dies without disturbing its neighbors.
📖 What is Apoptosis?
Definition: Apoptosis is a genetically controlled, energy-dependent process of programmed cell death, in which a cell activates its own internal machinery to self-destruct in a safe and non-inflammatory manner.
It is essential for:
Developmental sculpting (e.g., fingers separating in the embryo)
Immune regulation
Removal of damaged or old cells
Cancer prevention
🧠 Think of apoptosis as the body’s internal “quality control” system.
🧩 Features of Apoptosis
Apoptosis
Necrosis
Programmed, regulated
Accidental, uncontrolled
Individual cells affected
Groups of cells affected
No inflammation
Often causes inflammation
Membrane stays intact
Membrane ruptures
Cell shrinks (cellular condensation)
Cell swells (hydropic change)
DNA fragmentation in a regular pattern
Random DNA breakdown
⚙️ Mechanism / Pathogenesis of Apoptosis
Apoptosis can be triggered via two main pathways:
🔹 1. Intrinsic (Mitochondrial) Pathway
Triggered by internal stress like:
DNA damage
Growth factor withdrawal
Oxidative stress
Mitochondria release cytochrome c
Activates caspase-9 → initiator caspase
Leads to executioner caspase activation (e.g., caspase-3)
Cell undergoes orderly disassembly
🔹 2. Extrinsic (Death Receptor) Pathway
Triggered by external signals:
Binding of Fas ligand or TNF-α to death receptors
Activates caspase-8 (initiator)
Converges with intrinsic pathway at executioner phase
🧪 Key Steps in Apoptosis (Regardless of Trigger):
Cell shrinkage
Chromatin condensation
Nuclear fragmentation (karyorrhexis)
Blebbing of plasma membrane
Formation of apoptotic bodies
Phagocytosis by macrophages (no inflammation)
🔬 Microscopic Appearance of Apoptotic Cells
Shrunken cells with dense cytoplasm
Pyknotic nuclei (condensed)
No surrounding inflammation
“Apoptotic bodies” visible (fragments enclosed in membrane)
Autoimmune diseases (failure to delete self-reactive cells)
Viral infections (some viruses block apoptosis to persist)
🧠 Apoptosis vs. Necrosis – A Quick Review
Feature
Apoptosis
Necrosis
Type of death
Programmed (suicide)
Accidental (homicide)
Trigger
Internal or external signals
Injury, infection, toxins
Cell membrane
Intact, blebbing
Ruptured
DNA fragmentation
Ordered (ladder pattern)
Random
Inflammation
No
Yes
Clinical relevance
Seen in development, cancer therapy
Seen in infarctions, infections
👩⚕️ Nursing & Clinical Implications
✅ Why Nurses Should Understand Apoptosis:
Assists in understanding cancer resistance to chemotherapy
Helps explain tissue loss in neurodegenerative and autoimmune conditions
Supports education in cancer screening and therapy
Enhances ability to interpret biopsy reports or disease prognosis
🧬 Therapies like chemotherapy and radiation aim to re-trigger apoptosis in cancer cells that have evaded it.
📚 In Summary
Apoptosis is a natural, regulated process of cell death that maintains tissue health
Triggered via intrinsic (mitochondrial) or extrinsic (death receptor) pathways
Involves caspases, DNA fragmentation, and cell shrinkage without inflammation
Vital in development, immune control, and disease prevention
Dysregulation of apoptosis contributes to cancer, autoimmune disorders, and degenerative diseases
🔑 Apoptosis is the body’s silent guardian — removing flawed cells before they become a threat.
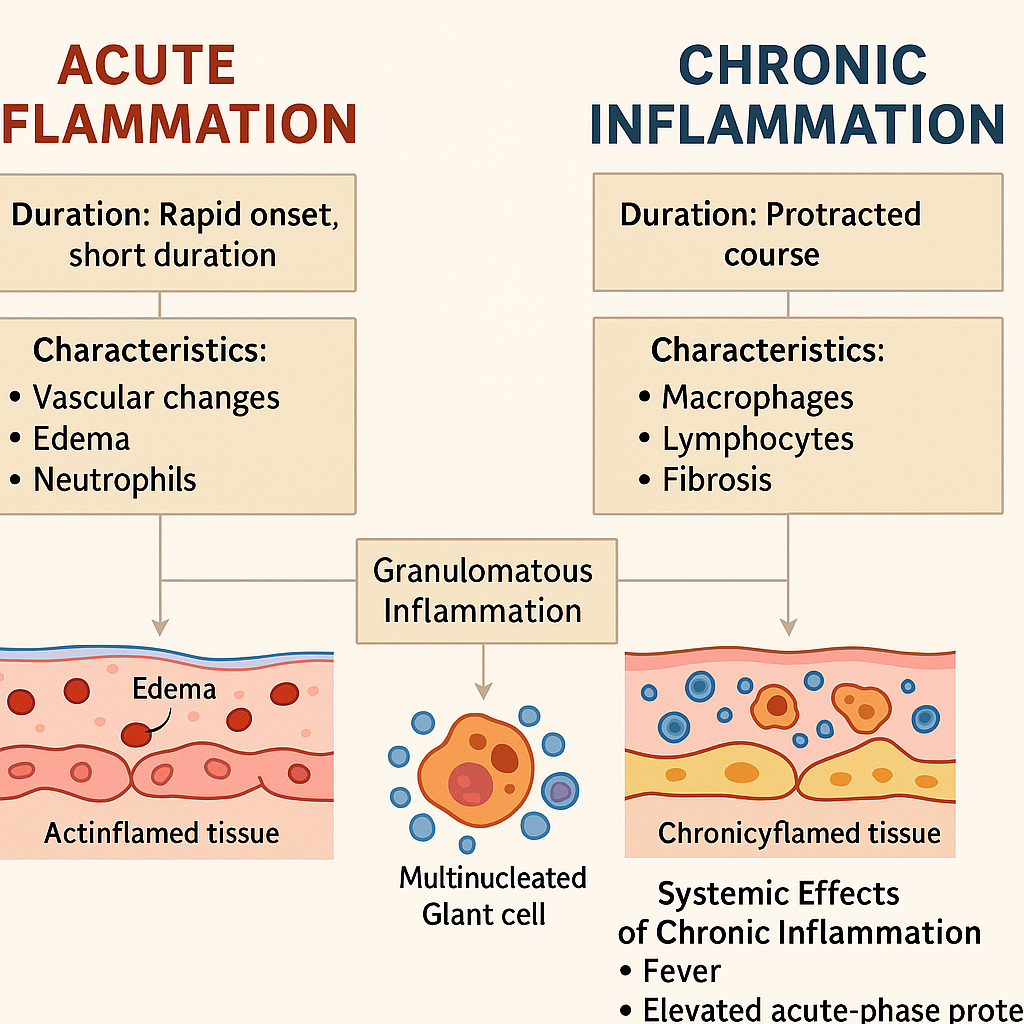
🔥 Acute Inflammation – The Body’s First Responder
Inflammation is the body’s protective, biological response to injury, infection, or irritation. When tissues are damaged, the immune system kicks into action to isolate, eliminate, and initiate repair. The earliest and most intense phase of this defense is called acute inflammation.
Acute inflammation is rapid in onset, short in duration (hours to days), and characterized by exudation of plasma and migration of leukocytes, particularly neutrophils. Its primary goal? Neutralize the threat and initiate healing — all while trying to limit collateral damage.
📖 Definition of Acute Inflammation
Acute inflammation is a rapid, nonspecific response of vascularized tissue to injury or infection, characterized by:
Vascular changes
Edema (fluid exudation)
Migration of leukocytes (mainly neutrophils)
🔍 It is the body’s emergency alarm system and clean-up crew combined.
🧠 Classical Signs of Acute Inflammation (Celsus & Galen)
Latin Term
English Translation
Cause
Rubor
Redness
Vasodilation and increased blood flow
Calor
Heat
Increased blood flow and metabolic activity
Tumor
Swelling
Fluid exudation and cell infiltration
Dolor
Pain
Chemical mediators (e.g., bradykinin, PGE2)
Functio laesa
Loss of function
Pain and swelling impair tissue activity
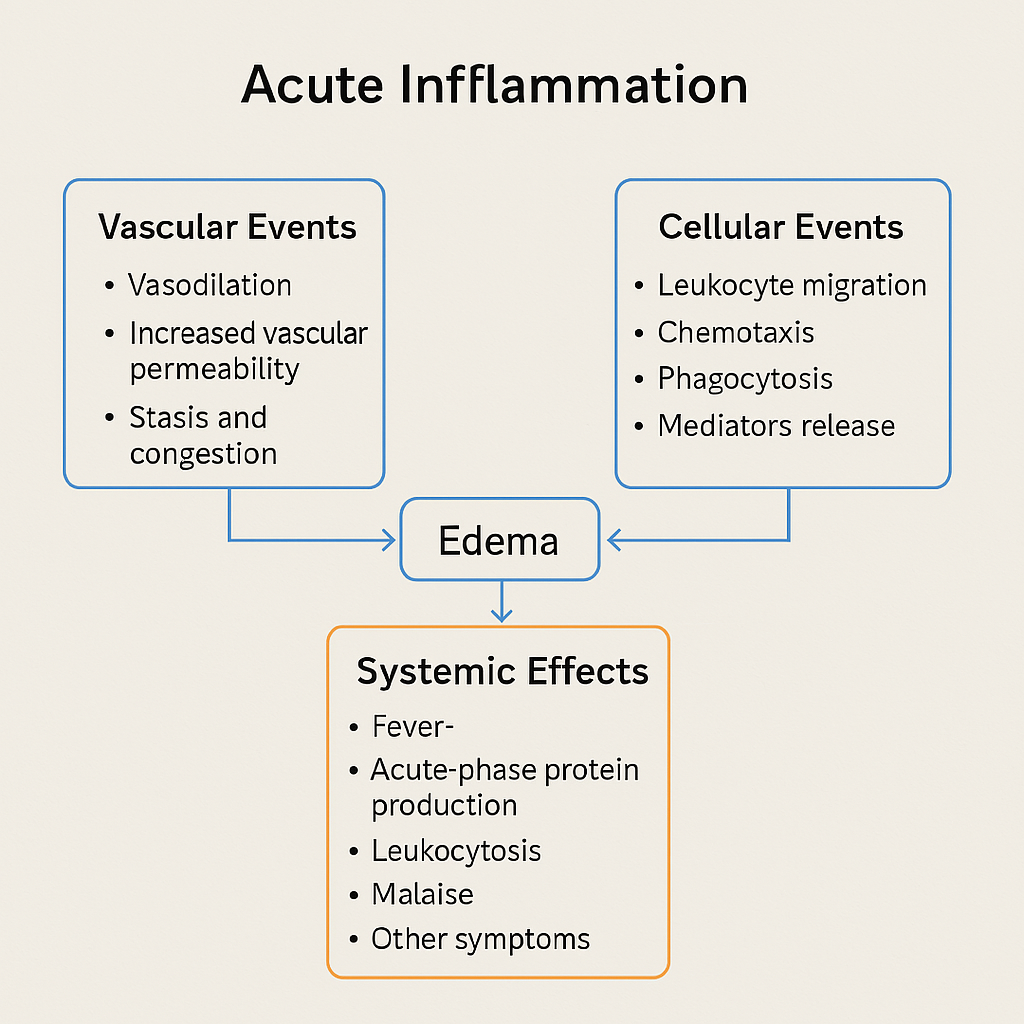
🧬 I. Vascular Events of Acute Inflammation
These events prepare the tissue bed for leukocyte arrival and immune action.
🔹 1. Vasodilation
Initiated by histamine, nitric oxide, and prostaglandins
Leads to increased blood flow → redness and warmth
🔹 2. Increased Vascular Permeability
Endothelial cells contract or get damaged, creating gaps
Plasma proteins (fibrinogen, antibodies) and fluid leak into tissue → edema
🔹 3. Slowing of Blood Flow (Stasis)
As fluid leaves vessels, blood becomes more concentrated
Neutrophils recognize pathogens via PRRs (e.g., TLRs) and opsonins (e.g., IgG, C3b)
🔸 3. Phagocytosis
Ingest pathogens into a phagosome
Fuses with lysosomes → phagolysosome
🔸 4. Killing and Degradation
Reactive oxygen species (ROS) and enzymes (e.g., myeloperoxidase) destroy pathogens
🔸 5. Resolution or Progression
If successful, inflammation resolves
If the injury persists, it may progress to chronic inflammation or cause tissue damage
🌡️ III. Systemic Effects of Acute Inflammation
The effects of inflammation extend beyond the local site when cytokines enter the bloodstream.
🩺 1. Fever
IL-1 and TNF-α stimulate prostaglandin E2 in the hypothalamus
Raises body temperature to inhibit pathogens
🩺 2. Acute Phase Protein Production
Liver releases proteins like:
C-reactive protein (CRP)
Fibrinogen
Serum amyloid A (SAA)
Increases ESR (erythrocyte sedimentation rate) — a nonspecific marker of inflammation
🩺 3. Leukocytosis
Increased WBC count, especially neutrophils
Left shift = more immature neutrophils (bands)
🩺 4. Constitutional Symptoms
Malaise, fatigue, anorexia, muscle pain, and chills due to systemic cytokines
🩺 5. Septic Shock (Severe Cases)
Massive cytokine release → vasodilation, hypotension, organ failure
Caused by infections, especially gram-negative bacteria
🧾 Outcomes of Acute Inflammation
Outcome
Description
✅ Resolution
Complete return to normal if injury is minor
➖ Suppuration
Formation of pus (abscess) due to neutrophils + debris
➖ Healing by fibrosis
Scar formation if tissue cannot regenerate
❌ Progression
Becomes chronic inflammation if stimulus persists
👩⚕️ Nursing and Clinical Relevance
Understanding acute inflammation enables nurses to:
✅ Monitor signs of infection (fever, swelling, discharge) ✅ Explain lab values (e.g., ↑ CRP, ↑ WBC, ↑ ESR) ✅ Implement anti-inflammatory treatments (NSAIDs, cold therapy) ✅ Educate patients about the healing process ✅ Recognize early signs of sepsis or systemic inflammation
📌 Inflammatory responses, though protective, can become dangerous — nurses are key in recognizing when defense turns into damage.
📚 In Summary
Acute inflammation is an early, protective response to injury or infection
It involves vascular changes, leukocyte migration, and systemic effects
Mediated by cytokines, histamine, prostaglandins, and immune cells
If resolved, leads to healing; if not, can progress to chronic inflammation or abscess
🔑 Inflammation is the body’s built-in emergency system — powerful, necessary, but sometimes in need of regulation.
🔥🧬 Chronic Inflammation – When Defense Becomes a Long-Term Battle
While acute inflammation is the body’s emergency response team, chronic inflammation is more like a long-term standoff — a persistent, simmering war between injurious agents and the immune system. Unlike the rapid-onset, short-lived nature of acute inflammation, chronic inflammation is prolonged, less intense, and often subtle in onset — but its consequences can be far more destructive.
📖 Definition of Chronic Inflammation
Chronic inflammation is a prolonged inflammatory response characterized by:
Simultaneous tissue destruction and healing attempts
Presence of mononuclear inflammatory cells (macrophages, lymphocytes, plasma cells)
Often follows unresolved acute inflammation or arises de novo in response to low-grade persistent irritants
🧠 It’s a cycle of damage, repair, and further damage — often seen in autoimmune disorders, infections, and chronic irritant exposure.
Key players in phagocytosis, cytokine release, and tissue destruction
Secrete growth factors for repair and fibrosis
🔹 2. Lymphocytes (T & B cells)
T cells: Activate macrophages and help sustain inflammation
B cells → Plasma cells: Produce antibodies against persistent antigens
🔹 3. Eosinophils
Prominent in parasitic infections and allergic diseases
🔹 4. Mast cells
Release histamine, play roles in both acute and chronic inflammation
🌰 Granulomatous Inflammation – A Special Type of Chronic Inflammation
📖 Definition:
Granulomatous inflammation is a distinctive pattern of chronic inflammation where the immune system tries to wall off a foreign substance it cannot eliminate.
🔹 Key Histologic Feature:
Granuloma: A focal aggregation of macrophages that appear as epithelioid cells, often surrounded by lymphocytes and sometimes multinucleated giant cells
🧠 Types of Granulomas
Type
Cause/Trigger
Example
Caseating granuloma
Central necrosis
Tuberculosis
Non-caseating granuloma
No necrosis
Sarcoidosis, Crohn’s disease
Foreign body granuloma
Reaction to inert materials
Talc, sutures, splinters
🔬 Composition of a Granuloma
Epithelioid macrophages (transformed from monocytes)
Multinucleated giant cells (Langhans-type)
Peripheral lymphocytes
May show central necrosis (in infections like TB)
🌡️ Systemic Effects of Chronic Inflammation
When inflammatory mediators spill into the bloodstream, chronic inflammation can affect multiple systems.
🧪 1. Constitutional Symptoms
Low-grade fever
Fatigue, malaise
Weight loss
Anemia of chronic disease
🧫 2. Acute Phase Protein Elevation
Liver increases production of:
C-reactive protein (CRP)
Serum amyloid A (SAA)
Fibrinogen → ↑ ESR
Contributes to chronic inflammatory burden
🦴 3. Anemia of Chronic Disease
Inflammatory cytokines impair iron utilization and erythropoiesis
Common in RA, TB, chronic infections
🧠 4. Tissue Destruction and Fibrosis
Chronic inflammation leads to ongoing tissue injury
Monitor for systemic signs (fatigue, weight loss, joint pain)
Evaluate chronic wounds, ulcers, or infections
✅ Support & Education:
Educate about chronic disease progression (RA, Crohn’s, TB)
Reinforce adherence to long-term therapy (e.g., immunosuppressants, antibiotics)
✅ Collaborative Care:
Work with physicians to monitor CRP, ESR, hemoglobin
Assist in procedures like biopsy, imaging, or sputum testing in suspected granulomatous disease
📚 In Summary
Chronic inflammation is long-lasting, marked by macrophages, lymphocytes, and fibrosis
Granulomatous inflammation is a specialized form seen in TB, sarcoidosis, and more
Systemic effects include anemia, fever, fatigue, and organ dysfunction
Nurses play a crucial role in early recognition, symptom management, and patient education
🔑 Chronic inflammation is the body’s ongoing negotiation with danger — but if the battle drags on too long, healing turns to harm.
Absolutely! Here’s a detailed, academic, and well-structured narrative explanation of Wound Healing, written in an engaging, clinical-friendly style perfect for nursing, medical, and allied health learners.
🩹 Wound Healing – The Body’s Marvel of Regeneration and Repair
Every time you get a cut, a burn, or undergo surgery, your body begins an orchestrated biological process to restore tissue integrity. This miracle of self-repair is called wound healing — a complex, dynamic process involving cells, cytokines, growth factors, and structural proteins. Whether the damage is superficial or deep, wound healing is essential to prevent infection, restore function, and maintain the body’s protective barrier.
📖 Definition of Wound Healing
Wound healing is the restorative process by which the body repairs tissue damage after injury. It involves inflammation, new tissue formation, and remodeling, resulting in either regeneration (complete restoration) or scar formation (repair).
🧠 Wound healing is both cellular choreography and molecular teamwork.
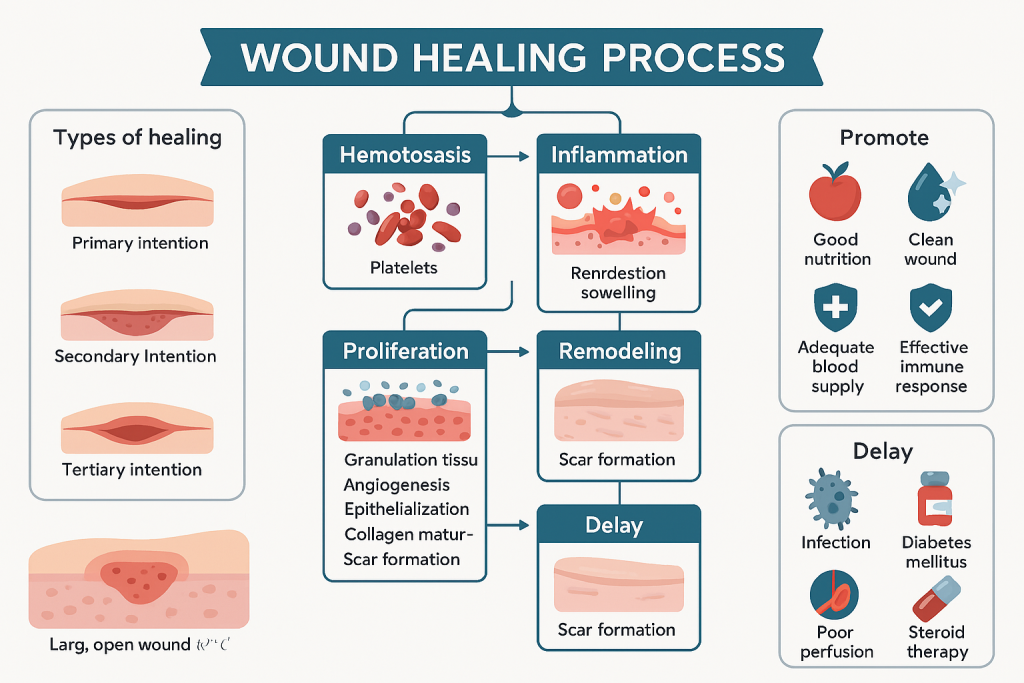
🧪 Phases of Wound Healing (4 Overlapping Stages)
⏱️ 1. Hemostasis (Immediate – within minutes)
Goal: Stop bleeding and initiate the healing cascade.
🔹 Vasoconstriction → Platelet plug formation 🔹 Platelets release clotting factors and growth factors (PDGF, TGF-β) 🔹 Fibrin clot forms → stabilizes wound and acts as a scaffold
🩸 Hemostasis = Biological band-aid
🔥 2. Inflammatory Phase (Day 0–3)
Goal: Remove debris, pathogens, and recruit immune cells.
🔹 Vasodilation → increases permeability 🔹 Neutrophils arrive first: phagocytosis of bacteria and damaged cells 🔹 Macrophages follow: release cytokines and growth factors 🔹 Redness, swelling, warmth, pain are classic signs
🛡️ Inflammation = Wound defense and cleanup
🌱 3. Proliferative Phase (Day 3–10)
Goal: Rebuild tissue matrix and blood supply.
🔹 Fibroblasts lay down collagen and extracellular matrix 🔹 Angiogenesis: new capillaries form (driven by VEGF) 🔹 Granulation tissue fills the wound: soft, red, and vascular 🔹 Epithelialization: new skin cells migrate to cover the wound 🔹 Wound contracts (via myofibroblasts)
🔹 Type III collagen is replaced by Type I collagen 🔹 Collagen is cross-linked for tensile strength 🔹 Capillaries regress → scar becomes pale and flat 🔹 Final tensile strength = ~70–80% of original tissue
Wound healing is a multi-phase process: hemostasis → inflammation → proliferation → remodeling
Healing can occur by primary, secondary, or tertiary intention
Influenced by local and systemic factors (nutrition, infection, disease)
Nurses are critical in monitoring, supporting, and educating during wound healing
🔑 Healing is the body’s art of restoration — with the nurse as its skilled guide and guardian.
🌱 Neoplasia: Nomenclature, Normal vs. Cancer Cells – A Detailed Academic Overview
🔍 I. What is Neoplasia?
The term Neoplasia literally means “new growth.” It refers to the abnormal and uncontrolled proliferation of cells, forming a mass or neoplasm (tumor). Neoplasia differs from hyperplasia and regeneration because it persists even after the causative stimulus is removed.
🧬 Definition:
Neoplasia is the process of abnormal and autonomous cell proliferation that results in the formation of a mass of tissue called a neoplasm or tumor.
📘 II. Nomenclature of Neoplasms
Medical naming of neoplasms follows a systematic classification based on:
Tissue of origin
Benign or malignant nature
Microscopic characteristics
A. 🌿 Benign Tumors
Grow slowly, well-demarcated
Usually non-invasive, and do not metastasize
Named with suffix “-oma”
Tissue Type
Benign Tumor Name
Fibrous tissue
Fibroma
Adipose tissue
Lipoma
Cartilage
Chondroma
Glandular epithelium
Adenoma
Smooth muscle
Leiomyoma
B. 🔥 Malignant Tumors
Rapid growth, poorly demarcated
Invasive and metastatic
Named based on origin with:
“-carcinoma” for epithelial origin
“-sarcoma” for mesenchymal origin
Tissue Type
Malignant Tumor Name
Epithelial tissue
Adenocarcinoma, Squamous cell carcinoma
Connective tissue
Fibrosarcoma, Osteosarcoma
Blood-forming tissue
Leukemia, Lymphoma
Melanocytes
Melanoma (Note: Always malignant)
📝 Special Terms:
Teratoma: Tumor containing multiple germ layers
Blastoma: Arises from embryonic tissues (e.g., retinoblastoma)
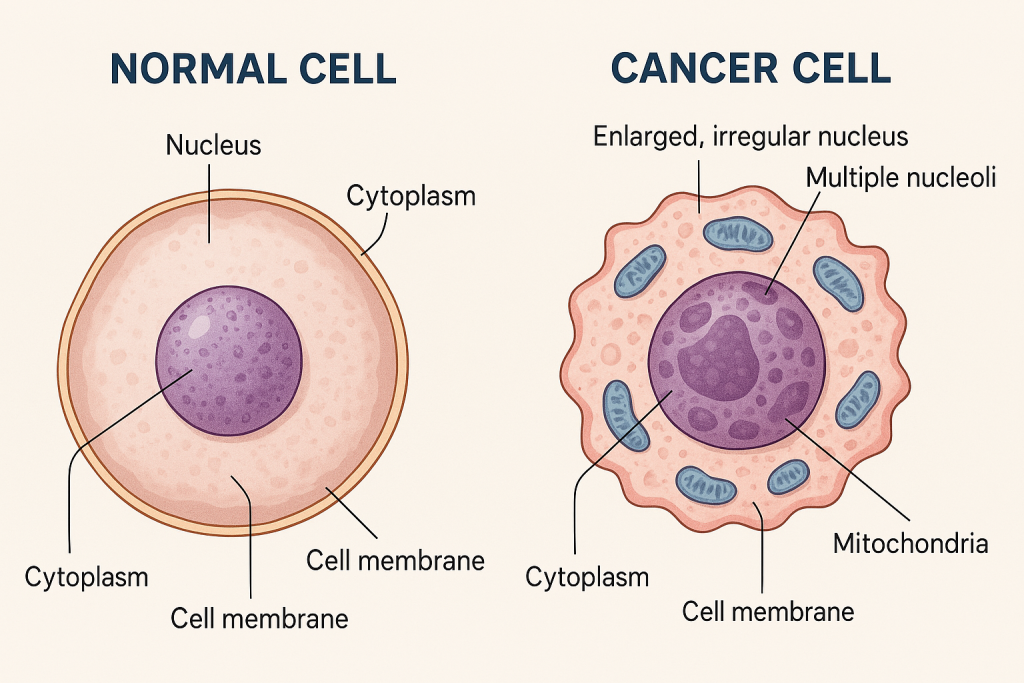
🧠 III. Difference Between Normal and Cancer Cells
Feature
Normal Cells
Cancer Cells
Growth Regulation
Controlled by signals
Uncontrolled; ignores regulatory signals
Cell Cycle
Normal checkpoints and repair mechanisms
Mutated checkpoints; avoids apoptosis
Cell Morphology
Uniform, organized
Irregular size, shape, and disorganized structure
Function
Differentiated and specific
Loss of specialization (dedifferentiation)
Contact Inhibition
Stop dividing when in contact with other cells
Loss of contact inhibition; grow over boundaries
Lifespan
Finite (undergo senescence)
Immortal due to telomerase activation
Genetic Stability
Stable DNA with repair systems
Genomic instability and mutations
Metastasis Potential
None
Can invade and spread to other tissues
Angiogenesis
Normal blood supply
Induces abnormal new blood vessels (VEGF)
🔬 Cancer cells behave like “selfish cells” – they prioritize their own survival and proliferation over the host body’s normal functions, often to the detriment of the organism.
🧬 V. Key Characteristics of Neoplasia
🔹 Autonomous Growth – independent of physiological growth signals 🔹 Genetic Instability – mutations in oncogenes, tumor suppressor genes 🔹 Invasiveness – potential to destroy adjacent tissues 🔹 Metastasis – ability to colonize distant organs
🧪 VI. Clinical Relevance in Nursing
👩⚕️ As a nurse, understanding neoplasia helps in:
Early detection of abnormal growths
Monitoring for metastasis
Providing emotional and physical support to patients undergoing cancer diagnosis or therapy
Educating patients about risk factors and preventive strategies
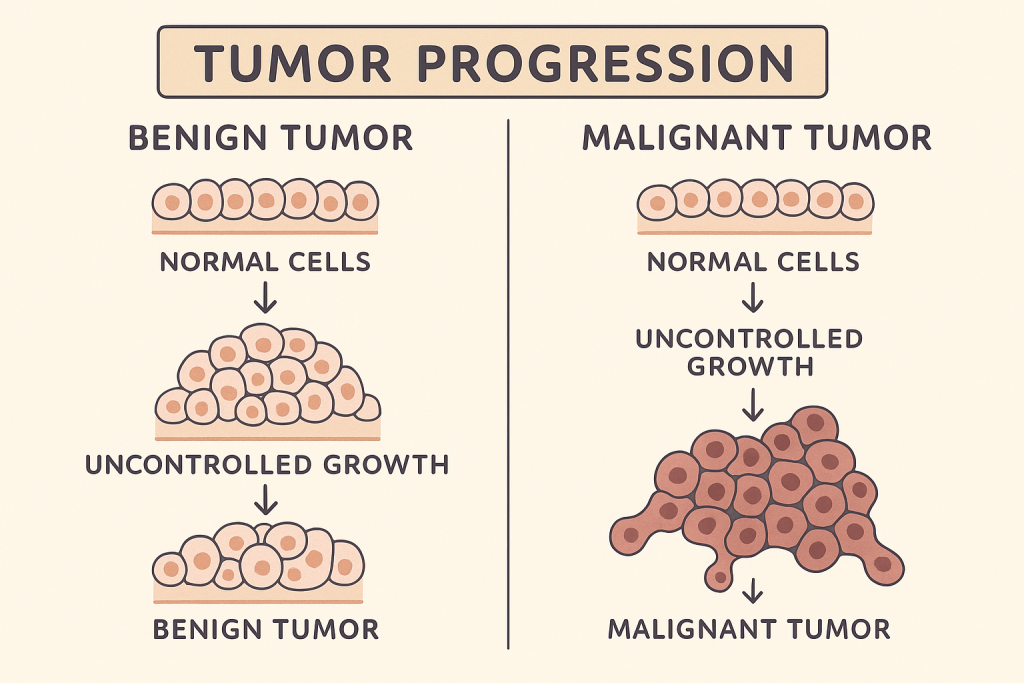
🧠 Benign and Malignant Tumors:
🔍 I. Introduction to Tumors
The term tumor (or neoplasm) refers to an abnormal mass of tissue that arises from uncontrolled cell proliferation. Tumors are classified into two major types:
Benign Tumors (non-cancerous)
Malignant Tumors (cancerous)
While both types originate from abnormal cell growth, their behavior, growth pattern, recurrence, and prognosis differ significantly.
🌱 II. Benign Tumors
📖 Definition:
A benign tumor is a non-cancerous growth of cells that remains localized and does not invade surrounding tissues or metastasize to distant organs.
A malignant tumor is a cancerous growth characterized by uncontrolled cell division, local tissue invasion, and the ability to spread (metastasize) to distant organs.
🧬 Characteristics of Malignant Tumors:
🔸 Feature
🔺 Malignant Tumors
Growth Rate
Rapid and uncontrollable
Borders
Poorly defined, infiltrative
Invasiveness
Invades surrounding tissues
Metastasis
Present – spreads via blood or lymph
Cell Differentiation
Poorly differentiated or undifferentiated (anaplasia)
Malignant tumors are life-threatening, require multimodal treatment, and demand early diagnosis for better outcomes.
🧾 IV. Summary Table: Benign vs. Malignant Tumors
🧪 Feature
✅ Benign Tumor
⚠️ Malignant Tumor
Growth Speed
Slow
Rapid
Differentiation
Well-differentiated
Poorly differentiated (Anaplasia)
Encapsulation
Encapsulated
Not encapsulated
Invasion
No tissue invasion
Invasive
Metastasis
Absent
Present (blood/lymph spread)
Recurrence
Rare
Common
Systemic Effects
Minimal
Weight loss, anemia, cachexia
Prognosis
Good (after removal)
Poor (depends on stage and grade)
💡 VI. Nursing Relevance
👩⚕️ Nurses play a vital role in:
Recognizing warning signs of malignancy (e.g., unexplained weight loss, lumps)
Educating patients about tumor behavior and screening
Providing emotional and physical care throughout treatment
Assisting in biopsy, surgery prep, chemo/radiotherapy support
Monitoring for recurrence or metastasis
📌 VII. Key Points for Quick Review
✅ Benign tumors grow slowly, do not invade, and rarely recur 🚫 Malignant tumors are fast-growing, invasive, and metastatic 🎯 Accurate diagnosis (biopsy, imaging) is essential 💉 Treatment depends on type, grade, and stage – includes surgery, chemotherapy, radiotherapy 📚 Nurses are pivotal in early detection, patient support, and palliative care
🧬 Carcinoma In Situ (CIS) – A Detailed, Academic, and Engaging Explanation
🔍 Definition:
Carcinoma in situ (CIS) is a pre-invasive stage of cancer in which abnormal epithelial cells are present, but have not yet invaded the basement membrane or spread to surrounding tissues. It is localized, non-invasive, and considered Stage 0 cancer. Though not yet malignant, it has the potential to progress to invasive cancer if not identified and treated.
🧫 Pathophysiology:
Carcinoma in situ arises due to a series of genetic mutations and epigenetic alterations in epithelial cells that:
Disrupt cell cycle regulation
Cause abnormal proliferation
Lead to loss of differentiation
Result in atypical cellular architecture
These abnormal cells are confined within their tissue of origin (such as the squamous epithelium of the cervix, skin, or ducts of the breast) and are bounded by an intact basement membrane. Once the basement membrane is breached, the condition evolves into invasive carcinoma.
🧠 Key Features of CIS:
🔸 Feature
🔬 Description
Location
Confined to epithelial layer
Basement membrane
Intact
Invasion
None
Cell morphology
Dysplastic, pleomorphic nuclei, hyperchromatic, high N:C ratio
Mitotic activity
Increased
Reversibility
Possible with early detection and treatment
📍 Common Sites of Carcinoma In Situ:
🌍 Site
🧬 Type
Cervix
Cervical intraepithelial neoplasia (CIN III)
Breast
Ductal carcinoma in situ (DCIS) or Lobular carcinoma in situ (LCIS)
Skin
Bowen’s disease
Bladder
Urothelial carcinoma in situ
Oral cavity
Leukoplakia with carcinoma in situ
Lung
Bronchioloalveolar carcinoma in situ
🔬 Histological Appearance:
Full-thickness epithelial dysplasia
High mitotic index
Disorganized architecture
No stromal invasion
Well-demarcated from surrounding normal cells
🧪 Special stains and immunohistochemistry may be used for diagnosis:
Ki-67 (for proliferation index)
p53 (mutations often associated)
Cytokeratins (to assess epithelial origin)
🔍 How CIS Differs from Other Lesions:
Type
Basement Membrane
Invasion
Reversible?
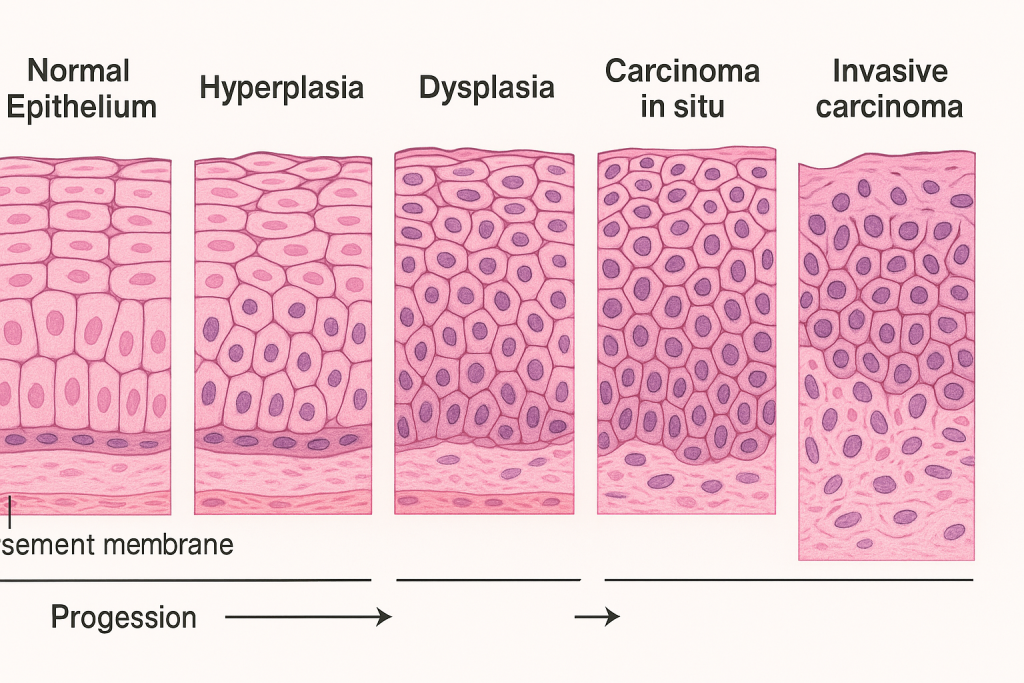
Hyperplasia
Intact
❌ No
✅ Yes
Dysplasia
Intact
❌ No
✅ Possibly
Carcinoma in situ
Intact
❌ No
⚠️ Risk of becoming invasive
Invasive carcinoma
❌ Breached
✅ Yes
❌ No
⚠️ Clinical Significance:
CIS is a critical early warning stage of cancer:
Highly treatable
Early treatment prevents progression
Screening programs, like Pap smear (cervical CIS) or mammography (DCIS), are essential
💊 Management:
Treatment depends on location and risk of progression:
Excisional biopsy or surgical excision
Laser ablation or cryotherapy (for skin/CIN)
Intravesical therapy (for bladder CIS)
Regular follow-up and screening
👩⚕️ Nurse’s Role:
Health education on importance of screening
Emotional support post-diagnosis
Preparing and assisting during biopsies or minor procedures
Educating about treatment options and follow-up
🧠 Mnemonic to Remember CIS Features – “CIS IS IN”:
C: Confined to epithelium
I: Intact basement membrane
S: Silent (often asymptomatic)
I: Increased mitotic activity
N: No invasion
Normal Epithelium ↓ Hyperplasia ↓ Dysplasia ↓ Carcinoma in situ (CIS) ↓ Invasive Carcinoma (if untreated)
🧠 Tumor Metastasis
🔍 Definition:
Tumor metastasis is the spread of cancer cells from the primary site to distant organs or tissues, forming secondary tumors. It is a hallmark of malignancy and signifies a poor prognosis in many cancers.
🧬 General Mechanism of Tumor Metastasis:
Metastasis is a complex, multi-step process involving cellular, molecular, and systemic interactions. It includes the following main stages:
📊 Step-by-Step Mechanism of Metastasis:
1. Detachment (Loss of Adhesion):
🔹 Tumor cells lose adhesion molecules (e.g., E-cadherin) 🔹 Cells detach from the primary tumor mass 🔹 Loss of polarity and cell-to-cell communication
2. Local Invasion:
🔹 Tumor cells invade the surrounding stroma 🔹 Secretion of proteolytic enzymes (e.g., matrix metalloproteinases – MMPs) 🔹 Degradation of extracellular matrix (ECM) and basement membrane
3. Intravasation:
🔹 Tumor cells enter nearby blood vessels or lymphatics 🔹 Facilitated by angiogenesis and endothelial barrier disruption 🔹 Interaction with immune cells and platelets for survival in circulation
4. Survival in Circulation:
🔹 Circulating Tumor Cells (CTCs) face immune attack, shear stress, and anoikis (detachment-induced apoptosis) 🔹 Protected by platelet cloaking and immune evasion strategies
5. Extravasation:
🔹 CTCs adhere to endothelial lining in distant capillaries 🔹 They exit blood vessels by breaching the vascular wall 🔹 Form micrometastases in new tissue
6. Colonization and Angiogenesis:
🔹 Tumor cells adapt to new microenvironment 🔹 Stimulate angiogenesis via VEGF to sustain growth 🔹 Form clinically detectable secondary tumor (macrometastasis)
🔄 Flowchart: Tumor Metastasis Mechanism
Primary Tumor ↓ Loss of adhesion (↓ E-cadherin) ↓ Invasion of ECM & stroma (↑ MMPs) ↓ Intravasation (entry into vessels) ↓ Survival in bloodstream (CTCs) ↓ Extravasation (exit at distant site) ↓ Colonization & angiogenesis ↓ Secondary Tumor Formation (Metastasis)
🔬 Molecular Changes Involved:
🔸 Molecule
🔬 Function
E-cadherin ↓
Loss of adhesion between cells
Integrins altered
Change in cell-matrix interaction
MMPs ↑
Degrade ECM for invasion
VEGF ↑
Promotes angiogenesis
CXCR4 & chemokines
Help tumor cells home to specific tissues
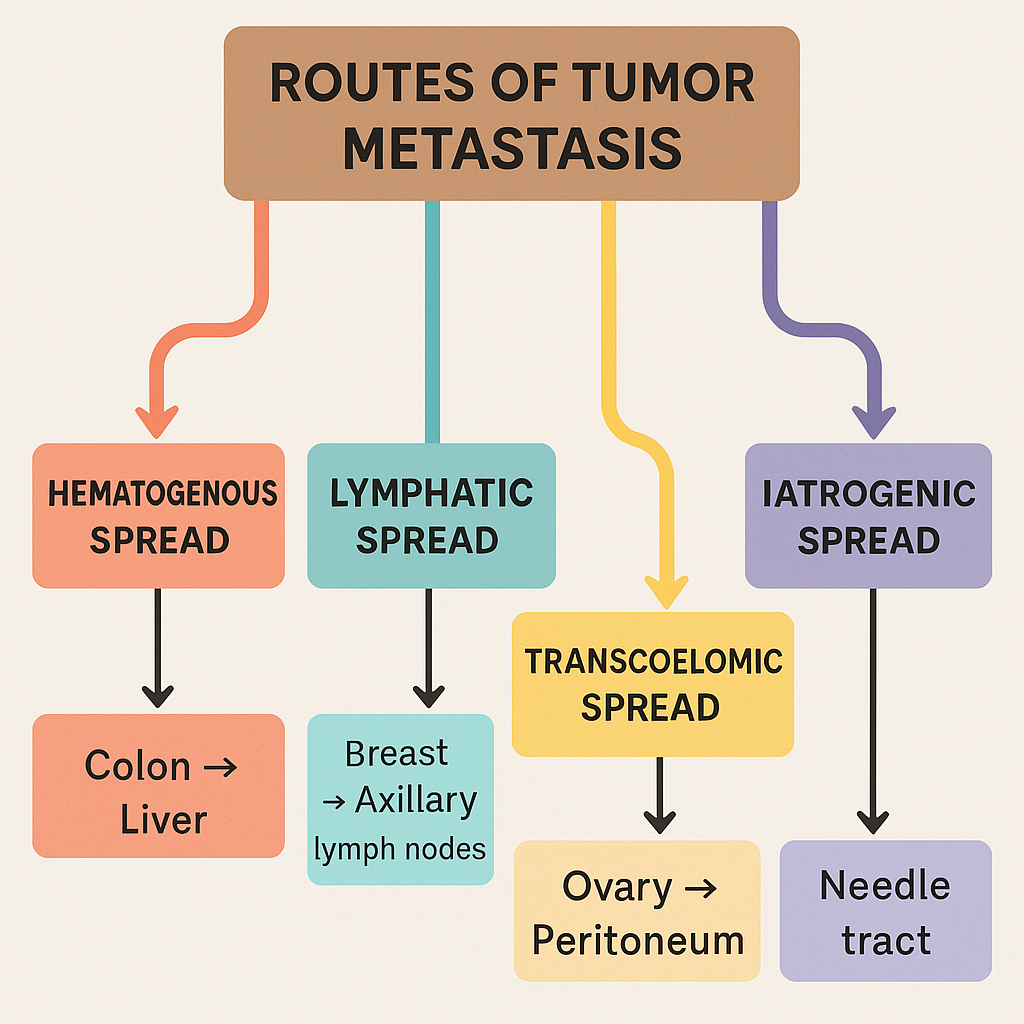
🧠 Routes of Metastasis:
🛣 Route
📍 Common Sites
Lymphatic
Breast, melanoma → lymph nodes
Hematogenous
Sarcomas, liver, lungs, brain, bone
Transcoelomic
Ovarian cancer → peritoneum
Iatrogenic
Surgical seeding
🧠 “Seed and Soil” Hypothesis (Stephen Paget):
Seed = Tumor cell
Soil = Target organ environment 🔹 Metastasis depends not only on the tumor cell but also on the compatibility of the distant site
👩⚕️ Nursing and Clinical Relevance:
Early identification of metastatic signs (e.g., bone pain, seizures, cough)
Importance of screening and regular monitoring
Patient education on treatment options (chemotherapy, targeted therapy, palliative care)
Emotional and psychological support
⚠️ Why Metastasis Is Dangerous:
✅ Often asymptomatic initially ✅ Can affect vital organs like lungs, liver, brain ✅ Makes treatment more complex and less curative ✅ Causes systemic symptoms like weight loss, fatigue, and pain
🌟 Summary Mnemonic – “I MET Cancer”
I: Invasion
M: Migration
E: Entry (intravasation)
T: Travel (circulation)
C: Colonization
A: Angiogenesis
N: New growth
C: Clinical tumor (secondary)
🌍 Tumor Metastasis – Routes of Spread and Examples
🧬 Introduction to Metastatic Spread:
Tumor metastasis is not a random process. Malignant tumors spread to distant sites through specific anatomical and physiological routes, guided by tumor type, vascular anatomy, and microenvironmental compatibility.
There are four major routes by which cancer cells metastasize:
Each route is associated with certain tumor types and specific patterns of organ involvement.
🔁 1. Hematogenous Spread (via Blood Vessels)
📌 Definition:
This route involves the dissemination of cancer cells through blood vessels, especially veins, to distant organs. It’s most common in sarcomas and some carcinomas.
🧪 Mechanism:
Tumor cells invade nearby blood vessels (especially venules or capillaries)
Enter systemic circulation
Lodge in distant capillary beds
Form secondary tumors
📍 Common Sites Affected:
Liver (via portal circulation)
Lungs (via systemic venous return)
Brain, bones, adrenal glands
🧠 Examples:
🔬 Primary Tumor
📍 Metastatic Site
🧭 Route
Colorectal carcinoma
Liver
Portal vein
Renal cell carcinoma
Lungs
Renal vein → IVC → Lungs
Osteosarcoma
Lungs
Venous blood spread
Hepatocellular carcinoma
Lungs and bones
Hepatic veins
🌿 2. Lymphatic Spread (via Lymphatic Channels)
📌 Definition:
This route is characteristic of carcinomas, where cancer cells spread through lymph vessels and lodge in regional lymph nodes.
🧪 Mechanism:
Tumor cells infiltrate lymphatics in the tumor bed
Transported to sentinel and regional lymph nodes
Can further disseminate to distant lymph nodes or systemic circulation
Cancer cells exfoliate from the primary tumor and spread across serous membranes, such as the peritoneum, pleura, or pericardium.
🧪 Mechanism:
Tumor cells break through the outer surface of an organ
Float in serous fluid
Implant on serosal surfaces of adjacent structures
📍 Common Sites Affected:
Peritoneal cavity (most frequent)
Pleural cavity
Pericardial cavity
🧠 Examples:
🔬 Primary Tumor
📍 Site of Spread
🧭 Route
Ovarian carcinoma
Peritoneum, omentum (“omental caking”)
Transcoelomic
Gastric carcinoma
Peritoneum (Krukenberg tumor in ovaries)
Transcoelomic
Lung carcinoma
Pleura
Transpleural spread
Pancreatic cancer
Peritoneum
Transcoelomic
🛠️ 4. Iatrogenic (Implantation) Spread
📌 Definition:
This artificial route involves mechanical transfer of tumor cells during surgery, biopsy, or other procedures.
🧪 Mechanism:
Tumor cells are displaced or seeded along the surgical tract
Can result in local recurrence or metastasis at the site of instrumentation
🧠 Examples:
🛠️ Procedure
🔬 Spread Site
⚠️ Note
FNAC (Fine needle aspiration) of a tumor
Needle tract
Rare but documented
Laparoscopic surgery
Port site metastasis
Ovarian or gastric cancers
Tumor resection
Scar site recurrence
Inadequate precautions
🧠 Summary Table of Routes of Spread:
Route of Spread
Common Tumor Types
Typical Sites
Example
Hematogenous
Sarcomas, RCC, colon
Liver, lungs
Colon → Liver
Lymphatic
Carcinomas
Lymph nodes
Breast → Axilla
Transcoelomic
Ovarian, stomach
Peritoneum, pleura
Ovary → Omentum
Iatrogenic
Any surgical tumor
Surgical tract
Needle tract
💡 Mnemonic for Routes of Spread – “HiLT Invasion”
H – Hematogenous
L – Lymphatic
T – Transcoelomic
I – Iatrogenic
👩⚕️ Nursing Importance in Metastasis Monitoring:
Monitor signs of lymph node enlargement
Look for organ-specific symptoms (e.g., breathlessness in lung metastasis)
Ensure sterile and tumor-safe techniques in procedures
Educate patients on importance of early diagnosis and treatment
🩸 Thrombosis – A Circulatory Disturbance in Focus
Thrombosis is a pathological process wherein a solid mass of blood constituents (called a thrombus) forms within the cardiovascular system during life. This clot is composed of platelets, fibrin, red blood cells, and white blood cells, and unlike hemostasis (which is a beneficial response to vascular injury), thrombosis is often harmful and blocks blood flow, potentially leading to ischemia (lack of oxygen to tissues), infarction (tissue death), or embolism (migration of clot fragments to distant sites).
🧠 The Underlying Mechanisms – Virchow’s Triad
The development of thrombosis is classically explained by Virchow’s Triad, proposed by the renowned pathologist Rudolf Virchow. It consists of three interrelated factors that predispose to thrombus formation:
Endothelial Injury: Damage to the endothelial lining of blood vessels is the most potent factor leading to thrombosis. Endothelium normally produces anticoagulant substances like prostacyclin, nitric oxide, and thrombomodulin. However, when it is disrupted by trauma, hypertension, atherosclerosis, or inflammation, these protective mechanisms are lost, allowing platelets to adhere and clotting cascades to initiate.
Abnormal Blood Flow: Normally, blood flows in a laminar pattern, with cells in the center and plasma at the periphery. When this flow is altered—either by stasis (as seen in immobility, congestive heart failure, or varicose veins) or turbulence (due to atherosclerotic plaques, aneurysms, or cardiac valve abnormalities)—it leads to endothelial damage and promotes clot formation. Stasis, in particular, allows platelets to come into close contact with the endothelium and prevents dilution of activated clotting factors.
Hypercoagulability: This refers to an increased tendency of the blood to clot, which may be genetic (such as Factor V Leiden mutation or deficiencies of Protein C, S, or antithrombin III) or acquired (due to conditions like pregnancy, cancer, oral contraceptive use, or dehydration). This condition shifts the balance toward pro-coagulant forces and reduces fibrinolytic activity.
🧪 Formation and Structure of a Thrombus
The process of thrombus formation begins when platelets adhere to exposed subendothelial collagen at the site of endothelial damage. They then activate and aggregate, forming a primary platelet plug. Simultaneously, the coagulation cascade is triggered, resulting in the generation of fibrin, which stabilizes the clot. In flowing blood, the thrombus develops characteristic “Lines of Zahn”, which are alternating layers of platelets/fibrin and red blood cells—indicating formation during life and not post-mortem.
🗺️ Types of Thrombi Based on Location
Thrombi are classified by their location and composition. Arterial thrombi, rich in platelets, usually develop on atherosclerotic plaques and may occlude coronary or cerebral arteries, leading to myocardial infarction or stroke. Venous thrombi, on the other hand, are rich in red blood cells and fibrin and are often found in deep veins of the legs (deep vein thrombosis). These can dislodge and travel to the lungs, resulting in pulmonary embolism. Mural thrombi can form on the walls of the heart after myocardial infarction or in aneurysmal dilations of blood vessels.
🔁 Fate of a Thrombus
Once a thrombus is formed, several outcomes are possible. It may propagate by accumulating additional platelets and fibrin, further obstructing blood flow. Alternatively, it might embolize, with parts breaking off and traveling to other parts of the body. In some cases, the body may dissolve the thrombus through fibrinolysis, especially if it is recent. Chronic thrombi may become organized, where fibroblasts and capillaries invade, potentially recanalizing the vessel to restore some degree of flow.
🚨 Clinical Consequences and Complications
Thrombosis can have grave consequences. A thrombus in a coronary artery can lead to myocardial infarction, while one in a cerebral artery can cause an ischemic stroke. Deep vein thrombosis (DVT), often silent, may progress to pulmonary embolism, which can be life-threatening. In disseminated intravascular coagulation (DIC), widespread microthrombi form in capillaries throughout the body, consuming clotting factors and paradoxically causing bleeding.
💊 Management and Prevention
Prevention strategies include early mobilization after surgery, use of compression stockings, and adequate hydration. Pharmacologic interventions involve anticoagulants like heparin and warfarin, antiplatelet agents like aspirin, or thrombolytic drugs like streptokinase or tPA in acute settings. The choice of therapy depends on the location, size, age, and risk of embolization of the thrombus.
🩺 Nursing Considerations
Nurses play a vital role in preventing and managing thrombosis. They must recognize early signs, such as calf pain and swelling (DVT), sudden breathlessness (PE), or neurological deficits (stroke). Nurses ensure compliance with medication, monitor for side effects (e.g., bleeding with anticoagulants), and educate patients about lifestyle modifications, such as avoiding smoking and staying physically active.
🌟 Conclusion:
Thrombosis represents a fundamental mechanism underlying many life-threatening conditions. Understanding its etiology, formation, types, outcomes, and prevention is crucial in clinical practice. While it shares a physiological origin with hemostasis, thrombosis is inherently pathological and requires prompt recognition and management to prevent morbidity and mortality.
🩸 Circulatory Disturbances – Embolism
🔍 Definition:
Embolism is the sudden blockage of a blood vessel by a detached intravascular mass (called an embolus) that is carried by the bloodstream from its point of origin to a distant site, where it causes vascular obstruction. It is one of the most serious forms of circulatory disturbance and often leads to ischemia, infarction, or death of tissues.
🧬 Nature of an Embolus:
An embolus is a solid, liquid, or gaseous mass that travels through blood vessels. It usually originates from a thrombus, but may also be composed of fat, air, tumor cells, amniotic fluid, or foreign bodies. Once lodged in a smaller vessel, the embolus blocks blood flow, depriving tissues downstream of oxygen and nutrients.
🧠 Types of Embolism (Based on Nature of Embolus):
1. Thromboembolism (most common)
Fragment of a blood clot (thrombus) that breaks off and travels
Can cause pulmonary embolism or systemic embolism
2. Fat Embolism
Fat globules, typically from fractured long bones or soft tissue trauma
Can lead to fat embolism syndrome (FES) with respiratory distress and neurological symptoms
3. Air Embolism
Air bubbles introduced via trauma, surgery, or intravenous access
100 mL of air in circulation can be fatal
Decompression sickness in divers is a classic example
4. Amniotic Fluid Embolism
Rare but catastrophic; amniotic fluid enters maternal circulation during labor
Leads to DIC, respiratory failure, and high mortality
5. Septic Embolism
Embolus consisting of infected material (e.g., vegetations from infective endocarditis)
6. Tumor Embolism
Malignant cells traveling through blood causing vascular occlusion
🌍 Classification Based on Circulatory Path:
🔹 Pulmonary Embolism (PE):
Origin: Usually deep vein thrombosis (DVT) of legs
Path: Right heart → pulmonary arteries → lung
Effect: May be asymptomatic, or cause dyspnea, chest pain, sudden death
🔹 Systemic Embolism:
Origin: Left heart chambers (e.g., due to atrial fibrillation, MI)
Path: Arteries of systemic circulation (brain, kidneys, spleen, etc.)
Effect: Stroke, renal infarcts, limb gangrene
🔹 Paradoxical Embolism:
Definition: A venous embolus enters systemic circulation via a heart defect (e.g., patent foramen ovale)
Unusual but dangerous as it bypasses the lung filter
🧪 Pathophysiology of Embolism:
Formation of embolic material (thrombus, fat, gas, etc.)
Detachment and entry into circulation
Travel through bloodstream following the pressure gradient
Lodgment in a vessel too small to pass through
Occlusion → impaired perfusion → ischemia or infarction
🚨 Clinical Consequences of Embolism:
Infarction: Sudden cessation of blood supply → cell death
Organ dysfunction: Lungs (PE), Brain (stroke), Kidneys (renal infarcts)
Hemodynamic collapse: Especially with large pulmonary emboli
Sudden death: If embolus blocks a major artery like pulmonary trunk
💊 Diagnosis and Management:
🔬 Diagnosis:
D-dimer test (for thromboembolism)
Doppler ultrasound (for DVT)
CT pulmonary angiography (for PE)
Echocardiogram (to detect cardiac source)
💊 Management:
Anticoagulants: Heparin, warfarin, DOACs
Thrombolytics: For large, life-threatening clots (e.g., tPA)
Surgical embolectomy: In severe PE or arterial embolism
Oxygen therapy and hemodynamic support in critical cases
👩⚕️ Nursing Responsibilities:
Early identification of symptoms like leg swelling, chest pain, or sudden breathlessness
Monitoring vital signs, oxygen saturation, and neurological status
Ensuring compliance with anticoagulant therapy
Educating patients about mobility, hydration, and avoiding prolonged immobility
Preparing patient for diagnostic tests and supportive care
🌟 Mnemonic – FAT BAT (Types of Emboli)
F: Fat
A: Air
T: Thrombus
B: Bacteria (septic)
A: Amniotic fluid
T: Tumor
🧭 Conclusion:
Embolism is a life-threatening circulatory event where materials from one part of the body travel and block vessels elsewhere. It can affect any organ, often striking suddenly and silently, and can be fatal if not diagnosed early. Understanding the types, mechanisms, and consequences of embolism is crucial for effective prevention, diagnosis, and timely intervention — especially in nursing and critical care settings.
⚠️ Circulatory Disturbance – SHOCK
🔍 Definition:
Shock is a clinical syndrome characterized by inadequate tissue perfusion and oxygen delivery to meet cellular metabolic demands. This results in cellular hypoxia, energy failure, and if not reversed, leads to multi-organ dysfunction and death. Despite varying causes, the final common pathway in all types of shock is circulatory collapse and tissue hypoperfusion.
🧬 Pathophysiology of Shock:
At its core, shock results from either:
Reduced cardiac output, or
Maldistribution of blood flow, or both.
This causes:
↓ oxygen and nutrient supply
Anaerobic metabolism
Lactic acid accumulation
Cellular damage
Inflammatory mediator release
Capillary leakage → edema
Progressive organ failure
🧠 Classification of Shock:
Shock is broadly categorized into four major types, each with distinct causes and clinical features:
Maintain IV access, administer fluids and medications
Monitor urine output (foley catheter) – important indicator of renal perfusion
Assess mental status and skin temperature
Provide oxygen therapy
Prepare for advanced life support if needed
Educate and emotionally support patients and families
🔁 Key Differences – Hypovolemic vs Cardiogenic vs Septic Shock:
Feature
Hypovolemic
Cardiogenic
Septic (early)
BP
↓
↓
↓
HR
↑
↑
↑
Skin
Cold, clammy
Cold, mottled
Warm, flushed (early)
Neck Veins
Flat
Elevated
Normal or low
Treatment
Fluids
Inotropes
Fluids + Antibiotics
🌟 Conclusion:
Shock is a medical emergency and a dynamic process where every second counts. While the types of shock vary by cause, the unifying theme is inadequate tissue perfusion leading to cellular and organ failure. Early identification, classification, and targeted resuscitation are vital for reversing the cascade and saving lives. In nursing and clinical practice, vigilant monitoring and timely intervention play a life-saving role.
💧 Disturbance of Body Fluids and Electrolytes – Edema
🔍 Definition:
Edema is the abnormal accumulation of fluid in the interstitial (extracellular) spaces of tissues, resulting in visible swelling. While a certain amount of fluid exchange between blood vessels and tissues is normal, edema signifies a disruption of fluid homeostasis due to imbalances in hydrostatic and oncotic pressures or lymphatic drainage.
🧪 Physiology Recap – Normal Fluid Exchange:
Under normal circumstances, fluid movement across capillary membranes is governed by Starling forces:
Hydrostatic pressure (pushes fluid out of vessels)
Oncotic (colloid osmotic) pressure (pulls fluid into vessels due to plasma proteins)
A balance between these forces maintains fluid equilibrium. Edema occurs when this balance is disturbed.
🧬 Pathophysiology of Edema:
Edema develops when any of the following mechanisms are altered:
↑ Capillary Hydrostatic Pressure
Common in heart failure, venous obstruction, or fluid overload
Pushes more fluid into interstitial space
↓ Plasma Oncotic Pressure
Due to low plasma protein levels (mainly albumin) in nephrotic syndrome, liver disease, malnutrition
Less fluid is reabsorbed into capillaries
↑ Capillary Permeability
Seen in inflammation, burns, sepsis, or allergic reactions
Allows proteins and fluid to leak into interstitial space
Lymphatic Obstruction
Occurs in filariasis, tumors, or surgical removal of lymph nodes
Prevents drainage of interstitial fluid
🧠 Types of Edema:
1. Localized Edema
Affects a specific region or organ
Often due to inflammation, trauma, allergy, or venous/lymphatic obstruction
Examples:
Cerebral edema (brain injury)
Pulmonary edema (left heart failure)
Periorbital edema (nephrotic syndrome)
Angioedema (allergic reaction)
2. Generalized Edema (Anasarca)
Widespread, systemic swelling
Seen in severe hypoalbuminemia, congestive heart failure, renal failure, or liver cirrhosis
📍 Clinical Features of Edema:
Swelling in dependent areas (e.g., ankles, sacrum)
Shiny, stretched skin
Pitting edema: indentation remains after pressure is applied (common in cardiac/renal causes)
Non-pitting edema: firm, no indentation (seen in lymphedema or myxedema)
Weight gain due to fluid retention
Shortness of breath if pulmonary edema is present
🧪 Diagnosis of Edema:
Physical examination (pitting vs. non-pitting)
Serum albumin, renal function tests, liver function tests
Chest X-ray (pulmonary edema)
Ultrasound or lymphoscintigraphy (for lymphatic obstruction)
Echocardiogram (for heart function)
💊 Management of Edema:
Management depends on underlying cause:
Diuretics (e.g., furosemide) for heart failure or fluid overload
Albumin infusion in hypoalbuminemia
Salt and fluid restriction
Elevating limbs, compression stockings for dependent edema
Treating infections or allergies (e.g., antihistamines, corticosteroids)
Surgical intervention in case of tumors causing lymphatic obstruction
👩⚕️ Nursing Considerations:
Monitor daily weight and intake/output
Assess edema grading and skin integrity
Educate patient on salt/fluid restriction
Encourage mobility and limb elevation
Watch for signs of worsening (e.g., SOB, decreased urine output)
🌟 Mnemonic – EDEMA:
E – Excess fluid in interstitial space
D – Dependent areas swelling
E – Elevate limbs and restrict salt
M – Monitor vitals, weight, I&O
A – Assess cause and treat accordingly
🎯 Conclusion:
Edema is a common manifestation of underlying systemic or local disease. It reflects a disturbance in fluid and electrolyte balance, and understanding its pathophysiological basis is crucial for correct diagnosis and management. Whether it’s a minor swelling from standing too long or a life-threatening pulmonary edema, timely assessment and intervention are key to improving outcomes.
💧 Disturbances of Body Fluids and Electrolytes – Transudates and Exudates
🔍 Introduction:
Fluid accumulation in body cavities such as the pleural space (pleural effusion), peritoneal cavity (ascites), or pericardial sac (pericardial effusion) is a common clinical finding in many disease conditions. To determine the cause and appropriate treatment, it is essential to distinguish between transudate and exudate—two types of pathological fluid accumulations that differ in mechanism, content, and implications.
🧬 What are Transudates and Exudates?
🔹 Transudate:
A transudate is a plasma-derived ultrafiltrate that accumulates due to systemic factors affecting the balance of Starling forces, such as increased hydrostatic pressure or decreased plasma oncotic pressure. There is no inflammation, and vascular permeability remains normal.
🔸 Exudate:
An exudate is a protein-rich fluid that escapes from blood vessels due to inflammation-induced increased vascular permeability. It often contains leukocytes, inflammatory mediators, fibrin, and sometimes microorganisms or malignant cells.
🔬 Detailed Mechanisms of Formation:
🔹 Transudate Formation – Non-inflammatory Causes:
Increased Hydrostatic Pressure:
Seen in congestive heart failure, especially right-sided heart failure, where blood backs up into systemic veins, pushing fluid into interstitial or serous cavities.
Decreased Plasma Oncotic Pressure:
Occurs when plasma proteins (mainly albumin) are reduced, leading to less reabsorption of interstitial fluid.
Causes: Cirrhosis, nephrotic syndrome, protein-losing enteropathy, severe malnutrition.
Impaired Lymphatic Drainage:
Rare in transudates but may contribute when combined with other factors.
Sodium and Water Retention:
Seen in renal failure, leading to plasma volume expansion and transudation.
🔸 Exudate Formation – Inflammatory or Neoplastic Causes:
Increased Vascular Permeability:
Inflammatory mediators (histamine, bradykinin, cytokines) open endothelial gaps, allowing proteins and immune cells to escape.
Endothelial Cell Injury or Damage:
Due to infection, trauma, burns, or autoimmune diseases.
Lymphatic Obstruction Due to Inflammation or Cancer:
Prevents fluid clearance and causes protein-rich fluid to accumulate.
Neovascularization in Tumors:
Tumors develop abnormal vessels prone to leakage.
🔎 Laboratory & Biochemical Differentiation:
Clinical labs use Light’s Criteria to distinguish between transudates and exudates in pleural or peritoneal fluid.
✅ An effusion is an exudate if ANY of the following are true:
Pleural fluid protein / serum protein ratio > 0.5
Pleural fluid LDH / serum LDH ratio > 0.6
Pleural fluid LDH > 2/3 of upper limit of normal serum LDH
If none of these criteria are met, it is classified as a transudate.
📍 Comparative Features of Transudates vs Exudates:
Feature
Transudate
Exudate
Cause
Systemic (e.g., CHF, cirrhosis)
Local (e.g., infection, cancer)
Appearance
Clear, pale yellow
Cloudy, turbid, bloody
Protein Content
< 3 g/dL
> 3 g/dL
Specific Gravity
< 1.012
> 1.020
LDH
Low
High
Cell Count
Low (mostly mesothelial)
High (neutrophils, lymphocytes)
Glucose
Normal
Often decreased
Clotting
Does not clot
May clot (due to fibrin)
🌍 Common Clinical Examples:
🔹 Transudative Effusions:
Congestive Heart Failure: Bilateral pleural effusion due to increased venous pressure.
Cirrhosis: Ascites from low albumin and portal hypertension.
Nephrotic Syndrome: Generalized edema and possible ascites from protein loss.
🔸 Exudative Effusions:
Pneumonia (Parapneumonic Effusion): Inflammatory exudate in pleural space.
Exudate → Local pathology → Investigate locally (e.g., infection, malignancy)
🎯 Conclusion:
Transudates and exudates represent two fundamentally different fluid types with distinct etiologies. Recognizing their biochemical differences and pathophysiological basis allows healthcare professionals to make accurate diagnoses, select the right investigations, and initiate appropriate therapies. In clinical nursing practice, it is essential to monitor such fluid accumulations diligently and act promptly based on symptom evolution and diagnostic findings.