BSC SEM 3 UNIT 10 ADULT HEALTH NURSING 1
UNIT 10 Nursing management of patients with musculoskeletal problems
🦴🧠 Review of Anatomy & Physiology of the Musculoskeletal System 💪🏽🦵🏼
🔷 I. INTRODUCTION
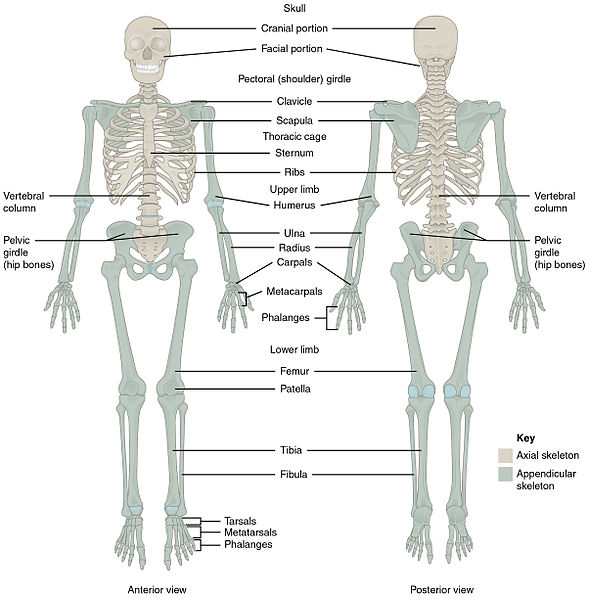
The musculoskeletal system is the body’s framework that provides support, movement, protection, and mineral storage. It is made up of:
🔹 Bones
🔹 Joints
🔹 Muscles
🔹 Tendons
🔹 Ligaments
🔹 Cartilage
🧩 This system is a functional integration of two systems:
➡️ Skeletal System (🦴) – Rigid framework
➡️ Muscular System (💪) – Generates movement
🦴 II. SKELETAL SYSTEM: STRUCTURE & FUNCTION
🦷 A. Types of Bones (based on shape)
| Shape | Description | Examples |
|---|---|---|
| 🟥 Long Bones | Longer than wide, support weight & movement | Femur, Tibia |
| 🟨 Short Bones | Cube-shaped, stability & movement | Carpals, Tarsals |
| ⬜ Flat Bones | Protect internal organs | Skull, Ribs |
| 🟪 Irregular Bones | Complex shapes | Vertebrae, Mandible |
| ⚪ Sesamoid Bones | Embedded in tendons | Patella |
🧱 B. Functions of Bones
✅ Support – Frame for the body
✅ Protection – Skull 🧠, Ribs ❤️, Vertebrae 🧬
✅ Movement – Acts as levers for muscles
✅ Mineral Storage – 🧂 Calcium & 🧪 Phosphate
✅ Blood Cell Formation – In red bone marrow (🔴⚪ platelets)
✅ Fat Storage – Yellow marrow stores lipids (⚠️ Energy reserve)
🧠 III. STRUCTURE OF A TYPICAL LONG BONE
🔹 Diaphysis – Shaft, compact bone
🔹 Epiphysis – Ends, spongy bone with red marrow
🔹 Metaphysis – Between shaft & end (includes growth plate)
🔹 Medullary cavity – Hollow center, contains yellow marrow
🔹 Periosteum – Outer fibrous membrane
🔹 Endosteum – Inner lining of medullary cavity
⚙️ IV. JOINTS (ARTICULATIONS)
Joints = Connections between bones 🧩
They allow mobility and provide stability.
🧍♂️ Types of Joints (Based on structure)
| Type | Examples | Movement |
|---|---|---|
| 🔵 Fibrous | Skull sutures | Immovable |
| 🟠 Cartilaginous | Vertebrae, Pubic symphysis | Slight movement |
| 🟢 Synovial | Knee, Shoulder | Freely movable |
💡 Synovial Joints have:
➡️ Articular cartilage
➡️ Synovial cavity with fluid
➡️ Joint capsule
➡️ Ligaments
💪 V. MUSCULAR SYSTEM: STRUCTURE & FUNCTION
🎯 A. Types of Muscles
| Muscle Type | Characteristics | Location | Control |
|---|---|---|---|
| 💪 Skeletal | Striated, multinucleated | Attached to bones | Voluntary |
| 💓 Cardiac | Striated, branched, intercalated discs | Heart only | Involuntary |
| 🫁 Smooth | Non-striated, spindle-shaped | Walls of hollow organs | Involuntary |
🧬 B. Functions of Muscles
✅ Movement – via tendon attachments
✅ Posture Maintenance
✅ Joint Stability
✅ Heat Production – 85% of body heat 🥵
✅ Circulation (Cardiac) & Peristalsis (Smooth)
🔌 VI. MECHANISM OF MUSCLE CONTRACTION
💥 Sliding Filament Theory (in skeletal muscles):
🟢 Actin (thin) + 🔴 Myosin (thick) filaments slide over each other → contraction
Steps:
- Nerve impulse → Acetylcholine (ACh) release
- Calcium ions (Ca²⁺) released from sarcoplasmic reticulum
- Ca²⁺ binds to troponin → shifts tropomyosin
- Myosin heads attach to actin → form cross-bridges
- ATP allows power stroke → muscle shortens
- Relaxation occurs when Ca²⁺ is reabsorbed
🔗 VII. CONNECTIVE TISSUE COMPONENTS
| Structure | Function |
|---|---|
| 🔩 Tendons | Connect muscle to bone |
| 🔗 Ligaments | Connect bone to bone |
| 🧊 Cartilage | Smooth, cushioning surface in joints |
🧠 VIII. PHYSIOLOGY OF MOVEMENT
- Initiated by the nervous system (CNS → PNS)
- Motor neurons release signals to muscle fibers
- Agonist muscles contract, antagonists relax
- Synergists help, stabilizers maintain balance
🎯 Example:
👉 To flex the elbow:
- Agonist = Biceps brachii
- Antagonist = Triceps brachii
- Stabilizer = Deltoid
🧪 IX. AGE-RELATED CHANGES
🔸 Loss of bone density (osteopenia/osteoporosis)
🔸 Muscle mass decreases (sarcopenia)
🔸 Joint stiffness, ↓ flexibility
🔸 ↑ Risk of fractures & falls
🧾 X. KEY TERMS TO REMEMBER
- Osteocyte 🧬 – Mature bone cell
- Osteoblast 🏗️ – Bone-forming cell
- Osteoclast 🪓 – Bone-resorbing cell
- Sarcoplasm – Muscle cell cytoplasm
- Sarcomere – Functional unit of muscle fiber
- Synovial fluid 💧 – Lubricates joints
- Isotonic contraction – Muscle changes length
- Isometric contraction – Muscle tension without length change
📌 CONCLUSION
The musculoskeletal system is essential for posture, protection, locomotion, and daily functioning. A healthy diet, physical activity, and proper ergonomics help maintain its strength and integrity across the lifespan.
🩺🦴 Nursing Assessment of Patients with Musculoskeletal Problems 💪🏽🧑⚕️
🔷 I. PURPOSE OF NURSING ASSESSMENT
✅ Identify musculoskeletal dysfunctions
✅ Determine severity and impact on daily life
✅ Establish baseline data
✅ Guide nursing care planning and evaluation
✅ Monitor for complications (e.g., immobility, fractures, infections)
🔍 II. ASSESSMENT APPROACH
🔹 A. Health History Interview 🗣️📋
Ask the patient about:
| Aspect | Key Questions |
|---|---|
| 🧬 Chief complaint | “What brings you in today?” |
| 🤕 Pain | Location, intensity, quality (aching, burning, sharp), duration, what aggravates or relieves it |
| ⚠️ Injury/Trauma | Any falls, fractures, sports/work injuries |
| 🏃 Mobility Issues | Difficulty walking, stiffness, limping, gait changes |
| 🧱 Deformities | Any visible bone or joint deformities |
| 😫 Weakness or Fatigue | In limbs, muscles, reduced endurance |
| 📜 Medical history | Arthritis, osteoporosis, muscular dystrophy, past surgeries |
| 🧬 Family history | Hereditary conditions (RA, SLE, osteoporosis) |
| 💊 Medications | Steroids, calcium/vitamin D supplements, NSAIDs |
| 🧠 Psychosocial Impact | Effects on work, ADLs, mood, social life |
🔹 B. Physical Examination (Head-to-Toe) 👩⚕️🔍
🛏️ Ensure patient comfort and proper lighting before proceeding.
1. 🧍♀️ Inspection
Look for:
- Swelling/edema 💦
- Redness or bruising ❤️💜
- Muscle wasting or hypertrophy 💪
- Joint deformities (e.g., genu valgum, kyphosis)
- Abnormal posture or gait 🚶♂️🚶♀️
2. 🖐️ Palpation
Use fingertips and hands to assess:
- Tenderness or pain
- Crepitus (grating sound in joints)
- Warmth or temperature changes
- Muscle tone – flaccid, spastic, rigid
- Joint effusion – presence of fluid
3. 📏 Range of Motion (ROM)
Assess active and passive ROM:
- Flexion ↘️
- Extension ↗️
- Abduction ➡️
- Adduction ⬅️
- Rotation 🔄
📝 Note any limitations, pain, or asymmetry
4. 💪 Muscle Strength Grading (0 to 5 scale)
| Grade | Description |
|---|---|
| 0️⃣ | No contraction |
| 1️⃣ | Flicker, no movement |
| 2️⃣ | Movement only with gravity eliminated |
| 3️⃣ | Movement against gravity |
| 4️⃣ | Movement against some resistance |
| 5️⃣ | Full strength, normal |
5. ⚖️ Posture & Gait
- Observe standing/sitting posture
- Analyze gait pattern: smooth, symmetrical?
- Check for assistive devices use (canes, walkers)
🧪 III. DIAGNOSTIC TESTS REVIEWED BY NURSE
Be aware of results that support musculoskeletal assessment:
| Test | What It Shows |
|---|---|
| 🩸 Serum Calcium & Phosphate | Bone metabolism |
| 🧪 Alkaline Phosphatase (ALP) | Bone formation activity |
| 🩸 Rheumatoid Factor (RF), ANA, CRP, ESR | Autoimmune & inflammatory markers |
| 🩻 X-rays | Bone fractures, arthritis, deformities |
| 📊 DEXA scan | Bone mineral density (osteoporosis screening) |
| 🧲 MRI/CT scan | Soft tissues, ligaments, tendons |
| 🔬 Joint aspiration | Rule out infection or gout |
🚩 IV. RED FLAGS TO REPORT IMMEDIATELY
⚠️ Sudden loss of movement
⚠️ Severe unrelieved pain
⚠️ Cold or pale limb (↓ circulation)
⚠️ Numbness or tingling (nerve damage)
⚠️ Signs of infection in joint (fever, warmth, redness, swelling)
🧾 V. NURSING DOCUMENTATION TIPS
📝 Record:
- Type, location, and severity of symptoms
- Functional limitations (e.g., can’t climb stairs)
- Assistive device use
- Pain scale rating before and after interventions
- Patient’s emotional status and coping
💡 VI. CLINICAL TIPS FOR ASSESSMENT
✅ Compare both sides (bilateral limbs)
✅ Use anatomical terms (e.g., proximal, distal)
✅ Involve the patient actively (e.g., “Can you lift your leg?”)
✅ Assess impact on ADLs (bathing, dressing, walking)
✅ Be alert for compensatory movements or guarding
📌 SUMMARY
Nursing assessment of the musculoskeletal system involves: 👉 Comprehensive history
👉 Thorough physical exam
👉 Functional evaluation
👉 Monitoring diagnostic results
👉 Prompt recognition of complications
🧠 Remember: Early detection = Better outcome
🩺🦴 History and Physical Assessment of Patients with Musculoskeletal Problems 💪🧑⚕️

🔷 I. HISTORY TAKING (Subjective Data Collection)
A thorough musculoskeletal history helps identify the nature, onset, and impact of the problem. Use open-ended questions, pain scales, and ADL-based queries.
🔹 A. Presenting Complaint
🗣️ Ask:
“What brought you here today?”
“What are you experiencing?”
➡️ Common complaints include:
✅ Joint or muscle pain
✅ Swelling, stiffness
✅ Weakness
✅ Deformity
✅ Limited range of motion
✅ Numbness or tingling
🔹 B. Pain Assessment – PQRST Format 📌
| Factor | Question |
|---|---|
| P – Provocation | What triggers it? (Movement, rest?) |
| Q – Quality | Dull, sharp, aching, burning? |
| R – Region/Radiation | Where is it? Does it spread? |
| S – Severity | Pain scale 0–10 |
| T – Timing | Constant, intermittent, duration? |
🔹 C. Functional Assessment 🧍
Ask about the patient’s ability to perform activities of daily living (ADLs):
🧼 Bathing
👗 Dressing
🚶 Walking
🍽️ Eating
🪑 Sitting or getting up
🛏️ Sleeping position & comfort
🔹 D. Past Medical and Surgical History 🗂️
✅ Previous fractures, dislocations, arthritis, osteoporosis
✅ Orthopedic surgeries (joint replacement, spine surgery)
✅ Use of orthopedic devices (braces, walkers, canes)
✅ Medications: NSAIDs, corticosteroids, calcium/vitamin D
✅ History of falls or trauma
🔹 E. Family History 👨👩👧👦
🧬 Hereditary musculoskeletal disorders:
- Rheumatoid arthritis
- Osteoporosis
- Muscular dystrophy
- Ankylosing spondylitis
🔹 F. Lifestyle and Occupation 🧳🏋️
✅ Job type (physical labor vs. sedentary)
✅ Exercise routine or lack thereof
✅ Sports involvement or overuse injuries
✅ Nutrition, calcium/vitamin D intake
✅ Smoking/alcohol (affect bone health)
🔹 G. Psychosocial Impact 🧠
- Emotional effects of chronic pain
- Dependency or reduced mobility
- Social isolation due to disability
- Coping mechanisms
🔶 II. PHYSICAL ASSESSMENT (Objective Data Collection)
✅ Perform assessment in a systematic head-to-toe approach
🔹 A. Inspection 👀
Observe:
- Posture – Normal alignment or deformity (e.g., kyphosis, scoliosis)
- Gait – Limping, dragging, balance issues
- Swelling, redness, bruising
- Deformities or asymmetry
- Muscle wasting or hypertrophy
- Use of assistive devices
🔹 B. Palpation ✋
Feel for:
- Tenderness or warmth
- Swelling/fluid accumulation (effusion)
- Crepitus – Grinding sensation in joints
- Muscle tone – Rigid, spastic, flaccid
- Joint stability
🔹 C. Range of Motion (ROM) 📏
- Assess Active ROM – Patient moves joint on their own
- Assess Passive ROM – You move the joint for the patient
- Compare bilaterally
- Look for pain, stiffness, or limitation
💡 Movements to assess:
🦵 Flexion ↘️ | Extension ↗️
➡️ Abduction | ⬅️ Adduction
🔄 Rotation | Circumduction
🔹 D. Muscle Strength Testing 💪
🧠 Use Muscle Strength Grading Scale (0–5)
| Grade | Description |
|---|---|
| 0️⃣ | No muscle contraction |
| 1️⃣ | Flicker only |
| 2️⃣ | Movement without gravity |
| 3️⃣ | Movement against gravity |
| 4️⃣ | Movement against some resistance |
| 5️⃣ | Full strength |
🔹 E. Gait and Balance Analysis 🚶
Observe the patient walking:
- Steady? Limping? Ataxic?
- Heel-to-toe walking
- Tandem gait
- Balance while turning or standing
🔹 F. Joint Assessment 🦴
- Inspect major joints: shoulder, elbow, wrist, fingers, hip, knee, ankle
- Check alignment, swelling, ROM, deformity
- Palpate for joint line tenderness
🔹 G. Spine Evaluation 🌀
Assess posture and curvature:
- Cervical spine – Flexion, extension, rotation
- Thoracic spine – Kyphosis or scoliosis
- Lumbar spine – Lordosis, mobility
- Perform straight leg raising test (for sciatica)
🧪 III. ADDITIONAL DIAGNOSTIC EVALUATION (Reviewed by Nurse)
🔬 Test results often used to confirm findings:
- 🧪 ESR / CRP – Inflammation
- 🧪 Rheumatoid factor (RF), ANA – Autoimmune markers
- 🧲 X-ray / MRI / CT – Bone, cartilage, soft tissues
- 📊 DEXA scan – Bone density
- 🧫 Joint aspiration – Infection or crystals (gout)
🚨 IV. ALERT SIGNS TO LOOK FOR
⚠️ Sudden muscle weakness
⚠️ Severe, unrelieved pain
⚠️ Numbness, tingling, or cold extremities
⚠️ Swelling with warmth and redness
⚠️ Loss of mobility or joint locking
🧾 V. DOCUMENTATION IN NURSE’S NOTES
Include: ✅ Pain scale and description
✅ Joint and muscle condition
✅ ROM findings
✅ Functional ability and gait
✅ Diagnostic results and trends
✅ Patient’s verbal reports and emotional status
📌 SUMMARY
Nursing history and physical assessment of the musculoskeletal system provide crucial data for:
🩺 Diagnosis
📅 Planning
🧠 Monitoring
🤝 Patient-centered care
🎯 A thorough and empathetic approach leads to early detection, effective treatment, and better quality of life for patients with musculoskeletal problems.
🧪🦴 Diagnostic Tests for Musculoskeletal Problems 💉🧲
🔷 I. BLOOD TESTS 🩸
Laboratory investigations help detect inflammation, autoimmune disorders, bone metabolism, or infection.
| 🔬 Test | 💡 Purpose | ⬆️⬇️ Interpretation |
|---|---|---|
| Erythrocyte Sedimentation Rate (ESR) | Detects inflammation | ↑ in arthritis, infections |
| C-Reactive Protein (CRP) | More sensitive than ESR for inflammation | ↑ in RA, osteomyelitis |
| Rheumatoid Factor (RF) | Autoantibody for rheumatoid arthritis | ↑ in RA, SLE |
| Anti-Nuclear Antibody (ANA) | Detects autoimmune disease | ↑ in SLE, RA |
| Serum Calcium | Bone strength marker | ↑ in bone destruction; ↓ in osteoporosis |
| Serum Phosphorus | Works with calcium in bone | ↑ or ↓ in bone disease |
| Alkaline Phosphatase (ALP) | Indicates bone formation activity | ↑ in Paget’s disease, fractures |
| Creatine Kinase (CK-MM) | Muscle damage indicator | ↑ in muscle injury, myopathies |
| Uric Acid | Evaluates gout | ↑ in gout or renal failure |
| HLA-B27 | Genetic marker | Positive in ankylosing spondylitis |
🧲 II. IMAGING STUDIES
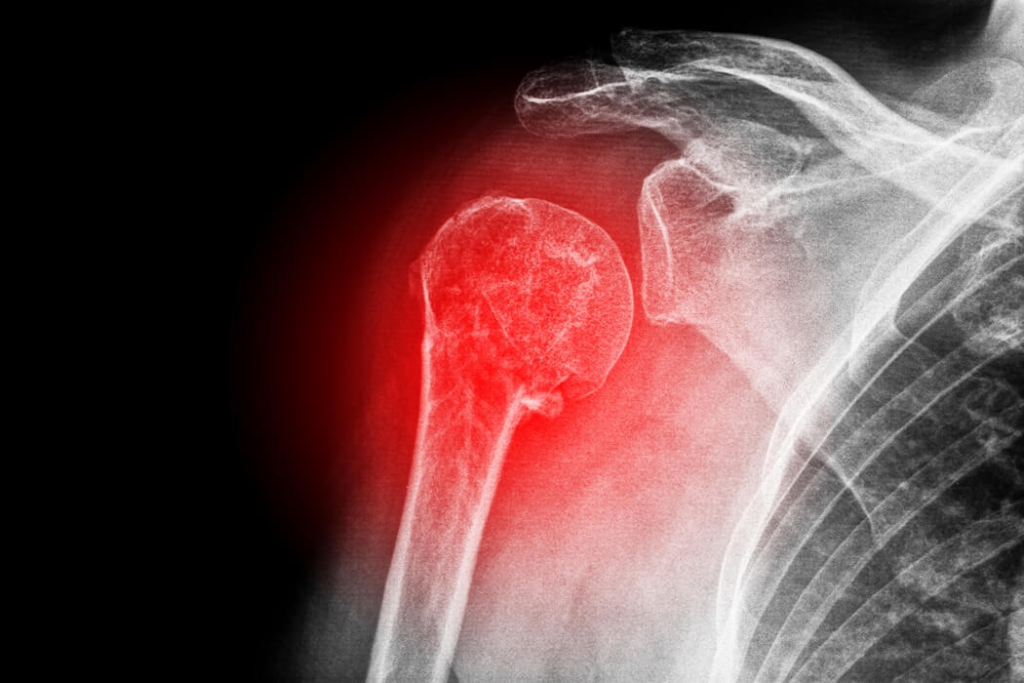
1. X-ray (Radiography) 🩻
✅ First-line test
✅ Detects:
- Fractures 🦴
- Dislocations
- Osteoarthritis (joint space narrowing)
- Bone tumors
- Bone alignment
2. CT Scan (Computed Tomography) 🧠
✅ Cross-sectional view of bones & soft tissues
✅ Better than X-ray for:
- Complex fractures
- Bone tumors
- Spinal pathology
💡 Can be done with contrast for detailed view
3. MRI (Magnetic Resonance Imaging) 🧲
✅ Best for soft tissues
✅ Shows:
- Ligament or tendon tears
- Herniated discs
- Spinal cord compression
- Bone marrow conditions
💡 Avoid in patients with metal implants or pacemakers
4. Bone Scan (Radionuclide Scintigraphy) ☢️
✅ Injects radioactive isotope
✅ Detects:
- Bone metastases
- Stress fractures
- Osteomyelitis
- Avascular necrosis
💡 Requires hydration post-test to flush dye
5. Dual-Energy X-ray Absorptiometry (DEXA) 📊
✅ Measures Bone Mineral Density (BMD)
✅ Gold standard for osteoporosis diagnosis
✅ T-score interpretation:
- ≥ -1 = Normal
- -1 to -2.5 = Osteopenia
- ≤ -2.5 = Osteoporosis
6. Ultrasound (MSK Sonography) 🎯
✅ Non-invasive & radiation-free
✅ Best for:
- Joint effusions
- Tendon inflammation (e.g., rotator cuff)
- Soft tissue masses
🧫 III. SPECIAL PROCEDURES
1. Arthrocentesis (Joint Aspiration) 💉
✅ Aspiration of synovial fluid
✅ Used for:
- Gout (urate crystals)
- Septic arthritis (infection)
- Hemarthrosis (blood in joint)
💡 Analyze fluid for color, clarity, cell count, crystals, and bacteria
2. Electromyography (EMG) & Nerve Conduction Studies (NCS) ⚡
✅ Assesses muscle & nerve function
✅ Used in:
- Neuromuscular disorders
- Carpal tunnel syndrome
- Peripheral neuropathy
💡 May involve mild discomfort
3. Muscle or Bone Biopsy 🔬
✅ Removal of tissue sample
✅ Used to diagnose:
- Bone tumors (benign or malignant)
- Muscle dystrophies or infections
💡 Done via needle or surgically
4. Arthroscopy 📹
✅ Minimally invasive scope into joint
✅ Direct visualization of joint surfaces
✅ Can diagnose and treat:
- Torn cartilage
- Ligament injury
- Synovial disorders
💡 Often used for knee and shoulder joints
🚨 IV. NURSING RESPONSIBILITIES
🧑⚕️ Before the Test:
- Explain procedure and purpose
- Check allergies (esp. to contrast)
- Obtain informed consent (for invasive tests)
- NPO status if ordered
- Remove metal objects (for MRI)
🧑⚕️ After the Test:
- Monitor vital signs
- Encourage fluid intake (after contrast)
- Watch for allergic reactions
- Observe puncture or aspiration sites for infection or bleeding
🧾 SUMMARY CHART
| Category | Tests | Use |
|---|---|---|
| Blood Tests | ESR, CRP, RF, CK, Calcium, ALP | Inflammation, autoimmune disease, bone metabolism |
| Imaging | X-ray, CT, MRI, Bone Scan, DEXA | Structure, density, soft tissue, tumors |
| Procedures | Arthrocentesis, Biopsy, EMG, Arthroscopy | Diagnosis of joint, muscle, nerve disorders |
📌 These tests are essential tools in identifying, monitoring, and planning treatment for musculoskeletal problems. Nurses play a key role in preparation, education, and post-test care to ensure patient safety and accurate results.
🦴🔄 Dislocation (Joint Displacement)
🔷 DEFINITION
🧠 A dislocation is the complete displacement or separation of the articular surfaces of a joint, causing loss of joint alignment and function.
In simpler terms:
Dislocation = Bone out of joint place 💥
🆘 It is often accompanied by ligament tearing, pain, swelling, and restricted movement.
🔶 CAUSES OF DISLOCATION
Dislocations usually result from trauma, but other factors may contribute as well:
✅ 1. Traumatic Injury
- 🚗 Road traffic accidents
- 🏀 Sports injuries
- 🤕 Falls (especially on an outstretched hand)
✅ 2. Congenital Disorders
- Congenital dislocation of the hip (CDH) in infants 👶
✅ 3. Pathological Conditions
- 🦴 Rheumatoid arthritis, osteomyelitis, or tumors weakening joint structure
✅ 4. Neuromuscular Disorders
- Muscle weakness/spasticity may allow joints to dislocate (e.g., stroke, cerebral palsy)
✅ 5. Repetitive Stress
- Overuse or repeated strain (e.g., shoulder in athletes)
🔷 TYPES OF DISLOCATION
Dislocations can be classified based on several factors:
🔹 A. Based on Duration
| Type | Description |
|---|---|
| Acute Dislocation ⚠️ | Sudden and recent; usually due to trauma |
| Chronic Dislocation 🕰️ | Long-standing; may go unnoticed or untreated |
| Recurrent Dislocation 🔁 | Occurs repeatedly at the same joint (e.g., shoulder) |
🔹 B. Based on Completeness
| Type | Description |
|---|---|
| Complete Dislocation ❌ | Total loss of contact between joint surfaces |
| Subluxation (Partial) ✅ | Partial or incomplete dislocation – joint surfaces still partially in contact |
🔹 C. Based on Location (Joint Affected)
| Joint | Common Name | Notes |
|---|---|---|
| Shoulder | Glenohumeral dislocation | Most common dislocation 💪 |
| Hip | Hip dislocation | Often due to high-impact trauma or in newborns |
| Knee | Patellar or tibiofemoral | Less common but serious |
| Elbow | Elbow dislocation | Seen in falls or sports |
| Fingers/Toes | Phalangeal dislocation | Due to twisting injuries |
| Jaw (TMJ) | Temporomandibular dislocation | Can occur during yawning, trauma, or dental work |
🩺 KEY POINTS TO REMEMBER
🟥 Dislocations = Ortho Emergencies
🟨 Untreated = Risk of nerve damage, vascular injury, or joint deformity
🟩 Reduction (manual or surgical) is necessary to reposition the joint
🧊 Apply cold compress, immobilize, and monitor neurovascular status before treatment
🔬 I. PATHOPHYSIOLOGY OF DISLOCATION
Dislocation involves displacement of bones at a joint, leading to loss of articulation and structural disruption. Here’s how it happens:
🧠 Step-by-step Pathophysiology:
- Traumatic force or pathological condition → sudden or gradual stress on the joint
- Joint capsule stretches or tears
- Ligaments rupture or become lax
- Articular surfaces of bones separate completely (dislocation)
- Surrounding tissues (muscles, tendons, nerves, blood vessels) may be stretched or damaged
- Results in:
- Pain, swelling
- Loss of function
- Joint deformity
- Risk of neurovascular compromise
📌 In subluxation, partial contact between articular surfaces is still retained.
🚨 II. SIGNS AND SYMPTOMS
Dislocation presents with obvious and immediate symptoms, especially after trauma.
| Symptom | Description |
|---|---|
| 🔺 Severe Pain | Sudden, sharp, localized to joint |
| 🔻 Swelling | Due to inflammation and fluid accumulation |
| 🚫 Immobility | Inability to move the joint normally |
| 🦴 Deformity | Abnormal joint shape or contour; joint may appear “out of place” |
| ✋ Tenderness | On palpation over the joint |
| 🩸 Bruising or Redness | Overlying skin may change color due to internal bleeding |
| ⚡ Numbness or Tingling | If nerves are compressed or stretched |
| ❄️ Cold or Pale Extremity | Sign of vascular compromise (serious complication) |
| 🧊 Muscle Spasm | Due to protective reflex and irritation |
🧪 III. DIAGNOSTIC EVALUATION
✅ Performed to confirm dislocation, rule out fractures, and plan treatment.
🔹 A. Physical Examination
- Visual Inspection: Abnormal shape/contour
- Palpation: Detects tenderness, swelling
- ROM Test: Limited or absent due to pain
- Neurovascular Check: Pulses, capillary refill, sensation, motor function
🔹 B. Imaging Studies
| Test | Purpose |
|---|---|
| 🩻 X-ray | Confirms bone displacement, rules out fractures |
| 🧲 MRI | Evaluates soft tissue damage (ligaments, cartilage, tendons) |
| 🧠 CT Scan | Detailed bone view, especially in complex joints |
| 🎯 Ultrasound | Useful in shoulder dislocations or infants (e.g., developmental dysplasia of hip) |
🔹 C. Special Tests (Joint-specific)
- Apprehension Test – For recurrent shoulder dislocation
- Drawer Test – For knee instability (ligament injury)
- Barlow/Ortolani Test – For neonatal hip dislocation
🧾 Additional: Laboratory Tests (only if infection/inflammation suspected)
- WBC Count – Elevated in septic arthritis
- CRP, ESR – To rule out underlying inflammatory conditions
📌 Quick Summary Table
| Aspect | Key Points |
|---|---|
| Pathophysiology | Trauma → ligament tear → joint misalignment → pain & immobility |
| Symptoms | Pain, swelling, deformity, loss of motion, numbness |
| Diagnosis | X-ray, MRI, CT scan, physical exam, special tests |
🔷 I. MEDICAL MANAGEMENT
The primary goals are to relieve pain, realign the joint, and restore function while preventing complications.
✅ 1. Initial Emergency Care (First Aid)
🆘 At the scene or in the ER:
- 🧊 Immobilize the affected joint immediately
- ❌ Do NOT attempt to realign without medical supervision
- 📦 Apply cold compress to reduce swelling
- 🧼 Elevate the limb (if possible)
- 🚑 Transport to hospital promptly
💊 2. Pharmacological Management
| Drug | Purpose |
|---|---|
| 💊 Analgesics (e.g., Paracetamol) | Relieve pain |
| 💉 NSAIDs (e.g., Ibuprofen, Diclofenac) | Reduce inflammation and pain |
| 💤 Muscle Relaxants (e.g., Diazepam) | Reduce muscle spasms before or after reduction |
| 💊 Sedation/Anesthesia (IV midazolam or propofol) | Used during joint reduction |
| 💉 Local/Regional Anesthetic | For pain control during manual manipulation |
| 💊 Antibiotics | If open dislocation or infection risk present |
| 💊 Tetanus prophylaxis | For open injuries or wounds |
👐 3. Closed Reduction (Manual Realignment)
➡️ Performed by an orthopedic specialist
➡️ Uses gentle traction and manipulation
➡️ Often done under sedation or local anesthesia
➡️ Followed by immobilization with:
- Sling
- Splint
- Cast
- Brace
🦵 4. Immobilization & Rest
✅ Duration: 2–6 weeks depending on joint and severity
✅ Purpose: Allow ligaments and joint capsule to heal
🏃 5. Physical Therapy (Rehabilitation)
Begins after immobilization phase to regain:
- 💪 Strength
- 🌀 Range of motion
- ⚖️ Joint stability
- 🔄 Functional independence
🔶 II. SURGICAL MANAGEMENT
Surgery is indicated when:
🚫 Closed reduction fails
🔁 Recurrent dislocations occur
🦴 Accompanying fractures or ligament tears
🧬 Congenital dislocation (e.g., hip in infants)
💥 Vascular or nerve damage present
🛠️ Common Surgical Procedures:
| Surgery Type | Description |
|---|---|
| 🛠️ Open Reduction | Surgical realignment of the joint when manual (closed) reduction fails |
| 🪛 Internal Fixation | Screws, plates, or pins used to stabilize bones (if fracture involved) |
| ⚙️ Ligament Repair or Reconstruction | Repair torn ligaments to prevent future dislocations (e.g., ACL repair) |
| 🦴 Joint Capsule Tightening | Tightens loose joint structures (common in recurrent shoulder dislocations) |
| 🦿 Arthroplasty | Joint replacement, typically in chronic or degenerative dislocations |
| 📹 Arthroscopy | Minimally invasive procedure to inspect/repair joint structures |
🔄 Post-Surgical Management
🧑⚕️ Nursing & Rehab care includes:
- Pain management
- Wound care
- Monitoring for infection or neurovascular impairment
- Gradual physiotherapy to restore mobility
- Patient education on avoiding re-injury
📌 Summary Chart
| Management Type | Includes |
|---|---|
| Medical | Analgesics, NSAIDs, muscle relaxants, closed reduction, immobilization, physiotherapy |
| Surgical | Open reduction, internal fixation, ligament repair, joint capsule repair, arthroplasty |
🧑⚕️🦴 Nursing Management of Dislocation
(Complete joint displacement)
🎯 Goals of Nursing Care
✅ Relieve pain and discomfort
✅ Prevent complications (e.g., nerve damage, stiffness)
✅ Promote joint healing
✅ Restore joint mobility and function
✅ Educate the patient for rehabilitation and prevention
🔷 I. NURSING ASSESSMENT
🔍 A. Initial Assessment
| Parameter | Assessment |
|---|---|
| 🔺 Pain | Use pain scale (0–10), location, quality |
| 🔄 ROM | Limited, painful, or absent movement |
| 🧊 Swelling | Localized edema and inflammation |
| 🧠 Neurovascular Status | Color, warmth, sensation, pulses, capillary refill, movement distal to injury |
| ⚙️ Deformity | Obvious joint displacement, abnormal shape |
| 🧾 History | Trauma, injury mechanism, past dislocations, comorbidities |
📝 II. NURSING DIAGNOSES
Some common nursing diagnoses for a patient with dislocation:
- Acute Pain related to joint injury and inflammation
- Impaired Physical Mobility related to dislocation and immobilization
- Risk for Neurovascular Dysfunction related to swelling or compression
- Risk for Infection (if surgical wound or open dislocation)
- Deficient Knowledge related to condition, treatment, and prevention
🔶 III. NURSING INTERVENTIONS
💊 1. Pain Management
- Administer prescribed analgesics and NSAIDs
- Apply cold compress to reduce swelling and pain
- Encourage immobilization and rest of the joint
- Position for comfort and support
🩺 2. Neurovascular Monitoring
- Perform frequent neurovascular checks (every 2–4 hours):
- Color
- Temperature
- Pulse
- Sensation
- Movement
- Capillary refill
- Report immediately if signs of nerve/vascular compromise (numbness, cyanosis, weak pulse)
🧍 3. Mobility & Safety
- Maintain joint immobilization as prescribed (splint, sling, brace)
- Encourage gradual mobilization with physiotherapist post-reduction
- Teach safe use of assistive devices (walker, crutches if needed)
- Prevent falls and further injury
🧼 4. Post-Operative/Wound Care (if surgery done)
- Monitor wound site for signs of infection (redness, warmth, drainage)
- Follow aseptic dressing change technique
- Educate on wound care at home
🧠 5. Patient Education
- Instruct on joint protection techniques
- Demonstrate range of motion (ROM) exercises as advised
- Emphasize importance of adhering to rehabilitation plan
- Teach signs to report (numbness, increasing pain, swelling)
- Educate on recurrence prevention:
- Avoid risky activities until cleared
- Strengthening surrounding muscles
🧾 IV. EVALUATION
✅ Pain is managed (patient verbalizes relief)
✅ Joint function is gradually restored
✅ Neurovascular status remains intact
✅ No signs of infection or complications
✅ Patient demonstrates understanding of care and prevention
📌 Quick Summary Chart
| Nursing Action | Rationale |
|---|---|
| Pain relief | Promote comfort and rest |
| Immobilization | Support healing and prevent further injury |
| Neurovascular checks | Detect early complications like ischemia |
| Physiotherapy | Restore strength and mobility |
| Education | Prevent recurrence and enhance self-care |
⚠️🦴 Complications & Key Points of Dislocation
🔶 I. COMPLICATIONS OF DISLOCATION
If not treated promptly and properly, dislocation can lead to several acute and long-term complications:
🚨 1. Neurovascular Compromise
- Compression or stretching of nerves or blood vessels
- May lead to:
- Numbness or tingling
- Cold, pale limb
- Weak or absent pulse
- Permanent nerve damage if untreated
🩻 2. Associated Fractures
- Dislocation + fracture = complex injury
- Common in shoulder, elbow, hip
- Requires surgical fixation
🔁 3. Recurrent Dislocations
- Once dislocated, the joint may become unstable
- Common in shoulder and patella
- May need ligament repair or capsular tightening surgery
🧠 4. Joint Stiffness and Limited Mobility
- Due to prolonged immobilization
- May result in frozen joint (adhesive capsulitis)
- Requires aggressive physiotherapy
🧪 5. Infection (if open injury or post-op)
- Can lead to septic arthritis or osteomyelitis
- Requires antibiotics and wound care
🧬 6. Avascular Necrosis (AVN)
- Occurs when blood supply is cut off to a bone (especially in hip dislocations)
- Bone tissue dies → joint collapses → may need joint replacement
🧠 7. Chronic Pain and Arthritis
- Due to cartilage damage or incomplete healing
- Leads to post-traumatic osteoarthritis
📌 II. KEY POINTS TO REMEMBER
📝 Use these as a quick revision list or nursing highlights:
✅ Dislocation = complete displacement of joint surfaces
✅ Most common joints: shoulder, finger, hip, knee
✅ Immediate management = Immobilize ➕ Cold compress ➕ Pain control ➕ Hospital referral
✅ Closed reduction is the first line of treatment
✅ Post-reduction care includes immobilization and physical therapy
✅ Perform neurovascular assessments regularly
✅ Monitor for swelling, numbness, or deformity
✅ Patient education is crucial to prevent recurrence
✅ Early rehab = better outcomes and restored mobility
✅ Complications include nerve injury, AVN, recurrence, arthritis
🦴💥 Fracture
(Definition & Causes)
🔷 DEFINITION
A fracture is a break in the continuity of a bone due to trauma, stress, or a pathological process.
In simpler terms:
💥 Fracture = Cracked or broken bone
🧠 It may involve a complete or incomplete break and can affect bone shape, alignment, and function.
🔶 CAUSES OF FRACTURE
Fractures can result from external trauma or internal weakening of the bone.
✅ 1. Traumatic Causes
🛑 Direct or Indirect Force applied to the bone
- 🚗 Road Traffic Accidents – High-impact injuries
- 🤕 Falls – Common in elderly and children
- 🏋️ Sports Injuries – Sudden impact, twisting, or overuse
- 🔨 Assault or Violence – Blunt force trauma
✅ 2. Pathological Causes
🦴 Bone breaks due to disease even with minor stress
- 🧬 Osteoporosis – Brittle bones due to calcium loss
- 🎗️ Bone Tumors (Benign/Malignant) – Weakens bone integrity
- 🧪 Osteomyelitis – Bone infection
- 🤒 Cancers with Bone Metastasis – From breast, prostate, lung
- 💊 Long-term steroid use – Causes bone thinning
✅ 3. Stress or Fatigue Fractures
🔁 Repeated stress over time causes tiny cracks in the bone
- Common in athletes, military recruits, dancers
- Affects weight-bearing bones: tibia, metatarsals, femur
✅ 4. Congenital or Genetic Conditions
🧬 Bone deformities from birth or inherited diseases
- Osteogenesis Imperfecta – “Brittle bone disease”
- Rickets – Vitamin D deficiency causing soft bones in children
✅ 5. Iatrogenic Causes (Medical Interventions)
🛠️ Bone fracture caused during surgical procedures, manipulations, or by incorrect use of orthopedic devices.
📌 Quick Summary Table: Causes of Fracture
| Cause Type | Examples |
|---|---|
| Traumatic | Falls, RTA, sports injuries |
| Pathological | Osteoporosis, bone cancer, osteomyelitis |
| Stress/Fatigue | Repeated strain in athletes |
| Congenital/Genetic | Osteogenesis imperfecta, Rickets |
| Iatrogenic | Surgical error, medical mishandling |
🦴📚 Types of Fractures
(Based on pattern, skin, bone condition, and mechanism)
🔷 I. BASED ON SKIN INVOLVEMENT
1️⃣ Closed Fracture (Simple)
- Bone breaks but skin remains intact
- No external wound
🩹 Less infection risk
2️⃣ Open Fracture (Compound)
- Bone breaks and pierces through the skin
- External wound visible
⚠️ High infection risk
💉 Needs urgent debridement & antibiotics
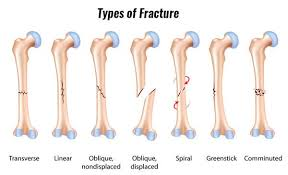
🔶 II. BASED ON PATTERN/SHAPE OF BREAK
1. Transverse Fracture ➖
🦴 Break is horizontal across the bone shaft
📌 Caused by direct force
2. Oblique Fracture ⬡
🦴 Break is angled across the bone
🔁 Caused by twisting with force
3. Spiral Fracture 🌀
🦴 Break spirals around the bone
⚠️ Often due to rotational or twisting injury
🧠 May raise suspicion in child abuse
4. Comminuted Fracture 🔨
🦴 Bone is broken into 3 or more fragments
💥 High-impact trauma (e.g., crush injury)
5. Segmental Fracture 🍂
🦴 Multiple fractures in the same bone with separate segments
6. Impacted Fracture 🔩
🦴 Bone ends are driven into each other
⚠️ Common in falls from height (e.g., hip fracture)
7. Greenstick Fracture 🌿
🦴 Incomplete break where one side bends and the other breaks
🧒 Seen only in children (softer bones)
8. Compression Fracture 🧱
🦴 Bone is crushed or compressed
🔻 Common in vertebrae of osteoporotic patients
9. Avulsion Fracture 🪢
🦴 A tendon or ligament pulls off a piece of bone
🏃 Seen in athletes (e.g., ankle, knee)
10. Hairline or Stress Fracture 🩻
🦴 Tiny, thin cracks due to repetitive strain
😣 Often missed on early X-rays
🎯 Common in tibia, metatarsals
🔷 III. BASED ON LOCATION
| Fracture Type | Common Location |
|---|---|
| Colles’ fracture | Distal radius (wrist) – fall on outstretched hand |
| Smith’s fracture | Reverse of Colles’ – fall on flexed wrist |
| Pott’s fracture | Ankle fracture – malleoli of tibia/fibula |
| Supracondylar fracture | Above elbow – common in children |
| Intertrochanteric fracture | Between femoral trochanters – elderly falls |
| Femoral neck fracture | High-risk in osteoporosis – leads to hip replacement |
🔶 IV. BASED ON STABILITY
| Type | Description |
|---|---|
| Stable Fracture | Bone ends remain aligned – minimal displacement |
| Unstable Fracture | Bone ends are misaligned or displaced – higher risk of complications |
🔷 V. SPECIAL TYPES
🧒 Pediatric Fractures
- Greenstick
- Torus (buckle) – cortex bulges but doesn’t break
- Growth plate (physeal) fracture – may affect bone growth
💀 Pathological Fractures
- Occur in bones weakened by disease
(e.g., osteoporosis, tumors, infections)
🔁 Recurrent/Old Fractures
- Improperly healed = malunion or non-union
📌 QUICK RECAP TABLE
| Classification | Type | Example |
|---|---|---|
| By Skin | Closed / Open | Simple vs. Compound |
| By Pattern | Transverse, Oblique, Spiral, Comminuted | Direction of break |
| By Completeness | Complete / Incomplete | Greenstick (incomplete) |
| By Bone Condition | Pathological / Stress | Osteoporosis, athletes |
| By Special Site | Colles’, Pott’s, Femoral neck | Location-specific |
| By Mechanism | Impacted, Avulsion, Compression | Trauma-type |
🔬🦴 Pathophysiology of All Types of Fractures
💥 GENERAL PATHOPHYSIOLOGY OF A FRACTURE
Regardless of the type, all fractures follow a similar pathophysiological process after the break:
🧠 Step-by-Step General Mechanism:
- Trauma or stress → Bone exceeds its strength
- 💢 Break in bone continuity occurs
- ⚠️ Bleeding from damaged vessels → Hematoma formation
- 😣 Inflammation sets in (pain, swelling, warmth)
- 🧱 Fibroblasts and osteoblasts proliferate → Callus formation
- 🏗️ Bone remodeling occurs → Hard bone replaces soft callus
- ⏳ Healing time depends on age, site, type of fracture, and comorbidities
🔷 I. PATHOPHYSIOLOGY BY FRACTURE PATTERN
1️⃣ Transverse Fracture ➖
- Caused by direct perpendicular force
- Bone splits straight across
- Stable if not displaced
- Good healing prognosis if immobilized
2️⃣ Oblique Fracture ⬡
- Caused by angled force or fall
- Creates diagonal fracture line
- Often unstable → risk of displacement
3️⃣ Spiral Fracture 🌀
- Caused by twisting or rotational force
- Spiral pattern along the shaft
- Often seen in child abuse or sports injuries
- High risk of soft tissue damage
4️⃣ Comminuted Fracture 🔨
- High-energy trauma leads to bone shattering into 3+ pieces
- Soft tissues are severely injured
- Healing is prolonged due to multiple fragments
5️⃣ Segmental Fracture 🍂
- Two or more distinct breaks in same bone → floating segment
- Very unstable
- High risk for malunion or nonunion
6️⃣ Impacted Fracture 🔩
- One bone fragment is driven into another
- Absorbs shock but disrupts normal alignment
- Common in falls and osteoporotic bones
7️⃣ Greenstick Fracture 🌿 (Pediatric)
- One side of the bone bends, other side cracks
- Due to soft, pliable bones in children
- Heals well but may be missed on initial X-rays
8️⃣ Compression Fracture 🧱
- Bone is crushed or flattened due to axial force
- Occurs in vertebrae, especially with osteoporosis
- May cause kyphosis or nerve compression
9️⃣ Avulsion Fracture 🪢
- Tendon or ligament pulls a bone piece away
- Caused by sudden muscle contraction
- Seen in athletes (ankle, hip, knee)
🔟 Hairline/Stress Fracture 📏
- Tiny cracks due to repetitive overuse
- Often missed initially
- Seen in runners, military recruits
- Healing is slow; worsens if ignored
🔶 II. PATHOPHYSIOLOGY OF SPECIAL FRACTURE TYPES
⚠️ Open (Compound) Fracture
- Bone breaks through the skin
- Risk of infection (osteomyelitis)
- Must address bleeding and contamination
- Delayed healing due to soft tissue involvement
🚫 Closed (Simple) Fracture
- Skin intact
- Lower infection risk
- Standard healing pathway applies
🦴 Pathological Fracture
- Occurs in weakened bone due to disease
(e.g., osteoporosis, tumors, osteomyelitis) - Minimal or no trauma needed to cause break
- Healing is delayed due to poor bone quality
🔁 Recurrent or Non-union Fractures
- Improper healing or instability leads to:
- Malunion (heals in wrong position)
- Non-union (fails to heal at all)
- Requires surgical fixation or bone grafting
🌱 Pediatric/Growth Plate Fracture
- Involves epiphyseal plate (growth center)
- Risk of growth disturbance if not treated properly
- Salter-Harris classification used for grading
📌 Summary Table: Fracture Type vs Pathophysiology
| Fracture Type | Key Pathophysiology |
|---|---|
| Transverse | Direct blow → clean horizontal break |
| Oblique | Angled force → diagonal fracture line |
| Spiral | Twisting force → spiral fracture, risk of soft tissue injury |
| Comminuted | High energy trauma → multiple fragments |
| Greenstick | Pediatric bending → incomplete break |
| Compression | Axial load crushes vertebrae |
| Avulsion | Tendon/ligament force → bone fragment pulled |
| Stress | Microtrauma over time → small crack |
| Open | Bone exposed through skin → infection risk |
| Pathological | Weak bone structure breaks with minimal trauma |
🔷 I. SIGNS & SYMPTOMS OF FRACTURE
Fracture symptoms vary by location and severity but typically include pain, deformity, and loss of function.
🧠 Common Clinical Features
| Symptom | Description |
|---|---|
| 🔺 Pain | Sudden, sharp, localized at the site of fracture; worsens with movement or pressure |
| 🔻 Swelling | Due to inflammation and bleeding in surrounding tissues |
| 🩸 Bruising (Ecchymosis) | Discoloration due to subcutaneous bleeding |
| 🦴 Deformity | Limb appears crooked, shortened, or misaligned |
| ✋ Tenderness | On palpation over the fractured area |
| ⚠️ Crepitus | Grating sound or sensation when bone ends rub together |
| 🚫 Loss of Function | Inability to move or bear weight on the affected part |
| ❄️ Coolness or Pallor | Sign of vascular compromise in severe fractures |
| ⚡ Numbness or Tingling | If nerve injury is associated with the fracture |
| 💢 Muscle Spasms | Reflex spasm around broken bone causing more pain |
⚠️ Open fractures will also have external wound and possible bone protrusion.
🚨 Red Flag Symptoms (Indicate Emergency)
- Absent or weak distal pulses
- Cyanosis or cold extremity
- Severe, increasing pain despite analgesia
- Loss of sensation or motor function
- Bone visible through the skin
🔶 II. DIAGNOSTIC EVALUATION
Proper diagnosis is essential for confirming the type, location, and extent of the fracture.
🩺 A. Physical Examination
- Inspection: Observe swelling, bruising, deformity, open wounds
- Palpation: Check tenderness, warmth, abnormal mobility, crepitus
- Neurovascular check: Assess capillary refill, pulses, movement & sensation below the injury site
🧪 B. Imaging Studies
| Test | Purpose |
|---|---|
| 🩻 X-ray | ✅ First-line test |
| 🔍 Shows fracture line, displacement, alignment | |
| 🧲 MRI | ✅ Detailed soft tissue view |
| 📍 Detects occult/stress fractures, ligament injury | |
| 🧠 CT Scan | ✅ 3D view |
| 📐 Used for complex fractures (e.g., pelvis, spine, joints) | |
| 📊 Bone Scan | ✅ Detects hidden stress fractures or AVN |
| ☢️ Uses radioactive tracer | |
| 🔬 Ultrasound (Pediatrics) | ✅ Detects subtle fractures in children, especially around the hip or wrist |
🧫 C. Laboratory Tests (If Needed)
Used when fracture is associated with disease or complication:
| Test | Indication |
|---|---|
| 🩸 CBC (Complete Blood Count) | Detects blood loss or infection |
| 🧪 ESR / CRP | Elevated in infection or inflammation (e.g., open fracture, osteomyelitis) |
| 🧬 Calcium, Phosphorus, ALP | Bone metabolism in pathological fractures |
| 💊 Vitamin D level | Checked in recurrent or spontaneous fractures |
| 🔍 Culture & Sensitivity | From open wound or pus if infection is suspected |
📌 SUMMARY TABLE
| Category | Findings |
|---|---|
| Signs & Symptoms | Pain, swelling, bruising, deformity, crepitus, loss of function |
| Emergency Signs | Absent pulses, numbness, cold limb, open wound |
| Diagnosis | X-ray (first-line), MRI/CT (for complex), bone scan (occult), labs (if infection/pathology suspected) |
🩹🛠️ Medical and Surgical Management of Fractures
🔷 I. GOALS OF MANAGEMENT
✅ Relieve pain
✅ Restore bone alignment
✅ Promote bone healing
✅ Preserve joint function
✅ Prevent complications (infection, deformity, neurovascular compromise)
🩺 II. MEDICAL MANAGEMENT
Medical (non-surgical) management is preferred when fractures are:
- Stable
- Non-displaced
- In children, or
- Where surgery is contraindicated (e.g., elderly, high-risk patients)
💊 A. Initial Emergency Care (First Aid)
At the site of injury or ER:
| Action | Purpose |
|---|---|
| 🧊 Immobilize the affected part | Prevent further damage |
| 🩸 Control bleeding (if open fracture) | Minimize blood loss |
| ❌ Do NOT attempt realignment | Could damage nerves/vessels |
| 🚑 Transport carefully | To avoid worsening the injury |
💉 B. Pharmacological Management
| Medication | Purpose |
|---|---|
| 💊 Analgesics (e.g., Paracetamol) | Relieve mild to moderate pain |
| 💉 NSAIDs (e.g., Ibuprofen, Diclofenac) | Control inflammation and pain |
| 💊 Muscle Relaxants (e.g., Diazepam) | Reduce muscle spasms |
| 💊 Antibiotics | Prevent/treat infection in open fractures |
| 💉 Tetanus Toxoid | If wound is open or contaminated |
🩼 C. Immobilization Methods
Used to maintain alignment and stability during healing.
| Method | Description |
|---|---|
| 🪢 Splints | Temporary immobilization (acute phase) |
| 🦵 Casts | Plaster or fiberglass to hold bone in place |
| 🛏️ Traction | Weights & pulleys to align bone gradually |
| 🧯 Braces/Slings | Support during recovery |
| 📏 Functional Cast Bracing | Allows partial movement during healing |
🏃 D. Rehabilitation
After healing or immobilization:
- 🌀 Gradual ROM (Range of Motion) exercises
- 💪 Muscle strengthening
- 🚶 Gait training (if limb affected)
- 🧠 Patient education on activity restriction & fall prevention
🛠️ III. SURGICAL MANAGEMENT
Surgery is needed when:
- Fracture is displaced, unstable, or compound
- There’s failure of healing (non-union)
- In multiple or complex fractures
- There’s joint involvement or neurovascular damage
🔧 Common Surgical Techniques
| Procedure | Purpose |
|---|---|
| 🧲 Open Reduction & Internal Fixation (ORIF) | Open surgical exposure of fracture and alignment using plates, screws, or rods |
| 📍 External Fixation | Pins placed through skin & bone connected by external frame – ideal for open or infected fractures |
| 🔩 Intramedullary Nailing | Metal rod inserted into medullary cavity of long bones (e.g., femur, tibia) |
| 🧱 Bone Grafting | Used when there’s bone loss or non-union |
| 🧼 Debridement & Wound Closure | For open fractures to remove debris and prevent infection |
| 🦿 Arthroplasty | Joint replacement in case of fracture with joint destruction (e.g., hip replacement in elderly femoral neck fracture) |
🧾 Post-Operative Care Includes:
- Pain management
- Monitoring for infection and bleeding
- Neurovascular assessments
- Wound care and dressing changes
- Early mobilization under supervision
- Thromboprophylaxis (to prevent blood clots)
📌 SUMMARY TABLE
| Management Type | Key Interventions |
|---|---|
| Medical | Immobilization, medications, closed reduction, rest, rehab |
| Surgical | ORIF, external fixation, bone grafting, arthroplasty |
| Rehab | ROM, strengthening, assistive device training |
🧑⚕️🦴 Nursing Management of Fractures
🎯 GOALS OF NURSING CARE
✅ Relieve pain
✅ Promote bone healing
✅ Prevent complications (e.g., infection, DVT, contractures)
✅ Restore mobility and function
✅ Provide patient education for recovery and self-care
🔷 I. NURSING ASSESSMENT
Perform comprehensive initial and ongoing assessments:
🔍 Physical Examination
| Component | What to Assess |
|---|---|
| 🩹 Pain | Location, intensity, duration, nature (sharp, dull) |
| 🦴 Deformity or Swelling | Compare both sides |
| ✋ Tenderness & Crepitus | On palpation |
| 🚫 ROM | Limited or absent due to pain |
| 🧠 Neurovascular Status | 6 P’s: Pain, Pallor, Paralysis, Paresthesia, Pulselessness, Poikilothermia |
| 💉 Wound Site (if open fracture) | Signs of infection, drainage, wound care status |
📝 II. COMMON NURSING DIAGNOSES
- 🩻 Acute Pain related to fracture and muscle spasm
- 🚷 Impaired Physical Mobility related to immobilization or pain
- ⚠️ Risk for Neurovascular Dysfunction related to compression from swelling or cast
- 🧫 Risk for Infection related to open fracture or surgical wound
- 🧠 Deficient Knowledge regarding condition and self-care
- 🛌 Risk for Constipation related to immobility and analgesic use
- 🩸 Risk for Deep Vein Thrombosis (DVT) related to reduced mobility
🩺 III. NURSING INTERVENTIONS
💊 1. Pain Management
- Administer prescribed analgesics and NSAIDs
- Apply ice packs during the acute phase (first 24–48 hours)
- Elevate the affected limb to reduce edema
- Ensure proper alignment and support of the limb
- Provide calm environment to reduce anxiety-induced pain
🩼 2. Maintain Immobilization and Support
- Monitor tightness or fit of casts, splints, or braces
- Reposition limb gently and regularly
- Do not disturb traction weights if applied
- Ensure traction ropes are free, aligned, and unobstructed
🧠 3. Neurovascular Monitoring (EVERY 1–2 HOURS INITIALLY)
- Capillary refill time
- Peripheral pulses distal to the injury
- Color, temperature, sensation, and movement
- Report immediately if signs of neurovascular compromise appear
🧼 4. Wound & Pin Site Care
- Maintain aseptic technique during dressing changes
- Monitor for redness, pus, foul odor or warmth
- Educate on signs of infection
🧍 5. Mobility and DVT Prevention
- Encourage early mobilization as tolerated
- Perform active/passive ROM exercises for unaffected limbs
- Encourage use of walker or crutches as advised
- Apply compression stockings if prescribed
- Encourage leg elevation and hydration
🍽️ 6. Nutrition & Elimination
- Encourage high-protein, calcium, and vitamin D intake for bone healing
- Maintain adequate fluid and fiber to prevent constipation
- Administer stool softeners or laxatives if prescribed
🧾 7. Patient and Family Education
- Importance of cast care (e.g., keep dry, do not insert objects)
- Recognize and report red flags:
➤ Numbness
➤ Increasing pain
➤ Swelling under the cast
➤ Fever or discharge - Instructions on mobility aids, weight-bearing restrictions, and follow-ups
- Smoking cessation, as it delays bone healing
📌 IV. EVALUATION (OUTCOMES TO MONITOR)
| Goal | Expected Outcome |
|---|---|
| ✅ Pain relief | Patient reports decreased pain |
| ✅ Neurovascular integrity | Normal pulses, sensation, and movement maintained |
| ✅ Infection prevention | Wound heals without signs of infection |
| ✅ Mobility improvement | Patient performs ROM and ambulates with/without aid |
| ✅ Knowledge gained | Patient verbalizes cast care and follow-up instructions |
⚠️🦴 Fractures: Complications & Key Points
🔶 I. COMPLICATIONS OF FRACTURES
Fractures can lead to local and systemic complications, especially if not managed properly or timely.
🔹 A. Early (Acute) Complications
| Complication | Description |
|---|---|
| ⚠️ Neurovascular Injury | Damage to surrounding nerves or blood vessels → numbness, tingling, pulseless limb |
| 💥 Compartment Syndrome | Increased pressure within muscle compartments → severe pain, pallor, paralysis (surgical emergency!) |
| 🩸 Hemorrhage/Shock | Excessive bleeding (especially in long bone fractures like femur or pelvis) |
| 🧫 Infection | Especially in open or compound fractures → may lead to osteomyelitis |
| ❌ Fat Embolism Syndrome | Fat globules enter bloodstream (common in femur fracture) → respiratory distress, petechiae, altered sensorium |
| 🧊 Venous Thromboembolism (VTE) | DVT or pulmonary embolism due to immobility |
🔹 B. Late (Chronic) Complications
| Complication | Description |
|---|---|
| 🦴 Delayed Union/Non-union | Fracture heals very slowly or not at all |
| 🔀 Malunion | Bone heals in wrong position causing deformity |
| 🔁 Joint Stiffness & Loss of Function | Especially if immobilization is prolonged |
| 🔄 Post-traumatic Arthritis | Cartilage damage leads to chronic joint pain and stiffness |
| 🧬 Avascular Necrosis (AVN) | Bone dies due to loss of blood supply (e.g., femoral head) |
| 🪛 Hardware-related issues | Loosening, breakage, or infection from plates/screws |
📌 II. KEY POINTS TO REMEMBER
📝 Use these as high-yield summary points for quick recall:
✅ Fracture = break in bone continuity
✅ Causes: trauma, osteoporosis, tumors, stress, pathology
✅ Classified by skin involvement, pattern, location, stability
✅ Common symptoms: pain, swelling, deformity, crepitus, loss of function
✅ X-ray is first-line diagnostic tool
✅ Management includes immobilization, pain relief, reduction (closed/open), surgery
✅ Watch for neurovascular compromise – do frequent 6 P’s check
✅ Start early physiotherapy to prevent stiffness & restore mobility
✅ Monitor for signs of compartment syndrome, fat embolism, infection
✅ Patient education is crucial for cast care, mobility, diet, and follow-up
🦶⚠️ SPRAIN: Complete Overview

🔷 1. DEFINITION
A sprain is a stretching or tearing of ligaments, which are the tough bands of fibrous tissue connecting bones to one another in a joint.
🧠 Ligaments = Bone to bone
Sprain = Injury to ligament (not muscle or bone)
🔶 2. CAUSES OF SPRAIN
| Cause | Description |
|---|---|
| 🤸♀️ Sudden twisting movement | Common in sports, falls, or awkward landings |
| 🕳️ Stepping on uneven surfaces | Ankle sprains common in outdoor activity |
| 🚶♂️ Overstretching of joint | During sudden impact or excessive load |
| 🧍♀️ Poor footwear or posture | Adds strain to joints |
| 🛠️ Accidents or trauma | Slips, trips, falls, vehicle accidents |
🔷 3. TYPES OF SPRAIN (Based on Severity)
| Grade | Description | Symptoms |
|---|---|---|
| Grade I (Mild) | Slight stretching, microscopic tears | Mild pain, swelling, no instability |
| Grade II (Moderate) | Partial tearing of ligament | Moderate pain, swelling, bruising, some joint looseness |
| Grade III (Severe) | Complete tear of the ligament | Severe pain, instability, inability to bear weight |
🦶 Most common site:
- Ankle sprain (esp. lateral ligaments)
- Also occurs in knee, wrist, thumb
🔬 4. PATHOPHYSIOLOGY
- Sudden force or twist stretches the ligament beyond normal range
- ➡️ Micro-tears or complete rupture occurs
- ➡️ Local tissue damage → inflammatory response
- ➡️ Increased blood flow → swelling, redness, warmth
- ➡️ Pain receptors activated
- ➡️ Joint instability may result if ligaments are severely torn
- ➡️ Healing process begins (takes weeks to months depending on grade)
🚨 5. SIGNS AND SYMPTOMS
| Symptom | Description |
|---|---|
| 🔺 Pain | At affected joint, especially on movement or pressure |
| 💢 Swelling | Due to inflammation and fluid accumulation |
| 💜 Bruising | Discoloration from internal bleeding |
| ❄️ Tenderness | Over the ligament or joint line |
| ⚠️ Instability | Feeling of “giving way” in joint (in moderate/severe sprain) |
| 🚫 Limited ROM | Due to pain or swelling |
| 🌡️ Warmth & Redness | Localized inflammation (in acute phase) |
🧪 6. DIAGNOSTIC EVALUATION
| Test | Purpose |
|---|---|
| 🧑⚕️ Physical Exam | Check swelling, tenderness, joint stability, ROM |
| 🩻 X-ray | To rule out fractures |
| 🧲 MRI | Best for viewing ligament tears |
| 📸 Ultrasound | Can assess soft tissue injury dynamically |
| 🧠 Stress Tests | (e.g., anterior drawer for ankle sprain) assess ligament laxity |
💊 7. MEDICAL MANAGEMENT
🧊 Initial: R.I.C.E. Protocol (First 48–72 hours)
| Component | Action |
|---|---|
| 🅁 = Rest | Avoid weight-bearing on affected joint |
| 🅄 = Ice | Apply 15–20 mins every 2–3 hours to reduce swelling |
| 🄲 = Compression | Elastic bandage or support wrap |
| 🄴 = Elevation | Keep injured area above heart level |
💊 Medications
| Drug | Purpose |
|---|---|
| NSAIDs (Ibuprofen, Diclofenac) | Reduce pain & inflammation |
| Topical analgesics | For localized pain relief |
| Muscle relaxants | If spasms are present |
| Vitamin C, Zinc | Aid tissue repair |
🛠️ 8. SURGICAL MANAGEMENT
Usually not required for mild/moderate sprains. Indicated in:
✅ Grade III (complete ligament tear)
✅ Recurrent sprains with chronic instability
✅ Failure of conservative management
🔧 Surgical Procedures
- Ligament repair (suturing torn ends)
- Ligament reconstruction (using grafts)
- Arthroscopy – Minimally invasive technique to assess and treat joint damage
🧑⚕️ 9. NURSING MANAGEMENT
✅ Nursing Assessment
- Monitor pain level, swelling, skin color, ROM
- Neurovascular assessment – check pulses, sensation, movement
- Evaluate mobility limitations and assistive device needs
✅ Nursing Interventions
| Intervention | Rationale |
|---|---|
| Elevate limb | Reduces swelling |
| Apply cold packs | Decrease pain & inflammation |
| Administer analgesics | Relieves discomfort |
| Educate on RICE protocol | Promotes healing |
| Support with splint/bracing | Prevents further injury |
| Teach ROM exercises (after 48–72 hrs) | Prevents stiffness |
| Encourage safe ambulation | Prevent falls |
| Explain signs of complications | Empower early reporting |
⚠️ 10. COMPLICATIONS
| Complication | Description |
|---|---|
| 🔁 Chronic Joint Instability | From repeated or severe sprains |
| 🧊 Stiffness & Reduced ROM | Due to prolonged immobilization |
| 🧫 Ligamentous Calcification | Abnormal healing or poor blood supply |
| 😖 Persistent Pain or Swelling | From poor healing or unrecognized complete tear |
| ⚠️ Associated injuries | Meniscus tear (knee), tendon strain, fractures |
📌 11. KEY POINTS TO REMEMBER
✅ Sprain = ligament injury (vs. strain = muscle/tendon injury)
✅ Common in ankle, wrist, knee
✅ Graded I–III based on severity
✅ RICE + NSAIDs = first-line treatment
✅ Severe cases may need surgery or prolonged rehab
✅ Always assess for fracture or neurovascular issues
✅ Teach joint protection and exercises post-recovery
💪⚠️ STRAIN: Complete Overview
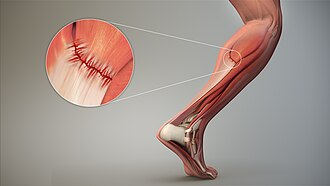
🔷 1. DEFINITION
A strain is the overstretching or tearing of a muscle or tendon (which connects muscle to bone), typically caused by excessive force, overuse, or improper movement.
🧠 Strain = Muscle or tendon injury
(Remember: Strain = Soft tissue like muscle)
🔶 2. CAUSES OF STRAIN
| Cause | Description |
|---|---|
| 🏃♂️ Overuse | Repeated movement (e.g., lifting, sports, running) |
| ⚡ Sudden force or overstretching | Quick acceleration/deceleration |
| ❌ Improper lifting technique | Heavy weights without warm-up |
| 😣 Muscle fatigue | Weak or tired muscles are prone to injury |
| 🛠️ Trauma | Direct impact or fall |
🔷 3. TYPES OF STRAIN (Based on Severity)
| Grade | Description | Symptoms |
|---|---|---|
| Grade I (Mild) | Slight overstretching, small tears | Mild pain, tenderness, no weakness |
| Grade II (Moderate) | Partial muscle or tendon tear | Moderate pain, swelling, weakness |
| Grade III (Severe) | Complete tear of muscle/tendon | Severe pain, swelling, loss of function, visible deformity |
🧍 Common Sites:
- Back (lumbar strain)
- Hamstrings
- Calf (gastrocnemius)
- Shoulder
🔬 4. PATHOPHYSIOLOGY
- Excessive force/stretching → muscle or tendon fibers tear
- ➡️ Tissue damage triggers inflammation
- ➡️ Inflammatory chemicals stimulate pain receptors
- ➡️ Swelling & bruising due to micro-bleeding
- ➡️ Healing begins with fibrous tissue repair
- ➡️ Prolonged or repeated strain can lead to scar formation, decreased flexibility
🚨 5. SIGNS AND SYMPTOMS
| Symptom | Description |
|---|---|
| 🔺 Pain | At the injured muscle or tendon, especially during use |
| 💢 Swelling | Due to inflammation |
| 💜 Bruising | May appear if blood vessels are torn |
| 😖 Tenderness | On palpation |
| 🚫 Muscle weakness | Inability to contract muscle effectively |
| ⚠️ Muscle spasm or cramping | Protective response |
| 🤕 Limited motion | Due to pain and stiffness |
| 🧱 Visible deformity | If complete tear or large hematoma |
🧪 6. DIAGNOSTIC EVALUATION
| Test | Purpose |
|---|---|
| 👨⚕️ Physical exam | Assess swelling, pain, ROM, strength |
| 🩻 X-ray | Rule out fracture (especially in severe cases) |
| 🧲 MRI | Best for viewing muscle/tendon tears |
| 📸 Ultrasound | Dynamic view of soft tissues |
💊 7. MEDICAL MANAGEMENT
🧊 R.I.C.E. Protocol (First 48–72 Hours)
- R – Rest
- I – Ice application (15–20 mins every few hours)
- C – Compression bandage
- E – Elevation above heart level
💊 Medications
| Drug | Purpose |
|---|---|
| NSAIDs | Reduce pain and inflammation |
| Topical analgesics | Temporary pain relief |
| Muscle relaxants | Reduce spasm and stiffness |
| Vitamin C, protein supplements | Aid tissue healing |
🛠️ 8. SURGICAL MANAGEMENT
Surgery is rare, but may be required if:
- Complete muscle/tendon tear (Grade III)
- Severe tendon rupture (e.g., Achilles tendon)
- Persistent symptoms despite conservative treatment
🔧 Surgical Procedures:
- Tendon repair
- Muscle reattachment
- Debridement of scar tissue (in chronic strain)
🧑⚕️ 9. NURSING MANAGEMENT
✅ Nursing Assessment
- Evaluate pain, ROM, swelling, muscle strength
- Monitor for complications like hematoma or deformity
- Assess ability to perform ADLs and mobility
✅ Nursing Interventions
| Intervention | Rationale |
|---|---|
| Apply ice packs | Reduce swelling and pain |
| Elevate limb | Promote venous return |
| Administer prescribed meds | Pain and inflammation relief |
| Encourage gentle ROM exercises (after acute phase) | Prevent stiffness |
| Educate on proper posture and lifting | Prevent recurrence |
| Provide assistive devices if needed | Ensure mobility and safety |
⚠️ 10. COMPLICATIONS
| Complication | Description |
|---|---|
| 🔁 Recurrent strain | Especially if not rested adequately |
| 🧱 Chronic muscle weakness or tightness | Due to improper healing |
| 🧬 Scar tissue formation | Reduces flexibility |
| ❌ Complete rupture | If strain is ignored or worsens |
| ⌛ Delayed healing | In diabetics, elderly, or athletes under pressure |
📌 11. KEY POINTS TO REMEMBER
✅ Strain = muscle or tendon injury (vs sprain = ligament)
✅ Caused by overuse, sudden force, or poor technique
✅ Common in back, hamstring, calf
✅ Follows Grade I–III classification
✅ RICE + NSAIDs are the first line of care
✅ Strengthening & flexibility exercises prevent recurrence
✅ Warm-up before activity is essential
✅ Watch for signs of complete rupture or chronic strain
💢 Contusion (Bruise): Complete Overview

🔷 1. DEFINITION
A contusion is a soft tissue injury caused by blunt force trauma that results in bleeding under the skin without breaking the skin’s surface. This leads to pain, swelling, and discoloration (bruise).
🧠 “Contusion” = internal bleeding within skin, muscle, or soft tissue
Also called a bruise
🔶 2. CAUSES OF CONTUSION
| Cause | Description |
|---|---|
| 🤕 Blunt trauma | Direct hit from object, punch, fall, sports injury |
| 🛠️ Accidental impact | Bumping into hard surfaces or equipment |
| 🏀 Sports injuries | Collisions in contact sports (football, boxing) |
| 🚗 Motor vehicle accidents | Seatbelt or steering wheel trauma |
| 💊 Bleeding disorders or anticoagulants | Increased risk of easy bruising and severe contusions |
🔷 3. TYPES OF CONTUSIONS
| Type | Description |
|---|---|
| Skin contusion (superficial) | Bleeding under skin, commonly known as a bruise |
| Muscle contusion (deep tissue) | Injury to underlying muscle fibers; common in athletes |
| Bone contusion (bone bruise) | Micro-trauma to bone without fracture, seen on MRI |
| Organ contusion | Internal injury to organs like liver, kidney, or brain (e.g., cerebral contusion) – life-threatening |
🔬 4. PATHOPHYSIOLOGY
- Blunt trauma damages capillaries and small blood vessels
- ➡️ Blood leaks into interstitial tissues
- ➡️ Accumulated blood forms hematoma
- ➡️ Causes pain, swelling, and skin discoloration (ecchymosis)
- ➡️ Inflammatory process initiates tissue healing
- ➡️ Hemoglobin breaks down into biliverdin and bilirubin, changing bruise color from red → purple → green → yellow over days
🚨 5. SIGNS AND SYMPTOMS
| Symptom | Description |
|---|---|
| 🔴 Red or purplish skin discoloration | Early stage of bruise |
| 💜 Blue/black patch | Mid-stage contusion (2–4 days) |
| 💛 Yellow-green fading color | Healing stage |
| 💢 Pain or tenderness | At the site of impact |
| 💧 Swelling | Due to inflammation and tissue damage |
| ⚠️ Stiffness or limited movement | If near joint or muscle |
| 😖 Hematoma or lump | Large contusions may form a firm swelling of clotted blood |
🧪 6. DIAGNOSTIC EVALUATION
| Test | Purpose |
|---|---|
| 👁️ Physical Examination | Observe skin color, swelling, tenderness |
| 🧲 MRI | Detect deep tissue or bone contusions |
| 🧫 CBC | Rule out bleeding disorders or anemia |
| 💉 Coagulation profile (PT, aPTT) | Especially if bruising is recurrent or unexplained |
| 📸 X-ray/CT | Rule out associated fractures or organ damage (in high-impact trauma) |
💊 7. MEDICAL MANAGEMENT
🧊 First-line: R.I.C.E. Protocol (First 48–72 hrs)
| R | Rest – Avoid using the injured part |
|---|---|
| I | Ice – 15–20 minutes every 2–3 hours |
| C | Compression – With elastic bandage |
| E | Elevation – To reduce swelling & bleeding |
💊 Medications
| Drug | Purpose |
|---|---|
| NSAIDs (e.g., Ibuprofen) | Pain relief and anti-inflammatory |
| Topical analgesics | For minor contusions |
| Muscle relaxants | For associated spasms (muscle contusions) |
| Vitamin K or platelet therapy | In bleeding disorders |
| Antibiotics | If secondary infection develops (rare) |
🛠️ 8. SURGICAL MANAGEMENT
Surgery is rarely needed, but may be indicated in:
| Condition | Surgical Option |
|---|---|
| Large hematoma | Incision & drainage |
| Organ contusion (e.g., liver, spleen) | Emergency surgery to stop internal bleeding |
| Cerebral contusion with edema | Craniotomy or decompression |
| Compartment syndrome | Fasciotomy (surgical decompression) |
🧑⚕️ 9. NURSING MANAGEMENT
✅ Nursing Assessment
- Monitor pain, size and color of bruise, ROM, and swelling
- Assess for neurovascular integrity if limb is involved
- Identify cause and risk factors (e.g., medications, hemophilia)
✅ Nursing Interventions
| Intervention | Rationale |
|---|---|
| Apply ice packs (first 48 hrs) | Reduces inflammation and pain |
| Elevate affected limb | Promotes venous return and reduces edema |
| Administer NSAIDs as prescribed | Pain and inflammation control |
| Monitor skin color progression | To evaluate healing |
| Educate on avoiding further trauma | Prevent recurrence |
| Encourage gentle ROM exercises | Restore function in affected limb |
| Report unexplained or frequent bruising | May indicate systemic disorder |
⚠️ 10. COMPLICATIONS
| Complication | Description |
|---|---|
| 🩸 Large hematoma | Can cause pressure, pain, and deformity |
| 💥 Compartment syndrome | Increased pressure in muscle compartments, cutting off circulation |
| 🧠 Cerebral edema | In head contusions – may lead to brain herniation |
| 🧫 Secondary infection | Rare, but can occur in deep or untreated contusions |
| 🧬 Tissue fibrosis | From chronic or improperly healed contusions |
📌 11. KEY POINTS TO REMEMBER
✅ Contusion = soft tissue bruise due to blunt trauma
✅ Types include skin, muscle, bone, and organ contusions
✅ Follows RICE + NSAIDs for most cases
✅ Monitor for hematoma, neurovascular changes, or compartment syndrome
✅ Color change in bruise = normal healing process
✅ Deep contusions may mimic more serious injuries → always assess properly
✅ Prevention: protective gear, safe movement, fall prevention
✂️🦿 Amputation:
🔷 1. DEFINITION
Amputation is the surgical or traumatic removal of all or part of a limb, extremity, or body part such as an arm, leg, finger, toe, hand, or foot.
🧠 It may be performed to save life, prevent the spread of infection/gangrene, or remove a nonviable part.
🔶 2. CAUSES OF AMPUTATION
Amputations may be surgical (planned) or traumatic (accidental).
✅ A. Medical/Surgical Causes
| Cause | Description |
|---|---|
| ⚠️ Peripheral Vascular Disease (PVD) | Poor circulation leads to tissue death (esp. in diabetics) |
| 🤒 Diabetes Mellitus | Causes neuropathy and ischemia → foot ulcers → gangrene |
| 🧫 Infection | Chronic osteomyelitis or sepsis unresponsive to antibiotics |
| 🔥 Malignancy | Bone or soft tissue tumors (e.g., osteosarcoma) requiring radical excision |
| 🧬 Congenital Deformities | Nonfunctional or malformed limbs |
🚧 B. Traumatic Causes
| Cause | Description |
|---|---|
| 🚗 Road traffic accidents | High-impact injuries with irreparable damage |
| 🛠️ Industrial or agricultural accidents | Machinery or heavy equipment trauma |
| 🔫 War or blast injuries | Landmines, gunshots, or explosions |
| 🐍 Severe animal or snake bites | Leading to necrosis or infection |
🔷 3. TYPES OF AMPUTATION
Amputations can be classified based on level, site, and urgency:
✅ A. Based on Site/Body Part
| Type | Description |
|---|---|
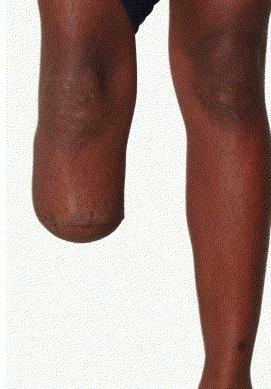
| 🦶 Toe/Finger Amputation | Common in diabetic foot or frostbite |
| 🦵 Below-Knee Amputation (BKA) | Retains knee joint; easier rehabilitation |
| 🦿 Above-Knee Amputation (AKA) | More disabling; prosthetic fitting is more complex |
| ✋ Below-Elbow Amputation (BEA) | Preserves elbow function |
| 💪 Above-Elbow Amputation (AEA) | Complete arm loss up to shoulder |
| 🧍♂️ Disarticulation | Amputation through a joint (e.g., hip or shoulder disarticulation) |
| 🦴 Hemipelvectomy | Removal of entire leg + part of pelvis |
| 💀 Facial/Organ Amputation | Rare, includes eye enucleation, breast mastectomy (sometimes categorized as amputations in extended sense) |
✅ B. Based on Urgency
| Type | Description |
|---|---|
| ⏱️ Emergency Amputation | Performed to save life (e.g., gangrene, crush injury with infection) |
| 🗓️ Elective Amputation | Planned and scheduled; often for chronic conditions (e.g., cancer, PVD) |
✅ C. Based on Method
| Method | Description |
|---|---|
| ✂️ Open (Guillotine) Amputation | Done rapidly without skin closure (infection or emergency); later followed by closure |
| 🧵 Closed (Flap) Amputation | Performed with skin flap creation and primary wound closure |
📌 Summary Table
| Classification | Types |
|---|---|
| By site | Toe, foot, BKA, AKA, upper limb |
| By urgency | Emergency, Elective |
| By method | Open (Guillotine), Closed (Flap) |
| By cause | Surgical (disease/infection), Traumatic (accident/injury) |
🔬 1. PATHOPHYSIOLOGY OF AMPUTATION
Amputation is the removal of a part of the body, typically due to irreversible tissue damage, ischemia, trauma, or infection. Whether surgical or traumatic, the physiological process involves the following steps:
🧠 Pathophysiological Sequence (Surgical Amputation)
- Initial insult (e.g., ischemia, trauma, infection, tumor) causes tissue death or non-viability.
- Progressive necrosis or infection spreads if untreated.
- To prevent systemic complications (like sepsis), surgical removal of the non-viable part is planned.
- In surgery:
- Blood vessels are ligated (tied off)
- Muscles are cut or sutured
- Nerves are sealed or trimmed to prevent neuroma
- Skin flaps are used to cover the stump
- Post-amputation, the body initiates:
- Wound healing
- Scar formation
- Possible neuroma or phantom limb development
⚠️ Traumatic Amputation Pathophysiology
- Sudden force/trauma severs the limb/tissue.
- Leads to hemorrhage, shock, pain, and inflammation.
- Requires urgent control of bleeding, wound decontamination, and possible re-amputation or revision surgery.
🚨 2. SIGNS AND SYMPTOMS (PRE and POST-AMPUTATION)
✅ Before Amputation (Indications for Surgery)
| Symptom | Cause |
|---|---|
| ❌ Non-healing wound or ulcer | Common in diabetics/PVD patients |
| 🖤 Gangrene or necrosis | Dead, blackened tissue |
| 😷 Severe infection (e.g., osteomyelitis) | Not responding to treatment |
| ⚠️ Uncontrolled pain | In ischemic limb |
| 💢 Loss of function or sensation | From irreversible nerve/muscle damage |
| 🧊 Cold, pulseless extremity | Poor circulation (ischemia) |
✅ After Amputation
| Symptom | Description |
|---|---|
| 🔺 Postoperative pain | Due to surgical trauma and healing |
| 🧠 Phantom limb sensations | Feeling the presence of removed limb (normal, may or may not be painful) |
| 😖 Stump swelling, redness | Normal inflammatory response |
| 🩸 Drainage from surgical site | Should decrease over time |
| 🦿 Mobility limitations | Requires rehab and prosthetic fitting |
| 😔 Emotional disturbance | Body image issues, grief, anxiety, depression common |
🧪 3. DIAGNOSTIC EVALUATION
Used to evaluate the need for amputation and plan surgical site.
🧫 A. Laboratory Tests
| Test | Purpose |
|---|---|
| 🩸 CBC | Detects infection (↑WBC) or anemia |
| 💉 Blood glucose, HbA1c | Uncontrolled diabetes is a major risk factor |
| 🧪 Coagulation profile (PT, INR, aPTT) | Especially important before surgery |
| 🧫 Wound culture | Identifies infecting organisms in ulcers or gangrene |
| 🧪 Serum creatinine/urea | Kidney function if sepsis or diabetic nephropathy present |
🩻 B. Imaging Studies
| Imaging | Purpose |
|---|---|
| 🧲 Doppler Ultrasound | Assesses blood flow to the limb |
| 🧠 Arteriography/Angiography | Shows vascular occlusion or stenosis |
| 🧱 X-ray | Identifies bone destruction or gas gangrene |
| 🧠 MRI/CT Scan | Determines extent of soft tissue and bone involvement |
| 📸 Bone Scan | Detects osteomyelitis or bone death |
📌 Summary Table
| Aspect | Key Points |
|---|---|
| Pathophysiology | Tissue necrosis due to ischemia/infection → removal prevents systemic spread |
| Pre-op Symptoms | Gangrene, non-healing ulcer, infection, loss of function |
| Post-op Symptoms | Pain, swelling, phantom limb sensation, mobility issues |
| Diagnosis | Labs for infection/metabolism, imaging for vascular & bone status |
🔷 I. MEDICAL MANAGEMENT
(Pre-operative and Post-operative supportive care)
Medical management focuses on preparing the patient, treating the underlying condition, and supporting recovery post-amputation.
✅ A. Pre-operative Medical Care
| Intervention | Purpose |
|---|---|
| 💉 Control of underlying disease | – Diabetes: insulin, oral hypoglycemics |
- PVD: antiplatelets, vasodilators | |
- 🧫 Infection control | Broad-spectrum or culture-specific antibiotics for infected wounds or osteomyelitis | |
- 💊 Pain management | NSAIDs or opioids for ischemic or neuropathic pain | |
- 🩸 Hemodynamic stabilization | IV fluids, blood transfusions in case of bleeding/anemia | |
- 🧠 Psychological preparation | Counseling, patient education to reduce anxiety & depression | |
- 📝 Pre-anesthetic evaluation | Ensure patient is fit for anesthesia (CBC, ECG, renal function) | |
- 🧼 Wound and skin care | Clean, dress, and protect compromised skin and ulcers |
✅ B. Post-operative Medical Care
| Care Component | Description |
|---|---|
| 💊 Pain control | Opioids, NSAIDs, PCA pumps as needed |
| 🧠 Phantom limb pain management | Gabapentin, antidepressants, mirror therapy, TENS |
| 💧 Fluid and electrolyte balance | Monitor I&O, hydration |
| 🧫 Infection prevention | Continue IV/oral antibiotics as needed |
| 🩹 Wound care | Monitor for drainage, infection, and healing progress |
| 🍽️ Nutritional support | High-protein, vitamin C & zinc-rich diet for wound healing |
| 🧍 Rehabilitation referral | For physiotherapy and prosthetic planning |
🔶 II. SURGICAL MANAGEMENT
Surgical management of amputation involves the removal of non-viable tissue and preparation of the stump for future prosthetic fitting or healing.
✅ A. Goals of Surgery
- Remove infected, gangrenous, ischemic, or cancerous tissue
- Create a functional, prosthesis-ready stump
- Prevent complications (bleeding, infection, neuroma)
- Preserve maximum limb length and joint mobility
✅ B. Types of Surgical Amputation
| Type | Description |
|---|---|
| ✂️ Open (Guillotine) Amputation | – Skin is left open |
- Used in infected or emergency cases
- Followed later by closure | | 🧵 Closed (Flap) Amputation | – Skin and soft tissue are sutured over the bone
- Preferred in elective surgeries with clean margins |
✅ C. Surgical Techniques
| Procedure | Purpose |
|---|---|
| 🔩 Blood vessel ligation | Prevent bleeding |
| ✂️ Nerve retraction/trimming | Prevent painful neuroma formation |
| 🧵 Muscle shaping (myoplasty or myodesis) | Anchor muscles to allow mobility and shape |
| 🔧 Bone beveling | Smooth edges of the cut bone to prevent sharp edges or stump pain |
| 🧼 Drain placement | Prevent accumulation of fluid or hematoma |
✅ D. Special Surgical Types
| Procedure | Indication |
|---|---|
| 🦿 Below-Knee Amputation (BKA) | Most common; preserves knee for mobility |
| 🦵 Above-Knee Amputation (AKA) | Used when tissue damage extends above knee |
| 💪 Upper limb amputations | Less common; used in trauma, tumors |
| 🔄 Disarticulations | Through-joint removal (e.g., hip, shoulder) |
| 🦴 Hemipelvectomy / Forequarter amputation | Radical surgeries for malignancies |
📌 Summary Chart
| Management Type | Key Interventions |
|---|---|
| Medical (Pre-op) | Manage diabetes, infection, pain, nutrition, counseling |
| Medical (Post-op) | Pain control, wound care, fluid balance, rehab |
| Surgical (Open/Closed) | Remove diseased tissue, shape stump, prevent complications |
🧑⚕️🦿 Nursing Management of Amputation
🎯 Goals of Nursing Care
✅ Prevent infection and complications
✅ Promote wound healing
✅ Relieve pain, including phantom limb pain
✅ Restore mobility and independence
✅ Support psychological adjustment
✅ Educate for self-care and rehabilitation
🔷 I. NURSING ASSESSMENT
Perform both pre-operative and post-operative assessments:
🩺 Pre-Operative Assessment
| Focus Area | Assessment |
|---|---|
| 🔢 Vitals | Monitor BP, HR, temperature (signs of infection or shock) |
| 🧫 Wound/infection status | Gangrene, ulcers, discharge, odor |
| 🔋 Nutritional status | Protein, vitamin levels, albumin |
| 🧠 Emotional response | Anxiety, denial, depression |
| 💊 Comorbidities | Diabetes, PVD, renal function, cardiovascular risk |
🩹 Post-Operative Assessment
| Parameter | Description |
|---|---|
| 👁️ Stump | Inspect for bleeding, swelling, drainage, dressing condition |
| 🩸 Neurovascular check | Check circulation and sensation in remaining limb |
| 🧠 Phantom limb sensation/pain | Assess for burning, tingling, or pain in missing limb |
| 💢 Pain | Type, location, severity (surgical vs phantom) |
| 🧑🦯 Mobility | Ability to sit, stand, transfer, and use assistive devices |
| 🧠 Mental health | Grief reaction, body image disturbance, coping mechanisms |
📝 II. COMMON NURSING DIAGNOSES
- Acute Pain related to surgical incision, muscle spasm, phantom pain
- Risk for Infection related to surgical wound or poor hygiene
- Impaired Physical Mobility related to loss of limb
- Disturbed Body Image related to amputation
- Grieving related to loss of body part
- Self-care Deficit related to impaired mobility
- Risk for Impaired Skin Integrity related to pressure on remaining limb or prosthesis use
🧑⚕️ III. NURSING INTERVENTIONS
💊 1. Pain Management
- Administer prescribed analgesics and anti-inflammatory drugs
- Use mirror therapy, TENS, or massage for phantom limb pain
- Encourage relaxation techniques, distraction, and guided imagery
🧼 2. Wound and Stump Care
- Inspect wound daily for signs of infection or hematoma
- Perform dressing changes using aseptic technique
- Keep stump clean, dry, and elevated (first 24–48 hours)
- Shape the stump using compression bandage or shrinker socks
🧠 3. Emotional & Psychological Support
- Encourage expression of feelings
- Provide empathy and active listening
- Involve counseling or psychiatric referral as needed
- Support participation in peer support groups or amputee networks
🦿 4. Promote Mobility and Rehabilitation
- Encourage early use of assistive devices (crutches, walker, wheelchair)
- Collaborate with physiotherapists and prosthetists
- Begin ROM and strengthening exercises for unaffected limbs
- Teach safe transfer techniques and fall prevention
🧑🎓 5. Patient and Family Education
- Teach stump care and signs of infection
- Instruct on use of prosthesis (when ready)
- Educate on nutritional support for healing
- Discuss home modifications for safety and mobility
📈 IV. EVALUATION / EXPECTED OUTCOMES
| Goal | Expected Outcome |
|---|---|
| ✅ Pain Relief | Patient reports manageable or no pain |
| ✅ Wound Healing | Stump heals without signs of infection |
| ✅ Improved Mobility | Patient ambulates with assistive device or prosthesis |
| ✅ Body Image Acceptance | Patient participates in care, accepts self-image |
| ✅ Emotional Recovery | Patient expresses feelings and demonstrates coping |
| ✅ Independence | Performs ADLs with/without assistance |
📌 V. KEY REMINDERS FOR NURSES
✔️ Always perform neurovascular checks on the remaining limb
✔️ Early rehabilitation = better long-term outcomes
✔️ Phantom limb pain is real – validate and manage it
✔️ Holistic care includes emotional, physical, and educational support
✔️ Encourage positive reinforcement and patient empowerment
🔶 I. COMPLICATIONS OF AMPUTATION
Complications can be physical, psychological, or prosthetic-related, and may occur early (acute) or late (chronic).
🩺 A. Early (Immediate/Postoperative) Complications
| Complication | Description |
|---|---|
| 🩸 Hemorrhage | Bleeding from surgical site or major vessel |
| 🧫 Infection | Common in open wounds or diabetic patients |
| 💥 Wound Dehiscence | Surgical site reopens due to poor healing or tension |
| 🔥 Hematoma | Accumulation of blood under the flap or stump |
| 🧠 Phantom Limb Pain (PLP) | Painful sensation in the missing limb; can be sharp, burning, or cramping |
| ⚠️ Stump Edema | Swelling due to inflammation or improper positioning |
| 💧 Shock | From blood loss or sepsis (especially in trauma cases) |
🧠 B. Late (Chronic) Complications
| Complication | Description |
|---|---|
| 🔁 Phantom Limb Sensation | Non-painful sensation of the missing limb (normal, not harmful) |
| ❌ Chronic Stump Pain | Due to neuroma formation or scar tissue |
| 🧬 Neuroma | Painful nerve-end growth at stump site |
| 💢 Contractures | Muscle shortening due to poor positioning or lack of mobility (e.g., hip/knee flexion contracture) |
| 🧼 Prosthetic Complications | Poor fit, skin irritation, breakdown, pressure sores |
| 😞 Psychological Issues | Depression, anxiety, PTSD, body image disturbance |
| ⚖️ Imbalance/Decreased Mobility | Leads to falls, pressure injuries, and deconditioning |
📌 II. KEY POINTS TO REMEMBER
🧠 Use these high-yield points for clinical practice and quick exam revision:
✅ Amputation = removal of part or whole limb due to infection, trauma, ischemia, or malignancy
✅ Common indications: PVD, diabetes, osteomyelitis, trauma
✅ BKA (Below Knee Amputation) has better rehab outcomes than AKA (Above Knee)
✅ Open (guillotine) amputation is for infection/emergency; closed (flap) is planned/elective
✅ Monitor for phantom limb pain and neuroma – treat with meds, mirror therapy, or TENS
✅ Post-op care includes stump positioning, compression, ROM exercises, and wound inspection
✅ Start early rehabilitation with physiotherapy and prosthetic consultation
✅ Provide emotional support and counseling to address grief and altered body image
✅ Long-term success depends on nutritional support, infection control, education, and rehab
✅ Nurses play a vital role in promoting stump care, mobility, psychological support, and independence.
🦴🧫 Musculoskeletal Infections:

🔷 1. DEFINITION
Musculoskeletal infections refer to infections involving the bones, joints, muscles, or surrounding soft tissues. These infections may be acute or chronic, and they can be localized or spread systemically.
🧠 Commonly affected areas: bones (osteomyelitis), joints (septic arthritis), muscles (pyomyositis), and soft tissues (cellulitis, abscesses).
🔬 2. TYPES OF MUSCULOSKELETAL INFECTIONS
| Type | Description |
|---|---|
| Osteomyelitis | Infection of the bone and bone marrow (acute or chronic) |
| Septic Arthritis | Infection of the synovial joint space, often rapid and destructive |
| Pyomyositis | Suppurative bacterial infection of skeletal muscles |
| Tenosynovitis | Inflammation of tendon sheath due to infection |
| Bursitis | Infected bursa (fluid-filled sacs near joints) |
| Necrotizing Fasciitis | Rapidly spreading infection of muscle fascia and soft tissue (life-threatening) |
🔶 3. CAUSES / ETIOLOGY
✅ Infectious Organisms
| Organism | Example of Conditions |
|---|---|
| Bacteria (most common) | Staphylococcus aureus (most common), Streptococcus, Pseudomonas, Mycobacterium tuberculosis |
| Viruses | Hepatitis, HIV-related arthropathy |
| Fungi | Candida, Aspergillus (immunocompromised patients) |
| Mycobacteria | Tuberculous osteomyelitis or TB arthritis |
✅ Routes of Infection
- Hematogenous spread (via blood) – especially in children
- Direct inoculation – trauma, surgery, injections
- Contiguous spread – from nearby infections (e.g., diabetic ulcer, cellulitis)
- Post-operative or prosthesis-related infections
🔬 4. PATHOPHYSIOLOGY
- Pathogen enters musculoskeletal tissue via bloodstream, trauma, or surgery
- Causes local inflammation → neutrophil infiltration
- In bones: pus accumulates in marrow, increasing pressure and cutting off blood supply
- Bone necrosis (sequestrum) develops → may form chronic infection
- In joints: synovial membrane inflamed → cartilage destruction
- Muscles: abscess formation can lead to fibrosis or systemic spread
🚨 5. SIGNS AND SYMPTOMS
✅ General Symptoms
- 🌡️ Fever and chills
- 🤒 Malaise, fatigue
- 💧 Sweating
- 📉 Weight loss (chronic cases)
✅ Localized Symptoms (Site-specific)
| Site | Symptoms |
|---|---|
| Bone (Osteomyelitis) | Deep, dull pain, tenderness, swelling, erythema, reduced ROM |
| Joint (Septic Arthritis) | Red, swollen, warm joint, intense pain, inability to move joint |
| Muscle (Pyomyositis) | Muscle tenderness, firm mass, warmth, difficulty in movement |
| Soft Tissue | Redness, warmth, swelling, sometimes pus or open wound |
🧪 6. DIAGNOSTIC EVALUATION
✅ Laboratory Tests
| Test | Purpose |
|---|---|
| 🔬 CBC | ↑ WBC count (infection indicator) |
| 🧪 CRP, ESR | Elevated in inflammation |
| 🧫 Blood cultures | Identify causative organism |
| 💉 Joint aspiration / Wound culture | Direct sample of infected site |
| 🔬 Procalcitonin | Marker of bacterial infection |
| 🧪 TB test (Mantoux, GeneXpert) | If tubercular infection suspected |
✅ Imaging Studies
| Test | Use |
|---|---|
| 🩻 X-ray | Bone destruction or sequestrum in chronic osteomyelitis |
| 🧲 MRI | Soft tissue, early infection, joint effusion |
| 🧠 CT Scan | Abscess location, bony involvement |
| 🧪 Bone Scan (Radionuclide) | Detects early osteomyelitis |
| 📸 Ultrasound | Joint effusion or soft tissue abscesses |
💊 7. MEDICAL MANAGEMENT
✅ Antibiotic Therapy (First Line)
- Empiric broad-spectrum IV antibiotics initially
- Modified according to culture/sensitivity
- Typical duration:
- 4–6 weeks for bone infections
- 2–4 weeks for joint or soft tissue
Common antibiotics used:
- Vancomycin
- Ceftriaxone
- Piperacillin-Tazobactam
- Clindamycin
- Linezolid (for MRSA)
✅ Supportive Care
- Analgesics – Paracetamol, NSAIDs for pain relief
- Antipyretics – Fever management
- Nutritional support – Protein-rich diet
- Hydration – Especially in fever or systemic infection
🛠️ 8. SURGICAL MANAGEMENT
| Procedure | Indication |
|---|---|
| Surgical debridement | Removal of necrotic tissue or abscess |
| Incision & drainage | Large abscesses or purulent joints |
| Bone drilling / resection | In chronic osteomyelitis |
| Arthrotomy | Joint washout in septic arthritis |
| Amputation | Severe, life-threatening infection unresponsive to treatment |
| Implant removal | If prosthetic joint or hardware is infected |
🧑⚕️ 9. NURSING MANAGEMENT
- Monitor vital signs, especially fever and heart rate
- Perform wound care with sterile technique
- Administer and monitor IV antibiotics
- Pain assessment and management
- Encourage mobility as tolerated (to prevent stiffness or DVT)
- Provide psychological support
- Educate patient on medication adherence, hygiene, and follow-up care
⚠️ 10. COMPLICATIONS
| Complication | Description |
|---|---|
| 🦴 Chronic osteomyelitis | Persistent bone infection requiring surgery |
| 🛏️ Septicemia | Systemic infection (life-threatening) |
| 🔁 Joint destruction/deformity | In septic arthritis |
| 🧬 Pathological fracture | Weakened bone breaks |
| 🚑 Amputation | If severe or unmanageable |
| 😔 Functional disability | Limited mobility or joint function |
| 💊 Antibiotic resistance | Due to incomplete treatment or inappropriate use |
📌 11. KEY POINTS TO REMEMBER
✅ Musculoskeletal infections can affect bones, joints, or muscles
✅ Most are bacterial, especially Staph aureus
✅ Early symptoms include pain, swelling, fever, limited movement
✅ Diagnosis via labs + imaging + cultures
✅ Management includes long-term antibiotics ± surgery
✅ Nurses play a key role in medication adherence, wound care, and rehabilitation
✅ Prompt diagnosis and aggressive treatment are critical to prevent permanent damage or systemic spread
🦴🧫 OSTEOMYELITIS:

🔷 1. DEFINITION
Osteomyelitis is a serious infection of the bone and bone marrow, most commonly caused by bacteria (especially Staphylococcus aureus), but also by fungi or mycobacteria. It leads to inflammation, pus formation, bone destruction, and, if untreated, can cause permanent bone damage or systemic infection.
🧠 Osteo = bone, Myelo = marrow, Itis = inflammation
Osteomyelitis = infection and inflammation of bone + marrow
🔶 2. CAUSES OF OSTEOMYELITIS
Osteomyelitis occurs when infectious organisms reach the bone through one of the following routes:
✅ A. Hematogenous Spread (via bloodstream)
- Most common in children
- Source: urinary tract infection, respiratory infection, dental abscess
- Infection spreads to long bones (femur, tibia, humerus)
✅ B. Contiguous Spread (from nearby infection)
- Common in adults
- Occurs from infected wounds, ulcers (e.g., diabetic foot), cellulitis, or dental infections
- Seen in patients with trauma, joint replacement, or open fractures
✅ C. Direct Inoculation
- Through open fractures, surgical procedures, orthopedic implants, or puncture wounds
- Common in trauma or post-operative infections
✅ D. Other Contributing Factors
| Risk Factor | Mechanism |
|---|---|
| 😷 Diabetes mellitus | Poor wound healing, neuropathy, and increased infection risk |
| 🚬 Peripheral vascular disease (PVD) | Reduced blood flow to bone |
| 🔬 Immunosuppression (e.g., HIV, chemotherapy) | Decreased ability to fight infection |
| ⚙️ Presence of foreign body (e.g., joint prosthesis) | Surface for bacteria to colonize |
| 🧒 Sickle cell disease | Predisposes to Salmonella osteomyelitis |
🔷 3. TYPES OF OSTEOMYELITIS
✅ A. Based on Duration
| Type | Description |
|---|---|
| Acute Osteomyelitis | – Develops quickly (within 2 weeks of infection) |
- Common in children
- Symptoms: severe pain, fever, swelling, redness | | Chronic Osteomyelitis | – Long-standing infection (≥1 month)
- May follow untreated acute infection
- Involves necrotic bone (sequestrum)
- Associated with sinus tracts, poor wound healing |
✅ B. Based on Route of Infection
| Type | Description |
|---|---|
| Hematogenous | Infection spread through blood — common in children |
| Contiguous-focus | Spread from nearby infected tissue (e.g., ulcers, trauma) — common in adults |
| Direct Inoculation | Post-surgical, penetrating injury, or open fracture |
✅ C. Specific Clinical Forms
| Type | Description |
|---|---|
| Vertebral Osteomyelitis | Common in adults; often hematogenous; causes back pain, fever |
| Diabetic Foot Osteomyelitis | Seen in long-standing diabetics with foot ulcers |
| Prosthetic Joint Infection | Infection around an implanted joint; may require removal of prosthesis |
| Tuberculous Osteomyelitis | Caused by Mycobacterium tuberculosis, often affects spine (Pott’s disease) |
📌 SUMMARY TABLE
| Classification | Examples |
|---|---|
| By duration | Acute, Chronic |
| By spread | Hematogenous, Contiguous, Direct inoculation |
| By site | Vertebrae, long bones, diabetic foot |
| By organism | Bacterial (Staph, Salmonella), TB, Fungal |
🔬 1. PATHOPHYSIOLOGY OF OSTEOMYELITIS
Osteomyelitis begins with microbial invasion of the bone, leading to inflammation, necrosis, and progressive bone destruction if not treated early.
🔄 Step-by-Step Pathophysiology:
- Infectious agent enters the bone via:
- Bloodstream (hematogenous spread)
- Direct inoculation (injury, surgery)
- Contiguous tissue spread (e.g., infected ulcer)
- Bacteria multiply rapidly in the bone marrow cavity.
- Local inflammation occurs → neutrophils and inflammatory cells migrate to the site.
- Pus formation increases intraosseous pressure, compressing blood vessels.
- ↓ Blood supply → ischemia and necrosis of bone.
- Dead bone = sequestrum → becomes a reservoir for bacteria.
- Body attempts healing by forming involucrum (new bone over sequestrum), trapping infection.
- In chronic cases, sinus tracts may form, draining pus through the skin.
🚨 2. SIGNS AND SYMPTOMS
The presentation depends on whether the condition is acute or chronic, and whether it affects children or adults.
🟠 Acute Osteomyelitis (Common in children)
| Sign/Symptom | Description |
|---|---|
| 🌡️ High fever and chills | Often > 38.5°C |
| 💢 Severe localized bone pain | Worsens with movement |
| 🔴 Swelling and redness | Over the infected bone |
| 🔥 Warmth over area | Due to inflammation |
| 🚫 Limited movement | Of nearby joints or limb |
| 😴 Fatigue, malaise | Systemic symptoms present |
🔵 Chronic Osteomyelitis (Common in adults)
| Sign/Symptom | Description |
|---|---|
| 📉 Low-grade fever or may be absent | |
| 💧 Persistent drainage | From sinus tract or wound |
| ⚠️ Localized dull pain | Intermittent or constant |
| 🦴 Deformity or swelling | Over affected bone |
| ❌ Non-healing wound or ulcer | Often over bony prominence |
| 🧬 History of previous infection, trauma, or surgery |
⚠️ Special Site Symptoms
| Site | Symptoms |
|---|---|
| Vertebral | Back pain, neurological deficits (if spinal cord compression) |
| Foot (diabetics) | Swelling, warmth, ulcer, foul odor, little to no pain (due to neuropathy) |
🧪 3. DIAGNOSTIC EVALUATION
A combination of clinical signs, laboratory markers, imaging, and microbiological tests is used to confirm osteomyelitis.
✅ A. Laboratory Investigations
| Test | Purpose |
|---|---|
| 🩸 CBC (WBC Count) | ↑ WBC in acute infection |
| 🧪 ESR / CRP | Elevated in both acute and chronic infections |
| 💉 Blood cultures | Identify causative organisms (positive in hematogenous spread) |
| 🧫 Wound/pus culture | For antibiotic sensitivity testing |
| 🧬 Procalcitonin (PCT) | Elevated in severe bacterial infection |
| 🔬 Bone biopsy (gold standard) | Confirms diagnosis & identifies organism directly from bone tissue |
✅ B. Imaging Studies
| Imaging | Role |
|---|---|
| 🩻 X-ray | May show bone changes (late: after 10–14 days) – lytic areas, sequestrum |
| 🧠 MRI (Best for early diagnosis) | Shows marrow edema, abscess, soft tissue involvement |
| 🧲 CT Scan | Detailed bony architecture, useful in surgical planning |
| ☢️ Bone Scan (Technetium-99) | Detects early changes – highly sensitive but less specific |
| 📸 Ultrasound | Useful for detecting subperiosteal abscesses or joint effusions |
📌 Quick Summary Table
| Category | Key Points |
|---|---|
| Pathophysiology | Infection → inflammation → pus → pressure → necrosis → chronic sequestrum |
| Acute Symptoms | Fever, pain, swelling, redness, immobility |
| Chronic Symptoms | Draining sinus, dull pain, deformity, intermittent swelling |
| Diagnosis | CBC, ESR, CRP, MRI, bone biopsy, cultures |
🔷 I. MEDICAL MANAGEMENT
The primary goal of medical treatment is to eradicate infection, preserve bone integrity, and prevent complications like chronic infection or amputation.
✅ A. Antibiotic Therapy (Cornerstone of Treatment)
| Phase | Approach |
|---|---|
| Empirical Phase | Start broad-spectrum IV antibiotics immediately (before culture reports) |
| Targeted Phase | Switch to culture-specific antibiotics once sensitivity results are available |
🧪 Common IV Antibiotics Used
| Organism | Drugs |
|---|---|
| Staphylococcus aureus (MSSA) | Cloxacillin, Nafcillin, Cefazolin |
| MRSA | Vancomycin, Linezolid, Daptomycin |
| Gram-negative bacteria | Ciprofloxacin, Ceftriaxone, Piperacillin-Tazobactam |
| Anaerobes | Metronidazole, Clindamycin |
| Tubercular osteomyelitis | Anti-tubercular therapy (ATT) for 9–12 months |
🔁 Duration of Antibiotic Therapy
- Acute osteomyelitis: 4–6 weeks
- Chronic osteomyelitis: ≥6 weeks (may need oral continuation)
✅ B. Adjunct Medical Treatments
| Treatment | Purpose |
|---|---|
| 💊 NSAIDs or acetaminophen | Pain and inflammation control |
| 💉 IV fluids | Maintain hydration in febrile patients |
| 🍽️ High-protein, high-calorie diet | Promotes tissue repair |
| 🧬 Glycemic control (in diabetics) | Prevents progression and recurrence |
| ⚠️ Bed rest and limb elevation | In acute phase to reduce swelling |
| 🧦 Immobilization (splint or cast) | Reduces pain, promotes healing |
🔶 II. SURGICAL MANAGEMENT
Surgery is required when there is:
- Necrotic bone (sequestrum)
- Abscess or sinus tract formation
- Failure of medical therapy
- Chronic osteomyelitis
- Prosthetic joint infection
🔧 Common Surgical Procedures
| Procedure | Indication |
|---|---|
| 🧼 Surgical Debridement | Removal of necrotic bone (sequestrum), pus, and infected tissue |
| 💉 Incision and Drainage (I&D) | Abscess or pus collection in soft tissues or bone |
| 🦴 Sequestrectomy | Specific removal of dead bone |
| 🛠️ Curettage | Scraping out infected cavity in bone |
| 🦿 Implant removal or replacement | In prosthetic joint infections |
| 🧱 Bone grafting | Fills cavity after debridement to promote healing |
| 🦿 Amputation | Last resort in uncontrolled infection or gangrene |
🧩 Advanced Options
| Option | Use |
|---|---|
| 💉 Antibiotic-impregnated beads | Local antibiotic delivery at surgical site |
| 🧬 Negative Pressure Wound Therapy (NPWT) | Enhances drainage and healing in large wounds |
| 🔁 Ilizarov or external fixation | For infected non-union or deformity correction |
📌 Summary Table
| Management Type | Key Components |
|---|---|
| Medical | IV antibiotics, pain relief, nutrition, glycemic control |
| Surgical | Debridement, drainage, sequestrectomy, grafting, prosthesis revision |
🧑⚕️🦴 Nursing Management of Osteomyelitis
🎯 Nursing Goals
✅ Relieve pain
✅ Prevent the spread of infection
✅ Promote healing of bone and soft tissue
✅ Support mobility and function
✅ Educate patient for self-care and long-term management
🔷 I. NURSING ASSESSMENT
Perform continuous and focused assessments on:
| Category | What to Assess |
|---|---|
| 🔺 Pain | Type, intensity, duration (before and after intervention) |
| 🌡️ Fever | Monitor temperature and signs of systemic infection |
| 🔬 Wound/Site | Look for redness, swelling, warmth, drainage, odor |
| 🧫 Labs | Monitor WBC, CRP, ESR trends |
| 🦶 Mobility | Ability to bear weight, joint stiffness, limb use |
| 💊 Antibiotic effects | Side effects, signs of allergy or superinfection |
| 🧠 Psychosocial status | Anxiety, depression, coping with chronic illness |
| 📋 Adherence | Understanding of long-term antibiotic therapy and follow-up needs |
📝 II. COMMON NURSING DIAGNOSES
- Acute pain related to inflammation and infection of bone
- Impaired physical mobility related to pain, weakness, or immobilization
- Risk for infection (spread/systemic) related to bacterial invasion
- Ineffective tissue perfusion related to edema, pressure, or vascular compromise
- Deficient knowledge related to disease process, medication regimen, or wound care
- Risk for impaired skin integrity related to immobility or surgical intervention
- Anxiety or fear related to prolonged illness and potential disability
🩺 III. NURSING INTERVENTIONS
💊 1. Infection Control
- Administer prescribed IV antibiotics on time, and monitor for adverse effects
- Use aseptic technique during dressing changes and wound care
- Monitor drainage characteristics (amount, color, odor)
- Report any signs of worsening infection or sepsis
🧊 2. Pain Management
- Assess pain level regularly using pain scales
- Administer analgesics and antipyretics as prescribed
- Encourage limb elevation and rest
- Apply cold compresses (if ordered) during acute pain phase
🛌 3. Mobility Support
- Encourage bed rest in the acute stage
- Assist with positioning and splinting of the affected limb
- Promote gentle range-of-motion exercises to prevent stiffness
- Refer to physiotherapy for long-term rehabilitation
🧼 4. Wound and Skin Care
- Assess surgical site or sinus tracts for signs of healing or breakdown
- Perform regular sterile dressing changes
- Prevent pressure injuries by turning schedule and skin checks
🧠 5. Patient Education
- Teach the importance of completing the full course of antibiotics
- Educate on signs of re-infection: fever, drainage, new pain
- Instruct on wound care, hygiene, and nutrition
- Explain possible need for follow-up imaging or surgery
- Encourage mobility with assistive devices if needed
💬 6. Psychosocial & Emotional Support
- Allow expression of fears and anxieties
- Encourage family involvement in care
- Refer to counselor or support group for chronic cases
📈 IV. EVALUATION: EXPECTED OUTCOMES
| Goal | Expected Result |
|---|---|
| ✅ Infection is controlled | Normal temperature, ↓ WBC, ↓ ESR/CRP, no purulent discharge |
| ✅ Pain is relieved | Patient verbalizes comfort and uses less analgesia |
| ✅ Mobility improves | Participates in physiotherapy or ADLs |
| ✅ Knowledge gained | Demonstrates wound care and understands treatment plan |
| ✅ No complications | Skin remains intact, no signs of systemic spread |
📌 V. KEY NURSING POINTS TO REMEMBER
✔️ Osteomyelitis requires prolonged IV antibiotics (4–6 weeks or more)
✔️ Early surgical debridement may be necessary to remove necrotic bone
✔️ Strict asepsis is critical to prevent secondary infections
✔️ Multidisciplinary approach (physician, nurse, physiotherapist, pharmacist) improves outcomes
✔️ Long-term follow-up and patient adherence are essential to prevent relapse
🔶 I. COMPLICATIONS OF OSTEOMYELITIS
Osteomyelitis, if not treated early and effectively, can lead to serious local and systemic complications:
🟠 A. Local Complications
| Complication | Description |
|---|---|
| 🦴 Chronic Osteomyelitis | Persistent or recurrent infection with necrotic bone (sequestrum) and sinus formation |
| 💥 Bone Necrosis (Sequestrum) | Dead bone acts as a reservoir for infection |
| 🔁 Pathological Fracture | Bone becomes weakened and may break easily |
| ❌ Joint Destruction | In nearby joints due to spread of infection (especially in septic arthritis) |
| 🧬 Contractures and Stiffness | Due to prolonged immobility or inflammation |
| 🩸 Impaired Limb Growth (in children) | If epiphyseal plate is involved, may lead to deformity or limb length discrepancy |
| 🛌 Immobility-related Complications | Pressure sores, DVT, muscle wasting |
🔴 B. Systemic Complications
| Complication | Description |
|---|---|
| 🧫 Sepsis (Bacteremia) | Infection enters bloodstream → may become life-threatening |
| 💀 Septic Shock | Severe infection → hypotension, multi-organ failure |
| 🧠 Amyloidosis (chronic cases) | Protein build-up from chronic inflammation damages kidneys and other organs |
| 🦿 Amputation | May be necessary if infection is unresponsive to treatment or causes extensive tissue death |
📌 II. KEY POINTS TO REMEMBER
✅ Osteomyelitis = Infection of bone & marrow, often by Staphylococcus aureus
✅ Occurs via hematogenous spread, direct inoculation, or contiguous spread
✅ Acute type = rapid onset; chronic type = persistent with sinus and necrosis
✅ Diagnosis = labs (ESR, CRP, WBC) + MRI or bone scan + bone biopsy/culture
✅ IV antibiotics for 4–6 weeks minimum are essential
✅ Surgery is needed to remove sequestrum or drain abscesses
✅ Nurses must monitor pain, infection signs, mobility, and emotional health
✅ Educate on wound care, medication adherence, and nutrition
✅ Long-term follow-up prevents recurrence and disability
🦴🧬 Tumors of the Musculoskeletal System
(Benign vs. Malignant)
🔷 1. DEFINITION
- A musculoskeletal tumor is an abnormal growth arising from bone, cartilage, muscle, fat, connective tissue, or synovial tissues.
- It may be benign (non-cancerous) or malignant (cancerous).
🟢 2. BENIGN MUSCULOSKELETAL TUMORS
Benign tumors are non-invasive, slow-growing, and do not spread (no metastasis). However, they can cause pain, deformity, or compression.
✅ Common Benign Tumors:
| Tumor | Origin | Features |
|---|---|---|
| Osteochondroma | Bone + cartilage | Most common benign bone tumor; occurs near growth plates |
| Osteoid osteoma | Bone | Small, painful lesion (worse at night), common in young males |
| Enchondroma | Cartilage | Often affects hands/feet; may cause swelling or fracture |
| Giant Cell Tumor (GCT) | Epiphysis of long bones | May be locally aggressive; may recur if not fully excised |
| Lipoma | Fat tissue | Soft, painless mass in subcutaneous tissue |
| Myxoma | Muscle/connective tissue | Rare, slow-growing mass, painless |
🔴 3. MALIGNANT MUSCULOSKELETAL TUMORS
Malignant tumors are aggressive, can invade nearby structures, and often metastasize (spread to lungs, liver, brain, etc.).
✅ Common Malignant Tumors:
| Tumor | Origin | Features |
|---|---|---|
| Osteosarcoma | Bone (especially around knee) | Most common primary bone cancer; occurs in children/young adults; rapidly growing |
| Chondrosarcoma | Cartilage | Affects pelvis, femur, or ribs; occurs in older adults |
| Ewing Sarcoma | Bone marrow or soft tissue | Highly aggressive tumor in children; often affects pelvis or femur |
| Multiple Myeloma | Plasma cells (bone marrow) | Systemic malignancy; lytic bone lesions, anemia, renal failure |
| Rhabdomyosarcoma | Skeletal muscle | Rare soft tissue tumor in children; aggressive and fast-growing |
| Fibrosarcoma | Connective tissue | Often in thigh, knee, or retroperitoneum; can recur and spread |
🔁 4. KEY DIFFERENCES: BENIGN vs. MALIGNANT TUMORS
| Feature | Benign Tumor | Malignant Tumor |
|---|---|---|
| 🧬 Growth rate | Slow | Rapid |
| 🧠 Local invasion | None | Yes |
| 📤 Metastasis | No | Yes |
| 📍 Borders | Well-defined | Poorly defined, irregular |
| 📸 X-ray findings | Clear margins, sclerotic rim | Lytic lesions, cortical destruction |
| 😖 Pain | Often absent or mild | Present, severe, progressive |
| 🧪 Biopsy | Confirms benign cells | Shows atypical, cancerous cells |
| 🔄 Recurrence | Rare (if removed completely) | Common without complete treatment |
📌 Key Points to Remember
✅ Osteochondroma is the most common benign bone tumor
✅ Osteosarcoma and Ewing’s sarcoma are most common in children and adolescents
✅ Chondrosarcoma is common in middle-aged adults
✅ Multiple myeloma causes multiple lytic bone lesions
✅ MRI and biopsy are essential for diagnosis
✅ Treatment may include surgery, chemotherapy, radiation, or amputation (for malignant tumors)
✅ Nurses play a key role in symptom monitoring, pre/post-op care, pain relief, and emotional support
🔷 I. CAUSES (ETIOLOGY)
While many tumors are idiopathic (unknown cause), several risk factors and triggers are associated with musculoskeletal tumors:
| Factor | Description |
|---|---|
| 🧬 Genetic mutations | TP53 mutation (Li-Fraumeni syndrome), RB gene mutation (retinoblastoma) |
| 🧒 Age | Osteosarcoma & Ewing’s: children/adolescents |
| Chondrosarcoma: middle-aged to elderly | |
| ☢️ Radiation exposure | Prior radiation therapy increases tumor risk |
| 💉 Chronic infections | E.g., chronic osteomyelitis may lead to sarcoma |
| 🧫 Paget’s disease | Bone remodeling disorder, can turn malignant |
| 🧬 Inherited syndromes | Neurofibromatosis, Gardner’s syndrome, Li-Fraumeni |
| ⚠️ Chemical exposure | Vinyl chloride, arsenic, phenol (linked to sarcomas) |
🔶 II. SIGNS AND SYMPTOMS
| Symptom | Description |
|---|---|
| 💢 Localized pain | Persistent, deep, increases at night |
| 🦴 Swelling or mass | Painless at first; may become painful later |
| 🚷 Limited mobility | Tumor near joints may restrict movement |
| 💥 Pathological fractures | Bone weakened by tumor breaks easily |
| 🧠 Fever or fatigue | Common in Ewing sarcoma or systemic spread |
| 💧 Weight loss, night sweats | In malignant tumors |
| 🩸 Anemia or hypercalcemia | Seen in multiple myeloma or advanced bone cancers |
🔬 III. DIAGNOSTIC EVALUATION
| Test | Purpose |
|---|---|
| 📸 X-ray | Initial test; shows lytic/sclerotic lesions, periosteal reactions |
| 🧲 MRI | Defines soft tissue involvement, tumor extent |
| 🧠 CT Scan | Bony details, lung metastasis |
| 💉 Bone biopsy (Gold Standard) | Differentiates benign from malignant |
| 🧫 Bone scan | Detects active bone lesions (multiple or metastatic) |
| 🔬 Blood tests | ESR, CRP, ALP, calcium levels, LDH |
| 🧬 Genetic/molecular testing | For specific sarcomas (e.g., Ewing’s translocation t(11;22)) |
🔁 IV. PATHOPHYSIOLOGY (Generalized Overview)
Benign Tumors:
- Arise from uncontrolled proliferation of localized bone or soft tissue cells.
- Grow slowly, remain well-circumscribed, and do not metastasize.
- May compress surrounding tissues or cause deformity if large.
Malignant Tumors:
- Begin as genetic mutations in bone/cartilage/muscle cells.
- Tumor cells grow uncontrollably → destroy normal bone architecture.
- Invade surrounding tissues and enter bloodstream/lymphatics.
- Metastasize, especially to lungs, liver, and brain.
- Bone destruction leads to pain, fractures, and systemic signs.
💊🛠️ V. MEDICAL & SURGICAL MANAGEMENT
💊 Medical Management
| Treatment | Purpose |
|---|---|
| 💉 Chemotherapy | Osteosarcoma, Ewing’s sarcoma (before and after surgery) |
| ⚛️ Radiation therapy | Ewing sarcoma, soft tissue sarcomas, unresectable tumors |
| 💊 Bisphosphonates | In metastatic bone lesions to prevent fractures |
| 💊 Targeted therapy | Denosumab for giant cell tumors; immunotherapy for soft tissue sarcomas |
| 💉 Pain management | NSAIDs, opioids for moderate to severe pain |
| 🍽️ Nutrition and hydration | High-calorie, protein-rich diet to support healing |
🛠️ Surgical Management
| Surgery | Indication |
|---|---|
| 🦴 Wide excision / Limb-sparing surgery | Remove tumor while preserving function |
| 🛑 Amputation | If tumor is extensive or involves major vessels/nerves |
| 🔄 Curettage + bone grafting | For benign tumors like enchondroma |
| 🧱 Internal fixation or joint replacement | If bone integrity is compromised |
| 🧼 Debulking surgery | In metastatic or palliative settings |
🧑⚕️ VI. NURSING MANAGEMENT
🩺 Assessment
- Monitor for pain, swelling, ROM, neurovascular status of affected limb
- Assess response to chemo/radiation
- Monitor lab results and wound healing post-op
- Watch for psychological impact (body image, fear, anxiety)
📝 Nursing Interventions
| Focus | Actions |
|---|---|
| 💊 Pain management | Administer analgesics, monitor effectiveness |
| 🧼 Wound care | Aseptic dressing, observe for infection |
| 🛌 Mobility support | Assist with ambulation, provide assistive devices |
| 🧠 Psychological care | Offer emotional support, involve counselors |
| 🧾 Education | Teach about medication adherence, wound care, follow-ups |
| 🧬 Monitor chemo/radiation side effects | Handle nausea, neutropenia, fatigue, mucositis |
| 🧦 Prevent complications | DVT prophylaxis, fall prevention, skin care |
📌 VII. KEY POINTS TO REMEMBER
✅ Musculoskeletal tumors can be benign or malignant
✅ Osteosarcoma & Ewing’s sarcoma are most common malignant tumors in children/adolescents
✅ X-ray, MRI, and biopsy are essential for diagnosis
✅ Chemotherapy + surgery is the mainstay for most bone cancers
✅ Early detection = better outcome
✅ Nurses must support physical, emotional, and rehabilitative needs of the patient
✅ Monitor for signs of metastasis, especially lung symptoms
✅ Encourage regular follow-up and nutritional support
🔷 ORTHOPEDIC TREATMENT MODALITIES FOR MUSCULOSKELETAL PROBLEMS
Musculoskeletal problems may include fractures, sprains, strains, arthritis, dislocations, infections, tumors, congenital deformities, and degenerative diseases. The goal of orthopedic treatment is to restore function, relieve pain, and prevent further injury or deformity.
🟩 1. Conservative (Non-Surgical) Treatment Modalities
These are the first-line treatments in many musculoskeletal conditions.
A. Rest and Immobilization
- Purpose: To prevent further injury, reduce inflammation, and allow healing.
- Methods: Bed rest, activity restriction, or immobilization using slings, splints, braces, or traction.
- Nursing Role: Monitoring for complications of immobility like pressure sores, DVT, or muscle atrophy.
B. Medications
- Analgesics: For pain relief (e.g., paracetamol, opioids).
- NSAIDs: Reduce inflammation and pain (e.g., ibuprofen, diclofenac).
- Muscle Relaxants: Used in muscle spasms.
- Antibiotics: For musculoskeletal infections.
- Steroids: For autoimmune or severe inflammatory conditions (e.g., rheumatoid arthritis).
- Disease-Modifying Anti-Rheumatic Drugs (DMARDs): For autoimmune diseases.
- Bisphosphonates/Calcium/Vitamin D: In osteoporosis.
C. Physical Therapy (Physiotherapy)
- Goals: Improve mobility, strengthen muscles, restore function.
- Techniques Used:
- Active and passive range-of-motion exercises
- Heat and cold therapy
- Electrical stimulation
- Ultrasound therapy
- Hydrotherapy
- Nursing Role: Encourage compliance, teach exercises, monitor pain or discomfort.
D. Occupational Therapy
- Helps patients with daily activities by modifying tools or teaching adaptive techniques.
E. Orthotic Devices
- Devices like braces, shoe inserts, spinal supports, and custom shoes are used to support joints or deformities.
🟩 2. Surgical Treatment Modalities
Used when conservative management fails or in severe cases.
A. Fracture Management
- Open Reduction and Internal Fixation (ORIF): Surgical alignment and fixation using plates, screws, rods.
- External Fixation: Pins or wires placed into bone and connected to an external frame.
- Intramedullary Nailing: A rod inserted into the marrow canal for long bone fractures.
B. Arthroscopy
- Minimally invasive procedure to visualize, diagnose, and treat joint problems using a small camera.
- Common for knee, shoulder, and wrist injuries.
C. Arthroplasty (Joint Replacement Surgery)
- Total Hip/Knee Replacement: Replacement of damaged joint surfaces with artificial implants.
- Indications: Osteoarthritis, rheumatoid arthritis, avascular necrosis.
D. Amputation
- Surgical removal of a limb or part, usually due to severe infection, trauma, or cancer.
- Nursing Focus: Stump care, phantom limb pain management, psychological support.
E. Spinal Surgery
- Includes discectomy, laminectomy, spinal fusion for conditions like herniated disc, scoliosis, or spinal stenosis.
F. Bone Grafting
- Used to repair or rebuild damaged bones using autografts or allografts.
G. Corrective Osteotomy
- Cutting and realigning bones to correct deformities (e.g., clubfoot, bowlegs).
H. Tumor Resection and Limb Salvage Surgery
- Removal of benign/malignant tumors with reconstruction when possible.
🟩 3. Traction
Used to align bones and relieve pressure before surgical fixation.
Types:
- Skin traction (Buck’s traction): Non-invasive, for temporary alignment.
- Skeletal traction: Involves pins inserted into bone and attached to weights.
Nursing Considerations:
- Maintain proper weight and alignment
- Monitor for infection at pin sites
- Neurovascular checks
🟩 4. Rehabilitation and Supportive Care
A. Rehabilitation
- Essential part of recovery post-surgery or injury.
- Includes physiotherapy, occupational therapy, and psychological counseling.
B. Pain Management
- May involve pharmacological and non-pharmacological approaches.
- TENS therapy, guided imagery, and relaxation techniques.
C. Nutritional Support
- High-protein diet, calcium, vitamin D, and supplements for healing and bone strength.
D. Psychological Counseling
- Important for amputees, chronic pain patients, and those with permanent disabilities.
🟩 5. Assistive and Adaptive Devices
- Canes, walkers, crutches, prosthetics
- Aid in mobility and independence during recovery or permanent disability
🔷 NURSING RESPONSIBILITIES IN ORTHOPEDIC CARE
- Assessment:
- Pain, swelling, neurovascular status (5 Ps: pain, pallor, pulselessness, paresthesia, paralysis)
- Wound and pin site care
- Pre- and post-operative care
- Assisting in application/removal of cast or traction
- Prevention of complications: pressure sores, contractures, DVT
- Patient education: mobility aids, exercises, wound care, medication use
- Psychosocial support and rehabilitation coordination
🔷 KEY POINTS
- Early mobilization prevents complications.
- Always monitor for signs of neurovascular compromise in limb injuries.
- Proper cast care and traction maintenance are crucial.
- Multidisciplinary approach enhances outcomes – orthopedists, nurses, physiotherapists, and occupational therapists must coordinate.
🦴✨ ORTHOPEDIC CAST ✨🦴

A cast is a rigid external immobilizing device that is molded to the body to support and stabilize fractured bones and injured soft tissues.
🔷 🧱 DEFINITION
A cast is a non-removable, molded external support made from materials like plaster of Paris or fiberglass, used to immobilize bones or joints for proper healing.
🔷 📌 PURPOSES OF CASTING
🔹 Immobilize fractured bone
🔹 Maintain bone alignment and prevent displacement
🔹 Reduce pain and swelling
🔹 Support weakened joints and soft tissues
🔹 Promote healing by restricting movement
🔷 📂 TYPES OF CASTS
| 🔢 Type of Cast | 📍 Description | ✅ Common Uses |
|---|---|---|
| 1. Short Arm Cast | Below elbow to hand | Wrist fractures, minor forearm injuries |
| 2. Long Arm Cast | From upper arm to hand | Elbow or forearm fractures |
| 3. Short Leg Cast | Below knee to foot | Ankle sprains, foot fractures |
| 4. Long Leg Cast | From thigh to foot | Tibia/fibula fractures |
| 5. Spica Cast | Encloses part of trunk and one/both limbs | Hip dysplasia, femoral fractures (mostly kids) |
| 6. Body Cast | Encases the torso | Spine stabilization |
| 7. Cast Braces | Allows controlled motion while supporting bone | During fracture healing phase |
🔷 📋 INDICATIONS
✅ Bone fractures (simple/compound)
✅ Post-operative orthopedic procedures
✅ Congenital bone deformities (e.g., clubfoot)
✅ Dislocations (to maintain reduction)
✅ Correction of deformities using serial casting (e.g., scoliosis)
🔷 ⛔ CONTRAINDICATIONS
❌ Open wounds or infected skin in casting area
❌ Severe soft tissue swelling (risk of compartment syndrome)
❌ Vascular compromise
❌ Allergy to casting material
❌ Skin conditions (eczema, dermatitis)
🔷 🧰 EQUIPMENTS REQUIRED FOR CAST APPLICATION
🔧 Basic Setup:
- Gloves, apron
- Stockinette (cotton base layer)
- Cast padding (soft roll)
- Plaster of Paris (POP) rolls or fiberglass tape
- Water basin (for dipping POP)
- Bandage scissors
- Bucket/liner for waste
- Marker (to date/label cast)
- Splinting shears (for fiberglass)
Optional: Cast saw (for later removal), protective drapes or sheets
🔷 📝 PROCEDURE STEPS FOR CAST APPLICATION
🔹 Preparation
- ✔ Explain procedure to patient and obtain consent
- 🧼 Wash hands and ensure privacy
- 🔍 Assess injured area – check for swelling, open wounds, circulation
- 🧦 Apply stockinette and padding to protect skin
🔹 Casting
- 💧 Dip POP/fiberglass roll in lukewarm water
- 🌀 Wrap cast material smoothly around the limb
- 🧤 Mold it gently for proper contour and fit
- 🕒 Allow the cast to set (10–15 mins for fiberglass; 24–72 hrs for POP)
🔹 Aftercare
- 📝 Document procedure, type of cast, time, and limb alignment
- 🧠 Educate patient about care, signs of complications
🔷 👩⚕️ ROLE OF NURSE IN CAST CARE
✅ Before Application
- Assess neurovascular status (color, temperature, capillary refill, movement, sensation)
- Assist in positioning and comfort
- Prepare materials and assist physician
✅ During Application
- Support limb during wrapping
- Ensure smooth padding and no wrinkles (prevent pressure sores)
- Monitor for patient discomfort or distress
✅ After Application
- Recheck neurovascular status hourly for first 24 hours
- Elevate the limb to reduce swelling
- Instruct patient not to insert objects inside the cast
- Keep cast dry and clean
- Look for signs of complications (see below)
🔷 ⚠️ COMPLICATIONS TO WATCH FOR (RED FLAGS)
🚨 Severe pain unrelieved by medication
🚨 Swelling or tightness under the cast
🚨 Numbness, tingling, or loss of movement
🚨 Blue/cold fingers or toes
🚨 Foul odor or drainage from cast
🚨 Skin irritation or burns from wet cast
🔷 ✅ PATIENT & FAMILY EDUCATION
📌 Keep cast dry – use plastic covering during bathing
📌 Do not insert sharp objects inside the cast
📌 Elevate limb on pillows to prevent swelling
📌 Perform finger/toe exercises to promote circulation
📌 Report signs of poor circulation or infection immediately
📌 Follow-up for cast removal and checkups
🔷 💡 KEY POINTS TO REMEMBER
🔸 Always assess circulation, movement, and sensation before and after cast
🔸 Plaster casts take longer to dry – handle with palms, not fingers
🔸 Do not cover wet cast – can cause burns
🔸 Monitor for compartment syndrome
🔸 Provide proper cast care instructions to prevent complications
🦴✨ SPLINT – A Life-Saving Immobilizer ✨🦴

A splint is a temporary, rigid or semi-rigid device used to support, protect, or immobilize injured bones and soft tissues.
🔷 📘 DEFINITION
A splint is an orthopedic device used to immobilize an injured part (bone/joint), prevent movement, reduce pain, and allow healing — often used as initial management of fractures, sprains, or dislocations.
🔷 🎯 PURPOSES OF SPLINTING
✅ Immobilization of injured bone or joint
✅ Temporary stabilization before definitive treatment
✅ Relief from pain and muscle spasm
✅ Maintain bone alignment and prevent further damage
✅ Protect soft tissue injuries and reduce swelling
🔷 🧱 TYPES OF SPLINTS
| 🔢 Type of Splint | 📍 Description & Use |
|---|---|
| 1. Rigid Splints | Made of wood, plastic, metal — provide firm support |
| 2. Soft Splints | Includes pillows, blankets, or padded boards |
| 3. Air Splints | Inflatable, transparent plastic sleeves |
| 4. Vacuum Splints | Malleable; becomes rigid when air is removed |
| 5. Traction Splints | Used for femur fractures to apply traction & alignment |
| 6. Anatomical Splints | Injured part is strapped to an uninjured adjacent body part |
| 7. Preformed Splints | Ready-made (e.g., wrist or ankle brace) |
| 8. Slab (POP) Splints | Temporary immobilization using half-cast slab |
🔷 📋 INDICATIONS
✅ Fractures (initial stabilization)
✅ Sprains and strains
✅ Dislocations (pre and post-reduction)
✅ Soft tissue injuries
✅ Post-surgical immobilization
✅ Congenital limb deformities
✅ Burns and contractures (positioning splints)
✅ Joint inflammation (e.g., arthritis)
🔷 ⛔ CONTRAINDICATIONS
❌ Open wounds without dressing
❌ Severe swelling (may compress tissues)
❌ Poor circulation in the affected limb
❌ Allergy to splint materials
❌ Unstable fracture needing immediate surgical intervention
🔷 🧰 EQUIPMENTS REQUIRED
🔧 Splinting Materials:
- Type-appropriate splint (rigid, soft, air, vacuum, slab, etc.)
- Padding material (cotton rolls, gauze)
- Stockinette (if using POP/fiberglass)
- Bandages or straps (to secure splint)
- Gloves
- Scissors
- Tape
- Water basin (for POP if required)
Optional: Sling or crutches for mobility
🔷 📝 PROCEDURE STEPS
🟢 1. Preparation
- 👩⚕️ Explain the procedure to the patient
- 🧼 Wash hands, wear gloves
- 🛏️ Position the patient comfortably
- 🔍 Assess injury site for swelling, bleeding, circulation
🟢 2. Application
- 🧦 Apply stockinette and soft padding over limb
- 📐 Place splint along the injured part maintaining neutral position
- 🩹 Secure with bandages without excessive tightness
- 🧼 Smooth edges to avoid pressure points
- 🕒 Check limb for circulation, sensation, and movement
🟢 3. Aftercare
- 📌 Elevate limb and monitor for swelling
- 📝 Document time, type of splint, and findings
- 🧠 Educate patient about splint care and warning signs
🔷 👩⚕️ ROLE OF NURSE IN SPLINT CARE
✅ Before Application
- Assess 5 P’s: Pain, Pallor, Pulses, Paresthesia, Paralysis
- Prepare the site: cleanse, dress wounds
- Explain the need and gain cooperation
✅ During Application
- Maintain proper alignment
- Prevent pressure areas with adequate padding
- Provide emotional support
✅ After Application
- Regular neurovascular checks (every 1–2 hrs initially)
- Monitor for signs of compartment syndrome
- Educate patient/family:
- Keep splint dry
- No insertion of objects inside
- Avoid weight-bearing unless advised
- Document all findings and responses
🔷 🚨 SIGNS OF COMPLICATIONS
🔴 Severe or increasing pain
🔴 Cold or blue fingers/toes
🔴 Numbness or tingling
🔴 Foul odor or discharge
🔴 Loosened or broken splint
🔴 Pressure sores or skin breakdown
🔷 ✅ PATIENT EDUCATION
📌 Keep the splint dry and clean
📌 Do not remove or tamper with splint
📌 Elevate limb to reduce swelling
📌 Do active finger/toe movements regularly
📌 Report any signs of circulation issues or discomfort
📌 Follow-up with healthcare provider
🔷 💡 KEY POINTS TO REMEMBER
✔ Splints are temporary and meant for initial immobilization
✔ Always assess neurovascular status before and after application
✔ Proper padding and positioning are crucial to avoid complications
✔ Nurses play a critical role in monitoring and educating patients
✔ Early recognition of compartment syndrome saves limbs!
🧲✨ TRACTION in Orthopedic Care ✨🧲
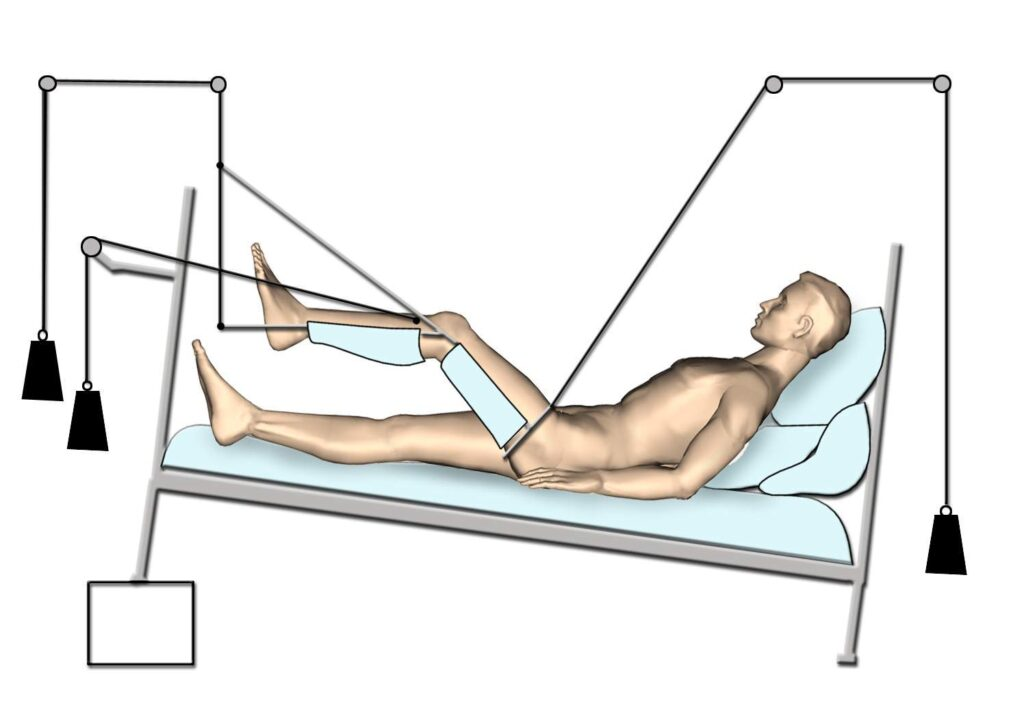
Traction is a therapeutic technique that uses a pulling force to treat musculoskeletal disorders—especially fractures, dislocations, and deformities.
🔷 📘 DEFINITION
Traction is the application of a steady pulling force to align bones, reduce fractures or dislocations, relieve muscle spasm, and correct deformities by maintaining proper bone position.
🔷 🎯 PURPOSES OF TRACTION
🔹 Align fractured bones
🔹 Reduce and immobilize dislocations
🔹 Relieve pain from muscle spasm
🔹 Prevent or correct deformities
🔹 Reduce/prevent soft tissue damage
🔹 Maintain limb in functional position pre- or post-operatively
🔷 🧱 TYPES OF TRACTION
🟡 A. Based on Method:
| 🔢 Type | 📍 Description | ✅ Examples/Use |
|---|---|---|
| 1. Skin Traction | Pulling force is applied to skin using straps/tape | Buck’s, Russell’s, Bryant’s |
| 2. Skeletal Traction | Pulling force applied directly to bone via pins/wires | Femur fractures, cervical spine injuries |
🟢 B. Common Traction Types:
| Type | Used For |
|---|---|
| Buck’s Traction | Hip fractures, knee injuries |
| Russell’s Traction | Femur or lower leg fractures |
| Bryant’s Traction | Pediatric hip/femur fractures |
| Cervical Traction | Cervical spine injuries (halo brace, tongs) |
| Pelvic Traction | Low back pain, lumbar spine injuries |
| Balanced Suspension | Femoral fractures (maintains alignment) |
🔷 📋 INDICATIONS
✅ Fractures (especially long bones like femur, tibia)
✅ Dislocations (hip or shoulder)
✅ Cervical or lumbar spine injuries
✅ Joint contractures or congenital deformities
✅ Muscle spasms and pain
✅ Post-surgical stabilization
🔷 ⛔ CONTRAINDICATIONS
❌ Open or infected wounds at traction site
❌ Severe vascular disease
❌ Fragile or elderly skin (risk with skin traction)
❌ Poor bone integrity (osteoporosis – caution in skeletal traction)
❌ Active infection or osteomyelitis in bone
🔷 🧰 EQUIPMENTS USED IN TRACTION
🔧 General Items:
- Traction frame (e.g., Thomas splint or Balkan frame)
- Pulleys and ropes
- Traction weights (2–10 kg, based on purpose)
- Traction cords
- Spreader bar (to maintain distance in skin traction)
- Adhesive straps, foam boots, slings (for skin traction)
- Skeletal traction pins (Steinmann pin, Kirschner wire)
- Pin care kit (antiseptic, gauze, gloves, dressing)
- Overhead trapeze for patient movement
- Bed blocks (to maintain countertraction)
🔷 📝 PROCEDURE STEPS (General Traction Setup)
🟢 Preparation
- 🧼 Wash hands, explain procedure, obtain consent
- 🛏️ Position patient with body alignment
- 🔍 Inspect skin or bone site (based on traction type)
🟢 Application
- 🧦 Apply foam boots or adhesive straps for skin traction
- 📍 Insert pins/wires (done by doctor in sterile setting for skeletal traction)
- 🧵 Connect pulleys, ropes, and weights ensuring smooth motion
- ⚖ Adjust weights as prescribed, ensuring balanced traction
- 🕒 Monitor alignment and patient’s response
🔷 👩⚕️ NURSING RESPONSIBILITIES IN TRACTION CARE
✅ Before & During Application
- Assess neurovascular status of the limb (color, pulse, movement)
- Prepare and assist in application
- Maintain proper alignment and position
- Ensure traction setup is correct and uninterrupted
✅ Ongoing Care
- Skin Care (in skin traction): prevent pressure ulcers
- Pin Site Care (in skeletal traction): prevent infection
- Monitor for compartment syndrome or nerve compression
- Reposition patient using trapeze (do not disturb traction)
- Check for signs of infection, DVT, foot drop
- Educate patient on immobility complications prevention
🔷 🚨 COMPLICATIONS OF TRACTION
🔴 Skin breakdown and ulcers
🔴 Neurovascular compromise (numbness, pallor, cyanosis)
🔴 Pin site infection (osteomyelitis in skeletal traction)
🔴 Muscle atrophy or joint stiffness
🔴 Constipation, urinary stasis due to immobility
🔴 Anxiety, depression
🔷 ✅ PATIENT & FAMILY EDUCATION
📌 Do not remove weights or adjust traction yourself
📌 Report pain, numbness, tingling, or burning immediately
📌 Perform deep breathing and limb exercises
📌 Use trapeze for movement – never pull on traction setup
📌 Maintain hygiene, especially skin under straps or near pins
📌 Prevent constipation and DVT – encourage fluids & foot movement
🔷 💡 KEY POINTS TO REMEMBER
✔ Traction must be continuous unless ordered otherwise
✔ Countertraction is essential for traction to work (often patient’s body weight or elevated foot end)
✔ Never place weights on bed or floor
✔ Ensure alignment, balance, and comfort
✔ Monitor for neurovascular signs frequently
✔ Traction can be lifesaving in trauma and fracture management
🚶♂️🦯 CRUTCH WALKING.

🔷 📘 DEFINITION
Crutches are mobility aids that help transfer body weight from the legs to the upper body, allowing safe ambulation when a patient is partially or completely non-weight bearing on one or both legs.
🔷 🧱 TYPES OF CRUTCHES
| Type | Description and Use |
|---|---|
| 1. Axillary Crutches 🦯 | Placed under the arms; common for temporary use in fractures, sprains |
| 2. Forearm (Lofstrand) Crutches 💪 | Cuff fits around forearm; for long-term users or better control |
| 3. Platform Crutches 🪵 | Forearm rests on a platform; used in patients with weak hands or arthritis |
| 4. Gutter Crutches 🛠️ | Similar to platform crutch with arm support; used in rheumatologic conditions |
🔷 🎯 INDICATIONS
✅ Lower limb fractures or injuries
✅ Post-operative recovery (e.g., joint replacements)
✅ Weakness or paralysis of one or both legs
✅ Amputation
✅ Neuromuscular disorders
✅ Balance issues requiring support
🔷 ⛔ CONTRAINDICATIONS
❌ Severe upper body weakness (unable to support weight with arms)
❌ Poor coordination or cognitive impairment
❌ Severe arthritis or pain in shoulders/wrists
❌ Cardiopulmonary conditions preventing exertion
🔷 🧰 EQUIPMENT NEEDED
🔧 Pair of crutches (adjusted to height)
🧤 Padded hand grips and axillary pads
👟 Non-slip shoes
🛏️ Flat, clutter-free walking space
👩⚕️ Gait belt (if training support is needed)
🔷 🧠 MEASURING FOR AXILLARY CRUTCHES
📏 Crutch length:
- 2 inches below axilla
- 6 inches lateral and 6 inches in front of foot
- Elbow should flex 20–30° when holding hand grips
✅ Always avoid pressing into axilla — to prevent brachial nerve damage!
🔷 🚶♂️ CRUTCH WALKING GAITS (Based on Weight Bearing Status)
| Gait Type | Suitable For | Description |
|---|---|---|
| 1. 4-Point Gait | Partial weight-bearing both legs | Move R crutch → L foot → L crutch → R foot (slow & stable) |
| 2. 3-Point Gait | Non-weight bearing one leg | Move both crutches → swing good leg forward |
| 3. 2-Point Gait | Partial weight-bearing both legs | R crutch + L foot → L crutch + R foot (faster, less stable) |
| 4. Swing-To Gait | Paraplegics or severe weakness | Move both crutches → swing legs to crutches |
| 5. Swing-Through Gait | Good upper body strength | Move both crutches → swing legs beyond crutches |
🔷 👩⚕️ NURSE’S ROLE IN CRUTCH WALKING TRAINING
✅ Before Training:
- Assess weight-bearing status (per doctor’s order)
- Measure and fit crutches properly
- Educate on posture, gait, and fall precautions
- Clear walking area of obstacles
✅ During Training:
- Teach correct gait based on need
- Monitor for signs of fatigue, pain, or imbalance
- Use gait belt for initial supervision
- Reinforce not to rest on axilla
- Encourage correct arm and leg coordination
✅ After Training:
- Reassess mobility, confidence, and safety
- Encourage home safety (no rugs, good lighting)
- Educate family/caregivers
- Document progress and response to therapy
🔷 ⚠️ SAFETY TIPS FOR CRUTCH USERS
🚫 Do not lean on armpits
👟 Wear well-fitting, non-slip shoes
🚿 Install grab bars and use rubber tips on crutches
🛑 Avoid wet floors and clutter
🔁 Inspect crutch tips regularly for wear
🔋 Rest between walks to avoid fatigue
🔷 💡 KEY POINTS TO REMEMBER
✔ Always match the gait to the patient’s strength and weight-bearing ability
✔ Crutches should be measured properly to avoid nerve injuries
✔ Supervision is critical during initial mobility training
✔ The four-point gait is most stable but slow
✔ Swing-through gait requires strength and balance – used by paraplegics
🦴🔥 Musculoskeletal Inflammation: BURSITIS
🔷 📘 DEFINITION
Bursitis is the inflammation of a bursa, which is a small fluid-filled sac that acts as a cushion between bones, tendons, muscles, and skin near joints. Inflammation causes pain, swelling, and restricted movement.
🔷 🧾 CAUSES OF BURSITIS
✅ Common Causes:
- 🔁 Repetitive motion or overuse (e.g., kneeling, throwing)
- 🧱 Prolonged pressure on joints (e.g., resting elbows on hard surfaces)
- 🦠 Infection (septic bursitis)
- 🤕 Trauma or injury to the joint
- 💊 Inflammatory conditions like rheumatoid arthritis, gout
- 🔧 Improper posture or joint alignment
🔷 🧱 TYPES OF BURSITIS
| Type | Description | Common Site |
|---|---|---|
| 1. Prepatellar | Inflammation of knee bursa | 🦵 Knee (Housemaid’s knee) |
| 2. Olecranon | Affects elbow tip | 💪 Elbow (Student’s elbow) |
| 3. Subacromial | In shoulder joint | 🦴 Shoulder |
| 4. Trochanteric | Over greater trochanter | 🍑 Hip |
| 5. Ischial | Over ischial tuberosity | 🍑 Buttocks (Weaver’s bottom) |
| 6. Retrocalcaneal | Near Achilles tendon | 🦶 Heel |
| 7. Septic Bursitis | Bacterial infection in bursa | Any site |
🔷 🔬 PATHOPHYSIOLOGY OF BURSITIS
- Repetitive use / trauma / infection leads to
- ➡️ Micro-tears in the bursa lining
- ➡️ Inflammatory response is activated
- ➡️ Synovial cells secrete excess fluid
- ➡️ Bursa becomes swollen, inflamed, and painful
- ➡️ In severe cases, may lead to fibrosis, thickening, or infection
🔷 🩺 SIGNS & SYMPTOMS
| Symptom | Description |
|---|---|
| 🔴 Pain | Localized, worsens with movement or pressure |
| 🌡️ Swelling | Visible enlargement over affected joint |
| 🔥 Warmth | Especially in septic bursitis |
| 🚫 Limited mobility | Due to pain and swelling |
| 😣 Tenderness | On palpation of the inflamed site |
| 💊 Systemic signs | Fever, malaise (in infectious cases) |
🔷 🧪 DIAGNOSTIC INVESTIGATIONS
| Test | Purpose |
|---|---|
| ✅ Clinical examination | Location, swelling, movement limitation |
| 💉 Bursa aspiration | Rule out infection or crystals (e.g., gout) |
| 🔬 Gram stain/culture | Detect causative bacteria (in septic bursitis) |
| 🧪 CBC, ESR, CRP | Elevated in infection or inflammation |
| 🖥️ X-ray/Ultrasound | Rule out bone involvement or visualize bursal fluid |
| 🧲 MRI (if needed) | Detailed imaging of soft tissues |
🔷 💊 MEDICAL MANAGEMENT
| Category | Examples | Purpose |
|---|---|---|
| 🧴 Rest & Immobilization | Splinting, avoiding activity | Reduce irritation |
| ❄️ Cold Compress | 15–20 minutes a few times/day | Decrease swelling and pain |
| 💊 NSAIDs | Ibuprofen, naproxen | Control pain and inflammation |
| 💉 Corticosteroid injection | Methylprednisolone into bursa | For persistent inflammation |
| 💊 Antibiotics | If septic bursitis (e.g., cefazolin) | Treat bacterial infection |
| 🏃 Physical therapy | Stretching and strengthening | Restore joint function |
| ⚖️ Weight loss/Ergonomics | In overweight or active individuals | Reduce joint stress |
🔷 🛠️ SURGICAL MANAGEMENT
Surgery is rare and reserved for chronic, recurrent, or infected bursitis that doesn’t respond to conservative measures.
🟢 Types of Surgical Intervention:
| Procedure | Description |
|---|---|
| 🛑 Bursa aspiration/drainage | For large fluid collections |
| 🗑️ Bursectomy | Surgical removal of inflamed bursa |
| 🔬 Arthroscopic debridement | Minimal invasion to clean infected tissue |
👩⚕️🦴 NURSING MANAGEMENT OF BURSITIS
🔷 🎯 GOALS OF NURSING CARE
✅ Relieve pain and inflammation
✅ Promote joint mobility and function
✅ Prevent complications (e.g., infection, stiffness)
✅ Support healing and comfort
✅ Educate the patient for self-care and prevention
🔷 📝 NURSING ASSESSMENT
🔍 Subjective Data:
- Pain history: onset, location, severity, aggravating/relieving factors
- Functional limitations
- History of trauma, repetitive use, systemic diseases (RA, gout)
🔍 Objective Data:
- Swelling, redness, warmth over joint
- Tenderness on palpation
- Limited range of motion (ROM)
- Signs of systemic infection (in septic bursitis)
🔷 🧰 NURSING INTERVENTIONS
💊 1. Pain and Inflammation Management
- Administer NSAIDs or prescribed analgesics as ordered
- Apply cold compress for 15–20 minutes several times daily (first 48–72 hrs)
- Monitor for side effects of medications (e.g., GI upset, allergy)
🛏️ 2. Rest and Immobilization
- Encourage rest of affected joint during acute phase
- Apply splints or supports as advised to limit movement
- Avoid pressure or repetitive movements to the joint
🌡️ 3. Infection Control (Septic Bursitis)
- Aseptic technique during dressing changes or aspiration
- Administer antibiotics as prescribed
- Monitor for fever, increased pain, purulent drainage
- Educate about hand hygiene and wound care
🏃♂️ 4. Mobility and Physical Therapy
- Encourage gentle ROM exercises once inflammation subsides
- Collaborate with physiotherapist for strength and mobility training
- Avoid complete immobility to prevent stiffness or muscle atrophy
🧠 5. Patient Education
- Explain nature and cause of bursitis
- Teach postural correction and ergonomic techniques
- Advise activity modification to prevent recurrence
- Educate on use of supportive devices if needed
- Encourage weight management if overweight
🧾 6. Monitoring and Evaluation
- Regularly assess pain level and joint function
- Observe for signs of improvement or complications
- Evaluate effectiveness of treatment and patient compliance
- Reassess neurovascular status of affected limb if immobilized
🔷 📌 DISCHARGE TEACHING
✅ How to care for the joint at home
✅ When and how to apply ice packs or heat therapy
✅ Signs to report: increasing pain, swelling, redness, fever
✅ Importance of follow-up visits and physiotherapy
✅ Preventive actions (e.g., cushioning joints, avoiding overuse)
🔷 💡 KEY NURSING POINTS
✔ Early recognition and intervention prevent complications
✔ Use cold therapy in acute phase, heat therapy in chronic phase
✔ Never massage or apply pressure on an inflamed bursa
✔ Individualize care based on cause (e.g., trauma, infection, RA)
✔ Ongoing education and support empower patient for long-term self-care
⚠️🦴 COMPLICATIONS OF BURSITIS
While most cases of bursitis respond well to conservative treatment, untreated or recurrent bursitis can lead to complications.
🔷 ❗ MAJOR COMPLICATIONS
| 🚨 Complication | 🔍 Description |
|---|---|
| 1. Chronic Bursitis | Recurrence leads to thickening of the bursal wall, fibrosis, and ongoing pain/stiffness. |
| 2. Infection (Septic Bursitis) | May spread to nearby tissues causing cellulitis or osteomyelitis. Needs urgent antibiotics or drainage. |
| 3. Abscess Formation | In untreated septic bursitis; collection of pus in bursa requiring surgical drainage. |
| 4. Reduced Joint Mobility | Due to prolonged inflammation, pain, or improper rest. May lead to joint contracture. |
| 5. Muscle Atrophy | From disuse due to pain or prolonged immobility. |
| 6. Recurrence | Without proper preventive measures (e.g., posture correction), bursitis can reappear. |
| 7. Nerve Compression | Swollen bursa may compress nearby nerves, leading to numbness or tingling. |
✅✨ KEY POINTS TO REMEMBER
📌 Bursitis = Inflammation of a bursa, mostly caused by repetitive motion, trauma, or infection.
📌 Most commonly affects shoulder, elbow, knee, hip, and heel.
📌 Types include: Prepatellar, Olecranon, Subacromial, Trochanteric, Retrocalcaneal, etc.
📌 NSAIDs, rest, cold compresses, and corticosteroid injections are mainstays of treatment.
📌 Septic bursitis needs urgent aspiration + antibiotics (may need surgical drainage).
📌 Nursing care includes pain management, rest, mobility support, infection monitoring, and patient education.
📌 Avoid repetitive joint strain and encourage ergonomic practices to prevent recurrence.
📌 Assess neurovascular status regularly in immobilized patients.
📌 Patient education is key to long-term prevention and compliance.
🦴🔥 Synovitis – Inflammation of Synovial Membrane
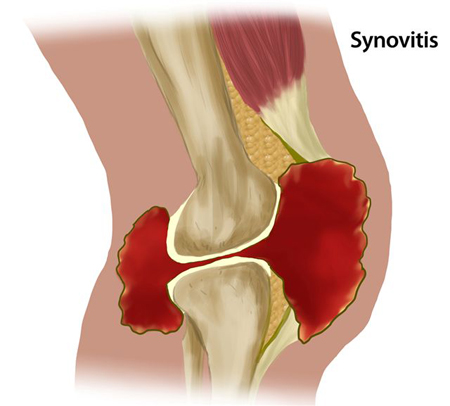
🔷 📘 DEFINITION
Synovitis is the inflammation of the synovial membrane that lines joints, tendons, and bursae. This results in pain, swelling, warmth, and reduced mobility due to excess synovial fluid production.
🧪 It is commonly associated with arthritis and autoimmune joint disorders.
🔷 🧾 CAUSES OF SYNOVITIS
| Category | Examples |
|---|---|
| ✅ Autoimmune disorders | Rheumatoid arthritis, lupus, juvenile arthritis |
| 🤕 Trauma/injury | Joint sprains, ligament tears |
| 🦠 Infection | Septic arthritis, viral/bacterial infections |
| 🦴 Degenerative joint disease | Osteoarthritis |
| 🧬 Crystal deposition | Gout (uric acid), Pseudogout (calcium crystals) |
| 🔄 Repetitive use/strain | Sports-related joint overuse |
| 🧒 Pediatric cause | Transient synovitis (in children, post-viral) |
🔷 🧱 TYPES OF SYNOVITIS
| Type | Description |
|---|---|
| 1. Acute Synovitis | Sudden onset, often due to trauma or infection |
| 2. Chronic Synovitis | Long-standing, seen in autoimmune diseases like RA |
| 3. Septic Synovitis | Bacterial infection of synovial fluid |
| 4. Transient Synovitis | Temporary, viral-related inflammation (common in children) |
| 5. Villonodular Synovitis | Rare proliferative disorder of synovium (benign) |
🔷 🔬 PATHOPHYSIOLOGY
- Trigger (injury, infection, autoimmunity) →
- Activation of inflammatory mediators (cytokines, prostaglandins) →
- Synovial membrane hyperplasia and infiltration by WBCs →
- Increased vascular permeability → fluid accumulation →
- Formation of excess synovial fluid + joint effusion →
- Pain, swelling, stiffness, and cartilage damage if chronic.
🔷 🩺 SIGNS AND SYMPTOMS
| Symptom | Description |
|---|---|
| 🔴 Joint pain | Especially during movement |
| 💨 Swelling | Due to fluid buildup in joint capsule |
| 🔥 Warmth & redness | Over the affected joint (especially in infection) |
| 🚫 Limited ROM | Due to pain or fluid obstruction |
| ❗ Morning stiffness | Common in autoimmune synovitis (RA) |
| 😷 Fever | In septic or systemic cases |
🔷 🧪 DIAGNOSIS
| Test | Purpose |
|---|---|
| 🩺 Physical Examination | Joint inspection, palpation, ROM assessment |
| 🧪 Blood Tests | CBC, ESR, CRP – shows inflammation |
| 💉 Synovial Fluid Aspiration | Analyzed for color, WBCs, culture, crystals |
| 🖥️ X-ray | Joint space narrowing, bone damage (chronic) |
| 🧲 Ultrasound/MRI | Detects effusion, synovial thickening |
| 🧬 Rheumatoid factor, ANA, uric acid | Rule out autoimmune or gout causes |
🔷 💊 MEDICAL MANAGEMENT
| Treatment | Purpose |
|---|---|
| 💊 NSAIDs (ibuprofen, naproxen) | Reduce pain and inflammation |
| 💉 Corticosteroids (oral/injection) | For severe inflammation or autoimmune synovitis |
| 💊 DMARDs (methotrexate, sulfasalazine) | For chronic autoimmune causes (RA, lupus) |
| 🧪 Antibiotics | If synovitis is septic (based on culture) |
| ❄️ Cold therapy | For acute swelling and pain |
| 🛏️ Rest and joint protection | To prevent further joint stress |
| 🏃♂️ Physiotherapy | Improves ROM and prevents stiffness |
🔷 🛠️ SURGICAL MANAGEMENT
Surgery is needed in chronic, non-responsive, or proliferative synovitis.
| Surgery | Indication & Description |
|---|---|
| 🔪 Synovectomy | Surgical removal of inflamed synovial tissue (done arthroscopically or openly) |
| 💉 Joint lavage/aspiration | For infected or severely swollen joints |
| 🦿 Joint replacement | End-stage damage (e.g., in rheumatoid arthritis) |
| 🧬 Biological therapy (anti-TNF) | In resistant autoimmune synovitis |
👩⚕️🦴 NURSING MANAGEMENT OF SYNOVITIS
🔷 🎯 GOALS OF NURSING CARE
✅ Relieve joint pain and inflammation
✅ Promote joint function and mobility
✅ Prevent joint deformity and complications
✅ Provide emotional and physical support
✅ Educate the patient and family on disease management and prevention
🔷 📝 NURSING ASSESSMENT
🔍 Subjective Data:
- Pain characteristics (onset, severity, timing)
- Morning stiffness duration (especially in RA-related synovitis)
- Functional limitations (walking, dressing, working)
- History of trauma, infection, or autoimmune disease
🔍 Objective Data:
- Swelling, warmth, redness over joint
- Decreased range of motion (ROM)
- Fever or systemic signs (if septic synovitis)
- Gait disturbances or joint deformity
- Laboratory and radiological reports
🔷 🧰 NURSING INTERVENTIONS
💊 1. Pain and Inflammation Management
- Administer NSAIDs, corticosteroids, or DMARDs as prescribed
- Apply cold compresses during acute inflammation (15–20 minutes, 2–3 times daily)
- Assess pain using appropriate pain scales and respond promptly
- Monitor for adverse drug reactions (e.g., GI upset with NSAIDs, immunosuppression with DMARDs)
🛏️ 2. Joint Rest and Protection
- Encourage rest during acute phase; avoid weight-bearing if painful
- Position joint in functional alignment using pillows or splints
- Support use of mobility aids (e.g., cane, walker) as needed
- Avoid prolonged immobilization to prevent stiffness and muscle atrophy
🏃♂️ 3. Mobility and Rehabilitation
- Collaborate with physiotherapist for range-of-motion and strengthening exercises
- Encourage gradual activity increase as pain subsides
- Promote active and passive exercises to maintain joint flexibility
- Prevent complications like contractures or muscle wasting
🧠 4. Infection Control (If Septic Synovitis)
- Strict aseptic technique during dressing changes or aspirations
- Administer IV or oral antibiotics as ordered
- Monitor for systemic infection signs (fever, chills, increased WBC count)
📚 5. Patient and Family Education
- Explain the nature of synovitis and importance of medication compliance
- Teach joint protection techniques and ergonomic posture
- Encourage regular follow-ups and monitoring of disease activity
- Educate about early warning signs of flare-ups or complications
- Discuss lifestyle modifications – weight control, joint-friendly activities, avoiding high-impact exercise
🧾 6. Monitoring and Evaluation
- Assess progress in pain control, joint mobility, and activity tolerance
- Monitor lab values (ESR, CRP, RF) and medication effectiveness
- Reassess for any signs of drug toxicity or adverse reactions
- Provide emotional support and evaluate coping mechanisms
🔷 📌 DISCHARGE TEACHING
✅ Proper medication use (especially immunosuppressants or antibiotics)
✅ How and when to apply cold or heat therapy
✅ Importance of joint exercises and physiotherapy
✅ When to seek medical help (e.g., increased pain, swelling, fever)
✅ Maintaining a healthy diet and hydration
✅ Regular medical follow-ups for chronic cases
🔷 💡 KEY NURSING POINTS
✔ Pain relief and joint protection are top priorities
✔ Early physiotherapy prevents long-term disability
✔ Always monitor for signs of infection or systemic complications
✔ Patient education and emotional support are essential in chronic or autoimmune synovitis
✔ Nurses play a crucial role in early recognition, monitoring, and multidisciplinary coordination
⚠️🦴 COMPLICATIONS OF SYNOVITIS
If untreated, recurrent, or poorly managed, synovitis can lead to serious musculoskeletal issues:
🔷 ❗ MAJOR COMPLICATIONS
| 🚨 Complication | 🔍 Description |
|---|---|
| 1. Joint Destruction | Chronic synovitis (especially in RA) can erode cartilage and bone. |
| 2. Joint Deformity | Prolonged inflammation can cause misalignment and permanent joint damage. |
| 3. Reduced Joint Mobility | Stiffness due to fibrosis or scar tissue limits range of motion. |
| 4. Muscle Atrophy | From disuse or immobilization around inflamed joints. |
| 5. Septic Arthritis | Infection can spread rapidly, damaging joint permanently. |
| 6. Bursitis or Tendonitis | Inflammation can extend to nearby bursae or tendons. |
| 7. Disability or Functional Limitation | In chronic or untreated cases, especially in weight-bearing joints. |
| 8. Side Effects of Long-Term Medication | Steroid use can cause osteoporosis, weight gain, and immunosuppression. |
✅✨ KEY POINTS TO REMEMBER
📌 Synovitis is inflammation of the synovial membrane — the joint lining.
📌 Can be acute or chronic, and is commonly seen in RA, lupus, gout, and trauma.
📌 Typical symptoms include joint pain, swelling, warmth, and restricted movement.
📌 Diagnosis is clinical, supported by labs (ESR, CRP), imaging, and joint fluid aspiration.
📌 Medical management includes NSAIDs, corticosteroids, antibiotics (for infection), and DMARDs for autoimmune causes.
📌 Surgical options like synovectomy are used in severe or unresponsive cases.
📌 Nursing management focuses on pain relief, joint rest, mobility support, infection prevention, and patient education.
📌 Early treatment prevents complications like joint deformity, disability, and chronic pain.
🦴🔥 ARTHRITIS
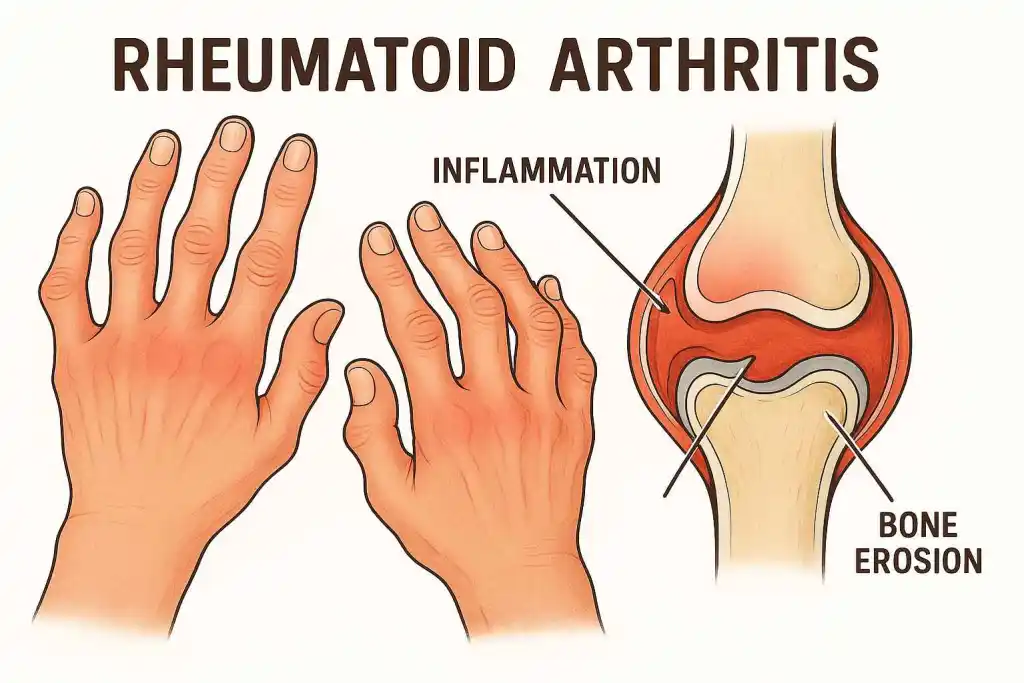
🔷 📘 DEFINITION
Arthritis is a chronic or acute inflammatory disorder that affects one or more joints, leading to pain, swelling, stiffness, and reduced mobility. It can be degenerative, autoimmune, infectious, or metabolic in origin.
📌 The word “arthritis” literally means “inflammation of a joint.”
🔷 🧾 CAUSES OF ARTHRITIS
Arthritis can be caused by a variety of factors, categorized as follows:
✅ 1. Autoimmune Causes
- 🧬 Rheumatoid Arthritis (RA) – Immune system attacks synovial lining
- 🧬 Systemic Lupus Erythematosus (SLE)
- 🧬 Psoriatic Arthritis
🔁 2. Degenerative Causes
- 🦴 Osteoarthritis (OA) – Wear and tear of cartilage over time
- 🧓 Age-related joint degeneration
- 💪 Repetitive stress or overuse injuries
🦠 3. Infectious Causes
- 🦠 Septic Arthritis – Bacterial or viral infection in the joint (e.g., Staphylococcus aureus)
- 🦠 Reactive Arthritis – Post-infection response (e.g., after GI or urinary tract infection)
- 🦟 Lyme Disease – Tick-borne bacterial infection
💎 4. Metabolic Causes
- 💎 Gout – Uric acid crystal deposition in joints
- 🧂 Pseudogout – Calcium pyrophosphate crystal accumulation
⚠️ 5. Traumatic/Mechanical Causes
- 🤕 Joint injuries or fractures
- 🧱 Repeated pressure or strain on joints (occupational/sports)
🔗 6. Genetic and Lifestyle Factors
- 👨👩👧 Family history (genetic predisposition)
- 🍔 Poor diet, obesity, sedentary lifestyle
- 🚬 Smoking (linked to RA and systemic inflammation)
🦴📚 TYPES OF ARTHRITIS
Arthritis includes over 100 disorders affecting joints, but here are the main clinically significant types, grouped for better understanding:
🔷 ✅ I. DEGENERATIVE ARTHRITIS (WEAR & TEAR)
| Type | Description |
|---|---|
| 1. Osteoarthritis (OA) | Most common type. Caused by cartilage breakdown due to aging, overuse, or injury. Usually affects knees, hips, spine, and hands. |
| 2. Spondylosis | OA of the spine (cervical or lumbar) causing stiffness, nerve compression, and back pain. |
| 3. Post-Traumatic Arthritis | Develops after joint injury or fracture. Can mimic OA symptoms. |
🔷 🧬 II. AUTOIMMUNE / INFLAMMATORY ARTHRITIS
| Type | Description |
|---|---|
| 1. Rheumatoid Arthritis (RA) | Autoimmune inflammation of synovial membrane. Affects small joints (hands, wrists). Symmetrical, progressive. |
| 2. Juvenile Idiopathic Arthritis (JIA) | Childhood version of RA. Causes joint swelling, stiffness, and growth problems. |
| 3. Psoriatic Arthritis | Occurs in people with psoriasis. Affects skin and joints. May involve fingers, toes, spine. |
| 4. Ankylosing Spondylitis (AS) | Chronic inflammation of spine and sacroiliac joints. Can lead to spinal fusion. |
| 5. Reactive Arthritis | Post-infection arthritis (usually GI or GU). Can cause eye, urinary, and joint symptoms (Reiter’s Syndrome). |
| 6. Systemic Lupus Erythematosus (SLE) | Autoimmune disease that can cause arthritis-like joint pain with multi-organ involvement. |
| 7. Enteropathic Arthritis | Associated with inflammatory bowel diseases (Crohn’s, Ulcerative Colitis). Affects spine and large joints. |
🔷 💎 III. METABOLIC ARTHRITIS
| Type | Description |
|---|---|
| 1. Gout | Caused by uric acid crystal buildup in joints (often big toe). Sudden, severe pain and swelling. |
| 2. Pseudogout | Caused by calcium pyrophosphate crystals. Affects larger joints like knee or wrist. |
🔷 🦠 IV. INFECTIOUS ARTHRITIS
| Type | Description |
|---|---|
| 1. Septic Arthritis | Bacterial infection inside a joint (commonly Staph aureus). Needs urgent treatment. |
| 2. Viral Arthritis | Caused by viruses like Hepatitis B/C, Parvovirus, Chikungunya. Often resolves on its own. |
| 3. Tubercular Arthritis | Caused by Mycobacterium tuberculosis. Usually affects spine (Pott’s disease) or large joints. |
| 4. Lyme Arthritis | Caused by Borrelia burgdorferi, transmitted by tick bites. Affects knees and large joints. |
🔷 👶 V. PEDIATRIC ARTHRITIS TYPES
| Type | Description |
|---|---|
| 1. Juvenile Idiopathic Arthritis | Most common arthritis in children under 16. Several subtypes (oligoarticular, polyarticular, systemic). |
| 2. Still’s Disease | Systemic-onset JIA with fever, rash, and arthritis. Can be life-threatening if not treated. |
🔷 ⚠️ VI. RARE / MISCELLANEOUS TYPES
| Type | Description |
|---|---|
| 1. Palindromic Rheumatism | Recurrent, short episodes of joint pain without lasting damage. |
| 2. Seronegative Arthritis | Group of autoimmune arthritides (like AS, psoriatic arthritis) that are RF-negative. |
| 3. Hemarthrosis (Bleeding into Joint) | Seen in hemophilia; mimics arthritis with joint swelling and damage over time. |
| 4. Villonodular Synovitis | Benign overgrowth of synovium causing joint swelling and pain. |
🧠 Summary by Category
| Category | Examples |
|---|---|
| 🧬 Autoimmune | RA, JIA, Psoriatic, Lupus, AS |
| 🦴 Degenerative | OA, Spondylosis |
| 💎 Metabolic | Gout, Pseudogout |
| 🦠 Infectious | Septic, Viral, TB, Lyme |
| 👶 Pediatric | JIA, Still’s Disease |
| 🧪 Miscellaneous | Palindromic, Hemarthrosis, PVNS |
🧬🦴 PATHOPHYSIOLOGY OF DIFFERENT TYPES OF ARTHRITIS
🔷 1. OSTEOARTHRITIS (OA) – Degenerative Arthritis
🔁 Wear and tear of cartilage over time
- Mechanical stress or aging causes cartilage degradation
- ➡️ Cartilage loses water content, becomes brittle
- ➡️ Joint space narrows, subchondral bone becomes exposed
- ➡️ Osteophytes (bone spurs) form at joint margins
- ➡️ Leads to joint pain, stiffness, crepitus, and reduced mobility
🔍 Affects weight-bearing joints like knees, hips, spine
🔷 2. RHEUMATOID ARTHRITIS (RA) – Autoimmune Inflammatory
🔬 Chronic autoimmune synovial inflammation
- Autoimmune trigger → activation of T-cells and cytokines
- ➡️ Synovial membrane becomes inflamed and thickened (pannus)
- ➡️ Cartilage and bone erosion by inflammatory cells
- ➡️ Joint capsule stretches and ligaments weaken
- ➡️ Leads to joint deformity, ankylosis, and loss of function
🔍 Usually affects small joints bilaterally (hands, wrists)
🔷 3. JUVENILE IDIOPATHIC ARTHRITIS (JIA)
👶 Autoimmune inflammation in children
- Similar mechanism to RA but in children
- Chronic synovial inflammation leads to joint growth disturbances, deformities, and potential systemic symptoms like fever and rash
🔷 4. PSORIATIC ARTHRITIS
🧬 Inflammation associated with psoriasis
- Immune system attacks skin and joints
- ➡️ Synovial inflammation and enthesitis (inflammation at tendon-bone junctions)
- ➡️ May cause asymmetrical arthritis, dactylitis (“sausage digits”), and nail changes
🔷 5. ANKYLOSING SPONDYLITIS (AS)
🦴 Chronic inflammation of spine and sacroiliac joints
- Inflammation begins in sacroiliac joints
- ➡️ Affects ligaments and spinal joints
- ➡️ Bone attempts repair → new bone formation (syndesmophytes)
- ➡️ Leads to fusion of vertebrae (bamboo spine)
🔷 6. GOUT (Metabolic Arthritis)
💎 Uric acid crystal deposition
- Elevated serum uric acid (hyperuricemia)
- ➡️ Uric acid crystals deposit in joints (commonly big toe)
- ➡️ Crystals trigger intense inflammatory response
- ➡️ Neutrophil infiltration → redness, heat, swelling
- ➡️ Repeated attacks may cause joint destruction and tophi formation
🔷 7. PSEUDOGOUT
🧂 Calcium pyrophosphate crystal deposition
- Same mechanism as gout but crystals are calcium pyrophosphate, not uric acid
- Common in elderly; affects knees and wrists
🔷 8. SEPTIC ARTHRITIS (Infectious)
🦠 Bacterial invasion of joint space
- Pathogens (e.g., Staphylococcus aureus) invade joint → acute infection
- ➡️ Rapid accumulation of pus and inflammatory cells
- ➡️ Synovial membrane destruction → cartilage damage
- ➡️ Can lead to joint destruction if untreated
🔷 9. REACTIVE ARTHRITIS
⚠️ Post-infectious autoimmune response
- Triggered by infections (GI or GU e.g., Chlamydia, Salmonella)
- ➡️ Immune system mistakenly targets joints
- ➡️ Inflammation of synovium, tendons, and eyes
- ➡️ Classic triad: arthritis, urethritis, conjunctivitis
🔷 10. SYSTEMIC LUPUS ERYTHEMATOSUS (SLE)-RELATED ARTHRITIS
🌡️ Autoimmune disease with systemic effects
- Autoantibodies form immune complexes → deposit in joints
- ➡️ Triggers inflammatory response
- ➡️ Unlike RA, lupus arthritis rarely causes joint deformity
🔷 11. TUBERCULAR ARTHRITIS
🧫 Chronic granulomatous joint infection (TB)
- Mycobacterium tuberculosis infects synovium
- ➡️ Chronic granulomatous inflammation
- ➡️ Caseation necrosis and cartilage damage
- ➡️ Usually affects spine (Pott’s disease) or weight-bearing joints
🔷 12. LYME ARTHRITIS
🦟 Tick-borne bacterial infection
- Caused by Borrelia burgdorferi
- ➡️ Inflammation primarily affects knees and large joints
- ➡️ May lead to recurrent joint swelling and stiffness
🔷 13. PALINDROMIC RHEUMATISM
🔁 Episodic arthritis with full recovery between attacks
- Sudden inflammation in one or more joints
- Episodes last hours to days
- No lasting joint damage, but may progress to RA
🩺🦴 SIGNS, SYMPTOMS & DIAGNOSIS OF ARTHRITIS (Major Types)
🔷 ✅ 1. OSTEOARTHRITIS (OA)
🔍 Signs & Symptoms
- 🔸 Joint pain worsens with activity, relieved by rest
- 🔸 Morning stiffness (< 30 mins)
- 🔸 Crepitus (grating sound)
- 🔸 Limited range of motion
- 🔸 Swelling without redness
- 🔸 Joint deformities (e.g., Heberden’s and Bouchard’s nodes in fingers)
🧪 Diagnosis
- X-ray: Joint space narrowing, osteophytes (bone spurs)
- Physical exam: Reduced joint mobility, crepitus
- MRI (if soft tissue involvement is suspected)
- Lab tests: Usually normal (no systemic inflammation)
🔷 🧬 2. RHEUMATOID ARTHRITIS (RA)
🔍 Signs & Symptoms
- 🔸 Painful, swollen, symmetrical joints (hands, wrists, feet)
- 🔸 Morning stiffness > 1 hour
- 🔸 Warmth, redness around joints
- 🔸 Fatigue, weight loss, low-grade fever
- 🔸 Joint deformities: ulnar deviation, swan neck, boutonnière deformity
🧪 Diagnosis
- Blood tests: ↑ ESR, ↑ CRP
- Rheumatoid factor (RF): Positive in ~70%
- Anti-CCP antibodies: More specific
- X-ray: Joint erosion, osteopenia near joints
- Ultrasound/MRI: Detect early synovial inflammation
🔷 👶 3. JUVENILE IDIOPATHIC ARTHRITIS (JIA)
🔍 Signs & Symptoms
- 🔸 Joint swelling in children >6 weeks
- 🔸 Limping or reduced activity
- 🔸 Morning stiffness
- 🔸 Rash or fever (in systemic type)
- 🔸 Growth retardation
🧪 Diagnosis
- Clinical criteria (before age 16, duration >6 weeks)
- ANA: May be positive
- ESR/CRP: Elevated
- Imaging: To assess joint damage or effusion
🔷 🎨 4. PSORIATIC ARTHRITIS
🔍 Signs & Symptoms
- 🔸 Joint pain with psoriasis skin lesions
- 🔸 Asymmetrical joint involvement
- 🔸 Dactylitis (“sausage digits”)
- 🔸 Nail changes: pitting, onycholysis
- 🔸 Back or sacroiliac pain
🧪 Diagnosis
- Clinical exam + psoriasis history
- ESR/CRP: Elevated
- RF: Negative (seronegative)
- X-ray: “Pencil-in-cup” deformity in advanced cases
🔷 🧍 5. ANKYLOSING SPONDYLITIS (AS)
🔍 Signs & Symptoms
- 🔸 Chronic lower back pain, better with exercise
- 🔸 Morning stiffness >30 mins
- 🔸 Reduced spine flexibility
- 🔸 Stooped posture (late stages)
- 🔸 Enthesitis (pain where ligaments attach)
🧪 Diagnosis
- X-ray/MRI: “Bamboo spine” appearance (fusion)
- HLA-B27: Positive in ~90% of patients
- ESR/CRP: Elevated
- Schober’s test: Measures lumbar spine flexibility
🔷 💎 6. GOUT
🔍 Signs & Symptoms
- 🔸 Sudden, intense joint pain (often 1st toe)
- 🔸 Swelling, warmth, redness
- 🔸 Tophi (chalky uric acid deposits in chronic cases)
- 🔸 Fever may occur
🧪 Diagnosis
- Serum uric acid: Elevated (>6.8 mg/dL)
- Joint aspiration: Monosodium urate crystals (needle-shaped, negatively birefringent)
- X-ray: Erosions with “overhanging edges” in chronic gout
- CBC: Mild leukocytosis
🔷 🧂 7. PSEUDOGOUT
🔍 Signs & Symptoms
- 🔸 Sudden joint pain, commonly in knee or wrist
- 🔸 Swelling and stiffness
- 🔸 No tophi
🧪 Diagnosis
- Joint aspiration: Calcium pyrophosphate crystals (rhomboid-shaped, positively birefringent)
- X-ray: Chondrocalcinosis (calcium deposits in cartilage)
🔷 🦠 8. SEPTIC ARTHRITIS
🔍 Signs & Symptoms
- 🔸 Sudden onset of severe joint pain
- 🔸 Swelling, redness, and fever
- 🔸 Limited ROM
- 🔸 Systemic signs: chills, malaise
🧪 Diagnosis
- Joint aspiration: Purulent fluid, elevated WBCs
- Gram stain/culture: Identify pathogen
- Blood culture: May be positive
- ESR/CRP: Elevated
- X-ray: May show joint space narrowing or effusion
🔷 🦟 9. LYME ARTHRITIS
🔍 Signs & Symptoms
- 🔸 History of tick bite or bullseye rash
- 🔸 Intermittent swelling/pain in knees or large joints
- 🔸 Fatigue, fever, headache (systemic signs)
🧪 Diagnosis
- ELISA for Lyme antibodies
- Western blot for confirmation
- Joint aspiration (in some cases)
- ESR/CRP: Elevated
🔷 🧫 10. TUBERCULAR ARTHRITIS
🔍 Signs & Symptoms
- 🔸 Chronic joint pain, often spine or large joints
- 🔸 Swelling, stiffness
- 🔸 Weight loss, low-grade fever, night sweats
- 🔸 Cold abscess (no heat or redness)
🧪 Diagnosis
- Joint aspiration: AFB stain, TB culture
- Mantoux test (positive)
- Chest X-ray (to check for pulmonary TB)
- ESR: Elevated
- MRI: Shows bone destruction, abscess
💊🦴 MEDICAL & SURGICAL MANAGEMENT OF ARTHRITIS
🔷 ✅ 1. OSTEOARTHRITIS (OA)
💊 Medical Management
- NSAIDs (e.g., ibuprofen, diclofenac) – for pain and inflammation
- Acetaminophen – for mild pain
- Topical analgesics – capsaicin, diclofenac gel
- Intra-articular corticosteroid injections – for acute inflammation
- Viscosupplementation (Hyaluronic acid injections) – for joint lubrication
- Glucosamine & chondroitin – as supportive supplements
- Weight loss and physical therapy
🛠️ Surgical Management
- Arthroscopy – to remove loose fragments or debris
- Osteotomy – realignment of bone for load redistribution
- Joint replacement (Arthroplasty) – Total Knee Replacement (TKR), Total Hip Replacement (THR)
🔷 🧬 2. RHEUMATOID ARTHRITIS (RA)
💊 Medical Management
- NSAIDs – for pain relief
- Corticosteroids – low-dose oral or intra-articular (e.g., prednisone)
- DMARDs (Disease-Modifying Antirheumatic Drugs):
- Methotrexate, Sulfasalazine, Leflunomide, Hydroxychloroquine
- Biologic agents (if DMARDs fail):
- TNF inhibitors (e.g., etanercept, infliximab), IL-6 inhibitors, JAK inhibitors
- Calcium + Vitamin D – for bone health
🛠️ Surgical Management
- Synovectomy – removal of inflamed synovial tissue
- Tendon repair or joint reconstruction – in advanced deformity
- Joint arthroplasty – for severely damaged joints
🔷 👶 3. JUVENILE IDIOPATHIC ARTHRITIS (JIA)
💊 Medical Management
- NSAIDs – naproxen, ibuprofen
- Corticosteroids – oral or intra-articular
- DMARDs – methotrexate
- Biologics – etanercept, adalimumab
- Physical therapy to prevent contractures
🛠️ Surgical Management
- Rare, but may include joint release surgery or joint replacement in severe cases
🔷 🎨 4. PSORIATIC ARTHRITIS
💊 Medical Management
- NSAIDs – first-line for mild cases
- DMARDs – methotrexate, sulfasalazine
- Biologic therapy – TNF inhibitors, IL-17 inhibitors
- Topical corticosteroids – for skin lesions
- UV therapy or retinoids – if skin involvement is severe
🛠️ Surgical Management
- Joint replacement surgery for advanced joint damage
- Synovectomy in localized disease
🔷 🧍 5. ANKYLOSING SPONDYLITIS (AS)
💊 Medical Management
- NSAIDs – indomethacin preferred
- DMARDs – sulfasalazine (mainly for peripheral joints)
- Biologics – anti-TNF drugs (etanercept, infliximab)
- Exercise and posture training – lifelong requirement
🛠️ Surgical Management
- Spinal osteotomy – for severe spinal deformity
- Hip joint replacement – if ankylosis affects mobility
🔷 💎 6. GOUT
💊 Medical Management
- Acute attack:
- NSAIDs (indomethacin), colchicine, corticosteroids
- Long-term management:
- Allopurinol or febuxostat (to lower uric acid)
- Probenecid (uricosuric)
- Low-purine diet, hydration, weight control
🛠️ Surgical Management
- Tophi excision – if large or infected
- Joint surgery – in advanced joint destruction
🔷 🧂 7. PSEUDOGOUT
💊 Medical Management
- NSAIDs – for acute attack
- Colchicine – for prevention
- Corticosteroids – oral or intra-articular
- Correct underlying metabolic issues (e.g., hemochromatosis, hyperparathyroidism)
🛠️ Surgical Management
- Rare; joint lavage or synovectomy may be considered in chronic cases
🔷 🦠 8. SEPTIC ARTHRITIS
💊 Medical Management
- IV antibiotics based on culture sensitivity
- (e.g., vancomycin, ceftriaxone)
- Analgesics, antipyretics
- Immobilization during acute phase
🛠️ Surgical Management
- Joint aspiration (arthrocentesis) – repeated to remove pus
- Arthroscopic washout or open drainage
- Synovectomy if chronic infection
🔷 🦟 9. LYME ARTHRITIS
💊 Medical Management
- Oral antibiotics: Doxycycline or amoxicillin
- IV ceftriaxone if neurological or late-stage
- NSAIDs – for symptom relief
🛠️ Surgical Management
- Rarely needed; arthroscopic synovectomy if persistent arthritis
🔷 🧫 10. TUBERCULAR ARTHRITIS
💊 Medical Management
- Anti-tubercular therapy (ATT) for 9–12 months
- NSAIDs for joint pain and inflammation
- Immobilization during active infection
🛠️ Surgical Management
- Joint debridement or drainage
- Synovectomy in non-responsive cases
- Joint reconstruction or arthrodesis in advanced destruction
👩⚕️🦴 NURSING MANAGEMENT OF ARTHRITIS
🔷 🎯 GOALS OF NURSING CARE
✅ Relieve joint pain and inflammation
✅ Preserve joint mobility and function
✅ Prevent deformities and complications
✅ Promote independence in daily activities
✅ Educate the patient for long-term self-care and lifestyle modification
🔷 📝 NURSING ASSESSMENT
🔍 Subjective Data:
- Location, severity, and duration of joint pain
- History of stiffness (morning or after rest)
- Fatigue, fever, or other systemic symptoms
- Impact on activities of daily living (ADLs)
🔍 Objective Data:
- Swelling, redness, warmth over joints
- Range of motion (ROM) limitations
- Deformities (e.g., ulnar deviation, nodules)
- Gait abnormalities or difficulty with movement
- Results of lab investigations (ESR, CRP, RF, uric acid)
🔷 🧰 NURSING INTERVENTIONS
💊 1. Pain and Inflammation Management
- Administer prescribed medications (NSAIDs, steroids, DMARDs, urate-lowering drugs, etc.)
- Monitor for side effects of long-term drug therapy (e.g., GI issues, immunosuppression)
- Use cold packs for acute inflammation and warm compresses for chronic stiffness
- Encourage joint rest during flare-ups and position joints with supportive pillows or splints
🏃♀️ 2. Promote Joint Mobility and Function
- Encourage active and passive ROM exercises as advised by physiotherapist
- Assist with ambulation aids (crutches, cane, walker) to reduce joint stress
- Prevent contractures and muscle wasting through daily mobility routines
- Educate about joint protection techniques (e.g., using larger joints, avoiding repetitive motions)
🍽️ 3. Nutrition and Weight Management
- Encourage a balanced, anti-inflammatory diet (rich in omega-3s, calcium, and vitamin D)
- Promote weight loss in obese patients to reduce stress on weight-bearing joints
- Teach about low-purine diets in patients with gout
🧠 4. Patient and Family Education
- Educate on:
- Medication compliance and regular follow-ups
- Proper use of heat/cold therapy
- Signs of flare-up or complications
- Lifestyle changes: exercise, posture, assistive devices
- Preventing falls and joint injuries at home
🛏️ 5. Assist with ADLs (Activities of Daily Living)
- Modify environment for safety and ease (e.g., grab bars, raised toilet seats)
- Assist with grooming, dressing, or bathing during flare-ups
- Encourage independence with proper techniques and assistive devices
🧾 6. Monitor and Evaluate
- Assess effectiveness of pain management strategies
- Monitor joint changes, side effects of medications, and patient adaptation
- Evaluate patient’s emotional response to chronic illness
- Coordinate multidisciplinary care (physio, ortho, dietician, rheumatologist)
🔷 📚 DISCHARGE TEACHING
✅ Importance of medication adherence
✅ When to report signs of flare-up or infection
✅ Use of exercise, braces, assistive devices
✅ How to perform home joint care safely
✅ Regular follow-up visits and lab monitoring
✅ Nutritional advice based on arthritis type (e.g., gout vs. RA)
🔷 💡 KEY POINTS FOR NURSES
✔ Arthritis is chronic, requires holistic care
✔ Nurses play a central role in symptom monitoring and patient support
✔ Early intervention prevents complications like joint deformities
✔ Patient education is critical for long-term disease control
✔ Emotional and psychological support enhances quality of life
⚠️🦴 COMPLICATIONS OF ARTHRITIS
If not properly managed, arthritis can lead to serious health problems affecting joints, organs, and quality of life.
🔷 ❗ MAJOR COMPLICATIONS BY TYPE
✅ Common to Most Types of Arthritis:
| Complication | Description |
|---|---|
| 1. Joint Deformity | Due to chronic inflammation (e.g., RA, PsA) causing cartilage and bone erosion. |
| 2. Joint Stiffness and Immobility | Due to fibrosis, disuse, or ankylosis. |
| 3. Functional Disability | Affects ability to perform daily activities, walk, or work. |
| 4. Muscle Atrophy | From disuse or immobilization of painful joints. |
| 5. Chronic Pain | Affects sleep, mood, and function. |
| 6. Depression/Anxiety | From chronic disease and disability. |
🔷 Type-Specific Complications:
| Type | Complications |
|---|---|
| Rheumatoid Arthritis | Extra-articular complications: nodules, lung fibrosis, pericarditis, anemia |
| Gout | Tophi (uric acid deposits), kidney stones, chronic joint damage |
| Osteoarthritis | Bone spurs, joint instability, falls in elderly |
| Ankylosing Spondylitis | Spinal fusion (bamboo spine), difficulty breathing, vision issues |
| Septic Arthritis | Rapid joint destruction, osteomyelitis, sepsis |
| Lupus Arthritis | Multisystem damage (kidneys, CNS, skin) |
✅✨ KEY POINTS TO REMEMBER (FOR NURSING & CLINICAL PRACTICE)
🔹 Arthritis is not just joint pain – it can be systemic and disabling.
🔹 Early diagnosis and treatment prevent long-term damage.
🔹 Rheumatoid and autoimmune arthritis need long-term immunosuppressive therapy.
🔹 Gout and pseudogout are metabolic; lifestyle changes are essential.
🔹 Infection-related arthritis needs prompt antibiotic and drainage.
🔹 Exercise, weight control, and assistive devices help maintain mobility.
🔹 Patient education is key for compliance, self-care, and flare-up prevention.
🔹 Multidisciplinary care (nurse, physiotherapist, rheumatologist, dietitian) ensures better outcomes.
🧘♂️🦴 SPECIAL THERAPIES FOR PATIENTS WITH MUSCULOSKELETAL PROBLEMS
🔷 🎯 GOALS OF SPECIAL THERAPIES
✅ Reduce pain and inflammation
✅ Restore joint mobility and muscle strength
✅ Promote independence in activities of daily living (ADLs)
✅ Prevent complications like contractures or atrophy
✅ Enhance overall quality of life
🔷 🧰 CATEGORIES OF SPECIAL THERAPIES
1️⃣ 🏃 PHYSIOTHERAPY (PHYSICAL THERAPY)
🧠 Core component of musculoskeletal rehabilitation
🔹 Techniques:
- Range of Motion (ROM) exercises – prevent joint stiffness
- Strengthening exercises – improve muscle power
- Stretching – improve flexibility and reduce contractures
- Postural training – especially important in spinal disorders
- Gait training – teaches proper walking with/without aids
- Hydrotherapy (pool therapy) – for arthritis, reduces joint stress
- Balance and coordination exercises – reduce fall risk
🔍 Indicated In:
- Arthritis, fractures, joint replacements, spinal disorders, contractures
2️⃣ 👐 OCCUPATIONAL THERAPY (OT)
🧠 Helps patients regain independence in daily life
🔹 Services:
- Training in ADLs – dressing, bathing, feeding
- Use of assistive devices – adapted utensils, dressing aids
- Energy conservation techniques – for fatigue-prone conditions
- Workplace/home modification – for safety and ease of access
- Splinting/positioning devices – prevent deformities
🔍 Indicated In:
- RA, stroke, spinal injuries, chronic pain, joint deformities
3️⃣ ❄️🔥 COLD AND HEAT THERAPY (CRYOTHERAPY & THERMOTHERAPY)
🔹 Cold Therapy (Cryotherapy)
- Reduces swelling and pain in acute injuries
- Used after sprains, strains, fractures, and surgeries
🔹 Heat Therapy (Thermotherapy)
- Increases blood flow and relieves chronic stiffness or muscle spasm
- Used in OA, chronic back pain, fibromyalgia
4️⃣ 🌀 ULTRASOUND THERAPY
🔹 Uses sound waves to deliver deep heat into tissues
- Promotes healing, reduces stiffness and pain
- Improves circulation and tissue repair
🔍 Indicated In:
- Tendonitis, bursitis, frozen shoulder, soft tissue injuries
5️⃣ ⚡ ELECTRICAL STIMULATION THERAPY
A. TENS (Transcutaneous Electrical Nerve Stimulation)
- Small electric pulses to block pain signals
- Non-invasive, patient-controlled therapy
B. NMES (Neuromuscular Electrical Stimulation)
- Stimulates weak muscles to maintain tone and prevent atrophy
🔍 Indicated In:
- Chronic pain, post-stroke rehab, post-surgical immobilization
6️⃣ 🌬️ RESPIRATORY THERAPY (For thoracic musculoskeletal issues)
- Breathing exercises – for patients with scoliosis or kyphosis
- Postural drainage & incentive spirometry – in immobile patients
- Prevents pulmonary complications
7️⃣ 🎨 RECREATIONAL & DIVERSIONAL THERAPY
🔹 Helps cope with chronic disability or pain
- Includes music therapy, art therapy, gardening, crafts
- Improves mental health and motivation
🔍 Used In:
- Long-term rehab units, elderly care, chronic pain conditions
8️⃣ 🧘♀️ YOGA AND MEDITATION
🔹 Improves flexibility, strength, posture, and mental relaxation
- Practices like asana, pranayama, and mindfulness meditation
- Reduces stress and improves coping with chronic illness
🔍 Beneficial In:
- OA, RA, fibromyalgia, chronic back pain
9️⃣ 🥗 NUTRITIONAL THERAPY
- Adequate calcium, vitamin D, and protein for bone healing
- Anti-inflammatory diet for arthritis (omega-3, antioxidants)
- Weight management to reduce load on joints
🔟 💬 PSYCHOLOGICAL COUNSELING & CBT
- Chronic musculoskeletal problems often lead to depression, anxiety, or frustration
- Cognitive Behavioral Therapy (CBT) helps in pain perception and coping
- Support groups enhance motivation and reduce isolation
✅ ✨ KEY POINTS FOR NURSES & CLINICIANS
✔ Always individualize therapy based on the patient’s age, condition, and goals
✔ Educate patients and families about therapies and self-care at home
✔ Monitor for improvements or adverse responses to therapy
✔ Encourage patient participation to build independence
✔ Collaboration with physiotherapists, occupational therapists, psychologists, dieticians is vital
🌿🧘♂️ ALTERNATIVE THERAPIES IN MUSCULOSKELETAL CARE

🔷 🎯 GOALS OF ALTERNATIVE THERAPIES
✅ Relieve chronic pain and inflammation
✅ Enhance physical and emotional well-being
✅ Improve joint flexibility and muscle tone
✅ Reduce drug dependency for pain management
✅ Support relaxation, sleep, and coping
🔷 🌿 1. AYURVEDA (Traditional Indian Medicine)
🔹 Key Elements:
- Abhyanga (Oil massage) – reduces stiffness, improves circulation
- Panchakarma therapy – detoxifies body (e.g., Virechana, Basti)
- Herbal medications – e.g., Shallaki (Boswellia), Ashwagandha, Guggulu
- Diet and lifestyle modifications based on dosha balance
🔍 Useful in:
- Osteoarthritis, Rheumatoid arthritis, back pain, muscle stiffness
🔷 🧘♀️ 2. YOGA THERAPY
🔹 Benefits:
- Improves flexibility, muscle strength, posture
- Reduces pain, stress, and stiffness
- Enhances breathing and mental clarity
🔹 Key Practices:
- Asanas – Trikonasana, Bhujangasana, Tadasana for joint support
- Pranayama – deep breathing to improve oxygenation and relaxation
- Meditation and mindfulness for coping with chronic conditions
🔷 💆 3. MASSAGE THERAPY
🔹 Techniques:
- Swedish massage – for general relaxation and circulation
- Deep tissue massage – targets muscle knots and chronic pain
- Trigger point therapy – relieves localized tightness
🔍 Benefits:
- Relieves muscle spasms, stiffness, improves mobility
- Stimulates blood flow and lymphatic drainage
🔷 🪷 4. ACUPUNCTURE & ACUPRESSURE (Traditional Chinese Medicine)
🔹 Acupuncture:
- Insertion of fine needles at specific energy points (meridians)
- Stimulates nerves and releases endorphins (natural painkillers)
🔹 Acupressure:
- Uses fingers instead of needles to apply pressure
🔍 Benefits:
- Pain relief, muscle relaxation, reduction of inflammation
🔷 🧂 5. NATUROPATHY
🔹 Therapies:
- Mud therapy – reduces joint swelling and pain
- Hydrotherapy – alternating hot/cold water compresses
- Sunlight therapy – improves vitamin D levels
- Diet correction – alkaline diet, anti-inflammatory foods
🔍 Useful in:
- Joint pain, gout, arthritis, post-injury recovery
🔷 🍵 6. HERBAL AND HOME REMEDIES
🔹 Common Herbs:
- Turmeric (Curcumin) – anti-inflammatory
- Ginger – pain relief and digestion
- Fenugreek, Castor oil packs, Epsom salt baths
🔍 Note:
- Use under guidance of qualified practitioner to avoid drug interactions
🔷 🎶 7. MUSIC, ART, AND DANCE THERAPY
🔹 Benefits:
- Reduce pain perception, elevate mood
- Encourage gentle movement and joint use (in dance therapy)
🔍 Useful in:
- Fibromyalgia, chronic arthritis, elderly rehab
🔷 🧠 8. MINDFULNESS & COGNITIVE BEHAVIORAL THERAPY (CBT)
🔹 Focuses on:
- Pain acceptance, stress reduction, and emotional coping
- Relaxation training, guided imagery, positive reframing
🔍 Effective in:
- Chronic musculoskeletal pain, fibromyalgia, post-surgical recovery
🔷 🪙 9. CHIROPRACTIC CARE
- Manual adjustments of the spine or joints
- Improves posture, alignment, and movement
- Caution: Not advised in osteoporosis or inflammatory arthritis
✅ ✨ KEY POINTS FOR USING ALTERNATIVE THERAPIES
✔ Use as complementary, not substitute for medical therapy
✔ Must be customized to patient’s condition, age, and safety
✔ Always check for herb-drug interactions and contraindications
✔ Emphasize qualified, licensed practitioners
✔ Ideal for long-term relief, promoting self-care and empowerment
🦴⚠️ OSTEOPOROSIS
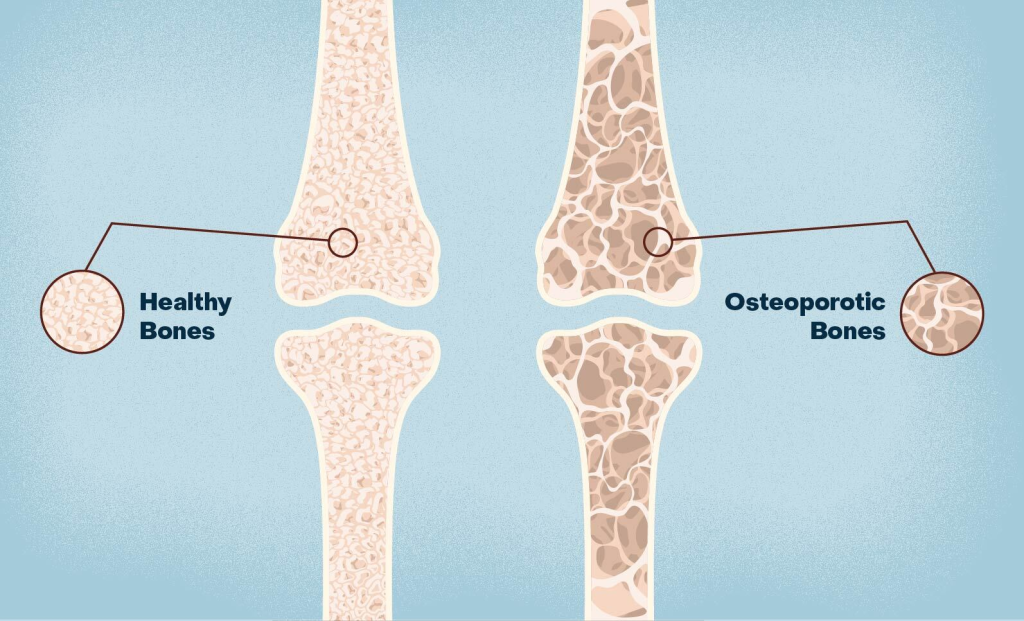
🔷 📘 DEFINITION
Osteoporosis is a systemic skeletal disorder characterized by low bone mass, microarchitectural deterioration of bone tissue, and increased bone fragility, leading to a higher risk of fractures.
🧪 Bones become porous, brittle, and fragile, often breaking from minor stress or trauma.
🔷 🧾 CAUSES OF OSTEOPOROSIS
✅ 1. Primary Causes (Age-related / Natural Causes)
| Type | Explanation |
|---|---|
| Postmenopausal (Type I) | Due to estrogen deficiency after menopause (common in women over 50) |
| Senile (Type II) | Due to age-related bone loss in both men and women over age 70 |
⚠️ 2. Secondary Causes (Underlying Diseases or Medications)
| Cause Category | Examples |
|---|---|
| 🧬 Endocrine Disorders | Hyperparathyroidism, Cushing’s syndrome, diabetes, thyrotoxicosis |
| 💊 Medications | Long-term corticosteroids, anticonvulsants, proton pump inhibitors |
| 🧂 Nutritional Deficiencies | Calcium, vitamin D, protein, malnutrition |
| 🚭 Lifestyle Factors | Smoking, alcohol, sedentary lifestyle, excess caffeine intake |
| 🩺 Other Diseases | Chronic kidney disease, rheumatoid arthritis, malabsorption (e.g., celiac disease) |
| 👶 Genetic Disorders | Osteogenesis imperfecta (in children), familial osteoporosis |
🔷 🧱 TYPES OF OSTEOPOROSIS
| Type | Description |
|---|---|
| 1. Primary Osteoporosis | Most common type; age-related or postmenopausal bone loss without identifiable disease |
| 2. Secondary Osteoporosis | Caused by medical conditions or medications that interfere with bone metabolism |
| 3. Idiopathic Osteoporosis | Rare, usually in children or young adults without clear cause |
| 4. Juvenile Osteoporosis | Occurs in growing children/teens; can be due to genetic or nutritional issues |
| 5. Localized Osteoporosis | Occurs in a specific part of the skeleton due to immobilization or localized trauma |
| 6. Disuse Osteoporosis | Caused by prolonged immobility or paralysis (e.g., in bedridden patients) |
🔷 🧬 PATHOPHYSIOLOGY OF OSTEOPOROSIS
Osteoporosis results from an imbalance between bone resorption and bone formation, favoring bone loss.
🔁 Normal Bone Remodeling:
- Bone tissue is constantly remodeled through the coordinated activity of:
- Osteoclasts (break down bone)
- Osteoblasts (build new bone)
🔍 In Osteoporosis:
- Estrogen deficiency (in postmenopausal women) or age-related decline in osteoblast activity
- ➡️ Increased osteoclastic activity (more bone resorption)
- ➡️ Decreased osteoblastic activity (less bone formation)
- ➡️ Loss of bone mineral density (BMD) and thinning of trabecular (spongy) bone
- ➡️ Bones become porous, fragile, and fracture-prone, especially in the spine, hip, and wrist
🔷 🩺 SIGNS AND SYMPTOMS
Osteoporosis is often called the “silent disease” because it may remain asymptomatic until a fracture occurs.
🔍 Common Symptoms:
| Symptom | Description |
|---|---|
| ❗ Fractures | Especially of the spine, hip, and wrist from minor falls or trauma |
| ↘️ Loss of height | Due to compression fractures in vertebrae |
| 🔄 Kyphosis (Dowager’s hump) | Curvature of upper spine from vertebral collapse |
| ⚠️ Back pain | Sudden or chronic pain due to vertebral fractures |
| 🧍♀️ Postural changes | Stooped posture or difficulty standing upright |
| 🚶♀️ Impaired mobility | Fear of falling, reduced independence |
🔷 🧪 DIAGNOSIS OF OSTEOPOROSIS
Diagnosis is based on clinical history, physical examination, and bone mineral density (BMD) testing.
| Diagnostic Tool | Purpose |
|---|---|
| 🧪 Dual-energy X-ray Absorptiometry (DEXA) | Gold standard for measuring BMD (hip and spine). T-score ≤ -2.5 confirms osteoporosis |
| 📈 FRAX Score (WHO Tool) | Assesses 10-year fracture risk based on clinical factors + BMD |
| 🩻 X-rays | May show fractures, bone thinning, and vertebral compression (only in advanced stages) |
| 🧬 Blood Tests | Rule out secondary causes: |
| – Calcium, phosphate | |
| – Vitamin D levels | |
| – Parathyroid hormone (PTH) | |
| – Thyroid function tests | |
| – Renal function | |
| – Serum protein electrophoresis (if suspecting multiple myeloma) |
🔷 💊 MEDICAL MANAGEMENT
The goals of medical therapy are to:
✅ Prevent fractures
✅ Preserve or increase bone density
✅ Reduce bone pain
✅ Treat underlying causes (e.g., hormone deficiency, nutritional deficits)
🧂 1. Calcium and Vitamin D Supplementation
- Calcium: 1000–1500 mg/day (diet + supplements)
- Vitamin D3: 800–2000 IU/day (aids calcium absorption)
- Essential for bone mineralization and fracture prevention
🧬 2. Anti-Resorptive Drugs (Prevent Bone Loss)
| Drug Class | Examples | Action |
|---|---|---|
| Bisphosphonates | Alendronate, Risedronate, Ibandronate, Zoledronic acid | Inhibit osteoclasts, reduce bone breakdown |
| Selective Estrogen Receptor Modulators (SERMs) | Raloxifene | Mimic estrogen’s protective effects on bone |
| Calcitonin | Nasal spray or injection | Decreases osteoclastic activity; mild analgesic in vertebral fracture pain |
| Denosumab | SC injection every 6 months | Monoclonal antibody that inhibits RANKL → prevents osteoclast formation |
🦴 3. Anabolic Agents (Promote Bone Formation)
| Drug | Action |
|---|---|
| Teriparatide (PTH analog) | Stimulates new bone formation (used for severe osteoporosis) |
| Romosozumab | New agent that increases bone formation and decreases resorption |
📦 4. Hormone Replacement Therapy (HRT)
- Estrogen + progesterone in postmenopausal women (short-term use)
- Not first-line due to risk of cardiovascular disease, breast cancer
🍏 5. Lifestyle & Supportive Measures
- Weight-bearing exercises (walking, stair climbing)
- Smoking cessation
- Limiting alcohol and caffeine
- Fall prevention strategies: safe home setup, proper footwear
🔷 🛠️ SURGICAL MANAGEMENT
Surgery is indicated when there are osteoporotic fractures causing pain, deformity, or functional limitations.
🦴 1. Vertebroplasty
- Minimally invasive procedure
- Cement is injected into fractured vertebra to stabilize and reduce pain
- No correction of deformity
🦴 2. Kyphoplasty
- Similar to vertebroplasty, but uses a balloon to restore vertebral height before injecting cement
- Used in vertebral compression fractures
⚒️ 3. Fracture Fixation or Joint Replacement
- Open reduction and internal fixation (ORIF) for hip or wrist fractures
- Total hip/knee replacement if joint is severely damaged
- Spinal stabilization surgeries in multiple vertebral fractures
✅ ✨ KEY POINTS TO REMEMBER
✔ Medical treatment must be long-term and consistent
✔ Bisphosphonates are first-line drugs but require correct administration (empty stomach, upright posture)
✔ Monitor renal function when using bisphosphonates or calcium supplements
✔ Surgical intervention is mainly for fracture stabilization and pain relief
👩⚕️🦴 NURSING MANAGEMENT OF OSTEOPOROSIS
🔷 🎯 GOALS OF NURSING CARE
✅ Prevent fractures and falls
✅ Relieve pain and discomfort
✅ Promote mobility and physical activity
✅ Improve nutritional status for bone health
✅ Educate the patient and family for long-term self-care and prevention
🔷 📝 NURSING ASSESSMENT
🔍 Subjective Data:
- Reports of back pain, joint pain, or reduced height
- History of fractures, immobility, or menopause
- Lifestyle: smoking, alcohol, diet, physical activity level
🔍 Objective Data:
- Postural changes (kyphosis, stooping)
- Limited ROM or difficulty walking
- Fall history or use of mobility aids
- Diagnostic reports (DEXA scan, calcium/vitamin D levels)
🔷 🧰 NURSING INTERVENTIONS
🛡️ 1. Fall and Fracture Prevention
- Ensure safe environment: non-slip mats, grab bars, adequate lighting
- Use of walking aids or assistive devices as needed
- Encourage slow movements and correct posture
- Educate family/caregivers on safety precautions at home
💊 2. Medication Administration and Monitoring
- Administer prescribed medications (e.g., calcium, vitamin D, bisphosphonates)
- Instruct to take bisphosphonates on an empty stomach, with water, and remain upright for 30 mins
- Monitor for side effects: GI upset, jaw pain (osteonecrosis), allergic reactions
- Encourage regular follow-up for DEXA scans and blood work
🧘♀️ 3. Promote Physical Activity and Mobility
- Encourage weight-bearing exercises (walking, mild aerobics)
- Collaborate with physiotherapist for ROM and strengthening exercises
- Avoid high-impact or twisting activities that may increase fracture risk
- Assist patient in maintaining independence in ADLs
🥗 4. Nutrition and Lifestyle Counseling
- Promote intake of calcium-rich foods (milk, leafy greens, tofu, yogurt)
- Ensure vitamin D through diet and safe sun exposure
- Counsel on avoiding smoking, excessive alcohol, caffeine
- Educate on hydration and preventing constipation (especially when taking calcium)
🧠 5. Health Education and Counseling
- Explain the chronic nature of osteoporosis and need for long-term care
- Educate about:
- Fall prevention strategies
- Proper medication usage and compliance
- Signs of new fractures to report early
- Importance of routine BMD (DEXA) testing
📋 6. Psychosocial and Emotional Support
- Provide emotional reassurance to reduce fear of falling
- Encourage participation in support groups
- Address body image issues in patients with postural deformities
🔷 📚 DISCHARGE TEACHING
✅ Take all medications as prescribed
✅ Maintain a bone-healthy diet and exercise plan
✅ Report new pain, height loss, or falls
✅ Schedule regular bone density checks
✅ Modify home for safety (rugs, stairs, lighting)
🔷 💡 KEY POINTS FOR NURSING CARE
✔ Osteoporosis is chronic and silent until fractures occur — focus on prevention
✔ Fall prevention is a top priority in elderly patients
✔ Nutrition, exercise, and lifestyle modifications are pillars of care
✔ Nurses must emphasize education and compliance for long-term management
✔ A holistic and multidisciplinary approach leads to better outcomes
⚠️🦴 COMPLICATIONS OF OSTEOPOROSIS
Osteoporosis is often silent until complications arise — usually in the form of fragility fractures that can lead to disability, loss of independence, or death, especially in elderly patients.
🔷 ❗ MAJOR COMPLICATIONS
| Complication | Description |
|---|---|
| 1. Fragility Fractures | Most common; caused by minor falls or even normal activities |
| ➤ Vertebral Fractures | Result in height loss, kyphosis (“dowager’s hump”), chronic back pain |
| ➤ Hip Fractures | High risk in elderly; often requires surgery; associated with immobility and high mortality |
| ➤ Wrist Fractures | Common in early stages, especially in postmenopausal women |
| 2. Chronic Pain | From vertebral collapse or multiple microfractures |
| 3. Postural Changes | Kyphosis leading to respiratory compromise and poor balance |
| 4. Reduced Mobility | Leads to deconditioning, muscle wasting, increased fall risk |
| 5. Depression & Anxiety | From chronic pain and loss of independence |
| 6. Loss of Independence | May result in institutionalization or long-term care needs |
| 7. Surgical Complications | From fracture repair or hip replacement, especially in the elderly |
✅✨ KEY POINTS TO REMEMBER
✔ Osteoporosis = “Silent disease” until fracture occurs — early screening is essential
✔ Postmenopausal women and elderly are at highest risk
✔ DEXA scan is the gold standard for diagnosis (T-score ≤ -2.5)
✔ Calcium + Vitamin D, bisphosphonates, and lifestyle changes are key in prevention and treatment
✔ Fall prevention is the most important nursing intervention
✔ Encourage weight-bearing exercises to strengthen bones
✔ Monitor for drug side effects, especially GI issues and osteonecrosis of jaw with bisphosphonates
✔ Educate patients about safe home environments and medication adherence
✔ Multidisciplinary care involving nurses, physiotherapists, nutritionists, and physicians improves outcomes
✔ Regular follow-ups and bone density assessments are necessary for long-term management
🦴🌑 OSTEOMALACIA
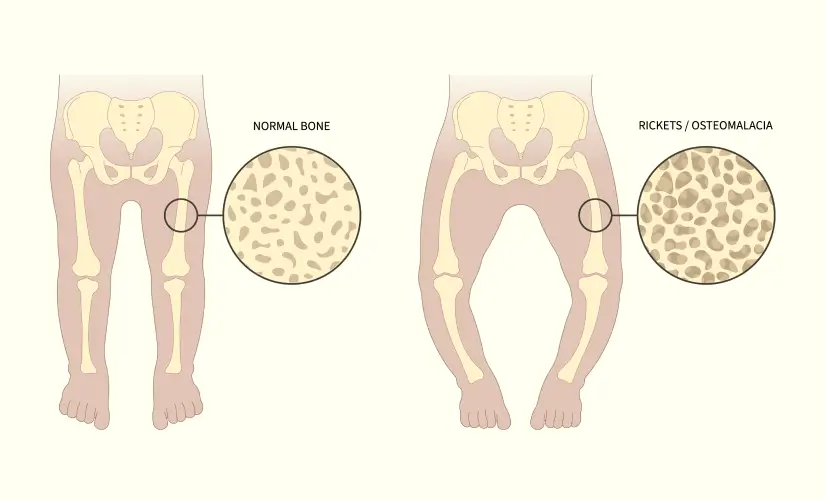
🔷 📘 DEFINITION
Osteomalacia is a metabolic bone disorder characterized by softening of bones in adults due to defective bone mineralization, primarily caused by vitamin D deficiency or phosphate metabolism disorders.
🧪 It results in inadequate calcium and phosphate deposition in the bone matrix, leading to bone pain, fractures, and muscle weakness.
🔍 In children, a similar condition is called Rickets.
🔷 ❗ CAUSES OF OSTEOMALACIA
Osteomalacia usually develops from impaired bone mineralization, caused by one or more of the following:
✅ 1. Nutritional Deficiencies
- Vitamin D deficiency – most common cause
- Calcium deficiency – due to poor diet or absorption
- Phosphorus deficiency – rare, but seen in certain disorders
🚫 2. Malabsorption Syndromes
- Celiac disease
- Crohn’s disease
- Chronic pancreatitis
- Post-gastrointestinal surgeries (e.g., gastric bypass)
🦠 3. Chronic Kidney Disease (CKD)
- Leads to secondary hyperparathyroidism and impaired vitamin D activation
- Causes renal osteodystrophy (bone changes due to CKD)
💊 4. Medications
- Anticonvulsants (phenytoin, phenobarbital)
- Long-term use of aluminum-containing antacids
- Glucocorticoids – inhibit bone formation and vitamin D metabolism
⚙️ 5. Genetic or Inherited Disorders
- Hypophosphatemic osteomalacia
- Vitamin D–resistant rickets
- Familial renal tubular acidosis
🔷 🧬 TYPES OF OSTEOMALACIA
| Type | Description |
|---|---|
| 1. Nutritional Osteomalacia | Due to dietary deficiency of vitamin D, calcium, or phosphate (most common type) |
| 2. Renal Osteomalacia | Due to chronic kidney disease causing poor phosphate reabsorption and impaired vitamin D activation |
| 3. Drug-Induced Osteomalacia | Caused by medications interfering with vitamin D metabolism or phosphate levels |
| 4. Tumor-Induced Osteomalacia | Rare, caused by phosphaturic mesenchymal tumors that secrete substances impairing phosphate metabolism |
| 5. Genetic/Inherited Forms | X-linked hypophosphatemic rickets (in adults), vitamin D–resistant osteomalacia |
🔷 🧬 PATHOPHYSIOLOGY OF OSTEOMALACIA
- 🧪 Vitamin D deficiency or impaired metabolism
→ leads to reduced intestinal calcium and phosphate absorption - ⬇️ Hypocalcemia
→ stimulates parathyroid hormone (PTH) secretion - 🔄 PTH increases bone resorption to maintain serum calcium
→ results in bone demineralization and softening - 🧱 New bone matrix (osteoid) is formed by osteoblasts but remains poorly mineralized
→ leads to weak, soft, and pliable bones - ⚠️ Results in bone pain, deformities, fractures, and muscle weakness
🔍 In renal osteomalacia, phosphate loss and reduced vitamin D activation worsen mineralization defects.
🔷 🩺 SIGNS AND SYMPTOMS
Osteomalacia develops gradually and symptoms may be non-specific in early stages.
| Symptom | Description |
|---|---|
| 🔴 Bone pain | Especially in the lower back, hips, pelvis, legs, and ribs; dull, aching, worsens with movement |
| ❗ Muscle weakness | Usually proximal muscles (e.g., thighs, shoulders), leading to difficulty standing or climbing stairs |
| ↘️ Difficulty walking | Waddling gait, due to weakened pelvic and leg muscles |
| 🚶 Frequent falls or instability | Due to weak bones and poor muscle support |
| 🦴 Bone tenderness | On palpation, especially over long bones |
| ❗ Fragility fractures | Especially in ribs, spine, pelvis, and femur |
| ⛓️ Skeletal deformities | Bowed legs or spinal curvature in chronic/severe cases |
| 😴 Fatigue | Due to poor muscle function and chronic pain |
🔷 🧪 DIAGNOSIS OF OSTEOMALACIA
🧬 1. Blood Tests
| Test | Expected Findings |
|---|---|
| Serum calcium | ↓ Low or borderline low |
| Serum phosphate | ↓ Often low (especially in renal causes) |
| Alkaline phosphatase (ALP) | ↑ Elevated (marker of increased bone turnover) |
| Vitamin D (25-OH) | ↓ Deficient levels |
| Parathyroid hormone (PTH) | ↑ Elevated (secondary hyperparathyroidism) |
🔍 2. Urine Tests
- Low calcium and phosphate reabsorption in renal osteomalacia
- Increased phosphate excretion in tumor-induced osteomalacia
🖥️ 3. Imaging
| Imaging Test | Findings |
|---|---|
| X-ray | Looser’s zones (pseudofractures), generalized bone demineralization |
| DEXA scan | Shows reduced bone mineral density (similar to osteoporosis) |
| Bone scan | Increased uptake in multiple skeletal areas |
| MRI/CT | If tumor-induced osteomalacia is suspected |
🔬 4. Bone Biopsy (Rarely Needed)
- Confirms diagnosis in unclear or complex cases
- Shows excess unmineralized osteoid
🔷 💊 MEDICAL MANAGEMENT
The goals of treatment are to:
✅ Correct the underlying cause
✅ Restore normal bone mineralization
✅ Relieve pain and muscle weakness
✅ Prevent fractures and skeletal deformities
🔹 1. Vitamin D Supplementation (Cornerstone Therapy)
| Type | Route & Dosage |
|---|---|
| Cholecalciferol (Vitamin D₃) | Oral: 1000–2000 IU/day or high-dose weekly therapy for deficiency |
| Ergocalciferol (Vitamin D₂) | Used in some cases depending on availability |
| Calcitriol (1,25-dihydroxy D) | Used in renal osteodystrophy or vitamin D–resistant osteomalacia |
📌 Sunlight exposure (15–20 minutes/day) is also encouraged when possible.
🔹 2. Calcium Supplementation
- Calcium carbonate or calcium citrate: 1000–1500 mg/day
- Ensures adequate bone mineralization
- Should be taken with meals for better absorption
🔹 3. Phosphate Supplements (For hypophosphatemic osteomalacia)
- Used only when phosphate deficiency is documented
- Often combined with vitamin D analogs in resistant cases
- Requires careful monitoring to avoid secondary hyperparathyroidism
🔹 4. Treat Underlying Conditions
| Condition | Treatment |
|---|---|
| Malabsorption syndromes | Gluten-free diet (in celiac), pancreatic enzymes |
| Chronic kidney disease | Phosphate binders, calcitriol, dialysis if needed |
| Drug-induced osteomalacia | Discontinue offending drugs (e.g., anticonvulsants, aluminum antacids) |
| Tumor-induced osteomalacia | Locate and remove tumor (see surgery) |
🔹 5. Pain and Symptom Management
- NSAIDs or mild analgesics for bone/muscle pain
- Physiotherapy to improve muscle strength and gait
- Orthotic devices or braces to support weakened bones
- Fall prevention strategies in elderly patients
🔷 🛠️ SURGICAL MANAGEMENT
Surgery is not usually required in most cases of osteomalacia but may be necessary in the following conditions:
🦴 1. Fracture Repair
- If osteomalacia has led to pathologic or stress fractures
- Internal fixation (e.g., plates, screws) may be needed to stabilize bones
- Bone healing may be delayed, requiring longer recovery
🧠 2. Correction of Skeletal Deformities
- In severe or long-standing cases with bone bowing or spinal curvature
- Osteotomy may be performed to realign bones
🔬 3. Tumor Removal
- For oncogenic (tumor-induced) osteomalacia caused by phosphaturic mesenchymal tumors
- Tumor resection often leads to complete reversal of the condition
✅ ✨ KEY NURSING POINTS IN MANAGEMENT
✔ Ensure compliance with vitamin D and calcium therapy
✔ Monitor for hypercalcemia during supplementation
✔ Educate on diet, sunlight exposure, and physical activity
✔ Support with mobility aids to prevent falls
✔ Coordinate multidisciplinary care (endocrinologist, dietician, physiotherapist, orthopedic surgeon)
👩⚕️🦴 NURSING MANAGEMENT OF OSTEOMALACIA
🔷 🎯 GOALS OF NURSING CARE
✅ Relieve bone pain and muscle weakness
✅ Prevent falls and fractures
✅ Improve nutritional status
✅ Promote mobility and independence
✅ Educate the patient and family for long-term self-care and prevention
🔷 📝 NURSING ASSESSMENT
🔍 Subjective Data
- Bone pain (especially in hips, back, and legs)
- Fatigue and difficulty walking or rising from a seated position
- History of fractures, poor diet, or sun avoidance
- History of chronic illness or long-term medications (e.g., anticonvulsants)
🔍 Objective Data
- Muscle weakness (especially proximal muscles)
- Waddling gait or gait instability
- Skeletal deformities (e.g., bowed legs, kyphosis)
- Lab values: low calcium, phosphate, vitamin D; elevated ALP
🔷 🧰 NURSING INTERVENTIONS
💊 1. Medication and Supplementation Support
- Administer vitamin D (cholecalciferol/calcitriol) and calcium as prescribed
- Monitor for signs of hypercalcemia: nausea, vomiting, confusion
- Educate on proper timing and dosing (e.g., calcium with food)
- Emphasize adherence to treatment regimen for months to years
🥗 2. Nutritional Support
- Encourage calcium-rich foods: milk, cheese, leafy greens, fish with bones
- Encourage vitamin D-rich foods: eggs, fortified cereals, oily fish
- Refer to a dietitian if patient has malabsorption or complex needs
- Promote adequate protein intake to support muscle strength
☀️ 3. Sunlight Exposure Guidance
- Educate on safe, moderate sunlight exposure (15–20 minutes/day)
- Expose face, arms, and legs if culturally acceptable
- Monitor for patients who may need vitamin D alternatives (e.g., renal failure, indoor patients)
🚶 4. Mobility and Fall Prevention
- Encourage gentle, progressive physical activity to improve strength and mobility
- Provide mobility aids (walker, cane) for balance and fall prevention
- Modify home environment: good lighting, remove rugs, install grab bars
- Reassure and assist with ADLs as needed to prevent fatigue and injury
📚 5. Patient & Family Education
- Explain the nature of the disease and importance of long-term therapy
- Teach correct medication usage and food sources of calcium and vitamin D
- Discuss potential causes (e.g., malabsorption, kidney disease) if applicable
- Stress the importance of regular follow-up and lab monitoring
🧠 6. Psychosocial Support
- Provide emotional reassurance for those with deformity or limited mobility
- Encourage participation in support groups or community rehab programs
- Address fear of falling or dependency, especially in older adults
🔷 📋 DISCHARGE TEACHING
✅ Continue vitamin D/calcium therapy as prescribed
✅ Eat a balanced, bone-friendly diet
✅ Perform safe home exercises to build muscle strength
✅ Be aware of signs of worsening (new fractures, weakness, bone pain)
✅ Attend regular follow-up appointments and lab checks
✅ Maintain a safe environment to prevent injuries
🔷 💡 KEY NURSING POINTS
✔ Osteomalacia is treatable if recognized early — nurses play a key role in early identification
✔ Focus on diet, sunlight, and medication compliance
✔ Ensure fall prevention and mobility assistance at all stages
✔ Monitor lab values regularly to assess treatment effectiveness
✔ Provide compassionate care for those with chronic pain and limited independence
⚠️🦴 COMPLICATIONS OF OSTEOMALACIA
If left untreated or undiagnosed, osteomalacia can lead to progressive skeletal weakening and serious complications.
🔷 ❗ MAJOR COMPLICATIONS
| 🛑 Complication | 📋 Description |
|---|---|
| 1. Pathological Fractures | Bones may break with minimal or no trauma (especially in ribs, hips, pelvis, and spine) |
| 2. Skeletal Deformities | Bowing of legs, kyphosis, and spinal curvature due to prolonged softening of bones |
| 3. Chronic Bone Pain | Persistent pain that limits mobility and affects quality of life |
| 4. Muscle Weakness | Especially in proximal muscles (thighs, shoulders), leading to gait instability |
| 5. Gait Abnormalities | Waddling gait, difficulty standing or climbing stairs |
| 6. Increased Fall Risk | Due to weak bones and reduced muscle strength |
| 7. Secondary Hyperparathyroidism | Overactive parathyroid due to chronic hypocalcemia, further weakening bones |
| 8. Delayed Bone Healing | Fractures take longer to heal due to poor mineralization |
| 9. Functional Disability | In advanced or neglected cases, can lead to loss of independence |
✅✨ KEY POINTS TO REMEMBER
✔ Osteomalacia = Soft bones due to defective mineralization (commonly from vitamin D deficiency)
✔ It is most common in adults, especially elderly, people with poor diets, or limited sunlight exposure
✔ Rickets is the equivalent disorder in children
✔ Signs include bone pain, muscle weakness, fractures, waddling gait, and skeletal deformities
✔ Lab findings:
‣ ↓ Calcium, ↓ Phosphate, ↓ Vitamin D
‣ ↑ Alkaline phosphatase
‣ ↑ PTH (secondary hyperparathyroidism)
✔ Treatment = Vitamin D + calcium supplementation, sunlight exposure, and addressing underlying causes
✔ Nurses should focus on:
‣ Fall prevention
‣ Medication compliance
‣ Nutritional counseling
‣ Promoting safe activity
‣ Educating on lifestyle changes
✔ Early recognition and treatment can reverse bone changes and prevent disability
🦴🔄 PAGET’S DISEASE OF BONE (OSTEITIS DEFORMANS)

🔷 📘 DEFINITION
Paget’s disease of bone is a chronic metabolic disorder characterized by abnormal bone remodeling, where there is excessive bone resorption followed by disorganized and excessive bone formation.
🧱 This results in bones that are enlarged, structurally weak, and deformed, making them more susceptible to pain, fractures, and arthritis.
🔷 ❗ CAUSES OF PAGET’S DISEASE
The exact cause is unknown, but the disease appears to result from a combination of genetic, viral, and environmental factors.
✅ 1. Genetic Factors
- Positive family history is seen in up to 25–40% of patients
- Associated genetic mutations:
- SQSTM1 gene mutation (affects osteoclast activity)
- TNFRSF11A gene
🦠 2. Viral Infections (Theoretical)
- Some evidence suggests a slow viral infection of osteoclasts (e.g., paramyxoviruses like measles virus) may trigger the disease in genetically predisposed individuals
🌍 3. Environmental Factors
- More common in Europe, North America, and Australia
- Rare in Scandinavia, Africa, and Asia
- Possibly related to diet, pollution, or mineral exposure
🔄 4. Age and Gender
- Affects people over 50 years of age
- Slightly more common in men than women
🔷 🧬 TYPES OF PAGET’S DISEASE
| Type | Description |
|---|---|
| 1. Monostotic Paget’s Disease | Involves only one bone (e.g., femur, tibia, skull) – seen in 35% of cases |
| 2. Polyostotic Paget’s Disease | Involves multiple bones – more common form |
| 3. Familial Paget’s Disease | Inherited type, runs in families (autosomal dominant) |
| 4. Juvenile Paget’s Disease | Extremely rare; occurs in infancy or childhood due to genetic mutations; causes rapid bone turnover and deformity early in life |
🔷 🧬 PATHOPHYSIOLOGY
Paget’s disease involves abnormal bone remodeling in three distinct phases:
1️⃣ Lytic Phase (Osteoclastic Activity ↑)
- Increased activity of abnormally large osteoclasts
- Excessive bone resorption
- Bone becomes porous and weakened
2️⃣ Mixed Phase (Osteoclast + Osteoblast activity ↑)
- Compensatory increase in osteoblastic activity
- New bone is laid down disorganizedly (woven bone)
- Bone becomes enlarged but structurally weak
3️⃣ Sclerotic Phase (Osteoblastic activity > Osteoclastic)
- Irregular bone thickening and marrow fibrosis
- Bone appears dense on X-ray but lacks strength
- Risk of deformities, fractures, and nerve compression
🔄 Bone turnover rate is up to 20 times faster than normal in affected areas.
📍 Commonly affected bones:
- Skull, spine, pelvis, femur, tibia
🔷 🩺 SIGNS AND SYMPTOMS
Paget’s disease may be asymptomatic in early stages and is often discovered incidentally on X-rays or blood tests.
✅ Common Symptoms:
| Symptom | Description |
|---|---|
| 🦴 Bone pain | Most common symptom; deep, aching pain; worsens at night |
| 🦶 Bone deformities | Bowing of long bones, skull enlargement, spinal kyphosis |
| ↘️ Height loss | Due to spinal compression or vertebral collapse |
| 💥 Fractures | Especially in weight-bearing bones (femur, pelvis) due to weakness |
| 🧠 Skull involvement | Enlargement, headaches, hearing loss (due to nerve compression) |
| 🚶 Gait disturbances | From leg bowing or pelvic deformities |
| 🔄 Joint stiffness or arthritis | Secondary osteoarthritis in nearby joints |
| 🔊 Tinnitus or dizziness | Due to skull base involvement affecting inner ear structures |
🔷 🧪 DIAGNOSIS OF PAGET’S DISEASE
🧬 1. Blood Tests
| Test | Result |
|---|---|
| Serum alkaline phosphatase (ALP) | ↑ Elevated (reflects high bone turnover) |
| Serum calcium and phosphate | Usually normal (unless complications occur) |
| Serum P1NP and CTX | Markers of bone formation/resorption (used for monitoring) |
🧪 2. Urine Tests
- Urinary hydroxyproline or deoxypyridinoline may be elevated (markers of bone breakdown)
🖥️ 3. Imaging Studies
| Imaging Test | Findings |
|---|---|
| X-ray | Classic “mosaic” or “cotton wool” appearance, bone expansion, cortical thickening |
| Bone scan (Radionuclide) | Identifies extent of bone involvement — shows areas of increased uptake |
| CT or MRI | Used if neurological complications are suspected (e.g., spinal stenosis, hearing loss) |
🔍 4. Biopsy (Rarely Required)
- Performed only when malignancy (Paget’s sarcoma) or other pathology is suspected
🔷 💊 MEDICAL MANAGEMENT
The main goals of treatment are to:
✅ Reduce bone turnover
✅ Relieve bone pain
✅ Prevent complications such as fractures and deformities
✅ Preserve function and quality of life
🔹 1. Bisphosphonates (First-line Therapy)
| Drug Name | Route & Dose |
|---|---|
| Alendronate | Oral, 40 mg/day for 6 months |
| Risedronate | Oral, 30 mg/day for 2 months |
| Pamidronate | IV infusion for severe cases |
| Zoledronic acid | Single IV infusion – highly effective, long-lasting |
📌 They inhibit osteoclast-mediated bone resorption, normalize ALP levels, and reduce bone pain.
🔹 2. Calcitonin (Second-line or adjunct)
- SC or intranasal spray
- Reduces osteoclastic activity
- Used when bisphosphonates are contraindicated (e.g., renal insufficiency)
🔹 3. Pain Management
- NSAIDs (e.g., ibuprofen, naproxen)
- Acetaminophen for mild to moderate bone pain
- Opioids for severe pain if not responsive to other therapy
🔹 4. Supplementation
- Calcium (1000–1500 mg/day)
- Vitamin D (800–1000 IU/day)
- Ensures adequate bone mineralization during anti-resorptive therapy
🔹 5. Monitoring
- Serum alkaline phosphatase (ALP) to assess response
- Periodic bone scans or X-rays to monitor progression
- Check renal function if on bisphosphonates
🔷 🛠️ SURGICAL MANAGEMENT
Surgery is considered when complications arise due to deformity, fracture, or nerve compression.
🦴 1. Fracture Repair
- Open reduction and internal fixation (ORIF) for pathologic fractures
- Bone healing may be delayed, so careful surgical planning is needed
🧍♂️ 2. Joint Replacement
- Total hip or knee arthroplasty if severe arthritis develops from misalignment or joint degeneration
🧠 3. Decompression Surgery
- For neurological complications such as spinal stenosis or cranial nerve compression (e.g., hearing loss from skull involvement)
🔧 4. Osteotomy
- Corrective surgery to realign deformed bones, especially in the femur or tibia
🔍 5. Tumor Resection (Rare)
- In case of sarcomatous transformation (Paget’s sarcoma), which is rare but aggressive
- Requires oncology and orthopedic collaboration
✅✨ KEY NURSING POINTS IN MANAGEMENT
✔ Educate patient about long-term nature of disease and medication compliance
✔ Monitor for bisphosphonate side effects (GI irritation, jaw osteonecrosis, renal dysfunction)
✔ Encourage safe activity, fall prevention, and assistive devices
✔ Support pain management and emotional coping for chronic illness
✔ Regular follow-up with labs and imaging is essential for monitoring progress
👩⚕️🦴 NURSING MANAGEMENT OF PAGET’S DISEASE OF BONE
🔷 🎯 GOALS OF NURSING CARE
✅ Relieve pain and discomfort
✅ Promote mobility and prevent fractures
✅ Monitor and support medication compliance
✅ Educate the patient and family
✅ Prevent complications (neurological, skeletal, and emotional)
🔷 📝 NURSING ASSESSMENT
🔍 Subjective Data:
- Reports of deep bone pain (often in hips, pelvis, or spine)
- Difficulty walking, climbing stairs
- History of hearing loss or neurological symptoms (if skull is involved)
🔍 Objective Data:
- Skeletal deformities (bowed legs, enlarged skull)
- Waddling gait, kyphosis
- Limited ROM or stiffness in joints
- X-ray/scan findings showing pagetic lesions
- Lab results: ↑ ALP, normal calcium/phosphate (unless fractured)
🔷 🧰 NURSING INTERVENTIONS
💊 1. Medication Administration and Monitoring
- Administer bisphosphonates as prescribed (e.g., alendronate, zoledronic acid)
- Monitor for:
- GI issues (with oral bisphosphonates)
- Renal function (with IV therapy)
- Osteonecrosis of the jaw (educate on dental hygiene)
- Ensure adequate calcium and vitamin D intake
🛏️ 2. Pain Management
- Administer prescribed NSAIDs or analgesics
- Teach use of heat or cold therapy as needed
- Encourage rest during flare-ups, but avoid prolonged immobility
🧍♀️ 3. Mobility and Fall Prevention
- Provide walking aids or supportive braces as needed
- Modify environment to prevent falls:
- Remove loose rugs
- Install handrails and non-slip mats
- Ensure adequate lighting
- Encourage gentle exercises to maintain muscle tone and bone strength (in collaboration with physiotherapy)
📚 4. Patient and Family Education
- Explain:
- Nature of disease (chronic but manageable)
- Importance of medication adherence
- Signs of complications (fractures, hearing loss, vision issues)
- Educate on correct posture, safe lifting, and joint protection
- Discuss need for regular monitoring (ALP, bone scans, hearing tests)
🧠 5. Psychosocial Support
- Address concerns related to skeletal deformity or physical limitations
- Encourage participation in support groups
- Support emotional well-being in case of chronic pain or dependency
🔷 📋 DISCHARGE TEACHING
✅ Continue medications and supplements regularly
✅ Schedule regular lab and imaging follow-ups
✅ Perform safe, daily exercises as advised
✅ Take precautions to avoid falls or injuries
✅ Report new/worsening symptoms (bone pain, hearing loss, fractures) immediately
✅ Visit the dentist regularly (especially with IV bisphosphonates)
🔷 💡 KEY NURSING POINTS
✔ Paget’s disease leads to abnormal, enlarged, but weak bones
✔ Nurses play a key role in pain management, mobility promotion, and fall prevention
✔ Bisphosphonates are first-line — ensure patient understanding and adherence
✔ Monitor for long-term complications (fractures, arthritis, nerve compression)
✔ Educate and emotionally support the patient through chronic illness management
⚠️🦴 COMPLICATIONS OF PAGET’S DISEASE
Paget’s disease, if not treated effectively, can lead to several skeletal and systemic complications due to structurally abnormal bone formation.
🔷 ❗ MAJOR COMPLICATIONS
| 🔥 Complication | 📝 Description |
|---|---|
| 1. Pathological Fractures | Weak, deformed bones fracture easily with minor trauma (especially femur, tibia, pelvis) |
| 2. Bone Deformities | Bowing of long bones, skull enlargement, spinal curvature (kyphosis or lordosis) |
| 3. Arthritis (Osteoarthritis) | Joint damage occurs due to bone misalignment or stress from deformity |
| 4. Neurological Complications | Due to nerve compression (cranial nerves, spinal cord): hearing loss, tinnitus, facial numbness, spinal stenosis |
| 5. Cardiovascular Complications | In extensive disease: increased blood flow to bones may cause high-output heart failure (rare) |
| 6. Paget’s Sarcoma (Malignant Transformation) | Rare (<1%), aggressive bone cancer arising from pagetic bone |
| 7. Dental Complications | If the maxilla is involved — tooth misalignment or loss |
| 8. Delayed Bone Healing | After fractures or surgery, healing may be prolonged due to abnormal bone metabolism |
✅✨ KEY POINTS TO REMEMBER (For Nursing and Exams)
✔ Paget’s disease = abnormal bone remodeling → enlarged but weak bones
✔ Usually affects skull, spine, pelvis, femur, tibia
✔ Often asymptomatic early; detected by ↑ serum ALP or abnormal X-ray
✔ Bone pain, deformities, and fractures are common presentations
✔ Bisphosphonates are the treatment of choice – they slow bone turnover
✔ Nurses must monitor for fracture risk, pain, and medication side effects
✔ Educate patients on fall prevention, exercise, and regular monitoring
✔ Neurological signs (hearing loss, facial pain, back numbness) suggest complications
✔ Early intervention helps prevent disability and improve quality of life
🦴🧍 SPINAL COLUMN DEFECTS AND DEFORMITIES
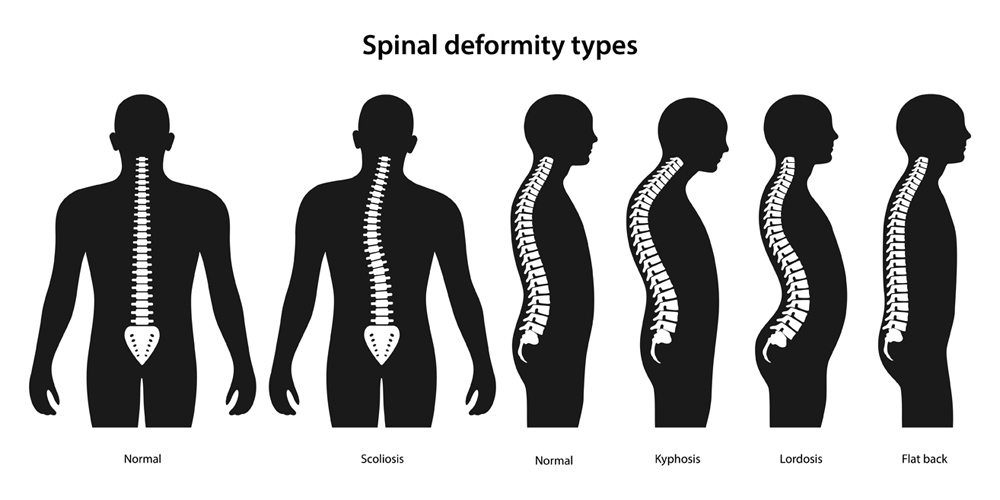
🔷 📘 DEFINITION
Spinal column defects and deformities refer to abnormalities in the structure, alignment, or formation of the spine, either present at birth (congenital) or developed later (acquired). These can affect posture, movement, and neurological function, depending on severity and location.
🧠 Such deformities may lead to back pain, abnormal gait, reduced mobility, or even nerve compression in severe cases.
🔷 ❗ CAUSES OF SPINAL COLUMN DEFECTS AND DEFORMITIES
They can be categorized into congenital, developmental, neuromuscular, and acquired causes:
✅ 1. Congenital Causes
| Cause | Description |
|---|---|
| Congenital scoliosis | Malformation of vertebrae during fetal development (e.g., hemivertebra, fused ribs) |
| Spina bifida | Failure of spinal column closure during embryogenesis (neural tube defect) |
| Klippel-Feil syndrome | Congenital fusion of cervical vertebrae, leads to limited neck movement |
🧒 2. Developmental Causes (During Growth)
| Cause | Description |
|---|---|
| Adolescent idiopathic scoliosis | Most common form; appears in puberty without a known cause |
| Scheuermann’s disease | Affects adolescents, causes thoracic kyphosis due to wedged vertebrae |
💪 3. Neuromuscular Causes
| Cause | Description |
|---|---|
| Cerebral palsy | Muscle imbalance and poor posture affect spine alignment |
| Muscular dystrophy | Weakening of spinal support muscles leads to curvature |
| Spinal muscular atrophy | Progressive muscle weakness affects spinal support |
🩹 4. Acquired Causes
| Cause | Description |
|---|---|
| Osteoporosis | Vertebral compression fractures can lead to kyphosis in elderly |
| Trauma or injury | Fractures, dislocations, or surgery may result in spinal misalignment |
| Infections (e.g., TB) | Spinal tuberculosis (Pott’s disease) can cause kyphosis or collapse |
| Tumors | Bone tumors or metastasis may destroy vertebrae and cause deformity |
| Poor posture / heavy backpacks | Common in children/adolescents and can lead to postural kyphosis |
🦴📚 TYPES OF SPINAL COLUMN DEFECTS AND DEFORMITIES
Spinal deformities may be structural (fixed) or postural (flexible). They may affect the spine in the coronal (side-to-side), sagittal (front-back), or axial (rotational) planes.
🔷 🌀 1. SCOLIOSIS – Lateral (sideways) curvature of the spine
🧾 Definition: Curvature >10° in the coronal plane, often with spinal rotation.
| Type | Description |
|---|---|
| Idiopathic scoliosis | Most common; occurs in adolescence without known cause |
| Congenital scoliosis | Due to abnormal vertebral development in the womb (e.g., hemivertebra) |
| Neuromuscular scoliosis | Seen in cerebral palsy, muscular dystrophy due to poor muscle control |
| Degenerative scoliosis | Occurs in older adults due to disc degeneration, arthritis |
| Functional scoliosis | Due to postural habits, leg length discrepancy (reversible) |
🔷 ↘️ 2. KYPHOSIS – Exaggerated forward rounding of the upper spine
🧾 Definition: Curvature >45° in the thoracic spine.
| Type | Description |
|---|---|
| Postural kyphosis | Common in adolescents; due to slouching; flexible and correctable |
| Scheuermann’s kyphosis | Structural kyphosis from wedged vertebrae (adolescents) |
| Congenital kyphosis | Malformation of vertebrae during fetal development |
| Age-related (senile) kyphosis | Due to osteoporosis and vertebral compression fractures |
| Pott’s kyphosis | From vertebral collapse in spinal tuberculosis |
🔷 ↗️ 3. LORDOSIS (Hyperlordosis) – Exaggerated inward curve of the lower back (lumbar spine)
🧾 Definition: Increased concavity of the lumbar or cervical spine.
| Type | Description |
|---|---|
| Postural lordosis | From poor posture or prolonged standing |
| Congenital lordosis | Present at birth due to abnormal spinal development |
| Neuromuscular lordosis | Associated with muscular weakness (e.g., Duchenne muscular dystrophy) |
| Compensatory lordosis | Due to hip deformity, pregnancy, or obesity (to maintain balance) |
🔷 💥 4. SPINA BIFIDA – Congenital defect due to failure of neural tube closure
| Type | Description |
|---|---|
| Spina bifida occulta | Mildest form; no visible external defect; may cause back dimpling |
| Meningocele | Meninges protrude through a vertebral opening |
| Myelomeningocele | Most severe form; spinal cord and meninges protrude → neurological deficits |
🔷 🧬 5. KYPHOSCOLIOSIS – Combined kyphosis and scoliosis
- Seen in congenital deformities, neuromuscular diseases, or advanced tuberculosis
- Causes severe postural imbalance and may impair lung or heart function
🔷 🧱 6. BLOCK VERTEBRA / HEMIVERTEBRA
| Type | Description |
|---|---|
| Hemivertebra | One side of a vertebral body fails to form, causing curvature |
| Block vertebra | Two or more vertebrae fused congenitally, limiting flexibility |
| Klippel-Feil syndrome | Fusion of cervical vertebrae causing short neck and limited motion |
🔷 🧍♂️ 7. FLATBACK SYNDROME
- Loss of normal lumbar lordosis, leading to a flat appearance and difficulty standing upright
- Often occurs after spinal fusion surgery or in degenerative spine conditions
🔷 🩻 8. SPONDYLOLISTHESIS – One vertebra slips over the one below
| Type | Description |
|---|---|
| Congenital | Due to malformation of vertebrae |
| Isthmic | Common in athletes, due to stress fracture of pars interarticularis |
| Degenerative | Seen in elderly due to facet joint arthritis |
| Traumatic or pathological | Due to injury or tumor |
🔷 🧓 9. VERTEBRAL COMPRESSION FRACTURES (VCFs)
- Seen in osteoporosis or trauma
- Leads to kyphotic deformities and height loss
🧠 Summary Table: Spinal Column Deformities
| Deformity | Direction of Curve | Common Causes |
|---|---|---|
| Scoliosis | Lateral (sideways) | Idiopathic, neuromuscular, congenital |
| Kyphosis | Forward (humpback) | Postural, Scheuermann’s, osteoporosis |
| Lordosis | Inward (swayback) | Postural, muscular, compensatory |
| Spina Bifida | Neural tube defect | Congenital |
| Spondylolisthesis | Forward vertebral slippage | Congenital, trauma, degeneration |
🧬🦴 PATHOPHYSIOLOGY OF SPINAL COLUMN DEFECTS AND DEFORMITIES
🔷 🌀 1. SCOLIOSIS (Lateral curvature)
🔬 Pathophysiology:
- Abnormal curvature (>10°) develops in the coronal plane, often with vertebral rotation
- Causes asymmetrical loading on vertebrae and intervertebral discs
- Leads to muscle imbalance, rib cage distortion, and possible pulmonary compromise in severe cases
- In idiopathic scoliosis, etiology is unknown, but thought to involve genetics, abnormal growth, and neuromuscular control
🔷 ↘️ 2. KYPHOSIS (Forward curvature)
🔬 Pathophysiology:
- Exaggerated curvature of the thoracic spine (>45°) in the sagittal plane
- Can be due to:
- Postural kyphosis: reversible, muscular imbalance from poor posture
- Structural kyphosis (e.g., Scheuermann’s): wedge-shaped vertebrae due to abnormal vertebral endplate development
- Osteoporotic kyphosis: anterior vertebral body collapse → spinal shortening
- May compress lungs, reduce thoracic volume, and impair balance
🔷 ↗️ 3. LORDOSIS (Hyperlordosis)
🔬 Pathophysiology:
- Exaggerated lumbar or cervical curvature, often compensatory to balance thoracic or pelvic abnormalities
- May arise from pelvic tilt, hip flexor contracture, or abdominal obesity
- Puts stress on posterior spinal structures, causing back pain and possible nerve compression
🔷 💥 4. SPINA BIFIDA (Neural tube defect)
🔬 Pathophysiology:
- Failure of the neural tube to close during embryonic development (3rd–4th week gestation)
- Leads to incomplete formation of the vertebral arch, allowing protrusion of spinal contents
- Severity depends on type:
- Occulta: mild, no neural tissue involvement
- Meningocele: meninges protrude
- Myelomeningocele: spinal cord and nerves protrude → neurological deficits
🔷 🔄 5. KYPHOSCOLIOSIS (Combined kyphosis and scoliosis)
🔬 Pathophysiology:
- Simultaneous lateral and anteroposterior deformities
- Causes severe spinal distortion, leading to chest wall asymmetry and restrictive lung disease
- Common in neuromuscular disorders, severe TB, or congenital malformations
🔷 🧱 6. BLOCK VERTEBRA / HEMIVERTEBRA
🔬 Pathophysiology:
- Block vertebra: fusion of adjacent vertebrae due to failure of segmentation
- Hemivertebra: partial vertebral formation → spinal tilt and progressive curvature
- Disturbs spinal growth symmetry, often leading to congenital scoliosis or kyphosis
🔷 🧍♂️ 7. FLATBACK SYNDROME
🔬 Pathophysiology:
- Loss of normal lumbar lordosis results in a “flat” spinal profile
- Seen after spinal fusion or degenerative disc disease
- Causes forward shifting of the center of gravity → difficulty in upright posture and chronic pain
🔷 🩻 8. SPONDYLOLISTHESIS
🔬 Pathophysiology:
- One vertebra slips forward over the one below due to:
- Congenital defects in pars interarticularis
- Stress fracture (isthmic type) from overuse
- Degeneration of facet joints (common in elderly)
- Leads to nerve compression, back pain, and instability of the spine
🔷 🧓 9. VERTEBRAL COMPRESSION FRACTURES (VCFs)
🔬 Pathophysiology:
- Weak or brittle vertebrae (especially from osteoporosis) collapse under axial load
- Causes anterior wedge shape of vertebral body → kyphosis
- Results in reduced height, back pain, and possible spinal cord compression
🦴🩺 SPINAL COLUMN DEFECTS AND DEFORMITIES
(Signs & Symptoms + Diagnosis)
🔷 🌀 1. SCOLIOSIS
✅ Signs & Symptoms
- Visible lateral curvature of spine (S or C shaped)
- Uneven shoulders or hips
- One shoulder blade more prominent
- Back pain (in adults or advanced cases)
- Asymmetrical waistline
- Fatigue after standing/walking
- In severe cases: Respiratory difficulty due to rib cage deformity
🧪 Diagnosis
- Adam’s forward bend test – visible rib hump
- Scoliometer – measures angle of trunk rotation
- X-ray – confirms diagnosis and measures Cobb angle
- MRI/CT – if underlying causes (tumor, spinal cord involvement) are suspected
🔷 ↘️ 2. KYPHOSIS
✅ Signs & Symptoms
- Rounded upper back (hunchback appearance)
- Back pain, stiffness
- Fatigue
- Height loss in elderly
- In severe kyphosis: breathing difficulty, chest tightness
🧪 Diagnosis
- Physical examination – curvature visible in standing posture
- X-ray – confirms thoracic angle > 45°
- MRI – to rule out spinal cord compression
- Bone scan – if suspecting infection or malignancy
🔷 ↗️ 3. LORDOSIS
✅ Signs & Symptoms
- Inward curve of lower back (swayback)
- Low back pain or stiffness
- Protruding abdomen and buttocks
- Difficulty standing for long periods
🧪 Diagnosis
- Observation in side view posture
- X-ray – shows increased lumbar curvature
- MRI or CT – to assess soft tissue or disc involvement if symptomatic
🔷 💥 4. SPINA BIFIDA
✅ Signs & Symptoms
| Type | Symptoms |
|---|---|
| Occulta | Often asymptomatic, may have dimple or hair tuft on lower back |
| Meningocele | Sac protruding with meninges, no neural deficits |
| Myelomeningocele | Neurological deficits: weakness, bladder/bowel incontinence, hydrocephalus, clubfoot |
🧪 Diagnosis
- Prenatal ultrasound – detects neural tube defects
- Maternal serum alpha-fetoprotein (AFP) – elevated in open defects
- MRI/CT of spine – postnatal confirmation
- Neurological assessment – motor/sensory deficit evaluation
🔷 🔄 5. KYPHOSCOLIOSIS
✅ Signs & Symptoms
- Combination of kyphosis and scoliosis signs
- Severe postural imbalance
- Restricted lung expansion, shortness of breath
- Chronic back pain
🧪 Diagnosis
- X-ray – confirms combined spinal curvature
- Pulmonary function tests – evaluate restrictive lung pattern
- MRI – if neurological symptoms or spinal cord compression suspected
🔷 🧱 6. BLOCK VERTEBRA / HEMIVERTEBRA
✅ Signs & Symptoms
- Visible spinal deformity in childhood
- Reduced spinal mobility
- May cause progressive scoliosis or kyphosis
🧪 Diagnosis
- X-ray – reveals fused vertebrae or incomplete vertebral formation
- MRI – assesses spinal cord or soft tissue involvement
- Genetic testing – if part of a syndrome (e.g., Klippel-Feil)
🔷 🧍♂️ 7. FLATBACK SYNDROME
✅ Signs & Symptoms
- Flat appearance of lower back
- Inability to stand upright
- Back pain and fatigue
- Difficulty walking uphill or standing long periods
🧪 Diagnosis
- Postural assessment
- X-ray (lateral view) – shows decreased lumbar lordosis
- Spinal alignment tests – sagittal balance
🔷 🩻 8. SPONDYLOLISTHESIS
✅ Signs & Symptoms
- Low back pain (worse with activity)
- Tight hamstrings
- Postural changes, protruding abdomen
- Neurological symptoms: leg pain, numbness if nerve root compression
- Visible step-off in severe slippage
🧪 Diagnosis
- X-ray (lateral view) – shows vertebral slippage
- MRI – checks nerve root compression
- CT scan – better visualization of bone defects
🔷 🧓 9. VERTEBRAL COMPRESSION FRACTURES (VCFs)
✅ Signs & Symptoms
- Sudden back pain (often after minor fall or bending)
- Height loss
- Stooped posture (kyphosis)
- Pain worsens with standing or walking
🧪 Diagnosis
- X-ray – reveals wedge-shaped vertebra
- DEXA scan – to assess for underlying osteoporosis
- MRI – distinguishes acute vs. old fractures
- Bone scan – if infection or tumor is suspected
💊🧍♂️ MEDICAL MANAGEMENT OF SPINAL COLUMN DEFECTS & DEFORMITIES
🎯 Goals of medical management:
- Relieve pain and inflammation
- Prevent progression of deformity
- Improve posture and mobility
- Prevent complications (e.g., neurological, respiratory)
🔷 🌀 1. SCOLIOSIS
💊 Medical Management:
- Mild to moderate cases (Cobb angle < 25°–30°):
- Observation with periodic X-rays to monitor curve progression
- Physical therapy to strengthen core and back muscles
- Analgesics (NSAIDs) for back pain
- Bracing (for adolescents with progressive curves 25–40°):
- Boston brace or Milwaukee brace
- Worn for 18–23 hours/day to prevent curve progression
🔷 ↘️ 2. KYPHOSIS
💊 Medical Management:
- Postural kyphosis:
- Corrective exercises, yoga, posture training
- Ergonomic support for prolonged sitting
- Scheuermann’s kyphosis or age-related:
- Back braces in adolescents
- NSAIDs for pain relief
- Calcium and Vitamin D supplementation (if osteoporosis is present)
- Physical therapy for spinal extension exercises
🔷 ↗️ 3. LORDOSIS
💊 Medical Management:
- Treat underlying causes (e.g., obesity, pregnancy, hip contractures)
- Posture correction exercises
- Strengthening abdominal and hamstring muscles
- Pain management: NSAIDs or muscle relaxants if associated with spasm
🔷 💥 4. SPINA BIFIDA
💊 Medical Management:
- Spina bifida occulta: Often requires no treatment
- Meningocele / Myelomeningocele:
- Folic acid supplementation during pregnancy (prevention)
- Antibiotics for infection prevention if sac is exposed
- Bladder and bowel management (intermittent catheterization)
- Physiotherapy to prevent contractures and enhance mobility
- Orthotic support for walking
🔷 🔄 5. KYPHOSCOLIOSIS
💊 Medical Management:
- Combination of treatments for scoliosis and kyphosis
- Bracing if deformity is still flexible
- Pulmonary rehabilitation if lung function is impaired
- Analgesics and anti-inflammatory drugs for pain
- Respiratory support in severe cases (e.g., BiPAP or oxygen)
🔷 🧱 6. BLOCK VERTEBRA / HEMIVERTEBRA
💊 Medical Management:
- Observation if no symptoms or minimal curve
- Physical therapy to maintain spinal strength and flexibility
- Pain control as needed
- Early detection of curve progression for surgical planning
🔷 🧍♂️ 7. FLATBACK SYNDROME
💊 Medical Management:
- Physical therapy to improve core strength and posture
- Pain management with NSAIDs or muscle relaxants
- Activity modification
- Supportive bracing (temporary)
- Monitor for balance and fall risk
🔷 🩻 8. SPONDYLOLISTHESIS
💊 Medical Management:
- NSAIDs for pain control
- Activity restriction in acute cases
- Back brace to stabilize spine
- Core-strengthening and hamstring-stretching exercises
- Epidural steroid injections if nerve compression causes radiating leg pain
🔷 🧓 9. VERTEBRAL COMPRESSION FRACTURES (VCFs)
💊 Medical Management:
- Pain control: NSAIDs, acetaminophen, opioids if severe
- Calcitonin spray – may reduce bone pain
- Bisphosphonates or teriparatide – for underlying osteoporosis
- Calcium and Vitamin D supplementation
- Bracing (TLSO brace) to support healing
- Physical therapy for posture correction and muscle strengthening
✅ ✨ GENERAL SUPPORTIVE MEASURES FOR ALL TYPES
- Regular monitoring: X-rays, MRIs, or DEXA scans depending on condition
- Nutritional support: Adequate protein, calcium, and vitamin D
- Pain management: Tailored to severity and patient response
- Posture correction training and ergonomic modifications
- Psychosocial support for children and adults with body image concerns
- Multidisciplinary approach: Ortho, physio, neuro, nutrition, and nursing teams
🛠️🧍♂️ SURGICAL MANAGEMENT OF SPINAL COLUMN DEFECTS AND DEFORMITIES
🎯 Goals of surgical treatment:
- Correct spinal alignment
- Stabilize the spine
- Relieve nerve compression
- Improve posture, function, and quality of life
- Prevent progression of deformity
🔷 🌀 1. SCOLIOSIS
🔧 Surgical Options:
- Indicated if Cobb angle > 40–50° (progressive or severe curves)
| Procedure | Description |
|---|---|
| Spinal Fusion Surgery | Fusing curved vertebrae to prevent further movement |
| Instrumentation (Rods, Screws) | Used with fusion to support correction and stability |
| Growing Rods (in children) | Expandable rods to allow spinal growth during childhood |
🔷 ↘️ 2. KYPHOSIS
🔧 Surgical Options:
- Indicated in severe curves (>70°), progressive deformity, or neurological deficits
| Procedure | Description |
|---|---|
| Posterior spinal fusion | Stabilizes the spine from the back side |
| Osteotomy | Removal of wedge-shaped bone segments to correct curvature |
| Vertebral column resection | Reserved for extreme deformities not responsive to other techniques |
🔷 ↗️ 3. LORDOSIS
🔧 Surgical Options:
- Rarely needed unless severe or causing nerve compression
| Procedure | Description |
|---|---|
| Spinal fusion with rods | Used to stabilize and correct hyperlordosis |
| Decompression surgery | If spinal canal narrowing occurs due to abnormal curvature |
🔷 💥 4. SPINA BIFIDA
🔧 Surgical Options:
| Type | Procedure |
|---|---|
| Meningocele / Myelomeningocele | Surgical closure of the defect within 48 hours of birth to prevent infection |
| Hydrocephalus (commonly associated) | Ventriculoperitoneal (VP) shunt insertion |
| Orthopedic surgery | For clubfoot, scoliosis, or hip dislocation in older children |
| Urologic surgery | Bladder augmentation or catheterization access in severe cases |
🔷 🔄 5. KYPHOSCOLIOSIS
🔧 Surgical Options:
- Complex procedures often combining methods for kyphosis + scoliosis
| Procedure | Description |
|---|---|
| Multilevel spinal fusion | For combined curves and instability |
| Decompression + correction | If neurological symptoms are present |
| Thoracoplasty | May be done to reduce rib prominence |
🔷 🧱 6. BLOCK VERTEBRA / HEMIVERTEBRA
🔧 Surgical Options:
- Needed if the deformity is progressive or symptomatic
| Procedure | Description |
|---|---|
| Hemivertebra excision | Surgical removal of malformed vertebra |
| Spinal fusion | Prevents further spinal curvature |
🔷 🧍♂️ 7. FLATBACK SYNDROME
🔧 Surgical Options:
- Surgery may be required for post-fusion syndrome or severe imbalance
| Procedure | Description |
|---|---|
| Osteotomy + fusion | Restores lumbar lordosis and corrects sagittal imbalance |
🔷 🩻 8. SPONDYLOLISTHESIS
🔧 Surgical Options:
- Indicated if slippage >50%, instability, or neurological symptoms
| Procedure | Description |
|---|---|
| Spinal fusion (with or without reduction) | Stabilizes vertebrae and prevents further slippage |
| Decompression (laminectomy) | Relieves pressure on nerve roots |
🔷 🧓 9. VERTEBRAL COMPRESSION FRACTURES (VCFs)
🔧 Surgical Options:
- Required if pain is severe or vertebral collapse is progressive
| Procedure | Description |
|---|---|
| Vertebroplasty | Bone cement is injected into fractured vertebra to stabilize it |
| Kyphoplasty | Balloon inserted and inflated to restore height, then filled with cement |
✅ ✨ GENERAL SURGICAL CONSIDERATIONS
✔ Preoperative Evaluation: Includes imaging, pulmonary function tests (in severe kyphoscoliosis), cardiac assessment
✔ Postoperative Care: Pain control, wound care, bracing, physiotherapy
✔ Complication Management: Watch for infection, nerve injury, implant failure, or loss of correction
✔ Multidisciplinary Approach: Involves orthopedic surgeons, neurologists, physiotherapists, and nurses
👩⚕️🧍♂️ NURSING MANAGEMENT OF SPINAL COLUMN DEFECTS AND DEFORMITIES
🔷 🎯 GOALS OF NURSING CARE
✅ Relieve pain and promote comfort
✅ Support spinal alignment and prevent further deformity
✅ Enhance mobility and physical functioning
✅ Prevent complications (e.g., pressure sores, respiratory issues, infections)
✅ Provide emotional support and patient/family education
✅ Facilitate rehabilitation and long-term care planning
🔷 📝 NURSING ASSESSMENT
🔍 Subjective Data:
- Reports of back pain, muscle weakness, or fatigue
- Difficulty with standing, walking, or posture
- History of spinal deformity or recent diagnosis
- Emotional distress or body image concerns
🔍 Objective Data:
- Observation of posture, gait, spinal alignment
- Presence of assistive devices or bracing
- Respiratory rate (in kyphoscoliosis or severe deformities)
- Neurological status (sensory/motor deficits, bladder/bowel control)
- Diagnostic reports: X-rays, MRI, Cobb angle, ALP (if metabolic cause suspected)
🔷 🧰 NURSING INTERVENTIONS
💊 1. Pain Management
- Administer prescribed NSAIDs, analgesics, or muscle relaxants
- Apply warm/cold compresses as needed
- Encourage position changes for comfort and spinal relief
- Monitor pain scale regularly and evaluate effectiveness
🚶 2. Promote Mobility and Functional Independence
- Encourage gentle exercises and ROM movements under guidance
- Use braces or spinal orthoses as prescribed (e.g., Boston brace)
- Assist with ambulation aids (walker, cane) to prevent falls
- Refer to physiotherapy and occupational therapy for gait training and ADL support
🛌 3. Post-Surgical Care (if surgery performed)
- Monitor vitals, neuro checks, and surgical site for bleeding/infection
- Maintain spinal alignment (logrolling technique) when turning
- Manage drains, catheters, or IV lines as needed
- Administer antibiotics or DVT prophylaxis as ordered
- Educate on brace or corset application and wound care
🧠 4. Psychosocial and Emotional Support
- Address body image concerns, especially in adolescents
- Encourage self-esteem building activities
- Involve family and support groups in the care plan
- Offer counseling or refer to mental health services as needed
📚 5. Patient and Family Education
- Teach:
- Importance of regular follow-up and imaging
- Bracing schedules (e.g., 18–23 hrs/day for scoliosis)
- Signs of complications: numbness, weakness, loss of bowel/bladder control
- Postural hygiene, correct lifting, ergonomic tips
- Nutritional support: calcium, vitamin D, high protein for healing
🧼 6. Prevent Complications
- Skin care: Check under braces for redness/sores
- Respiratory support: Incentive spirometry in kyphoscoliosis
- Prevent pressure ulcers in immobile patients
- Prevent urinary retention or constipation in neurological types (e.g., spina bifida)
- Encourage hydration and fiber intake
🔷 📋 DISCHARGE PLANNING
✅ Continue medication and follow-up appointments
✅ Adhere to bracing or rehabilitation protocols
✅ Modify home for safety and accessibility
✅ Encourage school re-entry or vocational rehab if applicable
✅ Teach warning signs to report: pain, deformity, neurological changes
✅✨ KEY POINTS FOR NURSES
✔ Individualize care based on type, severity, and age of the patient
✔ Monitor for neurological deficits, posture changes, or complications
✔ Nurses play a vital role in education, motivation, and support
✔ Collaborate with multidisciplinary teams (orthopedic, physio, neuro, nutrition)
✔ Empower patients to actively participate in their long-term care.
⚠️🧍♂️ COMPLICATIONS OF SPINAL COLUMN DEFECTS AND DEFORMITIES
Spinal deformities can lead to progressive structural, functional, and systemic issues if not managed effectively.
🔷 ❗ MAJOR COMPLICATIONS
| 🧨 Complication | 📋 Description |
|---|---|
| 1. Chronic Pain | From muscle strain, joint degeneration, or nerve compression |
| 2. Respiratory Dysfunction | Seen in kyphoscoliosis — rib cage deformity restricts lung expansion |
| 3. Cardiovascular Compromise | In severe deformities (kyphoscoliosis) → reduced cardiac output |
| 4. Neurological Impairment | Due to spinal cord or nerve root compression → weakness, numbness, paralysis |
| 5. Bowel and Bladder Dysfunction | Especially in spina bifida or spondylolisthesis |
| 6. Mobility and Postural Issues | Gait disturbances, imbalance, risk of falls and fractures |
| 7. Spinal Instability | Especially in spondylolisthesis or advanced scoliosis |
| 8. Deformity Progression | If untreated in childhood → worsening curvature and disability |
| 9. Psychosocial Impact | Body image issues, social withdrawal, low self-esteem (especially adolescents) |
| 10. Surgical Complications | Infections, implant failure, nerve damage, blood loss |
✅✨ KEY POINTS TO REMEMBER
✔ Spinal deformities can be congenital, neuromuscular, or acquired
✔ Common types include scoliosis, kyphosis, lordosis, spina bifida, spondylolisthesis
✔ Early detection, especially in children and adolescents, prevents progression
✔ Bracing and physiotherapy are first-line in mild to moderate cases
✔ Surgery is needed for severe curves or neurological compromise
✔ Nurses must focus on pain relief, posture support, fall prevention, and education
✔ Multidisciplinary care (orthopedic, neuro, physio, OT, nursing) improves outcomes
✔ Emotional and psychological support is crucial for long-term adaptation
✔ Encourage adherence to follow-ups, bracing schedules, and home modifications
🧠🦴 SPINAL CORD TUMORS
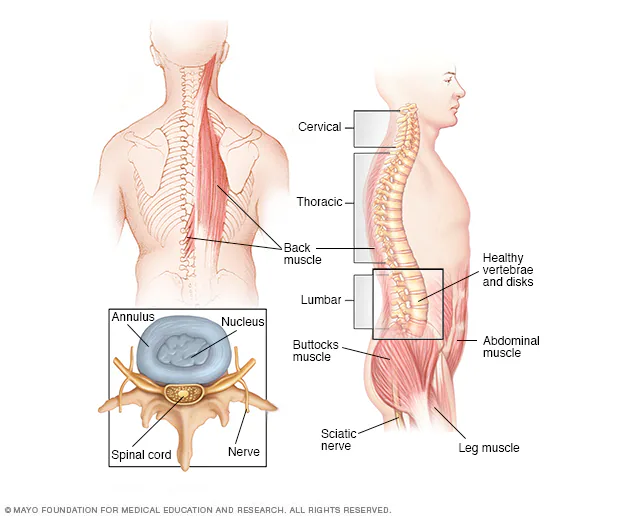
🔷 📘 DEFINITION
A spinal cord tumor is an abnormal growth of tissue within or surrounding the spinal cord or spinal column that may be benign (non-cancerous) or malignant (cancerous). These tumors can compress the spinal cord or nerve roots, leading to neurological deficits and functional impairments.
🔷 ❗ CAUSES
| Cause Type | Examples |
|---|---|
| Primary tumors | Arise from spinal cord tissues or coverings (e.g., meningiomas, astrocytomas) |
| Secondary tumors | Metastatic spread from lung, breast, prostate, or kidney cancers |
| Genetic disorders | Neurofibromatosis type 1 & 2, von Hippel–Lindau disease |
| Radiation exposure | Prior spinal radiation increases tumor risk |
| Unknown/Idiopathic | Many primary spinal tumors have no identifiable cause |
🔷 🧬 TYPES OF SPINAL CORD TUMORS
✅ Based on Location:
| Type | Description |
|---|---|
| Intramedullary | Within the spinal cord itself (e.g., astrocytoma, ependymoma) |
| Extramedullary | Outside the spinal cord but within dura (e.g., meningioma, schwannoma) |
| Extradural | Outside the dura mater, often metastatic tumors or vertebral tumors |
✅ Based on Behavior:
- Benign tumors: Slow-growing, localized (e.g., meningioma, schwannoma)
- Malignant tumors: Rapid growth, may infiltrate spinal cord (e.g., glioblastoma, lymphoma)
🔷 🔬 PATHOPHYSIOLOGY
- Tumor develops within or around the spinal cord
- Leads to compression or infiltration of spinal cord tissues or nerve roots
- Disrupts blood supply, impairs nerve conduction, and causes edema and ischemia
- Resulting in motor, sensory, and autonomic dysfunction
- If untreated, leads to permanent neurological damage or paralysis
🔷 🩺 SIGNS AND SYMPTOMS
| Symptom | Description |
|---|---|
| Back or neck pain | Persistent, often worse at night or lying down |
| Radicular pain | Radiating along nerve path (sciatica-like) |
| Muscle weakness | In arms, legs depending on tumor level |
| Sensory changes | Numbness, tingling, burning, or loss of sensation |
| Bladder/bowel dysfunction | Incontinence or retention |
| Gait instability | Difficulty walking or imbalance |
| Paralysis | In late stages if compression persists |
🔷 🧪 DIAGNOSIS
| Test | Purpose |
|---|---|
| MRI with contrast | Gold standard to visualize tumor size, location, and type |
| CT scan | Useful for evaluating bone involvement |
| Spinal X-rays | May show vertebral collapse or deformity |
| Myelogram | Shows spinal cord compression (if MRI unavailable) |
| Biopsy | Confirms tumor type and guides treatment |
| CSF analysis | May show malignant cells (in leptomeningeal metastasis) |
🔷 💊 MEDICAL MANAGEMENT
| Treatment | Role |
|---|---|
| Corticosteroids (e.g., dexamethasone) | Reduce inflammation and edema around tumor |
| Pain management | NSAIDs, opioids, nerve pain agents (gabapentin, pregabalin) |
| Radiation therapy | Used for malignant tumors or inoperable lesions |
| Chemotherapy | For radiosensitive tumors (e.g., lymphoma, metastasis) |
| Targeted therapy / Immunotherapy | Based on tumor type (e.g., checkpoint inhibitors) |
| Physical therapy | Improves strength and mobility during/after treatment |
🔷 🛠️ SURGICAL MANAGEMENT
| Procedure | Description |
|---|---|
| Laminectomy | Removal of part of vertebral bone to relieve pressure |
| Tumor resection | Total or partial removal of tumor mass (microsurgical techniques) |
| Spinal stabilization | Use of rods or screws if vertebral instability occurs post-resection |
| Biopsy surgery | For histopathological diagnosis before definitive treatment |
📌 Surgical decision depends on tumor location, accessibility, neurological status, and general health.
🔷 👩⚕️ NURSING MANAGEMENT
✅ Preoperative Care
- Explain procedure and obtain informed consent
- Administer steroids and pain medications as prescribed
- Perform neurological assessments (motor strength, sensation, reflexes)
- Provide emotional support and reduce anxiety
✅ Postoperative Care
- Monitor neurological status closely (e.g., limb movement, bladder function)
- Maintain spinal alignment (log rolling, firm mattress)
- Monitor vitals, wound site, drainage
- Administer medications: pain relief, antibiotics, steroids
- Encourage deep breathing, cough exercises to prevent pneumonia
- Start early physiotherapy as advised
✅ Ongoing Nursing Care
- Assist with ADLs, ambulation, and bowel/bladder care
- Prevent pressure sores with regular repositioning
- Support emotional adjustment to mobility changes
- Educate about follow-up, home modifications, brace/corset use
🔷 ⚠️ COMPLICATIONS
| Complication | Description |
|---|---|
| Permanent neurological deficits | Due to delayed diagnosis or irreversible compression |
| Paraplegia/quadriplegia | In cervical or thoracic spinal cord involvement |
| Bladder/bowel incontinence | Due to nerve damage |
| Spinal instability | After tumor erosion or surgery |
| Infection or CSF leak | Postoperative risks |
| Recurrence/metastasis | In malignant tumors |
✅✨ KEY POINTS TO REMEMBER
✔ Spinal cord tumors can be benign or malignant, but all can cause neurological damage
✔ MRI with contrast is the best diagnostic tool
✔ Early treatment = better outcomes — delay can lead to paralysis
✔ Corticosteroids help reduce edema and preserve function
✔ Surgery is often needed for decompression and tumor removal
✔ Nurses play a vital role in neuro checks, post-op care, mobility assistance, and education
✔ Multidisciplinary approach (neuro, oncology, rehab, nursing) improves patient recovery and QOL.
🦴💥 PROLAPSED INTERVERTEBRAL DISC (PIVD)
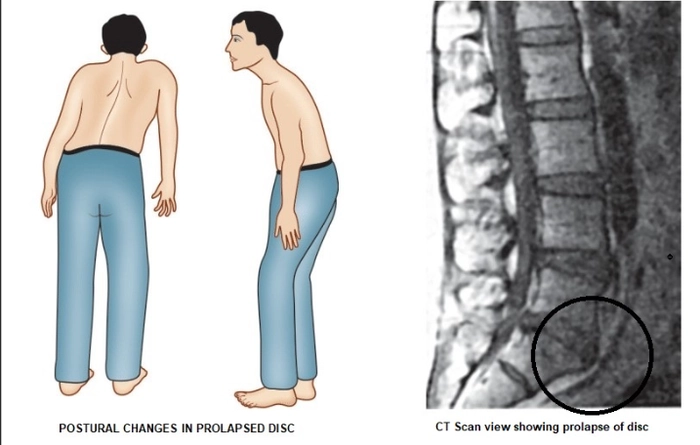
(Also known as Herniated Disc, Slipped Disc, or Disc Prolapse)
🔷 📘 DEFINITION
A Prolapsed Intervertebral Disc (PIVD) is a condition where the nucleus pulposus (inner gel-like center) of an intervertebral disc protrudes through a weakened or torn annulus fibrosus (outer fibrous ring), often compressing adjacent spinal nerves or the spinal cord.
➡️ This may result in pain, numbness, weakness, or neurological deficits, especially in the lower back or neck.
🔷 ❗ CAUSES
PIVD is typically caused by a combination of degeneration, trauma, and mechanical stress.
✅ 1. Degenerative Changes (Most common)
- Age-related disc wear and tear
- Loss of water content → reduced disc flexibility and height
- Breakdown of collagen and proteoglycans in annulus fibrosus
💥 2. Trauma or Sudden Pressure
- Heavy lifting, twisting, or high-impact injuries
- Falling, vehicular accidents, or sports injuries
🧬 3. Congenital or Structural Weakness
- Narrow spinal canal
- Weak annulus fibrosus
📉 4. Risk Factors
| Risk Factor | Examples |
|---|---|
| Occupation | Frequent lifting, twisting, vibration exposure (e.g., drivers, laborers) |
| Obesity | Increases spinal load |
| Smoking | Affects disc nutrition and healing |
| Sedentary lifestyle | Weak back muscles increase injury risk |
| Genetics | Family history of disc disease |
🔷 🧬 TYPES OF PROLAPSED INTERVERTEBRAL DISC
Classified based on extent of disc herniation:
| Type | Description |
|---|---|
| 1. Disc Protrusion (Bulge) | Annulus is intact but nucleus pushes outward, forming a bulge |
| 2. Disc Extrusion | Nucleus pulposus breaks through annulus but remains within the disc area |
| 3. Disc Sequestration (Free Fragment) | A piece of the nucleus pulposus breaks away and moves freely in the spinal canal |
| 4. Contained vs. Non-contained | If the nucleus remains inside the annulus = contained; if it exits = non-contained |
✅ Based on Location in Spine:
| Location | Common Terms & Presentation |
|---|---|
| Cervical spine (C3–C7) | Neck pain, shoulder/arm numbness, weakness |
| Thoracic spine (T1–T12) | Rare; may cause mid-back pain or band-like chest pain |
| Lumbar spine (L4–L5, L5–S1) | Most common; causes lower back pain, sciatica, leg weakness, numbness |
🔷 🧬 PATHOPHYSIOLOGY
The intervertebral disc consists of:
- Nucleus pulposus – soft, jelly-like center
- Annulus fibrosus – tough outer fibrous ring
➤ Sequence of Events in PIVD:
- Degeneration or injury causes weakening or tearing of the annulus fibrosus
- The nucleus pulposus herniates (bulges or extrudes) through the annular tear
- This herniated disc material compresses adjacent spinal nerves or spinal cord
- Compression leads to:
- Inflammation
- Reduced nerve conduction
- Neuropathic pain
- Motor and sensory deficits
- If herniation persists, it may lead to chronic nerve damage and muscle atrophy
📍 Most commonly occurs at L4-L5 and L5-S1 (lumbar spine) and C5-C6 or C6-C7 (cervical spine)
🔷 🩺 SIGNS AND SYMPTOMS
Symptoms vary by the level and severity of nerve compression:
✅ General Symptoms
- Localized back or neck pain
- Radicular pain (shooting pain along the affected nerve pathway)
- Stiffness and restricted movement
- Muscle spasms and tenderness over the affected area
✅ Region-specific Symptoms
| Affected Region | Signs & Symptoms |
|---|---|
| Cervical PIVD | – Neck pain and stiffness |
- Pain radiating to shoulders and arms
- Numbness, tingling in fingers (dermatomal pattern)
- Weakness in arms/hands | | Thoracic PIVD | – Rare
- Mid-back pain
- Chest or abdominal band-like pain
- May mimic cardiac or GI conditions | | Lumbar PIVD | – Low back pain
- Pain radiating to buttocks, thighs, legs (sciatica)
- Numbness, tingling in lower limb
- Muscle weakness (foot drop)
- Difficulty walking or prolonged standing |
⚠️ Red Flag Symptoms (Indicate emergency):
- Bowel/bladder incontinence
- Saddle anesthesia (numbness in groin/perineum)
- Progressive motor weakness
➡️ May indicate Cauda Equina Syndrome — requires urgent surgical intervention
🔷 🧪 DIAGNOSIS
| Test | Purpose |
|---|---|
| MRI (Magnetic Resonance Imaging) | 🔹 Gold standard |
| 🔹 Clearly visualizes soft tissues — disc, nerves, spinal cord | |
| 🔹 Identifies level, size, and type of herniation | |
| CT scan | Useful when MRI is contraindicated (e.g., pacemaker) |
| Better for bony structures | |
| X-ray (Spine) | Shows disc space narrowing or spinal alignment, but not disc herniation itself |
| Myelogram | Dye + X-ray or CT to visualize nerve compression if MRI is unavailable |
| Nerve conduction studies / EMG | Assesses nerve and muscle function |
| Useful in chronic or unclear cases | |
| Straight Leg Raise Test (SLR) | Positive if raising leg causes pain radiating below the knee (suggests lumbar PIVD) |
🔷 💊 MEDICAL MANAGEMENT (Conservative Treatment)
🎯 Goals:
✅ Reduce pain and inflammation
✅ Relieve nerve compression
✅ Improve mobility
✅ Prevent recurrence
✅ 1. Rest and Activity Modification
- Short-term bed rest (1–2 days) during acute pain phase
- Avoid heavy lifting, twisting, bending
- Gradual return to daily activities with correct posture
✅ 2. Pharmacologic Therapy
| Drug Type | Examples | Purpose |
|---|---|---|
| NSAIDs | Ibuprofen, Diclofenac | Reduce inflammation and relieve pain |
| Muscle relaxants | Tizanidine, Cyclobenzaprine | Reduce muscle spasms |
| Neuropathic pain meds | Gabapentin, Pregabalin | Treat nerve-related pain (sciatica, tingling) |
| Oral steroids | Prednisone (short course) | Reduce nerve root inflammation |
| Analgesics | Acetaminophen, Tramadol | Additional pain control if needed |
✅ 3. Physical Therapy
- After acute phase subsides
- Includes:
- Stretching and strengthening exercises
- McKenzie technique (extension exercises)
- Lumbar stabilization exercises
✅ 4. Hot/Cold Therapy
- Ice for acute pain/swelling
- Heat for muscle stiffness and spasms
✅ 5. Epidural Steroid Injections
- Corticosteroids injected into epidural space
- Provides temporary relief by reducing inflammation
- Used in severe cases not responding to oral meds
🔷 🛠️ SURGICAL MANAGEMENT
💡 Indications for Surgery:
- Persistent pain > 6 weeks despite medical treatment
- Progressive neurological deficits (e.g., weakness, numbness)
- Cauda equina syndrome (emergency!)
- Severe disability affecting quality of life
✅ 1. Microdiscectomy (Lumbar or Cervical)
- Minimally invasive
- Removal of the herniated disc portion pressing on nerves
- Most common and effective for lumbar PIVD
✅ 2. Laminectomy / Laminotomy
- Removal of part of the vertebral lamina to relieve spinal cord/nerves
- Often done with discectomy in large or multiple-level disc herniation
✅ 3. Discectomy with Spinal Fusion
- In recurrent or multi-level PIVD
- Involves removing disc and fusing adjacent vertebrae with bone grafts, screws, or cages
- Used to maintain spinal stability
✅ 4. Artificial Disc Replacement
- Replacement of degenerated disc with artificial implant
- Preserves motion (unlike fusion)
- Used in selected cervical or lumbar PIVD
✅ 5. Endoscopic Spine Surgery (Minimally Invasive)
- Performed through small incision with camera-guided tools
- Faster recovery and less muscle damage
🧠 POSTOPERATIVE GOALS:
- Relieve nerve pressure
- Restore function
- Prevent recurrence
- Improve patient’s quality of life
👩⚕️🦴 NURSING MANAGEMENT OF PROLAPSED INTERVERTEBRAL DISC (PIVD)
(Slipped Disc / Herniated Disc)
🔷 🎯 GOALS OF NURSING CARE
✅ Relieve pain and discomfort
✅ Prevent neurological deterioration
✅ Support mobility and posture
✅ Educate patient for self-care and prevention of recurrence
✅ Promote rehabilitation and emotional well-being
🔷 📝 NURSING ASSESSMENT
🔍 Subjective Data:
- Location, severity, and radiation of pain
- Sensory complaints: numbness, tingling, burning
- History of trauma, lifting, or prior episodes
- Activity limitation and functional impact
- Sleep and psychosocial effects
🔍 Objective Data:
- Gait disturbance
- Muscle weakness or spasms
- Positive Straight Leg Raise test (lumbar PIVD)
- Neurological signs: altered reflexes, dermatomal loss
- Bladder or bowel dysfunction (red flag)
🔷 🧰 NURSING INTERVENTIONS
💊 1. Pain Relief and Comfort Measures
- Administer prescribed medications (NSAIDs, muscle relaxants, nerve pain meds)
- Apply cold compress during acute phase, warm compress for muscle relaxation
- Assist with positioning:
- Supine with knees flexed (lumbar)
- Cervical support for neck disc herniation
- Encourage relaxation techniques (deep breathing, guided imagery)
🚶♂️ 2. Promote Mobility and Prevent Complications
- Encourage gradual mobilization as pain subsides
- Monitor for postural imbalances and gait disturbances
- Assist with safe ambulation and transfers
- Use lumbar support or cervical collar if prescribed
- Turn and reposition regularly to prevent pressure ulcers
🧠 3. Neurological Monitoring
- Perform frequent neuro checks (motor strength, sensation, reflexes)
- Monitor for worsening signs:
- Foot drop, limb weakness
- Bladder/bowel incontinence
- Saddle anesthesia
➡️ Report immediately — may indicate cauda equina syndrome
🗣️ 4. Patient and Family Education
- Instruct on:
- Proper body mechanics and lifting techniques
- Posture correction during sitting, standing, and sleeping
- Importance of completing physiotherapy and home exercises
- Signs of recurrence or complication
- Educate on medication adherence and side effects
- Encourage lifestyle changes: weight loss, quitting smoking, ergonomic setup at work
🏋️ 5. Pre- and Post-Operative Care (if surgery performed)
✅ Pre-op:
- Explain procedure and expected outcomes
- Ensure completion of consent and investigations
- Provide psychological support
✅ Post-op:
- Monitor vitals and wound site
- Maintain spinal alignment (logrolling, firm mattress)
- Neurological monitoring (motor/sensory function)
- Promote early ambulation as per surgeon’s advice
- Prevent complications: DVT, UTI, infection, pressure ulcers
❤️ 6. Psychosocial and Emotional Support
- Address fears of chronic pain or paralysis
- Support body image concerns in younger patients
- Encourage participation in support groups if available
- Refer to psychologist or counselor if needed
🔷 📋 DISCHARGE TEACHING
✅ Take medications as prescribed
✅ Continue physical therapy and avoid bed rest for long
✅ Maintain ergonomic posture at work/home
✅ Avoid lifting heavy objects, bending, twisting
✅ Report red flags: increasing pain, numbness, weakness, bladder issues
✅ Regular follow-up with orthopedist/neurosurgeon
✅✨ KEY NURSING RESPONSIBILITIES
✔ Frequent neuro assessment to detect progression
✔ Ensure pain relief and mobility support
✔ Prevent complications of immobility
✔ Educate about long-term posture care and lifestyle changes
✔ Provide holistic care: physical, emotional, and social
⚠️🦴 COMPLICATIONS OF PROLAPSED INTERVERTEBRAL DISC (PIVD)
If left untreated or if severe, PIVD can lead to significant neurological and musculoskeletal complications.
🔷 ❗ MAJOR COMPLICATIONS
| Complication | Description |
|---|---|
| 1. Chronic low back or neck pain | Persistent pain due to long-standing disc irritation or inflammation |
| 2. Radiculopathy | Nerve root compression causing pain, numbness, or tingling along the nerve’s path (sciatica) |
| 3. Motor weakness | Muscle weakness or foot drop due to prolonged nerve compression |
| 4. Bladder or bowel dysfunction | Especially in Cauda Equina Syndrome → urgency, retention, or incontinence |
| 5. Sensory loss | Numbness or loss of sensation in legs, feet, arms, or fingers |
| 6. Gait disturbances | Impaired walking due to weakness or nerve involvement |
| 7. Disability | Inability to perform routine activities, affecting personal and professional life |
| 8. Recurrent disc prolapse | Especially if risk factors remain unmodified |
| 9. Surgical complications | Infection, CSF leak, nerve injury, failed back surgery syndrome |
| 10. Psychological impact | Chronic pain and immobility may lead to depression, anxiety, or social withdrawal |
✅✨ KEY POINTS TO REMEMBER (FOR REVISION & PRACTICE)
✔ PIVD = Herniation of nucleus pulposus through annulus fibrosus → nerve compression
✔ Commonly occurs at L4-L5 and L5-S1 (lumbar) and C5-C6 (cervical) levels
✔ Most common cause: degeneration + mechanical stress
✔ Classic symptom: radicular pain (e.g., sciatica), along with numbness or weakness
✔ MRI with contrast is the gold standard for diagnosis
✔ Conservative treatment (NSAIDs, physiotherapy, postural correction) is first-line
✔ Surgery indicated if pain is persistent, neurological deficit worsens, or cauda equina signs appear
✔ Nurses must focus on:
- Pain relief
- Neuro assessment
- Posture and mobility education
- Fall and complication prevention
✔ Educate patients about lifestyle changes, proper lifting, and long-term back care
✔ Early treatment and multidisciplinary approach lead to better recovery and quality of life
🦴🧠 POTT’S SPINE
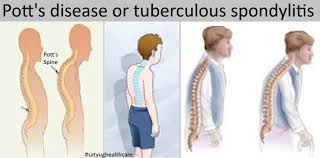
(Also known as Spinal Tuberculosis / Tuberculous Spondylitis)
🔷 📘 DEFINITION
Pott’s spine is a form of extrapulmonary tuberculosis that affects the vertebral column, leading to destruction of intervertebral discs and adjacent vertebrae, usually in the thoracic and lumbar regions.
🦴 It is the most common form of skeletal tuberculosis, and if untreated, it may result in:
- Spinal deformity (kyphosis)
- Neurological deficits (paraplegia)
- Abscess formation
🔷 ❗ CAUSES
The primary cause is infection by Mycobacterium tuberculosis, which spreads to the spine hematogenously from a primary site (usually the lungs) or via lymphatics.
✅ Pathways of Spread to the Spine:
- Hematogenous dissemination from pulmonary or renal TB
- Lymphatic spread from nearby infected nodes
- Direct extension from paravertebral abscess or infected tissues
🔍 Predisposing Factors:
| Factor | Description |
|---|---|
| Pulmonary TB | Most common primary site leading to spinal involvement |
| Immunosuppression | HIV/AIDS, cancer, corticosteroid therapy |
| Malnutrition | Compromises immune response |
| Poor living conditions | Crowded areas, low socioeconomic status |
| Inadequate TB treatment | Incomplete therapy can cause reactivation |
📍 Most commonly affected spinal regions:
- Thoracic spine (most frequent)
- Lumbar spine
- Cervical spine (less common, but more dangerous due to proximity to brainstem)
🧠🦴 TYPES OF POTT’S SPINE (SPINAL TUBERCULOSIS)
🔷 ✅ 1. Based on Anatomical Location in the Spine
| Type | Description |
|---|---|
| Cervical Pott’s spine | Rare but dangerous; may cause respiratory distress or quadriplegia |
| Thoracic Pott’s spine | Most common location (due to vascular supply); kyphosis and paraplegia are common |
| Thoracolumbar Pott’s spine | Junctional area vulnerable due to transition of spinal curvature |
| Lumbar Pott’s spine | Often associated with psoas abscess and lower limb weakness |
| Sacral/coccygeal TB | Rare; may present with pelvic pain or rectal/bladder issues |
🔷 🧬 2. Based on Pattern of Vertebral Involvement
| Type | Description |
|---|---|
| Paradiscal type (most common) | Infection starts at the end plates of adjacent vertebrae and spreads to the disc |
| Central type | Infection starts in the center of vertebral body → vertebral collapse |
| Anterior type | Involves anterior part of the vertebral body → leads to abscess formation and deformity |
| Appendiceal type | Involves posterior elements (spinous process, lamina, pedicles); rare |
| Skip lesions | Non-contiguous vertebral TB — lesions separated by normal vertebrae (seen in immunocompromised patients) |
🔷 🔍 3. Based on Presence of Complications
| Type | Description |
|---|---|
| Uncomplicated Pott’s spine | No neurological deficit or abscess; limited to bone and disc |
| Complicated Pott’s spine | Associated with: |
- Paravertebral abscess
- Kyphotic deformity
- Neurological deficits (Pott’s paraplegia)
🔷 📸 4. Based on Radiological Classification (Rajasekaran’s Types)
| Radiological Type | Key Feature |
|---|---|
| Type 1 – Paradiscal | Classic type involving disc and adjacent vertebral bodies |
| Type 2 – Central | Complete collapse of one vertebral body |
| Type 3 – Anterior | Subperiosteal spread under anterior longitudinal ligament |
| Type 4 – Posterior | Involvement of neural arch only (rare) |
| Type 5 – Skip lesions | Multiple non-contiguous vertebral involvement |
🧠🦴 PATHOPHYSIOLOGY OF POTT’S SPINE (SPINAL TUBERCULOSIS)
🔷 📘 Overview
Pott’s spine results from the hematogenous spread of Mycobacterium tuberculosis from a primary site (usually the lungs) to the vertebral column, leading to destruction of vertebrae and intervertebral discs, with potential for abscess formation, spinal deformity, and neurological compromise.
🔷 🔬 STEPS IN PATHOPHYSIOLOGY
1️⃣ Primary TB Infection
- Mycobacterium tuberculosis enters the body, typically affecting the lungs
- Bacteria may remain latent or become active in immunocompromised individuals
2️⃣ Hematogenous Spread to Spine
- TB bacilli spread via Batson’s venous plexus or arterial blood supply
- Preferentially lodge in the highly vascularized metaphyseal region of vertebral bodies
3️⃣ Initial Infection in the Vertebrae
- Most commonly in anterior part of the vertebral body or endplates
- In paradiscal type, infection spreads to adjacent vertebrae through disc space
4️⃣ Tissue Destruction and Granuloma Formation
- The immune response forms tuberculous granulomas with caseating necrosis
- Leads to:
- Destruction of bone tissue
- Collapse of vertebral body
- Loss of intervertebral disc height
5️⃣ Formation of Abscess
- Caseous necrotic material and pus may accumulate, forming a paravertebral or psoas abscess
- These abscesses can track along tissue planes to the groin or thoracic cavity
6️⃣ Spinal Deformity
- Collapsed vertebrae lead to kyphotic angulation (humpback)
- Severity depends on the number of vertebrae involved and rate of collapse
7️⃣ Neurological Involvement
- Pott’s paraplegia may occur due to:
- Direct compression by abscess or collapsed bone
- Ischemia from vascular compromise
- Granulomatous inflammation compressing the spinal cord
- Formation of epidural granulation tissue
🔷 🧠 Summary of Effects:
| Effect | Result |
|---|---|
| Bone destruction | Vertebral collapse, instability |
| Disc space narrowing | Loss of height, stiffness |
| Kyphosis/gibbus | Angular deformity, cosmetic and functional issues |
| Abscess formation | Paraspinal, psoas, or cold abscesses |
| Spinal cord compression | Paraplegia, sensory loss, bowel/bladder issues |
🔷 🩺 SIGNS AND SYMPTOMS
Pott’s spine presents with a combination of local, constitutional (systemic), and neurological symptoms, depending on the stage, location, and extent of spinal cord involvement.
✅ A. Constitutional Symptoms (Systemic TB signs)
- 🌡️ Low-grade fever (especially evening rise)
- 😓 Night sweats
- ⚖️ Weight loss
- 😴 Fatigue and malaise
- Anorexia (loss of appetite)
✅ B. Local Spinal Symptoms
| Symptom | Description |
|---|---|
| Back pain | Persistent, dull ache; worsens with movement or at night |
| Tenderness | On palpation over affected vertebrae |
| Stiffness | Reduced spinal flexibility |
| Muscle spasm | Especially in paraspinal muscles |
| Gibbus deformity | Sharp angular kyphosis due to vertebral collapse |
| Swelling or abscess | Cold abscess near spine or tracking along muscle (e.g., psoas abscess presenting as groin swelling) |
✅ C. Neurological Symptoms (if cord or nerve root compression occurs)
| Symptom | Description |
|---|---|
| Pott’s paraplegia | Weakness or paralysis of lower limbs |
| Numbness or tingling | Sensory disturbances |
| Loss of bladder/bowel control | In advanced or severe spinal cord compression |
| Spasticity or reflex changes | Hyperreflexia, positive Babinski reflex |
🔷 🧪 DIAGNOSIS OF POTT’S SPINE
A combination of clinical suspicion, imaging, and laboratory tests is essential.
✅ A. Imaging Studies
| Test | Purpose |
|---|---|
| X-ray (Spine) | Shows late-stage changes: vertebral collapse, disc space narrowing, kyphosis, gibbus |
| MRI with contrast | Gold standard |
| ‣ Early detection of disc, bone, spinal cord, and abscess involvement | |
| ‣ Detects spinal cord compression | |
| CT Scan (Spine) | Better bone detail; used for surgical planning or when MRI is contraindicated |
| Ultrasound/CT Abdomen | Detects psoas or paravertebral abscesses |
✅ B. Laboratory Tests
| Test | Findings |
|---|---|
| CBC | Mild anemia, leukocytosis |
| ESR / CRP | Elevated — markers of inflammation |
| Mantoux test (Tuberculin skin test) | May be positive but not definitive |
| GeneXpert / CB-NAAT | Detects Mycobacterium tuberculosis DNA in tissue or pus |
| AFB staining / Culture (Ziehl–Neelsen) | Confirms TB bacilli in biopsy or aspirate |
| Biopsy / FNAC | Confirms granulomatous inflammation with caseous necrosis (gold standard) |
| HIV test | Recommended due to association with immunosuppression |
💊🦴 MEDICAL MANAGEMENT OF POTT’S SPINE
(Tuberculous Spondylitis)
🎯 Goals of Medical Treatment:
✅ Eradicate Mycobacterium tuberculosis
✅ Prevent or manage neurological deficits
✅ Control spinal pain and inflammation
✅ Prevent progression to deformity
✅ Promote vertebral healing and spinal stability
🔷 ✅ 1. Anti-Tuberculosis Therapy (ATT)
🦠 Mainstay of Treatment
According to WHO and RNTCP (India) guidelines, Pott’s spine is treated like extrapulmonary tuberculosis using first-line anti-TB drugs.
💊 Standard Regimen (6–12 months)
| Phase | Drugs | Duration |
|---|---|---|
| Intensive Phase | HRZE → Isoniazid (H) | |
| Rifampicin (R) | ||
| Pyrazinamide (Z) | ||
| Ethambutol (E) | First 2 months | |
| Continuation Phase | HR (± E based on case) | Next 10 months (may vary from 4–10 months based on response) |
📌 In spinal TB with neurological involvement, 12–18 months of ATT is often recommended.
🚨 Monitor for Drug Toxicity:
- Liver function (Hepatotoxicity – H, R, Z)
- Vision (Optic neuritis – E)
- Neuropathy (Isoniazid – give pyridoxine supplement)
- Compliance using DOTS (Directly Observed Treatment, Short-course) approach
🔷 ✅ 2. Supportive Therapy
| Supportive Measure | Purpose |
|---|---|
| Bed Rest | Especially in early or painful stages (4–6 weeks) to reduce stress on spine |
| Analgesics | NSAIDs (ibuprofen, diclofenac) for pain and inflammation |
| Steroids (short course) | In cases of cord compression, edema, or severe inflammatory response |
| Nutritional support | High-protein, calorie-rich diet with vitamins (especially B-complex, C, D) |
| Orthotic support | Braces or spinal corsets to prevent kyphotic deformity and support healing spine |
🔷 🧪 3. Management of Abscess (if present)
| Type of Abscess | Management |
|---|---|
| Cold abscess | May resolve with ATT |
| If large or fluctuant → aspiration or drainage under imaging guidance | |
| Psoas abscess | Ultrasound-guided or CT-guided aspiration |
| Repeat drainage may be required in chronic cases |
🔷 🧠 4. Neurological Deficit Management
- Most early neurological symptoms respond well to ATT
- Steroids may be given short-term to reduce spinal cord edema
- Neurological improvement usually starts within 2–6 weeks of therapy
- If no improvement or worsening → consider surgical decompression
🔷 📅 Monitoring Response to Treatment
| Monitor | Frequency |
|---|---|
| ESR, CRP | Every 4–6 weeks to assess inflammation |
| Neurological exams | Periodically to detect recovery or deterioration |
| MRI (follow-up) | 3–6 months if needed to assess healing, abscess resolution |
| Drug side effects | Monthly or as symptoms appear |
🛠️🧠 SURGICAL MANAGEMENT OF POTT’S SPINE
(Tuberculous Spondylitis)
🎯 Goals of Surgical Treatment:
✅ Decompress the spinal cord and nerve roots
✅ Drain abscesses or infected tissue
✅ Correct or prevent spinal deformity (kyphosis)
✅ Stabilize the spinal column
✅ Relieve pain and restore function
🔷 ✅ INDICATIONS FOR SURGERY
Surgery is not needed in all cases, but becomes essential in the following:
| Indication | Example |
|---|---|
| 1. Neurological deficit | Pott’s paraplegia (especially progressive or late-onset) |
| 2. Large abscess | Psoas or paravertebral abscess not responding to aspiration |
| 3. Spinal instability | Collapse of vertebrae, risk of mechanical instability |
| 4. Severe kyphotic deformity | Progressive or disabling spinal curvature |
| 5. Failure of medical treatment | No improvement after 3–6 months of ATT |
| 6. Diagnostic uncertainty | Biopsy or decompression when diagnosis is doubtful |
🔷 🛠️ TYPES OF SURGICAL PROCEDURES
🔧 1. Anterior Decompression with Fusion
- Most commonly performed surgery for thoracic and lumbar TB
- Removal of infected vertebral bodies, pus, and granulation tissue
- Followed by bone grafting and fusion using autologous bone (usually from iliac crest)
- May use titanium cages or mesh to support anterior column
🔧 2. Posterior Decompression (Laminectomy)
- Indicated when compression is from the posterior elements or in cervical spine TB
- May also be used in combination with anterior approach for 360° decompression
🔧 3. Instrumented Stabilization (Spinal Fixation)
- Use of rods, screws, and plates to stabilize the spine
- Prevents deformity progression and allows early mobilization
- May be done posteriorly or anteriorly, depending on lesion site
🔧 4. Costotransversectomy / Transthoracic Approach
- In thoracic TB, especially for large abscesses or vertebral body destruction
- Allows access to paravertebral abscesses and anterior spinal structures
🔧 5. Abscess Drainage / Debridement
- CT- or ultrasound-guided aspiration for cold abscesses (e.g., psoas)
- Open drainage if abscess is large, organized, or causing compressive symptoms
🔧 6. Corpectomy with Cage Placement
- Removal of diseased vertebral bodies and reconstruction with mesh cage + bone graft
🔷 ✅ POSTOPERATIVE CARE
- Continue anti-tubercular therapy (ATT) for 12–18 months
- Monitor neurological status and signs of infection
- Provide bracing or spinal support post-surgery as needed
- Early physiotherapy and ambulation under guidance
- Regular follow-up with MRI or X-rays to assess healing and alignment
🧠📝 Summary
| Surgery Type | Best for |
|---|---|
| Anterior decompression + fusion | Thoracic/lumbar TB with cord compression |
| Posterior fixation | Spinal instability, multi-level involvement |
| Abscess drainage | Cold/psoas abscess |
| Biopsy or open debridement | Diagnostic uncertainty, severe cases |
| Combined anterior-posterior | Severe kyphosis, extensive disease |
👩⚕️🧠 NURSING MANAGEMENT OF POTT’S SPINE
(Spinal Tuberculosis / Tuberculous Spondylitis)
🔷 🎯 NURSING CARE OBJECTIVES
✅ Control infection and inflammation
✅ Relieve pain and support spinal alignment
✅ Monitor and preserve neurological function
✅ Prevent deformity and complications
✅ Promote early mobility and rehabilitation
✅ Educate patient and caregivers
✅ Ensure adherence to long-term treatment (ATT)
🔷 📝 NURSING ASSESSMENT
🔍 Subjective Data:
- Pain location and intensity (especially back or neck pain)
- History of TB or exposure
- Fatigue, fever, weight loss
- Paresthesia or muscle weakness
- Difficulty walking or voiding
🔍 Objective Data:
- Gibbus deformity, tenderness, muscle spasms
- Restricted spinal mobility
- Signs of abscess (swelling, groin bulge, warmth)
- Neurological signs: reflex changes, motor/sensory loss
- Elevated temperature, ESR, or CRP levels
🔷 🧰 NURSING INTERVENTIONS
💊 1. Infection Control and Drug Compliance
- Administer anti-tubercular therapy (ATT) on time
- Monitor for side effects (hepatotoxicity, visual changes, peripheral neuropathy)
- Provide vitamin B6 (pyridoxine) with isoniazid to prevent neuropathy
- Encourage DOTS approach if applicable
- Educate on completing full course (6–18 months)
🤕 2. Pain Relief and Comfort Measures
- Administer NSAIDs or prescribed analgesics
- Encourage bed rest during acute pain phase
- Apply heat to reduce muscle spasm (if no abscess)
- Ensure proper spinal alignment using firm mattress or spinal brace
🧠 3. Neurological Monitoring
- Perform frequent neurological checks:
- Limb movement and strength
- Reflexes
- Bladder/bowel control
- Sensation (light touch, pain, vibration)
- Monitor for signs of Pott’s paraplegia or cauda equina syndrome
🛌 4. Positioning and Mobility Support
- Encourage log rolling technique to maintain spinal alignment
- Assist with gradual mobilization using spinal orthoses/braces
- Prevent pressure sores through repositioning and skin care
- Collaborate with physiotherapy for ROM and strengthening exercises
🧬 5. Nutrition and Hydration
- Promote a high-protein, high-calorie diet with iron, calcium, and vitamins
- Encourage fluids to prevent constipation and support metabolism
- Refer to dietitian if the patient is malnourished or immunocompromised
💬 6. Health Education and Psychological Support
- Teach about:
- Disease nature and duration of treatment
- Importance of ATT adherence
- Safe handling of sputum or drainage (if open TB present)
- Address fears about paralysis or deformity
- Encourage participation in support groups or counseling sessions
🏥 7. Postoperative Nursing Care (if surgery done)
- Monitor vital signs, wound site, drains
- Assess for infection, CSF leak, or bleeding
- Provide IV antibiotics, pain management
- Encourage early ambulation as per surgeon’s instructions
- Continue spinal brace use and physiotherapy
🔷 📋 DISCHARGE TEACHING
✅ Complete ATT as prescribed (up to 18 months)
✅ Attend regular follow-ups and lab monitoring
✅ Use brace or support devices as advised
✅ Practice safe posture, lifting, and mobility techniques
✅ Report signs of worsening pain, weakness, or bladder changes immediately
✅ Maintain proper nutrition and personal hygiene
✅ Educate family about infection prevention and caregiving support
⚠️🧠 COMPLICATIONS OF POTT’S SPINE
(Tuberculous Spondylitis)
Pott’s spine can lead to severe, sometimes irreversible complications, especially if left untreated or diagnosed late.
🔷 ❗ MAJOR COMPLICATIONS
| 🔥 Complication | 📋 Description |
|---|---|
| 1. Spinal deformity (Kyphosis/Gibbus) | Collapse of vertebral bodies leads to angular kyphotic hump |
| 2. Pott’s Paraplegia | Compression of spinal cord results in motor weakness/paralysis of lower limbs |
| 3. Cold abscess formation | Paravertebral or psoas abscess may spread and cause pressure effects or rupture |
| 4. Neurological deficits | Numbness, tingling, reflex loss, loss of bowel/bladder control |
| 5. Spinal instability | Destruction of vertebrae leads to misalignment and risk of spinal collapse |
| 6. Persistent or recurrent infection | Due to incomplete ATT or resistant TB strains |
| 7. Chronic pain and disability | Impaired mobility and functional dependence |
| 8. Social and psychological issues | Body image issues (kyphosis), anxiety, depression, isolation |
✅✨ KEY POINTS TO REMEMBER
(For nursing practice, exams, and patient education)
✔ Pott’s spine = spinal tuberculosis → destruction of vertebrae + disc
✔ Most common in the thoracic spine, followed by lumbar
✔ Commonly presents with back pain, spinal deformity, and constitutional symptoms (fever, weight loss)
✔ MRI is the gold standard for early detection and assessing cord compression
✔ Anti-tubercular therapy (ATT) is the cornerstone of treatment (at least 12–18 months)
✔ Surgery is indicated for:
- Neurological deficits
- Large abscess
- Spinal instability/deformity ✔ Nurses play a critical role in:
- Medication adherence
- Neuro checks
- Rehabilitation
- Emotional support ✔ Early detection + proper treatment = excellent prognosis and functional recovery
✔ Preventable with early diagnosis of TB and public health education
🧍♂️💪 REHABILITATION IN MUSCULOSKELETAL PROBLEMS
🔷 📘 DEFINITION
Musculoskeletal rehabilitation refers to a comprehensive and structured process aimed at restoring function, mobility, strength, endurance, and independence in individuals with injury, disease, deformity, or surgery involving the bones, joints, muscles, tendons, or ligaments.
🩼 The goal is to:
- Alleviate pain
- Enhance physical capacity
- Prevent deformity
- Improve quality of life
- Facilitate return to work and daily living
🔷 🔍 INDICATIONS FOR MUSCULOSKELETAL REHABILITATION
Rehabilitation is essential in patients with:
✅ Fractures and joint dislocations
✅ Osteoarthritis and rheumatoid arthritis
✅ Post-operative recovery (e.g., joint replacement, spinal surgery)
✅ Amputations
✅ Low back pain or disc prolapse
✅ Muscle strains or ligament injuries
✅ Spinal cord injury or deformities (e.g., scoliosis, Pott’s spine)
✅ Congenital or developmental disorders (e.g., cerebral palsy)
🔷 🎯 GOALS OF REHABILITATION
- Relieve pain and inflammation
- Restore joint mobility and muscle strength
- Improve gait and posture
- Prevent contractures and deformities
- Promote independence in ADLs (activities of daily living)
- Provide psychological and social support
🔷 🧰 KEY COMPONENTS OF REHABILITATION PROGRAM
✅ 1. Medical Management
- Pain control: NSAIDs, analgesics, muscle relaxants
- Treatment of inflammation: corticosteroids, DMARDs (in arthritis)
- Antibiotics (if infectious), anti-TB drugs (in Pott’s spine)
- Osteoporosis management: calcium, vitamin D, bisphosphonates
✅ 2. Physical Therapy / Physiotherapy
| Goal | Interventions |
|---|---|
| Improve ROM & mobility | Passive & active joint exercises |
| Strengthen muscles | Resistance and isotonic exercises |
| Reduce pain | Hot/cold therapy, TENS, ultrasound |
| Improve posture/gait | Gait training, balance exercises |
| Prevent contractures | Splinting, stretching, PROM |
✅ 3. Occupational Therapy
- Focuses on independent functioning in daily life
- Training in:
- Self-care: dressing, eating, bathing
- Home and work modifications
- Use of adaptive devices (e.g., reachers, grab bars)
- Energy conservation techniques for chronic pain/fatigue patients
✅ 4. Orthotic and Prosthetic Support
| Device | Purpose |
|---|---|
| Braces/splints | Stabilize or correct deformity |
| Walkers/canes | Improve mobility and prevent falls |
| Prosthetic limbs | For amputees to regain ambulation |
| Shoe inserts | Correct gait issues (e.g., flat foot) |
✅ 5. Psychological and Social Support
- Emotional counseling for depression, anxiety, body image
- Support groups and family counseling
- Vocational therapy and career re-training if disability affects job
- Encourage independence, self-confidence, and motivation
✅ 6. Patient and Family Education
- Teach about disease process and home care
- Proper use of assistive devices
- Importance of exercise adherence
- Fall prevention and environmental safety at home
- Dietary advice: protein, calcium, vitamin D-rich foods
🔷 🧑⚕️ ROLE OF NURSE IN REHABILITATION
✔ Assess mobility, pain, and independence level
✔ Administer medications and monitor effects
✔ Assist in exercise and ambulation
✔ Ensure skin care, prevent pressure sores
✔ Educate on posture, joint protection, and assistive device use
✔ Provide emotional support and encourage social interaction
✔ Coordinate with multidisciplinary team (PT, OT, physician, psychologist)
🔷 📅 STAGES OF MUSCULOSKELETAL REHABILITATION
| Stage | Focus |
|---|---|
| Acute Stage | Pain relief, inflammation control, immobilization |
| Subacute Stage | Start gentle ROM, prevent stiffness and atrophy |
| Rehabilitation Stage | Strengthening, mobility training, ADL retraining |
| Maintenance Stage | Continue home exercises, return to work/society |
✅✨ KEY POINTS TO REMEMBER
✔ Rehabilitation is a multi-disciplinary, patient-centered process
✔ Begins early and continues through recovery and reintegration
✔ Includes physical, psychological, and social dimensions
✔ Individualized plans are essential based on diagnosis and ability
✔ Nurses play a vital role in motivation, education, and continuity of care
✔ Goal = maximum functional independence + best possible quality of life
🦿🧍♂️ PROSTHESIS FOR PATIENTS WITH MUSCULOSKELETAL PROBLEMS
🔷 📘 DEFINITION
A prosthesis (plural: prostheses) is an artificial device used to replace a missing body part, typically a limb, to restore functional mobility, improve cosmetic appearance, and enhance quality of life.
🧠 Prostheses are especially crucial for patients with amputations, congenital limb deficiencies, or after limb salvage surgeries due to trauma, tumors, or infections.
🔷 🎯 GOALS OF PROSTHETIC REHABILITATION
✅ Restore mobility and independence
✅ Improve gait and body mechanics
✅ Prevent secondary deformities and complications
✅ Facilitate psychological and social reintegration
✅ Enhance patient’s self-confidence and body image
🔷 🦴 INDICATIONS FOR PROSTHESIS
Prosthetic fitting may be necessary in patients with:
- Traumatic amputation (e.g., accidents, war injuries)
- Surgical amputation (due to diabetes, gangrene, tumors, osteomyelitis)
- Congenital limb absence or deformity
- Musculoskeletal tumors (after limb resection)
- Severe infections or vascular diseases
- Failed joint replacement requiring limb sacrifice
🔷 🧬 TYPES OF PROSTHESES
✅ A. Based on Limb Involved
| Type | Description |
|---|---|
| Upper limb prosthesis | Replaces hand, forearm, or entire arm (cosmetic or functional) |
| Lower limb prosthesis | Replaces foot, leg, or thigh to assist in ambulation |
✅ B. Based on Functionality
| Type | Features |
|---|---|
| Passive (cosmetic) | Lightweight, for appearance only |
| Body-powered | Controlled by body movement (e.g., shoulder harness) |
| Externally powered | Uses motors and batteries (e.g., myoelectric hand) |
| Hybrid prosthesis | Combines body-powered and electric components |
| Activity-specific | For sports (e.g., running blades), swimming, etc. |
✅ C. Based on Amputation Level (Lower Limb)
| Amputation Level | Prosthesis Type |
|---|---|
| Transfemoral (above knee) | Artificial knee joint with socket and foot |
| Transtibial (below knee) | Socket with pylon and foot (no knee joint needed) |
| Syme’s amputation | Foot prosthesis with ankle alignment |
| Hip disarticulation | Full leg prosthesis with pelvic support |
🔷 🧰 COMPONENTS OF A LIMB PROSTHESIS
| Component | Function |
|---|---|
| Socket | Custom-fitted mold for the residual limb |
| Suspension | Holds the prosthesis in place (belts, suction, straps) |
| Pylon | The supportive structure (metal or carbon fiber) |
| Joints | Artificial knee or elbow (if needed) |
| Terminal device | Foot or hand; may be functional or cosmetic |
🔷 🏥 PROSTHETIC REHABILITATION PROCESS
⏳ Phases:
- Pre-prosthetic phase
- Wound healing, pain control
- Residual limb shaping and strengthening
- Psychological support and patient motivation
- Prosthetic fitting
- Measurement and customization
- Trial fitting and adjustments
- Training and adaptation
- Gait training and limb usage
- Occupational therapy (especially for upper limb)
- Follow-up and maintenance
- Skin care, fit checks, realignments
- Replacement every 3–5 years or earlier if needed
🔷 👩⚕️ ROLE OF NURSE IN PROSTHETIC CARE
✔ Educate on limb hygiene and skin inspection (prevent pressure ulcers)
✔ Monitor for signs of infection, swelling, or poor prosthetic fit
✔ Support emotional and psychological adjustment
✔ Encourage exercise and physiotherapy compliance
✔ Assist in prosthesis donning/doffing training
✔ Reinforce fall prevention and balance techniques
✔ Coordinate with prosthetist, physiotherapist, and psychologist
🔷 🧠 PSYCHOSOCIAL CONSIDERATIONS
- Address grief, fear, and body image concerns
- Encourage peer support groups and role models
- Promote vocational rehabilitation and community integration
- Support family in understanding patient’s physical and emotional needs
✅✨ KEY POINTS TO REMEMBER
✔ Prosthesis restores mobility, function, and confidence in limb-loss patients
✔ Requires a multi-disciplinary approach for success
✔ Proper socket fitting and skin care are essential for long-term use
✔ Rehabilitation includes physical, emotional, and social support
✔ Nurses play a key role in education, motivation, and long-term care continuity
✔ Each prosthesis must be customized to patient’s needs, lifestyle, and goals
💊🧍♂️ MEDICATIONS FOR MUSCULOSKELETAL PROBLEMS
(Structured for clinical and academic use)
🔷 1. Nonsteroidal Anti-inflammatory Drugs (NSAIDs)
| Drug Names | Ibuprofen, Diclofenac, Naproxen, Aceclofenac |
|---|
📌 Uses:
- Reduce pain, inflammation, and swelling in arthritis, sprains, low back pain, and post-injury recovery.
⚙️ Action:
- Inhibits cyclooxygenase (COX-1 and COX-2) enzymes → reduces prostaglandin synthesis → decreases inflammation and pain.
✅ Indications:
- Osteoarthritis, rheumatoid arthritis, sprains, fractures, post-operative pain
❌ Contraindications:
- Peptic ulcer disease
- Renal impairment
- Bleeding disorders
- Pregnancy (especially 3rd trimester)
👩⚕️ Role of Nurse:
- Administer after food to prevent gastric irritation
- Monitor for signs of GI bleeding (e.g., black stools)
- Monitor renal function in long-term use
- Educate on dosage compliance and food intake
⚠️ Side Effects:
- Gastric ulcer, dyspepsia
- Kidney dysfunction
- Dizziness, headache
- Risk of bleeding
✨ Key Points:
✔ Avoid long-term use without monitoring
✔ Take with meals
✔ Avoid combining with other NSAIDs or steroids
🔷 2. Muscle Relaxants
| Drug Names | Tizanidine, Baclofen, Cyclobenzaprine, Methocarbamol |
|---|
📌 Uses:
- Relief of muscle spasms, stiffness, and cramps in back pain, disc prolapse, or injury.
⚙️ Action:
- Acts on the central nervous system to depress polysynaptic reflexes in the spinal cord → reduces muscle tone.
✅ Indications:
- Low back pain, muscle strains, spinal cord injury, post-op muscle tension
❌ Contraindications:
- Liver dysfunction
- Severe hypotension
- Pregnancy
- Concomitant CNS depressants
👩⚕️ Role of Nurse:
- Monitor level of consciousness, BP, and coordination
- Caution against driving or operating machinery
- Educate about gradual withdrawal to avoid rebound spasticity
⚠️ Side Effects:
- Drowsiness, dizziness
- Dry mouth
- Hypotension
- Fatigue
✨ Key Points:
✔ Monitor for sedation
✔ Start with low dose and titrate
✔ Avoid alcohol or CNS depressants
🔷 3. Analgesics (Non-opioid & Opioid)
| Drug Names | Paracetamol, Tramadol, Tapentadol, Morphine (for severe cases) |
|---|
📌 Uses:
- Pain management in musculoskeletal conditions (acute or chronic)
⚙️ Action:
- Paracetamol: Central inhibition of prostaglandin synthesis
- Tramadol: Weak opioid agonist and serotonin/norepinephrine reuptake inhibitor
✅ Indications:
- Osteoarthritis, post-operative pain, disc herniation, severe musculoskeletal pain
❌ Contraindications:
- Severe liver dysfunction (for paracetamol)
- History of opioid addiction
- Head injury (opioids)
👩⚕️ Role of Nurse:
- Monitor pain scale and sedation level
- Monitor for signs of respiratory depression (opioids)
- Educate on avoiding overdose, especially with paracetamol
⚠️ Side Effects:
- Nausea, constipation
- Dizziness, sedation
- Liver toxicity (paracetamol)
- Dependence (opioids)
✨ Key Points:
✔ Use lowest effective dose
✔ Paracetamol is safer in elderly
✔ Avoid combining multiple paracetamol-containing drugs
🔷 4. Calcium and Vitamin D Supplements
| Drug Names | Calcium carbonate, Calcium citrate + Vitamin D3 (Cholecalciferol) |
|---|
📌 Uses:
- Improve bone health, prevent/treat osteoporosis and fractures.
⚙️ Action:
- Calcium: Bone mineralization
- Vitamin D: Enhances calcium absorption in intestine
✅ Indications:
- Osteoporosis, osteomalacia, fracture healing, post-menopausal women
❌ Contraindications:
- Hypercalcemia
- Kidney stones
- Severe renal failure
👩⚕️ Role of Nurse:
- Administer after meals, ensure hydration
- Monitor for signs of hypercalcemia
- Encourage weight-bearing exercises
⚠️ Side Effects:
- Constipation
- Hypercalcemia (nausea, confusion, arrhythmia)
- Kidney stones
✨ Key Points:
✔ Ensure adequate fluid intake
✔ Combine with exercise for better bone strength
✔ Avoid excess dosing
🔷 5. Disease-Modifying Anti-Rheumatic Drugs (DMARDs)
| Drug Names | Methotrexate, Sulfasalazine, Leflunomide, Hydroxychloroquine |
|---|
📌 Uses:
- Slow disease progression and prevent joint destruction in autoimmune arthritis.
⚙️ Action:
- Suppress immune activity to reduce chronic inflammation in joints.
✅ Indications:
- Rheumatoid arthritis
- Psoriatic arthritis
- Ankylosing spondylitis
❌ Contraindications:
- Liver/kidney dysfunction
- Pregnancy (especially Methotrexate)
- Immunosuppressed patients
👩⚕️ Role of Nurse:
- Monitor CBC, LFT, renal function regularly
- Educate on infection prevention and contraception
- Ensure compliance due to slow onset of action
⚠️ Side Effects:
- Liver toxicity
- Bone marrow suppression
- GI upset
- Photosensitivity
- Oral ulcers (especially with Methotrexate)
✨ Key Points:
✔ Supplement with folic acid to reduce side effects
✔ Strict monitoring is essential
✔ Not for quick pain relief — takes weeks to months for effect
🔷 6. Corticosteroids
| Drug Names | Prednisolone, Methylprednisolone, Dexamethasone |
|---|
📌 Uses:
- Reduce severe inflammation in acute flare-ups of arthritis or autoimmune conditions.
⚙️ Action:
- Suppress immune response and inflammation by inhibiting prostaglandins and cytokines.
✅ Indications:
- Rheumatoid arthritis flare
- Severe disc inflammation
- Post-op inflammation
❌ Contraindications:
- Active infections
- Diabetes
- Peptic ulcer disease
- Uncontrolled hypertension
👩⚕️ Role of Nurse:
- Monitor blood sugar, BP, and signs of infection
- Educate on gradual tapering (never stop abruptly)
- Administer with food to prevent gastric upset
⚠️ Side Effects:
- Weight gain, mood swings
- Hyperglycemia, hypertension
- Osteoporosis (long-term use)
- Gastric ulcers
- Immunosuppression
✨ Key Points:
✔ Use short-term and lowest dose possible
✔ Provide calcium + vitamin D for bone protection
✔ Watch for masking of infection signs
🦴🛠️ REPLACEMENT SURGERIES IN MUSCULOSKELETAL DISORDERS
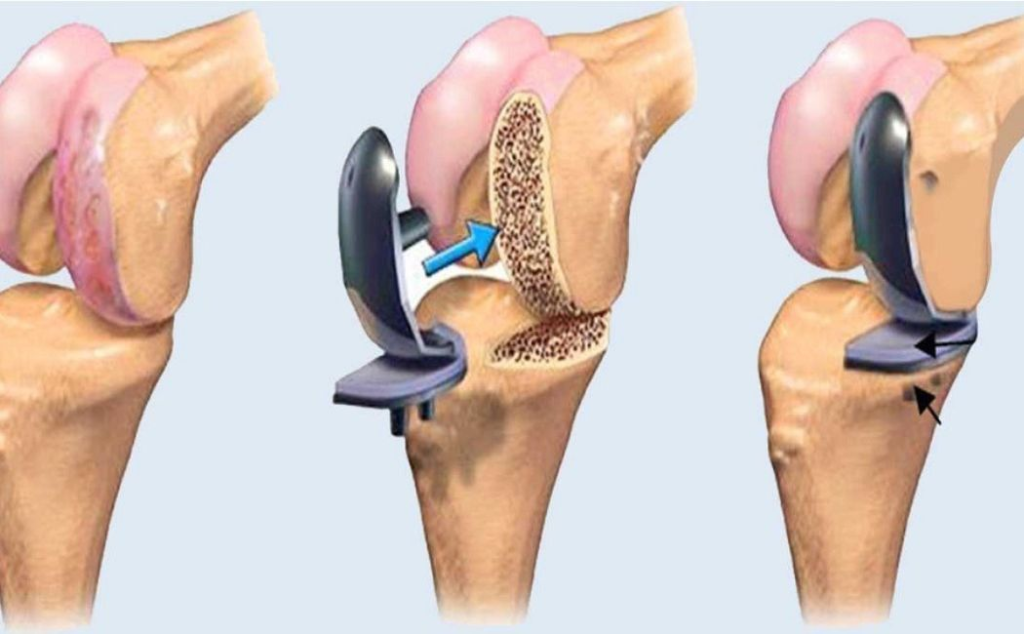
🔷 📘 DEFINITION
Replacement surgery (also known as arthroplasty) involves removing a damaged or diseased joint or bone and replacing it with an artificial prosthetic implant to restore mobility, function, and relieve pain.
🔷 🎯 GOALS OF REPLACEMENT SURGERY
✅ Relieve chronic joint pain
✅ Restore range of motion and function
✅ Improve joint alignment and stability
✅ Prevent or correct deformity
✅ Enhance quality of life and independence
🔷 🧍♂️ INDICATIONS
Replacement surgeries are usually performed in cases of:
- Severe osteoarthritis or rheumatoid arthritis
- Avascular necrosis (bone death due to poor blood supply)
- Joint deformity or contractures
- Fractures that cannot be repaired (e.g., femoral neck)
- Tumors involving joints or bones
- Failed previous surgeries or implants
🔷 🔍 COMMON TYPES OF REPLACEMENT SURGERIES
✅ 1. Total Hip Replacement (THR)
🔹 Diseased femoral head and acetabulum are replaced with prosthetic components
🔹 Indicated in hip arthritis, fractures, avascular necrosis
✅ 2. Total Knee Replacement (TKR)
🔹 Damaged femoral, tibial, and patellar surfaces are replaced with metal and plastic implants
🔹 Commonly done in advanced osteoarthritis or RA
✅ 3. Shoulder Replacement
🔹 Involves replacing humeral head and/or glenoid cavity
🔹 Used in rotator cuff arthropathy, shoulder fractures, arthritis
✅ 4. Elbow, Wrist, and Ankle Replacement
🔹 Less common
🔹 Indicated in trauma, rheumatoid arthritis, or post-injury deformities
✅ 5. Hemiarthroplasty
🔹 Partial joint replacement (e.g., replacing only the femoral head in hip fracture)
✅ 6. Spinal Disc Replacement
🔹 Artificial disc replaces the damaged intervertebral disc
🔹 Indicated in degenerative disc disease
🔷 🛠️ TYPES OF PROSTHETIC MATERIALS
| Material | Properties |
|---|---|
| Metal alloys | Stainless steel, titanium — durable and strong |
| Ceramics | Smooth surface, low wear rate |
| High-density polyethylene | Used for articulating surfaces (e.g., tibial component in TKR) |
| Cemented vs. uncemented fixation | Cemented uses bone cement; uncemented relies on bone ingrowth |
🔷 📋 PREOPERATIVE CONSIDERATIONS
- Thorough medical history and physical exam
- Imaging (X-ray, MRI, CT) to assess joint status
- Lab investigations (CBC, ESR, CRP, renal function)
- Infection screening (urine, dental, skin)
- Patient education: expectations, physiotherapy, postoperative care
- Control of diabetes, hypertension, anemia, infections
🔷 🏥 POSTOPERATIVE CARE
🛏️ Immediate Post-Op:
- Pain control (PCA pump, NSAIDs, opioids)
- IV fluids, antibiotics, DVT prophylaxis
- Monitoring for complications (bleeding, infection, embolism)
- Use of drains, catheters, TED stockings
🚶 Early Rehabilitation:
- Start physiotherapy within 24–48 hours
- Support with walker, crutches, or walking frame
- Teach joint protection and movement restrictions (e.g., no crossing legs after THR)
🩺 Follow-Up:
- Wound care and suture removal
- Functional evaluation
- Long-term prosthetic care and infection prevention
🔷 👩⚕️ ROLE OF NURSE IN REPLACEMENT SURGERY CARE
✔ Provide preoperative education and psychological support
✔ Ensure informed consent and pre-op prep
✔ Postoperative monitoring: vitals, pain, wound, neurovascular checks
✔ Assist in early mobilization and physiotherapy coordination
✔ Prevent complications: DVT, pneumonia, pressure ulcers
✔ Educate patient about:
- Home care and joint safety
- Signs of infection or implant failure
- Long-term follow-up
🔷 ⚠️ POTENTIAL COMPLICATIONS
| Complication | Description |
|---|---|
| Infection | Superficial or deep joint infection (may need implant removal) |
| DVT/PE | Clot formation due to immobility |
| Loosening of implant | May occur over years → causes pain or instability |
| Dislocation | Especially in hip replacement if precautions not followed |
| Nerve injury | Rare, but possible |
| Leg length discrepancy | Sometimes occurs after hip replacement |
✅✨ KEY POINTS TO REMEMBER
✔ Replacement surgery = removal of damaged joint + insertion of artificial component
✔ Common sites: hip, knee, shoulder
✔ Always includes pre-op planning, surgical intervention, post-op rehab
✔ Nurses play a key role in monitoring, mobilizing, preventing complications, and educating
✔ Lifelong care and regular follow-up are essential for prosthesis longevity
✔ Encourage weight management and joint-friendly activities to protect implants