BSC SEM 6 UNIT 3 MIDWIFERY / OBSTETRIC AND GYNECOLOGY NURSING- I
UNIT 3 Assessment and management of normal pregnancy(ante- natal)
🩺 Assessment and Management of Normal Pregnancy (Antenatal Care)

Antenatal care (ANC) is systematic, regular monitoring of a pregnant woman and her fetus from the time of conception until the onset of labor to ensure the wellbeing of both.
🌸 Objectives of Antenatal Care
- Ensure the birth of a healthy baby.
- Maintain the health of the mother during pregnancy.
- Recognize high-risk pregnancies and provide early interventions.
- Provide health education (nutrition, hygiene, childbirth preparation).
- Prepare the mother and family for labor, delivery, and parenthood.
I. 👩⚕️ Initial Assessment (First Visit)
Usually occurs around 6–12 weeks of gestation.
🔍 A. History Collection
- Personal details: Name, age, address, occupation.
- Obstetric history:
- Gravida (G), Para (P), Abortions (A), Living children (L) – e.g., G3P2A0L2.
- Menstrual history:
- Last Menstrual Period (LMP)
- Expected Date of Delivery (EDD) = LMP + 9 months + 7 days.
- Medical/surgical history: Diabetes, hypertension, asthma, surgeries.
- Family history: Genetic disorders, twin pregnancy.
- Socioeconomic status: Income, education, housing.
- Dietary habits, addictions (smoking, alcohol, etc.).
🩻 B. Physical Examination
- General Examination:
- Height and weight (baseline).
- BMI calculation.
- Blood pressure (rule out preeclampsia).
- Pallor, edema, jaundice, thyroid, lymph nodes.
- Breast Examination:
- To detect lumps or nipple retraction.
- Educate about breast care.
- Abdominal Examination:
- Palpation of uterus (fundal height).
- Lie, presentation, and fetal heart sounds after 20 weeks.
- Pelvic Examination:
- Done only if needed (bleeding, discharge, etc.)
🧪 C. Investigations
- Hemoglobin (Hb): To detect anemia.
- Blood group and Rh typing.
- Blood sugar (Fasting/Random): For gestational diabetes.
- Urine test: For albumin, sugar, and infection.
- HIV, HBsAg, VDRL (mandatory tests).
- Ultrasound:
- First trimester: Dating scan.
- Second trimester: Anomaly scan (~18–22 weeks).
- Third trimester: Growth and position.
II. 📅 Subsequent Antenatal Visits
WHO/INC Guidelines (Minimum Visits):
- 1st visit: By 12 weeks (1st trimester)
- 2nd visit: Between 14–26 weeks (2nd trimester)
- 3rd visit: Between 28–34 weeks
- 4th visit: After 36 weeks
(More visits if high-risk pregnancy)
✍️ Check-ups at Each Visit
- Weight and BP monitoring
- Urine test (sugar & albumin)
- Fundal height measurement (assess fetal growth)
- Fetal heart rate (120–160 bpm)
- Fetal movements after 20 weeks
- Look for danger signs:
- Bleeding
- Severe headache
- Swelling of hands/face
- Blurred vision
- Reduced fetal movement
III. 💊 Management of Normal Pregnancy
✅ Routine Care and Advice
- Iron & Folic Acid (IFA):
- 100 mg elemental iron + 500 mcg folic acid once daily after 14 weeks, for 180 days.
- Calcium Supplement:
- 500 mg twice daily from 14 weeks till 6 months postpartum.
- Tetanus + Adult Diphtheria (Td) Injection:
- 2 doses: 1st at 16 weeks, 2nd after 4 weeks (or booster if previously immunized).
- Deworming:
- Single dose of Albendazole 400 mg after 2nd trimester.
- Nutrition:
- High protein, iron, calcium, and fiber diet.
- 300 kcal extra per day.
- Hygiene:
- Personal cleanliness, avoid infections.
- Rest and Sleep:
- Minimum 8 hours at night + rest during day.
- Exercise:
- Light physical activity (walking, yoga).
- Sexual activity:
- Safe unless contraindicated by doctor.
🧘♀️ Health Education
- Danger signs in pregnancy
- Birth preparedness
- Institutional delivery
- Postnatal care and breastfeeding
- Family planning options after delivery
IV. 🚨 When to Refer to Higher Centre (Danger Signs)
- Bleeding per vagina
- Severe headache/visual disturbances
- Swelling of face and limbs
- Severe abdominal pain
- High fever
- No fetal movement >6 hours
- Convulsions, unconsciousness
- Blood pressure >140/90 mmHg
V. 🤱 Preparation for Labor and Delivery
- Encourage hospital delivery (Janani Suraksha Yojana / PMMVY schemes in India).
- Identify transportation.
- Arrange for blood donor if needed.
- Keep emergency contact numbers ready.
- Keep delivery kit ready after 36 weeks.
Summary Table 📋
| Assessment Area | Management/Action |
|---|---|
| History taking | Identify risks, plan care |
| Physical examination | Monitor health, detect abnormalities |
| Lab investigations | Identify anemia, infections, gestational diabetes |
| Nutritional advice | Balanced diet + supplements |
| Routine meds | IFA, Calcium, Albendazole, Td injection |
| Health education | Danger signs, birth preparedness, breastfeeding |
| Referral criteria | Danger signs or complications |
| Preparation for birth | Institutional delivery, emergency planning |
🌸 Pre-Pregnancy Care – Review of Sexual Development

Pre-pregnancy (preconception) care involves a comprehensive health assessment and guidance given to a woman or couple before conception to optimize maternal and fetal outcomes.
One key part of this is the Review of Sexual Development, which helps healthcare providers understand the biological, physical, hormonal, and psychological readiness of a woman for pregnancy.
🌼 I. Purpose of Reviewing Sexual Development in Pre-Pregnancy Care
- To assess normal pubertal and reproductive development.
- To identify any abnormalities in sexual or reproductive anatomy.
- To ensure hormonal balance for conception.
- To provide timely treatment for any sexual development disorders.
- To address psychosocial readiness for sexual activity and pregnancy.
🌺 II. Normal Sexual Development – A Brief Overview
Sexual development occurs in five major stages, mainly during adolescence and early adulthood:
1. Infancy and Childhood (0–8 years)
- Gender identity develops.
- No reproductive capability.
- Minimal sexual hormone activity.
2. Pre-Puberty (8–11 years)
- Subtle physical changes begin (breast budding in girls).
- Hormonal axis starts to mature.
3. Puberty (Average: Girls – 10–14 years)
Triggered by the Hypothalamic–Pituitary–Gonadal (HPG) Axis:
- Gonadotropin-Releasing Hormone (GnRH) from hypothalamus stimulates:
- FSH and LH from anterior pituitary.
- These act on ovaries to produce estrogen and develop ova.
In Girls:
- Thelarche – Breast development.
- Pubarche – Appearance of pubic hair.
- Menarche – First menstrual period (usually by 12–13 years).
- Growth spurt – Peak height velocity.
4. Reproductive Maturity (15–45 years)
- Ovulatory cycles become regular (about 2 years after menarche).
- Fertility potential is optimal.
- Menstrual cycles are usually 28±7 days with ovulation around day 14.
5. Perimenopause and Menopause
(Not directly relevant for pre-pregnancy, but important for long-term reproductive planning.)
🌹 III. Key Areas of Review in Pre-Pregnancy Sexual Development Assessment
| Area | Key Points to Assess |
|---|---|
| Menstrual history | Age at menarche, regularity, cycle length, flow amount. |
| Secondary sexual characteristics | Breast development, pubic/axillary hair – Tanner Staging. |
| Hormonal status | FSH, LH, estrogen, prolactin, thyroid hormones, if needed. |
| Anatomy of reproductive system | Uterus, ovaries, vagina – via pelvic exam or ultrasound. |
| Sexual activity history | Onset, frequency, use of contraception, sexual dysfunction. |
| Psychosocial maturity | Emotional readiness for sexual life and pregnancy. |
| Infections/STIs | History of UTIs, STDs, or genital tract infections. |
| Partner history | Sexual history, fertility, infections. |
🌿 IV. Abnormalities to Be Ruled Out
- Delayed puberty – No thelarche by age 13 or no menarche by 16.
- Primary amenorrhea – No menstruation by 16 years of age.
- Secondary amenorrhea – Cessation of periods for 3–6 months.
- Polycystic Ovarian Syndrome (PCOS) – Irregular menses, hirsutism, obesity.
- Thyroid dysfunction – Can delay menarche or cause irregular cycles.
- Congenital anomalies – E.g., Müllerian agenesis, imperforate hymen.
- Sexual dysfunction or abuse history – Requires psychological support.
💡 V. Nursing Responsibilities in Reviewing Sexual Development
- Maintain privacy and ensure non-judgmental attitude.
- Take detailed history with empathy and confidentiality.
- Educate the woman/couple about normal sexual development.
- Counsel on fertility, safe sex practices, and menstrual health.
- Refer to specialist if abnormalities are found.
- Involve the partner when appropriate for joint decision-making.
🌈 VI. Importance of Review for Fertility & Safe Pregnancy
- Ensures optimal physical and hormonal health for conception.
- Helps identify and treat conditions like PCOS, hypothyroidism, or anatomical barriers to conception.
- Promotes timely interventions to support reproductive health.
- Reduces the risk of complications during pregnancy like infertility, miscarriage, or preterm labor.
🌏 Socio-Cultural Aspects of Human Sexuality
Human sexuality is not just a biological or physical concept. It is also deeply influenced by social, cultural, religious, moral, and psychological factors. These aspects shape how individuals understand, express, and behave in relation to their sexuality.
🌸 I. Definition of Human Sexuality
Human sexuality refers to a person’s capacity for sexual feelings, orientation, identity, behavior, roles, and relationships. It includes biological sex, gender identity, sexual orientation, intimacy, reproduction, and eroticism.
🌍 II. Socio-Cultural Aspects of Human Sexuality
These aspects define how sexuality is perceived, accepted, and practiced in different societies.
🔹 1. Cultural Beliefs and Norms
- Each culture has specific values, rules, and expectations regarding sexuality.
- What is acceptable in one culture may be taboo in another.
- Example: Premarital sex may be accepted in Western cultures but discouraged in traditional societies.
🔹 2. Gender Roles and Expectations
- Societies assign gender-based behaviors (e.g., men expected to be dominant, women passive).
- These roles influence how men and women express sexuality.
- In some cultures, women are discouraged from speaking openly about sexual needs.
🔹 3. Religion and Morality
- Religions often guide sexual behavior with rules regarding:
- Marriage
- Contraception
- Masturbation
- Homosexuality
- Abortion
- Example: Islam and Christianity promote chastity before marriage.
🔹 4. Family and Social Influence
- Family upbringing impacts sexual understanding.
- Societies where open discussion is encouraged lead to better sexual health awareness.
- In conservative families, sexual matters may be considered shameful or private.
🔹 5. Media and Technology
- Exposure to TV, films, internet, and social media has changed sexual attitudes, especially in youth.
- Promotes both awareness and sometimes unrealistic expectations or risky behavior.
🔹 6. Education and Literacy
- Educated individuals are more likely to:
- Understand safe sex
- Use contraception
- Prevent STIs
- In areas with low literacy, myths and misconceptions about sexuality may persist.
🔹 7. Sexual Orientation and Identity
- Social and cultural settings affect the acceptance or rejection of LGBTQ+ individuals.
- Discrimination, stigma, or even violence may occur in societies with rigid gender norms.
🔹 8. Myths and Misconceptions
- Beliefs such as:
- “Masturbation causes weakness”
- “Only men have strong sexual desire”
- “First intercourse must involve pain/bleeding”
- These myths affect attitudes, self-esteem, and relationships.
🔹 9. Marriage and Sexuality
- Some cultures associate sexuality strictly with marriage and reproduction.
- Others see it as part of individual expression and pleasure.
📊 III. Examples of Socio-Cultural Impact on Sexual Health
| Factor | Impact |
|---|---|
| Taboos around discussing sex | Lack of knowledge, unsafe practices |
| Religious restrictions | Delayed or suppressed sexual expression |
| Gender inequality | Sexual violence, reproductive health issues |
| Media influence | Body image issues, early sexual exposure |
| Stigma on LGBTQ+ | Mental health problems, isolation |
🧠 IV. Nursing/Healthcare Implications
👩⚕️ Nurses should:
- Respect cultural and personal values.
- Offer non-judgmental, confidential sexual health counseling.
- Promote scientific education to counter myths.
- Advocate for sexual rights and gender equality.
- Encourage parent-child and teacher-student communication on sexuality.
🌸 Preconception Care (PCC)
Preconception care refers to a set of preventive, promotive, and curative health services provided before conception to improve maternal and fetal outcomes. It prepares a woman (and couple) for healthy pregnancy and childbirth by addressing health issues and promoting positive health practices.
🎯 Objectives of Preconception Care
- Optimize the health of the woman before conception.
- Identify and manage risk factors (medical, genetic, behavioral).
- Promote healthy lifestyle and nutrition.
- Educate the couple about fertility, pregnancy planning, and birth spacing.
- Reduce the risk of adverse maternal and neonatal outcomes.
🩺 Key Components of Preconception Care
1️⃣ Health and Medical Assessment
- Detailed personal, obstetric, menstrual, and family history.
- Past complications: miscarriages, stillbirths, cesarean, hypertension, diabetes.
- Current health status: Chronic diseases (e.g., thyroid, asthma, epilepsy, etc.).
2️⃣ Physical Examination
- General examination: Height, weight, BMI, blood pressure.
- Check for anemia, goiter, infections, or physical abnormalities.
- Pelvic exam (if needed): Assess reproductive organs.
3️⃣ Laboratory Investigations
- Hemoglobin level
- Blood group and Rh typing
- Blood sugar (to detect diabetes)
- Thyroid function test
- Urine test (for albumin, sugar, and infection)
- Screening for STIs, HIV, Hepatitis B & C, Rubella immunity, etc.
4️⃣ Nutritional Assessment & Intervention
- Check for undernutrition or obesity.
- Folic acid supplement (400 mcg/day at least 1 month before conception to prevent neural tube defects).
- Iron and calcium if anemic or malnourished.
- Advise balanced diet, plenty of fluids, fruits, vegetables, and proteins.
5️⃣ Immunization Status
- Ensure vaccines are updated:
- Rubella (if non-immune; avoid pregnancy for 1 month after vaccine).
- Hepatitis B, Tdap, COVID-19, etc., as per guidelines.
6️⃣ Genetic Counseling
- For couples with:
- Family history of genetic disorders
- Repeated pregnancy losses
- Known inherited diseases (e.g., Thalassemia, Sickle cell anemia)
- Screening and testing may be advised.
7️⃣ Lifestyle Modification
- Stop smoking, alcohol, and drug use.
- Encourage exercise and weight management.
- Manage stress and promote mental well-being.
8️⃣ Psychosocial Assessment
- Check for mental health issues (depression, anxiety).
- Evaluate family support, intimate partner violence, stressors.
- Promote healthy relationships and emotional readiness.
9️⃣ Sexual and Reproductive Health Counseling
- Educate about:
- Menstrual cycle and fertile period.
- Safe sex practices and STI prevention.
- Spacing between pregnancies.
- Fertility and ovulation tracking.
🔟 Environmental and Occupational Exposure
- Assess exposure to:
- Chemicals, radiation, pesticides.
- Harmful workplace substances.
- Guide for protective measures.
📌 Role of Nurse/Health Worker in Preconception Care
| Responsibility | Action |
|---|---|
| Education | Educate couples on health, pregnancy planning, and family life. |
| Screening | Conduct tests and identify risk factors. |
| Counseling | On nutrition, contraception, substance abuse, STDs. |
| Referral | Refer to higher center if needed (e.g., geneticist, obstetrician). |
| Follow-up | Regular check-ins to ensure readiness for pregnancy. |
🚫 Risk Factors Addressed in PCC
- Diabetes, hypertension, thyroid disease
- Anemia, obesity, underweight
- Poor nutrition, infections, uncontrolled chronic diseases
- Genetic diseases
- Psychological stress, domestic violence
- Environmental exposures
✅ Benefits of Preconception Care
- Reduces maternal and perinatal mortality and morbidity.
- Prevents neural tube defects and congenital anomalies.
- Helps achieve planned, wanted pregnancies.
- Promotes health-seeking behavior and early antenatal care.
- Enhances knowledge of reproductive health and rights.
🌸 Pre-conception Counseling.

🔹 Definition:
Pre-conception counseling is the process of providing information, education, and support to couples (especially women) before conception occurs, to ensure a healthy pregnancy and optimal outcomes for the mother and baby.
It is an essential aspect of reproductive and maternal health care, especially in the field of midwifery and gynecology nursing.
🔹 Objectives of Pre-conception Counseling in Midwifery:
- Assess and optimize the woman’s health before pregnancy.
- Identify and manage any risk factors that may affect conception, pregnancy, or childbirth.
- Promote awareness of normal birth, its process, benefits, and how to prepare for it.
- Encourage healthy lifestyle modifications.
- Educate about fertility and conception timing.
- Empower women to make informed choices about their reproductive health.
🔹 Components of Pre-conception Counseling (Midwifery Focus):
1️⃣ Comprehensive Health Assessment:
- Medical history (chronic diseases, infections, etc.)
- Menstrual history (cycle regularity, dysmenorrhea, etc.)
- Obstetric and gynecological history
- Family history (genetic or hereditary disorders)
- Lifestyle and nutrition
- Psychosocial evaluation
2️⃣ Nutritional Counseling:
- Balanced diet, rich in iron, calcium, folic acid.
- Start Folic acid (400 mcg/day) supplementation to prevent neural tube defects.
- Address anemia or malnutrition if present.
3️⃣ Fertility Awareness & Timing:
- Educate about ovulation period (usually days 12–16 of cycle).
- Teach fertility tracking methods (BBT, cervical mucus method).
- Inform about healthy sexual practices to enhance conception.
4️⃣ Immunization Status:
- Check for immunity to Rubella, Hepatitis B, Varicella, Tetanus, COVID-19, etc.
- Administer vaccines if needed before conception.
5️⃣ Infection Screening and Treatment:
- Screen for STIs, HIV, Hepatitis B & C, TORCH infections.
- Treat infections prior to conception.
6️⃣ Chronic Disease Management:
- Control of diabetes, hypertension, epilepsy, thyroid disorders, etc.
- Adjust medications to pregnancy-safe alternatives.
7️⃣ Lifestyle Modifications:
- Quit smoking, alcohol, and drugs.
- Encourage regular exercise and stress management.
- Avoid environmental toxins and hazards.
8️⃣ Genetic Counseling (if needed):
- For couples with family history of genetic conditions.
- In cases of consanguineous marriage, advanced maternal age, or previous child with genetic defect.
9️⃣ Psychological Preparation:
- Address mental health issues (anxiety, depression).
- Support through counseling or therapy if needed.
- Discuss emotional readiness for parenthood.
🔹 Counseling Regarding Normal Birth:
Awareness and Preparation for Normal Vaginal Delivery (NVD):
🌼 What to Cover:
- Benefits of normal birth: Less complications, quicker recovery, early bonding.
- Stages of labor and delivery: Latent, active, transition, pushing, delivery of placenta.
- Coping techniques: Breathing exercises, movement, massage, hydrotherapy.
- Support system: Role of birth partner/doula/midwife.
- Hospital vs home birth: Pros and cons, based on risk assessment.
🌼 Promotion of Normal Birth:
- Avoid unnecessary medical interventions (like elective C-sections).
- Educate on birth plans and women’s rights during childbirth.
- Encourage skin-to-skin contact and early breastfeeding.
- Use midwifery-led care model to reduce interventions.
🌼 Danger Signs to Watch:
- Preterm labor signs
- Bleeding
- High BP symptoms
- Abnormal fetal movements
- Prolonged or painful labor
🔹 Role of Midwifery and Gynecology Nurse in Pre-conception Counseling:
| Roles | Responsibilities |
|---|---|
| Educator | Teach women/couples about health, fertility, and normal birth. |
| Counselor | Provide emotional and mental health support. |
| Care Provider | Perform assessments, refer to specialists if needed. |
| Advocate | Promote women’s rights to informed, respectful maternity care. |
| Communicator | Coordinate between obstetrician, pediatrician, and woman. |
🔹 Importance in Reducing Maternal and Neonatal Morbidity/Mortality:
- Early interventions reduce complications during pregnancy and labor.
- Encourages planned and safe pregnancies.
- Improves maternal and neonatal outcomes.
🧬 Genetic Counseling.

🔷 Definition:
Genetic counseling is a communication process that deals with the occurrence or risk of a genetic disorder in a family. It includes risk assessment, education, support, and guidance to individuals or families who are at risk for or affected by genetic conditions.
WHO Definition: Genetic counseling is the process through which individuals or families receive advice and information about genetic disorders, their consequences, and the chances of recurrence.
🔷 Objectives of Genetic Counseling:
- To assess the risk of recurrence of genetic disorders.
- To provide accurate and updated information on genetic conditions.
- To offer emotional support and coping strategies.
- To guide on available tests and management options.
- To support informed decision-making about reproduction.
🔷 Types of Genetic Counseling:
| Type | Purpose |
|---|---|
| Prospective Counseling | For couples planning to marry or conceive. |
| Retrospective Counseling | Given after birth of an affected child. |
| Carrier Counseling | For individuals who carry a gene for a disorder. |
| Prenatal Counseling | For a woman already pregnant, with high-risk results. |
| Postnatal Counseling | After delivery if a baby is born with a genetic condition. |
| Cancer Genetic Counseling | For those with family history of cancers. |
🔷 Indications for Genetic Counseling (When it is needed):
- Family history of inherited disorders (e.g., thalassemia, sickle cell).
- Consanguineous marriage (marriage between close relatives).
- Advanced maternal age (>35 years).
- Previous child with congenital anomalies.
- History of multiple miscarriages or stillbirths.
- Carrier screening (e.g., cystic fibrosis, Tay-Sachs).
- Abnormal prenatal test results (ultrasound, amniocentesis).
- Newborn screening abnormalities.
- Suspected X-linked or autosomal disorders.
- Infertility or subfertility due to genetic causes.
🔷 Steps in Genetic Counseling Process:
- Referral – from obstetrician, pediatrician, or nurse.
- Collection of information:
- Family history (pedigree chart)
- Medical and reproductive history
- Risk assessment:
- Determine inheritance pattern (dominant, recessive, X-linked)
- Education:
- Explain the condition, cause, prognosis, and management
- Explain screening and diagnostic options
- Support and Decision-making:
- Help in understanding reproductive options
- Provide emotional support
- Follow-up and referrals:
- Refer to specialists (geneticist, psychologist)
- Plan next steps (testing, pregnancy planning, etc.)
🔷 Common Genetic Disorders Encountered in Counseling:
| Disorder | Inheritance Type |
|---|---|
| Thalassemia | Autosomal Recessive |
| Sickle Cell Anemia | Autosomal Recessive |
| Down Syndrome (Trisomy 21) | Chromosomal Nondisjunction |
| Hemophilia | X-linked Recessive |
| Turner Syndrome (XO) | Chromosomal Disorder |
| Cystic Fibrosis | Autosomal Recessive |
| Duchenne Muscular Dystrophy | X-linked Recessive |
| Tay-Sachs Disease | Autosomal Recessive |
🔷 Role of Nurse in Genetic Counseling (Midwifery and Gynecology Context):
| Role | Description |
|---|---|
| Educator | Teach couples about inheritance, risk factors, testing. |
| Counselor | Provide emotional support and non-directive guidance. |
| Advocate | Respect clients’ rights and decisions, promote informed choice. |
| Communicator | Bridge communication between client and geneticist. |
| Care Coordinator | Schedule and arrange necessary referrals and follow-ups. |
| Prenatal support | Assist in prenatal screening (NT scan, triple marker, amniocentesis). |
| Health Promoter | Educate community on consanguinity, carrier screening, and healthy conception. |
🔷 Ethical Considerations in Genetic Counseling:
- Confidentiality
- Informed consent
- Non-directiveness (the counselor should not impose personal views)
- Respect for autonomy
- Right to know and right not to know
- Cultural and religious sensitivity
🔷 Genetic Testing Options Explained in Counseling:
| Test | Description |
|---|---|
| Carrier Testing | Checks if a person carries a gene for a condition. |
| Prenatal Testing | Detects genetic conditions during pregnancy (e.g., amniocentesis). |
| Newborn Screening | After birth to detect treatable conditions early. |
| Preimplantation Genetic Diagnosis (PGD) | Testing embryos before IVF implantation. |
| Predictive Testing | For adult-onset conditions (e.g., Huntington’s). |
🔷 Impact of Genetic Counseling:
- Reduces birth of babies with severe genetic defects.
- Helps in early diagnosis and management.
- Reduces emotional and financial burden on families.
- Empowers couples with reproductive choices (e.g., IVF with PGD, adoption, etc.)
🌸 Planned Parenthood.
🔷 Definition:
Planned Parenthood is the practice of deciding when and how many children to have, through the use of education, counseling, and family planning services, including contraception. It aims to promote reproductive health, maternal well-being, child health, and empowered family life.
It enables couples to achieve their desired number of children and determine the spacing and timing of their births.
🔷 Objectives of Planned Parenthood:
- To prevent unplanned or unwanted pregnancies.
- To improve maternal and child health outcomes.
- To help in spacing pregnancies, allowing the woman’s body to recover.
- To empower couples with choices regarding reproduction.
- To reduce the incidence of unsafe abortions.
- To support women’s physical, emotional, and financial health.
🔷 Scope of Planned Parenthood Services:
| Area | Services Provided |
|---|---|
| Family Planning | Contraceptive education and provision |
| Maternal Health | Antenatal, intranatal, and postnatal care |
| Infertility Services | Counseling, basic investigations, referral |
| STD/HIV Prevention | Screening, prevention, education |
| Cancer Screening | Cervical and breast cancer screening |
| Youth Counseling | Adolescent sex education and menstrual health |
| Safe Abortion Services | MTP as per law and guidelines |
🔷 Role of Nurse in Planned Parenthood (Midwifery & Gynae):
| Nursing Role | Responsibilities |
|---|---|
| Health Educator | Teach about reproductive health, contraception, menstrual hygiene |
| Counselor | Offer pre- and post-family planning counseling |
| Service Provider | Distribute contraceptives, assist in IUCD insertion, monitor side effects |
| Care Provider | Offer antenatal/postnatal care and referrals for infertility |
| Advocate | Promote women’s rights in reproductive decisions |
| Record Keeper | Maintain records of contraceptive use, follow-ups, outcomes |
🔷 Family Planning Methods Under Planned Parenthood:
🔹 Temporary Methods:
| Method | Description |
|---|---|
| Barrier | Condoms, diaphragms |
| Hormonal Pills | Mala-N, Mala-D |
| Injectables | Antara (DMPA) |
| IUCDs | Copper-T 380A, Multiload |
| Emergency Contraceptive | Taken within 72 hours of unprotected sex |
| Natural Methods | Rhythm method, lactational amenorrhea method (LAM) |
🔹 Permanent Methods:
| Method | Description |
|---|---|
| Female Sterilization | Tubectomy |
| Male Sterilization | Vasectomy |
🔷 Importance of Planned Parenthood in Public Health:
- Reduces maternal and infant mortality.
- Promotes safe motherhood and child survival.
- Controls population growth.
- Supports economic and social development.
- Prevents unsafe abortions and complications.
- Empowers women through control over fertility.
🔷 Challenges in Planned Parenthood Implementation:
- Myths and misconceptions
- Cultural and religious barriers
- Lack of male participation
- Limited access in rural areas
- Poor health infrastructure
- Fear of side effects
🔷 Nursing Strategies to Promote Planned Parenthood:
- Health education in community & clinics
- Postpartum family planning counseling
- Involving male partners in counseling
- Organizing Adolescent Reproductive Health (ARSH) sessions
- Door-to-door outreach by ANMs/ASHA workers
- Collaborating with government schemes like:
- Mission Parivar Vikas
- National Family Welfare Programme
🔷 Planned Parenthood and Midwifery Practice:
Midwives and gynecology nurses are frontline workers in:
- Educating women during antenatal visits about spacing.
- Providing postnatal contraception counseling.
- Supporting safe abortion and reproductive rights.
- Integrating family planning into MCH (Mother and Child Health) services.
Pregnancy assessment and antenatal care (I, II & III Trimesters)
🌸 Assessment of Pregnancy.
🔷 Definition:
Assessment of pregnancy is the systematic evaluation of a woman to confirm the presence of pregnancy, determine its viability, establish gestational age, and identify any potential risks or complications.
It is the first and essential step in antenatal care, where the midwife or nurse plays a key role in early detection and support.
🔷 Objectives of Pregnancy Assessment:
- To confirm pregnancy accurately.
- To establish gestational age.
- To detect any early complications or high-risk conditions.
- To initiate early antenatal care (ANC).
- To provide appropriate health education and counseling.
🔷 Components of Pregnancy Assessment:
🔶 1️⃣ History Taking:
a. Personal & Demographic Information:
- Name, age, address, marital status, education, occupation
b. Menstrual History:
- Last Menstrual Period (LMP)
- Cycle regularity
- Estimated Due Date (EDD) using Naegele’s Rule:
➤ EDD = LMP + 9 months + 7 days
c. Obstetric History (GTPAL):
- G = Gravida (number of pregnancies)
- T = Term births
- P = Preterm births
- A = Abortions (spontaneous or induced)
- L = Living children
d. Medical & Surgical History:
- Diabetes, hypertension, epilepsy, thyroid, surgeries
e. Family History:
- Hereditary diseases (e.g., thalassemia, hemophilia)
f. Psychosocial History:
- Stress, domestic violence, support system, mental health
🔶 2️⃣ Physical Examination:
a. General Examination:
| Parameter | Significance |
|---|---|
| Weight | Baseline, nutrition status |
| Height | Short stature may relate to CPD |
| Blood pressure | Early detection of PIH/pre-eclampsia |
| Pulse | Circulatory status |
| Pallor | Anemia |
| Edema | Nutritional status, PIH |
| Jaundice | Liver disorders |
b. Breast Examination:
- Look for enlargement, tenderness, darkened areola, Montgomery tubercles
c. Abdominal Examination (from 12 weeks onward):
- Fundal height (to assess gestational age)
- Abdominal girth
- Fetal parts (palpation in 2nd & 3rd trimester)
- Fetal heart sounds (FHS) – heard by Doppler after 10–12 weeks
d. Pelvic Examination (if needed):
- Softening of cervix (Goodell’s sign)
- Softening of lower uterine segment (Hegar’s sign)
- Bluish discoloration of vagina (Chadwick’s sign)
- Size and position of uterus
🔶 3️⃣ Laboratory Investigations:
| Test | Purpose |
|---|---|
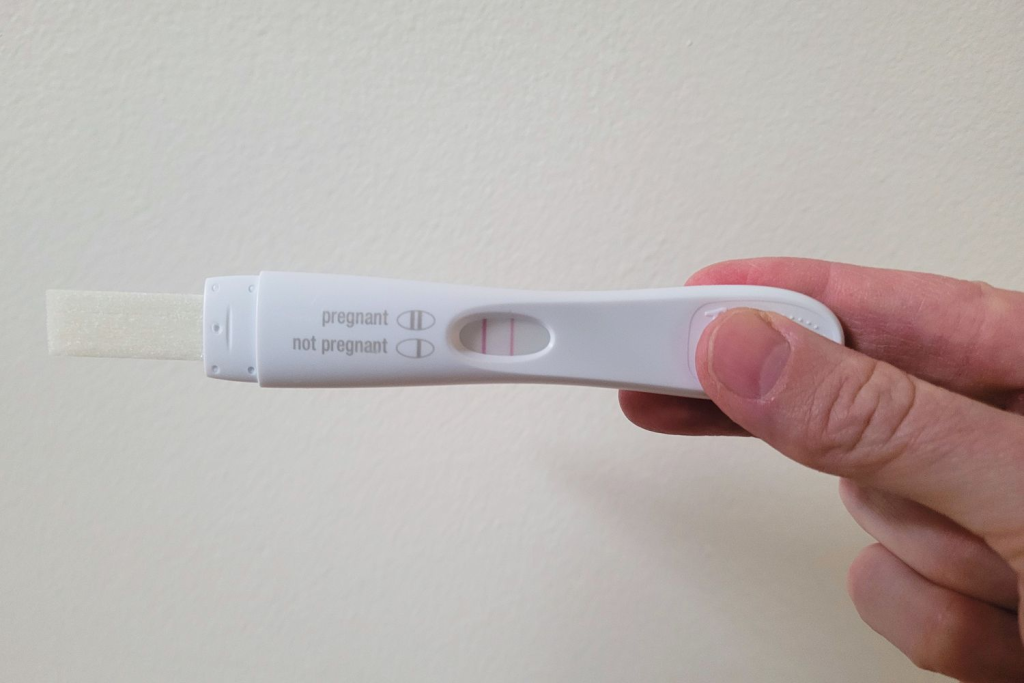
| Urine Pregnancy Test (UPT) | Detects hCG to confirm pregnancy |
| Blood group and Rh typing | To prevent Rh incompatibility |
| Hemoglobin (Hb%) | Detects anemia |
| VDRL | Syphilis screening |
| HIV, HBsAg | Infectious disease screening |
| Random Blood Sugar (RBS) | Diabetes screening |
| Urine Routine | Protein, sugar, infection |
| Thyroid profile | TSH abnormalities |
🔶 4️⃣ Ultrasound (USG):
| Timing | Purpose |
|---|---|
| 6–9 weeks (early scan) | Confirm intrauterine pregnancy, viability, gestational age |
| 11–13 weeks (NT scan) | Detect chromosomal abnormalities |
| 18–22 weeks (Anomaly scan) | Detect fetal anomalies |
| Third trimester | Assess growth, amniotic fluid, placenta |
🔷 Signs of Pregnancy Noted in Assessment:
🔹 Presumptive Signs (experienced by woman)
- Missed period (amenorrhea)
- Morning sickness
- Breast changes
- Frequent urination
- Quickening
🔹 Probable Signs (noted by examiner)
- Enlarged abdomen
- Positive urine pregnancy test
- Changes in cervix and uterus (Goodell’s, Hegar’s, Chadwick’s signs)
🔹 Positive Signs (confirmative)
- Fetal heart sounds
- Visualization of fetus on ultrasound
- Palpation of fetal parts
🔷 Tools Used in Pregnancy Assessment:
- Stethoscope / Doppler for FHS
- Measuring tape for fundal height
- Weighing scale
- Sphygmomanometer
- Speculum and sterile gloves (for pelvic exam)
- Urine pregnancy kit
- Ultrasound machine
🔷 Role of Midwife/Nurse in Pregnancy Assessment:
| Role | Duties |
|---|---|
| Care Provider | Conduct examinations, administer tests |
| Educator | Counsel on diet, rest, danger signs |
| Counselor | Support emotionally and psychologically |
| Health Promoter | Promote early ANC registration |
| Referrer | Refer high-risk pregnancies to specialists |
| Record Keeper | Maintain MCP card, ANC register, lab reports |
🔷 Importance of Early and Accurate Assessment:
- Ensures early detection of complications
- Helps in timely interventions
- Improves maternal and fetal outcomes
- Builds trust and rapport with the health system
- Promotes safe motherhood
🌸 Normal Pregnancy – Assess and Confirm Pregnancy.
🔷 Definition of Normal Pregnancy:
A normal pregnancy is a physiological condition where a fertilized ovum (zygote) implants in the uterine endometrium, grows and develops into a fetus over approximately 40 weeks (280 days), resulting in the birth of a healthy baby without complications.
🔷 Duration of Pregnancy:
- Measured from the first day of the Last Menstrual Period (LMP).
- Divided into three trimesters:
- First Trimester: 0–12 weeks
- Second Trimester: 13–28 weeks
- Third Trimester: 29–40 weeks
🔷 Assessing and Confirming Pregnancy:
Confirming pregnancy is the first step in antenatal care. It involves a combination of subjective symptoms, objective signs, and diagnostic tests.
🔶 1. Presumptive Signs of Pregnancy (Subjective – reported by the woman)
| Symptom | Explanation |
|---|---|
| Amenorrhea | Absence of menstruation is usually the first sign. |
| Nausea and Vomiting (Morning Sickness) | Due to increased hCG levels. |
| Breast changes | Tenderness, enlargement, darkened areola. |
| Urinary frequency | Due to hormonal changes and uterine pressure on bladder. |
| Fatigue | Early pregnancy leads to tiredness. |
| Quickening (by 16–20 weeks) | First fetal movements felt by mother. |
🔹 Note: These signs are not conclusive. They may be due to other conditions (e.g., stress, illness).
🔶 2. Probable Signs of Pregnancy (Objective – observed by examiner)
| Sign | Explanation |
|---|---|
| Chadwick’s sign | Bluish discoloration of vaginal mucosa. |
| Goodell’s sign | Softening of cervix. |
| Hegar’s sign | Softening of lower uterine segment. |
| Abdominal enlargement | Progressive uterine growth. |
| Positive pregnancy test (urine or serum hCG) | Detects hCG in body fluids. |
| Braxton Hicks contractions | Irregular, painless uterine contractions. |
| Uterine souffle | Soft blowing sound over uterus (maternal blood flow). |
🔹 These signs are stronger indicators but not 100% diagnostic.
🔶 3. Positive (Definitive) Signs of Pregnancy
These signs confirm the presence of a fetus and can be detected only by a skilled examiner or specific instruments.
| Sign | Detected By |
|---|---|
| Fetal heartbeat (110–160 bpm) | Doppler (by 10–12 weeks), Fetoscope (by 18–20 weeks) |
| Fetal movements felt by examiner | By 20 weeks |
| Ultrasound visualization of gestational sac, fetus, and heartbeat | Transvaginal USG (5–6 weeks), Transabdominal (6–8 weeks) |
| Palpation of fetal parts | During abdominal examination in 2nd or 3rd trimester |
🔷 Pregnancy Confirmation Methods in Clinical Practice:
✅ a. Urine Pregnancy Test (UPT):
- Home test kits or done in clinics.
- Detects hCG hormone.
- Best done with first morning urine (more concentrated).
- Can be positive as early as 6–10 days after conception.
✅ b. Serum β-hCG Test:
- More sensitive than urine test.
- Can confirm pregnancy earlier (as soon as 7–9 days after ovulation).
- Used to assess ectopic pregnancy or molar pregnancy.
✅ c. Ultrasound (USG):
- Transvaginal USG:
- Detects gestational sac as early as 4.5–5 weeks.
- Fetal heartbeat seen by 6–7 weeks.
- Transabdominal USG:
- Useful from 6–8 weeks onward.
🔷 Steps of Pregnancy Assessment by Nurse/Midwife:
- History Taking:
- Menstrual history (LMP)
- Symptoms of early pregnancy
- Sexual and obstetric history
- Physical Examination:
- General exam (weight, BP, edema)
- Abdominal palpation
- Pelvic examination (if needed)
- Laboratory Tests:
- UPT
- Blood hCG test (if needed)
- Baseline investigations (CBC, blood group, VDRL, HIV, HBsAg)
- Ultrasound Scan:
- First scan (6–9 weeks) to confirm viability, location (intrauterine), and gestational age.
- Documentation:
- Enter pregnancy details in Mother and Child Protection (MCP) Card
- Register in ANC register and schedule antenatal visits.
🔷 Nurse’s Role in Pregnancy Confirmation:
| Role | Description |
|---|---|
| Educator | Teach about signs of pregnancy and when to seek care. |
| Counselor | Support emotional aspects of pregnancy discovery. |
| Care provider | Perform UPT, assess vitals, arrange for USG and labs. |
| Advocate | Promote early ANC registration and safe motherhood. |
🔷 Importance of Early Pregnancy Confirmation:
- Initiate early antenatal care (ANC).
- Identify high-risk pregnancies.
- Prevent complications (e.g., anemia, PIH, GDM).
- Provide nutritional support (Iron, Folic acid).
- Educate on birth preparedness and danger signs.
🌸 Diagnosis of Pregnancy
🔷 Definition:
Diagnosis of pregnancy is the process of determining whether a woman is pregnant through the identification of specific signs, symptoms, physical changes, laboratory tests, and imaging studies.
It helps to confirm pregnancy, determine gestational age, and initiate antenatal care at the earliest.
🔷 Importance of Diagnosing Pregnancy Early:
- To confirm viable intrauterine pregnancy
- To establish the Estimated Date of Delivery (EDD)
- To begin early antenatal care (ANC)
- To identify high-risk pregnancies
- To educate the woman about pregnancy, nutrition, and danger signs
🔷 Categories of Signs Used for Diagnosis of Pregnancy:
The diagnosis of pregnancy is based on three categories of signs:
| Category | Type of Sign |
|---|---|
| 1️⃣ Presumptive Signs | Subjective symptoms reported by the woman |
| 2️⃣ Probable Signs | Objective signs observed by the clinician |
| 3️⃣ Positive Signs | Conclusive evidence of pregnancy |
🔶 1️⃣ Presumptive Signs of Pregnancy
(These are not diagnostic because they may occur due to other conditions)
| Sign/Symptom | Description |
|---|---|
| Amenorrhea | Absence of menstruation |
| Nausea/Vomiting | Common in early pregnancy (Morning sickness) |
| Breast changes | Tenderness, enlargement, darkened areola |
| Urinary frequency | Due to hormonal changes and pressure on bladder |
| Fatigue | General tiredness |
| Quickening | First fetal movement felt by the mother (16–20 weeks) |
| Food cravings or aversions | Altered taste preferences |
🔸 These signs are suggestive but not confirmative.
🔶 2️⃣ Probable Signs of Pregnancy
(These are stronger indicators but not 100% reliable)
| Sign | Description |
|---|---|
| Chadwick’s sign | Bluish discoloration of vaginal mucosa |
| Goodell’s sign | Softening of the cervix |
| Hegar’s sign | Softening of lower uterine segment |
| Enlarged abdomen | Due to growing uterus |
| Braxton Hicks contractions | Irregular painless uterine contractions |
| Positive urine pregnancy test (hCG detection) | Commonly used screening test |
| Ballottement | Rebounding of fetus when tapped per vagina |
🔸 These signs may still occur in non-pregnant conditions (e.g., tumors, hormonal disorders).
🔶 3️⃣ Positive (Confirmative) Signs of Pregnancy
(These signs confirm pregnancy without doubt)
| Sign | Method |
|---|---|
| Fetal heart sounds (110–160 bpm) | Heard via Doppler (10–12 weeks) or fetoscope (18–20 weeks) |
| Fetal movements felt by examiner | Palpated after 20 weeks |
| Ultrasound detection of gestational sac, fetal pole, or heartbeat | Transvaginal USG (5–6 weeks), Transabdominal (6–8 weeks) |
| X-ray (not preferred in pregnancy) | Used only in rare late cases where ultrasound not available |
🔹 These signs are conclusive evidence of pregnancy.
🔷 Laboratory and Diagnostic Methods to Confirm Pregnancy:
✅ 1. Urine Pregnancy Test (UPT):
- Detects hCG (Human Chorionic Gonadotropin) hormone.
- Best done using first morning urine.
- Positive as early as 6–10 days after conception.
✅ 2. Serum β-hCG Test (Blood Test):
- More sensitive and quantitative.
- Used in early pregnancy or in suspected ectopic pregnancy or molar pregnancy.
- hCG levels double every 48–72 hours in normal early pregnancy.
✅ 3. Ultrasonography (USG):
- Transvaginal USG: Detects gestational sac at 4.5–5 weeks, fetal heartbeat at 6–7 weeks.
- Transabdominal USG: Visible sac and fetus from 6–8 weeks.
- Most accurate method for early and definitive diagnosis.
🔷 Role of Nurse/Midwife in Diagnosis of Pregnancy:
| Role | Responsibilities |
|---|---|
| Care provider | Perform UPT, assist with pelvic exam |
| Health educator | Educate on early signs, testing methods, and healthy habits |
| Counselor | Provide emotional support after confirmation |
| Communicator | Explain test results and coordinate follow-up |
| ANC Registrar | Register the mother for antenatal care services |
| Referrer | Refer high-risk or complicated cases to physician/specialist |
🔷 Key Points to Remember:
- Diagnosis ≠ Just testing – It includes full clinical judgment, history, and observation.
- Urine test is usually the first step, but ultrasound gives final confirmation.
- Misdiagnosis may occur in cases of pseudocyesis (false pregnancy), tumors, or hormonal imbalances.
- Early diagnosis is crucial for safe motherhood, early interventions, and antenatal care.
🌸 Signs of Pregnancy.

🔷 Definition:
Signs of pregnancy are the observable changes in a woman’s body that suggest or confirm that she is pregnant. These are grouped based on their diagnostic reliability into presumptive, probable, and positive signs.
🔷 Classification of Signs of Pregnancy:
| Category | Description | Diagnostic Value |
|---|---|---|
| 1️⃣ Presumptive Signs | Felt by the woman herself | Least reliable |
| 2️⃣ Probable Signs | Observed by a healthcare provider | More reliable |
| 3️⃣ Positive Signs | Definitive signs confirming pregnancy | Absolutely reliable |
🔶 1️⃣ Presumptive Signs of Pregnancy
(Subjective signs – experienced by the woman; not confirmative)
| Sign | Description |
|---|---|
| Amenorrhea | Absence of menstruation (first and most common sign) |
| Morning sickness | Nausea and vomiting, usually during first trimester |
| Breast changes | Tenderness, enlargement, darkening of areola |
| Urinary frequency | Increased urination due to hormonal and uterine changes |
| Fatigue | Tiredness and low energy levels |
| Quickening | First perception of fetal movement (felt around 16–20 weeks) |
| Food cravings/aversions | Unusual desires or dislikes toward certain foods |
| Mood swings | Emotional instability due to hormonal changes |
🔸 These signs can be caused by other conditions (stress, illness, hormonal imbalance), so they are not confirmative.
🔶 2️⃣ Probable Signs of Pregnancy
(Objective signs – observed by nurse/midwife; more suggestive but still not confirmative)
| Sign | Description |
|---|---|
| Chadwick’s sign | Bluish coloration of the vaginal mucosa due to increased vascularity |
| Goodell’s sign | Softening of the cervix |
| Hegar’s sign | Softening of the lower uterine segment |
| Abdominal enlargement | Progressive increase in abdominal size due to growing uterus |
| Ballottement | Fetus rebounds when cervix is tapped during a vaginal exam |
| Braxton Hicks contractions | Irregular, painless uterine contractions felt after 16 weeks |
| Positive pregnancy test (UPT/serum hCG) | Detects presence of hCG hormone in urine or blood |
🔸 These signs may still be present in conditions like uterine tumors, hormonal changes, or pseudocyesis (false pregnancy).
🔶 3️⃣ Positive (Confirmative) Signs of Pregnancy
(Absolutely confirm the presence of a fetus)
| Sign | Detected by |
|---|---|
| Fetal heart sounds (FHS) | Heard using Doppler by 10–12 weeks or fetoscope by 18–20 weeks |
| Fetal movements felt by examiner | Palpated after 20 weeks |
| Ultrasound visualization of fetus | Gestational sac visible by 5–6 weeks; heartbeat by 6–7 weeks |
✅ These signs are conclusive and can only occur in pregnancy.
🔷 Summary Table: Signs of Pregnancy
| Category | Examples |
|---|---|
| Presumptive | Amenorrhea, nausea, breast tenderness, fatigue, quickening |
| Probable | Uterine enlargement, positive hCG test, cervical softening |
| Positive | Fetal heartbeat, fetal movements (felt by examiner), ultrasound findings |
🔷 Role of Nurse/Midwife in Identifying Signs of Pregnancy:
- Take complete history and assess signs and symptoms.
- Perform physical examination and interpret findings.
- Conduct and interpret UPT and lab investigations.
- Refer for ultrasound for confirmation.
- Provide health education and counseling based on gestational age.
🌸 Differential Diagnosis and Confirmatory Tests of Pregnancy.
🔷 Definition:
- Differential diagnosis refers to the process of distinguishing pregnancy from other medical conditions that may mimic the signs and symptoms of pregnancy (especially in early stages).
- Confirmatory tests are diagnostic tools used to definitively confirm pregnancy, especially when presumptive or probable signs are misleading or inconclusive.
🔶 Why is Differential Diagnosis Important?
- Because presumptive and probable signs of pregnancy (e.g., missed periods, nausea, breast tenderness, abdominal enlargement) may also occur in other conditions.
- It helps avoid misdiagnosis and ensures appropriate care.
🔷 Conditions Mimicking Pregnancy (Differential Diagnosis)
| Condition | Reason it Mimics Pregnancy |
|---|---|
| Pseudocyesis (False pregnancy) | Emotional or psychological cause leads to signs of pregnancy without actual conception. |
| Uterine fibroids (leiomyoma) | Can cause abdominal enlargement, amenorrhea, and uterine mass. |
| Ovarian cysts/tumors | May mimic a growing abdomen and pelvic mass. |
| Ectopic pregnancy | Early pregnancy symptoms present, but implantation occurs outside the uterus (e.g., in fallopian tube). |
| Hormonal imbalance | Causes amenorrhea, breast tenderness. |
| Menopause | Irregular periods, hot flashes, mood swings can be mistaken for pregnancy signs. |
| Obesity | May lead to misinterpretation of abdominal enlargement. |
| Molar pregnancy (Hydatidiform mole) | Rapid uterine growth, positive hCG but no viable fetus. |
| Ascites or abdominal tumors | Cause visible and palpable abdominal enlargement. |
| Stress or psychological disorders | May alter menstruation and mimic other pregnancy signs. |
🔷 Confirmatory Tests for Pregnancy
These are used to confirm or rule out pregnancy with certainty.
✅ 1. Pregnancy Test – Detection of hCG
| Test Type | Description |
|---|---|
| Urine Pregnancy Test (UPT) | Detects hCG hormone in urine. Simple, quick, and used in clinics or at home. Becomes positive around 6–10 days after conception. |
| Serum β-hCG Test | More sensitive and quantitative than UPT. Detects very early pregnancy. Useful in suspected ectopic or molar pregnancy. Normal pregnancy shows doubling of hCG every 48–72 hrs in early weeks. |
✅ 2. Ultrasonography (USG)
| Type | Use |
|---|---|
| Transvaginal USG | Confirms pregnancy as early as 4.5–5 weeks (gestational sac), fetal heartbeat by 6–7 weeks. |
| Transabdominal USG | Visible gestational sac from 6–8 weeks. Used for dating pregnancy, fetal well-being, and ruling out ectopic/molar pregnancy. |
🔹 Ultrasound is the gold standard for confirmatory diagnosis.
✅ 3. Clinical Examination Findings (Positive Signs)
| Sign | Description |
|---|---|
| Fetal Heart Sounds (FHS) | Heard via Doppler (10–12 weeks), fetoscope (18–20 weeks) |
| Fetal movements felt by examiner | Palpable from around 20 weeks |
| Palpation of fetal parts | Done in 2nd and 3rd trimester during abdominal examination |
✅ 4. Additional Investigations (in special cases)
| Investigation | Purpose |
|---|---|
| TVS (Transvaginal Sonography) | To rule out ectopic pregnancy or confirm early intrauterine pregnancy |
| Complete Blood Count (CBC) | To assess anemia, infections |
| Thyroid Profile | To rule out hypothyroidism-related amenorrhea |
| Pelvic MRI/CT scan | In case of pelvic masses, suspected tumors (not routine) |
| Histopathological examination | For molar pregnancy diagnosis (grape-like vesicles on USG and high hCG levels) |
🔷 Comparison Chart: Differential Diagnosis vs Confirmatory Tests
| Aspect | Differential Diagnosis | Confirmatory Tests |
|---|---|---|
| Purpose | Rule out other conditions mimicking pregnancy | Prove the presence of an intrauterine fetus |
| Based on | Clinical signs, history, and other diseases | Hormone levels, imaging, fetal activity |
| Examples | Pseudocyesis, fibroid uterus, PCOD, molar pregnancy | UPT, serum hCG, ultrasound, fetal heart sounds |
| Outcome | Avoid misdiagnosis, treat other causes | Confirms viable pregnancy |
🔷 Nurse/Midwife’s Role:
| Role | Responsibility |
|---|---|
| Assessment | Identify presumptive, probable, and positive signs |
| Testing | Perform or assist in urine pregnancy test |
| Referral | Refer for ultrasound or specialist opinion if suspicious findings |
| Education | Inform client about interpretation of test results |
| Support | Emotional counseling in false pregnancy, abnormal pregnancy, or unexpected outcomes |
| Documentation | Record all findings accurately in ANC records |
🌸 Review of Maternal Nutrition & Malnutrition.

🔷 Definition of Maternal Nutrition:
Maternal nutrition refers to the nutritional status of a woman before conception, during pregnancy, and after childbirth. It includes the intake of essential macronutrients (carbohydrates, proteins, fats) and micronutrients (vitamins and minerals) required to support the health of both the mother and the developing fetus.
🔷 Importance of Maternal Nutrition:
| For Mother | For Fetus/Infant |
|---|---|
| Prevents anemia, infections, fatigue | Supports brain development |
| Reduces risk of pre-eclampsia and GDM | Prevents intrauterine growth retardation (IUGR) |
| Promotes healthy weight gain | Reduces risk of preterm birth, LBW |
| Aids postpartum recovery | Ensures adequate birth weight and organ formation |
🔷 Daily Nutritional Requirements During Pregnancy:
| Nutrient | Recommended Intake & Role |
|---|---|
| Energy | +300 kcal/day (extra in 2nd & 3rd trimester) |
| Protein | +23g/day; for tissue building, fetal growth |
| Iron | 35–60 mg/day; prevent anemia, support blood volume |
| Folic Acid | 400–600 mcg/day; prevent neural tube defects |
| Calcium | 1000–1200 mg/day; fetal bones and teeth |
| Iodine | 150 mcg/day; prevent cretinism, brain development |
| Vitamin A | Essential for vision and immunity (but excess is teratogenic) |
| Water | 2.5–3 liters/day; to support increased blood volume and prevent dehydration |
💊 Iron + Folic Acid (IFA) tablets are given as per national guidelines during pregnancy.
🔷 Balanced Diet for Pregnant Women:
Should include:
- Cereals (rice, wheat, millets)
- Pulses and legumes
- Green leafy vegetables (iron, folate, calcium)
- Fruits (vitamins, fiber)
- Milk and dairy products (calcium, protein)
- Meat, fish, eggs (if non-vegetarian)
- Oils and fats (in moderation)
- Water (adequate hydration)
🔷 Malnutrition in Pregnancy:
🔶 Definition:
Maternal malnutrition refers to deficiency or imbalance of essential nutrients in pregnant women. It includes undernutrition, micronutrient deficiencies, or overnutrition (obesity).
🔶 Types of Maternal Malnutrition:
| Type | Features |
|---|---|
| Undernutrition | Low BMI (<18.5), low weight gain, fatigue |
| Micronutrient deficiencies | Iron, folic acid, iodine, vitamin A/D deficiency |
| Overnutrition/Obesity | Excessive weight gain, risk of GDM, hypertension |
🔷 Effects of Malnutrition During Pregnancy:
➤ On the Mother:
- Anemia
- Weakness, fatigue
- Increased susceptibility to infections
- Pre-eclampsia, eclampsia
- Postpartum hemorrhage
- Delayed wound healing
- Maternal mortality
➤ On the Fetus/Baby:
- Intrauterine growth retardation (IUGR)
- Low birth weight (LBW)
- Preterm birth
- Congenital anomalies (due to folate deficiency)
- Stillbirth or neonatal death
- Developmental delays
- Poor immune function
🔷 Common Nutritional Deficiencies in Pregnant Women:
| Nutrient Deficiency | Clinical Effects |
|---|---|
| Iron | Anemia, fatigue, poor oxygen supply |
| Folic acid | Neural tube defects, anemia |
| Calcium | Leg cramps, osteoporosis, preeclampsia |
| Iodine | Goiter, cretinism in newborn |
| Vitamin A | Night blindness, weak immunity |
| Vitamin D | Bone weakness, poor fetal bone growth |
| Protein | Edema, poor fetal tissue growth |
🔷 Assessment of Maternal Nutrition:
| Method | Parameters |
|---|---|
| Anthropometric | Weight, height, BMI, MUAC |
| Clinical examination | Pallor, edema, mouth/skin/nail changes |
| Dietary history | 24-hour recall, food frequency |
| Lab investigations | Hb%, serum proteins, calcium, iron, etc. |
🔷 Nutritional Interventions for Pregnant Women:
- Iron-folic acid supplementation (IFA)
- Deworming in 2nd trimester
- Calcium tablets in 2nd & 3rd trimester
- Nutrition education and counseling
- Extra meal support (in ICDS/Anganwadi centers)
- Monitoring weight gain during ANC visits
- High-protein, high-calorie diet for undernourished women
- Salt iodization for iodine intake
🔷 Government Programs Supporting Maternal Nutrition in India:
| Program | Features |
|---|---|
| POSHAN Abhiyaan | National nutrition mission for pregnant and lactating mothers |
| ICDS (Integrated Child Development Scheme) | Provides supplementary nutrition, health check-up, education |
| Janani Suraksha Yojana (JSY) | Encourages institutional deliveries and maternal care |
| IFA Supplementation Guidelines | Under National Iron+ Initiative (NIPI) |
🔷 Role of Nurse and Midwife:
| Role | Activities |
|---|---|
| Educator | Teach about balanced diet, meal planning |
| Screening agent | Identify undernourished women during ANC |
| Counselor | Provide individualized diet advice |
| Supplement provider | Distribute IFA, calcium, deworming tablets |
| Referral | Send severe cases to dietician or specialist |
| Monitoring | Track weight gain, Hb%, dietary compliance |
| Advocate | Promote use of government nutrition schemes |
🤝🌸 Building Partnership with Women Following RMC Protocol.
🔷 What is RMC?
RMC – Respectful Maternity Care is an approach that ensures women are treated with dignity, respect, and compassion during pregnancy, childbirth, and postpartum care. It is a fundamental human right and a key principle of quality maternal health care.
🔷 Definition of Building Partnership with Women:
Building partnership with women means establishing a mutual, trusting, respectful relationship between the health provider (nurse, midwife, doctor) and the woman. It involves collaborative decision-making, open communication, and the recognition of the woman’s rights, preferences, and values.
🔷 Principles of RMC (Respectful Maternity Care):
Based on White Ribbon Alliance’s Charter of Rights for Women and Newborns.
- Freedom from harm and ill-treatment
- Right to information, informed consent and refusal, and respect for choices
- Confidentiality and privacy
- Dignity and respect
- Equitable care (non-discrimination)
- Timely and quality care
- Freedom from abuse and neglect
- Right to companionship
- Continuity of care
🔷 Steps in Building Partnership with Women under RMC Protocol:
🔶 1️⃣ Establishing Trust and Rapport
- Greet the woman respectfully using her name.
- Introduce yourself and your role.
- Make her feel safe, valued, and comfortable.
🔶 2️⃣ Providing Complete Information
- Explain all procedures in simple, understandable language.
- Encourage questions and clarify doubts.
- Use visuals or local language aids when needed.
🔶 3️⃣ Informed Consent and Shared Decision-Making
- Always seek informed consent before examinations or interventions.
- Respect her right to refuse or accept care.
- Support her decisions regarding birth plan, pain relief, feeding, etc.
🔶 4️⃣ Maintaining Privacy and Confidentiality
- Ensure privacy using curtains, screens, or private areas.
- Do not discuss her personal health information publicly.
- Handle her documents and reports confidentially.
🔶 5️⃣ Allowing Birth Companions
- Encourage a supportive person (husband, mother, friend) to stay during labor and delivery, as per the woman’s preference.
🔶 6️⃣ Culturally Sensitive Care
- Respect her cultural practices and values, as long as they do not harm her or the baby.
- Adjust care plans to align with her beliefs when possible.
🔶 7️⃣ Empowering the Woman
- Encourage her to express pain, ask for comfort, change positions during labor.
- Support her participation in baby care and breastfeeding decisions.
- Appreciate her role and effort during childbirth.
🔷 Nurse/Midwife’s Role in Building Partnership:
| Role | Activities |
|---|---|
| Communicator | Use empathetic, non-judgmental communication |
| Advocate | Stand up for her rights and preferences |
| Educator | Teach her about her body, baby care, and options |
| Supporter | Offer emotional support during labor and postpartum |
| Protector | Prevent disrespect, discrimination, or abuse |
| Care Provider | Deliver safe, evidence-based care with kindness |
🔷 Examples of RMC in Practice:
| Situation | Respectful Care Approach |
|---|---|
| Woman asks about labor pain relief | Explain all options and allow her to choose |
| Woman from rural area feels shy | Speak gently, ensure female staff, maintain privacy |
| Woman wants to sit or walk in labor | Allow mobility unless medically contraindicated |
| Woman refuses a vaginal exam | Respect refusal, explain purpose, and seek consent again later |
| Woman cries or shows fear | Console, encourage, and offer continuous support |
🔷 Benefits of Building Partnership with Women in Maternity Care:
| For the Woman | For the Health System |
|---|---|
| Feels safe, respected, and confident | Higher satisfaction and institutional delivery rates |
| More likely to return for future care | Better maternal and newborn outcomes |
| Reduces birth trauma and depression | Builds community trust in health services |
| Improves cooperation and communication | Reduces staff burnout and conflict |
| Promotes positive childbirth experience | Encourages adherence to care recommendations |
🔷 Barriers to Building Partnership:
- Staff shortage or high workload
- Lack of training in RMC
- Poor infrastructure (privacy issues)
- Cultural bias or judgmental attitudes
- Language barriers
🔷 Overcoming Barriers – What Nurses Can Do:
- Practice empathy and active listening
- Participate in RMC training programs
- Use IEC materials to explain procedures
- Advocate for infrastructure improvements (e.g., screens for privacy)
- Collaborate with community health workers (ASHA/ANM)
👨👩👧 Father’s Engagement in Maternity Care.

🔷 Definition:
Father’s engagement in maternity care refers to the active involvement of the male partner (father) in all phases of maternity — pre-conception, pregnancy, childbirth, and postnatal care — to promote the health and well-being of the mother, baby, and family.
🔷 Why is Father’s Engagement Important?
| Benefits to Mother | Benefits to Baby | Benefits to Father |
|---|---|---|
| Emotional support, reduced stress | Better bonding, improved health | Builds attachment and confidence |
| Shared responsibility | Better breastfeeding outcomes | Promotes shared parenting |
| Encourages ANC visits | Lower neonatal morbidity | Improves relationship with partner |
| Decreased maternal depression | Safer delivery environment | Informed decision-making |
🔷 Stages Where Father’s Engagement is Needed:
✅ 1. Pre-Conception Phase:
- Family planning decisions
- Health screening (e.g., STDs)
- Discussing spacing between children
- Supporting lifestyle changes (e.g., quitting tobacco)
✅ 2. Antenatal Period (ANC):
- Attending ANC check-ups with the mother
- Participating in health education sessions
- Emotional support during pregnancy
- Assisting in dietary and medication compliance
- Helping with household chores to reduce maternal workload
✅ 3. Intra-Natal (Labour & Delivery):
- Acting as a birth companion if permitted
- Providing moral support during labor
- Being present during normal delivery or C-section (where allowed)
- Assisting in transport and logistics for institutional delivery
✅ 4. Postnatal Period (PNC):
- Supporting mother in breastfeeding and rest
- Helping with newborn care (bathing, changing, comforting)
- Monitoring postpartum danger signs
- Ensuring timely immunizations and PNC visits
- Preventing postpartum depression through shared responsibility
🔷 Barriers to Father’s Engagement:
| Cultural/Traditional | Practical | Systemic |
|---|---|---|
| Belief that maternity is “women’s domain” | Work responsibilities, time constraints | Lack of male-friendly hospital policies |
| Gender norms & stigma | Lack of awareness | No private space for fathers in labor rooms |
| Shyness or discomfort | Illiteracy | Poor communication from health workers |
🔷 Strategies to Promote Father’s Engagement:
| Strategy | Example/Activity |
|---|---|
| Health education | Conduct joint counseling sessions for couples during ANC |
| Birth preparedness sessions | Involve fathers in planning transport, hospital bag, birth plan |
| Male involvement campaigns | Community awareness using media, posters, videos |
| Policy support | Encourage health facilities to allow birth companions |
| Father-friendly spaces | Seating area and involvement in child immunization clinics |
| Role modeling | Encourage male CHWs or satisfied fathers to share experiences |
🔷 Role of Nurses and Midwives in Promoting Father’s Engagement:
| Role | Responsibilities |
|---|---|
| Educator | Explain the importance of male involvement in ANC, PNC |
| Facilitator | Welcome fathers during check-ups, encourage questions |
| Advocate | Promote respectful inclusion of men in birth preparedness |
| Supporter | Guide them in emotional and practical support to the mother |
| Bridge Builder | Reduce hesitation or cultural barriers between fathers and health staff |
| Record Keeper | Involve father’s contact in documentation for follow-up |
🔷 Examples of Father Involvement Activities:
- Husband attending health talks with wife at PHC
- Partner providing daily iron/folic acid tablets at home
- Father encouraging exclusive breastfeeding
- Father accompanying mother during labor for emotional support
- Sharing postnatal duties like baby’s immunization visits
🔷 National & Global Guidelines Promoting Father’s Engagement:
| Guideline/Program | Provisions |
|---|---|
| RMNCH+A Approach (India) | Encourages male involvement in maternal and child health |
| WHO Recommendations | Promote birth companionship and family-centered care |
| National Population Policy | Advocates male participation in reproductive health |
| LaQshya Program (India) | Encourages birth companion of choice (including father) |
🌸 Physiological Changes During Pregnancy.
🔷 Introduction:
Pregnancy is a physiological state, not a disease. To support the growth and development of the fetus, a woman’s body undergoes numerous changes across different systems. These changes are mainly influenced by pregnancy hormones such as estrogen, progesterone, hCG, hPL, and relaxin.
These changes begin as early as conception and continue until delivery and postpartum.
🔷 System-Wise Physiological Changes During Pregnancy:
✅ 1️⃣ Reproductive System Changes
a. Uterus
- Increases in size from 50g (non-pregnant) to ~1000g at term
- Capacity increases from 10 mL to ~5 liters
- Shape changes from pear-shaped to ovoid
- Increased blood flow (up to 500–800 mL/min at term)
b. Cervix
- Softening (Goodell’s sign)
- Bluish discoloration (Chadwick’s sign)
- Increased mucus production → forms mucus plug (operculum)
c. Vagina and Vulva
- Increased vascularity → bluish color
- Increased vaginal secretions → leukorrhea
d. Ovaries
- Ovulation stops
- Corpus luteum secretes progesterone until placenta takes over (~12 weeks)
✅ 2️⃣ Endocrine System Changes
| Gland | Change |
|---|---|
| Pituitary | Enlarges, increases prolactin secretion for milk production |
| Thyroid | Enlarges slightly; increased thyroid hormones (T3, T4) |
| Parathyroid | Increases → maintains calcium balance |
| Pancreas | Increased insulin production (to overcome insulin resistance from hPL) |
| Placenta | Acts as a temporary endocrine gland – secretes hCG, hPL, estrogen, progesterone |
✅ 3️⃣ Cardiovascular System Changes
| Change | Description |
|---|---|
| Blood volume | Increases by 40–50% → helps with uteroplacental perfusion |
| Cardiac output | Increases by 30–50% |
| Heart rate | Increases by 10–15 bpm |
| BP | Slight drop in 2nd trimester, returns to normal by term |
| Physiological anemia | Plasma volume increases more than RBC → hemodilution |
| Systolic murmur | May occur due to increased blood flow |
| Supine hypotension syndrome | Compression of inferior vena cava when lying flat |
✅ 4️⃣ Respiratory System Changes
| Change | Description |
|---|---|
| Oxygen demand | Increases by 20–30% to support fetal growth |
| Tidal volume | Increases by ~40% |
| Respiratory rate | Slightly increases or remains same |
| Shortness of breath | Common in late pregnancy due to upward displacement of diaphragm |
✅ 5️⃣ Gastrointestinal (GI) System Changes
| Change | Effect |
|---|---|
| Progesterone | Slows GI motility → constipation, bloating |
| Nausea and vomiting | Due to hCG (especially in 1st trimester) |
| Heartburn (pyrosis) | Due to relaxed lower esophageal sphincter |
| Ptyalism | Increased salivation |
| Gums | May become soft and bleed easily (gingivitis) |
✅ 6️⃣ Urinary System Changes
| Change | Description |
|---|---|
| Kidney size | Slightly increases to meet increased filtration needs |
| GFR (Glomerular Filtration Rate) | Increases by 50% |
| Urinary frequency | Due to increased blood flow and pressure on bladder |
| Risk of UTI | Increased due to urinary stasis and dilated ureters |
✅ 7️⃣ Musculoskeletal System Changes
| Change | Description |
|---|---|
| Relaxin hormone | Softens ligaments and joints for childbirth |
| Lordosis | Increased curvature of spine → back pain |
| Waddling gait | Due to relaxed pelvic joints |
| Leg cramps | Due to pressure on nerves, calcium/phosphate imbalance |
✅ 8️⃣ Integumentary System Changes
| Change | Description |
|---|---|
| Linea nigra | Dark line from pubic area to umbilicus |
| Striae gravidarum | Stretch marks (abdomen, breasts, thighs) |
| Melasma (Chloasma) | “Mask of pregnancy” – dark patches on face |
| Increased hair and nail growth | Due to hormonal changes |
| Sweat and oil glands | Become more active → acne, oily skin |
✅ 9️⃣ Breast Changes
| Change | Description |
|---|---|
| Breast enlargement | Due to estrogen and progesterone |
| Tenderness and tingling | Common early sign |
| Areola darkening and enlargement | Due to increased pigmentation |
| Montgomery’s tubercles | Small glands on areola become prominent |
| Colostrum | Yellowish pre-milk secretion from 16 weeks onward |
✅ 🔟 Hematological Changes
| Parameter | Change |
|---|---|
| Hemoglobin | May slightly decrease (due to hemodilution) |
| WBC count | Increases mildly (normal pregnancy leukocytosis) |
| Platelets | May decrease slightly |
| Coagulation factors | Increase → pregnancy is a hypercoagulable state (risk of thrombosis) |
🔷 Psychological Changes
| Trimester | Emotional State |
|---|---|
| First | Ambivalence, mood swings, anxiety |
| Second | Acceptance, increased body image awareness |
| Third | Impatience, anxiety about labor and baby’s health |
🔷 Role of Nurse/Midwife in Managing Physiological Changes:
| Role | Activities |
|---|---|
| Educator | Teach about normal changes and self-care |
| Counselor | Provide reassurance and emotional support |
| Health Promoter | Suggest diet, rest, and exercise for relief of discomforts |
| Care Provider | Monitor vitals, labs, and screen for complications |
| Referrer | Alert physician if changes indicate pathology (e.g., hypertension, bleeding) |
🌸 Physiological Changes in the Reproductive System During Pregnancy.
🔷 Introduction:
During pregnancy, the reproductive system undergoes significant anatomical, hormonal, and functional changes to support implantation, fetal development, labor, and postpartum recovery. These changes are primarily driven by pregnancy hormones like estrogen, progesterone, hCG, relaxin, and hPL.
🔶 1️⃣ Uterus
| Change | Description |
|---|---|
| Size and Weight | Uterus enlarges from 7.5 cm to ~30 cm; weight increases from 50 g to 1000 g by term. |
| Shape | Pear-shaped → spherical (early) → ovoid (late pregnancy). |
| Position | Rises out of the pelvis into abdominal cavity by 12–14 weeks. |
| Capacity | Increases from 10 mL to 5–10 liters. |
| Muscle hypertrophy | Myometrial cells enlarge and stretch, not multiply. |
| Blood supply | Increases up to 500–800 mL/min at term (90% goes to placenta). |
| Contractility | Braxton Hicks contractions (painless, irregular) begin ~2nd trimester – help tone the uterus. |
🔶 2️⃣ Cervix
| Change | Description |
|---|---|
| Softening | Known as Goodell’s sign – due to increased vascularity and hormonal effect. |
| Color change | Becomes bluish-purple due to increased blood flow – called Chadwick’s sign. |
| Glandular activity | Increases and forms a mucus plug (operculum) to seal cervical canal and protect fetus from infections. |
| Increased vascularity | Leads to edema, softening, and increased friability. |
🔶 3️⃣ Vagina and Vulva
| Change | Description |
|---|---|
| Increased vascularity | Bluish discoloration (part of Chadwick’s sign), congestion, and edema. |
| Softening of tissues | Due to estrogen and relaxin → allows stretching during delivery. |
| Increased vaginal discharge | Thick, white, non-foul smelling leukorrhea – protective but may increase infection risk if hygiene is poor. |
| Acidic pH | pH decreases (~3.5–6.0) due to increased lactic acid production – inhibits bacterial growth but favors Candida albicans (fungal infections). |
🔶 4️⃣ Ovaries
| Change | Description |
|---|---|
| Ovulation ceases | Suppressed due to high estrogen and progesterone levels. |
| Corpus luteum | Maintains early pregnancy by secreting progesterone until placenta takes over (~12 weeks). |
| No follicular development | Follicle-stimulating hormone (FSH) and luteinizing hormone (LH) levels are suppressed. |
🔶 5️⃣ Fallopian Tubes
| Change | Description |
|---|---|
| Congestion and edema | Occur due to increased estrogen levels. |
| No active role after conception | Transported ovum reaches uterus in early pregnancy; after that, tubes are relatively inactive. |
🔶 6️⃣ Breasts (Though not reproductive organs, they’re part of reproductive system functionally)
| Change | Description |
|---|---|
| Enlargement and tenderness | Caused by estrogen and progesterone. |
| Increased blood flow | Veins become more prominent. |
| Darkening of areola and nipple | Due to increased melanocyte activity. |
| Montgomery’s tubercles | Sebaceous glands become prominent on the areola. |
| Colostrum production | Begins as early as 16 weeks (thick, yellow pre-milk). |
| Preparation for lactation | Prolactin from the anterior pituitary increases gradually. |
🔷 Summary Table: Reproductive System Changes During Pregnancy
| Organ | Key Changes |
|---|---|
| Uterus | Enlargement, increased blood flow, Braxton Hicks contractions |
| Cervix | Goodell’s sign, Chadwick’s sign, mucus plug |
| Vagina | Leukorrhea, acidic pH, increased elasticity |
| Ovaries | Corpus luteum sustains early pregnancy, no ovulation |
| Breasts | Enlargement, colostrum secretion, areolar changes |
🔷 Clinical Significance of These Changes:
- Helps in early diagnosis of pregnancy (Goodell’s and Chadwick’s signs).
- Supports fetal growth and placental perfusion.
- Prepares the body for labor, delivery, and postpartum lactation.
- Nurses should differentiate normal physiological changes from pathological signs (e.g., infection vs leukorrhea).
🔷 Nurse/Midwife’s Role in Monitoring Reproductive Changes:
| Role | Responsibilities |
|---|---|
| Educator | Explain normal changes and how to manage discomforts. |
| Examiner | Assess for cervical changes, vaginal discharge, uterine growth. |
| Care provider | Ensure maternal hygiene, prevent infections, provide supplements. |
| Counselor | Reassure women about body changes and address concerns. |
| Referrer | Identify abnormal findings (e.g., bleeding, abnormal discharge) and refer. |
❤️ Cardiovascular System – Physiological Changes During Pregnancy.
🔷 Introduction:
During pregnancy, the cardiovascular system adapts significantly to meet the increased metabolic demands of the mother and the growing fetus. These changes begin early in pregnancy and peak in the second trimester, remaining until delivery.
They are mainly influenced by hormonal changes, especially estrogen, progesterone, relaxin, and increased blood volume.
🔷 Major Cardiovascular Changes in Pregnancy:
✅ 1️⃣ Blood Volume Increases
| Parameter | Change |
|---|---|
| Total blood volume | Increases by 40–50% (approx. 1500 mL extra) |
| Plasma volume | Increases more than red cell mass → causes hemodilution |
| Red cell mass | Increases by ~20–30% with iron supplementation |
| Clinical effect | Leads to physiological anemia of pregnancy (Hb may drop to 10.5–11 g/dL) |
✅ 2️⃣ Cardiac Output Increases
| Parameter | Change |
|---|---|
| Cardiac output | Increases by 30–50% due to increased stroke volume and heart rate |
| Peak | Reaches peak around 20–24 weeks |
| Heart rate | Increases by 10–15 beats/min |
| Stroke volume | Increases due to increased preload (blood return) |
✅ 3️⃣ Blood Pressure Changes
| Parameter | Change |
|---|---|
| Systolic BP | May remain same or slightly decrease |
| Diastolic BP | Drops in second trimester (~10–15 mmHg), returns to normal by term |
| Reason | Due to vasodilation from progesterone and relaxin |
| Clinical Tip | Persistent rise in BP after 20 weeks may indicate pre-eclampsia |
✅ 4️⃣ Vascular Resistance and Vasodilation
| Feature | Description |
|---|---|
| Peripheral vascular resistance | Decreases due to progesterone and increased blood volume |
| Vasodilation | Leads to warm skin, nasal congestion, and sometimes dizziness |
✅ 5️⃣ Heart Position and Sounds
| Feature | Description |
|---|---|
| Heart displacement | Slightly upward and to the left due to enlarging uterus |
| Auscultation changes | May hear systolic murmurs or louder heart sounds – physiological and benign |
| ECG changes | May show left axis deviation or slight changes, usually normal |
✅ 6️⃣ Supine Hypotension Syndrome (Aortocaval Compression)
| Condition | Description |
|---|---|
| Cause | When lying flat in late pregnancy, the gravid uterus compresses inferior vena cava |
| Symptoms | Dizziness, pallor, hypotension, nausea, sweating, fainting |
| Management | Advise woman to lie in left lateral position to relieve pressure |
✅ 7️⃣ Venous Circulation and Varicosities
| Feature | Change |
|---|---|
| Venous pressure in lower limbs | Increases due to pressure from the uterus |
| Varicose veins | May appear in legs, vulva, or rectum (hemorrhoids) |
| Risk of thrombosis | Pregnancy is a hypercoagulable state due to increased clotting factors – risk of DVT and embolism |
🔷 Summary Table: Cardiovascular Changes in Pregnancy
| Parameter | Change During Pregnancy |
|---|---|
| Blood volume | ↑ by 40–50% |
| Cardiac output | ↑ by 30–50% |
| Heart rate | ↑ by 10–15 bpm |
| Blood pressure | ↓ in 2nd trimester, normal at term |
| Vascular resistance | ↓ due to vasodilation |
| Murmurs | Systolic murmur may be heard |
| Clotting tendency | ↑ (hypercoagulability) |
| Supine hypotension | Risk increases after 20 weeks |
🔷 Clinical Significance:
| Significance | Explanation |
|---|---|
| Early detection of preeclampsia | Monitor BP trends in each trimester |
| Iron supplementation | To prevent or correct physiological anemia |
| Avoid supine position | Especially in 3rd trimester – left lateral recommended |
| Monitor for varicose veins or thrombosis | Elevate legs, advise light exercise |
🔷 Role of Nurse and Midwife:
| Role | Responsibilities |
|---|---|
| Monitor vital signs | BP, HR, signs of anemia |
| Educate woman | About position changes, warning signs (e.g., dizziness, palpitations) |
| Assess for edema and varicose veins | Suggest support stockings and leg elevation |
| Check for signs of thrombosis | Leg pain, swelling, redness |
| Provide iron and folic acid | Prevent anemia |
| Emergency referral | If symptoms of pre-eclampsia or cardiac distress are seen |
🌬️ Physiological Changes in the Respiratory System During Pregnancy.
🔷 Introduction:
During pregnancy, the respiratory system undergoes several physiological adaptations to meet the increased oxygen demands of both the mother and the growing fetus. These changes begin early in pregnancy and are influenced by hormones (especially progesterone and estrogen) and mechanical pressure from the growing uterus.
🔷 Goals of Respiratory Changes in Pregnancy:
- To increase oxygen availability for the fetus
- To remove excess carbon dioxide from the fetus through maternal lungs
- To maintain acid-base balance
- To adapt to mechanical changes in the thorax due to uterine enlargement
🔶 Major Respiratory Changes in Pregnancy:
✅ 1️⃣ Increased Oxygen Demand
| Feature | Description |
|---|---|
| Oxygen consumption | Increases by 20–30% |
| Basal metabolic rate (BMR) | Rises due to fetal growth and maternal tissue metabolism |
| Reason | To supply oxygen to placenta, uterus, fetus, and maternal organs |
✅ 2️⃣ Tidal Volume Increases
| Parameter | Change |
|---|---|
| Tidal volume | Increases by ~40% |
| Minute ventilation | Increases by 30–50% |
| Respiratory rate | May slightly increase or remain unchanged |
| Alveolar ventilation | Increases due to deeper breathing |
✅ 3️⃣ Chest and Diaphragm Adaptations
| Feature | Change |
|---|---|
| Diaphragm elevation | Rises by ~4 cm due to enlarging uterus |
| Chest circumference | Increases by 5–7 cm |
| Rib cage expansion | Ribs flare outward due to relaxin and estrogen |
| Effect | Though the lungs are compressed, total respiratory function is maintained through increased efficiency of breathing |
✅ 4️⃣ Respiratory Alkalosis
| Change | Description |
|---|---|
| Progesterone effect | Acts as a respiratory stimulant on the respiratory center |
| Result | Leads to mild respiratory alkalosis (↓ PaCO₂) and increased pH |
| Clinical importance | Facilitates CO₂ removal from fetal to maternal blood via placenta (feto-maternal gas exchange) |
✅ 5️⃣ Nasal and Upper Respiratory Tract Changes
| Change | Description |
|---|---|
| Capillary engorgement | Nasal mucosa becomes more vascular and congested |
| Nasal stuffiness & epistaxis | Common complaints due to estrogen effects |
| Voice changes or snoring | May occur due to swelling in vocal cords or nasal passages |
🔷 Summary Table: Respiratory Changes in Pregnancy
| Parameter | Change |
|---|---|
| Oxygen consumption | ↑ by 20–30% |
| Tidal volume | ↑ by ~40% |
| Minute ventilation | ↑ by ~50% |
| Respiratory rate | Slight ↑ or unchanged |
| Diaphragm position | Elevated by ~4 cm |
| Rib cage mobility | ↑ due to hormone-mediated relaxation |
| Nasal mucosa | Congested → nasal stuffiness/bleeding |
| ABG (Arterial Blood Gas) | Mild respiratory alkalosis (↓ PaCO₂, ↑ pH) |
🔷 Common Respiratory Discomforts During Pregnancy:
| Discomfort | Cause |
|---|---|
| Shortness of breath (dyspnea) | Increased tidal volume and upward diaphragm displacement |
| Nasal congestion | Estrogen-induced mucosal swelling |
| Mild hyperventilation | Due to progesterone’s effect on respiratory center |
| Snoring | Weight gain and mucosal edema |
📝 These symptoms are usually physiological and non-pathological, but they should be differentiated from respiratory diseases (e.g., asthma, pulmonary embolism).
🔷 Role of Nurse and Midwife:
| Role | Responsibilities |
|---|---|
| Educator | Explain that shortness of breath is common and usually not dangerous |
| Reassurer | Reduce anxiety about breathing changes in pregnancy |
| Health Promoter | Encourage sleeping in propped-up or semi-Fowler’s position |
| Monitor | Observe for signs of respiratory distress, cyanosis, or abnormal breath sounds |
| Referrer | Refer to physician if breathlessness is sudden, severe, or associated with chest pain or cough |
🔷 Clinical Alert Signs (Not Normal):
While most changes are physiological, watch for:
- Persistent or worsening breathlessness
- Tachypnea (>20 breaths/min)
- Chest pain
- Cough with sputum or blood
- Cyanosis or wheezing
- Signs of pulmonary embolism or asthma
🌊 Physiological Changes in the Urinary System During Pregnancy.
🔷 Introduction:
During pregnancy, the urinary system undergoes various structural and functional changes to accommodate the increased metabolic and circulatory demands of the mother and fetus. These changes are influenced by hormones (mainly progesterone and relaxin) and the mechanical pressure from the enlarging uterus.
🔷 Why Urinary Changes Are Important:
- To eliminate increased waste products from the mother and fetus
- To maintain fluid and electrolyte balance
- To support plasma volume expansion
- To adapt to mechanical compression from the gravid uterus
🔶 Key Structures Affected:
- Kidneys
- Ureters
- Urinary bladder
- Urethra
🔶 1️⃣ Kidney Changes
| Feature | Change |
|---|---|
| Size | Slight increase in kidney length (by 1–1.5 cm) |
| Renal plasma flow (RPF) | Increases by ~50–70% in early pregnancy |
| Glomerular filtration rate (GFR) | Increases by ~40–50% → leads to more urine formation |
| Functional adaptation | Enhances clearance of urea, creatinine, and waste from fetus and mother |
| Serum urea/creatinine | Slightly lower than normal due to increased excretion |
| Mild glycosuria/proteinuria | May occur due to increased GFR → should be monitored to rule out gestational diabetes or pre-eclampsia |
🔶 2️⃣ Ureteral Changes
| Feature | Change |
|---|---|
| Dilation (Hydroureter) | Progesterone causes relaxation of smooth muscles → ureters become dilated, especially on the right side |
| Urinary stasis | Increased risk of urinary tract infections (UTIs) and pyelonephritis |
| Length and tone | Peristalsis decreases, ureters elongate and become tortuous |
🔶 3️⃣ Bladder Changes
| Feature | Change |
|---|---|
| Bladder capacity | May reduce due to pressure from the growing uterus |
| Increased frequency of urination | Especially in 1st and 3rd trimesters |
| Nocturia | Common in later pregnancy |
| Urinary incontinence | Can occur due to relaxed pelvic floor muscles and pressure on the bladder |
| Risk of infection | Stagnation of urine increases risk of cystitis and ascending infections |
🔶 4️⃣ Urethral Changes
| Feature | Change |
|---|---|
| Softening | Due to estrogen and progesterone |
| Lengthening | Urethra becomes slightly elongated due to bladder displacement |
| Increased sensitivity | May lead to burning sensation or frequency even without infection |
🔷 Common Urinary Complaints in Pregnancy:
| Complaint | Cause |
|---|---|
| Frequency | Enlarged uterus pressing on bladder |
| Urgency | Hormonal effects and pressure |
| Nocturia | Increased renal perfusion in lying position |
| Mild stress incontinence | Relaxed pelvic muscles and pressure |
| Burning micturition | May be due to infection or mucosal sensitivity |
| UTIs | Due to urinary stasis and dilated ureters |
🔷 Clinical Significance:
- Increased risk of asymptomatic bacteriuria, which can progress to pyelonephritis if untreated
- Changes must be monitored to distinguish between normal physiology and pathology
- UTIs during pregnancy can lead to preterm labor, low birth weight, and other complications
🔷 Urine Tests in Pregnancy Monitoring:
| Test | Purpose |
|---|---|
| Routine urine examination | Check for albumin (protein), sugar, pus cells |
| Urine culture | For detecting asymptomatic or symptomatic infections |
| Proteinuria | Indicates risk of pre-eclampsia if persistent |
| Glycosuria | May suggest gestational diabetes – needs further evaluation |
🔷 Nurse/Midwife’s Role in Urinary Care During Pregnancy:
| Role | Responsibilities |
|---|---|
| Educator | Teach hygiene, hydration, and signs of UTI |
| Monitor | Observe urinary symptoms and perform regular urine testing |
| Care Provider | Encourage pelvic floor exercises to prevent incontinence |
| Referrer | Refer if there is persistent proteinuria, hematuria, or UTI symptoms |
| Health Promoter | Encourage at least 2.5–3 liters of fluid intake daily (unless contraindicated) |
🔷 Self-Care Advice for Pregnant Women:
- Drink plenty of water
- Empty bladder regularly
- Wipe front to back after urination
- Avoid holding urine for long periods
- Wear breathable, cotton underwear
- Practice Kegel exercises to strengthen pelvic muscles
🍽️ Gastrointestinal System – Physiological Changes During Pregnancy.
🔷 Introduction:
During pregnancy, the gastrointestinal (GI) system undergoes multiple anatomical and functional changes to support fetal growth and adapt to hormonal and mechanical influences. These changes are primarily caused by:
- Progesterone: Smooth muscle relaxant
- Estrogen: Increases vascularity and affects liver function
- Mechanical pressure from the enlarging uterus
🔷 Major Gastrointestinal Changes in Pregnancy:
✅ 1️⃣ Oral Cavity and Esophagus
| Change | Description |
|---|---|
| Gingivitis & gum bleeding | Due to increased vascularity and estrogen effect (common in 1st trimester) |
| Ptyalism (excessive salivation) | Often seen in early pregnancy |
| Dental caries | May increase due to acid reflux and poor oral hygiene |
| Esophageal reflux (Heartburn/Pyrosis) | Caused by relaxation of lower esophageal sphincter and increased intra-abdominal pressure → allows gastric acid to reflux into esophagus |
✅ 2️⃣ Stomach
| Change | Description |
|---|---|
| Nausea and vomiting | Common in 1st trimester due to hCG and estrogen – called morning sickness |
| Delayed gastric emptying | Due to progesterone-induced smooth muscle relaxation |
| Increased risk of gastritis or reflux | Especially in later pregnancy due to pressure from the uterus |
✅ 3️⃣ Intestines
| Change | Description |
|---|---|
| Constipation | Due to decreased peristalsis and water absorption; worsened by iron supplements |
| Flatulence and bloating | Caused by slowed digestion and increased gas formation |
| Hemorrhoids (Piles) | Caused by constipation and increased pelvic pressure; common in 3rd trimester |
✅ 4️⃣ Liver and Gallbladder
| Organ | Change |
|---|---|
| Liver | No size change, but slight changes in liver enzyme levels (alkaline phosphatase ↑ due to placental production) |
| Gallbladder | Becomes hypotonic → bile stasis → risk of gallstones and cholestasis |
| Cholestasis of pregnancy | Causes itching (pruritus), especially on palms and soles; may affect fetal outcome |
✅ 5️⃣ Appetite and Food Preferences
| Change | Description |
|---|---|
| Increased appetite | Often from 2nd trimester onward |
| Food cravings and aversions | Common, possibly due to hormonal changes |
| Pica | Craving for non-food substances (e.g., clay, ice, chalk) – indicates iron/zinc deficiency |
🔷 Common GI Symptoms in Pregnancy:
| Symptom | Likely Cause |
|---|---|
| Morning sickness | hCG, estrogen |
| Constipation | Progesterone, iron |
| Heartburn | Relaxed LES and uterine pressure |
| Hemorrhoids | Constipation, pelvic pressure |
| Bloating | Slowed digestion |
| Nausea/Vomiting | 1st trimester hormones |
| Excess salivation (ptyalism) | Increased estrogen |
| Itching (in cholestasis) | Bile stasis in liver |
🔷 Clinical Significance:
- Must differentiate between normal and abnormal (e.g., hyperemesis gravidarum = excessive vomiting with dehydration and weight loss)
- Monitor for signs of liver dysfunction in cholestasis
- Ensure nutritional adequacy despite nausea, vomiting, or food aversions
🔷 Nurse/Midwife’s Role in GI Care During Pregnancy:
| Role | Activities |
|---|---|
| Educator | Teach dietary habits, hydration, iron-rich foods |
| Counselor | Reassure about symptoms like nausea, heartburn |
| Monitor | Assess bowel habits, weight gain, appetite |
| Referrer | In case of persistent vomiting, jaundice, or bleeding piles |
| Care provider | Suggest remedies for constipation, prescribe iron with stool softeners if needed |
🔷 Self-Care Advice for GI Health in Pregnancy:
- Eat small, frequent meals
- Avoid spicy, oily, acidic foods
- Drink plenty of water
- Eat fiber-rich foods (fruits, vegetables, whole grains)
- Avoid lying down immediately after meals
- Practice gentle exercise or walking
- Sit in a comfortable position while eating
🔷 When to Seek Medical Help:
- Persistent vomiting with dehydration (hyperemesis gravidarum)
- Constipation lasting >5 days
- Severe or bleeding hemorrhoids
- Intense itching (possible intrahepatic cholestasis)
- Upper abdominal pain or jaundice
🔥 Metabolic Changes During Pregnancy.
🔷 Introduction:
Pregnancy is a hypermetabolic state. The body undergoes significant metabolic adaptations to:
- Support fetal growth and development
- Prepare the mother for labor, delivery, and lactation
- Ensure survival during fasting or stress
These changes are driven by hormones such as hPL (human placental lactogen), progesterone, estrogen, cortisol, insulin, and thyroid hormones.
🔷 Key Metabolic Changes in Pregnancy:
✅ 1️⃣ Increased Basal Metabolic Rate (BMR)
| Change | Description |
|---|---|
| BMR increases by 20–30% | Due to the increased energy needs of mother and fetus |
| Increased oxygen consumption | To meet fetal metabolic demands |
| Heat production rises | Pregnant women feel warm or may sweat more |
✅ 2️⃣ Carbohydrate Metabolism
| Trimester | Change |
|---|---|
| First trimester | ↑ Insulin sensitivity → mild hypoglycemia in fasting state |
| Second & Third trimesters | Placental hormones (especially hPL) cause insulin resistance → ensures glucose is available to the fetus |
🔹 The mother becomes slightly insulin-resistant in later pregnancy — this is physiological but may lead to gestational diabetes in some women.
✅ 3️⃣ Protein Metabolism
| Feature | Description |
|---|---|
| Positive nitrogen balance | Promotes fetal tissue growth, uterus, breasts, placenta |
| Protein demand increases | Especially in 2nd and 3rd trimester for fetal development |
| Sources | Dietary protein and maternal stores are mobilized |
✅ 4️⃣ Fat Metabolism
| Stage | Change |
|---|---|
| Early pregnancy | Fat storage increases in maternal adipose tissues (estrogen & insulin effect) |
| Late pregnancy | Fat is mobilized to meet increased maternal energy demands and fetal needs |
| Increased lipolysis | Leads to higher levels of free fatty acids and triglycerides in maternal blood |
🔹 This adaptation ensures glucose is reserved for the fetus while the mother uses fat as energy.
✅ 5️⃣ Mineral and Electrolyte Metabolism
| Mineral | Change |
|---|---|
| Calcium | Increased absorption from the gut; needed for fetal bones & teeth |
| Iron | ↑ requirement for fetal hemoglobin & maternal blood volume → risk of anemia if diet is inadequate |
| Sodium & Water | Retained → contributes to plasma volume expansion and physiological edema |
| Iodine | Needed for fetal brain development → deficiency may cause cretinism |
✅ 6️⃣ Water Metabolism
| Feature | Change |
|---|---|
| Fluid retention | ↑ total body water by ~6–8 liters (plasma, amniotic fluid, tissues) |
| Edema | Common in feet and legs due to sodium retention and pressure on veins |
| Risk of dehydration | Despite fluid retention, increased demand means mother must stay hydrated |
🔷 Summary Table: Metabolic Changes in Pregnancy
| Type of Metabolism | Change |
|---|---|
| BMR | ↑ by 20–30% |
| Glucose | ↑ insulin resistance (2nd & 3rd trimester) |
| Protein | Positive nitrogen balance, increased demand |
| Fat | Early storage → late mobilization |
| Iron & calcium | Increased absorption and demand |
| Water | Retained → ↑ plasma volume, slight edema |
🔷 Clinical Significance:
- Gestational diabetes can develop due to insulin resistance
- Nutritional counseling is essential to meet protein, iron, calcium, and calorie requirements
- Anemia and hypoglycemia must be monitored, especially in undernourished women
- Weight gain monitoring is important:
➤ Normal BMI women should gain 11–16 kg during pregnancy - Fluid intake and edema management are part of antenatal care
🔷 Role of Nurse/Midwife:
| Role | Responsibilities |
|---|---|
| Educator | Teach about balanced diet and nutrient needs |
| Monitor | Weight gain, blood sugar, edema, anemia |
| Supporter | Provide emotional and dietary support |
| Care provider | Distribute iron, calcium, IFA tablets |
| Referrer | Refer for gestational diabetes screening if risk factors are present |
🦴 Skeletal Changes During Pregnancy.
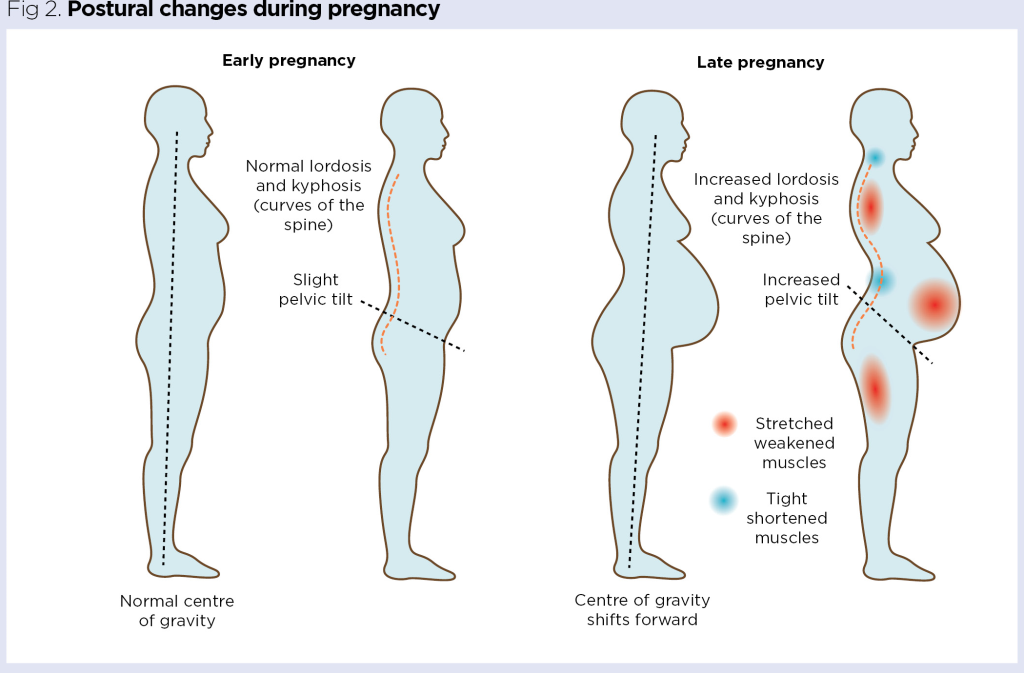
🔷 Introduction:
During pregnancy, the skeletal system undergoes various structural and postural changes to accommodate the growing fetus, support increased maternal weight, and prepare the body for labor and delivery. These changes are mostly due to the action of hormones such as relaxin, estrogen, and progesterone, and mechanical stress caused by the enlarging uterus.
🔷 Why Skeletal Changes Occur:
- To allow enlargement of the uterus and abdominal cavity
- To adjust posture and balance due to weight gain
- To loosen joints and ligaments for childbirth
- To support fetal nutrient requirements, especially calcium
🔶 Key Skeletal and Postural Changes During Pregnancy:
✅ 1️⃣ Postural Alterations
| Change | Description |
|---|---|
| Lumbar lordosis | Increased inward curve of the lower back to balance the shifting center of gravity → leads to backache |
| Waddling gait | Due to relaxation of pelvic joints and ligaments |
| Forward tilting of pelvis | Uterus pulls the pelvis forward, changing alignment |
| Rounded shoulders | Caused by breast enlargement and posture compensation |
✅ 2️⃣ Pelvic Joint and Ligament Softening
| Change | Description |
|---|---|
| Relaxation of ligaments | Due to hormone relaxin → increases flexibility of pelvic joints |
| Sacroiliac joint loosening | Pelvic bones move slightly apart to prepare for delivery |
| Symphysis pubis widening | Slight separation of pubic symphysis (can cause pain and instability) |
| Benefit | Allows pelvis to expand during childbirth (facilitates vaginal delivery) |
✅ 3️⃣ Calcium and Bone Metabolism
| Change | Description |
|---|---|
| Increased calcium demand | For fetal bone and teeth formation |
| Maternal calcium absorption | ↑ intestinal absorption of calcium under influence of vitamin D and parathyroid hormone |
| Bone density | May reduce temporarily if calcium intake is insufficient |
| Risk | In severe deficiency, maternal bones may demineralize → osteomalacia or bone pain |
✅ 4️⃣ Rib Cage Expansion
| Change | Description |
|---|---|
| Rib flare | Ribs widen outward and upward to allow lung expansion |
| Subcostal angle increases | From ~68° to 103° |
| Reason | Compensates for diaphragm elevation due to enlarged uterus |
🔷 Common Skeletal Discomforts in Pregnancy:
| Discomfort | Cause |
|---|---|
| Back pain | Due to increased lumbar lordosis and weight gain |
| Pelvic pain | Loosening of pelvic joints and pubic symphysis |
| Leg cramps | Possibly due to calcium/magnesium deficiency or nerve compression |
| Foot pain or flat feet | Due to relaxed ligaments and weight gain |
🔷 Preventive & Supportive Measures:
| Measure | Description |
|---|---|
| Posture correction | Sit and stand with back support, avoid high heels |
| Pelvic exercises | E.g., pelvic tilts, squats to strengthen back and pelvis |
| Calcium supplementation | As per ANC guidelines (usually 1000–1200 mg/day) |
| Light exercise | Walking, prenatal yoga to reduce stiffness and pain |
| Back support belts | For late pregnancy to relieve back pain |
| Avoid prolonged standing or sitting | To reduce musculoskeletal strain |
🔷 Nurse/Midwife’s Role in Managing Skeletal Changes:
| Role | Responsibilities |
|---|---|
| Educator | Teach posture, movement, and exercise techniques |
| Counselor | Reassure that mild discomfort is common and temporary |
| Care Provider | Recommend calcium and vitamin D supplements |
| Referrer | Refer for physiotherapy if severe back or pelvic pain |
| Supporter | Provide ergonomic tips during daily activities and work |
🔷 Summary Table: Skeletal Changes in Pregnancy
| Change | Effect |
|---|---|
| ↑ Lumbar lordosis | Backache |
| ↑ Joint laxity | Pelvic flexibility, waddling gait |
| ↑ Symphysis pubis width | Pelvic pain, instability |
| Rib cage expansion | Aids respiratory adaptation |
| ↑ Calcium requirement | Risk of deficiency if diet is poor |
🌺 Skin Changes During Pregnancy.

🔷 Introduction:
Pregnancy brings about many cutaneous (skin) changes, most of which are physiological and caused by hormonal fluctuations, increased vascularity, and stretching of the skin due to the enlarging uterus and breasts.
These changes vary in intensity and visibility from woman to woman and are influenced by genetics, ethnicity, and skin type.
🔷 Causes of Skin Changes in Pregnancy:
| Cause | Description |
|---|---|
| Hormones | Estrogen, progesterone, and melanocyte-stimulating hormone (MSH) |
| Increased blood volume | Causes vascular skin changes |
| Mechanical stretching | Leads to marks and thinning of skin |
| Immune changes | Can affect pre-existing skin conditions |
🔶 Common Physiological Skin Changes During Pregnancy:
✅ 1️⃣ Pigmentation Changes
| Skin Change | Description |
|---|---|
| Linea nigra | Dark vertical line from pubic area to umbilicus (or above); more prominent in darker-skinned women |
| Melasma (Chloasma/Mask of pregnancy) | Brown patches on cheeks, forehead, upper lip; triggered by sun exposure |
| Darkening of nipples, areola, genitalia | Due to increased melanin production |
| Nevi and freckles | May become darker or increase in size (should still be monitored for abnormal changes) |
✅ 2️⃣ Striae Gravidarum (Stretch Marks)
| Feature | Description |
|---|---|
| Appearance | Pink, red, or purple lines over abdomen, breasts, thighs, or buttocks |
| Cause | Skin stretching + breakdown of elastic tissue |
| When | Typically appear after 2nd trimester |
| After delivery | Fade to silvery or white lines over time (not completely disappear) |
✅ 3️⃣ Vascular Changes
| Change | Description |
|---|---|
| Spider angiomas | Small, red, spider-like blood vessels on face, neck, chest |
| Palmar erythema | Redness of palms due to estrogen effect |
| Varicose veins | In legs, vulva, or rectum (hemorrhoids) due to pressure and vascular congestion |
| Increased warmth of skin | Due to increased blood flow |
✅ 4️⃣ Hair and Nail Changes
| Change | Description |
|---|---|
| Hair growth | May increase due to estrogen (scalp, body hair); some may experience less hair fall during pregnancy |
| Hair loss after delivery | Common (called postpartum telogen effluvium) – usually temporary |
| Nails | May grow faster, become more brittle or soft |
✅ 5️⃣ Sweat and Oil Gland Changes
| Glands | Change |
|---|---|
| Sweat glands | More active → increased sweating (hyperhidrosis) |
| Sebaceous glands | ↑ oil secretion → acne may worsen or improve |
| Montgomery’s tubercles | Enlarged sebaceous glands on areola – normal and protective for breastfeeding |
✅ 6️⃣ Itching (Pruritus)
| Cause | Description |
|---|---|
| Skin stretching | Common over abdomen, breasts |
| Hormonal changes | Can make skin drier or more sensitive |
| Intrahepatic cholestasis of pregnancy | A pathological cause; causes intense itching, especially on palms and soles → needs urgent medical attention |
🔷 Summary Table: Skin Changes in Pregnancy
| Type of Change | Examples |
|---|---|
| Pigmentation | Linea nigra, melasma, darkened nipples |
| Structural | Stretch marks, spider veins, varicose veins |
| Glandular | Increased sweating, oiliness, acne |
| Hair/Nail | Increased hair growth, faster nail growth |
| Other | Palmar erythema, Montgomery’s tubercles |
🔷 Clinical Significance:
- Most changes are harmless and temporary
- Some may cause cosmetic concerns or discomfort
- Important to differentiate normal changes from skin disorders (e.g., rashes, infections, or pregnancy-specific dermatoses)
🔷 Nurse/Midwife’s Role:
| Role | Responsibilities |
|---|---|
| Educator | Reassure that skin changes are normal and usually fade postpartum |
| Supporter | Provide emotional support if woman feels self-conscious |
| Care Provider | Suggest safe skin care tips – moisturizers, mild cleansers, sun protection |
| Monitor | Watch for abnormal skin conditions like pruritic urticarial papules and plaques of pregnancy (PUPPP) or cholestasis-related itching |
| Referrer | Send to dermatologist if suspicious skin lesions, severe itching, or signs of allergy appear |
🔷 Skin Care Advice During Pregnancy:
- Use mild, non-irritating cleansers and moisturizers
- Avoid harsh cosmetics or bleaching agents
- Wear sunscreen to reduce melasma worsening
- Apply cocoa butter or vitamin E lotions to improve skin elasticity (limited evidence, but may help)
- Drink plenty of water
- Use loose, breathable clothing to avoid sweat rash
- Seek help if itching is severe or affecting sleep
🧬 Endocrine System Changes During Pregnancy.
🔷 Introduction:
The endocrine system plays a central role in pregnancy. It undergoes dramatic changes to support:
- Fetal growth and development
- Maternal adaptation
- Labor, delivery, and lactation
Multiple hormonal glands either increase their activity or produce new hormones via the placenta.
🔷 Major Endocrine Glands Involved in Pregnancy:
- Pituitary gland
- Thyroid gland
- Parathyroid gland
- Pancreas
- Adrenal glands
- Placenta (temporary endocrine organ)
🔶 1️⃣ Pituitary Gland Changes
| Hormone | Change & Function |
|---|---|
| Prolactin (from anterior pituitary) | ↑ dramatically to prepare for lactation |
| Oxytocin (from posterior pituitary) | Stored for labor (uterine contractions) and milk ejection reflex |
| FSH & LH | ↓ suppressed during pregnancy due to high estrogen & progesterone |
| ACTH & MSH | ↑ mildly, contributing to skin pigmentation changes |
🔶 2️⃣ Thyroid Gland Changes
| Change | Description |
|---|---|
| Size | Slight enlargement (↑ vascularity and activity) |
| T3 and T4 | ↑ levels due to stimulation by hCG (especially in early pregnancy) |
| TSH | ↓ mildly in 1st trimester; normalizes later |
| Function | Supports fetal brain development and maternal metabolism |
🔸 Iodine requirement increases to meet fetal thyroid needs.
🔶 3️⃣ Parathyroid Gland Changes
| Change | Function |
|---|---|
| Mild hypertrophy | ↑ Parathyroid hormone (PTH) to regulate calcium levels |
| Ensures | Adequate calcium transfer to fetus (for bones and teeth) |
🔶 4️⃣ Pancreatic Changes
| Change | Description |
|---|---|
| Early pregnancy | ↑ insulin sensitivity → may cause mild hypoglycemia |
| Later pregnancy (2nd–3rd trimester) | Insulin resistance increases due to hPL, estrogen, progesterone |
| Outcome | Maternal blood glucose ↑ → glucose available to fetus |
| Risk | Gestational diabetes in some women due to poor insulin compensation |
🔶 5️⃣ Adrenal Gland Changes
| Hormone | Change |
|---|---|
| Cortisol | ↑ due to estrogen; helps in metabolism and stress response |
| Aldosterone | ↑ to help in sodium and water retention → contributes to plasma volume expansion |
| Androgens (DHEA-S) | Secreted by fetal adrenal gland → converted to estrogen by placenta |
🔶 6️⃣ Placenta as an Endocrine Organ
The placenta acts as a temporary endocrine gland and produces key pregnancy hormones:
| Hormone | Function |
|---|---|
| hCG (human chorionic gonadotropin) | Maintains corpus luteum in early pregnancy; used in pregnancy tests |
| hPL (human placental lactogen) | Causes insulin resistance, mobilizes maternal fat for energy, promotes breast development |
| Estrogen | Stimulates uterine growth, breast changes, blood flow |
| Progesterone | Maintains uterine lining, prevents contractions, supports implantation |
| Relaxin | Softens ligaments and cervix for labor preparation |
🔷 Summary Table: Endocrine Changes in Pregnancy
| Gland | Hormonal Change | Function |
|---|---|---|
| Pituitary | ↑ Prolactin, Oxytocin | Lactation, labor |
| Thyroid | ↑ T3, T4 | Metabolism, fetal brain development |
| Parathyroid | ↑ PTH | Calcium regulation |
| Pancreas | ↑ Insulin resistance | Glucose supply to fetus |
| Adrenal | ↑ Cortisol, Aldosterone | Metabolism, fluid retention |
| Placenta | ↑ hCG, hPL, Estrogen, Progesterone | Pregnancy maintenance |
🔷 Clinical Significance:
| Condition | Related Hormone |
|---|---|
| Gestational diabetes | hPL, insulin resistance |
| Pregnancy goiter / Hyperthyroidism symptoms | ↑ thyroid hormones |
| Hypocalcemia in mother | High fetal calcium demand |
| Preterm labor | Imbalance in progesterone, oxytocin |
| Postpartum depression | Sudden drop in estrogen and progesterone after birth |
🔷 Nurse/Midwife’s Role in Managing Endocrine Changes:
| Role | Activities |
|---|---|
| Monitor | Weight, glucose levels, thyroid function, signs of hormonal imbalance |
| Educator | Teach about gestational diabetes, dietary management |
| Care provider | Ensure supplementation (e.g., iron, calcium, iodine) |
| Referrer | Suspected thyroid or endocrine disorders to endocrinologist |
| Supporter | Counsel about emotional and behavioral changes due to hormones |
🧠🌸 Psychological Changes During Pregnancy.
🔷 Introduction:
Pregnancy is not only a physical journey but also a psychological and emotional transformation. A woman undergoes a wide range of mental, emotional, and behavioral changes as she adjusts to the demands of pregnancy, impending motherhood, and changes in identity, relationships, and life roles.
These changes are influenced by:
- Hormones (estrogen, progesterone)
- Social factors (family support, financial situation)
- Previous pregnancy experiences
- Cultural expectations
🔷 Phases of Psychological Adaptation During Pregnancy (Trimester-Wise)
✅ 1️⃣ First Trimester: “Ambivalence and Adjustment”
| Emotional States | Description |
|---|---|
| Ambivalence | Mixed feelings – excitement, fear, disbelief, anxiety |
| Mood swings | Due to hormonal shifts (estrogen & progesterone) |
| Fatigue and irritability | Common, may feel overwhelmed |
| Concern about miscarriage | Common fear in early pregnancy |
| Body image awareness begins | Especially with nausea or bloating |
✅ 2️⃣ Second Trimester: “Acceptance and Attachment”
| Emotional States | Description |
|---|---|
| Better mood | Hormonal balance improves; physical discomforts lessen |
| Acceptance of pregnancy | Begins to feel more “real” as body changes and fetal movements begin |
| Fetal bonding starts | Talking to baby, imagining baby’s future |
| Feeling attractive or unattractive | Based on body changes and cultural norms |
| Focus shifts to baby and motherhood | Begins forming maternal identity |
✅ 3️⃣ Third Trimester: “Preparation and Anticipation”
| Emotional States | Description |
|---|---|
| Anxiety about labor | Worry about pain, complications, hospital stay |
| Fear of parenthood | Will I be a good mother? Can I manage everything? |
| Impatience and irritability | Due to physical discomfort, fatigue, restlessness |
| Increased dependence on partner/family | May need emotional and physical support |
| Nesting behavior | Urge to prepare home and surroundings for baby (common in late pregnancy) |
🔷 Factors Influencing Psychological Response to Pregnancy:
| Factor | Influence |
|---|---|
| Planned vs unplanned pregnancy | Planned = more acceptance; Unplanned = denial, stress |
| Support system | Partner and family support improve psychological well-being |
| Socioeconomic status | Financial insecurity → stress and anxiety |
| Age and maturity | Teen pregnancy may bring more confusion; older women may have more pressure |
| Past pregnancy experience | Previous miscarriage or complications → increased worry |
| Cultural beliefs and expectations | May affect emotional response and behaviors |
🔷 Common Psychological Issues in Pregnancy:
| Condition | Features |
|---|---|
| Anxiety | Worry about baby, labor, parenting, finances |
| Depression | Low mood, sleep disturbance, poor appetite, fatigue, hopelessness |
| Pregnancy denial | Rare; woman doesn’t acknowledge pregnancy |
| Obsessive thoughts | About baby’s health, cleanliness, safety |
| Fear of labor (Tokophobia) | Can affect decision on delivery method (e.g., request for elective C-section) |
🔷 Role of Nurse and Midwife in Supporting Mental Health:
| Role | Responsibilities |
|---|---|
| Observer | Watch for signs of depression, anxiety, fear, or emotional withdrawal |
| Counselor | Provide nonjudgmental emotional support and listening |
| Educator | Teach normal psychological changes and coping strategies |
| Supporter | Encourage involvement of family or birth partner |
| Referrer | Refer to mental health professional if needed |
| Advocate | Ensure privacy, respect, and dignity for the pregnant woman |
🔷 Mental Health Screening Tools:
Used in ANC clinics to detect perinatal depression/anxiety:
- Edinburgh Postnatal Depression Scale (EPDS)
- PHQ-9 (Patient Health Questionnaire)
- GAD-7 (for anxiety disorders)
🔷 Psychological Preparation for Childbirth:
- Antenatal classes – to reduce fear and increase confidence
- Breathing exercises & relaxation techniques
- Involving birth partner in support
- Clarifying doubts about labor and hospital stay
- Empowering woman to make informed choices
🔷 Summary Table: Emotional Changes by Trimester
| Trimester | Key Emotions |
|---|---|
| 1st | Ambivalence, anxiety, mood swings |
| 2nd | Acceptance, bonding, emotional stability |
| 3rd | Fear, anticipation, restlessness |
Ante-natal care: I Trimester.
🤰 Antenatal Assessment.

🔷 Introduction:
Antenatal assessment is the systematic evaluation of a pregnant woman during her pregnancy (antenatal period) to ensure the well-being of both the mother and fetus, identify risk factors or complications, and provide timely interventions. It is an essential component of antenatal care (ANC).
It includes physical, psychological, and laboratory assessments at regular intervals throughout pregnancy.
🔷 Aims of Antenatal Assessment:
- Confirm and monitor progress of pregnancy
- Identify high-risk pregnancies (e.g., diabetes, hypertension)
- Monitor fetal growth and well-being
- Educate and prepare the mother for childbirth
- Prevent, detect, and manage complications early
🔷 Timing of Antenatal Visits (As per Indian Guidelines):
| Visit | Time |
|---|---|
| 1st visit | Within 12 weeks (preferably as soon as pregnancy is suspected) |
| 2nd visit | Between 14–26 weeks |
| 3rd visit | Between 28–34 weeks |
| 4th visit | After 36 weeks (or more frequent if high-risk) |
Minimum 4 visits are essential (WHO recommends 8 for better outcomes).
🔷 Components of Antenatal Assessment:
✅ 1️⃣ History Collection
a. Personal History
- Name, age, address, education, occupation
- Diet, lifestyle, substance use (smoking, alcohol)
b. Obstetric History (G-P-A-L)
- Gravida, para, abortions, live births
- Previous pregnancies, complications, mode of delivery
c. Menstrual History
- Last menstrual period (LMP)
- Expected date of delivery (EDD) using Naegele’s Rule: EDD = LMP + 9 months + 7 days
d. Medical & Surgical History
- Hypertension, diabetes, tuberculosis, asthma
- Previous surgeries (e.g., C-section, appendectomy)
e. Family History
- Genetic disorders, twin pregnancies, diabetes
f. Psychosocial History
- Support system, mental health, domestic violence
✅ 2️⃣ Physical Examination
| Examination | Purpose |
|---|---|
| General Appearance | Nutritional status, hygiene, anemia signs |
| Height & Weight | Assess BMI, monitor weight gain |
| Pallor | Indicates anemia |
| Jaundice/Cyanosis | Suggest liver or heart disease |
| Edema | Common in feet (normal), face (warning sign) |
| Pulse & BP | Detect hypertension/pre-eclampsia |
| Respiratory rate | Monitor for breathlessness or infection |
| Breast Examination | For symmetry, lumps, and nipple readiness for breastfeeding |
✅ 3️⃣ Abdominal Examination (from 16–20 weeks onward)
| Step | Description |
|---|---|
| Inspection | Shape, size, striae, fetal movements |
| Palpation | |
| – Fundal height: To assess fetal growth | |
| – Leopold’s maneuvers: To determine lie, presentation, and position | |
| Auscultation | Fetal Heart Sound (FHS) with fetoscope/Doppler (~120–160 bpm is normal) |
| Measurement | Fundal height in cm = roughly gestational age in weeks after 24 weeks |
✅ 4️⃣ Pelvic Examination (if indicated)
- Done in late pregnancy or when needed (e.g., bleeding, labor signs)
- Assess pelvic adequacy, cervix condition
✅ 5️⃣ Laboratory Investigations
| Test | Purpose |
|---|---|
| Hemoglobin (Hb%) | Detect anemia |
| Blood group & Rh | Prepare for complications like Rh incompatibility |
| Urine (Albumin/Sugar) | Screen for UTI, pre-eclampsia, diabetes |
| Blood sugar (FBS/PPBS or GCT) | Screen for gestational diabetes |
| HIV, HBsAg, VDRL | Screen for infections |
| Thyroid profile (TSH) | Screen for thyroid disorders |
| Ultrasound (USG) | Confirm gestational age, fetal anatomy, placental location |
✅ 6️⃣ Fetal Assessment
| Tool | Purpose |
|---|---|
| Ultrasound | Growth, amniotic fluid, anomalies |
| Fetal Heart Sound (FHS) | Reassure fetal well-being |
| Kick Count | Maternal monitoring of fetal movement (after 28 weeks) |
10 kicks in 12 hours = normal
✅ 7️⃣ Health Education & Counseling
| Topic | Importance |
|---|---|
| Nutrition | Balanced diet, iron/calcium-rich food |
| Rest and exercise | Importance of sleep, light physical activity |
| Danger signs | Bleeding, blurred vision, convulsions, severe headache |
| Personal hygiene | Vulval, breast care, clothing |
| Breastfeeding | Early initiation and exclusive breastfeeding |
| Birth preparedness | Transportation, delivery kit, place of delivery |
| Family support | Emotional and physical support from husband/family |
🔷 Documentation in Antenatal Card / MCP Card (Mother-Child Protection Card)
- All findings should be recorded systematically
- Helps in continuity of care and decision-making during delivery
🔷 Nurse/Midwife’s Role in Antenatal Assessment:
| Role | Responsibilities |
|---|---|
| Examiner | Conduct physical and abdominal exams |
| Monitor | Track vital signs, fetal growth, and well-being |
| Educator | Teach about nutrition, rest, hygiene, and danger signs |
| Counselor | Address anxiety, emotional needs, birth planning |
| Care provider | Provide supplements (IFA, calcium), TT immunization |
| Referrer | High-risk cases referred to medical officer or specialist |
🔷 Danger Signs to Watch During ANC:
🚨 Immediate referral required if woman reports:
- Vaginal bleeding
- Severe abdominal pain
- Swelling of face or hands
- Severe headache or blurred vision
- No fetal movement
- Convulsions or fever
📝 History Taking During Antenatal Assessment.
🔷 Introduction:
History taking is the first and most crucial step in antenatal assessment. It involves systematically collecting relevant information about the pregnant woman’s past and present health, lifestyle, obstetric history, and risk factors. A thorough history helps in:
- Identifying high-risk pregnancies
- Planning individualized antenatal care
- Establishing a trusting relationship with the mother
🔷 Objectives of History Taking:
- To confirm pregnancy and calculate gestational age
- To detect risk factors and complications
- To assess maternal and fetal well-being
- To plan further investigations and care
- To educate and prepare the woman for safe motherhood
🔷 Components of Antenatal History Taking:
✅ 1️⃣ Identifying Data:
| Information | Examples |
|---|---|
| Name | Full name of the woman |
| Age | In completed years |
| Address | For follow-up and home visits |
| Registration number | For hospital/clinic record |
| Religion & caste | May influence diet and beliefs |
| Marital status | Married/single/divorced |
| Date of registration | First antenatal visit date |
✅ 2️⃣ Chief Complaints:
Ask the woman about any current symptoms (e.g.):
- Missed periods
- Nausea/vomiting
- Breast tenderness
- Fatigue
- Vaginal discharge
- Abdominal pain
Also ask if she has no complaints, to record well-being.
✅ 3️⃣ Menstrual History:
| Element | Description |
|---|---|
| Age at menarche | Age at first period |
| Cycle regularity and duration | 28-day cycle, 4–5 days bleeding? |
| Last menstrual period (LMP) | To calculate EDD (Expected Date of Delivery) using Naegele’s Rule |
| Any menstrual problems | Heavy flow, dysmenorrhea, irregular periods |
✅ 4️⃣ Obstetric History (G-P-A-L)
| Symbol | Meaning |
|---|---|
| G (Gravida) | Total number of pregnancies (including current) |
| P (Para) | Number of deliveries after 20 weeks |
| A (Abortions) | Number of spontaneous or induced abortions (<20 weeks) |
| L (Living children) | Number of currently living children |
For each past pregnancy, ask about:
- Year of delivery
- Gestational age at delivery
- Mode of delivery (normal/C-section)
- Sex of baby and birth weight
- Any complications (e.g., PPH, preeclampsia, stillbirth)
✅ 5️⃣ Medical and Surgical History:
Ask about:
- Chronic illnesses: Hypertension, diabetes, asthma, epilepsy, tuberculosis, thyroid disorders
- Previous surgeries: C-section, myomectomy, appendectomy, etc.
- Allergies to drugs, food
- Medications currently being taken
✅ 6️⃣ Family History:
- Genetic diseases: Thalassemia, sickle cell, hemophilia
- Multiple births (twins/triplets)
- Diabetes, hypertension, epilepsy
- History of maternal deaths, congenital anomalies in the family
✅ 7️⃣ Personal History:
| Subsection | Includes |
|---|---|
| Dietary habits | Vegetarian/non-vegetarian, likes/dislikes, nutrition awareness |
| Appetite & sleep | Changes during pregnancy |
| Bowel and bladder | Constipation, urinary frequency |
| Addictions | Smoking, tobacco, alcohol (ask sensitively) |
| Occupation | Physical labor, workplace stress, exposure to chemicals |
| Exercise & rest | Routine activities and fatigue level |
| Travel history | Recent long journeys, malaria-endemic areas |
✅ 8️⃣ Psychosocial and Emotional History:
- Support from husband/family
- Fear, anxiety, mood swings
- History of domestic violence or stress
- Willingness to continue the pregnancy
- Cultural or spiritual beliefs about pregnancy
✅ 9️⃣ Immunization and Supplement History:
| Item | Record |
|---|---|
| TT vaccination | Number of doses, date |
| Iron/Folic Acid intake | Duration, compliance |
| Calcium supplements | Ongoing or planned |
| Deworming (Albendazole) | Taken in 2nd trimester? |
🔷 Documentation Tool: Antenatal/ANC Card or MCP Card
All findings should be documented in:
- Antenatal card at health facility
- Mother and Child Protection (MCP) card (India) for community tracking
🔷 Nurse/Midwife’s Role in History Taking:
| Role | Responsibilities |
|---|---|
| Listener | Encourage open communication and trust |
| Observer | Note verbal and non-verbal cues |
| Recorder | Accurately document findings |
| Educator | Start health education based on findings |
| Referrer | Identify high-risk pregnancies for early referral |
🔷 Red Flag Findings in History (High-Risk Indicators):
- Previous C-section or complicated delivery
- Chronic diseases (diabetes, hypertension)
- History of stillbirth, miscarriage
- Teenage (<18) or elderly (>35) pregnancy
- History of multiple pregnancies
- Bleeding or severe vomiting in current pregnancy
- No antenatal checkups till 2nd trimester
👩⚕️ Physical Examination During Antenatal Assessment.
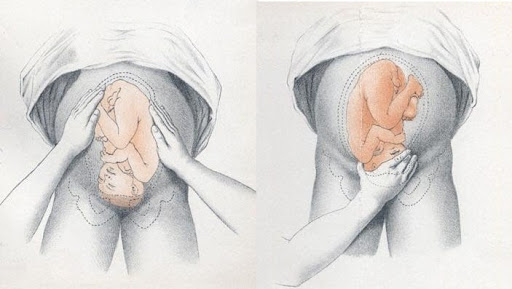
🔷 Introduction:
Physical examination during pregnancy is a systematic head-to-toe assessment of the expectant mother to evaluate her general health, detect physical changes, and monitor pregnancy progress. It helps in identifying high-risk conditions and ensures early interventions to promote safe motherhood and fetal well-being.
🔷 Objectives of Physical Examination:
- To establish baseline health status
- To detect signs of pregnancy and monitor progression
- To screen for complications (e.g., anemia, hypertension, edema)
- To assess maternal and fetal well-being
- To provide a basis for further care and investigations
🔷 Preparation Before Examination:
- Ensure privacy and good lighting
- Use clean, disinfected equipment (e.g., stethoscope, BP apparatus, weighing machine)
- Ask woman to empty bladder before abdominal exam
- Position her comfortably on a flat surface (supine or semi-Fowler’s)
- Ensure verbal consent and gentle approach
🔷 Components of Physical Examination:
✅ 1️⃣ General Appearance
| Observation | What to Look For |
|---|---|
| General health | Alertness, posture, fatigue |
| Hygiene | Personal cleanliness |
| Body build | Thin, average, obese |
| Facial expression | Anxious, pale, puffy (could indicate anemia or pre-eclampsia) |
| Gait | Normal or waddling gait (in late pregnancy) |
✅ 2️⃣ Vital Signs
| Parameter | Normal Range & Importance |
|---|---|
| Temperature | Normal or low-grade rise in early pregnancy |
| Pulse | ↑ 10–15 bpm is normal |
| Respiratory rate | Mild increase due to oxygen demand |
| Blood pressure | Should be <140/90 mmHg; elevated BP suggests pre-eclampsia |
✅ 3️⃣ Height and Weight
| Parameter | Use |
|---|---|
| Height | Short stature (<145 cm) may suggest cephalopelvic disproportion (CPD) risk |
| Weight | Monitor weight gain throughout pregnancy (normal gain: 11–16 kg for average BMI) |
✅ 4️⃣ Skin and Mucosa
| Observation | Significance |
|---|---|
| Pallor | Indicates anemia |
| Jaundice | May indicate liver disorder |
| Cyanosis | Suggests hypoxia |
| Edema | Normal in feet; facial or hand edema = warning sign |
| Skin pigmentation | Linea nigra, chloasma (normal) |
✅ 5️⃣ Head-to-Toe Examination
🔸 Head and Scalp
- Hair texture, dandruff, lice
- Headaches → may indicate pre-eclampsia
🔸 Eyes
- Pale conjunctiva → anemia
- Blurred vision → possible pre-eclampsia
- Pupil response, sclera (for jaundice)
🔸 Ears, Nose, Throat
- Check for nasal congestion (common), throat infections
🔸 Mouth and Gums
- Bleeding gums → due to estrogen
- Oral hygiene status
- Dental caries → risk of infection
✅ 6️⃣ Neck and Thyroid
| What to Assess | Importance |
|---|---|
| Thyroid enlargement | Mild is normal; significant swelling suggests hyper/hypothyroidism |
| Neck nodes | Enlarged lymph nodes may indicate infection |
✅ 7️⃣ Breast Examination
| What to Check | Significance |
|---|---|
| Size, symmetry | Enlarges during pregnancy |
| Areola and nipple | Darkening, Montgomery’s tubercles (normal), inverted nipples (may affect breastfeeding) |
| Colostrum secretion | Begins ~16 weeks onward |
| Lumps or masses | Should be ruled out for breast conditions |
✅ 8️⃣ Abdominal Examination (after ~16–20 weeks gestation)
| Step | Purpose |
|---|---|
| Inspection | Look for size, shape, fetal movement, scars, stretch marks |
| Palpation | Fundal height (in cm ≈ gestational age in weeks after 24 weeks) |
| Leopold’s maneuvers to assess: | |
| – Fundal presentation | |
| – Fetal lie | |
| – Position | |
| – Engagement | |
| Auscultation | Fetal heart sound (FHS): Normal = 120–160 bpm |
✅ 9️⃣ Pelvic Examination (only when indicated)
| Component | Use |
|---|---|
| Perineum | Check for hygiene, infections, varicosities |
| Vaginal exam | Performed in 3rd trimester or if complications arise (e.g., bleeding) |
| Assesses cervical effacement, dilation, and pelvic adequacy |
✅ 🔟 Extremities and Spine
| Observation | Significance |
|---|---|
| Edema | Pitting/non-pitting, localized or generalized |
| Varicose veins | In legs or vulva |
| Spinal curvature | Lordosis due to growing uterus |
| Clonus/reflexes | Hyperreflexia may suggest pre-eclampsia |
🔷 Common Abnormal Findings to Monitor:
| Finding | Possible Cause |
|---|---|
| Severe pallor | Moderate/severe anemia |
| Facial puffiness & hand swelling | Pre-eclampsia |
| High BP | Gestational hypertension |
| Absent FHS | Intrauterine fetal death |
| Excessive weight gain (>2 kg/month) | Risk of PIH or pre-eclampsia |
🔷 Nurse/Midwife’s Role in Physical Examination:
| Role | Responsibility |
|---|---|
| Assessor | Conduct the full head-to-toe and obstetric exam |
| Educator | Explain normal vs. warning signs to the woman |
| Supporter | Ensure privacy, comfort, and dignity during the exam |
| Referrer | Refer to medical officer if abnormal signs are detected |
| Recorder | Document all findings in ANC/MCP card accurately |
🩺 Breast Examination During Pregnancy.

🔷 Introduction:
Breast examination is a vital part of the physical examination during pregnancy, as it helps to assess the mother’s readiness for breastfeeding, identify abnormal findings, and educate her on breast care and lactation.
Performed during antenatal visits (preferably early in pregnancy and again later), this examination also builds the foundation for successful early initiation of breastfeeding.
🔷 Objectives of Breast Examination:
- Assess breast development and changes in pregnancy
- Identify conditions that may affect breastfeeding (e.g., inverted nipples)
- Detect any abnormalities, lumps, infections
- Educate mother on breast hygiene and care
- Promote confidence in breastfeeding and early lactation practices
🔷 Timing of Breast Examination:
- Initial examination: During the first antenatal visit
- Follow-up: During third trimester or if any complaints arise (pain, discharge, lumps)
🔷 Preparation for Breast Examination:
- Explain the procedure to the woman and take verbal consent
- Provide privacy and ensure a comfortable, warm room
- Ask the woman to lie down or sit with her upper clothing removed
- Ensure warm hands, clean gloves if needed
🔷 Steps of Breast Examination:
✅ 1️⃣ Inspection (Look)
Observe both breasts in the following positions:
- Arms by the side
- Hands on hips
- Arms raised above the head
| What to Look For | Significance |
|---|---|
| Size and symmetry | Mild asymmetry is normal; marked difference may need attention |
| Shape | Normal round/pendulous or flat |
| Skin changes | Redness, dimpling, shiny skin, peau d’orange (orange peel appearance = cancer suspicion) |
| Veins | May be more prominent in pregnancy (normal) |
| Areola and nipples | Darkening, enlargement (normal) |
| Montgomery’s tubercles | Raised sebaceous glands on areola – normal during pregnancy |
✅ 2️⃣ Palpation (Feel)
Ask the woman to lie on her back with one arm behind her head.
| Step | Description |
|---|---|
| Palpate each breast | Using flat fingers in a circular or up-down motion from outer to inner breast |
| Check all quadrants | Especially upper outer quadrant (common site of breast lumps) |
| Feel for lumps, masses | Note size, mobility, tenderness, borders |
| Check axillary (underarm) area | For lymph nodes (swollen nodes may indicate infection or malignancy) |
| Check nipple discharge | Squeeze gently – colostrum (thick yellow) may be seen after 16 weeks (normal) |
Bloody or purulent discharge is abnormal
✅ 3️⃣ Assess Nipple Type:
| Type | Effect on Breastfeeding |
|---|---|
| Normal/Protruding | Good for feeding |
| Flat | May need exercises/stimulation |
| Inverted | May make latching difficult → needs early correction |
Test for Inverted Nipple (Pinch Test):
Gently pinch the areola – if nipple retracts inward → inverted nipple.
🔷 Common Normal Breast Changes During Pregnancy:
| Change | Description |
|---|---|
| Breast enlargement | Due to hormonal effects (estrogen, progesterone, prolactin) |
| Areola darkening | Due to increased melanin |
| Increased tenderness | Especially in early pregnancy |
| Colostrum secretion | May start by 2nd trimester |
| Visible veins | Due to increased blood flow |
🔷 Abnormal Findings to Report or Refer:
- Hard, fixed lumps
- Painful swelling or redness
- Cracked, bleeding nipples
- Discharge that is bloody or foul-smelling
- Peau d’orange appearance
- Rapid nipple retraction or ulceration
🔷 Breast Care Advice for Pregnant Women:
| Advice | Purpose |
|---|---|
| Wash breasts daily with plain water | Keep nipples clean and infection-free |
| Avoid strong soaps or scrubbing | Prevent dryness and cracking |
| Wear a supportive cotton bra | Prevent sagging and reduce discomfort |
| Practice nipple rolling/stretching | For flat or inverted nipples (if needed) |
| Report any pain, lump, or discharge | Early detection of infection or issues |
| Learn about early initiation and exclusive breastfeeding | For successful lactation |
🔷 Role of Nurse and Midwife:
| Role | Responsibility |
|---|---|
| Examiner | Conduct proper and gentle breast exam |
| Educator | Teach about breast care and feeding techniques |
| Supporter | Prepare mother emotionally for breastfeeding |
| Referrer | In case of abnormal findings or feeding issues |
| Advocate | Promote early breastfeeding and skin-to-skin contact after birth |
🧪 Laboratory Investigations During Pregnancy.
🔷 Introduction:
Laboratory investigations during pregnancy are a crucial part of antenatal care (ANC). They help in the early detection and management of medical, nutritional, and infectious conditions that may affect the health of the mother and fetus.
These tests are done during the first visit and repeated as per clinical need or protocol, especially in high-risk pregnancies.
🔷 Aims of Laboratory Investigations:
- Confirm pregnancy and monitor progress
- Detect anemia, infections, gestational diabetes, and Rh incompatibility
- Assess renal, hepatic, and thyroid function if needed
- Screen for congenital infections and STDs
- Identify high-risk conditions early
🔷 Essential Lab Investigations During Pregnancy:
| Test | Purpose / Interpretation |
|---|
✅ 1️⃣ Hemoglobin (Hb%)
- Detects anemia
- Normal value in pregnancy: ≥11 g/dL
- <11 g/dL → mild anemia, <7 g/dL → severe anemia
✅ 2️⃣ Blood Grouping and Rh Typing
- Detects ABO and Rh incompatibility
- If mother is Rh-negative and father is Rh-positive, risk of isoimmunization
- May require anti-D immunoglobulin (Rhogam)
✅ 3️⃣ Urine Examination
a. Urine Routine & Microscopy
- Check for albumin (proteinuria → may suggest pre-eclampsia)
- Sugar (glycosuria → may suggest gestational diabetes)
- Pus cells (UTI)
b. Urine Culture
- If symptomatic or bacteriuria suspected
- Important to prevent pyelonephritis or preterm labor
✅ 4️⃣ Blood Sugar Testing
a. Random Blood Sugar (RBS)
b. Fasting Blood Sugar (FBS)
c. Oral Glucose Tolerance Test (OGTT / GCT)
- Done between 24–28 weeks
- To screen for gestational diabetes mellitus (GDM)
- Normal fasting sugar: <95 mg/dL; 2-hr post-glucose <140 mg/dL
✅ 5️⃣ VDRL Test (Venereal Disease Research Laboratory)
- Detects syphilis (a sexually transmitted disease)
- Positive cases are treated with penicillin to prevent fetal infection
✅ 6️⃣ HIV Test (with Pre- and Post-Counseling)
- Mandatory under PPTCT (Prevention of Parent-To-Child Transmission) program
- Helps plan ARV therapy and safe delivery if positive
✅ 7️⃣ HBsAg (Hepatitis B Surface Antigen)
- To detect hepatitis B infection
- Positive mothers → newborn must receive HBV vaccine + immunoglobulin at birth
✅ 8️⃣ Thyroid Function Test (TSH, T3, T4)
- Especially important in areas with iodine deficiency or if symptoms present
- Hypothyroidism → risk of fetal brain development issues
- Normal TSH in first trimester: ~0.1–2.5 mIU/L
✅ 9️⃣ Sickling Test / Hemoglobin Electrophoresis
- For detecting sickle cell anemia or thalassemia trait
- Done if there’s family history or regional risk (tribal areas)
✅ 🔟 TORCH Screening (if indicated)
Includes testing for:
- Toxoplasmosis
- Others (Hepatitis B, Syphilis, HIV)
- Rubella
- Cytomegalovirus (CMV)
- Herpes simplex virus
→ Only done if history of recurrent abortions, congenital anomalies, or IUGR
✅ 1️⃣1️⃣ COVID-19 Testing (As per current local guidelines)
🔷 Optional/Additional Tests (Based on Risk or Symptoms):
| Test | Reason |
|---|---|
| Liver Function Test (LFT) | If cholestasis, jaundice, or pre-eclampsia suspected |
| Renal Function Test (RFT) | If hypertension, proteinuria |
| Serum Ferritin | If severe anemia |
| Ultrasound (USG) | Early dating scan, anomaly scan, fetal well-being |
| Pap Smear | If not done in last 3 years |
🔷 When Are Tests Repeated?
| Test | Frequency |
|---|---|
| Hemoglobin | At booking, 24–28 weeks, and 36 weeks |
| Blood sugar | Between 24–28 weeks or earlier if high-risk |
| Urine routine | Every ANC visit or monthly |
| HIV/VDRL/HBsAg | Once during pregnancy, or more if indicated |
🔷 Nurse/Midwife’s Role in Lab Investigations:
| Role | Responsibilities |
|---|---|
| Educator | Explain importance of tests to mother |
| Counselor | Provide pre/post-test counseling (HIV, VDRL) |
| Sample collector | Collect or assist in proper sample collection |
| Recorder | Document results in ANC card / MCP card |
| Referrer | Notify doctor if abnormal results are found |
| Follow-up | Ensure repeat testing or treatment as required |
🔷 Documentation:
All test results must be recorded clearly in:
- ANC Register
- Mother and Child Protection (MCP) Card
- Hospital or PHC Records
🔷 Summary Table: Key Lab Investigations
| Test | Purpose |
|---|---|
| Hb% | Detect anemia |
| Blood Group & Rh | Identify incompatibility |
| Urine Routine | Detect protein, sugar, UTI |
| Blood Sugar (GCT/OGTT) | Screen for gestational diabetes |
| VDRL | Detect syphilis |
| HIV | For PPTCT management |
| HBsAg | Screen for hepatitis B |
| TSH | Assess thyroid function |
| USG | Confirm gestational age, anomalies |
🤰🩺 Identification and Management of Minor Discomforts of Pregnancy.
🔷 Introduction:
During pregnancy, women experience a variety of minor physiological discomforts due to hormonal changes, anatomical adaptations, and mechanical pressure from the growing fetus.
These discomforts are common and usually not dangerous, but they can affect a pregnant woman’s quality of life, sleep, and emotional well-being.
Midwives and nurses must:
- Identify them early
- Provide non-pharmacological remedies
- Educate the woman about normal vs. warning signs
🔷 Common Minor Discomforts of Pregnancy – Trimester-wise:
✅ 1️⃣ First Trimester Discomforts (0–12 weeks):
| Discomfort | Cause | Management |
|---|---|---|
| Nausea and vomiting (morning sickness) | hCG, estrogen, gastric sensitivity | Small frequent meals, avoid spicy/oily foods, dry toast/crackers in morning, drink fluids between meals |
| Breast tenderness | Hormonal changes (estrogen, progesterone) | Wear supportive bra, avoid tight clothing |
| Frequent urination | Pressure of uterus on bladder | Encourage fluid intake; avoid caffeine; empty bladder regularly |
| Fatigue | Hormonal changes, increased BMR | Rest, adequate sleep, iron-rich diet |
| Mood swings | Hormonal changes, stress | Emotional support, relaxation techniques |
✅ 2️⃣ Second Trimester Discomforts (13–28 weeks):
| Discomfort | Cause | Management |
|---|---|---|
| Heartburn (acid reflux) | Relaxed LES (progesterone) + uterine pressure | Eat small meals, avoid lying flat after meals, avoid spicy/fried food, elevate head while sleeping |
| Constipation | ↓ peristalsis, iron supplements | High-fiber diet, warm water, light exercise, stool softeners if prescribed |
| Flatulence/bloating | Hormonal + slow digestion | Avoid gas-forming foods, eat slowly, light walking |
| Backache | Weight gain, postural changes, lordosis | Good posture, pelvic tilt exercises, support belt, rest |
| Varicose veins | Increased venous pressure, hormones | Elevate legs, avoid prolonged standing, use support stockings |
| Skin changes (e.g., melasma, linea nigra, itching) | Increased melanin, estrogen | Reassurance, avoid harsh soaps, moisturize skin, sunscreen for melasma |
✅ 3️⃣ Third Trimester Discomforts (29–40 weeks):
| Discomfort | Cause | Management |
|---|---|---|
| Shortness of breath | Diaphragm pushed up by uterus | Sit upright, sleep with extra pillow, avoid tight clothes |
| Ankle/leg edema | Fluid retention, pressure on veins | Rest with legs elevated, avoid prolonged standing, hydration |
| Leg cramps | Mineral deficiency, poor circulation | Calf-stretching, massage, increase calcium & magnesium |
| Insomnia | Anxiety, discomfort | Sleep hygiene, warm bath before bed, left-side lying |
| Frequent urination | Fetal head pressing on bladder | Reassurance, fluid restriction at bedtime |
| Braxton-Hicks contractions | Uterine muscle practice | Normal unless regular/painful; rest, hydration, observe pattern |
| Hemorrhoids (piles) | Constipation, pelvic pressure | High-fiber diet, sitz bath, avoid straining, prescribed ointments |
🔷 General Guidelines for Managing Discomforts:
- Educate the mother on expected normal changes
- Encourage healthy diet and hydration
- Promote regular antenatal exercises
- Emphasize personal hygiene and rest
- Offer emotional reassurance and support
- Identify when to refer (in case discomfort turns into danger sign)
🔷 Danger Signs Needing Referral (Not Minor Discomforts):
| Symptom | May Indicate |
|---|---|
| Vaginal bleeding | Threatened abortion or placenta previa |
| Severe headache, blurred vision | Pre-eclampsia |
| Painful contractions before 37 weeks | Preterm labor |
| Decreased fetal movements | Fetal distress |
| Severe abdominal pain | Ectopic pregnancy or placental abruption |
| Persistent vomiting | Hyperemesis gravidarum |
🔷 Role of Nurse and Midwife:
| Role | Responsibility |
|---|---|
| Observer | Identify and assess discomforts |
| Educator | Teach self-care, posture, nutrition, warning signs |
| Supporter | Provide emotional reassurance |
| Care provider | Give remedies, monitor response |
| Referrer | If symptoms worsen or danger signs appear |
🤰🗣️ Antenatal Care and Counseling (Lifestyles in Pregnancy).
🔷 Introduction:
Antenatal care (ANC) is the care provided to a pregnant woman from the time of conception until the onset of labor. It includes routine checkups, screening, health education, counseling, and support to ensure the well-being of both mother and fetus.
A major part of ANC is counseling the mother about healthy lifestyle practices, which helps in preventing complications, promoting positive pregnancy outcomes, and empowering women to take charge of their health.
🔷 Objectives of Antenatal Care and Lifestyle Counseling:
- Promote healthy behavior during pregnancy
- Prevent maternal and fetal complications
- Ensure proper fetal growth and development
- Educate women about pregnancy changes and self-care
- Prepare the woman for labor, delivery, breastfeeding, and motherhood
- Detect and manage high-risk conditions early
🔷 Core Components of ANC Counseling on Lifestyle in Pregnancy:
✅ 1️⃣ Nutrition and Diet Counseling
| Aspect | Counseling Tips |
|---|---|
| Balanced diet | Teach about including cereals, pulses, vegetables, fruits, dairy, meat (if non-veg), and healthy fats |
| Calorie intake | Increase by ~300 kcal/day in 2nd and 3rd trimesters |
| Protein | Minimum 60–70 gm/day; crucial for fetal growth |
| Iron & Folic acid | Promote iron-rich foods (green leafy veg, jaggery, dates); counsel on IFA tablets (100 mg iron + 0.5 mg folic acid) |
| Calcium | Advise calcium-rich foods and supplements |
| Hydration | At least 8–10 glasses/day |
| Avoid | Junk food, excess salt/sugar, unpasteurized dairy, raw meat, and caffeine |
✅ 2️⃣ Rest, Sleep, and Physical Activity
| Aspect | Counseling Tips |
|---|---|
| Rest | Minimum 8 hours of night sleep + 1–2 hrs of daytime rest |
| Position | Encourage left-side lying in later pregnancy for better uterine blood flow |
| Exercise | Moderate walking, antenatal yoga, pelvic tilts; avoid heavy lifting or risky activities |
| Avoid prolonged standing or sitting | Encourage position changes, stretching |
✅ 3️⃣ Personal Hygiene
| Aspect | Counseling Tips |
|---|---|
| Daily bathing | To prevent skin infections, maintain cleanliness |
| Genital hygiene | Use clean, dry undergarments; wipe front to back |
| Breast care | Gentle cleaning with water, avoid harsh soaps, wear supportive bras |
| Oral hygiene | Brush twice daily, dental check-up if needed |
| Hair and nails | Keep clean and trimmed |
✅ 4️⃣ Clothing and Footwear
| Aspect | Counseling Tips |
|---|---|
| Clothing | Loose, breathable cotton clothes; avoid tight wear |
| Footwear | Low-heeled, non-slippery shoes; avoid heels and tight shoes to reduce fall risk and swelling |
✅ 5️⃣ Sexual Activity
| Advice | Counseling Tips |
|---|---|
| Safe in normal pregnancy | With comfortable positions and hygiene |
| Avoid | If history of miscarriage, bleeding, placenta previa, or ruptured membranes |
✅ 6️⃣ Avoidance of Harmful Substances
| Substance | Counseling Message |
|---|---|
| Tobacco | Increases risk of low birth weight, miscarriage, stillbirth |
| Alcohol | Can cause fetal alcohol syndrome (mental & physical defects) |
| Drugs | Avoid self-medication; many are teratogenic |
| Caffeine | Limit tea/coffee to <2 cups/day |
✅ 7️⃣ Mental and Emotional Health
| Counseling Focus | Tips |
|---|---|
| Emotional changes are normal | Due to hormones, body changes |
| Encourage family support | Especially from husband |
| Teach stress management | Deep breathing, meditation, rest |
| Identify signs of depression/anxiety | Refer if needed |
✅ 8️⃣ Immunization Advice
| Vaccine | When |
|---|---|
| Tetanus & Diphtheria (TT/TD) | 2 doses: First as early as possible, second after 4 weeks |
| COVID-19 vaccine (as per policy) | If not completed earlier |
| Influenza vaccine (if recommended) | To protect mother and newborn |
✅ 9️⃣ Supplementation Counseling
| Supplement | Advice |
|---|---|
| Iron & Folic Acid (IFA) | 1 tablet daily after 1st trimester for 180 days |
| Calcium | 2 tablets daily from 2nd trimester onwards |
| Deworming | Albendazole 400 mg once after 12 weeks if indicated |
✅ 🔟 Travel and Work Advice
| Topic | Counseling Tips |
|---|---|
| Travel | Avoid long, bumpy rides; use seat belts below the belly |
| Work | Safe to work unless complications; avoid standing too long or heavy lifting |
| Maternity leave | Explain benefits and legal rights |
✅ 1️⃣1️⃣ Danger Signs Counseling
Educate about warning signs that require immediate medical attention:
🚨 Red flags:
- Vaginal bleeding
- Severe headache or blurred vision
- Convulsions
- Fever
- Severe abdominal pain
- Reduced fetal movement
- Swelling of hands/face
🔷 Role of Nurse/Midwife in Counseling:
| Role | Responsibility |
|---|---|
| Educator | Provide accurate lifestyle and health education |
| Supporter | Offer emotional reassurance |
| Advocate | Promote healthy practices in home and community |
| Communicator | Use culturally sensitive, easy-to-understand language |
| Referrer | Identify and refer for special counseling or complications |
🥗🤰 Nutrition in Pregnancy.
🔷 Introduction:
Nutrition during pregnancy plays a crucial role in ensuring the health of the mother and fetus. Adequate and balanced nutrition promotes:
- Normal fetal growth and development
- Reduced complications in pregnancy and childbirth
- Enhanced maternal strength and postpartum recovery
- Better outcomes in lactation and newborn health
Pregnant women have increased needs for energy, proteins, vitamins, and minerals, especially in the 2nd and 3rd trimesters.
🔷 Goals of Nutrition in Pregnancy:
- Ensure appropriate weight gain
- Prevent anemia, low birth weight, and congenital defects
- Maintain maternal immunity and energy
- Prepare for breastfeeding
- Prevent nutritional deficiencies and malnutrition
🔷 Daily Nutritional Requirements During Pregnancy:
| Nutrient | Recommended Increase | Sources |
|---|---|---|
| Calories | +300 kcal/day (2nd & 3rd trimester) | Cereals, pulses, dairy, fruits |
| Protein | 60–70 g/day | Milk, eggs, meat, legumes, soy, paneer |
| Iron | 40–60 mg/day | Green leafy vegetables, dates, jaggery, liver, IFA tablets |
| Folic Acid | 0.5 mg/day | Leafy greens, nuts, citrus fruits, supplements |
| Calcium | 1200–1500 mg/day | Milk, curd, cheese, ragi, sesame |
| Iodine | 250 mcg/day | Iodized salt, seafood |
| Vitamin A | 800 mcg/day | Carrots, mango, pumpkin, liver |
| Vitamin C | 80 mg/day | Amla, citrus fruits, tomatoes |
| Zinc | 12 mg/day | Whole grains, meat, nuts |
🔷 Weight Gain in Pregnancy:
| Pre-pregnancy BMI | Recommended Weight Gain |
|---|---|
| Underweight (<18.5) | 12.5–18 kg |
| Normal (18.5–24.9) | 11.5–16 kg |
| Overweight (25–29.9) | 7–11.5 kg |
| Obese (>30) | 5–9 kg |
🔸 Weight gain should be gradual:
- ~1–2 kg in 1st trimester
- ~0.5 kg/week in 2nd and 3rd trimesters
🔷 Principles of Healthy Eating During Pregnancy:
- Eat a balanced diet including all food groups
- Include small frequent meals (5–6 times/day) to avoid nausea and heartburn
- Drink at least 8–10 glasses of water per day
- Avoid skipping meals, especially breakfast
- Choose fresh, home-cooked food
- Ensure clean and safe food handling to avoid infections
🔷 Special Considerations:
| Condition | Dietary Advice |
|---|---|
| Nausea/Vomiting | Dry crackers, small meals, avoid spicy/fatty foods |
| Constipation | High fiber diet, fruits, vegetables, warm water |
| Heartburn | Small frequent meals, avoid lying down after eating |
| Vegetarians | Ensure protein from pulses, soy, nuts, dairy |
| Underweight mothers | High-energy snacks: banana, nuts, peanut butter |
| Overweight mothers | Avoid junk food, sweets; opt for light, low-fat meals |
🔷 Foods to Encourage:
✅ Whole grains
✅ Leafy greens (spinach, fenugreek)
✅ Milk and milk products
✅ Seasonal fruits (banana, papaya, guava, orange)
✅ Eggs, fish, lean meat
✅ Nuts and seeds (almonds, sesame, flax)
🔷 Foods to Avoid:
🚫 Raw/undercooked meat, eggs
🚫 Unpasteurized milk or cheese
🚫 Excess caffeine (>2 cups/day)
🚫 Alcohol, smoking, tobacco
🚫 Junk/fast food, excess salt/sugar
🚫 Papaya and pineapple in early pregnancy (controversial; better to avoid)
🔷 Iron and Folic Acid Supplementation:
As per Indian guidelines:
- IFA tablets: 1 tablet daily after 1st trimester (100 mg elemental iron + 0.5 mg folic acid) for 180 days
- Continue post-delivery for 180 days more
- Take after meals with water (not tea/milk)
🔷 Calcium Supplementation:
- 2 tablets/day of 500 mg calcium from 2nd trimester onward
- Taken separately from iron tablets (e.g., iron in morning, calcium at night)
🔷 Nutrition Education by Nurse/Midwife:
| Role | Responsibilities |
|---|---|
| Educator | Explain nutritional needs and healthy food choices |
| Counselor | Handle food taboos, cultural practices, poor appetite |
| Motivator | Encourage compliance with supplements |
| Observer | Monitor weight gain, signs of deficiency |
| Referrer | For nutritionist support if severely undernourished or obese |
🔷 Pregnancy Nutrition Counseling Tips:
🔹 Use the “Rainbow plate” concept – variety of colors = variety of nutrients
🔹 Involve family members in counseling for better support
🔹 Address myths and misconceptions (e.g., “eat for two”)
🔹 Explain importance of exclusive breastfeeding preparation.
🤝 Shared Decision-Making (SDM) in Antenatal and Maternity Care.
🔷 Introduction:
Shared Decision-Making (SDM) is a collaborative process in which the pregnant woman and the health care provider (nurse, midwife, or doctor) work together to make decisions about her care, based on:
- The best available medical evidence,
- The woman’s preferences, values, needs, and
- Her individual context (social, emotional, cultural).
It empowers women to actively participate in their pregnancy care and strengthens respectful maternity care (RMC).
🔷 Definition:
Shared decision-making is a patient-centered approach where clinical decisions are made jointly by the health care provider and the pregnant woman, taking into account both clinical evidence and the woman’s informed preferences.
🔷 Key Principles of SDM:
- Respect for woman’s autonomy
- Two-way communication
- Mutual respect and trust
- Informed choice with unbiased information
- Partnership in care planning
🔷 Steps of Shared Decision-Making:
| Step | Description |
|---|---|
| 1. Introduce Choice | Let the woman know she has a say in her care (e.g., “There are different options available…”) |
| 2. Explain Options | Present risks, benefits, alternatives in simple language |
| 3. Explore Preferences | Ask about her values, fears, expectations (e.g., natural birth vs. C-section) |
| 4. Support Decision | Guide without pressure; use visuals, pamphlets if needed |
| 5. Confirm and Plan | Respect her choice, document it, and develop a care plan together |
🔷 Examples of Shared Decision-Making in Maternity Care:
| Situation | Choices Involved |
|---|---|
| Birth Plan | Natural birth, epidural, water birth, home vs. hospital |
| Mode of Delivery | VBAC (vaginal birth after cesarean) vs. elective C-section |
| Pain Relief | Breathing exercises, epidural, TENS, natural methods |
| Labor Induction | Induction vs. expectant management |
| Feeding Options | Breastfeeding vs. formula (if medical issues) |
| Vaccinations | COVID-19 or influenza vaccine in pregnancy |
| Antenatal Testing | Whether or not to do non-invasive prenatal testing (NIPT), amniocentesis |
🔷 Benefits of Shared Decision-Making:
✅ Increases maternal satisfaction and trust
✅ Improves compliance with care
✅ Reduces anxiety and fear
✅ Respects cultural and personal values
✅ Builds partnership and respectful care
✅ Helps in risk understanding and realistic expectations
🔷 Barriers to SDM in Maternity Care:
| Barrier | Solution |
|---|---|
| Low literacy or language barriers | Use pictures, interpreters, simple words |
| Power imbalance | Midwife must create a safe, respectful space |
| Lack of time in busy OPDs | Prioritize key decisions, schedule follow-up |
| Cultural factors | Respect beliefs while gently explaining evidence |
| Provider bias | Stay neutral and avoid judgment in counseling |
🔷 Role of Nurse/Midwife in SDM:
| Role | Responsibilities |
|---|---|
| Educator | Provide clear, unbiased information about all options |
| Facilitator | Create a respectful, open environment |
| Supporter | Encourage questions, validate concerns |
| Advocate | Ensure woman’s choice is respected by the team |
| Communicator | Document decisions in ANC card or birth plan |
| Empowerer | Help woman understand her rights and voice them confidently |
🔷 Tools to Support SDM:
- Decision aids (charts, comparison tables)
- Visual guides (infographics, videos)
- Printed leaflets or booklets
- Birth plan templates
- Checklists for preferences
⚠️ Risky Behaviors in Pregnancy.
🔷 Introduction:
Certain lifestyle behaviors or exposures during pregnancy are considered risky because they can harm the mother, fetus, or both. These behaviors increase the chances of complications such as miscarriage, birth defects, preterm labor, low birth weight, and even stillbirth.
Midwives and nurses play a vital role in identifying, counseling, and supporting women to avoid or stop such behaviors during antenatal care.
🔷 Definition:
Risky behaviors in pregnancy are actions, habits, or exposures that negatively impact maternal and fetal health and increase the risk of poor pregnancy outcomes.
🔷 Common Risky Behaviors During Pregnancy:
✅ 1️⃣ Smoking (Tobacco Use)
| Impact | Effects |
|---|---|
| 🚬 Smoking (cigarettes, bidi, hookah) or chewing tobacco | Causes intrauterine growth restriction (IUGR), placental abruption, low birth weight, preterm labor, stillbirth, sudden infant death syndrome (SIDS) |
| 🔹 Passive smoking is also harmful | |
| 🔸 Reduces oxygen supply to fetus due to carbon monoxide exposure |
✅ 2️⃣ Alcohol Consumption
| Impact | Effects |
|---|---|
| 🍷 Even small amounts of alcohol during pregnancy are unsafe | |
| May cause Fetal Alcohol Spectrum Disorders (FASD): | |
| – Mental retardation | |
| – Facial deformities | |
| – Behavioral issues | |
| Leads to miscarriage, stillbirth, poor neurodevelopment |
✅ 3️⃣ Illicit Drug Use
| Drugs | Possible Effects |
|---|---|
| Cocaine, heroin, marijuana, methamphetamine | Miscarriage, premature birth, low birth weight, neonatal withdrawal syndrome (NAS), congenital anomalies, stillbirth |
| May also cause placental abruption, poor bonding, and neonatal addiction |
✅ 4️⃣ Excessive Caffeine Intake
| Risk | Recommendation |
|---|---|
| High caffeine (>200 mg/day) linked to miscarriage, low birth weight | |
| Limit to 1–2 cups of tea/coffee per day |
✅ 5️⃣ Unsafe Sexual Practices
| Behavior | Risk |
|---|---|
| Unprotected sex with multiple partners | Increases risk of STIs (HIV, Syphilis, Hepatitis B) that can be transmitted to fetus |
| Can lead to premature rupture of membranes, miscarriage, congenital infections |
✅ 6️⃣ Poor Nutrition or Eating Disorders
| Risk | Effect |
|---|---|
| Skipping meals, crash dieting, eating junk food | Leads to nutrient deficiencies, anemia, poor fetal growth |
| Eating disorders (anorexia, bulimia) worsen pregnancy outcomes |
✅ 7️⃣ Self-medication and Use of Unsafe Drugs
| Issue | Effect |
|---|---|
| Taking unprescribed medicines or herbal drugs | May cause birth defects, miscarriage |
| Some antibiotics, acne meds, painkillers (e.g., NSAIDs) are teratogenic |
✅ 8️⃣ Exposure to Environmental Hazards
| Risk | Examples |
|---|---|
| Chemical exposures at work or home (e.g., pesticides, paint, cleaning agents) | May affect fetal brain development, cause miscarriage |
| Radiation (X-rays) in early pregnancy | Can lead to congenital anomalies if unprotected |
✅ 9️⃣ Sedentary Lifestyle / Lack of Physical Activity
| Impact | Risk |
|---|---|
| Leads to excessive weight gain, gestational diabetes, back pain, poor circulation | |
| Moderate activity like walking or prenatal yoga is encouraged |
✅ 🔟 Stress and Mental Health Neglect
| Risk | Effects |
|---|---|
| Chronic stress, anxiety, depression | Increases risk of preterm labor, low birth weight, postpartum depression |
| Also affects mother-infant bonding and breastfeeding |
🔷 Nurse/Midwife’s Role in Preventing Risky Behaviors:
| Role | Responsibilities |
|---|---|
| Educator | Inform the woman and family about risks and healthy alternatives |
| Supporter | Provide emotional support and safe space to talk |
| Counselor | Address addiction, stress, family problems |
| Referrer | Refer to psychiatrist, de-addiction, or support groups if needed |
| Motivator | Encourage compliance with health-promoting behavior |
🔷 Effective Counseling Techniques:
- Use non-judgmental approach
- Build trust and rapport
- Use visual aids or real stories
- Involve family members in behavior change
- Use 5 A’s model: Ask, Advise, Assess, Assist, Arrange (follow-up)
🔷 Summary Table: Risky Behaviors and Consequences
| Behavior | Consequence |
|---|---|
| Smoking | Low birth weight, IUGR, stillbirth |
| Alcohol | Fetal alcohol syndrome |
| Drugs | Neonatal withdrawal, preterm birth |
| Unprotected sex | STIs, congenital infections |
| Poor diet | Anemia, fetal malnutrition |
| Self-medication | Birth defects |
| Caffeine excess | Miscarriage |
| Stress | Preterm labor |
| Lack of exercise | GDM, obesity |
💞 Counseling Regarding Sexual Life During Pregnancy.

🔷 Introduction:
Sexual activity is a normal and important part of a couple’s relationship, including during pregnancy. However, hormonal, emotional, and physical changes may affect a woman’s sexual desire and comfort. Many couples have concerns or misconceptions about sex during pregnancy, which can cause stress or avoidance.
Therefore, sexual counseling during antenatal care is essential for promoting healthy relationships, emotional bonding, and safe practices.
🔷 Objectives of Sexual Counseling During Pregnancy:
- To educate couples about the safety and normalcy of sex in pregnancy
- To reduce fear, guilt, or anxiety about intercourse
- To promote emotional closeness and communication
- To clarify when sex is safe or unsafe
- To address cultural beliefs, taboos, or myths
- To screen for and prevent sexually transmitted infections (STIs)
🔷 Physiological and Psychological Changes Affecting Sexual Life:
| Trimester | Changes in Sexual Desire |
|---|---|
| 1st trimester | ↓ due to nausea, fatigue, breast tenderness, mood swings |
| 2nd trimester | ↑ due to improved energy, increased blood flow to genitals |
| 3rd trimester | ↓ due to physical discomfort, back pain, anxiety about labor |
Partner’s understanding and emotional support are important throughout.
🔷 Is Sex Safe During Pregnancy?
✅ YES – In normal, low-risk pregnancies, sex is safe
- The baby is well protected in the uterus by the amniotic sac and strong uterine muscles
- The mucus plug in the cervix prevents infection
- Orgasms and penetration do not cause miscarriage in a healthy pregnancy
🔷 When to Avoid Sexual Intercourse (High-Risk Cases):
| Condition | Reason |
|---|---|
| History of miscarriage | Risk of recurrence |
| Placenta previa | Risk of bleeding |
| Preterm labor or contractions | May trigger early labor |
| Leaking of amniotic fluid (PROM) | Risk of infection |
| Vaginal bleeding or unexplained spotting | Requires investigation |
| Cervical insufficiency | Risk of early labor |
| Multiple pregnancy with complications | More cautious approach |
| Active sexually transmitted infection (STI) | Risk of transmission to fetus |
| Painful intercourse or discomfort | May require medical evaluation |
🔷 Counseling Topics for Couples:
✅ 1️⃣ Normalize the Conversation
- Assure them that many couples have similar concerns
- Use sensitive, non-judgmental language
- Create a private and supportive environment
✅ 2️⃣ Discuss Safe Practices
| Aspect | Tips |
|---|---|
| Positions | Encourage comfortable, non-pressure positions (e.g., side-lying, woman on top) especially in late pregnancy |
| Lubrication | Can be used if vaginal dryness occurs |
| Gentle intimacy | Kissing, cuddling, massage to maintain connection |
| Use protection if needed | Especially if partner has STIs or multiple partners |
✅ 3️⃣ Dispel Myths
| Myth | Reality |
|---|---|
| Sex harms the baby | Baby is safe in the womb unless complications exist |
| Sex causes miscarriage | Not in normal pregnancy |
| Sex should be stopped after 5th month | Not necessary unless advised by doctor |
| All women lose sexual desire | Changes vary—some may feel increased or decreased desire |
✅ 4️⃣ Promote Communication Between Partners
- Encourage open sharing of feelings
- Address changes in desire or body image
- Emphasize emotional closeness and mutual respect
🔷 Nurse/Midwife’s Role in Sexual Counseling:
| Role | Responsibility |
|---|---|
| Educator | Provide facts about sex and safety in pregnancy |
| Counselor | Address myths, fears, discomforts |
| Supporter | Promote communication and intimacy in couple |
| Referrer | Refer to doctor or psychologist if dysfunction, trauma, or STI is suspected |
| Advocate | Ensure privacy, dignity, and cultural sensitivity |
🔷 Counseling Tips:
- Use simple language
- Respect cultural and personal beliefs
- Avoid making assumptions about the couple’s sexual preferences
- Involve the partner, if appropriate and acceptable
- Provide written material or leaflets if available
- Always document the counseling session if part of antenatal education
🚨 Danger Signs During Pregnancy.
🔷 Introduction:
Pregnancy is generally a physiological process, but complications can arise at any time. Some symptoms, if not identified and treated early, can lead to serious maternal or fetal morbidity or mortality.
Therefore, it is vital to educate every pregnant woman and her family about the danger signs of pregnancy so they can seek immediate medical attention when necessary.
🔷 Definition:
Danger signs during pregnancy are symptoms or signs that indicate potential complications that can threaten the life of the mother, fetus, or both, and require immediate medical evaluation and intervention.
🔷 Major Danger Signs During Pregnancy (According to WHO and RCH Guidelines):
✅ 1️⃣ Vaginal Bleeding
| Possible Causes | Risks |
|---|---|
| Threatened abortion, placenta previa, placental abruption | Miscarriage, hemorrhage, fetal death |
🔸 Any amount of bleeding is abnormal during pregnancy and must be reported.
✅ 2️⃣ Severe Headache
| Possible Causes | Risks |
|---|---|
| Pre-eclampsia (pregnancy-induced hypertension) | Risk of seizures (eclampsia), stroke, fetal growth restriction |
✅ 3️⃣ Blurred Vision / Dimming of Vision / Spots Before Eyes
| Possible Cause | Risk |
|---|---|
| Pre-eclampsia | Indicates risk of seizures or cerebral edema |
✅ 4️⃣ Severe Abdominal Pain
| Possible Causes | Risks |
|---|---|
| Ectopic pregnancy, placental abruption, uterine rupture | Life-threatening bleeding, maternal shock |
✅ 5️⃣ Convulsions or Fits
| Possible Cause | Risk |
|---|---|
| Eclampsia | Maternal and fetal death if untreated |
✅ 6️⃣ High Fever with Chills
| Possible Causes | Risks |
|---|---|
| Malaria, urinary tract infection, sepsis | Preterm labor, maternal infection, fetal distress |
✅ 7️⃣ Loss of Fetal Movement (No Fetal Kicks After 28 Weeks)
| Significance | Action |
|---|---|
| May indicate fetal distress or intrauterine fetal death (IUFD) | Needs immediate fetal monitoring and ultrasound |
🔹 Normal fetal movement: 10 kicks in 12 hours
✅ 8️⃣ Swelling of Face, Hands, and Feet (Sudden or Severe)
| Possible Cause | Risk |
|---|---|
| Pre-eclampsia | May lead to seizures, low birth weight, preterm birth |
🔸 Mild leg swelling is common, but facial or hand edema is abnormal.
✅ 9️⃣ Leaking of Amniotic Fluid Before Labor (PROM)
| Significance | Risk |
|---|---|
| Indicates rupture of membranes before labor begins | Increases risk of infection, cord prolapse, preterm birth |
✅ 🔟 Painful or Regular Uterine Contractions Before 37 Weeks
| Significance | Risk |
|---|---|
| Suggests preterm labor | Premature delivery, neonatal complications |
✅ 1️⃣1️⃣ Difficulty in Breathing / Chest Pain / Palpitations
| Possible Causes | Risks |
|---|---|
| Severe anemia, cardiac disease, pulmonary embolism | Respiratory failure, fetal hypoxia |
🔷 Other Warning Signs:
| Sign | Possible Problem |
|---|---|
| Excessive vomiting | Hyperemesis gravidarum → dehydration, electrolyte imbalance |
| Itching all over body, especially palms/soles | Cholestasis of pregnancy (risk to fetus) |
| Burning urination | Urinary tract infection |
| Painful swollen legs | DVT (deep vein thrombosis) |
| Unconsciousness or confusion | Seizure, stroke, metabolic imbalance |
🔷 Immediate Action When Danger Signs Are Observed:
- Do NOT delay in seeking help
- Refer to the nearest healthcare facility/hospital
- Inform the ANM/ASHA worker for transportation or support
- Monitor vital signs if in clinical setting
- Record all symptoms and timings
🔷 Role of Nurse and Midwife:
| Role | Responsibilities |
|---|---|
| Educator | Teach every pregnant woman about these signs during antenatal care |
| Observer | Identify early danger signs during routine checkups |
| Supporter | Provide emotional and physical support during emergency |
| Referrer | Ensure timely referral to higher centers |
| Documenter | Record observations and interventions in ANC card or register |
🔷 Health Education Tips for Pregnant Women (in Simple Language):
👉 “If you have bleeding, swelling of face, no baby movement, or severe headache, go to hospital immediately.”
👉 Use flipcharts, posters, videos during ANC clinics
👉 Involve family members/husbands in education
👉 Use MCP Card to write and explain danger signs
👶👜 Birth Preparedness and Complication Readiness (BPCR).

🔷 Introduction:
Birth Preparedness and Complication Readiness (BPCR) is a key component of safe motherhood programs. It ensures that the pregnant woman, her family, and health care providers are well-prepared for normal delivery and are also ready to handle emergencies.
It promotes timely use of skilled maternal and neonatal care, especially during the critical time of labor, delivery, and the immediate postpartum period.
🔷 Definition:
BPCR is a strategy that helps a pregnant woman and her family to plan for a safe delivery and to be ready for any obstetric complications or emergencies that may arise before, during, or after childbirth.
🔷 Objectives of BPCR:
- To reduce maternal and neonatal morbidity and mortality
- To ensure skilled birth attendance
- To facilitate timely care-seeking in emergencies
- To empower women and families to take decisions
- To improve communication between families and health providers
🔷 Key Components of Birth Preparedness:
| Component | Description |
|---|---|
| ✅ Identify a skilled birth attendant | Doctor, nurse-midwife, or trained ANM |
| ✅ Choose a place of delivery | PHC, CHC, sub-center, hospital, private or government facility |
| ✅ Arrange transport | Know the nearest transport options, keep contact numbers ready |
| ✅ Save money | For transport, medicine, food, emergency care |
| ✅ Pack a birth kit | Clothes, sanitary pads, baby clothes, soap, towel, ID, MCP card |
| ✅ Arrange a birth companion | Someone to accompany the woman during labor |
| ✅ Prepare for home care after delivery | Clean room, rest arrangements, newborn care supplies |
| ✅ Ensure nutrition and rest | For energy during labor and recovery afterward |
🔷 Key Components of Complication Readiness:
| Component | Description |
|---|---|
| ✅ Know danger signs | Bleeding, high fever, convulsions, no fetal movement, severe headache, labor >12 hours |
| ✅ Identify nearest referral center | Where emergency obstetric and newborn care (EmONC) is available |
| ✅ Arrange emergency transport | Local driver, ambulance services (like 108 in India) |
| ✅ Have blood donor available | In case of hemorrhage, anemia, or C-section |
| ✅ Involve key decision-makers | Ensure family members are informed and supportive |
| ✅ Keep emergency contacts ready | Hospital, midwife, ASHA, ANM, local health worker |
🔷 WHO Recommended Danger Signs for Counseling (Antenatal and Postnatal):
🔴 During Pregnancy:
- Vaginal bleeding
- Severe headache
- Blurred vision
- Abdominal pain
- Swelling of face/hands
- High fever
- Loss of fetal movement
🔴 During Labor/Postpartum:
- Prolonged labor (>12 hours)
- Heavy vaginal bleeding
- Convulsions
- Retained placenta
- Foul-smelling vaginal discharge
- High fever
🔴 For Newborn:
- Difficulty breathing
- Poor feeding
- Cold or hot to touch
- Yellow skin (jaundice)
- Inactivity
🔷 Role of Nurse and Midwife in BPCR:
| Role | Activities |
|---|---|
| Educator | Teach BPCR during every antenatal visit, especially in the 3rd trimester |
| Planner | Help mother make a personalized birth plan |
| Facilitator | Assist in linking with health services and referral centers |
| Supporter | Empower family to make informed decisions |
| Observer | Monitor compliance with the plan |
| Referrer | Prompt referral in case of complications |
🔷 Tools to Support BPCR:
- Mother and Child Protection (MCP) Card – space to document birth plan
- Flipcharts and Posters – for community education
- Birth Preparedness Checklist – simple tool for field health workers
- ASHA Home Visits – in 3rd trimester for counseling and preparation
🔷 Benefits of BPCR:
✅ Timely arrival at health facility
✅ Reduction in delays (Three Delays Model):
- Delay in deciding to seek care
- Delay in reaching care
- Delay in receiving care at the facility
✅ Improved maternal and neonatal outcomes
✅ Empowered families and communities
✅ Strengthened health system linkages
🤝🌸 Respectful Care and Compassionate Communication in Maternity Services.
🔷 Introduction:
Respectful maternity care (RMC) and compassionate communication are fundamental rights of every woman during pregnancy, childbirth, and postpartum. These principles ensure that care is provided in a dignified, supportive, and empathetic manner, free from abuse, neglect, or discrimination.
Midwives and nurses are at the frontline of maternal care, and their communication style and attitude can directly impact a woman’s health, trust, and birth experience.
🔷 Definition:
Respectful care is the delivery of maternal care that is human rights-based, woman-centered, and culturally appropriate, ensuring dignity, privacy, and informed consent at every stage.
Compassionate communication involves actively listening, empathizing, and responding to the physical and emotional needs of the woman using kindness and respect.
🔷 Key Principles of Respectful Maternity Care (RMC):
- Dignity and Respect
- Privacy and Confidentiality
- Informed Consent and Decision-making
- Non-discrimination (irrespective of caste, class, religion, economic status)
- Freedom from abuse, neglect, and coercion
- Companionship and emotional support
- Right to information and communication in understandable language
🔷 Importance of RMC and Compassionate Communication:
- Builds trust between provider and woman
- Improves maternal satisfaction and mental health
- Promotes positive health-seeking behavior
- Encourages institutional delivery and follow-up
- Reduces birth trauma, depression, and violence
- Supports early breastfeeding and bonding
🔷 Practical Examples of Respectful Care:
| Situation | Respectful Action |
|---|---|
| During examination | Always seek verbal consent, explain the procedure |
| During labor | Allow birth companion, provide reassurance and encouragement |
| Personal privacy | Cover with clean drapes, close doors/curtains |
| Communication | Use her name, speak gently, make eye contact |
| Decision-making | Explain options (e.g., normal birth vs. C-section), ask for her choice |
| Pain or fear | Acknowledge feelings, offer comfort and coping techniques |
| Discharge | Provide complete information about postnatal care and newborn care |
🔷 Common Disrespect and Abuse in Maternity Settings (To Be Avoided):
🚫 Scolding, shouting, blaming the woman
🚫 Performing procedures without consent
🚫 Not allowing a birth companion
🚫 Leaving the woman unattended during labor
🚫 Ignoring complaints of pain
🚫 Breach of confidentiality
🚫 Discrimination based on caste, age, or literacy
🚫 Threatening or forcing treatment
🔷 Skills for Compassionate Communication:
| Skill | Description |
|---|---|
| Active listening | Give full attention, nod, and respond empathetically |
| Empathy | Try to understand what the woman is feeling (e.g., “I can see you’re scared. I’m here to help you.”) |
| Gentle tone and body language | Calm voice, open posture, eye contact |
| Clear explanation | Use simple, local language and check understanding |
| Respect personal space and cultural norms | Ask before touching, adjust to customs if safe |
| Encouragement and reassurance | Use phrases like: “You are doing well,” “You’re strong,” “I am with you.” |
🔷 Role of Midwife/Nurse in Ensuring RMC and Compassionate Care:
| Role | Responsibility |
|---|---|
| Advocate | Stand for women’s rights in maternity care |
| Communicator | Build trust, rapport, and openness |
| Protector | Prevent mistreatment, abuse, or neglect |
| Educator | Inform the woman about her care, procedures, and options |
| Supporter | Offer emotional and physical support during labor and delivery |
| Team member | Promote respectful culture among staff and junior workers |
🔷 National and Global Initiatives Supporting RMC:
- WHO framework on quality maternal and newborn care
- LaQshya Program (India) – focuses on respectful and quality care during labor
- White Ribbon Alliance – promotes Respectful Maternity Care Charter
- Suman Program (India) – Surakshit Matritva Aashwasan for dignified care
📋🖊️ Recording and Reporting of Clinical Procedures as per Government of India (GoI) Guidelines
(Midwifery and Gynecology Nursing Perspective – as per RCH, RMNCH+A, and NHM norms)
🔷 Introduction:
Accurate recording and reporting of clinical procedures is a legal, ethical, and professional requirement in nursing and midwifery practice. It ensures continuity of care, supports monitoring and evaluation, guides policy-making, and improves accountability in maternal and child health services.
The Government of India (GoI), through the Ministry of Health & Family Welfare (MoHFW), has laid down standardized formats and protocols under various programs like:
- RCH Program
- RMNCH+A (Reproductive, Maternal, Newborn, Child & Adolescent Health)
- NHM (National Health Mission)
🔷 Objectives of Recording and Reporting in Clinical Practice:
- To ensure systematic documentation of all services provided
- To support referral, follow-up, and evaluation
- To provide legal evidence of procedures performed
- To ensure supply chain (logistics) planning
- To track key health indicators for planning and policy
🔷 What Should Be Recorded in Clinical Practice:
✅ During Antenatal Care (ANC):
| What to Record | Where to Record |
|---|---|
| ANC registration details | ANC register, MCP card |
| Obstetric history (G-P-A-L) | ANC card, register |
| Physical exam findings | ANC case sheet |
| Investigations (Hb, BP, urine, USG) | ANC lab records |
| IFA/Calcium tablet distribution | Supplementation record |
| Immunization (TT/TD doses) | MCP card, immunization register |
| Birth preparedness counseling | ANC checklist or BPCR plan |
| Danger signs taught | MCP card notes |
| High-risk identification | High-risk ANC register |
✅ During Intrapartum (Labor and Delivery):
| What to Record | Tool/Format |
|---|---|
| Date & time of admission | Labor room register |
| Partograph entries | Individual partograph chart |
| Fetal heart rate, BP, contractions | Partograph |
| Interventions (ARM, oxytocin, episiotomy) | Case sheet |
| Delivery details (time, mode, sex of baby, APGAR) | Delivery register |
| Maternal complications | Complication register |
| Referral details (if any) | Referral slip, register |
| Essential newborn care (ENBC) | Newborn care register |
✅ During Postnatal Care (PNC):
| What to Record | Where |
|---|---|
| Postnatal vitals | PNC register, home visit format |
| Lochia, uterine involution | Postnatal assessment sheet |
| Breastfeeding status | PNC visit checklist |
| Newborn condition | Newborn register |
| Family planning counseling | Eligible couple register |
| Discharge details | Case sheet, discharge slip |
✅ During Clinical Procedures (Perineal care, catheterization, injections, IUCD insertion):
Each procedure should include:
- Date and time
- Indication for procedure
- Procedure performed (with technique used)
- Consent (if applicable)
- Complications (if any)
- Follow-up advice
📝 Use standard procedure logbooks, nursing notes, or GoI registers (IUCD insertion register, injection register, etc.)
🔷 GoI Specified Registers and Formats:
| Tool/Format | Use |
|---|---|
| ANC Register | For ANC registration and visits |
| Delivery Register | Records of all institutional births |
| Postnatal Register | Mother & baby check-ups after delivery |
| High-Risk Pregnancy Register | Tracking special cases |
| MCP Card (Mother and Child Protection Card) | Hand-held record given to every mother |
| Partograph | To monitor labor progression |
| Referral Slip | Used when referring to higher facility |
| Family Planning Register | IUCDs, OCPs, injectable contraception |
| HMIS (Health Management Information System) | Monthly online reporting by ANM/ASHA/PHC |
| ANM Monthly Report (Form 6) | For sub-center-level reporting under NHM |
🔷 Essential Elements of Good Recording:
| Element | Description |
|---|---|
| ✅ Accuracy | No false data; based on actual observation |
| ✅ Clarity | Use clear handwriting or digital entry |
| ✅ Legibility | Easy to read and understand |
| ✅ Confidentiality | Keep patient data private |
| ✅ Timeliness | Enter data as soon as procedure is done |
| ✅ Completeness | All required fields must be filled |
| ✅ Signature & Date | Always sign after entry |
🔷 Legal and Ethical Importance:
- Medical records are legal documents
- Can be used in court or audits
- Incomplete or false entries may cause legal or professional action
- Respect for client confidentiality and informed consent is critical
🔷 Nurse/Midwife’s Role in Recording and Reporting:
| Role | Activities |
|---|---|
| Recorder | Accurately write all procedures, findings, and outcomes |
| Reporter | Submit monthly reports to supervisor/PHC |
| Verifier | Double-check calculations, lab reports, medication doses |
| Educator | Teach patients about the information in MCP card |
| Communicator | Report abnormal findings immediately to MO |
| Coordinator | Link with ASHA/AWW for follow-up and community reporting |
🔷 Digital Tools & e-Reporting (GoI Initiatives):
- e-Mamta (for mother and child tracking in Gujarat and other states)
- RCH Portal – web-based platform for service tracking
- ANMOL App – tablet-based application for ANMs
- HMIS Portal – national-level health service reporting system
🩺 Government of India (GoI) – Current Model of Antenatal Care (ANC) Provision
(As per RMNCH+A Strategy, LaQshya Guidelines, and latest MoHFW norms)
(Midwifery and Gynecology Nursing Perspective)
🔷 Introduction:
The Government of India has standardized the Antenatal Care (ANC) model to improve maternal and fetal outcomes, especially under the umbrella of the Reproductive, Maternal, Newborn, Child and Adolescent Health (RMNCH+A) strategy.
The model aims at universal, quality ANC services, focusing on early registration, risk identification, timely interventions, and continuity of care.
🔷 Current Model of ANC Provision – Key Highlights:
✅ 1. Early Registration of Pregnancy
- Within 12 weeks of gestation
- At any Sub-center, PHC, CHC, UPHC, or private facility
- Recorded in MCP Card and RCH Portal
- Allows early screening for risk factors like anemia, hypertension, diabetes
✅ 2. Recommended Minimum 4 ANC Visits
| Visit | Timing |
|---|---|
| 1st Visit | By 12 weeks (first trimester) |
| 2nd Visit | Between 14–26 weeks |
| 3rd Visit | Between 28–34 weeks |
| 4th Visit | Between 36 weeks and term |
🔹 In high-risk pregnancies, more frequent ANC visits are advised.
✅ 3. Monthly Village Health and Nutrition Day (VHND)
- Held at Anganwadi Center
- Services include ANC check-ups, IFA distribution, immunization, counseling
- Conducted by ANM, ASHA, and AWW collaboratively
✅ 4. Pradhan Mantri Surakshit Matritva Abhiyan (PMSMA)
- Conducted on 9th of every month
- Free and quality ANC services to all pregnant women
- Includes examination by specialists and MBBS doctors
- Focus on identifying high-risk pregnancies
✅ 5. Key Services Provided in ANC Model:
| Category | Services Included |
|---|---|
| Assessment | Height, weight, BP, abdominal exam, fetal heart sound |
| Laboratory | Hb%, blood group & Rh, urine (sugar/protein), HIV, VDRL, HBsAg, blood sugar, thyroid if needed |
| Immunization | 2 doses of TT/TD or 1 booster if vaccinated in last pregnancy |
| Supplementation | |
| – IFA tablets (100 mg Iron + 0.5 mg Folic Acid) – 180 days | |
| – Calcium 500 mg – twice daily | |
| – Albendazole 400 mg (single dose after 2nd trimester) | |
| Ultrasound | |
| – Early USG (before 12 weeks) for dating | |
| – Anomaly scan at 18–20 weeks | |
| – Growth scan if needed | |
| Counseling | Nutrition, danger signs, birth preparedness, family planning, breastfeeding, rest |
✅ 6. Identification and Management of High-Risk Pregnancy (HRP)
Common HRP indicators include:
- Age <18 or >35
- Severe anemia (Hb <7 gm/dL)
- Hypertension, diabetes
- Previous C-section, stillbirth
- Malpresentation
- Twin pregnancy
🩺 HRPs are tracked and referred using High-Risk ANC Register.
✅ 7. Record Keeping & Monitoring
| Tool | Use |
|---|---|
| MCP Card | Carried by the woman; records all services |
| ANC Register | Maintained at sub-center/PHC |
| RCH Portal (Mother Tracking System) | Digital entry of services provided |
| ANMOL App | Tablet-based tool for ANMs |
| LaQshya Dashboard | For quality monitoring in labor rooms and maternity OTs |
🔷 New GoI Initiatives Strengthening ANC Model:
🌟 LaQshya Program
- Ensures quality ANC, intrapartum, and postpartum care
- Focus on dignified and respectful care
- Monitors labor room and maternity OT standards
🌟 SUMAN (Surakshit Matritva Aashwasan)
- Provides free, quality, respectful maternal and newborn care
- Includes zero cost delivery, drugs, diagnostics, and transport
🔷 Role of ANM/Staff Nurse/Midwife in ANC Model:
| Role | Responsibilities |
|---|---|
| Service Provider | Conduct ANC checkups, physical exams, distribute supplements |
| Counselor | Educate women and family on diet, danger signs, and birth preparedness |
| Record Keeper | Maintain ANC register, MCP card, and digital records |
| Risk Identifier | Screen for and refer high-risk pregnancies |
| Community Link | Coordinate with ASHA and AWW for VHND and follow-ups |
🌸👩⚕️ Role of Doula and ASHA in Maternal and Newborn Care
(Midwifery and Gynecology Nursing Perspective – Respectful Maternity Care and Community-Based Services)
🔷 Who is a Doula?
A Doula is a trained, non-medical support person who provides continuous physical, emotional, and informational support to a woman before, during, and after childbirth.
- The term “Doula” comes from the Greek word meaning “a woman who serves.”
- While not a common designation under GoI programs yet, Doula-based care is being promoted in some states and private settings under respectful maternity care (RMC) initiatives.
- Doulas are not clinical staff (do not perform deliveries or administer medications), but offer psychosocial and physical comfort.
✅ Role of a Doula:
| Time | Activities |
|---|---|
| During Pregnancy |
- Provide education on labor and delivery
- Help with birth planning
- Offer emotional support and reduce anxiety
- Accompany to antenatal visits (if permitted) | | During Labor |
- Give continuous presence and encouragement
- Support breathing, massage, position changes
- Act as a link between woman and care provider
- Ensure woman’s voice is heard | | After Birth |
- Assist in early initiation of breastfeeding
- Support emotional transition to motherhood
- Help with newborn care and comfort measures
🌟 Research shows that having a doula can reduce C-section rates, shorten labor, and improve maternal satisfaction.
🔷 Who is an ASHA? (Accredited Social Health Activist)
- Introduced under the National Rural Health Mission (NRHM), now part of NHM (National Health Mission)
- ASHA is a trained female community health volunteer
- Selected from the same village/community, usually married/widowed/divorced women aged 25–45 years
ASHA means “hope,” and she serves as the bridge between the community and the public health system.
✅ Role of ASHA in Maternal and Newborn Care:
| Stage | Key Activities |
|---|---|
| Before Pregnancy |
- Promote family planning
- Distribute condoms, OCPs
- Counsel newlyweds about reproductive health | | During Pregnancy
- Register pregnant women at sub-center/PHC
- Escort women to ANC clinics and PMSMA days
- Home visits to educate on diet, rest, danger signs
- Promote birth preparedness and complication readiness (BPCR)
- Track high-risk pregnancies and support referral
- Ensure women get TT/TD injections, IFA tablets, calcium
- Distribute MCP cards | | During Labor |
- Accompany woman to delivery center
- Ensure institutional delivery at public facility
- Provide emotional support and comfort
- Ensure birth companion policy is implemented | | After Delivery |
- Make 6 postnatal home visits (as per HBNC guidelines)
- Monitor mother’s health, uterine involution, bleeding, breastfeeding
- Educate on exclusive breastfeeding and newborn care
- Identify danger signs in mother or baby
- Assist in birth registration and linking to nutrition services | | Child Health |
- Promote immunization
- Track growth and development
- Counsel on complementary feeding
- Mobilize for VHND (Village Health and Nutrition Day) |
🔷 ASHA Incentives (GoI Performance-Based):
| Activity | Incentive (approximate) |
|---|---|
| Early registration of pregnancy | ₹100 |
| Accompanying woman for ANC | ₹250 |
| Ensuring institutional delivery (JSY) | ₹600 (rural) / ₹400 (urban) |
| Postnatal visits (HBNC) | ₹250–350 |
| Full immunization | ₹100–200 |
(Incentive amounts may vary by state)
🔷 Comparison: Doula vs ASHA
| Feature | Doula | ASHA |
|---|---|---|
| Trained in childbirth support | Yes (non-medical) | Yes (community health) |
| Belongs to community | Sometimes | Always |
| Paid incentive by GoI | No (usually private/NGO) | Yes |
| Clinical responsibility | No | No (but links with ANM/PHC) |
| Emotional labor support | Strong role | Limited |
| Continuity of care | Antenatal to postpartum | Yes |
| Formal recognition by GoI | No (yet) | Yes |
II Trimester.
Education and Management of Physiological Changes & Discomforts in 2nd Trimester of Pregnancy (14–28 weeks)
📌 INTRODUCTION:
The second trimester is often referred to as the “honeymoon phase” of pregnancy. Many women feel more energetic and experience fewer symptoms compared to the first trimester. However, new physiological changes and minor discomforts may emerge, which require proper nursing assessment, anticipatory guidance, and interventions.
🧠 EDUCATION & MANAGEMENT BASED ON SYSTEM-WISE CHANGES:
1. Reproductive System Changes
| Change | Discomfort | Management/Nursing Interventions |
|---|---|---|
| Uterus enlarges (rises above the pelvis) | Abdominal stretching, round ligament pain | ➤ Teach abdominal support techniques ➤ Use maternity belt ➤ Encourage side-lying position |
| Increased vaginal discharge (leukorrhea) | May cause discomfort or concern | ➤ Reassure it’s normal unless foul-smelling or itchy ➤ Teach perineal hygiene ➤ Wear cotton underwear, avoid douching |
2. Cardiovascular System Changes
| Change | Discomfort | Management/Nursing Interventions |
|---|---|---|
| Increased blood volume and cardiac output | Palpitations, dizziness, dependent edema | ➤ Reassure unless persistent ➤ Encourage rest with legs elevated ➤ Avoid prolonged standing ➤ Monitor BP regularly (for gestational hypertension) |
3. Musculoskeletal System
| Change | Discomfort | Management/Nursing Interventions |
|---|---|---|
| Softening of ligaments, weight gain | Backache, postural changes | ➤ Advise good posture ➤ Use firm mattress ➤ Pelvic tilt exercises ➤ Avoid high heels |
4. Gastrointestinal System
| Change | Discomfort | Management/Nursing Interventions |
|---|---|---|
| Progesterone slows GI motility | Constipation, bloating, heartburn | ➤ High fiber diet, increase fluid intake ➤ Gentle physical activity ➤ Small, frequent meals for heartburn ➤ Avoid spicy/fatty foods |
5. Urinary System
| Change | Discomfort | Management/Nursing Interventions |
|---|---|---|
| Uterus presses on bladder | Frequency of urination (less than 1st trimester) | ➤ Reassure ➤ Encourage adequate hydration ➤ Teach UTI prevention (wiping front to back) |
6. Skin Changes
| Change | Discomfort | Management/Nursing Interventions |
|---|---|---|
| Melasma, linea nigra, striae gravidarum | Cosmetic concern, itching | ➤ Reassure – usually fades postpartum ➤ Use mild moisturizers for itching ➤ Avoid excessive sun exposure |
7. Breasts
| Change | Discomfort | Management/Nursing Interventions |
|---|---|---|
| Enlargement, areolar darkening, colostrum secretion | Breast tenderness, tightness | ➤ Wear supportive maternity bra ➤ Teach about colostrum being normal ➤ Avoid expressing milk |
🤰 COMMON MINOR DISCOMFORTS IN 2ND TRIMESTER AND NURSING MANAGEMENT:
| Discomfort | Cause | Nursing Education and Management |
|---|---|---|
| Leg cramps | Pressure on pelvic nerves, calcium deficiency | ➤ Leg elevation during rest ➤ Calf-stretching exercises ➤ Ensure calcium/magnesium intake |
| Varicose veins | Decreased venous return due to uterine pressure | ➤ Avoid standing for long ➤ Wear compression stockings ➤ Leg elevation |
| Nasal congestion/epistaxis | Estrogen-induced vascular engorgement | ➤ Use saline drops ➤ Humidifier use ➤ Avoid nasal sprays with medication unless prescribed |
| Mood swings | Hormonal shifts | ➤ Emotional support ➤ Encourage communication with partner/family ➤ Refer to counselor if needed |
🎓 HEALTH TEACHING/EDUCATION BY MIDWIFE:
- Fetal Movement Monitoring
- Starts to be felt around 18–22 weeks.
- Teach how to identify and record movements.
- Warning Signs to Report Immediately
- Vaginal bleeding
- Severe abdominal pain
- Severe headache or visual disturbances
- Sudden swelling of hands/face
- Absence of fetal movements
- Dietary Education
- Iron, calcium, protein-rich foods
- Iron + folic acid supplementation
- Adequate hydration
- Importance of Antenatal Check-ups
- Monitor fetal growth, BP, weight, urine protein, hemoglobin
- Immunization: Tetanus Toxoid (as per schedule)
- Safe Physical Activity
- Moderate walking, pelvic floor exercises
- Avoid heavy lifting or unsafe postures
- Sexual Activity
- Safe unless contraindicated by doctor (e.g., placenta previa, bleeding)
- Birth Preparedness
- Start discussing place of delivery, emergency plans, transportation
🧑⚕️ ROLE OF MIDWIFE IN NURSING CARE:
- Provide empathetic communication and address individual concerns
- Offer culturally sensitive health education
- Maintain documentation of changes and teaching given
- Encourage family involvement and support
- Screen for mental health issues or intimate partner violence
🌸 MIDWIFERY NURSING: Rh-Negative Mother & Prophylactic Anti-D Immunoglobulin
🧬 WHAT IS Rh FACTOR?
- Rh factor (Rhesus factor) is a protein found on red blood cells.
- People who have it are Rh-positive (Rh⁺).
- Those who do not have it are Rh-negative (Rh⁻).
⚠️ WHY IS Rh INCOMPATIBILITY A CONCERN IN PREGNANCY?
➤ Problem arises if:
- The mother is Rh-negative, and
- The baby is Rh-positive (inherited from Rh-positive father),
- Then fetal Rh⁺ red blood cells may enter mother’s bloodstream (called fetomaternal hemorrhage or FMH),
- Mother’s immune system sees Rh⁺ cells as “foreign” and produces antibodies against them (called anti-D antibodies).
➤ These antibodies:
- Don’t usually affect the first pregnancy.
- But in subsequent pregnancies, they can cross the placenta and destroy fetal Rh⁺ red blood cells, causing:
- Hemolytic Disease of the Fetus and Newborn (HDFN) or
- Erythroblastosis fetalis – a life-threatening condition for the baby.
💉 WHAT IS ANTI-D IMMUNOGLOBULIN?
- Anti-D (Rho(D) immune globulin) is a passive antibody injection that destroys fetal Rh-positive cells in the mother’s bloodstream before her body can react and make antibodies.
📆 WHEN IS PROPHYLACTIC ANTI-D GIVEN?
🔹 1. Antenatal prophylaxis
| Timing | Details |
|---|---|
| Around 28 weeks | To prevent sensitization due to silent FMH in late pregnancy |
| After any event that can cause fetal cells to enter maternal blood: | – Bleeding during pregnancy – Amniocentesis, chorionic villus sampling – External cephalic version – Trauma or abdominal injury – Miscarriage, abortion, ectopic pregnancy, MTP |
🔹 2. Postnatal prophylaxis
| Timing | Details |
|---|---|
| Within 72 hours after delivery | If baby is confirmed Rh-positive |
🩸 DOSE OF ANTI-D
| Situation | Usual Dose |
|---|---|
| Antenatal (28 weeks) | 300 µg IM (protects against 30 mL fetal blood) |
| Postnatal (within 72 hrs) | 300 µg IM |
| After miscarriage or invasive procedures | 50–300 µg depending on gestational age & risk |
🧪 TESTS BEFORE ADMINISTRATION
- Mother’s blood group & Rh typing
- Indirect Coombs test (ICT): to detect if the mother is already sensitized.
- ➤ If ICT is negative → give Anti-D
- ➤ If ICT is positive → she is already sensitized → no benefit of Anti-D
- Kleihauer–Betke test (if available): Measures the amount of fetal blood in maternal circulation to calculate Anti-D dose (especially in large fetomaternal hemorrhage)
🧑⚕️ ROLE OF MIDWIFE / NURSE
🌼 Nursing Assessment:
- Identify Rh-negative mothers early
- Take detailed obstetric and transfusion history
- Monitor for bleeding, trauma, or procedures
🌼 Nursing Education:
- Educate mother on importance of Anti-D injection
- Explain risk of not taking prophylaxis
- Inform about potential reactions (minor like soreness, rare allergic reaction)
🌼 Administration:
- Give IM in deltoid or gluteal muscle
- Document batch number, dose, time, and site
- Monitor for 15–30 mins post-injection for any allergic reaction
🚨 IF ANTI-D IS NOT GIVEN – RISK
- Mother becomes Rh-sensitized (permanently)
- Future pregnancies at high risk of HDFN
- May require:
- Intrauterine transfusion
- Early delivery
- Neonatal intensive care
- Risk of stillbirth or neonatal death
📝 IMPORTANT POINTS TO REMEMBER
- Anti-D is only effective if the mother has not yet formed her own anti-D antibodies
- Anti-D does not harm the baby or the mother
- Always check baby’s Rh type after delivery before deciding on postnatal Anti-D
- Anti-D is not a vaccine; it provides temporary protection
🌸 MIDWIFERY NURSING: Second Trimester Tests (14 to 28 Weeks)
📆 Overview:
The second trimester is a critical time to:
- Monitor fetal growth and development
- Detect congenital anomalies
- Identify maternal risks like gestational diabetes and anemia
- Ensure early interventions
🧪 MAJOR SECOND TRIMESTER TESTS:
| Test | Timing | Purpose | Nurse’s Role |
|---|
1. Ultrasound – Level II (Anomaly Scan)
| Usually at 18–22 weeks | | To assess: Fetal anatomy, congenital malformations, amniotic fluid, placental position, fetal heart & spine | | ➤ Explain procedure <br> ➤ Ensure full bladder if transabdominal <br> ➤ Provide emotional support |
2. Triple Marker or Quadruple Marker Test
| Between 15–20 weeks, ideally 16–18 weeks | | Triple Marker: Measures AFP, hCG, Estriol <br> Quad Marker: Adds Inhibin-A <br> Screens for Down syndrome, Trisomy 18, Neural tube defects | | ➤ Explain it’s a screening, not diagnostic <br> ➤ Refer for genetic counseling if abnormal <br> ➤ Ensure correct gestational age for accurate results |
3. Glucose Challenge Test (GCT) / Oral Glucose Tolerance Test (OGTT)
| Usually at 24–28 weeks | | Screens for gestational diabetes mellitus (GDM) | | ➤ 50g glucose given orally, check sugar after 1 hour (GCT) <br> ➤ If abnormal, confirm with OGTT (75g/100g) <br> ➤ Instruct fasting, explain procedure clearly |
4. Hemoglobin/Hematocrit
| Any time, but repeated at 24–28 weeks | | Detects anemia | | ➤ Educate on iron-rich foods <br> ➤ Reinforce compliance with iron + folic acid tablets |
5. Blood Pressure Monitoring
| At every antenatal visit | | Early identification of pregnancy-induced hypertension | | ➤ Teach warning signs (headache, swelling, vision changes) <br> ➤ Refer if elevated BP (>140/90 mmHg) |
6. Urine Routine and Microscopy
| Every visit | | Checks for proteinuria (PIH), glucosuria (GDM), UTI | | ➤ Explain clean-catch method <br> ➤ Collect sample properly <br> ➤ Educate on UTI prevention |
7. Indirect Coombs Test (If Rh-negative mother)
| At 28 weeks | | Detects Rh sensitization | | ➤ If negative → Administer Anti-D immunoglobulin <br> ➤ Monitor further exposure risks |
8. Fetal Movement Assessment
| Starts around 18–22 weeks | | Indicates fetal wellbeing | | ➤ Teach mother to feel for movements <br> ➤ Encourage “kick count” later in pregnancy |
🧑⚕️ ROLE OF MIDWIFE / NURSE:
- Educate the mother about the purpose and importance of each test.
- Prepare her physically and emotionally for invasive or anxiety-provoking tests.
- Ensure proper timing of tests according to gestational age.
- Follow up on abnormal results and coordinate with physicians.
- Provide non-judgmental support, especially if birth defects are suspected.
- Maintain accurate documentation of all test results.
🚨 Special Cases That May Need Additional Tests:
- Multiple pregnancy
- Previous congenital anomalies
- Advanced maternal age (≥35 years)
- Family history of genetic disorders
- Previous gestational diabetes or PIH
🌸 MIDWIFERY NURSING: Health Education in Second Trimester (14–28 Weeks)
🩺 WHY IS HEALTH EDUCATION IMPORTANT IN 2nd TRIMESTER?
This is the phase where the woman:
- Feels more stable physically and emotionally
- Begins to feel fetal movements
- Is receptive to learning about pregnancy and childbirth
- May start experiencing some physical discomforts
🧠 Hence, health education during this trimester focuses on:
- Promoting maternal and fetal well-being
- Early detection of complications
- Preparing for birth and parenthood
📚 SECOND TRIMESTER HEALTH EDUCATION TOPICS:
1. ✅ Antenatal Check-ups
- Regular visits every 4 weeks
- Monitoring BP, weight, fundal height, fetal heart rate, and urine tests
- Importance of follow-up tests (anomaly scan, GDM screening)
2. 🥗 Nutrition
- Balanced diet with adequate calories, proteins, calcium, iron, and vitamins
- Increase iron-rich foods (green leafy vegetables, jaggery, dates)
- Folic acid and iron supplementation
- Avoid junk food and excessive caffeine
3. 💊 Medications and Supplements
- Compliance with Iron + Folic acid (IFA) tablets
- Deworming (if advised)
- Anti-D injection for Rh-negative mothers at 28 weeks
4. 🤰 Fetal Movement Awareness
- Teach the mother to identify fetal movement (quickening usually starts around 18–22 weeks)
- Educate on importance of fetal movement as a sign of fetal health
5. 🧘♀️ Exercise and Physical Activity
- Encourage mild exercises like walking, stretching
- Introduce antenatal yoga or breathing exercises (if no contraindication)
- Avoid heavy lifting or sudden jerky movements
6. 💤 Rest and Sleep
- Encourage 8 hours of night sleep and short daytime rest
- Teach left lateral sleeping position for optimal uteroplacental blood flow
- Use pillow support for back and legs
7. 🧴 Body Changes and Hygiene
- Teach about normal physiological changes: breast enlargement, linea nigra, melasma
- Promote daily bath, clean and dry undergarments, perineal hygiene
- Address issues like leukorrhea, varicose veins, backache
8. 🧠 Mental and Emotional Wellbeing
- Discuss mood swings, fears, and expectations
- Involve family or partner for emotional support
- Encourage joining antenatal support groups
9. 🍼 Preparation for Breastfeeding
- Importance of exclusive breastfeeding
- Care of breasts during pregnancy
- Addressing myths or misconceptions
10. 🏥 Birth Preparedness and Complication Readiness
- Plan place of delivery (institutional delivery)
- Keep birth companion and emergency contacts ready
- Save money, arrange transport
- Recognize danger signs:
- Vaginal bleeding
- Severe headache or blurred vision
- Abdominal pain
- Reduced fetal movement
- Swelling of hands/face
11. ❤️ Sexual Activity
- Safe unless contraindicated
- Teach about safe positions, emotional understanding, and hygiene
12. 💉 Immunization
- Tetanus Toxoid or Tdap as per local guidelines
- Educate about timing and side effects
13. 🚭 Lifestyle Modifications
- Stop smoking, alcohol, tobacco, or pan masala
- Avoid self-medication
- Maintain a clean, stress-free environment
14. 👨👩👧 Involve the Family
- Educate spouse and family about mother’s needs
- Encourage shared responsibility and emotional support
🧑⚕️ ROLE OF MIDWIFE / NURSE:
- Conduct individual and group health education sessions
- Use charts, models, flipbooks, videos for better understanding
- Provide empathy and culturally sensitive care
- Keep records and follow-up for high-risk mothers
🌸 MIDWIFERY NURSING: Interpreting Screening Results in Pregnancy (2nd Trimester Focus)
🧠 WHAT ARE SCREENING TESTS?
- Screening tests are done to identify the risk of a condition (not to confirm it).
- In pregnancy, they help detect potential fetal anomalies, maternal risks, or complications early.
- If positive or abnormal, they must be followed up with diagnostic tests.
📋 COMMON SECOND TRIMESTER SCREENING TESTS & INTERPRETATION:
1. 🧪 Triple Marker Test (AFP, hCG, Estriol)
2. 🧪 Quadruple Marker Test (AFP, hCG, Estriol, Inhibin-A)
| Done at | 15–20 weeks gestation (ideal: 16–18 weeks) | | Purpose | Detect chromosomal abnormalities (like Down Syndrome, Trisomy 18) and Neural Tube Defects (NTDs) |
| Marker | High Level Indicates | Low Level Indicates |
|---|---|---|
| AFP | Neural tube defects, abdominal wall defects | Down syndrome |
| hCG | Down syndrome | Trisomy 18 |
| Estriol | – | Low in Down syndrome & Trisomy 18 |
| Inhibin-A (in Quad test) | High in Down syndrome | – |
➤ Interpretation:
- Normal result: Risk is low → no further testing needed.
- Abnormal result: Risk is high → offer diagnostic test (e.g., amniocentesis).
🧑⚕️ Nurse’s Role:
- Explain it’s a risk estimate, not a diagnosis.
- Provide emotional support if abnormal.
- Refer to fetal medicine specialist/genetic counselor.
3. 💉 Oral Glucose Challenge Test (GCT)
| Done at | 24–28 weeks | | Purpose | Screening for Gestational Diabetes Mellitus (GDM) | | Method | 50g glucose → Blood sugar checked after 1 hour |
| Result | Interpretation |
|---|---|
| < 140 mg/dL | Normal |
| ≥ 140 mg/dL | Abnormal – proceed to OGTT |
4. 🧬 Indirect Coombs Test (ICT)
| For | Rh-negative mothers at 28 weeks | | Purpose | Detects if mother has developed antibodies against Rh⁺ blood |
| Result | Interpretation |
|---|---|
| Negative | No antibodies → Give Anti-D |
| Positive | Sensitization occurred → No benefit from Anti-D, monitor closely |
5. 🔬 Hemoglobin (Hb)/Hematocrit
| Normal | Hb ≥ 11 g/dL | | Mild anemia | 10–10.9 g/dL | | Moderate anemia | 7–9.9 g/dL | | Severe anemia | < 7 g/dL |
🧑⚕️ Intervention:
- Iron + folic acid tablets
- Dietary advice
- Deworming
- IV iron or blood transfusion (if needed)
6. 🧫 Urine Routine & Microscopy
| Finding | Interpretation |
|---|---|
| Protein + | Possible PIH (Pre-eclampsia) |
| Glucose + | May indicate GDM |
| Pus cells | Suggests urinary tract infection (UTI) |
7. 🧍♀️ Blood Pressure Monitoring
| BP ≥ 140/90 mmHg | Hypertensive disorder in pregnancy | | BP < 90/60 mmHg | Hypotension – may cause fainting |
8. 🧼 Ultrasound – Anomaly Scan (Level II)
| Done at | 18–22 weeks | | Detects | Structural defects (heart, spine, brain, limbs, kidneys) | | Normal | No anomalies found | | Abnormal | Refer for detailed evaluation, genetic counseling, or fetal therapy |
📌 KEY POINTS IN SCREENING INTERPRETATION:
- Screening ≠ Diagnosis
- Positive screening needs confirmatory diagnostic tests.
- Early detection = better management and birth preparedness.
🧑⚕️ MIDWIFE’S RESPONSIBILITY:
- Educate pregnant women about purpose and process of screening tests.
- Ensure screening is done at the correct gestational age.
- Interpret reports along with the doctor and explain results simply to the mother.
- Provide emotional support, especially if the result is abnormal.
- Coordinate referrals to specialist clinics if needed.
🌸 MIDWIFERY NURSING: Health Education on IFA (Iron and Folic Acid)
✅ INTRODUCTION:
IFA tablets are essential supplements given to pregnant women to prevent:
- Anemia (due to iron deficiency)
- Neural tube defects in the fetus (due to folic acid deficiency)
- Low birth weight, preterm birth, and maternal complications
📚 KEY HEALTH EDUCATION POINTS:
1. ✨ Importance of IFA During Pregnancy
| Component | Function |
|---|---|
| Iron | Forms hemoglobin, prevents anemia, supports oxygen supply to baby |
| Folic Acid | Prevents neural tube defects (spina bifida), helps in cell growth and fetal development |
2. 💊 Recommended Dosage (As per Government of India/WHO guidelines)
| Group | Dose |
|---|---|
| Pregnant women (second trimester onward) | 1 tablet daily (60 mg elemental iron + 500 mcg folic acid) for 180 days |
| Postnatal mothers | 1 tablet daily for 6 months after delivery |
| Adolescent girls/women of reproductive age | 1 tablet weekly for anemia prevention |
3. 🕐 When and How to Take IFA Tablet
- Time: Preferably after meals, not on empty stomach
- With water (not tea, coffee, or milk)
- Take at same time daily for consistency
- Swallow whole tablet—do not crush or chew
4. ⚠️ Possible Side Effects (and their Management)
| Side Effect | Management Advice |
|---|---|
| Nausea | Take after food, at night if needed |
| Constipation | Drink plenty of fluids, eat fiber-rich foods |
| Dark stools | Normal – reassure mother |
| Metallic taste | Suck on lemon candy, rinse mouth |
| Vomiting | Report to nurse or doctor if persistent |
5. 🍲 Dietary Advice Along with IFA
- Encourage iron-rich foods: green leafy vegetables, jaggery, dates, lentils, red meat
- Enhance absorption by taking Vitamin C-rich foods (e.g., lemon, amla)
- Avoid tea or coffee 1 hour before/after taking the tablet
6. 🩸 Signs of Anemia to Watch For
- Fatigue and weakness
- Pale skin, lips, or palms
- Breathlessness or dizziness
- Headaches
- Palpitations
➡️ If these symptoms occur, consult health worker for evaluation.
7. 🧑⚕️ NURSE/MIDWIFE’S ROLE:
- Educate mother on importance of compliance
- Demonstrate how and when to take the tablet
- Dispel myths: IFA doesn’t make baby dark or heavy!
- Follow up regularly: Ask about side effects, ensure compliance
- Maintain records of IFA distribution and consumption
- If hemoglobin < 7 g/dL → refer for higher care or injectable iron
8. 📦 STORAGE AND HANDLING
- Keep in cool, dry place, away from children
- Check expiry date before use
✅ KEY MESSAGES FOR THE MOTHER:
- “Taking your red tablet daily gives you strength and helps your baby grow healthy.”
- “Don’t stop IFA if you have black stools—that means it’s working!”
- “IFA is like a daily health tonic for you and your baby!”
🌸 MIDWIFERY NURSING: Calcium and Vitamin D Supplementation
✅ INTRODUCTION:
Calcium and Vitamin D are essential micronutrients required during pregnancy and lactation for:
- Healthy bone and teeth development of the fetus
- Muscle and nerve function
- Prevention of pregnancy-related complications like preeclampsia, low birth weight, and maternal bone loss
🧠 WHY IS SUPPLEMENTATION NEEDED?
Even with a good diet, most pregnant women do not meet the increased demands of calcium and Vitamin D due to:
- Poor dietary intake
- Low sun exposure (especially in covered dress cultures)
- Increased fetal demands
- Hormonal changes affecting calcium metabolism
📆 WHEN TO START?
- Calcium and Vitamin D supplementation should begin from the second trimester (14–16 weeks) and continue throughout pregnancy and up to 6 months postpartum.
💊 RECOMMENDED DAILY DOSE:
| Group | Calcium | Vitamin D |
|---|---|---|
| Pregnant & lactating women | 1000–1200 mg/day | 400–600 IU/day (can go up to 1000 IU if needed) |
| As per Govt. of India (RCH Guidelines) | 500 mg elemental calcium + 250 IU Vitamin D twice daily | Total: 1000 mg calcium + 500 IU Vitamin D |
🔍 SOURCES:
🍲 Dietary Sources of Calcium:
- Milk, curd, paneer, cheese
- Ragi (finger millet), soybeans
- Green leafy vegetables (e.g., spinach, methi)
- Nuts and seeds (e.g., almonds, sesame)
- Fish with bones (e.g., sardines)
🌞 Sources of Vitamin D:
- Sunlight exposure (best source) – at least 30 minutes/day on face, hands
- Fortified foods (milk, cereals)
- Fish (salmon, tuna), eggs
🧪 DEFICIENCY RISKS:
In Mother:
- Leg cramps, backache, fatigue
- Osteomalacia (bone softening)
- Preeclampsia
- Risk of fractures (in long-term)
In Baby:
- Low birth weight
- Rickets
- Poor bone and tooth development
⚠️ SIGNS OF DEFICIENCY:
| Calcium Deficiency | Vitamin D Deficiency |
|---|---|
| Muscle cramps/spasms | Bone pain, fatigue |
| Weak nails, tooth decay | Delayed milestones in baby |
| Tingling in fingers | Increased risk of preeclampsia |
🧑⚕️ HEALTH EDUCATION POINTS FOR MOTHERS:
📍 On Supplementation:
- Take 2 tablets/day (morning and evening), each with 500 mg calcium + 250 IU vitamin D
- Avoid taking with Iron tablet – gap of 2 hours is important (iron and calcium compete for absorption)
- Take with food to improve absorption
- Continue even during breastfeeding period
📍 On Diet:
- Include milk/milk products daily
- Encourage sunlight exposure—preferably morning sun
- Increase physical activity for better calcium utilization
📦 STORAGE AND HANDLING:
- Store tablets in a cool, dry place
- Check for expiry date
- Keep out of reach of children
🧑⚕️ NURSE’S/MIDWIFE’S ROLE:
- Assessment:
- Identify women at risk (poor diet, multiple pregnancies, underweight, vitamin D deficiency)
- Education:
- Explain benefits of calcium and vitamin D for mother and baby
- Teach proper timing of intake with other supplements
- Emphasize diet + sunlight
- Distribution & Monitoring:
- As per government programs, give calcium tablets free under RCH or PMSMA
- Ensure compliance and follow-up
- Record and report side effects (e.g., constipation, nausea)
🔄 COMMON MISCONCEPTIONS TO ADDRESS:
| Myth | Fact |
|---|---|
| “Milk alone is enough” | No, supplementation is still needed to meet full requirement |
| “Sunlight exposure causes tanning” | Only early morning sunlight is needed for Vitamin D synthesis |
| “Too much calcium will make baby big” | Not true – calcium supports healthy bones, not baby weight |
🌸 MIDWIFERY NURSING: Glucose Tolerance Test (GTT) in Pregnancy
✅ INTRODUCTION
The Glucose Tolerance Test (GTT) is used to:
- Screen and diagnose gestational diabetes mellitus (GDM) during pregnancy
- Detect how well the body metabolizes glucose
📆 WHEN IS IT DONE?
| Test | Timing |
|---|---|
| Screening test (GCT) | 24–28 weeks gestation for all pregnant women |
| Early testing (before 24 weeks) | If high risk (obese, PCOS, history of GDM, family history of diabetes) |
🧪 TYPES OF TESTS
1. 💉 Glucose Challenge Test (GCT) – Screening Test
| Purpose | To screen for GDM |
|---|---|
| Procedure | – No fasting needed – Give 50g glucose orally – Blood sample taken after 1 hour |
| Interpretation | – < 140 mg/dL → Normal – ≥ 140 mg/dL → Abnormal → proceed to OGTT |
2. 💉 Oral Glucose Tolerance Test (OGTT) – Diagnostic Test
Based on WHO/IADPSG Guidelines (75g OGTT – one-step test)
| Preparation | – Fasting required (8–10 hours) <br> – Avoid heavy exercise or sugary foods 1 day prior | | Procedure | – Take fasting blood sample <br> – Administer 75g glucose orally (dissolved in 250–300 mL water) <br> – Collect blood at: <br> ➤ Fasting <br> ➤ 1 hour <br> ➤ 2 hours |
📊 WHO/IADPSG Criteria (2020):
| Time | Normal Value | GDM if ≥ |
|---|---|---|
| Fasting | ≤ 92 mg/dL | 92 mg/dL |
| 1 hour | ≤ 180 mg/dL | 180 mg/dL |
| 2 hour | ≤ 153 mg/dL | 153 mg/dL |
➡️ If any one of the above values is equal or more, GDM is diagnosed.
🧑⚕️ NURSE’S ROLE IN GTT:
🌼 Before the Test:
- Educate the woman on purpose and preparation
- Ensure fasting for 8–10 hours
- Take detailed history of risk factors (obesity, PCOS, previous GDM, macrosomic baby, family history)
- Prepare glucose solution (75g glucose in 250–300 mL water)
- Check for any vomiting tendencies or discomforts
🌼 During the Test:
- Take fasting sample
- Administer glucose solution within 5 minutes
- Monitor for nausea or vomiting
- Ensure the woman does not eat, drink (except water), or walk around during test period
- Take blood samples at 1 and 2 hours post-glucose
🌼 After the Test:
- Give light meal
- Record and document all results
- Communicate findings with doctor
- If abnormal: refer to dietician, diabetic counselor, or endocrinologist
🍽️ MANAGEMENT IF GDM IS DIAGNOSED:
- Medical Nutrition Therapy (MNT) – diet plan
- Daily glucose monitoring
- Exercise and lifestyle modification
- Insulin therapy if uncontrolled
- Close monitoring of fetal growth
- Plan for safe delivery
🧠 EDUCATION FOR MOTHER:
- Importance of taking the test even if no symptoms
- GDM can affect both mother and baby:
- Macrosomia (big baby)
- Shoulder dystocia
- Preeclampsia
- Neonatal hypoglycemia
- GDM usually resolves after delivery, but increases the risk of:
- Type 2 diabetes later in life
- GDM in future pregnancies
📝 GOVERNMENT GUIDELINES (INDIA – DIPSI Method):
- Single step test (Non-fasting)
- 75g oral glucose → Blood sugar checked after 2 hours
- If ≥ 140 mg/dL → GDM diagnosed
🔸 This method is used widely in community and rural settings.
🌸 MIDWIFERY NURSING: IMMUNIZATION DURING PREGNANCY
✅ INTRODUCTION
Immunization during pregnancy plays a critical role in:
- Protecting mother from infectious diseases
- Providing passive immunity to the newborn
- Reducing maternal and neonatal morbidity and mortality
💉 WHY IMMUNIZATION IS IMPORTANT IN PREGNANCY?
- Enhances maternal immunity
- Provides transplacental transfer of antibodies to fetus
- Prevents neonatal infections (e.g., neonatal tetanus, pertussis)
- Reduces complications from infections in pregnancy
📆 ROUTINE IMMUNIZATION SCHEDULE FOR PREGNANT WOMEN (India)
| Vaccine | When Given | Dose | Route | Purpose |
|---|---|---|---|---|
| Tetanus + Diphtheria (Td) (formerly TT) | – First dose: As early as possible after 12 weeks – Second dose: 4 weeks after the 1st dose | 0.5 mL IM | Intramuscular (Deltoid) | Prevents maternal and neonatal tetanus & diphtheria |
| Booster dose | If Td taken in last pregnancy within 3 years | 1 dose only | IM | Maintains immunity |
🔹 New Addition (Optional in India, Mandatory in Some Countries)
| Vaccine | When Given | Purpose |
|---|---|---|
| Tdap (Tetanus, Diphtheria, Pertussis) | Between 27–36 weeks (preferably before 32 weeks) | Protects mother and baby from whooping cough (pertussis) |
| Influenza Vaccine | Any trimester, preferably early in flu season | Protects against seasonal flu – reduces risk of preterm labor and complications |
| Hepatitis B (HBV) | If mother is at high risk or HBsAg negative | Prevents perinatal transmission of hepatitis B |
⚠️ VACCINES CONTRAINDICATED IN PREGNANCY:
- Live attenuated vaccines should NOT be given:
- Measles, Mumps, Rubella (MMR)
- Varicella (Chickenpox)
- Oral Polio Vaccine (OPV)
- HPV Vaccine
🔴 If accidentally given, counseling should be done. No need for termination.
🧠 EDUCATION TO PREGNANT WOMEN:
- Explain why immunization is necessary
- Assure that Td and other recommended vaccines are safe in pregnancy
- Inform about mild side effects (fever, pain at injection site)
- Encourage to bring and maintain the MCH card (Mother and Child Health card)
- Stress on timing and compliance with both doses
🧑⚕️ ROLE OF MIDWIFE/NURSE:
- Assessment:
- Check immunization history
- Determine eligibility for Td/Tdap/Influenza
- Education:
- Counsel on benefits and safety of vaccines
- Clear myths and misconceptions
- Administration:
- Use correct aseptic technique
- Maintain cold chain and expiry date checks
- Give IM injection in deltoid muscle
- Documentation:
- Record in ANC register and MCH card
- Note date, vaccine type, batch number, and site
- Follow-up:
- Remind mother for 2nd dose or booster
- Observe for any adverse reaction
📦 COLD CHAIN MAINTENANCE:
- Store vaccines between +2°C to +8°C
- Avoid exposure to sunlight and freezing
- Use vaccine carrier for field visits
🌸 MIDWIFERY NURSING: ANTENATAL ASSESSMENT
✅ INTRODUCTION
Antenatal assessment is the systematic evaluation of the pregnant woman throughout the course of her pregnancy to monitor:
- Maternal health
- Fetal development
- Early detection of complications
- Health education and counseling
This is a core function of midwifery nursing in both hospital and community settings.
📅 ANTENATAL VISIT SCHEDULE (WHO Recommended)
| Visit Number | Timing |
|---|---|
| 1st visit | Before 12 weeks (as early as possible) |
| 2nd visit | Between 14–26 weeks |
| 3rd visit | Between 28–32 weeks |
| 4th visit | Between 36–38 weeks |
🔹 High-risk pregnancies may require more frequent visits.
🧾 COMPONENTS OF ANTENATAL ASSESSMENT
1. 👩⚕️ History Taking
A. Personal History
- Name, age, marital status, address
- Occupation, dietary habits, lifestyle
B. Obstetric History (GTPAL)
- Gravida, Term, Preterm, Abortions, Living children
- Previous pregnancy outcomes
- Complications in past pregnancies
C. Medical/Surgical History
- Hypertension, diabetes, asthma, heart disease
- Surgeries (e.g., cesarean, fibroids, D&C)
D. Menstrual History
- Age at menarche, cycle regularity
- Last menstrual period (LMP)
- Estimated date of delivery (EDD) using Naegele’s Rule:
➤ LMP + 9 months + 7 days
E. Family History
- Genetic disorders, twins, hypertension, diabetes
F. Psychosocial History
- Stress, domestic violence, mental health
2. 🧍♀️ General Physical Examination
| Parameter | What to Assess |
|---|---|
| Appearance | General well-being |
| Weight | Initial and progression |
| Height | For BMI and pelvic assessment |
| Blood Pressure | Risk of preeclampsia |
| Pulse & Respirations | Vital signs |
| Pallor | Check for anemia |
| Edema | Face, hands, ankles |
| Breast Exam | Changes, readiness for breastfeeding |
| Teeth & Gums | Nutritional status, bleeding gums |
3. 📋 Obstetrical Examination
A. Abdominal Examination (after 16 weeks)
| Step | Purpose |
|---|---|
| Inspection | Shape, size, fetal movements, scars |
| Palpation (Leopold’s Maneuvers) | Determine lie, presentation, position, and engagement |
| Fundal Height (in cm) | Correlates with gestational age (after 20 weeks: cm ≈ weeks) |
| Auscultation | Fetal heart sounds with fetal Doppler or stethoscope (after 20 weeks) |
B. Pelvic Examination
- Performed only when necessary or at term
- Assess pelvic adequacy, vaginal infections, cervical status
4. 🧪 ROUTINE INVESTIGATIONS
| Test | Purpose |
|---|---|
| Hemoglobin (Hb) | Detect anemia |
| Blood Group & Rh Typing | For Rh incompatibility |
| VDRL | Syphilis screening |
| HIV, HBsAg | Prevent mother-to-child transmission |
| Urine (Albumin, Sugar, Microscopy) | Detect proteinuria (PIH), glucosuria (GDM), UTI |
| Blood Sugar / OGTT | Screening for GDM |
| Ultrasound | Dating scan, anomaly scan, fetal growth monitoring |
5. 🗣️ HEALTH EDUCATION & COUNSELING
- Importance of ANC visits
- Danger signs in pregnancy
- Nutrition and supplements (IFA, Calcium)
- Birth preparedness and complication readiness (BPCR)
- Hygiene, sleep, physical activity
- Breastfeeding and newborn care
- Immunization (Tetanus, Influenza, Tdap if applicable)
6. 📈 MONITORING FETAL GROWTH & WELL-BEING
| Method | When |
|---|---|
| Fundal height | Each visit after 20 weeks |
| Fetal movements | Starts ~18–22 weeks; mother to monitor daily |
| Fetal heart rate (FHR) | After 20 weeks (Normal = 110–160 bpm) |
| Ultrasound | Fetal growth, placental position, anomalies |
🧑⚕️ ROLE OF THE MIDWIFE/NURSE
- Assessment:
- Perform history-taking and full physical exam
- Interpret findings and identify high-risk pregnancies
- Care and Monitoring:
- Monitor vital signs, fetal development, lab reports
- Refer to doctor if any abnormal findings are observed
- Health Education:
- Provide targeted counseling based on the trimester
- Discuss danger signs and emergency readiness
- Documentation:
- Maintain ANC card and hospital record
- Ensure completeness of test results and follow-ups
- Support:
- Provide emotional support and family involvement
- Encourage open communication about discomforts or concerns
🔴 DANGER SIGNS TO WATCH FOR DURING ASSESSMENT
- Vaginal bleeding
- Severe headache, blurred vision
- Swelling of hands/face
- Reduced or absent fetal movement
- High blood pressure
- High fever or signs of infection
🌸 MIDWIFERY NURSING: Abdominal Palpation in Pregnancy
✅ INTRODUCTION
Abdominal palpation is a non-invasive clinical method used to assess the size, position, and well-being of the fetus by manually examining the pregnant woman’s abdomen.
It is a key component of antenatal assessment, especially from 24 weeks onward, and helps the midwife/nurse plan appropriate care for labor and delivery.
🎯 PURPOSE OF ABDOMINAL PALPATION
- Estimate gestational age and fetal growth
- Determine the fetal lie, presentation, and position
- Check engagement of presenting part
- Assess fetal movement and well-being
- Detect uterine abnormalities (multiple pregnancy, polyhydramnios, IUGR)
🧍♀️ PREPARATION OF MOTHER
| Step | Description |
|---|---|
| Explain | Purpose and procedure to reduce anxiety |
| Privacy | Provide privacy and maintain dignity |
| Position | Mother in supine position with knees flexed, head slightly elevated |
| Empty bladder | Ask mother to void before exam |
| Expose abdomen | Only lower abdomen exposed, cover other parts for comfort |
| Warm hands | Use warm hands to avoid discomfort |
| Stand on right side | Always stand on mother’s right side |
👋 TECHNIQUES – LEOPOLD’S MANEUVERS (4 Steps)
These are the standard steps used for abdominal palpation.
1️⃣ Leopold’s First Maneuver – Fundal Grip
| Purpose | Identify the fetal part in the fundus (head or breech) |
|---|---|
| Method | Use both hands to palpate the upper abdomen (fundus) |
| Findings |
- Round, hard, ballotable: Head
- Irregular, soft, bulky: Breech (buttocks)
2️⃣ Leopold’s Second Maneuver – Lateral Grip
| Purpose | Identify the fetal back and limbs (Lie and Position) |
|---|---|
| Method | Place hands on either side of the abdomen and palpate gently |
| Findings |
- Smooth, firm, curved surface: Back
- Irregular, nodular parts (limbs): Front side
3️⃣ Leopold’s Third Maneuver – Pawlik’s Grip
| Purpose | Identify the presenting part above the pelvic inlet |
|---|---|
| Method | Grasp the lower abdomen above the pubic symphysis with thumb and fingers |
| Findings |
- Hard, round, mobile: Head (not engaged)
- Soft, irregular: Breech
4️⃣ Leopold’s Fourth Maneuver – Pelvic Grip
| Purpose | Determine engagement of presenting part |
|---|---|
| Method | Face the mother’s feet, place both hands on lower abdomen, and press downwards |
| Findings |
- Deeply engaged: Head not easily movable
- Floating: Head can be moved side to side
🩺 AUSCULTATION OF FETAL HEART SOUND (FHS)
- Use fetoscope or Doppler
- Heard best over fetal back (after 20 weeks)
- Normal FHR: 110–160 bpm
- Always document and report abnormal FHR
📊 INTERPRETING FINDINGS
| Term | Meaning |
|---|---|
| Lie | Relationship of fetal long axis to mother’s long axis (Longitudinal, Transverse, Oblique) |
| Presentation | Part of fetus that enters pelvis first (Cephalic – head, Breech – buttocks) |
| Position | Fetal back in relation to mother’s side (LOA, ROA, LOP, etc.) |
| Engagement | When widest part of fetal head enters the pelvic inlet |
⚠️ ABNORMAL FINDINGS TO WATCH FOR
- Transverse lie → may need cesarean
- Breech presentation → refer for ECV or specialist opinion
- Polyhydramnios/oligohydramnios
- Multiple pregnancy
- Intrauterine growth restriction (IUGR)
🧑⚕️ MIDWIFE/NURSE’S ROLE
- Performing palpation skillfully and gently
- Educating the mother about fetal position
- Recording findings in ANC card
- Reporting abnormalities to doctor
- Reassuring the mother, especially if fetal movements are decreased
- Teaching mothers to monitor kick counts at home
🌸FETAL ASSESSMENT DURING PREGNANCY
✅ INTRODUCTION
Fetal assessment is the process of monitoring the growth, development, position, and well-being of the fetus during pregnancy. It ensures that the fetus is developing normally and helps detect any risks early to plan proper care.
Midwives and nurses play a vital role in regular fetal monitoring as part of antenatal care.
🩺 PURPOSE OF FETAL ASSESSMENT
- Monitor fetal growth and gestational development
- Detect fetal distress, anomalies, or growth restriction
- Assess fetal position and presentation for delivery planning
- Evaluate placental function and amniotic fluid levels
📋 METHODS OF FETAL ASSESSMENT (ANTENATAL)
1. 🗓️ Fundal Height Measurement
| When | From 20 weeks onward |
|---|---|
| How | Measure from pubic symphysis to uterine fundus using tape |
| Normal | Fundal height in cm ≈ gestational age in weeks (± 2 cm) |
| Abnormal | Discrepancy may indicate IUGR, multiple pregnancy, or poly/oligohydramnios |
2. 👶 Fetal Movement Monitoring (Quickening)
| Felt by mother | 18–22 weeks (earlier in multigravida) | | Purpose | Indicates fetal well-being | | Kick Count Method | 10 movements in 12 hours (or 4 in 1 hour) | | Nurse’s Role | Educate mother to monitor movements daily and report decreased movements |
3. 🧏♀️ Auscultation of Fetal Heart Rate (FHR)
| Instrument | Fetoscope or Doppler | | Heard from | Around 18–20 weeks with fetoscope, earlier with Doppler | | Normal Range | 110–160 bpm | | Abnormal | Bradycardia (<110), Tachycardia (>160) → may indicate fetal distress | | Nurse’s Role | Check FHR during each antenatal visit and report abnormalities immediately |
4. 🤰 Abdominal Palpation (Leopold’s Maneuvers)
| Purpose | Assess fetal lie, presentation, position, and engagement | | Useful for | Planning type of delivery | | Nurse’s Role | Perform palpation gently and interpret findings accurately |
5. 📺 Ultrasound Examination
| Early USG (dating scan) | 6–12 weeks: confirms gestational age, viability | | Anomaly Scan | 18–22 weeks: detects structural abnormalities | | Growth Scan | 28–34 weeks: checks fetal size, position, amniotic fluid, placenta | | Nurse’s Role | Prepare mother, provide emotional support, explain procedure |
6. 🩸 Biochemical Tests (Screening Tests)
| Triple/Quadruple Marker Test | Done between 15–20 weeks | | Purpose | Detect neural tube defects, Down syndrome, Trisomy 18 | | Nurse’s Role | Counsel mother on the purpose, ensure timely testing, and assist in follow-up for abnormal results |
7. 💉 Non-Stress Test (NST) – For High-Risk Pregnancies
| Done when | Reduced fetal movement, hypertension, diabetes, IUGR | | Method | Electronic fetal monitor records FHR in response to fetal movements | | Normal (Reactive) | 2 or more accelerations in 20 minutes | | Abnormal (Non-reactive) | May indicate fetal hypoxia or sleep cycle |
8. 💧 Amniotic Fluid Index (AFI)
| Done via | Ultrasound | | Normal Range | 8–18 cm | | < 5 cm | Oligohydramnios – risk of fetal distress, cord compression | | > 24 cm | Polyhydramnios – risk of preterm labor, congenital defects |
9. 🧪 Doppler Study (Advanced)
| Purpose | Measures blood flow in umbilical artery and placenta | | Used in | Suspected IUGR, hypertension, preeclampsia | | Nurse’s Role | Refer for timely scan, explain importance to mother |
🚨 SIGNS OF FETAL DISTRESS (TO WATCH FOR):
- Decreased or absent fetal movements
- Abnormal fetal heart rate
- Abnormal Doppler flow
- Oligohydramnios
- Abnormal NST
➡️ Immediate medical evaluation and management required.
🧑⚕️ NURSE’S/MIDWIFE’S RESPONSIBILITIES
- Perform and record routine fetal assessments
- Educate mother about kick counts and danger signs
- Support during ultrasound, NST, and other procedures
- Maintain accurate antenatal documentation
- Refer to doctor if any abnormal fetal findings
- Provide emotional reassurance to anxious mothers
🌸Auscultation of Fetal Heart Rate (FHR)
✅ INTRODUCTION
Auscultation of the fetal heart rate is a non-invasive, essential clinical skill used to assess fetal well-being during pregnancy and labor. It provides valuable information about the fetal condition and helps identify signs of distress early.
🎯 PURPOSE OF FHR AUSCULTATION
- Confirm fetal viability
- Monitor fetal well-being
- Detect fetal distress or abnormal heart rate
- Support decision-making regarding labor and delivery
🕰️ TIMING OF AUSCULTATION
| Period | When to Auscultate |
|---|---|
| Antenatal period | From 18–20 weeks (earlier with Doppler) at every ANC visit |
| During labor | Every 30 minutes in 1st stage, every 5–15 minutes in 2nd stage (or as per protocol) |
🛠️ EQUIPMENT USED
| Instrument | Description |
|---|---|
| Pinard Fetoscope | Trumpet-shaped instrument used from 18–20 weeks onward |
| Handheld Doppler | Uses ultrasound waves; can detect FHR as early as 10–12 weeks |
| CTG (Cardiotocography) | For continuous monitoring in high-risk pregnancies or labor |
🧍♀️ PREPARATION OF MOTHER
- Explain the procedure to reassure and gain cooperation
- Provide privacy
- Position: Semi-recumbent or supine with knees flexed
- Ensure the abdomen is exposed from the pubic area to the fundus
- Ask the mother to empty her bladder
📍 LOCATING FHR FOR AUSCULTATION
- Best heard over the fetal back, depending on fetal position
- Use Leopold’s maneuvers to determine fetal lie and position before auscultating
| Presentation | FHR Best Heard |
|---|---|
| Cephalic (LOA/ROA) | Below umbilicus, left or right side |
| Breech | Above umbilicus |
| Transverse lie | Near the flank |
👂 PROCEDURE
Using Pinard Fetoscope:
- Warm the fetoscope before use
- Place the wide end firmly on the mother’s abdomen
- Ask mother to remain quiet and still
- Listen for rhythmic “tick-tick” or “lub-dub” sound
- Count for 1 full minute
- Record the rate in beats per minute (bpm)
Using Handheld Doppler:
- Apply ultrasound gel to the area
- Turn on Doppler device
- Place probe over fetal back area
- Listen and adjust position until a clear heart sound is heard
- Count bpm or note device reading
- Clean the probe and remove gel after use
📊 NORMAL & ABNORMAL FHR VALUES
| Parameter | Value |
|---|---|
| Normal FHR | 110–160 bpm |
| Tachycardia | >160 bpm |
| Bradycardia | <110 bpm |
➡️ Abnormal values may indicate:
- Fetal distress
- Umbilical cord compression
- Maternal fever, anemia, dehydration
🧑⚕️ NURSE’S / MIDWIFE’S ROLE
- Perform FHR auscultation at each ANC visit
- Use Leopold’s maneuvers to locate fetal back
- Document findings: rate, rhythm, clarity, and location
- Educate mother on fetal movement and danger signs
- Report abnormal FHR immediately to obstetrician
- Monitor FHR closely during labor and high-risk situations
🔴 WHEN TO REFER OR ALERT DOCTOR
- FHR consistently <110 or >160 bpm
- Irregular rhythm
- Absent FHR
- Accompanied by decreased fetal movements or bleeding
🌸DOPPLER vs. PINARD’S STETHOSCOPE

(For Auscultation of Fetal Heart Rate)
✅ INTRODUCTION
Both the Doppler device and Pinard’s stethoscope are used to auscultate the fetal heart sounds during pregnancy and labor. They help assess fetal well-being and detect fetal distress.
Midwives and nurses must be skilled in using both, depending on the setting, availability, and gestational age.
🔍 1. PINARD’S STETHOSCOPE
📌 Description:
- A non-electronic, trumpet-shaped instrument made of metal, wood, or plastic.
- Used for manual auscultation of fetal heart sounds.
📅 When to Use:
- After 18–20 weeks of gestation (when FHR is audible through the abdominal wall)
✅ Advantages:
- No electricity or batteries required
- Inexpensive and durable
- Easy to clean and sterilize
- Promotes close physical contact, improving mother–midwife bonding
❌ Limitations:
- Requires training and skill to use properly
- May be difficult in obese mothers, anterior placenta, or noisy environments
- Cannot be used before 18 weeks
- No visual display or printout
🔍 2. DOPPLER FETAL MONITOR
📌 Description:
- A handheld ultrasound device that uses Doppler effect to detect and amplify fetal heart sounds.
- Has a digital display and/or speaker.
📅 When to Use:
- Detects FHR as early as 10–12 weeks
- Useful throughout pregnancy and during labor monitoring
✅ Advantages:
- Detects FHR early in pregnancy
- Louder, clearer sound
- Has digital display (bpm) for easy reading
- More comfortable and reassuring for the mother
- Effective in obese women or those with thick abdominal walls
❌ Limitations:
- Requires batteries or power
- More expensive than Pinard
- Needs gel application
- Less practical in low-resource/rural settings
🧾 COMPARISON TABLE
| Feature | Pinard’s Stethoscope | Doppler Fetal Monitor |
|---|---|---|
| Type | Manual | Electronic |
| Usable from | 18–20 weeks | 10–12 weeks |
| Power Source | None | Battery/electric |
| Cost | Very low | Moderate to high |
| Training Required | Moderate | Minimal |
| Display of FHR | No | Yes (digital display) |
| Use in noisy settings | Difficult | Easier |
| Useful in obese women | Less effective | More effective |
| Community/Rural Use | Excellent | Limited by power supply |
| Infection Control | Easy to disinfect | Requires cleaning of probe and gel |
🧑⚕️ NURSE’S/MIDWIFE’S ROLE:
- Know when and how to use each tool
- Educate mother about fetal heart sounds
- Maintain equipment hygiene and functionality
- Record:
- FHR (beats per minute)
- Time and date
- Position of fetus (LOA, ROA, etc.)
- Report any abnormal FHR or absence of fetal heart sounds
🌸ASSESSMENT OF FETAL WELL-BEING
✅ INTRODUCTION:
Fetal well-being assessment refers to the evaluation of the health status of the fetus in the uterus to ensure that it is growing normally and not in distress. It is a vital component of antenatal care, helping to reduce maternal and neonatal morbidity and mortality.
Midwives and nurses play a crucial role in early detection of fetal compromise through clinical skills, observation, and proper use of tools and techniques.
🎯 GOALS OF FETAL WELL-BEING ASSESSMENT:
- Confirm fetal viability and normal development
- Detect signs of fetal compromise or hypoxia
- Monitor growth and amniotic fluid volume
- Prevent complications such as stillbirth, IUGR, fetal distress
- Decide timing and mode of delivery in high-risk pregnancies
📆 WHEN TO ASSESS FETAL WELL-BEING?
- Routine assessments during every ANC visit
- More frequent in high-risk pregnancies, including:
- Hypertension
- Diabetes
- Previous stillbirth
- IUGR
- Rh incompatibility
- Decreased fetal movements
📋 METHODS OF FETAL WELL-BEING ASSESSMENT:
1. 🧍♀️ Fundal Height Measurement
| When | From 20 weeks onward |
|---|---|
| How | Measure from symphysis pubis to uterine fundus in cm |
| Interpretation | Fundal height (cm) ≈ gestational age (weeks) ±2 |
| Deviation | May indicate IUGR, macrosomia, polyhydramnios or oligohydramnios |
2. 🤰 Fetal Movement Monitoring (Kick Count)
| When Felt | ~18–20 weeks (earlier in multigravida) | | Method | Count fetal kicks: ≥10 movements in 12 hours or ≥4 in 1 hour | | Importance | Decreased movement can be an early sign of fetal hypoxia | | Nurse’s Role | Teach mother how to perform daily kick counts; report if <10 in 12 hrs |
3. 🩺 Fetal Heart Rate Monitoring (Auscultation)
| Instrument | Pinard stethoscope or Doppler | | Normal FHR | 110–160 bpm | | Abnormal | <110 (bradycardia), >160 (tachycardia) → Possible fetal distress | | Nurse’s Role | Auscultate FHR during each ANC visit and report abnormalities immediately |
4. 📺 Ultrasonography (USG)
a. Early Pregnancy Scan (Dating scan)
✔ Confirms viability, gestational age, and number of fetuses
b. Anomaly Scan (18–22 weeks)
✔ Detects congenital structural abnormalities
c. Growth Scan (28–34 weeks)
✔ Measures fetal weight, growth pattern, position, amniotic fluid
d. Biophysical Profile (BPP)
Assesses 5 parameters on USG:
| Parameter | Normal Score (2 points each) |
|---|---|
| Fetal movement | ≥3 movements |
| Fetal tone | ≥1 extension/flexion |
| Fetal breathing | ≥30 seconds |
| Amniotic fluid | ≥2 cm pocket |
| Non-Stress Test | Reactive |
✔ Total score: 8–10 = Normal; 6 = equivocal; ≤4 = abnormal
5. 💧 Amniotic Fluid Index (AFI)
| Normal | 8–18 cm | | <5 cm | Oligohydramnios (risk of fetal distress, cord compression) | | >24 cm | Polyhydramnios (risk of macrosomia, preterm labor) |
✔ Measured via ultrasound
6. 📉 Non-Stress Test (NST)
| Purpose | Monitors FHR response to fetal movement | | Method | External monitor placed on mother’s abdomen for 20 minutes | | Reactive (Normal) | ≥2 accelerations of ≥15 bpm lasting ≥15 seconds | | Non-Reactive | No acceleration → may need further evaluation (BPP, Doppler) | | Use | Done in high-risk cases or after reduced fetal movement |
7. 🧪 Doppler Flow Studies
| Use | Measures blood flow in umbilical artery and fetal vessels | | Purpose | Detect placental insufficiency in cases like IUGR, preeclampsia | | Interpretation | Abnormal flow indicates fetal compromise or hypoxia |
🧑⚕️ ROLE OF NURSE / MIDWIFE IN FETAL WELL-BEING ASSESSMENT:
- Assess fetal growth and development at every ANC visit
- Perform and interpret fundal height, FHR, fetal movement
- Educate the mother on fetal kick count and when to report abnormalities
- Assist with ultrasound, NST, Doppler as per doctor’s orders
- Record all findings accurately in ANC register/card
- Refer to higher center if signs of fetal compromise are present
- Provide emotional support to mother, especially in high-risk cases
🚨 DANGER SIGNS INDICATING FETAL DISTRESS:
- Decreased or absent fetal movement
- Abnormal FHR
- Poor fundal height growth
- Non-reactive NST
- Reduced amniotic fluid
- Intrauterine growth restriction (IUGR)
🌸DFMC – Daily Fetal Movement Count.
✅ INTRODUCTION:
DFMC (Daily Fetal Movement Count) is a simple, non-invasive, and effective method used to assess fetal well-being by counting fetal movements felt by the mother. It helps detect early signs of fetal distress or hypoxia, especially in the third trimester.
It is one of the most cost-effective self-monitoring tools for pregnant women.
🎯 PURPOSE OF DFMC:
- Detect decreased fetal activity, an early sign of fetal compromise
- Promote maternal-fetal bonding
- Empower the mother to be actively involved in fetal monitoring
- Prevent stillbirth or intrauterine death
📅 WHEN TO START DFMC?
- Generally recommended from 28 weeks of gestation onward
- Especially important in high-risk pregnancies:
- Hypertension, diabetes
- IUGR (Intrauterine Growth Restriction)
- Oligohydramnios
- Decreased fetal movements previously
- Previous stillbirth
🧾 METHODS OF COUNTING FETAL MOVEMENTS:
1️⃣ Cardiff “Count to Ten” Method (Most commonly used)
| Method | The mother counts fetal movements until 10 movements are felt | | Recommended Time | Same time daily (after a meal, when relaxed) | | Normal | 10 movements felt within 12 hours (usually within 1–2 hrs) | | Abnormal | Less than 10 movements in 12 hours → report to healthcare provider immediately |
2️⃣ Modified Count Method (2-Hour Method)
| Method | The mother lies on her side and counts movements for 2 hours after a meal | | Normal | At least 4 movements in 2 hours | | Abnormal | Less than 4 movements → further evaluation needed (NST or ultrasound) |
🧍♀️ INSTRUCTIONS TO THE MOTHER:
- Choose a quiet time daily (after food or in the evening)
- Sit comfortably or lie on left side
- Count and record every kick, roll, or flutter
- Maintain a kick count chart or notebook
- If movements are less than normal or suddenly decrease → report immediately
📝 SAMPLE DFMC CHART:
| Date | Start Time | No. of Movements | Time to Reach 10 Kicks | Remarks |
|---|---|---|---|---|
| 01/04/2025 | 9:00 AM | 10 | By 10:45 AM | Normal |
| 02/04/2025 | 9:00 AM | 6 | Till 12:00 PM | Needs evaluation |
🔴 ABNORMAL FINDINGS:
- Less than 10 movements in 12 hours
- Gradual or sudden decrease in usual pattern
- No movement felt for several hours
- Accompanied by other danger signs (bleeding, pain, leaking, headache)
➡️ Refer immediately for NST, ultrasound, or further evaluation
🧑⚕️ ROLE OF NURSE / MIDWIFE:
- Educate pregnant women on how and why to do DFMC
- Demonstrate the correct way to count and record movements
- Provide chart or sample format to record daily movements
- Reinforce during each ANC visit
- Take immediate action if mother reports decreased or absent fetal movement
- Offer emotional support, especially if mother is anxious or unsure
🌸BIOPHYSICAL PROFILE (BPP)
✅ INTRODUCTION
The Biophysical Profile (BPP) is a comprehensive, non-invasive test used to assess fetal well-being, especially in the third trimester or in high-risk pregnancies. It combines ultrasound findings and fetal heart rate monitoring to evaluate if the fetus is receiving adequate oxygen and nutrition.
🎯 PURPOSE OF BPP:
- Detect fetal hypoxia or distress
- Assess fetal central nervous system activity
- Decide the timing of delivery in high-risk pregnancies
- Prevent complications like stillbirth or intrauterine growth restriction (IUGR)
📅 INDICATIONS FOR BPP:
- Decreased fetal movement
- Prolonged pregnancy (> 40 weeks)
- Gestational diabetes mellitus (GDM)
- Pregnancy-induced hypertension (PIH)
- Intrauterine growth restriction (IUGR)
- Oligohydramnios or polyhydramnios
- Previous stillbirth
- Rh incompatibility
- Non-reactive NST (non-stress test)
📋 COMPONENTS OF BIOPHYSICAL PROFILE (5 Parameters):
Each parameter is assessed by ultrasound (except NST) and scored as either:
- 2 points = Normal
- 0 points = Abnormal
| Component | Criteria (Normal = 2 points) | Abnormal = 0 points |
|---|---|---|
| 1. Fetal Breathing Movements | At least 1 episode of rhythmic breathing lasting 30 seconds in 30 minutes | Absent or less than 30 seconds |
| 2. Gross Body Movements | At least 3 discrete body/limb movements in 30 minutes | Less than 3 |
| 3. Fetal Tone | At least 1 episode of extension/flexion of limbs or spine | Slow extension, no flexion |
| 4. Amniotic Fluid Volume (AFI or single pocket) | At least 1 vertical pocket of fluid ≥ 2 cm or AFI ≥ 5 cm | No pocket or < 2 cm |
| 5. Non-Stress Test (NST) | Reactive – 2 accelerations in 20 minutes | Non-reactive NST |
📊 TOTAL BPP SCORING:
| Score (Out of 10) | Interpretation | Action |
|---|---|---|
| 8–10 | Normal | Reassure, repeat weekly |
| 6 | Equivocal/Suspicious | Repeat BPP in 12–24 hours or do further testing |
| 4 or less | Abnormal (possible fetal distress) | Immediate evaluation and consider delivery |
🛠️ HOW BPP IS PERFORMED:
- Ultrasound is used to assess 4 parameters (breathing, movement, tone, amniotic fluid)
- Non-Stress Test (NST) is done using external fetal monitors
- Entire test takes 30 minutes to 1 hour
- Performed in tertiary care or diagnostic centers by trained personnel
🧑⚕️ ROLE OF MIDWIFE / NURSE:
- Preparation:
- Explain procedure to the mother and provide emotional support
- Ensure she has eaten something light before the test (for better fetal activity)
- Position mother comfortably
- During Procedure:
- Assist radiologist or doctor during ultrasound
- Help apply NST belts and monitor FHR for 20 minutes
- Encourage mother to relax and remain still
- After Procedure:
- Record and report the score
- Provide guidance based on the result
- If score is low, ensure referral and follow-up for emergency evaluation or delivery
- Educate the Mother:
- Teach about the importance of fetal movement and timely testing
- Reassure during normal results and counsel on warning signs
🔴 WHEN TO ALERT THE DOCTOR:
- Total BPP score is 4 or less
- Decreased fetal movement continues
- Non-reactive NST
- Abnormal amniotic fluid volume
🌸 NON-STRESS TEST (NST)
✅ INTRODUCTION:
The Non-Stress Test (NST) is a non-invasive, painless, and safe procedure used to assess fetal well-being by monitoring the fetal heart rate (FHR) in response to fetal movements.
It is called “non-stress” because no stress is applied to the fetus (like uterine contractions), unlike the contraction stress test.
🎯 PURPOSE OF NST:
- Evaluate the oxygenation and neurological function of the fetus
- Detect fetal hypoxia or distress early
- Assess placental function
- Help decide timing of delivery, especially in high-risk pregnancies
📆 WHEN IS NST DONE?
Usually performed in the third trimester (after 28 weeks), especially in:
- Decreased fetal movements
- Hypertension or preeclampsia
- Diabetes mellitus
- Post-dated pregnancy (beyond 40 weeks)
- Intrauterine growth restriction (IUGR)
- Multiple pregnancy
- Rh isoimmunization
- Previous stillbirth or miscarriage
- Oligohydramnios/polyhydramnios
🛠️ EQUIPMENT NEEDED:
- Cardiotocograph (CTG) machine
- With 2 external transducers:
- Ultrasound transducer (for fetal heart rate)
- Tocodynamometer (for uterine activity)
- With 2 external transducers:
- Gel, belts, watch/timer, bed or reclining chair
🧍♀️ PREPARATION OF THE MOTHER:
- Explain the procedure and obtain consent
- Ask the mother to eat a light meal before the test (to stimulate fetal activity)
- Encourage her to empty her bladder
- Position her in semi-Fowler’s or left lateral position
- Apply gel and secure the transducers on the abdomen
👩⚕️ PROCEDURE OF NST:
- Attach the FHR transducer and uterine activity transducer to the abdomen.
- Ask the mother to press a button every time she feels fetal movement.
- Monitor and record the fetal heart rate and uterine activity for 20 minutes (may be extended to 40 minutes if needed).
- Save or print the CTG strip.
📊 INTERPRETATION OF NST:
| NST Result | Criteria | Interpretation |
|---|---|---|
| Reactive NST (Normal) | – At least 2 accelerations in 20 minutes – Each acceleration: ≥15 bpm above baseline, lasting ≥15 seconds | ✅ Reassuring Normal fetal oxygenation |
| Non-Reactive NST | – No accelerations or – Accelerations do not meet above criteria | ⚠️ Needs further evaluation May indicate fetal distress or sleep cycle |
| Unsatisfactory/Incomplete | – Poor tracing quality – Unable to interpret results | ❌ Repeat NST or perform Biophysical Profile (BPP) |
📍 OTHER OBSERVATIONS ON NST:
- Baseline FHR: 110–160 bpm
- Variability: Moderate variability (6–25 bpm) is normal
- No decelerations: Late or variable decelerations may suggest hypoxia
🧑⚕️ NURSE / MIDWIFE’S RESPONSIBILITIES:
🌼 Before the Test:
- Explain the purpose, gain trust
- Ensure privacy and comfort
- Check that the mother has eaten
- Ask about fetal movement and any recent concerns
🌼 During the Test:
- Monitor fetal movements
- Check the CTG machine for proper tracing
- Reassure the mother throughout
- If fetus is inactive, try gentle stimulation (change position, juice intake)
🌼 After the Test:
- Interpret and record findings
- Report non-reactive or abnormal NST immediately to the obstetrician
- Document date, time, results, and mother’s condition
- If reactive, reassure the mother and schedule the next follow-up
- Advise kick counts and to report decreased fetal movement
📝 DOCUMENTATION FORMAT:
| Parameter | Observation |
|---|---|
| FHR baseline | 140 bpm |
| Variability | Moderate |
| Accelerations | 2 accelerations present |
| Decelerations | Absent |
| Fetal movements felt | 4 |
| Result | Reactive |
| Action Taken | No further intervention needed |
🌸 CARDIOTOCOGRAPHY (CTG)
(Also known as Electronic Fetal Monitoring – EFM)
✅ INTRODUCTION
Cardiotocography (CTG) is a non-invasive procedure used to monitor fetal heart rate (FHR) and uterine contractions simultaneously. It helps assess fetal well-being, especially during the third trimester and labor.
It is a vital tool in high-risk pregnancies and labor monitoring to detect early signs of fetal distress.
🧠 PURPOSE OF CTG:
- Monitor baseline fetal heart rate
- Evaluate fetal response to uterine contractions
- Detect fetal distress/hypoxia
- Monitor uterine contraction pattern
- Help guide decisions about timing and mode of delivery
📅 WHEN IS CTG USED?
During Antenatal Period:
- High-risk pregnancy (PIH, GDM, IUGR, Rh incompatibility)
- Decreased fetal movement
- Post-dated pregnancy (>40 weeks)
- Non-reactive NST
- Suspected placental insufficiency
During Intrapartum Period:
- To monitor fetal response during labor
- Induction of labor or oxytocin use
- Meconium-stained liquor
- Previous cesarean section
- Multiple gestation
🛠️ EQUIPMENT USED:
- CTG Machine with:
- Ultrasound transducer – to monitor FHR
- Tocodynamometer – to monitor uterine contractions
- Gel
- Belts or straps
🧍♀️ PREPARATION OF THE MOTHER:
- Explain procedure to obtain consent
- Ensure the mother has emptied her bladder
- Position: Semi-recumbent or left lateral
- Apply gel to abdomen and fix both probes:
- Ultrasound transducer over fetal back (detected via Leopold’s maneuvers)
- Toco probe over uterine fundus (where contractions are felt)
📋 PARAMETERS MONITORED:
1. Fetal Heart Rate (FHR)
| Normal Baseline | 110–160 bpm | | Tachycardia | >160 bpm | | Bradycardia | <110 bpm |
2. Baseline Variability
(The beat-to-beat fluctuation of FHR)
| Normal | 6–25 bpm variability | | Absent or Minimal | <5 bpm → Possible hypoxia/sleep | | Marked | >25 bpm → May be due to fetal activity or distress |
3. Accelerations
- Sudden ↑ in FHR by ≥15 bpm lasting ≥15 seconds
- Sign of fetal well-being
4. Decelerations
- Drop in FHR; may indicate cord compression or hypoxia
| Type | Meaning |
|---|---|
| Early | Normal, due to head compression |
| Late | Abnormal, due to uteroplacental insufficiency |
| Variable | Cord compression – may need intervention |
5. Uterine Contractions
- Frequency, duration, intensity (measured in mmHg on monitor)
📊 INTERPRETATION OF CTG (3-Tier System – FIGO/WHO)
| CTG Category | Features | Clinical Action |
|---|---|---|
| Normal | Baseline 110–160 bpm, moderate variability, no late decels | Continue routine monitoring |
| Suspicious | One abnormal feature (e.g., mild bradycardia, reduced variability) | Closer observation, repeat test |
| Pathological | Persistent bradycardia, absent variability, late decels | Urgent intervention or delivery |
🧑⚕️ ROLE OF NURSE / MIDWIFE:
- Preparation:
- Explain and reassure the mother
- Ensure comfortable positioning
- Apply transducers correctly
- Monitoring:
- Monitor FHR and contractions for at least 20–30 minutes
- Observe and record any abnormal patterns
- Note fetal movements during the trace
- Documentation:
- Record date, time, FHR, variability, accelerations, decelerations, uterine activity
- Keep printed CTG strip in patient’s file
- Action:
- Inform obstetrician immediately if abnormal CTG
- Assist with further evaluation (BPP, emergency delivery)
- Provide emotional support to anxious mothers
🛑 WHEN TO REPORT IMMEDIATELY:
- FHR <110 or >160 bpm
- No variability
- Late decelerations
- Prolonged contractions or hyperstimulation
🌸 USG – Ultrasonography in Pregnancy
✅ INTRODUCTION
Ultrasonography (USG) is a safe, non-invasive, and widely used imaging technique in obstetrics. It uses high-frequency sound waves to create images of the developing fetus, placenta, uterus, and surrounding structures.
USG is an essential tool in antenatal care for assessing fetal development, detecting abnormalities, and guiding decisions throughout pregnancy.
🎯 PURPOSE OF USG IN PREGNANCY:
- Confirm pregnancy and viability
- Determine gestational age and EDD
- Monitor fetal growth and position
- Detect congenital anomalies
- Assess placental location and amniotic fluid
- Diagnose multiple pregnancy
- Identify complications (IUGR, ectopic, molar pregnancy, etc.)
📅 TYPES & TIMING OF ROUTINE USGs:
| Scan | Timing | Purpose |
|---|---|---|
| Dating Scan (Early Pregnancy Scan) | 6–9 weeks | Confirm viability, rule out ectopic pregnancy, assess crown-rump length (CRL) for dating |
| NT Scan (Nuchal Translucency) | 11–14 weeks | Screen for chromosomal abnormalities (Down syndrome, Trisomy 18) |
| Anomaly Scan (Level II) | 18–22 weeks | Detect structural abnormalities (brain, heart, spine, kidneys, limbs) |
| Growth Scan | 28–32 weeks | Assess fetal size, weight, growth pattern, and well-being |
| Term Scan | 36–38 weeks | Confirm fetal position, placental site, and amniotic fluid volume |
| Other USGs | As needed | For complications like bleeding, pain, IUGR, PIH, or previous history of loss |
🧪 SPECIALIZED TYPES OF USG:
| Type | Use |
|---|---|
| Transvaginal USG (TVS) | Early pregnancy, cervical length |
| Doppler USG | Assesses blood flow in umbilical artery and fetal vessels |
| 3D/4D USG | Better visualization of fetal anomalies and movement |
📊 KEY ASSESSMENTS IN USG:
| Parameter | What It Shows |
|---|---|
| Fetal Heartbeat | Viability (usually visible by 6–7 weeks) |
| Gestational Age | Based on CRL, BPD, FL, HC, AC |
| Fetal Number | Singleton or twins/triplets |
| Fetal Position | Cephalic, breech, transverse |
| Fetal Weight and Growth | Assessed in later trimesters |
| Amniotic Fluid Index (AFI) | Normal: 8–18 cm Oligohydramnios: <5 cm Polyhydramnios: >24 cm |
| Placental Location | Anterior, posterior, fundal, low-lying (placenta previa) |
| Structural Anomalies | Cleft lip, neural tube defects, cardiac anomalies, limb deformities |
🧑⚕️ ROLE OF NURSE / MIDWIFE IN USG:
🌼 Before the USG:
- Educate the mother about the purpose of the scan
- Instruct about bladder filling if needed (for early transabdominal USG)
- Provide emotional support, especially in anxious mothers
- Review any prior test reports
🌼 During the USG:
- Assist in positioning the mother
- Help apply gel and ensure privacy
- Support the radiologist or sonographer if needed
- Calm and reassure the mother throughout the procedure
🌼 After the USG:
- Ensure mother understands results (as appropriate)
- Document USG findings in ANC card and records
- Guide next steps if abnormalities are suspected (referral, follow-up scans)
- Reinforce kick count monitoring and follow-up appointments
⚠️ WHEN TO ALERT DOCTOR:
- No fetal heartbeat after 7 weeks
- Low-lying placenta or placenta previa
- Major congenital anomalies
- Abnormal growth or IUGR
- Reduced amniotic fluid
- Non-cephalic presentation near term
✅ SAFETY OF USG:
- No ionizing radiation
- Safe in all trimesters
- Can be repeated as clinically indicated
- Transvaginal USG is safe and more accurate in early pregnancy
🌸 VIBROACOUSTIC STIMULATION (VAS)
✅ INTRODUCTION
Vibroacoustic Stimulation (VAS) is a non-invasive procedure used to stimulate the fetus using sound and vibration to provoke a fetal heart rate (FHR) acceleration. It is mainly used to assess fetal well-being and confirm fetal reactivity during a non-stress test (NST).
🎯 PURPOSE OF VAS:
- To stimulate fetal movement during a non-reactive NST
- Confirm the presence of fetal reactivity
- Reduce the need for extended monitoring or more invasive tests
- Differentiate between fetal sleep and hypoxia
- Assist in intrapartum fetal assessment
📅 WHEN IS VAS INDICATED?
- During a non-reactive NST (no accelerations within 20 minutes)
- In high-risk pregnancies where quick reassurance of fetal well-being is needed
- To stimulate fetal activity for better FHR evaluation
- Sometimes during labor to assess fetal response
🛠️ EQUIPMENT REQUIRED:
- VAS device (artificial larynx or acoustic stimulator)
- CTG/NST machine (cardiotocograph)
- Conductive gel (if needed)
- Watch/timer
🧍♀️ PREPARATION OF THE MOTHER:
- Explain the purpose of the procedure
- Ensure the mother is in a semi-recumbent or left lateral position
- Ask the mother to report fetal movements
- Place the FHR transducer using Leopold’s maneuver to locate fetal back
👩⚕️ PROCEDURE OF VAS:
- Apply the CTG transducer and ensure baseline FHR tracing is obtained.
- Place the VAS device over the fetal head area (usually over the fetal back) on the maternal abdomen.
- Deliver sound stimulus for 1–3 seconds.
- Repeat stimulus up to 3 times, at 1-minute intervals, if no response is noted.
- Monitor the fetal heart rate for 5–10 minutes after stimulation.
📊 INTERPRETATION OF VAS:
| Fetal Response | Interpretation |
|---|---|
| Acceleration of FHR ≥15 bpm lasting ≥15 seconds within 15–20 minutes | ✅ Reactive – reassuring |
| No acceleration or poor variability even after 3 attempts | ⚠️ Non-reactive – possible hypoxia or fetal compromise Requires further evaluation (BPP, Doppler, delivery if needed) |
📌 CONTRAINDICATIONS:
- Known fetal hearing loss
- Preterm pregnancy (<32 weeks) due to immature auditory system
- Known congenital malformations
- Placenta previa, unexplained vaginal bleeding
- Intrauterine infection or chorioamnionitis
🧑⚕️ ROLE OF NURSE / MIDWIFE:
🌼 Before the Procedure:
- Explain the procedure and gain cooperation
- Ensure CTG setup is functioning
- Perform Leopold’s maneuver to locate fetal back
🌼 During the Procedure:
- Correctly apply VAS device and limit stimulation to <3 seconds
- Observe and record FHR response
- Do not overuse stimulation to avoid fetal stress
🌼 After the Procedure:
- Continue CTG tracing for 10–20 minutes
- Interpret findings: Was the NST reactive after VAS?
- Record in ANC/labor record
- Report non-reactive VAS results to the obstetrician
✅ ADVANTAGES OF VAS:
- Quick and safe test
- Reduces false-positive non-reactive NSTs
- Improves accuracy of fetal surveillance
- Non-invasive and easy to perform
❌ LIMITATIONS:
- May not be effective if the fetus is compromised
- Can cause temporary fetal tachycardia if overused
- Should not be used indiscriminately
🌸 BIOCHEMICAL TESTS IN PREGNANCY
✅ INTRODUCTION:
Biochemical tests during pregnancy are essential for:
- Monitoring the health of the mother
- Screening for fetal abnormalities
- Detecting maternal infections and metabolic disorders
- Guiding timely medical or obstetric interventions
These tests typically involve analysis of blood, urine, and other body fluids to evaluate physiological changes and screen for diseases.
📅 TRIMESTER-WISE BIOCHEMICAL TESTS:
🩸 FIRST TRIMESTER (Up to 12 weeks)
| Test | Purpose |
|---|---|
| Hemoglobin (Hb%) | Detect anemia |
| Blood Group & Rh Typing | Identify Rh incompatibility |
| Blood Sugar (FBS/RBS) | Screen for undiagnosed diabetes |
| HIV, HBsAg, VDRL | Screen for infections (as per PPTCT guidelines) |
| Urine Routine & Microscopy | Detect proteinuria, UTI, glucose |
| Thyroid Function Test (TSH, T3, T4) | Assess thyroid health (especially in high-risk pregnancies) |
| Serum Creatinine & Urea | Assess kidney function |
| Serum Bilirubin, LFTs | If liver disease is suspected |
| Rubella IgG, Toxoplasma IgM, CMV, HSV (TORCH Panel) (if indicated) | Screen for infections causing fetal malformations |
🧪 SECOND TRIMESTER (13–28 weeks)
| Test | Purpose |
|---|---|
| Triple Marker Test (AFP, hCG, Estriol) | Screening for Down syndrome, Trisomy 18, Neural Tube Defects |
| Quadruple Marker Test (Adds Inhibin-A) | More accurate screening than triple marker |
| Glucose Challenge Test (GCT) or Oral Glucose Tolerance Test (OGTT) | Detect Gestational Diabetes Mellitus (GDM) |
| Repeat Hb and Urine Tests | Monitor anemia and UTIs |
| Indirect Coombs Test (ICT) (for Rh-negative mothers) | Detect Rh sensitization before Anti-D administration |
💉 THIRD TRIMESTER (29 weeks onward)
| Test | Purpose |
|---|---|
| Repeat Hb, Blood Sugar, and Urine Tests | Monitor maternal condition |
| HIV, HBsAg, VDRL (Re-test in some protocols) | Ensure infection control during delivery |
| Serum Uric Acid | Monitor preeclampsia |
| Liver and Renal Function Tests | In suspected PIH or HELLP syndrome |
| NST, Biophysical Profile, or Doppler | Assess fetal well-being (though not biochemical, often done alongside) |
🧬 SPECIAL BIOCHEMICAL TESTS (As Indicated)
| Test | Use |
|---|---|
| Serum Ferritin | Assess iron stores |
| Vitamin D & Calcium Levels | Evaluate in cases of bone pain or muscle cramps |
| HbA1c | Glycemic control over 3 months (for known diabetics) |
| Serum Progesterone / Beta-hCG | Evaluate early pregnancy viability |
| Cervical Fetal Fibronectin (fFN) | Predict risk of preterm labor |
🧑⚕️ ROLE OF MIDWIFE/NURSE:
🌼 Before Testing:
- Educate the mother on purpose and preparation (e.g., fasting for GTT)
- Verify identity and test requirements
- Ensure consent and comfort
🌼 During Testing:
- Assist with sample collection (blood/urine)
- Maintain asepsis and proper labeling
- Ensure cold chain/storage for sample transport (if needed)
🌼 After Testing:
- Interpret and report abnormal values to the doctor
- Document results in ANC card and records
- Counsel the mother on results and necessary precautions/treatments
- Ensure compliance with treatment (e.g., iron, insulin, antibiotics)
🌸 ANTENATAL CARE (ANC)
✅ INTRODUCTION:
Antenatal Care (ANC) refers to the supervised care of a pregnant woman from conception to the onset of labor. It is a crucial part of maternal and child health services and aims to ensure a healthy pregnancy outcome for both mother and baby.
🎯 OBJECTIVES OF ANTENATAL CARE:
- Promote and maintain the health of the mother and fetus
- Detect and manage high-risk pregnancies and complications
- Prepare the woman for labor, birth, and postpartum care
- Educate about nutrition, hygiene, newborn care, and breastfeeding
- Reduce maternal and perinatal morbidity and mortality
📆 ANTENATAL VISIT SCHEDULE (WHO & Indian Guidelines)
| Visit Number | When |
|---|---|
| 1st visit | Before 12 weeks |
| 2nd visit | 14–26 weeks |
| 3rd visit | 28–34 weeks |
| 4th visit | 36–38 weeks |
| ➡️ High-risk pregnancies may require more frequent visits. |
📋 COMPONENTS OF ANTENATAL CARE
1. 📝 History Taking
- Personal history: name, age, marital status, address
- Obstetric history: Gravida, Para, Abortions, Living children (G-P-A-L)
- Menstrual history: LMP, EDD (Naegele’s Rule)
- Medical/surgical history: diabetes, hypertension, asthma
- Family history: genetic disorders, twin pregnancy
- Dietary and lifestyle habits
- Socioeconomic status and support system
2. 🧍♀️ General Physical Examination
- Height and weight (BMI)
- Blood pressure
- Pulse and respiration
- Temperature
- Signs of anemia (pallor)
- Edema (face, hands, feet)
- Breast examination
- Oral hygiene and dental status
3. 🤰 Obstetric Examination
a. Abdominal Examination (from 16 weeks)
- Inspection: shape, size, movements, scars
- Palpation (Leopold’s Maneuvers):
- Fundal height (correlates with gestational age)
- Fetal lie, presentation, and position
- Engagement of the presenting part
- Auscultation of Fetal Heart Rate (FHR):
- Normal: 110–160 bpm
b. Pelvic Examination
- Done only if indicated (late pregnancy or in complications)
- Assess pelvic adequacy, cervical changes, vaginal infections
4. 🧪 Routine Laboratory Investigations
| Test | Purpose |
|---|---|
| Hemoglobin (Hb%) | Detect anemia |
| Blood Group & Rh Typing | Rh incompatibility |
| Urine Routine & Microscopy | Detect UTI, proteinuria, glycosuria |
| HIV, HBsAg, VDRL | Infections screening |
| Random Blood Sugar / OGTT | Detect gestational diabetes |
| Ultrasound | Confirm dating, fetal anomalies, growth monitoring |
| Indirect Coombs Test (ICT) | In Rh-negative mothers |
5. 💊 Supplementation & Immunization
| Intervention | Details |
|---|---|
| Iron + Folic Acid (IFA) | 1 tablet/day from 14–16 weeks for 180 days |
| Calcium + Vitamin D | 2 tablets/day from 14 weeks |
| Deworming (Albendazole 400 mg) | After first trimester |
| Tetanus + Diphtheria (Td) Vaccine | 2 doses 4 weeks apart, starting after 16 weeks Or 1 booster dose if previously vaccinated |
6. 📚 Health Education and Counseling
- Balanced diet and hydration
- Personal hygiene and adequate rest
- Antenatal exercises and posture
- Danger signs in pregnancy
- Importance of regular check-ups
- Birth preparedness and complication readiness (BPCR)
- Breastfeeding and newborn care
- Importance of institutional delivery
- Avoid alcohol, smoking, and self-medication
7. 🩺 Assessment of Fetal Well-being
- Fetal movement (kick count from 28 weeks)
- Fetal heart rate monitoring
- Ultrasound for growth and position
- Non-Stress Test (NST), Biophysical Profile (BPP) if high-risk
🚨 DANGER SIGNS TO REPORT IMMEDIATELY:
- Vaginal bleeding
- Severe headache, blurred vision
- Abdominal pain
- Swelling of face and hands
- Decreased or no fetal movements
- Fever or foul-smelling discharge
- Convulsions
🧑⚕️ ROLE OF MIDWIFE / NURSE IN ANC:
- Provide holistic antenatal assessment
- Perform routine examinations and assist in investigations
- Counsel the mother and her family
- Ensure immunization and supplement compliance
- Identify high-risk pregnancies early
- Maintain proper documentation (ANC card/record)
- Refer complicated cases to higher centers
- Provide emotional support and continuity of care
🌸 WOMEN-CENTERED CARE (WCC)
✅ INTRODUCTION
Women-Centered Care (WCC) is a philosophy of care that respects and prioritizes the individual needs, preferences, rights, and autonomy of the woman throughout her reproductive, maternal, and postnatal journey. It is based on holistic, respectful, and collaborative care.
WCC shifts the focus from the medical system’s needs to the woman’s experience, empowering her to make informed choices about her health.
🎯 OBJECTIVES OF WOMEN-CENTERED CARE:
- Empower women to participate actively in their own health decisions
- Promote dignity, respect, and compassion in maternity care
- Ensure safe, satisfying, and culturally sensitive experiences during pregnancy, birth, and postpartum
- Prevent disrespect, discrimination, and abuse in healthcare
- Strengthen the woman’s physical, emotional, social, and spiritual well-being
❤️ CORE PRINCIPLES OF WOMEN-CENTERED CARE:
| Principle | Explanation |
|---|---|
| Respect and dignity | Women are treated with courtesy, privacy, and respect regardless of background or choices |
| Autonomy and informed choice | Women have the right to make decisions about their care based on accurate and full information |
| Holistic care | Addresses physical, emotional, mental, social, spiritual, and cultural needs |
| Continuity of care | The same team/provider follows the woman throughout pregnancy, labor, and postnatal care |
| Communication and support | Open, non-judgmental, and compassionate communication |
| Collaboration | Woman is considered a partner in care along with the midwife, doctor, and other healthcare providers |
📍 APPLICATION OF WOMEN-CENTERED CARE IN MATERNITY SERVICES:
1. During Antenatal Care (ANC):
- Respect the woman’s choices about tests, supplements, birth plans
- Educate and support decision-making without forcing interventions
- Offer culturally acceptable information
- Recognize the importance of emotional well-being during pregnancy
2. During Labor and Delivery:
- Allow choice of birth position, pain relief methods, and birth companions
- Encourage physiological childbirth (natural unless medically indicated)
- Respect her dignity, modesty, and need for privacy
- Support delayed cord clamping and immediate skin-to-skin contact
3. During Postnatal Care:
- Support her choices around breastfeeding, newborn care, and postpartum rest
- Involve her in decisions about contraception and family planning
- Screen for postnatal depression or anxiety, and provide mental health support
👩⚕️ ROLE OF NURSE / MIDWIFE IN WOMEN-CENTERED CARE:
- Listen actively to the woman’s preferences, concerns, and values
- Provide evidence-based information in a clear, non-medical language
- Advocate for the woman’s rights in clinical settings
- Avoid judgment about personal, cultural, or reproductive choices
- Support informed consent before any procedure or intervention
- Promote shared decision-making with doctors and the woman
- Respect cultural practices as long as they are safe
- Ensure continuity of care and emotional support
- Protect against disrespect and abuse in maternity care
- Document clearly and truthfully about decisions made by the woman
🌍 GLOBAL IMPORTANCE (WHO Guidelines):
- Respectful Maternity Care (RMC) is a key component of women-centered care.
- WCC is essential to achieving Sustainable Development Goal 3 – reducing maternal and neonatal mortality.
- Promotes trust in the healthcare system, reducing home births without skilled attendants.
📝 EXAMPLES OF WOMEN-CENTERED CARE:
| Scenario | Women-Centered Approach |
|---|---|
| Woman requests not to be examined by male staff | Assign female provider where possible |
| Woman wants to try vaginal birth after cesarean (VBAC) | Provide information, risks, and support choice |
| Refuses certain tests due to religious beliefs | Respect decision and document accordingly |
| Experiencing fear of childbirth | Offer emotional support, education, and reassurance |
✅ BENEFITS OF WOMEN-CENTERED CARE:
- Improved maternal satisfaction and confidence
- Better adherence to antenatal/postnatal care
- Fewer unnecessary interventions (like cesarean)
- Safer, more respectful birthing experiences
- Strengthened mother-infant bonding and breastfeeding success
Respectful Maternity Care & Compassionate Communication
✅ INTRODUCTION:
Respectful Care and Compassionate Communication are essential components of humanized maternal healthcare. They ensure that every woman receives care that is dignified, empathetic, culturally appropriate, and free from abuse, neglect, or discrimination.
They form the foundation of Women-Centered Care and are central to the World Health Organization (WHO) standards for quality maternal and newborn care.
🎯 OBJECTIVES:
- Preserve the dignity, privacy, and autonomy of women in healthcare settings
- Build trust and therapeutic relationships between women and caregivers
- Prevent disrespect and abuse in maternity care
- Improve health outcomes and maternal satisfaction
- Encourage women to seek timely and regular health services
💗 RESPECTFUL MATERNITY CARE (RMC):
(As per WHO framework)
🌼 Key Rights of Women in Maternal Care:
- Right to be treated with respect and dignity
- Right to information, informed consent, and choice
- Right to privacy and confidentiality
- Right to equitable care without discrimination
- Right to freedom from harm and abuse
- Right to companionship during labor (if desired)
- Right to timely and appropriate care
🗣️ COMPASSIONATE COMMUNICATION:
A skill that involves speaking and listening with empathy, kindness, and sensitivity.
🌸 Principles of Compassionate Communication in Maternity Care:
| Principle | Description |
|---|---|
| Active Listening | Give full attention, avoid interruptions, nod, and show interest |
| Use of Simple Language | Avoid medical jargon; use words the woman can understand |
| Empathy | Acknowledge feelings; say “I understand this is difficult for you” |
| Non-verbal Cues | Maintain eye contact, smile, soft tone, gentle touch |
| Validation of Feelings | Respect fears, concerns, and cultural beliefs |
| Respect for Choice | Support the woman’s decisions even if they differ from routine practice |
| Calmness and Patience | Especially during labor, anxiety, or complications |
🧑⚕️ NURSE / MIDWIFE’S ROLE IN RESPECTFUL CARE & COMMUNICATION:
🔹 In Antenatal Care:
- Maintain privacy during examination
- Listen actively to the woman’s concerns
- Explain all procedures and seek consent
- Provide education without judgment
- Respect cultural practices as long as they are safe
🔹 In Labor and Delivery:
- Introduce yourself and explain your role
- Always ask before touching or performing any procedure
- Allow birth companions if the woman desires
- Use calming words and provide encouragement
- Avoid shouting, scolding, or blaming the woman
- Allow preferred birthing position if safe and possible
🔹 In Postnatal Care:
- Offer emotional support to new mothers
- Respect her choices about breastfeeding or infant care
- Address her mental and emotional health
- Encourage questions and offer guidance kindly
🚨 EXAMPLES OF DISRESPECT & ABUSE (To be Avoided):
- Yelling, scolding, or mocking the woman during labor
- Performing procedures without consent
- Leaving a woman unattended during labor
- Refusing care due to caste, religion, age, or marital status
- Denying pain relief without explanation
- Not allowing a birth companion (when policy allows)
✅ BENEFITS OF RESPECTFUL & COMPASSIONATE CARE:
- Increases maternal trust and satisfaction
- Promotes positive birth experiences
- Encourages women to return for future care
- Reduces maternal stress and improves health outcomes
- Builds respectful midwife-client relationships
📌 KEY PHRASES TO USE:
- “You are doing well. I’m here to help you.”
- “Do you have any questions or concerns?”
- “Would you like someone to be with you?”
- “I’ll explain what I’m going to do before we begin.”
- “Your feelings are valid. We will support you.”
REFERRAL SYSTEM IN MATERNAL AND CHILD HEALTHCARE
✅ INTRODUCTION:
A referral is the process of transferring a pregnant woman or neonate from one level of care to a higher-level facility for further assessment, treatment, or management when their condition goes beyond the available resources or skills at the primary care level.
Effective referrals are critical in preventing maternal and neonatal mortality, especially in high-risk or emergency situations.
🎯 OBJECTIVES OF REFERRAL:
- Provide timely and appropriate care at the correct level
- Ensure continuity of care
- Minimize delays in diagnosis and treatment
- Prevent complications and adverse outcomes
- Promote a functioning health system linkage between facilities
📦 TYPES OF REFERRAL:
| Type | Description |
|---|---|
| Routine Referral | Planned referral for conditions like anemia, previous cesarean, high BP |
| Emergency Referral | Urgent referral for complications like bleeding, eclampsia, obstructed labor |
| Self-Referral | When the woman directly goes to a higher center without recommendation |
| Back-Referral | Referred patient sent back to original facility for follow-up care after stabilization |
🧍♀️ CONDITIONS THAT REQUIRE REFERRAL (MATERNAL):
- Severe anemia (Hb < 7 g/dL)
- High-risk pregnancy (PIH, GDM, multiple pregnancy, IUGR)
- Antepartum hemorrhage (APH)
- Premature rupture of membranes (PROM)
- Eclampsia or convulsions
- Obstructed labor or prolonged labor
- Malpresentation (breech, transverse lie)
- Previous 2 or more cesarean deliveries
- Postpartum hemorrhage (PPH)
- Retained placenta or incomplete abortion
- Severe infections or fever with chills
👶 CONDITIONS THAT REQUIRE REFERRAL (NEWBORN):
- Low birth weight (<2 kg)
- Birth asphyxia or poor Apgar score
- Jaundice before 24 hours or very yellow skin
- Breathing difficulty, seizures, or convulsions
- Congenital anomalies
- Refusal to feed or lethargy
- Neonatal sepsis signs (fever, poor tone)
📝 ESSENTIAL COMPONENTS OF A GOOD REFERRAL:
- Assessment: Confirm the need for referral
- Stabilization: Do initial treatment to prevent deterioration (e.g., IV fluids, oxygen, injections)
- Communication: Inform the referral center in advance
- Documentation: Complete a referral slip/form with clear clinical notes
- Transport: Arrange for safe, quick, and comfortable transport
- Accompaniment: Send an attendant or staff if necessary
- Back-Referral: Encourage feedback and follow-up from higher center
📋 REFERRAL SLIP FORMAT (Key Elements):
- Patient name, age, gravida/para status
- Reason for referral
- Vital signs and examination findings
- Investigations done
- Treatment given before referral
- Facility details and referring person’s name
- Emergency contact or relative accompanying
🧑⚕️ ROLE OF MIDWIFE / NURSE IN REFERRAL:
| Responsibility | Details |
|---|---|
| Identification | Recognize danger signs or high-risk cases early |
| Decision-making | Consult doctor/medical officer if unsure |
| Communication | Clearly explain reason for referral to the patient and family |
| Stabilization | Start IV, give medication, monitor vitals before transfer |
| Documentation | Write complete and accurate referral form |
| Counseling | Reassure the woman and reduce fear during the transfer |
| Coordination | Arrange transport, call the referral center, inform higher facility |
📌 BARRIERS TO EFFECTIVE REFERRAL:
- Lack of transport or delay in ambulance
- Poor communication between facilities
- Incomplete referral documentation
- Family reluctance due to cost or distance
- Lack of awareness among patients
✅ IMPORTANCE OF A STRONG REFERRAL SYSTEM:
- Reduces maternal and newborn deaths
- Promotes continuity and efficiency of care
- Builds trust in the health system
- Supports team-based care between nurses, doctors, and specialists
COLLABORATION IN MATERNAL AND NEWBORN CARE
✅ INTRODUCTION:
Collaboration in healthcare means working together across different professions and levels of care to provide the best possible outcomes for the mother, baby, and family. It involves mutual respect, shared responsibilities, and effective communication between midwives, nurses, doctors, specialists, families, and other care providers.
🎯 OBJECTIVES OF COLLABORATION:
- Provide safe, comprehensive, and coordinated care
- Ensure early detection and timely management of complications
- Promote interdisciplinary decision-making
- Avoid duplication of services and delays in treatment
- Enhance patient satisfaction and healthcare provider efficiency
👩👩👦 WHO IS INVOLVED IN COLLABORATION?
| Stakeholder | Role |
|---|---|
| Midwife/Nurse | First point of contact, ongoing care, monitoring, education |
| Obstetrician/Gynecologist | High-risk pregnancy management, deliveries, surgical care |
| Pediatrician/Neonatologist | Newborn resuscitation, neonatal care |
| Anesthetist | Labor analgesia, C-section |
| Dietician | Nutritional counseling in pregnancy, anemia, GDM |
| Lab Technician | Timely and accurate investigations |
| Social Worker/Counselor | Psychosocial support, domestic violence cases |
| Family Members | Support, decision-making, postnatal care |
🔗 TYPES OF COLLABORATION IN MATERNAL CARE:
| Type | Example |
|---|---|
| Intraprofessional | Midwives working together in a labor ward |
| Interprofessional | Nurse-midwife collaborating with doctors and dieticians |
| Multidisciplinary | Entire team (OB-GYN, neonatologist, social worker) planning care for a high-risk mother |
| Client collaboration | Mother actively involved in decision-making about her birth plan |
🏥 EXAMPLES OF COLLABORATION IN PRACTICE:
- Midwife identifies PIH → Refers to doctor → Doctor prescribes medication → Nurse monitors BP and educates mother
- High-risk pregnancy (GDM) → Nurse monitors sugar → Dietician plans meals → Physician adjusts insulin
- Obstructed labor → Midwife informs doctor → Doctor assesses and prepares for C-section → Anesthetist and OT team are involved
- Neonatal resuscitation needed → Midwife delivers → Pediatrician resuscitates → NICU nurse takes over care
🌼 PRINCIPLES OF EFFECTIVE COLLABORATION:
| Principle | Explanation |
|---|---|
| Mutual Respect | Value each team member’s skills and contributions |
| Open Communication | Share relevant information clearly and promptly |
| Shared Decision-Making | All team members contribute to care planning |
| Trust & Accountability | Each person is responsible and dependable |
| Client-Centered Approach | Keep the woman and baby’s needs at the center |
🧑⚕️ ROLE OF MIDWIFE / NURSE IN COLLABORATION:
- Communicator: Share clinical findings and updates with the team
- Coordinator: Schedule appointments, ensure follow-ups
- Educator: Provide information to the mother and team members
- Advocate: Speak up for the woman’s rights and preferences
- Facilitator: Help bring the team together and resolve conflict if needed
- Observer: Monitor changes in condition and report promptly
- Documenter: Record all referrals, decisions, and outcomes clearly
🌟 BENEFITS OF COLLABORATIVE CARE:
- Better maternal and neonatal outcomes
- Increased efficiency and reduced medical errors
- Enhanced staff satisfaction and professional growth
- Faster and more coordinated responses to emergencies
- Empowered mothers through shared decision-making
🚫 CONSEQUENCES OF POOR COLLABORATION:
- Delayed or inappropriate care
- Miscommunication and medical errors
- Increased maternal or neonatal morbidity
- Staff frustration and burnout
- Loss of trust by the patient/family
EMPOWERMENT IN MATERNAL AND WOMEN’S HEALTHCARE
✅ INTRODUCTION:
Empowerment in nursing and midwifery refers to the process of enabling women to take control over their own health, decisions, and lives. It involves educating, supporting, encouraging, and respecting women so they can make informed choices about their bodies, pregnancies, childbirth, and families.
Empowered women are more likely to have healthy pregnancies, seek timely care, and make decisions that benefit their own health and that of their babies.
🎯 OBJECTIVES OF EMPOWERMENT IN MATERNAL CARE:
- Increase a woman’s confidence and self-efficacy
- Promote informed decision-making in pregnancy and childbirth
- Encourage women to actively participate in their own care
- Improve maternal and neonatal health outcomes
- Reduce gender inequalities and health disparities
- Protect women’s rights, dignity, and autonomy
💡 TYPES OF EMPOWERMENT (IN HEALTHCARE CONTEXT):
| Type | Description |
|---|---|
| Health Empowerment | Women understand their health conditions and know how to manage them |
| Emotional Empowerment | Women feel supported, heard, and emotionally secure |
| Educational Empowerment | Women are informed about their bodies, birth options, and baby care |
| Social Empowerment | Women can access resources, support systems, and make decisions freely |
| Economic Empowerment | Women have financial control and decision-making power regarding healthcare |
🌼 KEY PRINCIPLES OF EMPOWERMENT IN MIDWIFERY:
| Principle | Application in Practice |
|---|---|
| Respect for autonomy | Support women in making their own health decisions |
| Access to information | Educate in simple language using visual aids or local languages |
| Active participation | Encourage involvement in birth planning and self-care |
| Supportive care | Provide emotional encouragement and non-judgmental communication |
| Skill-building | Teach women about nutrition, hygiene, baby care, and breastfeeding |
🧑⚕️ ROLE OF MIDWIFE / NURSE IN EMPOWERING WOMEN:
- Educator:
- Provide antenatal and postnatal education
- Use group teaching, demonstrations, flipcharts, and individual counseling
- Counselor:
- Support women in emotional distress
- Discuss fears and encourage confidence
- Advocate:
- Stand up for the woman’s rights (e.g., informed consent, privacy)
- Intervene if care is disrespectful or discriminatory
- Facilitator:
- Encourage birth companions, birth plans, and choice of birthing positions
- Mentor:
- Teach adolescent girls and women about reproductive health, menstrual hygiene, and family planning
- Supporter of Decision-Making:
- Involve women in decisions regarding labor, delivery methods, pain relief, and newborn care
📌 EXAMPLES OF EMPOWERMENT IN MATERNAL CARE:
| Scenario | Empowered Action |
|---|---|
| Pregnant woman asks for birth plan | Midwife helps her create one |
| Woman requests to delay procedures | Her choice is respected unless urgent |
| First-time mother feels anxious | Nurse reassures, explains stages of labor, breathing techniques |
| Mother asks for breastfeeding help | Nurse shows proper latch and encourages her efforts |
🌟 BENEFITS OF EMPOWERMENT:
- Improves maternal confidence and self-worth
- Enhances compliance with health practices
- Reduces maternal stress and anxiety
- Leads to better birth outcomes and postpartum recovery
- Fosters positive mother-infant bonding
- Builds long-term trust in the healthcare system
🚫 BARRIERS TO EMPOWERMENT:
- Lack of education or health literacy
- Gender-based discrimination
- Cultural taboos or family restrictions
- Healthcare workers who are disrespectful or unapproachable
- Lack of privacy or choice in care settings
III Trimester
ONGOING RISK ASSESSMENT – MATERNAL MENTAL HEALTH
✅ INTRODUCTION:
Maternal mental health is a critical component of overall maternal well-being. Pregnancy and the postpartum period bring significant physical, emotional, and social changes, making women vulnerable to mental health challenges.
Ongoing risk assessment is the continuous process of identifying, monitoring, and responding to mental health concerns in pregnant and postpartum women to ensure timely support and care.
🎯 OBJECTIVES OF MENTAL HEALTH RISK ASSESSMENT:
- Detect early signs of emotional or psychological distress
- Identify risk factors for depression, anxiety, or other mental illnesses
- Promote timely referral and intervention
- Support the woman’s mental and emotional well-being
- Ensure a safe and nurturing environment for the baby
📅 WHEN TO ASSESS?
- At every ANC and PNC visit
- During home visits or community health check-ups
- On hospital admission for labor and post-delivery
- At the 6-week postpartum check-up
- Whenever the woman or family reports behavioral changes
🚩 COMMON MATERNAL MENTAL HEALTH CONDITIONS:
| Condition | Timeframe |
|---|---|
| Antenatal Depression/Anxiety | During pregnancy |
| Postpartum Depression (PPD) | Within 6 weeks to 12 months after delivery |
| Baby Blues | Mild mood swings within 3–5 days of birth |
| Postpartum Psychosis | Severe, rare condition, usually within 2 weeks of delivery |
🔍 RISK FACTORS FOR MATERNAL MENTAL ILLNESS:
| Psychological | Social | Biological |
|---|---|---|
| History of mental illness | Domestic violence | Hormonal changes |
| Lack of emotional support | Poverty, unemployment | Sleep deprivation |
| Low self-esteem | Unplanned pregnancy | Nutritional deficiencies |
| Fear of childbirth | Teenage pregnancy | Chronic medical illness |
| Previous perinatal loss | Marital conflict | Multiple pregnancy |
📋 SCREENING TOOLS USED:
| Tool | Description |
|---|---|
| Edinburgh Postnatal Depression Scale (EPDS) | 10-question tool to detect depression; score >10 indicates concern |
| PHQ-9 (Patient Health Questionnaire) | Screens for depression symptoms |
| GAD-7 | Screens for generalized anxiety disorder |
| Clinical interview | Based on behavior, appearance, mood, and speech |
👁️ SIGNS & SYMPTOMS TO WATCH FOR:
| Emotional | Behavioral | Physical |
|---|---|---|
| Sadness or tearfulness | Withdrawal from others | Sleep disturbance |
| Anxiety or excessive worry | Neglecting self-care or baby | Appetite changes |
| Irritability or anger | Crying spells | Fatigue |
| Loss of interest or pleasure | Suicidal thoughts | Headaches/body pain |
➡️ Red Flags: Suicidal ideation, hallucinations, severe withdrawal, or neglect of the baby → urgent referral needed
🧑⚕️ ROLE OF MIDWIFE / NURSE IN ONGOING RISK ASSESSMENT:
🌼 During Antenatal Care:
- Ask open-ended questions about emotional health
- Include mental health screening as part of ANC visits
- Provide privacy and non-judgmental listening
- Educate woman and family on common emotional changes in pregnancy
- Identify high-risk cases and refer to mental health professionals
🌼 During Postnatal Care:
- Assess mood and bonding with baby
- Check for sleep, appetite, and coping behavior
- Support breastfeeding and mother-infant attachment
- Monitor for baby blues vs. postpartum depression
- Arrange home visits or community follow-up when needed
🧾 SAMPLE ASSESSMENT QUESTIONS:
- “How have you been feeling emotionally lately?”
- “Do you feel overwhelmed or anxious often?”
- “Are you sleeping and eating well?”
- “Do you have thoughts of harming yourself or your baby?”
- “Would you like to talk to someone about your feelings?”
👩👩👧👦 FAMILY & COMMUNITY INVOLVEMENT:
- Educate family about warning signs and support methods
- Encourage involvement of husband/partner or caregivers
- Link with ASHA/ANM workers for home-based follow-up
- Use peer support groups or community health programs
✅ INTERVENTIONS & REFERRALS:
- Mild symptoms: Counseling, emotional support, relaxation, yoga, self-care tips
- Moderate to severe symptoms: Referral to psychiatrist, psychologist, or mental health counselor
- Emergency (suicidal thoughts, psychosis): Immediate hospital admission and psychiatric care
Education and Management of Physiological Changes & Discomforts in the Third Trimester (28–40 weeks)
✅ INTRODUCTION:
The third trimester marks the final phase of pregnancy (weeks 28 to delivery). The fetus undergoes rapid growth, and the mother’s body adapts to prepare for labor and birth. These changes can lead to physical discomforts, emotional stress, and the need for increased education and support.
🧠 PURPOSE OF NURSING EDUCATION IN 3rd TRIMESTER:
- Prepare the woman for labor and delivery
- Help her cope with discomforts
- Promote fetal and maternal well-being
- Encourage birth preparedness and complication readiness (BPCR)
- Reinforce healthy habits and emotional support
🌼 COMMON PHYSIOLOGICAL CHANGES & THEIR MANAGEMENT:
1. Increased Abdominal Size & Uterine Pressure
| Change | Discomfort | Nursing Advice |
|---|---|---|
| Growing uterus displaces internal organs | Shortness of breath, heaviness, pressure on bladder | – Encourage upright posture – Sleep with head elevated – Wear loose, supportive clothing |
2. Backache & Pelvic Pain
| Cause | Loosening of pelvic joints, increased weight | | Nursing Management |
- Teach good posture and back support
- Use maternity pillows for sleep
- Suggest mild exercises/yoga (e.g., cat-cow pose)
- Apply warm compresses
- Wear low-heeled shoes
3. Frequent Urination
| Cause | Uterine pressure on bladder | | Nursing Advice |
- Reassure that it’s common
- Encourage regular voiding
- Avoid caffeine and fluids close to bedtime
- Monitor for UTI symptoms (burning, pain)
4. Constipation
| Cause | Progesterone slows bowel movement, iron supplements | | Nursing Advice |
- High-fiber diet (fruits, vegetables, whole grains)
- Adequate fluid intake (8–10 glasses daily)
- Encourage walking or light activity
- Avoid overuse of laxatives
5. Heartburn & Indigestion
| Cause | Relaxation of esophageal sphincter and pressure from uterus | | Nursing Advice |
- Eat small, frequent meals
- Avoid spicy, fried, or acidic foods
- Don’t lie down immediately after meals
- Elevate head during sleep
6. Leg Cramps
| Cause | Compression of blood vessels/nerves, calcium deficiency | | Nursing Advice |
- Gentle leg stretching before bed
- Massage and apply warm compresses
- Ensure calcium + magnesium supplements
- Stay hydrated
7. Edema (Swelling of Feet & Ankles)
| Cause | Fluid retention, pressure on veins | | Nursing Advice |
- Elevate legs while resting
- Avoid standing or sitting for long periods
- Wear comfortable shoes
- Rule out preeclampsia if swelling is sudden/severe with high BP
8. Fatigue and Sleep Disturbances
| Cause | Hormonal changes, fetal movements, anxiety | | Nursing Advice |
- Encourage short naps during the day
- Use pillows to support the abdomen and back
- Practice breathing/relaxation techniques before bed
- Light walking or prenatal yoga
9. Breast Changes & Colostrum Leakage
| Cause | Hormonal preparation for breastfeeding | | Nursing Advice |
- Reassure the woman it is normal
- Use soft breast pads if leaking
- Wear supportive maternity bras
- Educate about early signs of milk production
10. Braxton Hicks Contractions (False Labor)
| Feature | Irregular, mild, non-progressive contractions | | Nursing Advice |
- Reassure that it prepares the uterus for labor
- Encourage hydration and rest
- Educate on the difference between true labor and false labor
👩🏫 HEALTH EDUCATION & PREPARATION TOPICS FOR 3RD TRIMESTER:
| Topic | Content |
|---|---|
| Birth preparedness | Pack hospital bag, choose birth companion, transport plan |
| Danger signs | Vaginal bleeding, leaking fluid, severe headache, vision problems, no fetal movement |
| Fetal movement monitoring (DFMC) | Count 10 kicks in 12 hours or 4 in 1 hour |
| Pre-labor signs | Lightening, mucus plug, regular contractions |
| Labor stages & pain management | Breathing exercises, massage, support techniques |
| Breastfeeding | Early initiation, exclusive breastfeeding, colostrum benefits |
| Postnatal care & newborn care | Personal hygiene, baby bathing, cord care, immunization |
🧑⚕️ NURSE / MIDWIFE’S ROLE:
- Assess: Monitor for high-risk signs at each ANC visit
- Educate: Explain all changes in a reassuring and simple manner
- Support: Address physical, emotional, and social concerns
- Refer: High-risk cases (e.g., PIH, IUGR, decreased fetal movement)
- Document: All assessments, education given, and interventions
- Empower: Help women feel confident about their bodies and upcoming labor
Third Trimester Tests and Screening (28–40 Weeks)
✅ INTRODUCTION:
The third trimester is a critical period for monitoring maternal health, fetal growth, and well-being, and to prepare for safe delivery. Various laboratory tests, imaging studies, and screenings are carried out to detect late pregnancy complications and guide decision-making for birth.
🎯 OBJECTIVES OF THIRD TRIMESTER TESTING:
- Detect maternal and fetal complications (e.g., anemia, GDM, preeclampsia, IUGR)
- Monitor fetal growth and position
- Assess placental function and amniotic fluid
- Prepare for timely referral or intervention
- Ensure the mother is ready for safe labor and delivery
📋 ROUTINE THIRD TRIMESTER INVESTIGATIONS:
| Test | Purpose | Timing |
|---|---|---|
| Hemoglobin (Hb%) | Monitor for anemia | ~28–32 weeks |
| Urine Albumin and Sugar | Detect proteinuria (PIH), glucosuria (GDM) | Every visit |
| Blood Sugar (RBS/FBS/OGTT) | Detect or monitor gestational diabetes | 28–32 weeks |
| Ultrasound (Growth Scan) | Check fetal growth, AFI, placenta | 28–34 weeks |
| Blood Grouping (if not done earlier) | Confirm Rh status | Before 32 weeks |
| Indirect Coombs Test (ICT) | For Rh-negative mothers to detect alloimmunization | At 28 weeks |
| HIV, HBsAg, VDRL (repeat in some protocols) | Detect infections before delivery | 32–36 weeks |
| Complete Blood Count (CBC) | Reassess anemia, infections | 28–32 weeks |
| Tetanus Toxoid Booster (Td) | Immunization (1 or 2 doses depending on status) | After 28 weeks |
🧪 SPECIAL/CONDITION-SPECIFIC TESTS:
| Test | Indication |
|---|---|
| NST (Non-Stress Test) | Decreased fetal movement, PIH, IUGR |
| Doppler Study | Suspected IUGR, abnormal AFI, hypertensive disorders |
| Liver Function Test (LFT), Renal Function Test (RFT) | If preeclampsia/HELLP is suspected |
| Serum Uric Acid | High BP, preeclampsia |
| Cervical Swab Culture (if leaking or discharge) | Suspected infection or PROM |
| GBS (Group B Streptococcus) Screening (optional or as per local policy) | Vaginal swab at 35–37 weeks to prevent neonatal sepsis |
📺 ULTRASOUND IN THIRD TRIMESTER:
| Purpose | Details |
|---|---|
| Fetal Biometry | Estimate fetal weight, growth parameters |
| Amniotic Fluid Index (AFI) | Normal: 8–18 cm Oligohydramnios: <5 cm Polyhydramnios: >24 cm |
| Placental Location & Maturity | Rule out placenta previa or calcification |
| Fetal Position & Presentation | Breech, cephalic, transverse |
| Biophysical Profile (BPP) | Fetal well-being scoring (movement, tone, breathing, AFI, NST) |
🧑⚕️ NURSE / MIDWIFE’S ROLE:
- Educate the mother about the importance of third-trimester tests
- Prepare the woman for each test (e.g., fasting for OGTT, hydration for USG)
- Assist in sample collection and ensure correct labeling
- Monitor and document test results
- Identify danger signs or abnormal reports
- Refer promptly if complications like anemia, GDM, preeclampsia, IUGR are detected
- Provide emotional support, especially if abnormal findings are discovered
🚨 DANGER SIGNS TO SCREEN FOR IN THIRD TRIMESTER:
- High BP (PIH/Preeclampsia)
- Reduced fetal movements
- Excessive weight gain or swelling (edema)
- Vaginal bleeding or watery discharge
- Signs of infection (fever, foul discharge)
Fetal Engagement in Late Pregnancy
✅ INTRODUCTION
Fetal engagement is a term used to describe when the presenting part of the fetus (usually the head) descends into the maternal pelvic brim and becomes fixed in the pelvis in preparation for labor and delivery.
This typically occurs in late third trimester, especially in primigravida women (first-time mothers), often 2–4 weeks before labor begins. In multigravidas, engagement may occur closer to or during labor.
📚 DEFINITION
Fetal engagement is said to have occurred when the biparietal diameter (BPD) of the fetal head passes through the pelvic inlet and enters the true pelvis.
🎯 PURPOSE OF ENGAGEMENT:
- Prepares the fetus for descent through the birth canal
- Indicates that the pelvis is adequate for vaginal delivery (especially in primigravida)
- Suggests that labor may start soon
🧠 FACTORS AFFECTING ENGAGEMENT:
| Factor | Effect |
|---|---|
| Parity | Earlier in primigravida, later in multigravida |
| Fetal Lie and Presentation | Only occurs in longitudinal lie, cephalic presentation |
| Pelvic adequacy | Adequate pelvis allows engagement |
| Uterine tone and fetal size | Overdistension or large baby may delay engagement |
| Position of fetus | Favorable (LOA, ROA) promotes easier engagement |
📍 SIGNS OF FETAL ENGAGEMENT:
| Sign | Description |
|---|---|
| Lightening | Woman feels lighter as the fundus descends |
| Relief from breathlessness | Less pressure on diaphragm |
| Increased pelvic pressure | Heaviness or pressure in lower pelvis and bladder |
| Frequent urination | Due to pressure on bladder |
| Changes in abdominal shape | Uterus appears lower |
| Backache | Due to shifting of fetal weight |
| Improved appetite | Due to reduced pressure on stomach |
✋ METHODS TO ASSESS ENGAGEMENT
1️⃣ Abdominal Palpation (Leopold’s Fourth Maneuver)
| Method | Midwife faces the woman’s feet and palpates just above the symphysis pubis to feel the presenting part | | Interpretation |
- Engaged: Head is fixed and cannot be moved side to side
- Not engaged: Head is still mobile or ballotable
2️⃣ Pelvic Examination (Per Vaginal – PV)
(Done by doctor or trained midwife in hospital setting)
| Method | Fingers assess how many fifths of the fetal head are palpable above the pelvic brim | | Interpretation |
- Fully engaged: 0/5 head palpable (none above pelvis)
- Partially engaged: 1/5 to 4/5 palpable
- Not engaged: 5/5 palpable (whole head above brim)
3️⃣ Imaging (Ultrasound)
- Confirms fetal position, engagement, and station of head
- Useful when abdominal findings are inconclusive
⚖️ STATION OF THE PRESENTING PART (In relation to ischial spines)
| Station | Meaning |
|---|---|
| 0 | Head at the level of ischial spines (engaged) |
| +1 to +5 | Below spines – descending through birth canal |
| –1 to –5 | Above spines – not yet engaged |
🧑⚕️ ROLE OF MIDWIFE / NURSE:
- Observe and assess for signs of engagement at each ANC visit after 36 weeks
- Reassure the woman about normal changes (lightening, increased urination)
- Differentiate engagement vs descent during labor
- Record findings in ANC card/partograph
- Encourage pelvic floor exercises and upright positions to aid engagement
- Refer for evaluation if engagement does not occur in primigravida by 38–39 weeks
🚨 WHEN TO SUSPECT NON-ENGAGEMENT / DELAYED ENGAGEMENT:
- Persistent high head in a primigravida at term
- Large fetus or abnormal lie (breech, transverse)
- Cephalopelvic disproportion (CPD)
- Pelvic tumor or placenta previa
➡️ Requires referral to an obstetrician for further evaluation and delivery planning.
3rd Trimester Antenatal Education Classes (Weeks 28–40)
✅ INTRODUCTION:
Antenatal education classes during the third trimester aim to prepare the pregnant woman (and her family) physically, emotionally, and mentally for labor, childbirth, and newborn care. These classes also promote maternal confidence, reduce anxiety, and encourage positive health-seeking behavior.
Midwives and nurses are key educators in delivering this life-enhancing knowledge in both hospital and community settings.
🎯 GOALS OF 3RD TRIMESTER ANTENATAL EDUCATION:
- Prepare the woman for labor, delivery, and breastfeeding
- Promote self-care, fetal well-being, and complication awareness
- Educate on birth preparedness and complication readiness (BPCR)
- Encourage informed decision-making and mother-friendly birth practices
- Involve family and support persons in care and planning
📚 TOPICS TO BE COVERED IN 3RD TRIMESTER ANTENATAL CLASSES:
1️⃣ Signs of Labor and When to Go to the Hospital
- True vs. false labor pains
- Show, rupture of membranes, regular contractions
- Danger signs in late pregnancy (bleeding, severe pain, reduced fetal movement)
- Hospital bag preparation
2️⃣ Stages of Labor & Delivery Process
- First, second, and third stages of labor
- Role of hormones
- What to expect physically and emotionally
- Labor room environment
- How birth companions can support
3️⃣ Pain Relief During Labor
- Natural methods (breathing techniques, massage, warm showers, position changes)
- Medical options (epidural, analgesics)
- Pros and cons of each
4️⃣ Birthing Positions & Delivery Choices
- Benefits of upright or alternative birthing positions
- Role of squatting, kneeling, water birth (if offered)
- Decision-making about vaginal vs cesarean delivery
5️⃣ Breathing & Relaxation Techniques
- Deep breathing, guided imagery
- Exercises to reduce stress and anxiety
- Support during contractions
6️⃣ Postpartum Self-Care & Recovery
- Physical recovery from birth (vaginal or cesarean)
- Perineal hygiene
- Rest and nutrition after birth
- Mental health awareness (baby blues, postpartum depression)
7️⃣ Breastfeeding Education
- Importance of early initiation and colostrum
- Proper latch and positioning
- Exclusive breastfeeding for 6 months
- Overcoming challenges like sore nipples or engorgement
8️⃣ Newborn Care Essentials
- First bath, diapering, clothing
- Umbilical cord care
- Danger signs in newborn
- Immunization schedule
- Mother-infant bonding and skin-to-skin contact
9️⃣ Nutrition in Late Pregnancy
- Iron-rich foods, calcium, protein
- Managing common discomforts (heartburn, constipation)
- Hydration and portion control
- Cultural and locally available nutritious food tips
🔟 Birth Preparedness and Complication Readiness (BPCR)
- Identify health facility for delivery
- Arrange transport and funds
- Choose a birth companion
- Plan for emergency care
- Know your blood group and Rh status
👨👩👧 WHO SHOULD ATTEND?
- Pregnant women (especially 28+ weeks)
- Husbands or partners
- Mothers/mothers-in-law
- Other caregivers or companions
🧑⚕️ NURSE / MIDWIFE’S ROLE IN ANTENATAL EDUCATION:
| Responsibility | Activities |
|---|---|
| Educator | Use simple language, visuals, and demonstrations |
| Counselor | Address fears, anxieties, myths, or misconceptions |
| Supporter | Encourage woman’s autonomy and confidence |
| Facilitator | Involve family in sessions to build a support system |
| Advocate | Promote respectful maternity care and informed choices |
📌 METHODS USED IN ANTENATAL CLASSES:
- Group discussions and Q&A sessions
- Role-play or drama (for danger signs, labor)
- Video demonstrations
- Flipcharts, posters, and models
- Breathing and relaxation exercises
- Peer sharing and storytelling
- Distributing handouts or checklists
✅ BENEFITS OF 3RD TRIMESTER ANTENATAL CLASSES:
- Reduced maternal anxiety and fear of childbirth
- Increased knowledge and preparedness
- Higher rates of exclusive breastfeeding
- Better pain management during labor
- Higher satisfaction with birth experience
- Stronger family involvement and support
Birth Preparedness and Complication Readiness (BPCR)
✅ INTRODUCTION:
BPCR is a strategy recommended by the World Health Organization (WHO) and the Ministry of Health and Family Welfare (India) to promote maternal and newborn survival by ensuring that women and their families are prepared for normal birth and can respond effectively to obstetric and newborn complications.
It is a key component of antenatal care (ANC), especially in the third trimester, and empowers women and their families to take informed, timely actions during labor and emergencies.
🎯 OBJECTIVES OF BPCR:
- Reduce delays in seeking, reaching, and receiving care
- Ensure safe delivery with a skilled birth attendant
- Encourage emergency readiness for maternal and newborn complications
- Promote community and family involvement in maternal health
- Improve institutional delivery rates and reduce maternal mortality
🧾 KEY ELEMENTS OF BPCR PLAN:
1️⃣ Identify a Skilled Birth Attendant & Health Facility
- Choose the nearest healthcare facility with delivery and emergency services
- Know the name of the doctor, midwife, or nurse who will attend the birth
- Make prior visits to the facility if possible
2️⃣ Arrange Transport
- Identify two or more reliable transportation options in advance
- Arrange for fuel, contact numbers, and driver availability
- Include backup options for night or bad weather emergencies
3️⃣ Save Money for Delivery and Emergencies
- Allocate funds for delivery charges, medicines, tests, transport
- Enroll in government schemes like:
- Janani Suraksha Yojana (JSY)
- Pradhan Mantri Matru Vandana Yojana (PMMVY)
- Janani Shishu Suraksha Karyakram (JSSK) – free transport, delivery, and treatment
4️⃣ Identify a Birth Companion
- Select a supportive person (husband, mother, sister) to accompany the woman
- Ensure the companion knows basic signs of labor and complications
- They can provide emotional, physical, and logistical support
5️⃣ Know the Danger Signs (During Pregnancy, Labor, Postpartum, Newborn)
Maternal:
- Severe abdominal pain or headache
- Vaginal bleeding or leaking
- High fever
- Convulsions or unconsciousness
- Decreased fetal movement
Newborn:
- Difficulty breathing
- Poor feeding
- Cold to touch or fever
- Yellow skin before 24 hours
- Convulsions or limpness
➡️ Immediate referral is critical
6️⃣ Arrange for Blood Donor
- Know your blood group in advance
- Identify willing donors (family/friends) with matching blood group
- Know the nearest blood bank or hospital providing transfusion services
7️⃣ Pack a Birth Preparedness Bag
Include:
- ANC card
- Two sets of clean clothes
- Baby clothes and blanket
- Sanitary pads
- Toiletries and soap
- Clean towel
- ID proof and health documents
- Mobile phone and charger
8️⃣ Family and Community Support
- Involve family members in planning
- Link with ASHAs, ANMs, or self-help groups (SHGs)
- Join antenatal classes or mothers’ support groups
🧑⚕️ ROLE OF NURSE / MIDWIFE IN BPCR:
| Responsibility | Actions |
|---|---|
| Educator | Teach women and families about BPCR during ANC visits and community sessions |
| Facilitator | Help enroll in government benefit schemes |
| Planner | Assist in making a written BPCR plan |
| Observer | Monitor signs of risk or delay in preparation |
| Communicator | Coordinate with ASHA, referral centers, and transport services |
| Supporter | Reassure and motivate the woman and family to prepare early |
📋 BPCR PLAN FORMAT (Simple Table):
| Component | Action Planned |
|---|---|
| Health facility | PHC, CHC, or district hospital |
| Transport | Auto, ambulance (108), neighbor’s car |
| Funds saved | ₹3000 |
| Companion | Husband / sister |
| Blood donor | Cousin (B+) |
| Danger signs awareness | Yes / No |
| Birth kit packed | Yes / No |
✅ BENEFITS OF BPCR:
- Timely care in emergencies
- Safe delivery with skilled attendance
- Reduced maternal and neonatal complications
- Increased family awareness and involvement
- Fewer home deliveries and unsafe practices
Health Education on Exclusive Breastfeeding (EBF)
✅ INTRODUCTION
Exclusive breastfeeding (EBF) means that the infant receives only breast milk — no other food or drink, not even water — for the first 6 months of life, except oral rehydration solution (ORS), drops, or syrups of vitamins, minerals, or medicines when medically needed.
EBF is recommended by the World Health Organization (WHO), UNICEF, and the Ministry of Health and Family Welfare (India) for optimal infant health and development.
🎯 OBJECTIVES OF BREASTFEEDING EDUCATION:
- Promote exclusive breastfeeding for 6 months
- Educate mothers on correct technique and timing
- Prevent common breastfeeding problems
- Encourage mother-baby bonding
- Improve infant survival and development
🧠 KEY MESSAGES TO EDUCATE MOTHERS:
1️⃣ Start Breastfeeding Early
- Begin within 1 hour of birth
- First milk (colostrum) is rich in antibodies and nutrients – essential for immunity
2️⃣ Feed Only Breast Milk for 6 Months
- No water, honey, animal milk, or food should be given
- Breast milk contains everything the baby needs — even in hot weather
3️⃣ Feed Frequently and on Demand
- Day and night, at least 8–12 times in 24 hours
- Let the baby finish one breast before switching
4️⃣ Recognize Signs of Effective Breastfeeding
- Baby latches well (mouth wide open, chin touching breast)
- Rhythmic sucking and swallowing
- Baby passes urine at least 6 times a day
- Steady weight gain
5️⃣ Do Not Use Bottles or Pacifiers
- They cause nipple confusion and can reduce milk supply
6️⃣ Continue Breastfeeding During Illness
- Both mother and baby should continue
- Breast milk provides protection from infection
🌟 BENEFITS OF EXCLUSIVE BREASTFEEDING:
| To Baby | To Mother |
|---|---|
| Enhances immunity, prevents infections | Promotes uterine involution (reduces bleeding) |
| Reduces risk of diarrhea, pneumonia | Delays return of menstruation (natural spacing) |
| Supports brain development | Lowers risk of breast and ovarian cancer |
| Prevents allergies and obesity | Creates emotional bonding |
| Easy to digest, always clean and ready | Cost-effective and convenient |
🤱 BREASTFEEDING TECHNIQUE – LATCHING & POSITION
Proper Position:
- Baby’s head and body aligned
- Baby facing the breast, tummy to tummy
- Mother supports breast with her hand
- Bring baby to breast (not breast to baby)
Proper Latch:
- Baby’s mouth covers areola, not just nipple
- Lower lip turned outward
- No clicking sounds or pain during feeding
🚼 SIGNS THAT THE BABY IS GETTING ENOUGH MILK:
- Baby sleeps well between feeds
- Gains weight after the first week
- Passes soft, yellow stool
- Satisfied and calm after feeds
💢 COMMON BREASTFEEDING PROBLEms AND SOLUTIONS:
| Problem | Cause | Management |
|---|---|---|
| Sore Nipples | Poor latch | Correct the latch, apply breast milk to nipple |
| Engorgement | Infrequent feeding | Feed frequently, warm compress |
| Blocked Duct/Mastitis | Incomplete emptying | Massage, feed on affected side, pain relief |
| Low Milk Supply | Stress, infrequent feeding | Increase frequency, skin-to-skin contact, hydration |
🧑⚕️ NURSE / MIDWIFE’S ROLE IN BREASTFEEDING EDUCATION:
- Educate: Antenatal and postnatal counseling on EBF
- Demonstrate: Correct positioning and latching
- Support: Encourage mothers who are tired or unsure
- Monitor: Baby’s feeding patterns and weight gain
- Empower: Help mothers overcome social or family pressures
- Involve family: Educate partners and caregivers about the importance of EBF
- Refer: Complicated cases to lactation consultants or pediatricians
📢 COMMUNITY-BASED MESSAGES (IEC/BCC):
- “Maa ka doodh, shishu ke liye amrit hai” (Mother’s milk is nectar for the baby)
- “Chhe mahine tak sirf maa ka doodh – na paani, na kuch aur”
- Posters, flipcharts, mothers’ support groups
- Counselling via ASHA, ANM, or health camps
Danger Signs of Pregnancy
✅ INTRODUCTION:
Danger signs of pregnancy are warning symptoms that indicate potential complications which can threaten the health or life of the mother, fetus, or both. Prompt recognition and immediate medical care are critical to prevent maternal and fetal morbidity and mortality.
Midwives and nurses play a vital role in educating pregnant women and families about these signs and encouraging timely health-seeking behavior.
🚨 GENERAL DANGER SIGNS TO WATCH FOR (Any Trimester):
| Danger Sign | Possible Complication |
|---|---|
| Severe vaginal bleeding | Miscarriage, placenta previa, abruption |
| Severe abdominal pain | Ectopic pregnancy, abruption, labor |
| Severe headache or blurred vision | Preeclampsia, high blood pressure |
| Swelling of face and hands | Preeclampsia |
| Fever and chills | Infection |
| Painful urination or burning | Urinary tract infection |
| Foul-smelling vaginal discharge | Infection |
| Convulsions or fits | Eclampsia |
| Loss of consciousness | Severe anemia, shock, eclampsia |
| Difficulty breathing | Anemia, cardiac issues, embolism |
📆 TRIMESTER-WISE DANGER SIGNS:
🔹 First Trimester (0–12 weeks):
| Danger Sign | Possible Indication |
|---|---|
| Vaginal bleeding or spotting | Threatened or missed abortion |
| Severe lower abdominal pain | Ectopic pregnancy, miscarriage |
| Fainting or dizziness | Anemia, ectopic pregnancy |
| High fever | Infection (UTI, TORCH) |
| Persistent vomiting (Hyperemesis gravidarum) | Dehydration, electrolyte imbalance |
🔹 Second Trimester (13–27 weeks):
| Danger Sign | Possible Indication |
|---|---|
| Bleeding or watery discharge | Threatened abortion, PROM |
| Abdominal pain or backache | Preterm labor, UTI |
| Decreased fetal movement (after 20 weeks) | Fetal distress or death |
| Sudden swelling of hands/face | Preeclampsia |
| High blood pressure symptoms | PIH, gestational hypertension |
🔹 Third Trimester (28–40 weeks):
| Danger Sign | Possible Indication |
|---|---|
| Vaginal bleeding | Placenta previa, placental abruption |
| Leaking fluid before 37 weeks | Preterm PROM |
| Severe abdominal pain with bleeding | Abruption placentae |
| Decreased or no fetal movement | Fetal hypoxia or death |
| Severe headache, visual disturbances | Severe preeclampsia |
| Convulsions | Eclampsia |
| Difficulty breathing | Pulmonary embolism, severe anemia |
| Signs of labor before 37 weeks | Preterm labor |
🧑⚕️ ROLE OF MIDWIFE / NURSE:
- Educate all pregnant women and families about danger signs at each ANC visit
- Use simple language and visual aids (charts, posters)
- Encourage women to report symptoms immediately
- Monitor for these signs during home visits and health camps
- Refer urgently to higher-level health facilities if any danger sign is observed
- Document and follow up on all referred cases
- Involve ASHA/ANM for community support and emergency transport
📢 KEY EDUCATION MESSAGES FOR PREGNANT WOMEN:
- “Bleeding anytime in pregnancy is not normal — go to the hospital immediately.”
- “If the baby is not moving like usual — don’t wait, seek help.”
- “Swelling of face, headache, and blurred vision can be signs of high BP — act fast.”
- “Labor pains before 9 months could mean preterm labor — go to the hospital.”
Recognition of Ruptured Membranes (Spontaneous Rupture of Membranes – SROM)
✅ INTRODUCTION:
Rupture of membranes refers to the breaking of the amniotic sac (bag of waters), resulting in the leakage of amniotic fluid through the cervix and vagina. This can occur:
- Spontaneously (on its own) before or during labor
- Or be artificially induced (Amniotomy) by a healthcare provider
Recognizing spontaneous rupture of membranes (SROM) is essential for safe and timely labor management, and to prevent infection or complications.
🧠 TYPES OF RUPTURE:
| Type | Description |
|---|---|
| Term PROM | Rupture after 37 weeks of gestation but before labor starts |
| Preterm PROM (PPROM) | Rupture before 37 weeks of gestation |
| Prolonged ROM | Rupture of membranes lasting >18 hours before delivery |
| Premature Rupture of Membranes (PROM) | Rupture before the onset of labor |
🔍 RECOGNITION – HOW TO IDENTIFY RUPTURED MEMBRANES:
1️⃣ Maternal Reported Symptoms:
- Sudden gush or continuous trickle of clear or pale fluid from the vagina
- Wetness in underwear that does not stop
- May or may not be associated with labor pains
- Fluid is odorless or slightly sweet in smell
- No control over leakage (unlike urine)
2️⃣ Assessment Techniques by Nurse/Midwife:
| Method | What to Observe |
|---|---|
| Visual inspection | Use a sterile speculum to check for fluid pooling in the vagina |
| Nitrazine Test | Litmus paper turns blue if fluid is alkaline (amniotic fluid) |
| Fern Test | A sample of fluid shows a fern-like pattern under microscope |
| AmniSure or ROM Plus test (if available) | Detects specific amniotic proteins (used in hospital settings) |
3️⃣ Characteristics of Amniotic Fluid:
- Color: Clear to slightly milky
- Odor: Mildly sweet (not foul)
- Volume: May be a small leak or large gush
- Consistency: Watery (not thick or sticky like vaginal discharge)
⚠️ Meconium-stained fluid (green or brown) suggests fetal distress and needs urgent attention.
🚨 DANGER SIGNS WITH RUPTURED MEMBRANES:
- Fever or foul-smelling discharge → Risk of infection
- No uterine contractions within 24 hours → Risk of prolonged ROM
- Cord prolapse (cord felt in vagina or visible outside) → Emergency
- Preterm rupture (<37 weeks) → High risk to fetus (lungs immature)
- Decreased fetal movement → Possible distress
🧑⚕️ ROLE OF NURSE / MIDWIFE:
🌼 On Recognition of Ruptured Membranes:
- Stay calm and reassure the woman
- Instruct her to lie on her side and limit movement (if not in labor)
- Avoid vaginal examinations unless sterile or indicated (to prevent infection)
- Use sterile pads or towels to observe color and amount of fluid
- Check fetal heart rate immediately
- Record:
- Time of rupture
- Color, amount, and odor of fluid
- Associated symptoms (pain, bleeding, fever)
🌼 Actions Based on Situation:
| Scenario | Action |
|---|---|
| Term with contractions | Admit for labor monitoring |
| Term without contractions | Observe for 12–24 hours; induce if needed |
| Preterm (<37 weeks) | Hospitalize, administer antibiotics, corticosteroids (per doctor) |
| Cord prolapse | Trendelenburg position + emergency C-section |
| Foul-smelling discharge or fever | Suspect infection; report immediately |
✅ EDUCATION FOR MOTHERS:
- “If you feel sudden wetness or trickling of water, report to the hospital immediately.”
- “Do not insert anything into the vagina (no douching or intercourse).”
- “Monitor for fever, pain, bleeding, or baby’s movements.”
- “Always carry your ANC card to the hospital.”
Ongoing Risk Assessment in Pregnancy
✅ INTRODUCTION:
Ongoing risk assessment refers to the continuous and systematic evaluation of the mother and fetus during pregnancy to identify actual or potential risks that may complicate the course of pregnancy, labor, or delivery.
This process ensures early detection, timely referral, and appropriate intervention to reduce maternal and neonatal morbidity and mortality.
🎯 OBJECTIVES OF ONGOING RISK ASSESSMENT:
- Detect high-risk pregnancies early
- Prevent complications by timely management or referral
- Plan for safe delivery and postpartum care
- Ensure individualized care based on risk status
- Educate the woman and her family on signs that require attention
🧾 COMPONENTS OF RISK ASSESSMENT (Throughout ANC):
1️⃣ Maternal History Assessment:
| Factor | Risk Indicators |
|---|---|
| Obstetric history | Previous cesarean, stillbirth, miscarriage, multiple pregnancies |
| Medical history | Hypertension, diabetes, epilepsy, cardiac disease |
| Surgical history | Uterine surgeries, pelvic surgery |
| Family history | Genetic disorders, twins, diabetes, hypertension |
| Lifestyle factors | Smoking, alcohol, poor nutrition, domestic violence |
2️⃣ Physical Examination & Monitoring:
| Check-up | Risk Indicators |
|---|---|
| BP monitoring | High BP (>140/90) indicates PIH or preeclampsia |
| Fundal height | Discrepancy with gestational age → IUGR or poly/oligohydramnios |
| Fetal heart rate | Bradycardia or tachycardia → fetal distress |
| Edema | Face/hand swelling → sign of preeclampsia |
| Weight gain | Sudden excessive weight gain → fluid retention, PIH |
| Urine test | Proteinuria (PIH), glycosuria (GDM), infection |
3️⃣ Laboratory Investigations:
- Hemoglobin <10 g/dL → Anemia
- Positive VDRL/HBsAg/HIV → Infections
- Raised blood sugar → Gestational Diabetes
- Abnormal USG findings → IUGR, anomalies
- ICT positive (in Rh-negative mothers) → Risk of hemolytic disease
4️⃣ Psychosocial Assessment:
| Area | Concerns |
|---|---|
| Mental health | Depression, anxiety, low self-esteem |
| Support system | Isolation, lack of family support |
| Domestic violence | Safety concerns for mother and fetus |
| Economic status | Inability to access proper nutrition, transport, care |
⚠️ HIGH-RISK CONDITIONS TO MONITOR:
- Teenage pregnancy (<18 years) or advanced maternal age (>35 years)
- Multiple pregnancy (twins, triplets)
- Malpresentation (breech, transverse)
- Rh incompatibility
- Antepartum hemorrhage
- Preterm labor or PROM
- Gestational hypertension, eclampsia
- Polyhydramnios or oligohydramnios
- IUGR (Intrauterine Growth Restriction)
- Previous cesarean section or uterine surgery
🧑⚕️ ROLE OF NURSE / MIDWIFE IN ONGOING RISK ASSESSMENT:
| Function | Actions |
|---|---|
| Assessment | Regularly evaluate vitals, fetal growth, symptoms |
| Documentation | Update ANC records, risk factors, referrals |
| Communication | Discuss findings with medical team |
| Counseling | Educate mother about her condition and care needs |
| Referral | Refer promptly to higher center for complications |
| Support | Provide emotional support and reassurance |
📝 EXAMPLE: RISK SCORING SYSTEM
(Used in some settings for easy tracking)
| Factor | Points |
|---|---|
| Hb < 10 g/dL | 1 |
| Age <18 or >35 years | 1 |
| High BP or PIH | 2 |
| Previous cesarean | 2 |
| Twins | 3 |
➡️ Total score guides the level of care:
0–2 = Low risk, 3–4 = Moderate risk, 5+ = High risk
Cultural Needs in Maternal and Newborn Care
✅ INTRODUCTION:
Cultural needs refer to the beliefs, values, customs, traditions, and practices that influence how individuals and families experience pregnancy, childbirth, and healthcare. Meeting cultural needs in midwifery involves providing respectful, sensitive, and individualized care that honors the woman’s background, ethnicity, language, and spirituality.
🎯 OBJECTIVES OF CULTURALLY SENSITIVE MATERNAL CARE:
- Provide respectful and dignified care to women from all backgrounds
- Enhance trust and communication between caregiver and client
- Prevent misunderstanding, discrimination, or discomfort
- Improve maternal satisfaction, health-seeking behavior, and outcomes
- Encourage family and community support by respecting cultural norms
🧾 COMPONENTS OF CULTURAL NEEDS IN MATERNAL CARE:
1️⃣ Language and Communication
- Use local language or an interpreter if needed
- Use non-verbal cues, pictures, or models
- Respect how the woman prefers to be addressed
- Avoid medical jargon; explain terms clearly
2️⃣ Religious and Spiritual Beliefs
- Respect practices like prayers, fasting, blessings
- Allow religious articles or symbols during labor
- Understand restrictions related to blood transfusions, medicines, or certain foods
3️⃣ Modesty and Privacy
- Many cultures value modesty during examination
- Provide female healthcare workers when possible
- Use screens, drapes, and explain each step before touching
4️⃣ Family Involvement and Decision-Making
- In some cultures, decisions are made by husband, elder women, or extended family
- Include family members in discussions where appropriate
- Respect family hierarchy while also protecting the woman’s autonomy
5️⃣ Food and Dietary Practices
- Understand food taboos or preferences during pregnancy and postpartum
- Support culturally accepted nutritious alternatives
- Avoid forcing supplements or meals that go against beliefs
6️⃣ Traditional Beliefs and Practices
- Postnatal rituals, confinement periods, massage, use of herbs, etc.
- Allow safe practices as long as they do not harm the mother or baby
- Gently educate or discourage harmful practices (e.g., delaying breastfeeding, giving honey to newborns)
7️⃣ Birthing Preferences
- Preference for home birth vs hospital
- Birth positions, use of chants, rituals, or oils
- Role of birth companions (mother, husband, midwife, doula)
🌍 EXAMPLES OF CULTURAL NEEDS:
| Culture/Region | Practice |
|---|---|
| Indian subcontinent | Warm food post-delivery, confinement for 40 days |
| Middle Eastern | Preference for female providers, modest clothing |
| African | Strong family involvement, preference for traditional birth attendants |
| East Asian | “Sitting month” postpartum rest, avoiding cold foods |
| Christian/Muslim/Jain | Dietary restrictions (e.g., no pork/beef), prayer needs |
🧑⚕️ ROLE OF NURSE / MIDWIFE:
| Role | Responsibilities |
|---|---|
| Cultural assessor | Ask open-ended questions about beliefs and preferences |
| Educator | Provide respectful education on safe motherhood while valuing traditions |
| Advocate | Ensure woman’s cultural needs are met in hospital policies |
| Supporter | Listen actively and provide emotional comfort |
| Collaborator | Involve family and community support systems in care planning |
🛑 CHALLENGES IN MEETING CULTURAL NEEDS:
- Language barriers
- Lack of knowledge about diverse practices
- Institutional policies not accommodating traditions
- Time constraints in busy settings
- Conflict between safety and beliefs (e.g., refusal of interventions)
➡️ Requires sensitivity, flexibility, and communication skills
Women-Centered Care (WCC)
✅ INTRODUCTION
Women-Centered Care (WCC) is a philosophy of care that places the needs, preferences, rights, and dignity of the woman at the center of all decision-making and care practices. It focuses on individualized care, empowerment, respect, and collaborative partnerships between the woman and healthcare providers.
This model is essential in maternity and reproductive health services, where the woman’s experience is as important as clinical outcomes.
🎯 OBJECTIVES OF WOMEN-CENTERED CARE:
- Promote autonomy and informed decision-making for women
- Ensure respect, dignity, and compassion in all care interactions
- Create a safe, supportive, and inclusive environment
- Improve maternal satisfaction and health outcomes
- Address the physical, emotional, psychological, social, and cultural needs of women
🌼 CORE PRINCIPLES OF WOMEN-CENTERED CARE:
| Principle | Description |
|---|---|
| Respect for dignity | Treat every woman with kindness, privacy, and without judgment |
| Informed choice | Provide clear, unbiased information to allow women to make decisions |
| Holistic care | Consider emotional, mental, social, spiritual, and physical health |
| Collaboration | Women are partners in care, not passive recipients |
| Continuity of care | Promote ongoing relationships with midwives or care teams |
| Individualized care | Recognize that each woman has unique needs and preferences |
| Cultural sensitivity | Respect cultural, religious, and personal beliefs and practices |
👩🍼 APPLICATION OF WOMEN-CENTERED CARE IN MATERNAL HEALTH:
1️⃣ Antenatal Care
- Educate the woman about her pregnancy and choices
- Provide respectful and private examinations
- Discuss birth plans and preferences
- Screen for mental health, domestic violence, and cultural needs
2️⃣ Intrapartum (Labor and Delivery) Care
- Allow choice of birth position, pain relief, and birth companion
- Offer emotional support and continuous presence
- Obtain informed consent before procedures (e.g., episiotomy, vaginal exam)
- Respect labor pacing unless there is a medical reason to intervene
3️⃣ Postnatal Care
- Encourage rooming-in and skin-to-skin contact
- Support breastfeeding choices without pressure
- Screen for postpartum depression and mental well-being
- Involve the woman in decisions regarding family planning and baby care
🤝 BENEFITS OF WOMEN-CENTERED CARE:
| For Women | For Health System |
|---|---|
| Increased satisfaction and trust | Improved quality of care |
| Improved maternal and neonatal outcomes | Better communication and teamwork |
| Reduced anxiety and trauma | Fewer unnecessary interventions |
| Empowerment and confidence | Enhanced patient-provider relationships |
🧑⚕️ ROLE OF MIDWIFE / NURSE IN WOMEN-CENTERED CARE:
- Listen actively to the woman’s values, beliefs, and wishes
- Build trust through empathy, honesty, and respectful communication
- Educate with clear, culturally sensitive information
- Support decision-making and do not impose personal or institutional bias
- Protect privacy and promote dignity in all care settings
- Advocate for the woman in the healthcare team
- Document preferences and concerns in the care plan
- Encourage family involvement (with the woman’s consent)
🚫 BARRIERS TO WOMEN-CENTERED CARE:
- Over-medicalization of pregnancy and birth
- Lack of time and staffing
- Cultural or language barriers
- Provider bias or judgment
- Lack of training in communication and empathy
➡️ These can be overcome with education, awareness, and respectful practice.
Respectful and Compassionate Communication in Maternity Care
✅ INTRODUCTION:
Respectful and compassionate communication is the foundation of quality, woman-centered maternity care. It involves interacting with pregnant and postpartum women in a way that is kind, empathetic, non-judgmental, and respectful of their dignity, beliefs, and choices.
In maternity care, communication must be both informative and emotionally supportive, especially as pregnancy and childbirth are sensitive and life-changing experiences.
🎯 OBJECTIVES:
- Build trust and comfort between the woman and caregiver
- Promote informed decision-making and autonomy
- Reduce fear, anxiety, and emotional distress
- Prevent disrespect and abuse in childbirth settings
- Improve maternal satisfaction, cooperation, and health outcomes
🧭 PRINCIPLES OF RESPECTFUL & COMPASSIONATE COMMUNICATION:
| Principle | Explanation |
|---|---|
| Empathy | Understand and acknowledge the woman’s feelings and fears |
| Active Listening | Listen with full attention, without interrupting |
| Clarity | Use simple, jargon-free language the woman can understand |
| Privacy & Confidentiality | Maintain personal boundaries and do not share private information |
| Non-Judgmental Approach | Accept all backgrounds, cultures, and choices without criticism |
| Emotional Support | Offer encouragement, reassurance, and kindness |
| Timely Information | Provide clear explanations before any procedure or action |
| Body Language | Maintain eye contact, use a calm tone, and respectful gestures |
👩🍼 EXAMPLES IN MATERNAL CARE:
| Situation | Respectful Response |
|---|---|
| Woman is in pain during labor | “You are doing great. I am right here with you.” |
| Woman refuses a procedure | “I understand your concern. Let me explain your options.” |
| Woman is anxious about delivery | “Many mothers feel the same. Let’s talk about what will happen.” |
| Woman speaks a different language | Use an interpreter, visual aids, or local language support |
| Cultural or religious belief affects care | Respect her practice unless it poses harm, and explain alternatives gently |
🤰 COMMON COMMUNICATION SCENARIOS & APPROACHES:
🔹 Before a Procedure:
“I would like to check your blood pressure now. May I go ahead?”
🔹 During Examination:
“Let me know if you feel any discomfort. You can stop me anytime.”
🔹 When Discussing Diagnosis:
“Your blood pressure is a little high. I will explain what that means and how we can manage it together.”
🔹 When the Woman is Upset or Afraid:
“It’s okay to feel this way. You are not alone—we will support you every step.”
🧑⚕️ ROLE OF NURSE / MIDWIFE IN COMMUNICATION:
- Create a safe and respectful environment
- Introduce yourself clearly and explain your role
- Listen actively to the woman’s story, concerns, and feelings
- Provide health information in a calm, positive, and understandable way
- Ask for consent before exams or procedures
- Reassure and encourage throughout labor and postpartum
- Ensure privacy in the labor room, ANC clinic, and postnatal ward
- Include the family (with consent) in communication and decisions
- Document all care discussions and decisions made
📌 COMMON BARRIERS TO RESPECTFUL COMMUNICATION:
- Time constraints in busy hospitals
- Language or cultural differences
- Provider stress or burnout
- Lack of training in communication skills
- Provider bias or judgmental attitude
➡️ These can be overcome through training, awareness, and practice.
✅ BENEFITS OF RESPECTFUL AND COMPASSIONATE COMMUNICATION:
- Increases maternal trust and satisfaction
- Improves cooperation and adherence to care
- Enhances safe childbirth experiences
- Reduces complaints and conflicts
- Builds positive professional relationships
Alternative Birthing Positions
✅ INTRODUCTION:
Traditionally, many hospitals follow the supine (lying on the back) position for childbirth. However, alternative birthing positions are those non-supine positions that women may adopt during labor and delivery to enhance comfort, labor progress, and natural birthing mechanisms.
Allowing a woman to choose her preferred birthing position is part of respectful, women-centered care, and can improve both the physical and emotional experience of childbirth.
🧘♀️ COMMON ALTERNATIVE BIRTHING POSITIONS:
1️⃣ Squatting Position
- Woman squats down with knees bent and hips open
- May use squatting bar, support from companion, or a stool
Benefits:
- Widens pelvic outlet
- Uses gravity to aid fetal descent
- Effective pushing and shorter second stage
2️⃣ Sitting Position
- Woman sits on a birth stool, chair, or edge of bed
Benefits:
- Promotes gravity
- Comfortable and easy to monitor
- Good for women with back pain
3️⃣ Kneeling or Hands-and-Knees (All-Fours) Position
- Woman kneels on the floor/bed, leaning forward on hands or pillows
Benefits:
- Relieves back pressure
- Helps rotate posterior-positioned baby
- Reduces risk of perineal tears
4️⃣ Side-Lying (Lateral) Position
- Woman lies on her side with one leg supported
Benefits:
- Good for rest and relaxation
- Reduces pressure on perineum
- Recommended for high BP or FHR abnormalities
5️⃣ Upright Standing or Walking
- Woman stands or walks during early labor, may lean on support
Benefits:
- Uses gravity for descent
- Improves contractions
- Helps in early labor stages
6️⃣ Water Birth Position
- Woman labors or delivers in warm water tub
Benefits:
- Soothes pain and relaxes muscles
- Improves mobility and sense of control
- Less need for pain medication
➡️ Requires trained staff and hygienic setup
🤝 ROLE OF MIDWIFE / NURSE IN SUPPORTING ALTERNATIVE BIRTHING POSITIONS:
| Role | Actions |
|---|---|
| Educator | Teach women about various positions during ANC and in labor |
| Supporter | Encourage mobility and position changes during labor |
| Facilitator | Provide equipment (birth stools, mats, squatting bars) |
| Safety Monitor | Ensure positions are safe and do not compromise fetal monitoring or maternal condition |
| Empowerer | Respect the woman’s choice unless a medical reason prevents it |
| Documenter | Note the position used during delivery in the birth record |
⚠️ WHEN TO AVOID CERTAIN POSITIONS:
- Squatting or upright positions: Avoid in high-risk cases with bleeding, cord prolapse, or preeclampsia
- Water births: Avoid if infection, preterm labor, or meconium-stained liquor is present
- Hands-and-knees: Caution in women with joint pain or limited mobility
🌼 ADVANTAGES OF ALTERNATIVE BIRTHING POSITIONS:
- Enhances comfort and sense of control
- Uses gravity to support descent
- Improves uterine contractions
- Reduces duration of second stage
- Lowers rates of episiotomy and assisted delivery
- May reduce perineal trauma
Women’s Preferred Choices in Birthing Position
✅ INTRODUCTION:
During childbirth, many women develop preferences for certain birthing positions based on comfort, cultural beliefs, body mechanics, and their sense of control. Respecting a woman’s choice in birthing position is a key component of women-centered, respectful maternity care and leads to better satisfaction and outcomes.
🎯 OBJECTIVES OF SUPPORTING BIRTHING POSITION CHOICES:
- Empower women to feel in control during childbirth
- Enhance comfort and effectiveness of labor and pushing
- Improve maternal satisfaction and birth outcomes
- Reduce unnecessary interventions (e.g., episiotomy, assisted delivery)
- Respect cultural, personal, or religious preferences
🧘♀️ COMMONLY PREFERRED BIRTHING POSITIONS:
Women may prefer a birthing position based on pain relief, ease of movement, familiarity, or recommendations by caregivers.
1️⃣ Upright Positions (Squatting, Standing, Sitting)
| Features | Benefits |
|---|---|
| Uses gravity to aid fetal descent | |
| May be supported or with use of equipment (e.g., squatting bar, birth stool) | |
| Often preferred by women seeking active, natural birth |
✔️ Promotes faster descent and shorter second stage
✔️ Increases pelvic dimensions
✔️ Reduces need for assisted delivery
2️⃣ Hands-and-Knees (All-Fours) Position
| Features | Benefits |
|---|---|
| Woman kneels with hands or arms resting on a support | |
| Often chosen in cases of back pain or posterior baby position |
✔️ Relieves backache
✔️ Helps rotate the fetus from posterior to anterior
✔️ Reduces perineal trauma
3️⃣ Side-Lying (Lateral) Position
| Features | Benefits |
|---|---|
| Woman lies on her side with upper leg supported | |
| Often preferred for comfort or when rest is needed |
✔️ Good for women with high BP or fatigue
✔️ Prevents compression of vena cava
✔️ Helps conserve energy
4️⃣ Sitting or Semi-Sitting Position
| Features | Benefits |
|---|---|
| Woman sits on a birthing chair, stool, or bed with back support | |
| Allows both mobility and comfort |
✔️ Uses gravity without too much strain
✔️ Allows good fetal monitoring
✔️ Preferred for controlled pushing
5️⃣ Supine or Lithotomy (on back with legs raised)
Most commonly used in hospitals but not usually the woman’s preferred choice.
| Limitation | Why many women avoid |
|---|---|
| Less use of gravity | |
| Can compress blood vessels | |
| Often chosen by providers for ease, not by women |
❌ Higher risk of assisted delivery and perineal tears
❌ Less comfortable for women during active labor
📌 FACTORS INFLUENCING WOMEN’S CHOICE OF POSITION:
| Factor | Impact |
|---|---|
| Cultural beliefs | Certain positions may be considered more acceptable or effective |
| Previous birth experience | Women may choose based on what worked for them before |
| Level of pain | Pain relief or discomfort guides position changes |
| Support from midwife or doula | Encouragement can help women try upright or active positions |
| Environment | Availability of tools (birthing balls, stools, clean floor space) affects choices |
| Freedom to move | Women with IVs, monitoring, or epidural may have limited options |
👩⚕️ ROLE OF MIDWIFE / NURSE IN SUPPORTING WOMEN’S CHOICES:
- Educate about different birthing positions during antenatal classes
- Encourage freedom of movement during labor
- Ask for the woman’s preferred position and explain all safe options
- Support her choice unless medically contraindicated
- Assist with equipment (birth stool, squatting bar, pillows)
- Provide continuous labor support and reassurance
- Monitor mother and fetus in all positions safely
- Respect cultural or personal values influencing her decision
✅ BENEFITS OF RESPECTING WOMEN’S CHOICE OF BIRTHING POSITION:
- Improves maternal satisfaction and confidence
- Enhances labor progress and efficiency
- Reduces perineal trauma and interventions
- Strengthens trust and communication between the woman and provider
- Promotes positive birth experience
Role of Doula / ASHA Worker in Maternal and Newborn Care
✅ INTRODUCTION
Both Doulas and ASHA workers are non-medical professionals who play a vital role in supporting pregnant women and new mothers, especially in low-resource or rural settings.
- A Doula is a trained birth companion who provides emotional, physical, and informational support during pregnancy, labor, and the postpartum period.
- An ASHA worker is a community-based health activist under the National Rural Health Mission (NRHM) in India, trained to motivate, assist, and link women to maternal and child health services.
Both work closely with nurses, midwives, and ANMs to ensure safe, respectful, and accessible care for every mother and baby.
🧘♀️ ROLE OF A DOULA:
A Doula is not a medical provider, but a trained support person for labor and birth.
🌼 During Antenatal Period:
- Educates the mother about pregnancy changes, diet, and exercises
- Helps in birth planning (positions, pain relief options, birth preferences)
- Reduces anxiety and emotional stress
- Promotes self-care and breastfeeding preparation
🌼 During Labor & Delivery:
- Provides continuous emotional support
- Suggests breathing techniques, massage, and relaxation
- Encourages the mother in her preferred birthing position
- Acts as an advocate for the mother’s choices and dignity
- Keeps the birth environment calm and respectful
🌼 Postnatal Support:
- Supports early breastfeeding and latching
- Encourages rest, nutrition, and newborn care
- Assists with emotional well-being and postpartum adjustment
- Refers to professionals in case of complications or depression
👣 BENEFITS OF HAVING A DOULA:
- Shorter labor duration
- Reduced need for cesarean and interventions
- Less pain medication required
- Better mother-infant bonding
- Higher rates of exclusive breastfeeding
- Positive birth experience and emotional support
🌾 ROLE OF ASHA (Accredited Social Health Activist):
ASHA is a female volunteer from the community, trained under NHM, and acts as a link between the community and health system.
🌼 During Antenatal Period:
- Identifies and registers all pregnant women
- Ensures 4 ANC check-ups and TT immunization
- Counsels on diet, IFA, calcium, rest, and danger signs
- Promotes birth preparedness and institutional delivery
- Arranges transport and health facility referrals
- Assists in Janani Suraksha Yojana (JSY) benefits
🌼 During Labor & Delivery:
- Accompanies woman to the hospital
- Provides emotional and basic physical support
- Ensures woman has her ANC card, ID, and necessary items
- Coordinates with ANM, nurse, or midwife during labor
🌼 Postnatal and Newborn Care:
- Conducts home visits on Day 1, 3, 7, 14, 21, 28
- Monitors lochia, uterine involution, breastfeeding, baby’s weight
- Encourages immunization, exclusive breastfeeding, and family planning
- Educates on newborn danger signs
- Refers sick mother or baby to PHC or CHC
- Mobilizes community for Village Health and Nutrition Day (VHND)
🧑⚕️ COLLABORATION WITH MIDWIVES & NURSES:
| Activity | How Doula / ASHA Helps |
|---|---|
| Antenatal check-ups | Brings women to health center, educates about care |
| Birth preparedness | Helps make plans for transport, money, hospital |
| Labor & delivery | Provides support, encourages respectful birth practices |
| Home care | Follows up on mother’s and baby’s recovery |
| Health records | Maintains or updates records for tracking and referral |
| Community health | Conducts awareness programs on maternal and newborn care |
📋 QUALITIES OF A GOOD DOULA / ASHA:
- Trustworthy and compassionate
- Good listener and communicator
- Patient and calm
- Understands local language and culture
- Committed to women’s dignity and safety
- Willing to work closely with the health team