BSC SEM 1 UNIT 2 APPLIED NUTRITION AND DIETETICS
UNIT 2 Carbohydrates
Introduction
Carbohydrates are the primary source of energy for the body. They are organic compounds made up of carbon (C), hydrogen (H), and oxygen (O), usually in a 1:2:1 ratio. Carbohydrates are essential for energy production, brain function, and metabolism.
Composition of Carbohydrates
Introduction
Carbohydrates are organic compounds made up of three primary elements:
- Carbon (C)
- Hydrogen (H)
- Oxygen (O)
The general formula of carbohydrates is (CH₂O)n, where n is the number of carbon atoms.
Carbohydrates are the body’s primary source of energy and are classified based on their composition and structure.
Composition of Carbohydrates
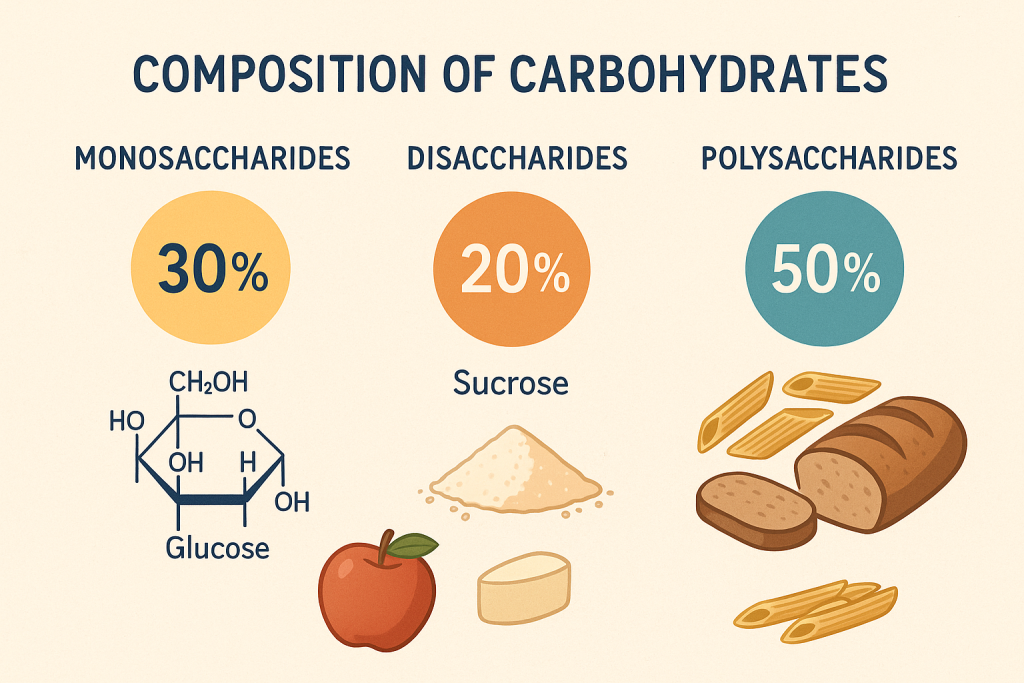
Carbohydrates are made up of sugar molecules (saccharides), which are categorized into three main types based on their complexity:
1. Sugars (Simple Carbohydrates)
- Definition: Small molecules that provide quick energy.
- Composition: Made of one or two sugar units.
- Examples:
- Monosaccharides (Single sugar unit) – Glucose, Fructose, Galactose.
- Disaccharides (Two sugar units) – Sucrose, Lactose, Maltose.
- Sources: Fruits, honey, milk, sugar.
2. Starches (Complex Carbohydrates)
- Definition: Long chains of sugar molecules used for energy storage.
- Composition: Made of multiple glucose units linked together.
- Types of Starches:
- Amylose – Straight-chain starch (e.g., found in rice, wheat).
- Amylopectin – Branched starch (e.g., found in potatoes, corn).
- Sources: Rice, wheat, potatoes, corn.
3. Cellulose (Dietary Fiber)
- Definition: A type of indigestible carbohydrate found in plant cell walls.
- Composition: Made of glucose molecules linked differently than starch.
- Function: Provides bulk to food, aids digestion, and prevents constipation.
- Sources: Vegetables, fruits, whole grains, legumes.
Chemical Structure of Carbohydrates
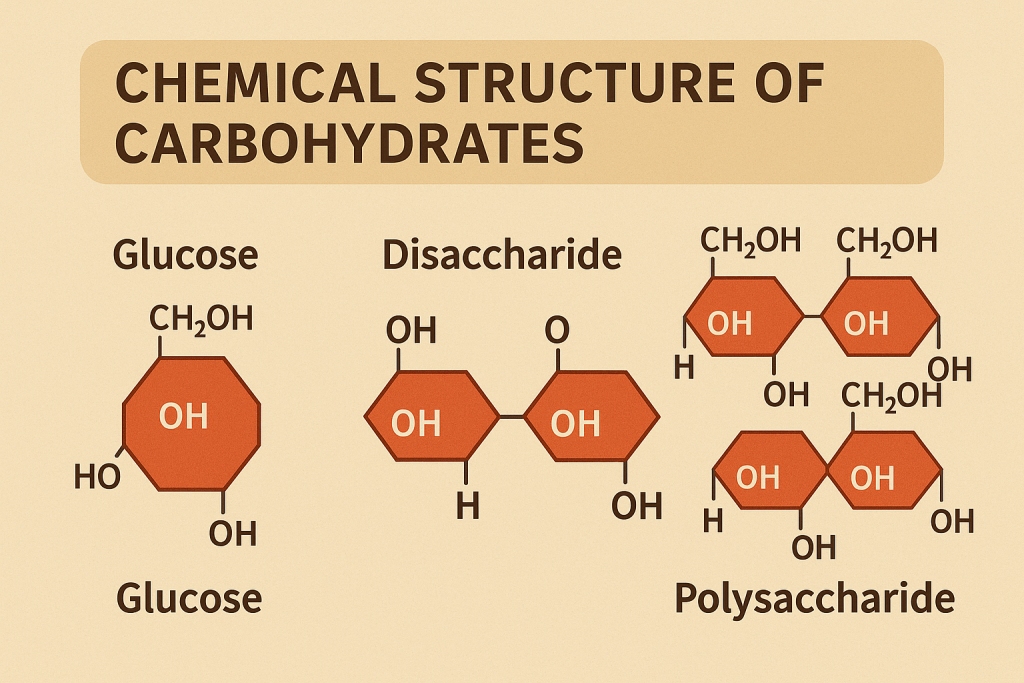
- Monosaccharides have a basic formula of C₆H₁₂O₆ (Glucose, Fructose, Galactose).
- Disaccharides are formed by combining two monosaccharides (e.g., Sucrose = Glucose + Fructose).
- Polysaccharides are large molecules made of many glucose units (e.g., Starch = multiple glucose units).
Classification of Carbohydrates
Introduction
Carbohydrates are organic compounds composed of carbon (C), hydrogen (H), and oxygen (O) in a ratio of 1:2:1. They are the primary source of energy for the body and are classified based on their complexity, structure, and digestibility.
Classification of Carbohydrates
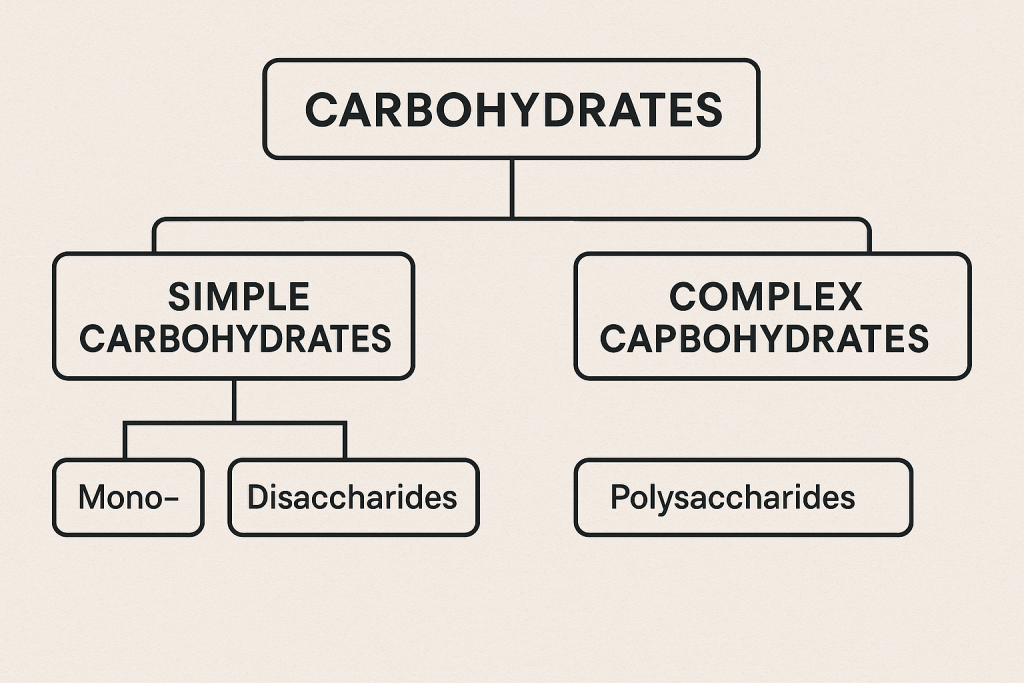
Carbohydrates are classified into three major types based on their structure and composition:
1. Simple Carbohydrates (Sugars)
- Contain one or two sugar units (monosaccharides or disaccharides).
- Easily digestible and provide quick energy.
- Sources: Fruits, honey, milk, sugar, candies.
a. Monosaccharides (Single Sugar Molecules)
- Definition: The simplest form of carbohydrates that cannot be broken down further.
- General Formula: C₆H₁₂O₆
- Examples:
- Glucose – Primary energy source (found in fruits, honey).
- Fructose – Sweetest sugar (found in fruits, honey).
- Galactose – Found in milk products.
b. Disaccharides (Two Sugar Units)
- Definition: Formed by the combination of two monosaccharides.
- General Formula: C₁₂H₂₂O₁₁
- Examples:
- Sucrose = Glucose + Fructose (Table sugar, sugarcane).
- Lactose = Glucose + Galactose (Milk sugar).
- Maltose = Glucose + Glucose (Found in germinating grains).
2. Complex Carbohydrates (Polysaccharides)
- Contain many sugar units linked together.
- Provide sustained energy and are harder to digest.
- Sources: Whole grains, rice, potatoes, legumes.
a. Oligosaccharides (3-10 Sugar Units)
- Definition: Short-chain carbohydrates found in plant foods.
- Examples: Raffinose, Stachyose (found in beans, legumes).
- Function: Act as prebiotics (support gut bacteria).
b. Polysaccharides (More than 10 Sugar Units)
- Definition: Long-chain carbohydrates that serve as energy storage or structural components.
- Examples:
- Starch – Energy storage in plants (Rice, wheat, potatoes).
- Glycogen – Energy storage in animals (Stored in liver and muscles).
- Cellulose – Structural carbohydrate in plants (Fiber found in fruits, vegetables).
- Chitin – Found in fungi and insect exoskeletons.
3. Digestibility-Based Classification1
Carbohydrates can also be classified based on whether the human body can digest them or not.
| Type | Function | Examples |
|---|---|---|
| Available Carbohydrates (Digestible) | Provide energy, easily absorbed | Glucose, Starch |
| Non-Available Carbohydrates (Indigestible) | Provide fiber, aid digestion | Cellulose, Hemicellulose |
Comparison of Different Types of Carbohydrates
| Type | Structure | Digestibility | Sources | Function |
|---|---|---|---|---|
| Monosaccharides | 1 sugar unit | Easily digested | Fruits, honey | Quick energy |
| Disaccharides | 2 sugar units | Easily digested | Milk, sugarcane | Energy supply |
| Oligosaccharides | 3-10 sugar units | Partially digestible | Beans, legumes | Gut health |
| Polysaccharides | Many sugar units | Slowly digested or indigestible | Rice, wheat, vegetables | Energy storage, digestion |
Sources of Carbohydrates
| Type | Food Sources |
|---|---|
| Simple Carbohydrates (Sugars) | Fruits, honey, milk, sugar, candy |
| Complex Carbohydrates (Starches) | Rice, wheat, potatoes, corn, legumes |
| Fiber (Cellulose & Hemicellulose) | Whole grains, vegetables, nuts, seeds |
Recommended Daily Allowance (RDA) for Carbohydrates
The RDA for carbohydrates varies based on age, gender, and activity level.
| Age Group | Carbohydrate Requirement (grams/day) |
|---|---|
| Infants (0-6 months) | 60 g |
| Children (1-3 years) | 130 g |
| Adolescents (14-18 years) | 130-150 g |
| Adults | 130-150 g |
| Pregnant Women | 175 g |
| Lactating Women | 210 g |
| Athletes | 200-400 g (depending on activity level) |
Carbohydrate Intake Guidelines
- 55-65% of daily calorie intake should come from carbohydrates.
- At least 50% should be from complex carbohydrates (whole grains, vegetables).
- Sugar intake should be limited to less than 10% of total calories.
- Dietary fiber intake: 25-30 g/day.
Functions of Carbohydrates
Introduction
Carbohydrates are the primary source of energy for the human body. They play a crucial role in metabolism, digestion, brain function, and overall health. Apart from providing energy, carbohydrates also contribute to various physiological processes.
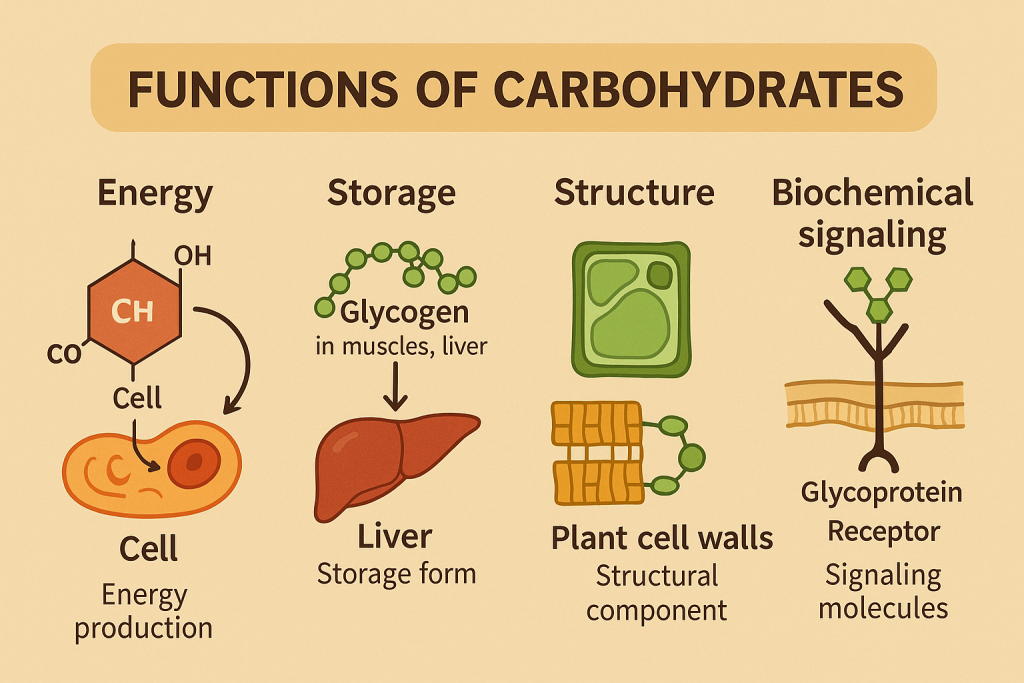
Major Functions of Carbohydrates
1. Primary Source of Energy
- Carbohydrates provide 4 kcal per gram.
- Glucose is the main fuel used by the brain, muscles, and nervous system.
- During physical activity, stored glycogen in muscles is converted to glucose for energy.
2. Protein-Sparing Action
- When sufficient carbohydrates are available, the body does not break down proteins for energy.
- This helps proteins to focus on tissue repair, enzyme production, and growth.
3. Aids in Fat Metabolism
- Carbohydrates are essential for the complete breakdown of fats.
- Insufficient carbohydrates lead to ketosis (accumulation of ketone bodies), which can cause metabolic imbalances.
4. Maintains Blood Sugar Levels
- Glucose homeostasis is regulated by insulin (lowers glucose) and glucagon (raises glucose).
- Complex carbohydrates (whole grains, fiber-rich foods) help in gradual absorption and stable blood sugar.
5. Supports Brain and Nervous System Function
- The brain relies on glucose as its primary fuel.
- A lack of carbohydrates can lead to fatigue, mental confusion, and reduced cognitive function.
6. Provides Dietary Fiber for Digestion
- Cellulose and fiber from plant foods aid in digestion, prevent constipation, and promote gut health.
- Soluble fiber (found in oats, legumes) helps in cholesterol control.
- Insoluble fiber (found in whole grains, vegetables) supports bowel movements.
7. Helps in Body Weight Regulation
- High-fiber carbohydrates promote fullness (satiety), reducing overeating.
- Balanced carbohydrate intake helps in maintaining a healthy weight.
8. Supports Immune Function
- Some carbohydrates (glycoproteins) are involved in immune response and cell signaling.
- They help in the recognition of pathogens and the formation of antibodies.
9. Acts as a Structural Component
- Certain carbohydrates (ribose, deoxyribose) are essential components of DNA and RNA, which are responsible for genetic information.
- Glycoproteins and glycolipids are involved in cell communication and membrane structure.
10. Storage of Energy (Glycogen)
- Excess glucose is stored as glycogen in the liver and muscles for later use.
- During fasting or intense exercise, glycogen is converted back to glucose to supply energy.
Summary Table of Carbohydrate Functions
| Function | Description | Example |
|---|---|---|
| Energy Source | Provides 4 kcal per gram | Glucose, Starch |
| Protein-Sparing | Prevents protein breakdown | Sufficient carbohydrate intake |
| Fat Metabolism | Prevents ketosis by aiding fat breakdown | Balance of fats and carbs |
| Blood Sugar Regulation | Maintains stable glucose levels | Insulin, Glucagon |
| Brain Function | Glucose is the main fuel for the brain | Cereals, Fruits |
| Digestive Health | Fiber aids digestion and prevents constipation | Whole grains, Vegetables |
| Weight Management | Increases satiety and reduces overeating | Fiber-rich foods |
| Immune Function | Supports immune response | Glycoproteins |
| Structural Role | Part of DNA, RNA, and cell membranes | Ribose, Glycolipids |
| Energy Storage | Stored as glycogen in liver and muscles | Glycogen |
Energy in Nutrition: Unit of Energy (Kcal) –
Introduction
Energy is essential for the growth, development, and functioning of the human body. In nutrition, energy refers to the capacity of food to fuel bodily functions such as movement, digestion, circulation, and metabolism. The body derives energy from macronutrients (carbohydrates, proteins, and fats), which are broken down during metabolism.
Unit of Energy in Nutrition: Kilocalorie (Kcal)
Definition of Kilocalorie (Kcal)
- A kilocalorie (Kcal) is the unit of measurement for energy provided by food.
- 1 Kcal = 1,000 calories (small calories).
- In simple terms, 1 Kcal is the amount of heat required to raise the temperature of 1 kilogram of water by 1°C.
- In nutrition, the term “Calorie” with a capital C is often used interchangeably with Kcal.
Energy Yield from Macronutrients
Different nutrients provide different amounts of energy:
| Nutrient | Energy Value (Kcal per gram) | Examples |
|---|---|---|
| Carbohydrates | 4 Kcal/g | Rice, wheat, fruits, potatoes |
| Proteins | 4 Kcal/g | Meat, fish, eggs, legumes |
| Fats | 9 Kcal/g | Butter, oil, nuts, seeds |
| Alcohol (not a nutrient) | 7 Kcal/g | Beer, wine, spirits |
Sources of Energy
- Primary Energy Source: Carbohydrates (55-65% of total energy intake).
- Secondary Energy Source: Fats (long-term energy storage).
- Protein as Energy: Used when carbohydrate and fat intake is insufficient.
Importance of Energy in Nursing and Nutrition
Energy is crucial for bodily functions in all individuals, especially in clinical settings where nutrition plays a key role in patient recovery and health maintenance.
1. Energy for Basic Metabolic Functions
- Basal Metabolic Rate (BMR): The minimum energy required for vital functions such as breathing, circulation, and cell repair.
- Resting Energy Expenditure (REE): Similar to BMR but includes minimal activity.
2. Energy for Physical Activity
- Light Activity: 30-50% of BMR (e.g., walking, light household work).
- Moderate Activity: 50-70% of BMR (e.g., brisk walking, exercise).
- Heavy Activity: 70-100% of BMR (e.g., running, manual labor).
3. Energy for Growth and Development
- Children and Adolescents: Require higher energy intake for rapid growth.
- Pregnancy and Lactation: Increased Kcal needs for fetal development and milk production.
4. Energy for Disease Recovery
- Malnutrition and Wasting Conditions: Require high-calorie diets to restore energy balance.
- Surgical and Trauma Patients: Need additional energy for wound healing and tissue repair.
Energy Requirements in Different Groups
The Recommended Daily Allowance (RDA) for energy varies based on age, gender, and activity level.
| Age Group | Energy Requirement (Kcal/day) |
|---|---|
| Infants (0-6 months) | 500-550 Kcal |
| Children (1-3 years) | 1000-1300 Kcal |
| Adolescents (14-18 years) | 2000-2800 Kcal (Males), 1800-2400 Kcal (Females) |
| Adults (Sedentary) | 2000-2500 Kcal (Males), 1600-2000 Kcal (Females) |
| Pregnant Women | +300 Kcal |
| Lactating Women | +500 Kcal |
| Elderly (60+ years) | 1800-2200 Kcal |
Energy Balance in Nursing Practice
Energy balance is critical in patient care, ensuring that calorie intake meets energy expenditure.
1. Positive Energy Balance
- Calorie intake > Energy expenditure
- Leads to weight gain and obesity.
- Seen in sedentary lifestyles and high-fat diets.
2. Negative Energy Balance
- Calorie intake < Energy expenditure
- Leads to weight loss, muscle breakdown, and fatigue.
- Seen in malnutrition, eating disorders, and critical illness.
3. Clinical Applications in Nursing
- Assessing Nutritional Status: Using BMI, dietary history, and calorie counting.
- Monitoring Malnutrition Risks: Identifying underweight or obese patients.
- Providing Diet Counseling: Recommending nutritionally balanced diets for patients with chronic diseases like diabetes, heart disease, and obesity.
Basal Metabolic Rate (BMR)

Introduction
Basal Metabolic Rate (BMR) is the minimum amount of energy required by the body to perform its basic vital functions while at rest. These functions include:
- Breathing
- Circulation (heart pumping)
- Cellular metabolism
- Body temperature regulation
- Brain function
- Muscle tone maintenance
Since BMR accounts for 60-75% of total daily energy expenditure (TDEE), it plays a crucial role in energy balance, weight management, and nutrition planning in nursing care.
Definition of BMR
- Basal Metabolic Rate (BMR) refers to the rate at which the body burns calories to maintain basic physiological functions at complete rest, in a neutral temperature environment, and after an overnight fast.
- It is measured in kilocalories per day (Kcal/day).
Key Characteristics of BMR
- Measured under resting conditions (fasting for 12 hours, complete physical rest).
- Represents energy used for vital organs (heart, lungs, liver, kidneys, brain, muscles).
- Accounts for 60-75% of total energy expenditure in most individuals.
- Influences caloric intake and weight management in patients.
How to Measure BMR?
1. Direct Calorimetry
- Measures heat production from the body in a controlled environment.
- Highly accurate but expensive and rarely used.
2. Indirect Calorimetry (Most Common)
- Measures oxygen consumption and carbon dioxide production.
- Uses a metabolic cart in hospitals or research settings.
3. Predictive Equations (Estimated BMR)
Several formulas help estimate BMR based on age, weight, height, and gender.
a. Harris-Benedict Equation (Most Common)
Used to calculate BMR based on body weight, height, and age.
- For Men:BMR=88.36+(13.4×weight in kg)+(4.8×height in cm)−(5.7×age in years)BMR = 88.36 + (13.4 \times \text{weight in kg}) + (4.8 \times \text{height in cm}) – (5.7 \times \text{age in years})BMR=88.36+(13.4×weight in kg)+(4.8×height in cm)−(5.7×age in years)
- For Women:BMR=447.6+(9.2×weight in kg)+(3.1×height in cm)−(4.3×age in years)BMR = 447.6 + (9.2 \times \text{weight in kg}) + (3.1 \times \text{height in cm}) – (4.3 \times \text{age in years})BMR=447.6+(9.2×weight in kg)+(3.1×height in cm)−(4.3×age in years)
b. Mifflin-St Jeor Equation (More Accurate)
- For Men: BMR=(10×weight in kg)+(6.25×height in cm)−(5×age in years)+5BMR = (10 \times \text{weight in kg}) + (6.25 \times \text{height in cm}) – (5 \times \text{age in years}) + 5BMR=(10×weight in kg)+(6.25×height in cm)−(5×age in years)+5
- For Women: BMR=(10×weight in kg)+(6.25×height in cm)−(5×age in years)−161BMR = (10 \times \text{weight in kg}) + (6.25 \times \text{height in cm}) – (5 \times \text{age in years}) – 161BMR=(10×weight in kg)+(6.25×height in cm)−(5×age in years)−161
BMR and Total Daily Energy Expenditure (TDEE)
To determine the total calories a person needs daily, BMR is multiplied by an activity factor.
TDEE Formula:
TDEE=BMR×Activity LevelTDEE = BMR \times \text{Activity Level}TDEE=BMR×Activity Level
| Activity Level | Multiplier | Description |
|---|---|---|
| Sedentary | BMR × 1.2 | Little or no exercise |
| Lightly Active | BMR × 1.375 | Light exercise (1-3 days/week) |
| Moderately Active | BMR × 1.55 | Moderate exercise (3-5 days/week) |
| Very Active | BMR × 1.725 | Hard exercise (6-7 days/week) |
| Super Active | BMR × 1.9 | Intense training or physical labor |
Clinical Importance of BMR in Nursing
1. Nutritional Assessment
- Helps in determining caloric needs for malnourished patients.
- Guides diet planning for diabetic, renal, and cardiac patients.
2. Weight Management
- Weight Gain: If energy intake > BMR, excess calories are stored as fat.
- Weight Loss: If energy intake < BMR, the body burns stored fat.
3. Managing Metabolic Disorders
- Hyperthyroidism: Increased BMR → Needs higher caloric intake.
- Hypothyroidism: Decreased BMR → Requires calorie-controlled diets.
4. Dietary Planning for Special Populations
- Pregnant women need extra calories to support fetal growth.
- Elderly require fewer calories due to reduced BMR.
5. ICU and Critical Care Nutrition
- Patients on ventilators or post-surgery require precise calorie intake based on BMR.
BMR and Energy Requirements for Different Age Groups
| Age Group | BMR Range (Kcal/day) |
|---|---|
| Infants (0-6 months) | 500-600 |
| Children (1-3 years) | 900-1200 |
| Adolescents (14-18 years) | 1400-2000 |
| Adults (Sedentary) | 1400-1800 (Females), 1600-2200 (Males) |
| Elderly (60+ years) | 1200-1600 |
Summary Table of BMR Concepts
| Factor | Effect on BMR |
|---|---|
| Age | Decreases with aging |
| Gender | Higher in males due to muscle mass |
| Muscle Mass | Increases BMR |
| Fat Mass | Decreases BMR |
| Hormones (Thyroid) | Increases or decreases BMR |
| Climate | Cold climates increase BMR |
| Physical Activity | Increases BMR |
Factors Affecting Basal Metabolic Rate (BMR)
Introduction
Basal Metabolic Rate (BMR) is the amount of energy the body requires at rest to maintain essential functions such as breathing, circulation, temperature regulation, and cellular metabolism. It accounts for 60-75% of total daily energy expenditure (TDEE) and varies among individuals based on several factors.
Understanding factors affecting BMR is crucial in nutrition and nursing for dietary planning, weight management, and clinical care.
Factors Affecting BMR
BMR is influenced by biological, physiological, and environmental factors.
1. Age
- BMR is highest in infants and children due to rapid growth and high metabolic activity.
- BMR gradually decreases with age due to a decline in muscle mass and hormonal changes.
- Elderly individuals have a lower BMR because of reduced physical activity and muscle loss (sarcopenia).
2. Gender
- Men have a higher BMR than women because of greater muscle mass and lower body fat percentage.
- Women have a lower BMR due to higher fat composition and hormonal differences (e.g., estrogen effects).
- During pregnancy and lactation, BMR increases due to higher energy demands.
3. Body Composition (Muscle Mass vs. Fat)
- Muscle tissue is metabolically active, requiring more energy for maintenance.
- Higher muscle mass = Higher BMR (e.g., athletes, bodybuilders).
- Fat tissue requires less energy, so individuals with higher fat percentages have a lower BMR.
4. Body Size and Weight
- Larger body size = Higher BMR due to increased metabolic activity to maintain organ function.
- Overweight individuals may have a slightly higher BMR due to greater body mass, but the rate of calorie burn per kilogram is lower than in lean individuals.
5. Hormonal Influence
- Thyroid hormones (T3, T4) play a crucial role in regulating metabolism:
- Hyperthyroidism (Overactive thyroid) → Increases BMR (rapid weight loss, heat intolerance).
- Hypothyroidism (Underactive thyroid) → Decreases BMR (weight gain, fatigue).
- Other hormones affecting BMR:
- Growth Hormone (GH) – Increases BMR.
- Testosterone – Increases muscle mass and BMR.
- Estrogen and Progesterone – Slightly decrease BMR.
6. Climate and Environmental Temperature
- Cold Environments:
- Increase BMR as the body needs more energy to generate heat.
- Example: People living in cold regions have a higher BMR.
- Hot Environments:
- Slightly raise BMR due to increased sweating and body cooling mechanisms.
7. Physical Activity and Exercise
- Regular exercise increases BMR by building muscle mass.
- Endurance training (e.g., running, swimming) increases overall energy expenditure.
- Strength training (weight lifting) significantly boosts BMR by increasing lean muscle mass.
8. Dietary Factors
- Thermic Effect of Food (TEF): Energy used for digestion, absorption, and metabolism.
- Protein-rich diets increase BMR (high thermic effect).
- Carbohydrates and fats have a lower effect on BMR.
- Starvation and Fasting:
- Lower BMR as the body conserves energy.
- Crash diets reduce muscle mass and slow metabolism.
9. Fever and Illness
- BMR increases by ~7% for every 1°C rise in body temperature.
- Infections, burns, trauma, and surgery elevate BMR due to increased metabolic activity for healing.
10. Genetics and Heredity
- Some people naturally have a higher or lower BMR due to genetic variations in metabolism and muscle composition.
- Family history of obesity or lean body structure may influence BMR levels.
11. Stress and Emotional State
- Stress hormones (e.g., cortisol, adrenaline) can increase BMR in short-term stressful situations.
- Chronic stress may lead to metabolic imbalances, affecting BMR and weight gain/loss.
12. Sleep and Rest
- Lack of sleep decreases BMR and disrupts hormonal balance (leptin, ghrelin), increasing hunger and fat storage.
- Good sleep promotes a healthy metabolism and optimal BMR function.
13. Drugs and Medications
- Stimulants (e.g., caffeine, amphetamines) increase BMR.
- Certain medications (e.g., beta-blockers, antidepressants) lower BMR.
- Steroids and anabolic hormones increase muscle mass, raising BMR.
Summary Table of Factors Affecting BMR
| Factor | Effect on BMR |
|---|---|
| Age | Decreases with aging |
| Gender | Higher in males due to more muscle mass |
| Muscle Mass | More muscle → Higher BMR |
| Fat Mass | More fat → Lower BMR |
| Thyroid Hormones | Overactive (↑ BMR), Underactive (↓ BMR) |
| Climate | Cold climates increase BMR |
| Exercise | Increases BMR (especially resistance training) |
| Diet (TEF Effect) | Protein-rich diets slightly increase BMR |
| Fasting/Starvation | Lowers BMR to conserve energy |
| Fever/Illness | Increases BMR (~7% per 1°C rise) |
| Stress (Cortisol, Adrenaline) | Short-term increases BMR, chronic stress may lower it |
| Sleep | Lack of sleep decreases BMR |
| Drugs/Medications | Some drugs (stimulants) increase BMR, others lower it |
Clinical Importance of BMR in Nursing
1. Nutritional Assessment
- Used to calculate daily caloric needs for patients.
- Helps determine total daily energy expenditure (TDEE).
2. Weight Management
- Weight Gain: Caloric intake > BMR → Weight gain.
- Weight Loss: Caloric intake < BMR → Weight loss.
3. Diet Planning for Special Conditions
- Thyroid disorders: Adjust calorie intake based on hyperthyroidism/hypothyroidism.
- Malnutrition patients: Higher caloric intake needed to restore energy balance.
- Burn patients, trauma, surgery patients: Require high-calorie, high-protein diets due to elevated BMR.
4. ICU and Critical Care Nutrition
- Ventilator-dependent patients, post-surgical patients require BMR-based feeding to prevent underfeeding or overfeeding.
FOR UNLOCK 🔓 FULL COURSE NOW. MORE DETAILS CALL US OR WATSAPP ON- 8485976407
