B.SC-PAEDIA-UNIT-SIX-Child health emergencies
Child Health Emergencies: Poisoning – Causes, Prevention, and Treatment

Definition:
Poisoning in children occurs when they ingest, inhale, inject, or come in contact with toxic substances, leading to adverse health effects. It is a major pediatric emergency requiring immediate identification and treatment to prevent severe complications or death.
Common Causes of Poisoning in Children:
1. Household Chemicals & Cleaning Agents (Most Common Cause)
- Sources:
- Bleach, disinfectants, toilet cleaners, floor cleaners.
- Pesticides, paint thinners, drain cleaners, kerosene, alcohol-based sanitizers.
- Toxic Effects:
- Mouth and throat burns, vomiting, abdominal pain.
- Difficulty breathing, convulsions, or unconsciousness (Severe cases).
2. Medications (Overdose or Accidental Ingestion)
- Sources:
- Over-the-counter drugs (Paracetamol, Ibuprofen).
- Prescription medications (Antidepressants, Sleeping pills, Blood pressure medicines).
- Iron tablets, vitamins (Excess dose).
- Toxic Effects:
- Drowsiness, dizziness, unconsciousness.
- Liver failure (Paracetamol overdose).
- Seizures, respiratory depression (Opioids, Sedatives).
3. Food Poisoning
- Sources:
- Contaminated food (Salmonella, E. coli, Staphylococcus).
- Expired, improperly stored food.
- Toxic Effects:
- Nausea, vomiting, diarrhea.
- Abdominal cramps, dehydration, fever.
4. Poisonous Plants & Mushrooms
- Sources:
- Oleander, castor beans, nightshade, lily-of-the-valley.
- Wild mushrooms, foxglove.
- Toxic Effects:
- Hallucinations, dizziness, seizures.
- Respiratory depression, irregular heartbeats.
5. Inhaled Poisons (Toxic Gases & Smoke)
- Sources:
- Carbon monoxide (Car exhaust, Gas heaters, Generators).
- Chemical fumes (Bleach, Paint, Kerosene, Ammonia).
- Smoke inhalation (House fires).
- Toxic Effects:
- Headache, dizziness, unconsciousness.
- Breathing difficulties, cardiac arrest (Severe exposure).
6. Alcohol & Drug Poisoning
- Sources:
- Alcoholic beverages, mouthwashes, hand sanitizers.
- Recreational drugs (Marijuana, Cocaine).
- Toxic Effects:
- Drowsiness, vomiting, low blood sugar (Hypoglycemia).
- Respiratory failure, coma in severe cases.
7. Animal & Insect Bites (Venomous Poisoning)
- Sources:
- Snake bites, scorpion stings, spider bites.
- Jellyfish or marine creature venom.
- Toxic Effects:
- Swelling, severe pain, tissue necrosis.
- Paralysis, difficulty breathing, anaphylaxis.
Diagnosis of Poisoning in Children
- History of exposure (What was taken, How much, When).
- Blood and urine tests (To check toxin levels).
- Toxicology screening (Identifies specific poisons).
- Imaging (X-ray, CT scan – For metal poisons like lead or iron).
Treatment of Poisoning in Children
1. General First Aid Measures
✔ Assess ABCs (Airway, Breathing, Circulation).
✔ Call Poison Control Center or Emergency Services immediately.
✔ Check for level of consciousness, breathing, and signs of shock.
2. Specific Poison Management
| Poison Type | First Aid Measures |
|---|---|
| Chemical Poisoning (Bleach, Acids, Pesticides) | Rinse mouth, DO NOT induce vomiting, give milk/water. |
| Medicine Overdose (Paracetamol, Opioids, Sedatives) | Activated charcoal (If within 1 hour), Antidotes if available. |
| Food Poisoning (Bacteria, Contaminated food) | Oral Rehydration Solution (ORS) for dehydration. |
| Inhaled Poisons (Carbon Monoxide, Smoke inhalation) | Move child to fresh air, give oxygen therapy. |
| Snake Bite or Venomous Stings | Keep child still, immobilize limb, DO NOT suck venom, seek antivenom. |
Medical Treatment in Hospital
- IV Fluids – To prevent dehydration and shock.
- Activated Charcoal – Absorbs poison in the stomach (If given within 1 hour).
- Gastric Lavage (Stomach Pumping) – Only for severe poisoning cases.
- Antidotes (Specific to poison type):
- Paracetamol overdose → N-Acetylcysteine (NAC).
- Opioid poisoning → Naloxone.
- Iron poisoning → Deferoxamine.
- Organophosphate poisoning → Atropine.
- Oxygen Therapy – For carbon monoxide poisoning.
- Dialysis – For severe poisoning affecting kidneys.
Prevention of Poisoning in Children
1. Safe Storage of Household Chemicals & Medications
✔ Keep all cleaning products, pesticides, and medicines locked away in child-proof cabinets.
✔ Store household chemicals in their original containers (Never transfer to drink bottles).
✔ Label all toxic substances clearly.
2. Medication Safety
✔ Use child-resistant caps on all medications.
✔ Never refer to medicine as “candy” to encourage a child to take it.
✔ Dispose of expired or unused medications safely.
3. Supervision and Awareness
✔ Always supervise young children, especially in kitchens and bathrooms.
✔ Teach children about the dangers of unknown substances.
✔ Keep emergency numbers (Poison Control, Ambulance) easily accessible.
4. Food Safety Measures
✔ Ensure proper food handling, cooking, and storage.
✔ Wash hands before handling food and wash fruits and vegetables thoroughly.
✔ Avoid giving young children honey (Risk of botulism) or raw/undercooked food.
5. Avoiding Poisonous Plants & Mushrooms
✔ Identify and remove toxic plants from home and garden.
✔ Educate children not to eat unknown berries, flowers, or mushrooms.
6. Preventing Carbon Monoxide & Gas Poisoning
✔ Install carbon monoxide detectors in homes.
✔ Ensure proper ventilation when using gas appliances.
✔ Do not leave cars running in closed garages.
7. Alcohol & Drug Safety
✔ Keep alcohol, hand sanitizers, and personal care products out of reach.
✔ Educate teens about the dangers of drug and alcohol consumption.
8. Preventing Bites & Stings
✔ Teach children to avoid unknown animals and insects.
✔ Wear protective clothing in areas with snakes, scorpions, or spiders.
✔ Use insect repellents in high-risk areas.
Emergency Measures for Poisoning Prevention:
- Have a first-aid kit ready at home.
- Know the nearest hospital that treats poisoning cases.
- Educate caregivers, teachers, and babysitters on poison first-aid measures.
Key Points:
✔ Poisoning in children is a serious emergency that can be prevented with proper safety measures.
✔ Household chemicals, medications, and food poisoning are the most common causes.
✔ Treatment includes first aid, activated charcoal, antidotes, IV fluids, and gastric lavage.
✔ Safe storage, supervision, food hygiene, and public awareness are essential prevention strategies.
✔ Immediate action and emergency care can prevent severe outcomes.
Child Health Emergencies: Foreign Body Accidents – Causes and Prevention

Definition:
Foreign body accidents in children occur when a non-food object is inhaled, ingested, inserted into the nose, ears, or other body parts, leading to choking, airway obstruction, infections, or organ damage. It is a common pediatric emergency and requires immediate medical attention in severe cases.
Common Causes of Foreign Body Accidents in Children
Foreign bodies can enter the airway, digestive tract, nose, ears, and even genitourinary system, causing serious complications. The most common age group affected is between 6 months to 5 years, as children tend to explore objects by putting them in their mouths, noses, or ears.
1. Foreign Body Aspiration (Inhalation into the Airway – LIFE-THREATENING)
- Common Objects:
- Small toys, marbles, beads.
- Coins, buttons, pen caps.
- Peanuts, popcorn, grapes, hot dogs.
- Dangers:
- Choking, severe airway obstruction.
- Respiratory distress, cyanosis (Blue skin color).
- Death if the airway is completely blocked.
2. Foreign Body Ingestion (Swallowing Objects into the Digestive Tract)
- Common Objects:
- Coins, batteries, magnets.
- Small jewelry, buttons, seeds.
- Sharp objects (Needles, glass pieces).
- Dangers:
- Stomach pain, vomiting.
- Intestinal obstruction or perforation (If sharp).
- Poisoning (If button batteries or lead-containing objects are swallowed).
3. Foreign Bodies in the Nose
- Common Objects:
- Small beads, peas, beans.
- Erasers, cotton balls, paper.
- Dangers:
- Nasal blockage, difficulty breathing.
- Nasal infections, foul-smelling nasal discharge.
- Risk of aspiration into the lungs if inhaled.
4. Foreign Bodies in the Ear
- Common Objects:
- Small beads, insects, food particles.
- Cotton swabs (When pushed inside).
- Dangers:
- Ear pain, hearing loss.
- Ear infections, eardrum perforation (If sharp objects are inserted).
5. Foreign Bodies in the Eye
- Common Objects:
- Sand, dust, metal particles.
- Small toys, crayons, glass fragments.
- Dangers:
- Eye irritation, redness, excessive tearing.
- Corneal scratches, infections, vision impairment.
6. Foreign Bodies in the Genitourinary Tract
- Common Objects:
- Beads, small stones, paper.
- Toilet paper, plastic pieces.
- Dangers:
- Pain, infection, urinary blockage.
- Damage to the urethra or vagina.
Prevention of Foreign Body Accidents in Children
1. Supervision and Childproofing the Environment
✔ Never leave small objects within reach of young children.
✔ Regularly inspect toys for small detachable parts.
✔ Supervise children while eating (Avoid small, hard foods like peanuts, grapes, and popcorn).
2. Safe Eating Practices
✔ Cut food into small pieces for toddlers.
✔ Encourage chewing food properly before swallowing.
✔ Avoid giving children hard candies, gum, or hot dogs in large pieces.
3. Toy Safety
✔ Ensure toys meet safety standards (No detachable small parts).
✔ Avoid giving toys with batteries to small children.
✔ Select age-appropriate toys.
4. Household Safety Measures
✔ Keep batteries, coins, and sharp objects locked away.
✔ Avoid keeping small magnetic items near children.
✔ Do not allow children to play with small buttons, jewelry, or sewing materials.
5. Educate Caregivers and Parents
✔ Teach children not to put objects in their mouths, noses, or ears.
✔ Make caregivers, babysitters, and teachers aware of choking hazards.
✔ Learn basic first-aid for choking emergencies.
Emergency Management of Foreign Body Accidents
1. Foreign Body Aspiration (Choking) – LIFE-THREATENING
- Signs:
- Difficulty breathing, coughing, gagging.
- Cyanosis (Bluish skin, especially lips and fingers).
- Inability to cry, speak, or make sounds.
- Immediate Action (First Aid for Choking):
- Infants (<1 year):
- Give 5 back blows followed by 5 chest thrusts.
- Lay the infant face-down on your forearm, support the head, and give back blows.
- Children (>1 year):
- Perform the Heimlich maneuver (Abdominal thrusts) – Stand behind the child, place hands above the navel, and give quick inward and upward thrusts.
- Infants (<1 year):
2. Foreign Body Ingestion (Swallowed Objects)
- Signs:
- Drooling, refusal to eat.
- Vomiting, stomach pain.
- Blood in stool (If sharp object causes internal injury).
- Immediate Action:
- If small and non-toxic (Coin, seed, bead):
- Observe for passage in stool within 24-48 hours.
- If large, sharp, or a button battery:
- Do NOT induce vomiting.
- Seek emergency medical attention immediately.
- If multiple magnets were swallowed:
- Immediate surgery may be required to prevent intestinal damage.
- If small and non-toxic (Coin, seed, bead):
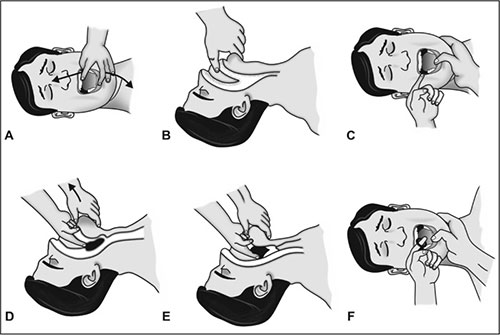
3. Foreign Bodies in the Nose
- Signs:
- Nasal blockage, difficulty breathing.
- Bad-smelling discharge, sneezing.
- Immediate Action:
- Encourage the child to breathe through the mouth.
- Try the “Parent’s Kiss Method” – Close the unaffected nostril and gently blow into the child’s mouth to expel the object.
- DO NOT insert tweezers or cotton swabs (Can push the object further).
4. Foreign Bodies in the Ear
- Signs:
- Ear pain, hearing loss.
- Foul-smelling ear discharge (If infection develops).
- Immediate Action:
- For small objects (Beads, buttons):
- Tilt the head to the side and allow gravity to help.
- For insects in the ear:
- Pour a few drops of warm water or mineral oil to flush it out.
- DO NOT try to remove with tweezers or sharp tools.
- For small objects (Beads, buttons):
5. Foreign Bodies in the Eye
- Signs:
- Excessive tearing, blinking, redness.
- Pain, difficulty opening the eye.
- Immediate Action:
- Rinse the eye with clean water or saline solution.
- Avoid rubbing the eye.
- Seek medical help if the object is embedded in the eye.
6. Foreign Bodies in the Genitourinary Tract
- Signs:
- Pain while urinating.
- Blood in urine, infection signs (Fever, swelling).
- Immediate Action:
- Do NOT attempt to remove the object at home.
- Seek immediate medical care.
When to Seek Emergency Medical Care?
- If the child is choking and cannot breathe.
- If the swallowed object is large, sharp, or a button battery.
- If the foreign body is causing severe pain, bleeding, or infection.
- If an insect or sharp object is stuck in the ear or eye.
- If magnets or multiple foreign bodies were ingested.
Key Points:
✔ Foreign body accidents are common in young children due to their natural curiosity.
✔ Choking on small objects, food, or toys can be life-threatening.
✔ Prevention includes childproofing the home, supervision, and toy safety.
✔ Emergency management involves first aid for choking, prompt medical attention for ingested objects, and safe removal of foreign bodies in the nose, ears, or eyes.
✔ Educating caregivers on foreign body hazards and first-aid techniques is essential.
Child Health Emergencies: Hemorrhage – Causes, Prevention, and Management
Definition:
Hemorrhage is excessive bleeding due to injury, trauma, or medical conditions, which can be internal or external. In children, hemorrhage is a life-threatening emergency that requires immediate medical intervention to prevent shock and organ failure.
Types of Hemorrhage:
- External Hemorrhage – Visible bleeding from cuts, wounds, or injuries.
- Internal Hemorrhage – Bleeding inside the body (Brain, Abdomen, Lungs).
- Arterial Bleeding – Bright red, spurting blood (Most dangerous).
- Venous Bleeding – Dark red, steady flowing blood.
- Capillary Bleeding – Slow oozing blood from minor cuts.
Causes of Hemorrhage in Children
1. Traumatic Causes (Most Common)
- Accidental Falls (Playgrounds, Stairs, Windows).
- Road Traffic Accidents (Bicycle, Pedestrian, Car Crashes).
- Sharp Object Injuries (Glass, Knives, Scissors).
- Sports Injuries (Fractures, Concussions, Cuts).
- Animal Bites or Deep Lacerations.
2. Medical Causes
- Bleeding Disorders (Hemophilia, Von Willebrand Disease).
- Leukemia & Blood Cancers.
- Vitamin K Deficiency (In Newborns).
- Severe Anemia (Reduced clotting ability).
3. Surgical & Postpartum Causes
- Complications after surgery (Uncontrolled bleeding).
- Birth injuries (Intracranial hemorrhage in newborns).
Prevention of Hemorrhage in Children
1. Injury Prevention at Home
✔ Keep sharp objects (Knives, Razors, Scissors) out of children’s reach.
✔ Use safety gates on stairs and secure windows.
✔ Keep electrical wires and furniture edges child-proofed.
2. Outdoor Safety Measures
✔ Ensure children wear helmets and knee guards while cycling.
✔ Teach road safety rules and supervise near traffic areas.
✔ Avoid letting children play near glass doors or sharp objects.
3. Preventing Sports & Playground Injuries
✔ Make children wear protective gear for sports.
✔ Ensure playgrounds have soft surfaces (Grass, Sand).
✔ Avoid high-risk stunts or unsafe play structures.
4. Medical & Surgical Precautions
✔ Screen for bleeding disorders in children with frequent bruising.
✔ Give Vitamin K at birth (To prevent newborn hemorrhagic disease).
✔ Monitor children for unusual bleeding after minor injuries.
Emergency Management of Hemorrhage in Children
Step 1: Initial Assessment
✔ Assess the severity of bleeding (Arterial, Venous, or Capillary).
✔ Check for signs of shock (Pale skin, Weak pulse, Rapid breathing).
✔ Ensure airway, breathing, and circulation (ABCs) are intact.
Management Based on Type of Hemorrhage
1. External Bleeding (Visible Blood Loss)
Immediate Actions:
- Apply Direct Pressure:
✔ Use a clean cloth or sterile gauze over the wound.
✔ Press firmly for 5-10 minutes (Do not remove the cloth). - Elevate the Injured Limb:
✔ Raise the bleeding area above heart level (Reduces blood flow). - Apply a Pressure Bandage:
✔ Wrap a bandage tightly to control bleeding but not cut off circulation. - Use a Tourniquet (Only for life-threatening bleeding):
✔ Apply 2 inches above the wound, tighten until bleeding stops.
✔ Note the time (Do not keep for more than 2 hours).
2. Internal Bleeding (Hidden Blood Loss – Dangerous)
Signs of Internal Bleeding:
✔ Abdominal pain, Swelling, Distended belly (Internal organ bleeding).
✔ Headache, Vomiting, Unconsciousness (Brain hemorrhage).
✔ Pale skin, Weak pulse, Rapid breathing (Shock).
✔ Coughing up blood or blood in urine.
Management:
✔ DO NOT give food or drink (Risk of surgery).
✔ Lay the child down with legs elevated (Improves blood circulation).
✔ Transport immediately to the hospital.
3. Arterial Bleeding (Bright Red, Spurting Blood – LIFE-THREATENING)
✔ Apply firm direct pressure with a thick cloth.
✔ If bleeding does not stop, use a tourniquet (Emergency only).
✔ Seek emergency medical help IMMEDIATELY.
4. Venous Bleeding (Dark Red, Steady Flowing Blood)
✔ Apply direct pressure and elevate the limb.
✔ Wrap the wound with a pressure bandage.
✔ Monitor for shock symptoms.
5. Minor Bleeding (Capillary Bleeding, Small Cuts & Scrapes)
✔ Clean the wound with saline or antiseptic.
✔ Apply pressure if needed, then cover with a bandage.
✔ Monitor for signs of infection (Redness, Swelling, Pus).
Hospital Management for Severe Hemorrhage
1. Fluid Resuscitation & Blood Transfusion
✔ IV Fluids (Normal Saline, Ringer’s Lactate) – To prevent shock.
✔ Blood Transfusion – If excessive blood loss occurs.
2. Medications to Control Bleeding
✔ Tranexamic Acid (TXA) – Prevents excessive clot breakdown.
✔ Vitamin K Injection – For newborns with bleeding disorders.
✔ Desmopressin (DDAVP) – Used in hemophilia or von Willebrand disease.
3. Surgical Intervention
✔ Suturing (For deep wounds, large cuts).
✔ Cauterization (Burning blood vessels to stop bleeding).
✔ Emergency Surgery (For internal bleeding in organs).
When to Seek Immediate Medical Help?
🚨 Call emergency services if:
✔ Bleeding does not stop after 10 minutes of pressure.
✔ The child is pale, weak, or unconscious.
✔ There is excessive blood loss from the head, neck, or abdomen.
✔ The wound is deep or gushing blood (Arterial bleeding).
✔ There is coughing or vomiting of blood.
Complications of Untreated Hemorrhage
- Hypovolemic Shock (Dangerously low blood volume).
- Organ Failure (Due to lack of oxygen supply).
- Infections (If open wounds are not treated properly).
- Death (If severe bleeding is not controlled in time).
Key Points:
✔ Hemorrhage in children can be external or internal and requires immediate attention.
✔ Common causes include falls, road accidents, sharp object injuries, and medical conditions.
✔ Prevention includes childproofing homes, safety during play, and medical precautions.
✔ First aid management includes direct pressure, elevation, and tourniquets (For life-threatening cases).
✔ Hospital treatment includes IV fluids, blood transfusions, medications, and surgery if needed.
✔ Early intervention can save lives and prevent complications.
Neonatal Advanced Life Support (NALS) – AHA Guidelines (2020-2025) in Full Detail
Introduction to Neonatal Advanced Life Support (NALS)
Neonatal Advanced Life Support (NALS), also known as Neonatal Resuscitation Program (NRP), is a set of systematic guidelines established by the American Heart Association (AHA) and the American Academy of Pediatrics (AAP) to improve neonatal survival through effective resuscitation practices.
NALS is used during and immediately after birth for neonates who experience respiratory distress, perinatal asphyxia, or cardiac arrest and require life-saving interventions.
Key Statistics on Neonatal Resuscitation
✔ Approximately 10% of newborns require some assistance at birth.
✔ 1% of newborns need extensive resuscitation, including chest compressions and medications.
✔ The first 60 seconds (“Golden Minute”) is critical for survival.
Indications for Neonatal Resuscitation
Resuscitation is needed if any of the following conditions are present at birth:
✔ Premature birth (<37 weeks gestation).
✔ Absent or weak breathing (Apnea) or gasping respirations.
✔ Heart rate (HR) <100 beats per minute (bpm).
✔ Poor muscle tone (Limp and floppy body).
✔ Meconium-stained amniotic fluid with poor respiratory effort.
✔ Maternal infections (Chorioamnionitis, GBS infection).
✔ Birth asphyxia (Prolonged labor, cord prolapse, placental abruption).
Neonatal Resuscitation Algorithm (NRP/NALS) – AHA Guidelines 2020-2025
Step 1: Initial Rapid Assessment (The First 30 Seconds)
As soon as the baby is born, assess three key factors:
✔ Gestational age (Full-term or preterm?).
✔ Breathing effort (Crying or not?).
✔ Muscle tone (Active or floppy?).
If the newborn is full-term, breathing well, and has good muscle tone → Provide routine newborn care (Skin-to-skin, Delayed cord clamping, Monitor breathing).
Step 2: Initial Stabilization (“Golden Minute” – First 60 Seconds)
If the baby does not meet the criteria for routine care, begin initial resuscitation:
- Provide warmth (Radiant warmer, Dry with warm towels).
- Position airway in a “sniffing” position (Slight neck extension).
- Clear secretions (If needed)
- Suction mouth first, then nose (Avoid deep suctioning).
- Stimulate breathing
- Gently rub the newborn’s back, flick the soles of the feet.
✔ Reassess Heart Rate (HR) at 30 seconds
- If HR ≥100 bpm and breathing well → Continue routine care.
- If HR <100 bpm, Gasping, or Apnea → Proceed to Positive Pressure Ventilation (PPV).
Step 3: Positive Pressure Ventilation (PPV) – If HR <100 bpm or Apnea Present
✔ Start PPV using a T-piece resuscitator or bag-mask ventilation (BMV).
✔ Ensure a proper mask seal and achieve visible chest rise.
✔ Provide ventilation at a rate of 40-60 breaths per minute.
✔ Use room air (21% oxygen) for term infants; 30-40% oxygen for preterm infants.
✔ Reassess HR and breathing after 30 seconds.
✔ If HR remains <100 bpm:
- Ensure adequate ventilation technique (Reposition mask, Suction airway).
- Increase FiO₂ as needed.
✔ If HR is improving and breathing is spontaneous:
- Gradually wean from PPV.
✔ If HR <60 bpm despite 30 seconds of PPV → Start Chest Compressions.
Step 4: Chest Compressions – If HR <60 bpm Despite PPV
✔ Use the Two-Thumb Encircling Technique:
- Place both thumbs on the lower third of the sternum.
- Encircle the chest with hands and provide support from the back.
✔ Compression Depth:
- At least 1/3rd of the chest diameter (Approx. 1.5 inches in neonates).
✔ Compression-to-Ventilation Ratio:
- 3:1 (90 compressions + 30 breaths per minute).
✔ Coordinate compressions with ventilation.
✔ Reassess HR every 30 seconds.
- If HR improves (>60 bpm) → Stop compressions but continue ventilation if needed.
- If HR remains <60 bpm → Administer Epinephrine.
Step 5: Medication Administration – If HR Remains <60 bpm
✔ Epinephrine (First-Line Medication)
- IV Route (Preferred): 0.01-0.03 mg/kg (1:10,000 dilution).
- ET Tube Route (If no IV access): 0.05-0.1 mg/kg (1:10,000 dilution).
✔ Volume Expansion (For Suspected Hypovolemia)
- Normal Saline or Ringer’s Lactate: 10 mL/kg IV bolus over 5-10 minutes.
- Consider Packed Red Blood Cells (PRBCs) if severe anemia is suspected.
Step 6: Advanced Airway Management
✔ If PPV fails to improve HR, consider:
- Endotracheal Intubation (ETT) – Confirm placement via CO₂ detector.
- Laryngeal Mask Airway (LMA) – If intubation is difficult.
✔ Indications for Intubation:
- Ineffective PPV.
- Meconium-stained fluid with respiratory distress.
- Need for prolonged respiratory support.
Step 7: Post-Resuscitation Care
✔ Monitor vital signs (HR, RR, SpO₂, BP, Glucose).
✔ Maintain normothermia (36.5 – 37.5°C).
✔ Prevent hypoglycemia (Treat if blood glucose <45 mg/dL).
✔ Consider NICU admission for continued monitoring.
Special Considerations in Neonatal Resuscitation
1. Preterm Neonates (<37 Weeks Gestation)
✔ Use plastic wrap or warming devices to prevent hypothermia.
✔ Avoid excessive oxygen (Use FiO₂ 30-40% initially).
✔ Gentle ventilation to avoid lung injury (Use CPAP if possible).
2. Meconium-Stained Amniotic Fluid
✔ If baby is vigorous (Good HR, Crying, Normal Tone) → No suctioning needed.
✔ If baby is non-vigorous (Poor tone, No cry, HR <100) → Intubation for suctioning before PPV.
3. Hypovolemic Shock or Severe Anemia
✔ Consider volume expanders (Normal Saline or PRBCs).
Key Updates in AHA 2020-2025 NALS Guidelines
✅ Routine Endotracheal Suctioning of Meconium-Stained Infants is NO LONGER Recommended
✅ More Emphasis on Delayed Cord Clamping (30-60 seconds) for Stable Babies
✅ Importance of Monitoring SpO₂ with Pulse Oximetry
✅ Avoidance of Excess Oxygen in Preterm Neonates
✅ Use of Laryngeal Mask Airway (LMA) if Intubation Fails
Key Takeaways
✔ NALS (NRP) is the standard protocol for neonatal resuscitation.
✔ The first 60 seconds (“Golden Minute”) is crucial for survival.
✔ PPV is the most effective initial intervention for non-breathing neonates.
✔ Chest compressions are indicated if HR <60 bpm after 30 seconds of PPV.
✔ Epinephrine and IV fluids are used for persistent bradycardia and hypovolemia.
✔ Post-resuscitation care includes temperature control, oxygen support, and glucose monitoring.
Pediatric Life Support (PLS) – AHA Guidelines (2020-2025) in Full Detail
Introduction to Pediatric Life Support (PLS)
Pediatric Life Support (PLS) is a structured resuscitation protocol designed for critically ill or injured infants and children who require immediate life-saving interventions. It includes Pediatric Basic Life Support (PBLS) and Pediatric Advanced Life Support (PALS).
The American Heart Association (AHA) updates these guidelines regularly to ensure effective management of pediatric emergencies, improving survival and outcomes in children.
Pediatric Basic Life Support (PBLS) – AHA Guidelines
PBLS focuses on early recognition of cardiac arrest, airway management, and high-quality cardiopulmonary resuscitation (CPR).
Step 1: Initial Assessment – Check Responsiveness and Breathing
✔ Assess child’s response (Tap and shout, “Are you okay?”).
✔ Look for normal breathing (Observe chest rise for 5-10 seconds).
✔ If unresponsive and not breathing normally → Activate Emergency Medical Services (EMS) and start CPR.
If a rescuer is alone:
- If sudden collapse is witnessed → Call EMS, Get an Automated External Defibrillator (AED), then start CPR.
- If collapse is unwitnessed → Start 2 minutes of CPR first, then activate EMS.
Step 2: Circulation – Check Pulse
✔ Infants (<1 year): Check brachial pulse (Inner arm, near elbow).
✔ Children (>1 year): Check carotid (Neck) or femoral (Groin) pulse.
If no pulse or HR <60 bpm with signs of poor perfusion (Weak pulse, Cyanosis, Poor capillary refill) → Start CPR.
Step 3: High-Quality Chest Compressions
✔ Compression depth: At least 1/3rd of the chest diameter (~1.5 inches in infants, ~2 inches in children).
✔ Compression rate: 100-120 per minute.
✔ Recoil: Allow full chest recoil after each compression.
✔ Interruptions: Minimize pauses in CPR.
Compression technique:
- Infants (<1 year, single rescuer): Two-finger technique (Place two fingers on the lower sternum).
- Infants (<1 year, two rescuers): Two-thumb encircling hands technique.
- Children (>1 year): Heel of one or both hands on lower sternum.
Compression-to-ventilation ratio:
- Single rescuer: 30:2 (30 compressions, 2 breaths).
- Two rescuers: 15:2 (15 compressions, 2 breaths).
Step 4: Ventilation (Rescue Breaths)
✔ If breathing is absent, provide rescue breaths.
✔ **Breaths should be delivered over 1 second each, with visible chest rise.
✔ Rescue breathing rate:
- Infants and children: 1 breath every 3-5 seconds (12-20 breaths per minute).
✔ If Bag-Mask Ventilation (BMV) is used:
- Ensure a proper seal, observe for chest rise.
- Avoid excessive ventilation, which can reduce cardiac output.
Step 5: AED Use for Defibrillation (If Needed)
✔ Attach AED as soon as available.
✔ Follow AED prompts and assess rhythm.
✔ If Shockable Rhythm (Ventricular Fibrillation/Pulseless Ventricular Tachycardia):
- Infants (<1 year): Manual defibrillator preferred, but AED with pediatric pads can be used.
- Children (1-8 years): AED with pediatric pads or dose attenuator.
- If no pediatric pads available, use adult pads (Do not overlap).
✔ Shock Energy:
- First shock: 2-4 J/kg.
- Subsequent shocks: 4-10 J/kg.
✔ After shock → Resume CPR immediately.
Pediatric Advanced Life Support (PALS) – AHA Guidelines
PALS is an advanced resuscitation strategy for managing critically ill or injured children, focusing on systematic assessment, airway stabilization, ventilation, circulation, and medication administration.
Step 1: Systematic Approach
✔ Evaluate: ABCDE assessment (Airway, Breathing, Circulation, Disability, Exposure).
✔ Intervene: Provide appropriate life support measures.
✔ Reassess: Monitor response and adjust treatment accordingly.
Step 2: Recognition of Respiratory or Circulatory Failure
✔ Early signs of respiratory failure:
- Increased work of breathing (Retractions, Grunting, Nasal Flaring).
- Cyanosis, Abnormal breath sounds (Stridor, Wheezing).
✔ Early signs of circulatory failure:
- Tachycardia, Weak pulses.
- Hypotension (Late sign in pediatrics).
Step 3: Cardiac Arrest Management – Pediatric Cardiac Arrest Algorithm
✔ Confirm pulselessness and start CPR immediately.
✔ Attach ECG monitor and identify rhythm.
1. Shockable Rhythms (Ventricular Fibrillation/Pulseless Ventricular Tachycardia)
- Defibrillate (First dose: 2-4 J/kg; Subsequent doses: 4-10 J/kg).
- Epinephrine: 0.01 mg/kg IV/IO (Every 3-5 minutes).
- Amiodarone (5 mg/kg IV) or Lidocaine (1 mg/kg IV).
2. Non-Shockable Rhythms (Asystole/Pulseless Electrical Activity – PEA)
- Continue high-quality CPR.
- Give Epinephrine (0.01 mg/kg IV/IO every 3-5 minutes).
- Identify and treat reversible causes (H’s & T’s).
Step 4: Advanced Airway Management
✔ Bag-Mask Ventilation (BMV) first.
✔ Endotracheal Intubation (ETT) if BMV is ineffective.
✔ Confirm ETT placement using Capnography (End-Tidal CO₂).
✔ Post-intubation Ventilation Rate:
- 10 breaths per minute (Avoid hyperventilation).
Step 5: Fluid Resuscitation & Shock Management
✔ Types of Pediatric Shock:
- Hypovolemic shock (Blood loss, Dehydration).
- Distributive shock (Sepsis, Anaphylaxis).
- Cardiogenic shock (Heart failure, Arrhythmias).
✔ IV/IO Fluid Resuscitation:
- Bolus of 20 mL/kg (Isotonic crystalloid – Normal Saline, Lactated Ringer’s).
- Repeat as needed (Up to 60 mL/kg), unless cardiogenic shock is suspected.
✔ Vasoactive Drugs:
- Epinephrine or Dopamine – For cold shock (Low BP, Poor perfusion).
- Norepinephrine – For warm shock (Septic shock with vasodilation).
Step 6: Post-Resuscitation Care
✔ Monitor oxygen saturation (SpO₂) and blood pressure.
✔ Prevent hypothermia (Maintain temperature between 36.5-37.5°C).
✔ Correct metabolic abnormalities (Glucose, Electrolytes).
✔ Supportive care (IV Fluids, Inotropic support if needed).
Key Updates in AHA 2020-2025 PLS/PALS Guidelines
✅ Emphasis on Early Recognition and Prevention of Cardiac Arrest.
✅ Prioritization of High-Quality CPR and Early Defibrillation.
✅ Minimizing Interruptions During CPR.
✅ Capnography Use for Confirming Airway Placement.
✅ Focus on Fluid Resuscitation and Shock Management.
Key Takeaways
✔ PLS includes PBLS (Basic Life Support) and PALS (Advanced Life Support).
✔ Early CPR, airway management, and defibrillation improve survival rates.
✔ High-quality chest compressions and rescue breaths are essential.
✔ Fluid resuscitation and medications play a critical role in shock management.
✔ Post-resuscitation care ensures better neurological outcomes.
Pediatric Advanced Life Support (PALS) – AHA Guidelines (2020-2025) in Full Detail
Introduction to PALS
Pediatric Advanced Life Support (PALS) is a systematic approach for managing critically ill or injured children. It is designed to improve survival rates in pediatric emergencies by following evidence-based protocols for assessment, resuscitation, and post-resuscitation care.
The American Heart Association (AHA) updates these guidelines regularly to ensure effective and timely interventions for children experiencing respiratory failure, shock, or cardiac arrest.
PALS Systematic Approach
PALS follows a structured assessment and intervention strategy, which includes:
- Initial Rapid Assessment (Evaluate, Identify, and Intervene).
- Pediatric Primary Assessment (ABCDE Approach).
- Pediatric Secondary Assessment (Focused History & Physical Examination).
- Pediatric Cardiac Arrest Algorithm (For Pulseless Arrest).
- Management of Respiratory Failure & Shock.
1. Initial Rapid Assessment
Before starting any intervention, quickly assess the child’s condition:
✔ Consciousness (Responsive or Unresponsive?).
✔ Breathing (Normal, Labored, or Absent?).
✔ Circulation (Pulse present or absent?).
✔ Skin Color (Pale, Cyanotic, or Normal?).
2. Pediatric Primary Assessment (ABCDE Approach)
A structured approach to assess and stabilize critically ill children.
A – Airway
✔ Assess if the airway is open, partially blocked, or completely obstructed.
✔ If airway is compromised → Open using head-tilt/chin-lift or jaw-thrust.
✔ Consider advanced airway (Endotracheal tube, LMA) if needed.
B – Breathing
✔ Observe chest rise, breathing rate, and effort.
✔ Check for abnormal breath sounds (Stridor, Wheezing, Crackles).
✔ Use pulse oximetry (SpO₂ >94% is the goal).
✔ If inadequate breathing → Provide oxygen or assist with bag-mask ventilation (BMV).
C – Circulation
✔ Check central pulse (Carotid, Femoral, or Brachial).
✔ Assess skin color, capillary refill time (<2 seconds is normal).
✔ Monitor Blood Pressure (Hypotension is a late sign of shock).
✔ Initiate IV/IO access and fluid resuscitation if needed.
D – Disability (Neurological Status)
✔ Assess AVPU Scale:
- A – Alert.
- V – Responds to verbal stimuli.
- P – Responds to pain.
- U – Unresponsive.
✔ Check pupil response to light.
✔ Monitor blood glucose (Correct if <60 mg/dL).
E – Exposure
✔ Check for signs of trauma, burns, infection (Rashes, Petechiae).
✔ Maintain normal body temperature (Avoid hypothermia).
3. Pediatric Secondary Assessment
SAMPLE History:
✔ S – Signs & Symptoms.
✔ A – Allergies.
✔ M – Medications.
✔ P – Past medical history.
✔ L – Last meal.
✔ E – Events leading to the illness/injury.
Focused Physical Examination:
✔ Head-to-toe assessment based on history and clinical findings.
✔ Identify and manage life-threatening conditions immediately.
4. Pediatric Cardiac Arrest Algorithm (PALS CPR Guidelines)
Step 1: Recognition of Cardiac Arrest
✔ Check unresponsiveness and no normal breathing.
✔ Check for a pulse (≤10 seconds).
If no pulse or HR <60 bpm with poor perfusion → Start CPR immediately.
Step 2: Start High-Quality CPR
✔ Compression-to-Ventilation Ratio:
- Single Rescuer: 30:2 (30 compressions, 2 breaths).
- Two Rescuers: 15:2 (15 compressions, 2 breaths).
✔ Compression Rate: 100-120 compressions per minute.
✔ Compression Depth:
- Infants: 1.5 inches (4 cm).
- Children: 2 inches (5 cm).
✔ Allow full chest recoil between compressions.
✔ Avoid excessive ventilation (1 breath every 6 seconds if intubated).
Step 3: Attach AED/Defibrillator and Assess Rhythm
✔ Shockable Rhythms: Ventricular Fibrillation (VF) or Pulseless Ventricular Tachycardia (VT).
✔ Non-Shockable Rhythms: Asystole or Pulseless Electrical Activity (PEA).
Step 4A: If Shockable (VF/Pulseless VT) – Defibrillation
✔ Give First Shock: 2-4 J/kg.
✔ Give Second Shock: 4-10 J/kg.
✔ Resume CPR immediately after shock.
✔ Give Epinephrine (0.01 mg/kg IV/IO every 3-5 min).
✔ Consider Antiarrhythmics:
- Amiodarone (5 mg/kg IV) or
- Lidocaine (1 mg/kg IV).
Step 4B: If Non-Shockable (Asystole/PEA)
✔ Continue High-Quality CPR.
✔ Give Epinephrine (0.01 mg/kg IV/IO every 3-5 min).
✔ Treat Reversible Causes (H’s & T’s).
Step 5: Identify and Treat Reversible Causes (H’s & T’s)
H’s (Common Causes of Pediatric Arrest)
✔ Hypoxia – Ensure adequate oxygenation.
✔ Hypovolemia – Give IV fluids.
✔ Hypoglycemia – Give dextrose.
✔ Hyper/Hypokalemia – Correct electrolyte imbalance.
✔ Hypothermia – Rewarm the child.
T’s (Reversible Conditions)
✔ Tension Pneumothorax – Needle decompression.
✔ Tamponade (Cardiac) – Pericardiocentesis.
✔ Toxins/Poisoning – Give antidotes.
✔ Thrombosis (Pulmonary or Coronary) – Thrombolysis.
5. Management of Shock in PALS
✔ Hypovolemic Shock (Blood Loss, Dehydration)
- 20 mL/kg IV bolus of Normal Saline or Lactated Ringer’s.
- Repeat up to 60 mL/kg if needed.
✔ Distributive Shock (Sepsis, Anaphylaxis)
- Fluids + Epinephrine for Anaphylaxis.
- Fluids + Vasopressors (Dopamine, Norepinephrine) for Septic Shock.
✔ Cardiogenic Shock (Heart Failure)
- Lower volume boluses (5-10 mL/kg).
- Consider inotropes (Dobutamine, Milrinone).
✔ Obstructive Shock (Tamponade, Tension Pneumothorax, PE)
- Needle decompression or pericardiocentesis.
6. Post-Resuscitation Care
✔ Maintain Oxygenation (SpO₂ 94-99%).
✔ Avoid Hyperventilation (Keep CO₂ between 35-45 mmHg).
✔ Monitor Hemodynamics (HR, BP, Perfusion).
✔ Prevent Hypoglycemia (Maintain glucose >60 mg/dL).
✔ Monitor for Seizures and Brain Injury.
Key Updates in AHA 2020-2025 PALS Guidelines
✅ Emphasis on Early Recognition and Prevention of Cardiac Arrest.
✅ Prioritization of High-Quality CPR and Early Defibrillation.
✅ Minimizing Interruptions During CPR.
✅ Use of Capnography to Confirm Airway Placement.
✅ Updated Dosing for Epinephrine & Antiarrhythmics.
Key Takeaways
✔ Early CPR and defibrillation significantly improve survival in pediatric arrest.
✔ High-quality chest compressions and rescue breaths are essential.
✔ Reversible causes (H’s & T’s) must be treated promptly.
✔ Post-resuscitation care prevents further deterioration and brain injury.