ENGLISH-NEW MIDWIFERY GNM TY UNIT 11 High Risk and Sick Newborn
Unit: 11 High Risk and Sick Newborn:

Assessment Of Newborn Baby:
Immediate assessment of the newborn after birth is crucial to assess their overall health, well-being and development. Here, some aspects of newborn assessment are given:
1) General Appearance (General Appearance) :

Color:
- Assess the child’s skin color, most children are pink or red. If there is cyanosis (bluish discoloration), it indicates breathing difficulties.
Posture:
- Note the baby’s muscle tone. A healthy newborn baby has slightly flexed hands and slightly arched feet along the spine.
Activity:
- Observe spontaneous movements, involving the sucking reflex and the grasping reflex.
2) Vital Sign :

Heart Rate:
- Normal range is 120-160/minute.
Respiratory Rate:
- A normal respiratory rate is 30-60 breaths.
Temperature:
- Normal temperature is 36.5-37.5°C (97.7-99.5°F).
3) Head And Face :

Fontanels:
- Palpat the anterior fontanelle (soft spot) and posterior fontanelle of the newborn. To assess proper closure of the fontanelles.
Eyes:
- Check the eyes for their cementum. Assess for red reflex (indicative of normal eye structure) and response to light.
Nose:
- Assess the patency of the nose to ensure that breathing is appropriate.
4) Mouth And Neck :

Oral mucosa:
- Assess the oral mucosa for cleft palate, oral thrush, and any lesions.
Neck:
- Any lesions in the neck Assess for mass-like structure or abnormality.
5) Chest And Lungs :

Breathing Sound:
- Listen to the child’s breathing sound properly.
Chest Movement:
- Properly assess whether the child’s chest rises and falls symmetrically with breathing.
6) Heart And Abdomen :

Heart Sound:
- Properly auscultate the heart sound to assess for any murmur-type abnormal sounds and abnormalities.
Abdomen:
- Palpate the abdomen and auscultate the bowel sounds to assess whether the child has any mass-like structures in the abdomen.
7) Genital area and anus:

Genital Area:
- Assess whether the anatomical structure of the genital area of the child, i.e. male (presence of testes in male child) and female (labial structure in female child), is proper or not.
Anus:
- Patency assessment of the anus and assess whether there is any abnormality.
Urine and stool:
- Urine is passed within 24 hours of birth and the first stool, called meconium, is greenish black in color, which occurs in the first 48 hours, three to four times a day for three to four days, and then transitional stools, which are greenish brown, are seen for three to four days.
8)Extremities:
Hands and Feet:
- Count the child’s fingers and toes. And assess symmetry or assess whether there are any abnormalities.
Movement:
- Assess whether the child has spontaneous movement and the range of motion of the hands and legs.
9) Skin And Umbelicus :

Skin:
- Assess the child to see if they have any birthmarks, lesions, or rashes on their skin.
Umbelics:
- Provide proper cord care to the child and assess for any signs and symptoms of infection and bleeding.
10) Behavioural Assessment:

State of Alertness:
- Properly assess the baby’s level of consciousness and the amount of response they provide to stimuli To do.
Crying:
- Properly assess whether the child is crying properly so that the child’s respiratory status can be properly assessed.
Additional Considerations (Additional) Considerations:
Documentation:
- Accurately record all findings on the Newborn Assessment Chart.
Parenteral Education:
- Provide education to parents about newborn care, including proper breastfeeding techniques, maintaining hygiene, and taking the child to a health care center immediately if any signs and symptoms of infection are seen in the child.
- Proper observation of the child after birth can identify any congenital abnormality or potential risk factor for any disease in the child early and take appropriate measures to prevent the child’s condition from becoming complicated.
Management Of The Newborn Wth Hyperbillirubinemia (Management Of The Newborn With Hyperbilirubinemia / Neonatal Jaundice) :

Definition:
- When yellow discoloration of the skin, sclera, and mucous membranes and body secretions is observed due to the accumulation of excessive bilirubin in body tissues, it is called “neonatal jaundice”/hyperbilirubinemia. Normal bilirubin in the blood is 0.1 to 0.8 mg/dl. Now when the level of bilirubin in the body is 5 mg/dl, it is called neonatal jaundice, also called icterus neonatorum or neonatal hyperbilirubinemia.

Incidence:
- Approximately 60% of full-term babies and 80% of preterm babies develop jaundice in the first week of life. Approximately 6% of term babies develop severe jaundice with bilirubin levels of 15 mg/dl or higher. happens.
Types Of Jaundice :

Jaundice is generally of two types, namely,
1) Physiological Jaundice,
2) Pathological Jaundice.
1) Physiological Jaundice
Characteristics:
- This jaundice mainly appears within 24 – 72 hours after birth.
- Maximum yellow discoloration is seen in full term babies by 4th – 5th day and in preterm babies by 6th – 7th day.
- It mostly disappears by 7th day in full term babies and by 14th day in pre-preterm babies. The bilirubin level in it does not exceed 12 – 15 mg/ dl.
- It mostly does not require treatment and gets relieved on its own.
Etiology:
- It is mostly seen due to excessive breakdown of RBC (red blood cells) due to short life span of red blood cells.
- Due to inadequate enzymatic action of the liver to convert bilirubin into soluble bilirubin due to hepatic immaturity.
- Due to reduced conversion of bilirubin by intestinal flora, the amount of bilirubin in the circulation increases.
Nursing Management:
- It does not require any specific treatment.
- Provide adequate amount of fluids to the baby.
- Carefully observe the premature baby.
- Advise the mother to provide adequate amount of breast feeding to her child.
- If there is evidence of excessive increase in bilirubin level, treat it with exchange transfusion.
- Use phenobarbitone and phototherapy to treat this jaundice.
- Provide proper daily routine or care to the child.
- Carefully observe the child if there are any signs of complications.
2) Pathological Jaundice
Definition:
- Pathological jaundice is seen in the mother within 24 hours of birth. And if it is a mature baby, it is usually seen for more than 1 week, while
if it is a pre-mature baby, mainly pathological jaundice is seen for up to 2 weeks. About 5% of pathological jaundice occurs in the first 24 hours due to hemolytic disease and intrauterine infection. - In this, bilirubin increases at a rate of 5mg/100 ml in 24 hours.
- Absolute bilirubin is more than 15 mg/ 100 ml (250 μ mol/ L).
Etiology (Etiology):
- Due to excessive hemolysis of red cells.
- Due to defective conjugation of bilirubin.
- Due to failure of excretion of conjugated bilirubin.
- Due to Rh incompatibility.
- Due to cephalohematoma.
- ABO incompatibility.
- Vitamin K therapy.
- Congenital spherocytosis.
- Due to glucose 6 phosphate dehydrogenase deficiency.
- Prematurity due to immature liver cells Due to reduced production of enzymes like glucuronyl transferase.
Types:
- Prolonged unconjugated hyperbilirubinemia
- It is mainly caused by hemolytic disease of the breast milk.
- Prolonged conjugated hyperbilirubinemia: It is mainly seen due to infection.
Sign And Symptoms:
- Yellow staining is seen on the face, trunk, palms and soles (bottom of the feet).
- Urine staining is seen on clothes.
- The color of the stool is clay, white or dark.
- The bilirubin level increases by 5 mg/dl/day.
- Then other features such as lethargy, drowsiness, poor sucking reflex, fever, infection, etc. are seen.
- When bilirubin develops above 15 mg/dl, kernicterus (a pathological condition of the brain due to unconjugated bilirubin) develops.
- Its features include vomiting, high-pitched crying, Convulsions, opisthotonus position, nystagmus, hyperpyrexia, and spasticity are seen.
Management:
The following methods are used to treat jaundice:
1) Phototherapy
2) Pharmacologic therapy
3) Exchange transfusion
Phototherapy:
- Phototherapy is best used in moderate cases when the bilirubin level rises above (12 mg%). Phototherapy is stopped when the serum bilirubin level is about 10 mg %. Once phototherapy is stopped, there may be a rebound increase in serum bilirubin. It is important to maintain adequate hydration of the newborn. Special blue lamps with an output of 420 to 470 nm wavelength are most effective in treatment.
- Phototherapy should be started as early as possible to allow maximum surface area to be exposed and ice to be applied.
Phototherapy causes insensible fluid loss in the newborn. Hydration is promoted by breastfeeding. Administer intravenous fluid therapy during phototherapy.
Phototherapy blanket protects the infant.
Phototherapy:
- Phototherapy is a non-invasive, effective, and inexpensive method of reducing unconjugated bilirubin. It uses light waves to convert unconjugated bilirubin into a water-soluble, non-toxic form through photooxidation, which is easily excreted from the blood. Phototherapy should be started when the bilirubin level reaches 15 mg/dl and in preterm babies when it is 5 mg/dl or more.
- The blue wavelength is 450-460 nm. The tube light and plexiglass are covered with a shield. The phototherapy unit is fixed on the crib or incubator. Fluorescent or halogen light can also be used.
Nursing Responsibility in Phototherapy:
- The baby should be completely exposed to the light source and the light should be kept at a distance of 45 cm.
- The child’s eyes and genital area should be properly covered.
- Advise the mother to provide frequent breast feeding to the child during phototherapy.
- Provide feeding through intravenous infusion or nasogastric tube if extra fluids are required
- The child’s position should be changed every two hours and the position should be changed in such a way that he gets maximum light.
- The child’s temperature, pulse, and respiration (TPR) should be checked every two hours.
- Continuously monitor the child for any side effects of phototherapy and get the serum bilirubin level checked at least every 12 hours.
- When, the serum bilirubin level Discontinue phototherapy when it reaches 10 mg/dl.
- Mostly, phototherapy should be continued for 2-3 days. Or,
- 6 hourly/day and,
- 2 hourly 3 times / day.
- Involve the mother in the baby’s care.
- Proper explanation, instruction and emotional support to the parents are important.
- Complications and side effects of phototherapy:
Immediate Problems:
- Dehydration, hypothermia, hyperthermia,
- Loose stool/green stool,
- Bronze baby syndrome (Bronze baby syndrome is a condition in which a child’s skin, mucous membranes, and urine develop a dark green-brown pigmentation after phototherapy.
- Skin rashes,
- hypocalcemia, etc. are seen.
Long-term problems:
- Disturbances occur in endocrine and sexual maturation. Damage to the retina.
- Getting skin cancer (rare condition).
Phenobarbital therapy:
- Phenobarbital therapy induces hepatic microsomal enzymes and increases bilirubin conjugation and excretion. A dose of 5.8 mg/kg every 24 hours. is used. It takes 3-7 days to become effective. However, as a prophylaxis, it can be used in In which the mother is provided with a rate of 90 mg/dl for two weeks before delivery.
Exchange Transfusion:
- Exchange transfusion is usually used to prevent kernicterus.
In which double volume exchange replaces up to 80% of red blood cells and helps reduce bilirubin levels by up to 50%. - Indication of Exchange Transfusion
- Despite phototherapy, the bilirubin level in the body is progressively increasing (more than 1mg/dl/hour).
- In cases where the neonate has anemia and congestive cardiac failure.
- If the serum bilirubin level of the newborn is more than 20 mg/dl.
- If the cord blood hemoglobin is less than 12 g/dl and the bilirubin level is more than 5 mg/dl.
Neonatal Hypoglycemia :
- A plasma glucose level of less than 30 mg/ dL (1.65 mmol/ L) in the first 24 hours of life after birth and less than 45 mg/ dL (2.5 mmol/ L) thereafter is called “Neonatal Hypoglycemia” It is said.
- Neonatal hypoglycemia is the most common metabolic problem in newborns. That is, if the blood sugar level of a newborn or neonate is low for a few days after the birth of the fetus, that condition is called neonatal hypoglycemia.
- Neonatal hypoglycemia is a metabolic disorder in which the blood glucose level of the neonate decreases below its normal level, then this condition is called neonatal hypoglycemia.
Normal Blood Glucose Level
- Normal levels in a one-day-old neonate are: 40-60 mg/dl.
- In neonates older than one day: 50-90 mg/ dl.
Etiology:
1) Maternal diabetes: Babies born to mothers with diabetes (especially if the diabetes is poorly controlled) are at increased risk of hypoglycemia in the neonate.
2) Prematurity: Premature infants often have an underdeveloped system for regulating blood sugar.
3) Intrauterine Growth Restriction (IUGR): Babies who are smaller than expected for their gestational age may have impaired glucose storage.
4)Birth asphyxia: A condition in which oxygen levels are low at the time of birth can affect the regulation of blood glucose levels.
5)Infection: Infection can affect the baby’s metabolism and increase the risk of hypoglycemia.
6) Hormonal deficiency: Issues with hormone production, such as adrenal insufficiency, can cause a condition of hypoglycemia.
7)Metabolic disorders: Sometimes, the condition of hypoglycemia can also arise due to inherited metabolic disorders.
8)Hyperinsulinemia: In some newborns, the production of insulin occurs in a higher amount, due to which the condition of hypoglycemia can arise.
Other causes:
Due to low supply of glucose,
Inadequate storage of glycogen,
Birth Due to defects and metabolic errors,
Glucose production is impaired,
Glucose utilization is increased due to hyperinsulinism,
Liver disease,
Some deficiencies during pregnancy.
Sign And Symptoms:
- Poor feeding,
- Lethargic look,
- Hypotonia,
- Bluish discoloration of skin (cyanosis),
- Apnea,
- Hyperthermia,
- Pallor,
- Neurological Damage,
- Grunting sound,
- Twitching,
- Nervousness,
- Seizures,
- Congestive heart failure,
- Hunger,
- Nausea,
- Vomiting
Diagnostic Evaluation:
- Serum and plasma glucose levels,
- Serum insulin,
- For metabolic disorders
- Screening,
- Urine test.
Management:
- Treat the condition of hypoglycemia as early as possible to prevent neurological damage.
- Advise the mother to provide early breast feeding to the newborn.
- Provide it properly if the newborn requires extra formula feeding.
- Continuously monitor the newborn’s blood glucose level.
- Properly evaluate the newborn for lethargy and poor muscle tone.
- Properly monitor the newborn for feeding problems.
- Provide continuous dextrose solution to the newborn if the blood sugar level of the newborn is continuously low and the newborn is not able to breastfeed.
- In rare situations when despite providing the above treatment If there is no improvement in the newborn’s condition, surgery to remove part of the pancreas may also be required, which may reduce insulin production.
Complications:
- Neurological damage,
- Heart failure (rare condition) Ma),
- Scissors (occasionally).
Hypothermia:

- Hypothermia is a condition in which the body temperature of newborns and infants is reduced below their normal physiological body temperature. It is usually reduced to 36.5 °C and 97.7 °F.
- This condition is usually caused by an imbalance between heat production and heat loss. This is usually caused by environmental factors, inadequate thermal production, and physiological issues. This condition of hypothermia can cause serious complications in the body, such as metabolic disturbances, impaired organ functions, and increased susceptibility to infection.
- Hypothermia is a condition in which the body temperature, i.e. the core or internal body temperature, falls below 95°F and 35°C.

Modes of Heat Loss in Newborns:
1) Evaporation: Evaporation of amniotic fluid from the skin surface of the baby after birth.
2) Conduction: Due to contact of the baby with any cold object, cloth and tray after birth.
3) Convection: A condition in which the cold air coming from open windows and fans around the baby is replaced by warm air. Due to.
4) Radiation: When the environment around a newborn after birth is colder than its body surface, the heat in its body passes through radiation to the surrounding environment.
Temperature Range:
- Normal Axillary Temperature: 36.5-37.4°C.
- Cold Stress: 36.0°C-36.4°C.
- Moderate Hypothermia: 32.0°C – 35.9°C.
- Severe Hypothermia: Temperature less than 32.°C.
Etiology:
1) Situation causes excessive heat loss:
- Cold Environment,
- Wet and Naked Baby,
- Cold Linen,
- During Transport,
- Infusion,
- Blood Sampling.
Poor Ability to Conserve Heat:
- Low Birth Weight ( LBW ),
- Intra Uterine Growth Retardation ( IUGR ).
Poor Metabolic Heat Production:
- Due to brown fat deficiency,
- CNS damage,
- Hypoxia,
- Hypoglycemia,
- Sepsis.
Sign And Symptoms:
Peripheral vasoconstriction:
- Cold extremities,
- Decreased peripheral perfusion,
- Acrocyanosis,
Increases metabolism:
- Hypoglycemia,
- Hypoxia,
- Metabolic acidosis,
Increases pulmonary artery Pressure:
- Distress,
- Tachypnea.
CNS Depression:
- Bradycardia,
- Lethargy,
- Poor feeding,
- Apnea.
Chronic signs:
- Weight loss,
- Poor weight gain.
Management:
Mild hypothermia:
- After birth, cover the neonate properly, especially the head, chest and feet.
- Keep the neonate properly warmed using any of the following methods, such as,
skin to skin contact,
warm room and bed,
radiant heater and incubator. - Monitor the temperature every half hour. Then monitor it every 1 hour for the next 4 hours until it reaches 36.5 °C, then Monitor temperature every 2 hours for 12 hours.
Moderate Hypothermia:
- Keep the room properly warm to prevent the newborn from hypothermia.
- Keep the child’s coat or bed properly warm.
- Use an incubator to maintain normal temperature in newborns.
- Use a radiant warmer properly.
- Continuously warm the newborn until its temperature reaches the normal range.
- Monitor the temperature every 15 – 30 minutes.
- Management of severe hypothermia (less than 32°C):
- Warm the room properly with a room heater or a 200 watt bulb.
- Use a properly air heated incubator (air temperature 35 – 36 ° C).
- Keep monitoring the neonate’s heart rate, temperature and glucose level properly.
- Take proper measures to minimize heat loss.
- I.V. Start 10% dextrose 60-80 ml/ kg/ day.
- Provide proper oxygen to the neonate.
- If the neonate is term, give him 1 mg of vitamin K injection and if he is preterm, give him 0.5 mg of vitamin K injection.
Prevention:
- Maintain the temperature of the delivery room properly, such as 28-32°c.
- Clean and dry the baby immediately after the birth of the newborn and then cover the baby properly with a warm towel.
- Properly cover the baby’s head and immediately assess whether his head is properly clean and dry after the birth.
- Place the baby in his Keep the baby close to the mother so that the baby gets warmth.
- Start breastfeeding the child within 30 minutes of the baby’s birth.
- If the baby is of low birth weight i.e. weighs less than 2500 gm, then provide him/her with proper Kangaroo Mother Care (KMC) due to which the temperature of the infant is maintained and the best feeding is observed due to which the bonding of the mother and the infant is improved.
Neonatal Convulsion:
- Neonatal convulsion is a life-threatening emergency that occurs in newborns due to cerebral and biochemical abnormalities. This condition is more common in preterm babies and low birth weight (LBW) babies.
Definition:
- Neonatal convulsions are paroxysmal behaviors that are caused by hypersynchronous discharges by groups of neurons. Neonatal convulsions occur between the time a child is born and the time they are 28 days old. They are usually caused by abnormal electrical activity in the brain. Due to which involuntary movements of the body occur, changes in muscle tone occur, and alterations are seen in the level of consciousness.
- This convulsive condition is seen due to various reasons such as metabolic imbalance, brain injury, infection, and congenital abnormalities.
Etiology:
Causes of Convulsions:
1) Traumatic:
Hypoxic ischemic injury,
Intracranial injury.
2) Biochemical:
Hypoglycemia,
Kernicterus,
Hypocalcemia,
Hypercalcemia,
Hyponatremia,
Hypomagnesemia,
Pyridoxine Dependence
3)Infectious:
High fever,
Meningitis,
TORCH
(T: Toxoplasmosis,
O: Other (includes various infections such as syphilis, varicella-zoster virus and parvovirus B19).
R: Rubella
C: Cytomegalovirus (CMV)
H: Herpes simplex virus (HSV) infection.
Tetanus.
4) Iatrogenic:
Respiratory stimulant,
Analeptic drugs,
Drug toxicity,
Theophylline.
5) Others:
Cerebral malformation
Classification Of Convulsion:
Convulsion is mainly classified into two types.
1) Generalized seizures
2) Partial and focal onset seizures.
1) Generalized Seizures
Generalized seizures are further divided into six types.
1) Tonic-clonic seizures.
2) Absent seizures.
3) Myoclonic seizures.
4) Tonic seizures.
5) Atonic seizures.
6) Clonic seizures.
2) Partial and focal onset seizures.
There are two more types of partial and focal onset seizures.
1) Simple focal seizures.
2) Complex focal seizures.
1) General Seizers
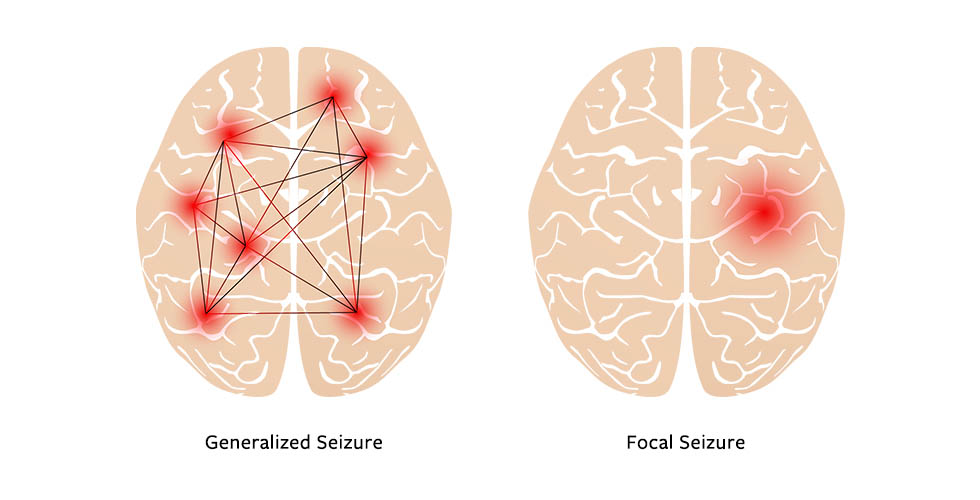
- There are six more types of generalized seizures.
- In generalized seizures, both the hemispheres of the brain, i.e. the right and left hemispheres, are involved. This means that uncontrolled electrical discharges occur in both the hemispheres of the brain. In this type of seizure, the neonate becomes unconscious. These seizures can last from a few seconds to a few minutes.
1) Tonic-clonic seizures.
- Tonic-clonic seizures are also called grandmal seizures. In these seizures, the neonate’s consciousness is completely lost. And the neonate also falls to the ground.
- In the tonic stage, the patient’s muscles stiffen and muscle tone increases.
- In the clonic phase, the patient’s muscle tone is lost.
2) Absence seizure.
- Absence seizures are also called petitmal seizures. This type of seizure is mainly seen in children.
- These seizures are seen for only a few seconds. In these seizures, the patient experiences episodes lasting only a few seconds and the patient does not even realize that he is having any kind of issue.
3) Myoclonic seizures.
- Myoclonic seizures involve muscles and there is an excessive jerking movement of the body. Therefore, excessive jerking movement is seen in myoclonic seizures.
4) Tonic seizures.
- In this seizure, muscle tone increases suddenly and the body becomes stiff and muscle tone increases greatly.
5) Atonic seizure.
- In this seizure, muscle tone is lost, so a drop attack is seen in this, i.e. the patient falls down because in this seizure, the patient’s muscle tone suddenly stops. In this seizure, the patient suddenly regains consciousness after a drop attack. In this seizure, the patient is at high risk of head injury.
6) Clonic seizure.
- In this seizure, the neonate’s muscle tone is suddenly lost. In this, the neonate is seen unconscious and its muscle tone is also lost. In this seizure, jerking moment of the limb and jerking moment of the extremities are seen.
2) Partial and focal onset seizures.
- This seizure is also called partial focal seizure and partial seizure. This seizure involves the involvement of one side of the hemisphere.
- Therefore, whatever body activity is regulated by the involved hemisphere is affected.
There are two more types of partial and focal onset seizures.
1) Simple focal Caesar.
- In this type of seizure, the neonate seems conscious but experiences unusual feelings and sensations.
- In this, the child may be very happy, very angry, or the neonate may suddenly become sad or have feelings of nausea suddenly and without any reason.
- In this seizure, only one hemisphere is involved, so the person may feel things that are not there in reality.
2) Complex focal seizure.
- In this seizure, the patient’s level of consciousness is altered or lost.
- In this seizure, the person experiences a dream-like experience. In this type of seizure, the person does not even remember the action he or she is doing. It is called complex focal seizure.
Sign And Symptoms:
- Temporary confusion.
- Uncontrolled jerking movements of the arms and legs.
- Loss of consciousness.
- Loss of awareness.
- Temporary confusion.
- Numbness in parts of the body.
- Loss of memory.
- Visual changes.
- Dizziness.
- Tingling in the chest Sensation.
Diagnostic Evaluation:
- History collection,
- Physical examination,
- Blood test.
- Lumbar puncture .
- Electroencephalogram.
- Computerized tomography (CT scan).
- Magnetic resonance imaging (MRI).
- Positron emission tomography (PET test).
- Single photo emission computerized tomography ( SPECT ).
- Neuropsychological test.
- Brain mapping.
Management (Management ):
- Properly maintain a safe environment to prevent injury to the neonate.
- Keep the side rails up to prevent injury to the neonate.
- Provide phenobarbitone 10 mg/ kg body weight slowly over 3-5 minutes to control convulsions.
- Do not put anything in the neonate’s mouth.
- If the neonate is wearing anything around the neck, loosen it.
- Do not provide restraint to the neonate as this may not prevent injury.
- Provide a small pillow under the neonate’s head.
- If the neonate is vomiting, take proper care to prevent aspiration.
- Keep suction readily available. Proper suctioning through the mouth and nose and keeping the child’s airway patent so that he can breathe properly.
- Advise the child to take proper bed rest.
- Provide the child with intravenous (IV) fluids.
- Provide oxygen therapy to the neonate.
- Provide the neonate with proper care and a comfortable environment.
- Advise the neonate to take proper medication.
Small for Date/Intrauterine Growth Retardation (IUGR)/Intrauterine Growth Restriction (IUGR) Dysmaturity/Chronic Placental Insufficiency:
Definition (Definition):
- A baby whose birth weight is less than the tenth percentile (10%) of its average gestational age is called intrauterine growth restriction/retardation (IUGR). Growth restriction/retardation can occur in preterm, term, or post-term babies.

Incidence of IUGR:
- Dysmaturity accounts for about 1/3 of low birth weight children.
- Its overall incidence in developed countries is 2-8%.
In term babies – 5%,
In post-term babies – 15%.
Types: Small fetuses are divided into the following two types based on clinical evaluation and ultrasound examination.
1) The fetus is small and healthy but its birth weight is less than the tenth percentile (10%) of its gestational age.
2) Growth restriction is due to pathological process hence it is again divided into two parts as,
(a) Symmetrical type I (20%),
(b) Asymmetrical type II (80%).
(a) Symmetrical type I (20%):
1. Uniformly small in size.
2. Ponderal index (birth weight/crown-hill length): normal.
3. HC(head circumference): AC(abdominal circumference) and femur length (FL): AC(abdominal circumference) ratio are normal.
4. Etiology: Due to genetic disease or infection.
5. Total cell number: low, end cell size: normal.
6. Neonatal- Complicated with poor prognosis.
(b) Asymmetrical type II( 80%):
1.Head is larger than abdomen.
2.Ponderal index (Birth weight/Crown Hill length): Low.
3.HC(Head circumference): AC(Abdominal circumference) and Femur length (FL): AC(Abdominal circumference) ratio is elevated.
4.Etiology: Due to chronic placental insufficiency.
5.Total cell number: Normal, smaller size.
6.Neonatal- Mostly uncomplicated with good prognosis.
Etiology (Etiology):
Fetal growth retardation is generally divided into four groups, namely,
1.Maternal,
2.Fetal,
3.Placental,
4.Unknown.
1.Maternal:
Constitutional: Small women due to maternal genetic and racial factors,
Maternal nutrition before and during pregnancy.
Poor weight gain.
Cyanotic heart disease due to low blood oxygen levels.
Inadequate substrate Level
Ex. Malabsorption syndrome.
Toxins such as alcohol, smoking, chronic renal failure, chronic urinary tract infection etc.
2.Fetal:
In this, maternal blood contains sufficient substrate and it crosses the placenta but its utilization by the fetus is not done due to the following:
1.Congenital anomalies: such as cardiovascular, renal and other factors.
2.Chromosomal abnormalities: such as trisomy 21, trisomy 18 (Edward syndrome) trisomy 16, trisomy 13 and Turner syndrome.
3.Torch agents accelerate the metabolic process of the fetus Happen.
4. Due to multiple pregnancy.
3. Placental: Due to poor uterine blood flow. Abruptio, circumvallate placenta, infraction
4.Unknown: Unknown is seen in about 40% of cases.
Diagnostic Evaluation:
- History collection,
- Physical Examination,
- Clinical: This involves palpation of fundal height, liker volume and screening of fetal mass. Symphysis fundal height is correlated with gestational age after 24 weeks. If it is 4 cm or less, it indicates growth restriction. If there is no maternal weight gain, abdominal girth does not increase.
- Biophysical: HC, AC ratio, femur length, amniotic fluid, anatomical survey, ultrasound Doppler parameters, etc.
- Biochemical markers: MSAFP and HCG levels are elevated in the second trimester.
Physical features at birth:
- Birth weight deficit is approximately 600 gm less than the percentile standard.
- Length is not affected.
- Asymmetrical head circumference More than the body.
- Dry and wrinkled skin, scaphoid abdomen, meconium stained umbilical cord give the baby a “scratchy” appearance. The cartilaginous ridges of the pinnae and plantar creases in the ears are well developed.
- The baby is alert, active, and cries normally, and keeps his eyes open.
- Reflexes are normal.
Management :
- Nursing management of the patient with intrauterine growth restriction usually occurs during the antenatal period, if possible.
- Whenever a fetus is suspected to be small for gestational age, a careful search is made by sonography to determine the presence of growth retardation.
- When growth retardation is present, possible causes should be found out.
- If growth retardation is present, the possible cause is identified.
- If the fetus is symmetrically growth retarded, a meticulous search should be made to identify fetal anomalies.
- To prevent unnecessary caesarean section in malformed babies, blood sampling and karyotyping of the fetus should be done.
- Adequate rest should be given to the mother in the pre-birth period, i.e. (in left lateral position).
- Then there should be a 2 hour break after lunch and a rest period of 8 hours during night time.
- Provide the mother with a balanced diet in adequate amount to correct the condition of malnutrition. For example, 300 extra calories should be provided.
- In selected cases, low dose aspirin (50 mg) daily is helpful.
- The patient should be properly hospitalized.
- The condition of IUGR should be properly confirmed.
- If the patient has any congenital malformation and genetic disorder, identify it.
- If there is any specific cause of intrauterine growth retardation, treat it first.
- Check the fetal heart sound and the mother’s condition regularly.
- Check the mother’s vital signs properly.
- Provide proper support and reassurance to the mother.
- If the pregnancy is more than 38 weeks, termination is done.
- If the pregnancy is less than 38 weeks, the degree of IUGR should be checked.
- If there is a condition of mild amount of retardation, advise the mother to take adequate amount of rest and provide adequate amount of supplementary therapy.
- Assessing the lung maturation of the fetus in severe cases.
- If lung maturity is achieved. It is assessed by L.S ratio (lecithin-sphingomyelin ratio), which is an indicator of lung maturity if the value of L.S ratio is more than 2.0-2.5. In such cases, delivery is done where the growth of the fetus cannot be improved by induction at 32-34 weeks and then vaginal delivery/cesarean delivery is done.
- If lung maturity is not achieved:
- Evaluation of lung maturity is done.
- Assessing the level of phosphatidyl glycerol.
- If the lungs are not mature, dexamethasone therapy is given and termination is done.
- Delivery can be done by:
- Lower rupture of membranes followed by oxytocin
- In cases of more than 34 weeks of pregnancy, the cervix is favorable and the head is deep in the pelvis. If the cervix is favorable, prostaglandin gel (PGE2) can be used.
- In unfavorable conditions, a cesarean section is performed.
- The following precautions are taken during vaginal delivery:
- Delivery should be done in a well-equipped hospital where intensive intranatal monitoring is possible and it has the facility of an intensive neonatal care unit.
- Otherwise, the child should be transferred to a well-equipped hospital.
- Precautions should be taken during pregnancy.
- The patient should be placed in the left lateral position.
- If there is even slight evidence of hypoxia (meconium staining and abnormal CTG), then immediate measures should be taken by cesarean section in the first stage and forceps in the second stage.
- A pediatrician should also be available for the care of the baby.
- The baby should be provided with care in the intensive neonatal care unit.
- If there is a condition of hypoglycemia, special precautions should be taken for it.
- Provide the mother with proper work and a comfortable environment.
Birth Asphyxia or Asphyxia Neonatrum (Birth Asphyxia):

- Asphyxia neonatorum is the failure to establish satisfactory pulmonary respiration at the time of birth, meaning the absence of a pulse. Clinically, it is also defined as the failure to initiate and maintain spontaneous respiration within one minute of birth.
- Which leads to varying degrees of hypoxic and ischemic injury to body tissues and organs. It is also accompanied by hypoventilation, anaerobic, glycolysis, and lactic acidosis.
- Its characteristics include progressive hypoxia, hypercapnia, hypoperfusion, and metabolic acidosis. It results in hypoxic ischemic encephalopathy and neuromotor sequelae (long-term neurological and motor impairment due to brain injury or dysfunction) with multi-organ dysfunction.
Etiology:
- Obstruction of the air passages due to inhaled mucus or amniotic fluid.
- Lungs expansion failure due to low alveolar surfactant.
- Morphine, pethidine and anesthetic agents given to the mother during the prenatal and intranatal periods can cause asphyxia due to depression of the baby’s respiratory center.
- In the placental circulation Intrauterine hypoxia is the main cause of neonatal hypoxia due to disturbances such as anatomical changes in the placenta, premature separation of the placenta, post-dated pregnancy, retroplacental hemorrhage, pregnancy-induced hypertension, and cord compression, etc.
- Due to birth trauma. Difficult forceps delivery, prolonged labor, contracted pelvis, breech delivery, oblique lie, occipito posterior position etc.
- Due to weak respiratory muscles, immature respiratory center, and poor lung expansion in premature babies.
- Due to congenital heart disease, blood loss, and circulatory collapse in shock.
Classification:
It is divided into two parts according to the intensity of clinical features such as:
1) Asphyxia Livida / Stage of Cyanosis / Blue Asphyxia
This is the primary condition of respiratory failure in which the APGAR SCORE may be 4-6.
2) Asphyxia Pallida / Stage of Shock / White Asphyxia
This is a condition of respiratory and vasomotor failure in which the APGAR SCORE can be 0 – 3.
Sign And Symptoms:
- The clinical features of neonatal asphyxia depend on the degree of depression, duration of low oxygen, plasma CO2 level and cause.
- It includes decreased muscle tone.
Respiratory distress.
Breathing difficulties.
Irregular breathing.
Cyanosis (bluish discoloration of the skin, especially around the lips and face.)
Abnormal heart rate (such as bradycardia and tachycardia).
Reduced alertness and responsiveness.
Seizures.
Feeding difficulties.
Management:
The management of asphyxia neonatorum is divided into two parts, namely,
1) Prophylactic management,
2) Definitive management
Prophylactic management:
In the antenatal period, high-risk To identify during antenatal care.
In high-risk pregnancies, early detection of early fetal growth is required. Due to which, if there is a condition of fetal distress, early identification can be done.
Use electronic fetal monitoring during the intrapartum period and perform scalp blood pH assessment as needed.
Use anesthetic agents and anti-depressant medication properly during labor.
Definitive Management
- Assess the baby’s APGAR score and provide proper treatment accordingly.
- If the APGAR score is between 7 – 10, it is considered normal.
- If there is mucus in the baby’s oropharynx and laryngopharynx, suction and clear it properly.
- Provide supplementary oxygen if necessary.
- Then reassess the neonate’s condition after five minutes. If normal, transfer the infant to the nursery.
- If the baby’s APGAR score is between 4-6,
- Immediately suction the baby’s mucus from the oropharynx and nasopharynx using a mucus sucker or suction operators.
- Then place the baby on a flat surface and in a head-down position, turning his face to one side so that the mucus drains through gravitational force. Drainage may be done.
- At the same time, administer oxygen to the baby through a bag and mask at a pressure range of 25-30 cm H2O.
- Provide intermittent positive pressure ventilation to the infant if necessary.
- Provide stimulation to the infant on the back and soles.
- In the majority of cases, the baby can take independent respiration using these simple measures. is.
- Then assess the baby’s APGAR score at five minutes and if satisfactory, return the infant to the mother.
- If the above measures fail,
- Do oral suctioning and start endotracheal intubation.
- Connect the endotracheal tube to the resuscitation bag, through which O2 can be administered at a rate of 6-8 liters/minute.
- Maintain intermittent positive pressure airway (IPPV) ventilation at 30 – 40/min.
- Perform central external cardiac massage if heart rate is less than 60/min.
- If the mother has a history of using central depressant drugs such as pethidine or morphine within 3 hours of delivery. Appropriate antidote, e.g. Naloxone hydrochloride 60 mg/kg IM (single dose) or 10 µg/kg IV is given and may need to be repeated.
- To combat acidosis, 8.4% NaHCO3 (sodium bicarbonate) 1 mEq/kg in 5% dextrose (diluted 1:1) is given very slowly (at a rate of 1 ml/min) via the umbilical or peripheral vein in the minimum dose.
- If the child’s APGAR score is below 4, immediately perform tracheal intubation and start intermittent positive pressure ventilation.
- If the mother has a history of using a central depressant drug such as pethidine or morphine within 3 hours after delivery. Appropriate antidote, e.g. Naloxone hydrochloride 10 µg/ kg IV is given to neonates.
- It is repeated every 2 – 3 minutes.
Complications:
- Respiratory distress syndrome,
- Cardiac Failure,
- Respiratory Infection,
- Septicemia,
- Disseminated Intravascular Coagulation (DIC),
- Hyperbilirubinemia,
- Cerebral Depression,
- Failure to Thrive,
- Mental Retardation,
- Cerebral Palsy,
- Convulsive Disorder.
Prevention:
- To prevent asphyxia, detect risk factors and provide intensive internal care.
- Manage risk factors through necessary facilities or referral.
- To detect fetal hypoxia, perform intranatal assessment of fetal condition. Manage distress.
- Prevent birth injuries through efficient management of malpresentation, contracted pelvis, instrumental delivery.
- Carefully use anesthetic and depressant agents during labor.
Prognosis:
The prognosis of neonatal hypoxia depends on the baby’s maturity, duration and intensity of hypoxia, acidosis, and competent management.
Respiratory Distress Syndrome (RDS)
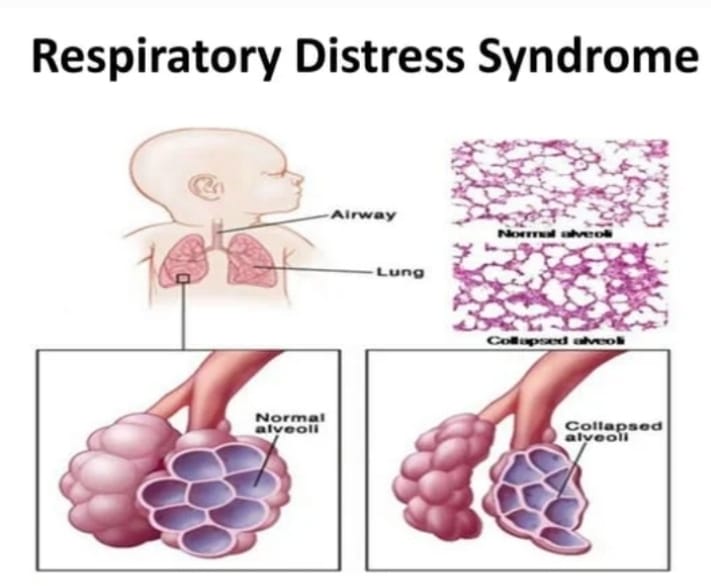
Definition:
- Respiratory distress syndrome is a lung disease seen in newborns/neonates. Which is mainly seen in premature babies, neonates whose mothers are diabetic, children whose birth is by cesarean section or children who have breech delivery.
- Respiratory distress syndrome (RDS) is usually seen in the neonate’s body due to the deficiency of surfactant {SURFACTANT (an enzyme that works to reduce the surface tension of the alveoli.)}. The main reason for this is that when the body of a newborn child cannot produce surfactant in an adequate amount and due to this surfactant not being in an adequate amount, the child The lungs cannot function properly due to which gaseous exchange does not take place properly, due to which the amount of oxygen in the child’s body is reduced, due to which the conditions of hypoxia and acidosis arise.

Surfectant (Surfactant) :
Introduction
Surfactant is a type of lipoprotein substance whose production is carried out by combining phospholipids. The main ones are lecithin and sphingomyelin. And their ratio is usually (lecithin (L)): sphingomyelin (S)) 2: 1. Thus, lecithin and sphingomyelin together produce surfactant.
Function
Surfactant works to reduce the surface tension inside the alveoli, its functional unit in the lungs, due to which the lungs and alveoli do not collapse and gaseous exchange continues to take place properly inside them.
Function
Surfactant works to reduce the surface tension inside the alveoli, its functional unit located inside the lungs, in the body, due to which the lungs and alveoli do not collapse and gaseous exchange continues to take place properly within them.
Production
Surfactant starts to be produced at 24 weeks of gestation and its maximum production occurs during the 37th week of gestation. The hormone cortisol helps in the production of surfactant. In newborns, surfactant is produced by alveolar type 2 epithelial cells of the lungs. And its storage occurs in the laminar bodies (LBS) of the alveolar cells. The maximum activity of surfactant to mature the lungs occurs at 34 weeks of gestation.
A child whose birth occurs before 37 weeks of gestation is called a preterm baby and due to the lack of adequate amount of surfactant production, the condition of respiratory distress syndrome (RDS) is seen more frequently. Therefore, among all premature children, 50 – 80% of them have the condition of respiratory distress syndrome.
Etiology:
- Prematurity,
- Low birth weight baby,
- Asphyxia,
- Maternal diabetes.
Sign And Symptoms:
- Rapid and shallow breathing,
- Respiratory rate >60/minute,
- Expiratory audible grating sound,
- Rib retraction,
- Intercostal or subcostal retraction,
- Cyanosis,
- In AD,
- Respiratory acidosis,
- Electrolyte disturbances,
- Dyspnea.
Diagnostic Evaluation (Diagnostic Evaluation) Evaluation) :
- History collection,
- Physical examination,
- Chest X ray.
Management (Management ):
- Aim of treatment:
- Provide surfactant replacement therapy.
- Provide breathing support through a nasal continuous positive airway pressure (NCPAP) machine or ventilator to help the infant breathe properly.
- Provide oxygen therapy.
Nursing Management:
- If infants and neonates are suffering from respiratory distress syndrome (RDS), they should be provided with artificial surfactant by inserting an artificial airway or breathing tube into the trachea/windpipe, which allows the surfactant to enter the lungs directly.
- Usually, surfactant starts to form in the lungs of the fetus from 24 weeks of gestation and is completely formed at 37 weeks of gestation. If adequate amounts are not formed, then artificial surfactant may be required in such conditions. is.
- Provide proper ventilatory support to the infant.
- Infants with respiratory distress syndrome require ventilatory support, which is provided by a mechanical ventilator connected to a breathing tube that passes through the infant’s mouth or nose into the windpipe.
- Provide breathing support to the neonate through nasal continuous positive airway pressure (NCPAP).
- To treat the condition of hypoxia and acidosis in neonates, provide warmed and humidified oxygen therapy at 35% to 40% positive pressure through endotracheal intubation.
- Provide continuous positive airway pressure (CPAP) to the neonate if the arterial oxygen tension PO2 is not greater than 50 mm of Hg.
- The levels of PO2, PCO2, and pH should be checked to identify any metabolic and respiratory acidosis conditions early. Do.
- If there is a condition of acidosis, administer sodium bicarbonate 4.2%. (0.5 meq/ ml Ex: 0.5 meq/ml amount to 1 meq/kg weight 1:1 with 5% glucose as the minimum dose.)
- Excessive use of alkaline can cause intraventricular hemorrhage or even death in preterm babies.
- An infant suffering from respiratory distress syndrome (RDS) should be given N. I. C. U. (NICU) and are kept in a radiant warmer or incubator to keep them warm and reduce the risk of infection.
- In this, the infant’s air passages are periodically cleaned by endotracheal suctioning.
- Continuous monitoring of heart rate, breathing and temperature through sensors taped to the infant’s body, in addition to using sensors on the fingers or toes to check the amount of oxygen in the infant’s blood.
- As prescribed by the pediatrician Administer albumin or colloid solution to treat the condition of hypovolemia.
- If there is a condition of anemia or electrolyte imbalance, then treat it properly.
Complications:
- Intraventricular hemorrhage,
- Pulmonary hemorrhage,
- Retrolental fibroplasia,
- Neurological abnormalities.
Prevention:
- Betamethasone should be administered to patients who are likely to deliver before 34 weeks.
- Assess lung maturity before induction of pre-mature labor and delay induction to minimize fetal risk.
- Prevent fetal hypoxia in diabetic mothers.
Umbelical Sepsis :

- Umbilical sepsis is the infection and inflammation of the umbilical cord stump in neonates. In which redness, swelling and discharge occur in the cord area.
Etiology:
- Staphylococcus aureus,
- Streptococcus species,
- Escherichia coli,
- Pseudomonas aeruginosa,
- Klebsiella species.
Risk Factores (Risk Factores):
- Poor hygiene,
- Premature birth,
- Low birth weight,
- Maternal infection,
- Delayed umbilical cord care.
Sign And Symptoms:
1) Local Symptoms:
- Redness,
- Swelling,
- Discharge,
- Pain.
2) Systemic symptoms:
- Fever,
- Lethargy,
- Poor feeding,
- Irritability,
- Signs of Apnea:
- Hypotension,
- Tachycardia,
- Abnormal Breathing Pattern
Diagnostic Evaluation (Diagnostic Evaluation) :
- History Collection,
Physical Examination, - Microbiological Testing
Umbilical Stump Culture,
Blood Culture,
Laboratory Tests
Complete Blood Count,
C – Reactive Protein,
Imaging
Management:
1) Initial assessment:
Clinical evaluation to properly examine the umbilical cord and neonate.
2) Antimicrobial Therapy:
Provide the child with appropriate broad spectrum antibiotic medication.
Provide the child with appropriate intravenous antibiotic medication (IV medication) such as cefotaxime, ampicillin, etc.
3) Local care:
Clean the clinical umbilical cord stump with sterile saline and Gently clean with antiseptic solution (Ex: Chlorhexidonel) Avoid using alcohol and iodine solutions which can cause irritation.
Drying: Keep the umbilical cord area dry to prevent further infection.
Wound Care: Apply a sterile dressing to the umbilical cord if necessary.
4) Supportive Care:
Monitoring: Monitor the child’s vital signs, including temperature, heart rate, and blood pressure, continuously.
Fluid Management: Provide intravenous fluids to maintain the child’s hydration and electrolyte balance to maintain their hydration status.
Nutritional Support: Provide adequate feeding and nutritional support to the child.
5)Follow-up:
Advise regular follow-up to assess the child’s condition.
Prevention:
Follow proper aseptic precautions while cutting the umbilical cord.
Low Birth Weight (Low Birth Weight) Preterm Baby OR Prematurity or Premature Baby
- Low Birth Weight i.e. if the weight of the child at the time of birth is less than 2500 gm, this condition is called Low Birth-Weight Baby (LBW).
- In which, Very Low Birth Weight i.e. if the weight of the child is 1500 gm or less, it is called Very Low Birth Weight (VLBW) baby.
- When, Extremely Low Birth Weight i.e. the birth weight of an infant is less than 1000 gm, then this condition is called Extreme Low Birth Weight (ELBW) baby.
Preterm Baby:

- Last A baby born before completing 37 weeks of pregnancy, calculated from the first day of the menstrual period, is defined as a preterm baby. These babies weigh 2500 grams or less.
Etiology:
- Uterine anomalies: Uterine anomalies such as malformation of the uterus and cervical incompetence can be causes of prematurity.
- Previous obstetric History: Women who have a history of previous abortions and preterm delivery may develop the condition of a premature baby.
- Multiple Pregnancy: When more than one fetus is growing in the uterine cavity, the condition of prematurity or low birth weight may arise.
- Maternal Diseases in Pregnancy: During pregnancy, certain disease conditions such as preeclampsia, polyhydramnios, antepartum hemorrhage (placenta previa, abortion) placenta).
- Causes of infection: Genital tract infection, acute appendicitis, pyelonephritis
- Chronic diseases: It involves pregnancy associated diseases such as diabetes, severe anemia, hypertension, etc.
- Fetal causes: It involves congenital anomalies due to which the condition of growth retardation can arise.
Classification:
Small For Gestational Age (SGA : Small For Gestational Age)
Preterm:
- Growth potential is normal and appropriate for the gestational period (10 to 90 percentile).
- Low Birth Weight i.e. if the weight of the child at the time of birth is less than 2500 gm, this condition is called Low Birth-Weight Baby (LBW).
- In which, Very Low Birth Weight i.e. if the weight of the child is 1500 gm or less, it is called Very Low Birth Weight (VLBW) baby.
- When, Extremely Low Birth Weight i.e. the birth weight of an infant is less than 1000 gm, then this condition is called Extreme Low Birth Weight (ELBW) baby.
Preterm Baby:
- Last A baby born before completing 37 weeks of pregnancy, calculated from the first day of the menstrual period, is defined as a preterm baby. These babies weigh 2500 grams or less.
Etiology:
- Uterine anomalies: Uterine anomalies such as malformation of the uterus and cervical incompetence can be causes of prematurity.
- Previous obstetric History: Women who have a history of previous abortions and preterm delivery may develop the condition of a premature baby.
- Multiple Pregnancy: When more than one fetus is growing in the uterine cavity, the condition of prematurity or low birth weight may arise.
- Maternal Diseases in Pregnancy: During pregnancy, certain disease conditions such as preeclampsia, polyhydramnios, antepartum hemorrhage (placenta previa, abortion) placenta).
- Causes of infection: Genital tract infection, acute appendicitis, pyelonephritis
- Chronic diseases: It involves pregnancy associated diseases such as diabetes, severe anemia, hypertension, etc.
- Fetal causes: It involves congenital anomalies due to which the condition of growth retardation can arise.
Classification:
Small For Gestational Age (SGA : Small For Gestational Age)
Preterm:
- Growth potential is normal and appropriate for the gestational period (10 to 90 percentile).
Small for gestational ageSGA : Small For Gestational age
Small for gestational age is a term used to describe a newborn with a birth weight less than the 10th percentile. It involves less than two standard deviations for gestational age. SGA fetuses may be constitutionally small or may be due to a pathologic process (fetal growth retardation).
Sign And Symptoms:
- Weight should be less than 2500 grams.
- Length should be less than 44 cm.
- Head and abdomen are large.
- Skull bones are soft with wide sutures and posterior fontanelles.
- Head circumference increases more than chest circumference.
- Ear pinnae are soft and flat.
- Skin is red, thin, and scaly due to low subcutaneous fat.
- Plantar creases are not visible before 34 weeks.
- Testicles are undescended.
- Labia minora are exposed because labia majora are not in contact.
- Nails are not properly grown to the finger tips.
Complication (Complications) :
- Asphyxia,
- Pulmonary syndrome,
- Cerebral hemorrhage,
- Fetal shock,
- Heart failure,
- Edema,
- Infection,
- Dehydration and acidemia,
- Anemia,
- Retrolental fibroplasia,
- Oliguria,
- Anuria,
- Jaundice.
Management:
- After the birth of the child, the cord should be clamped immediately, due to which the condition of hypervolemia can be treated. Then the condition of hyperbilirubinemia can be corrected.
- If there is a condition of hyperbilirubinemia and there is a need for exchange transfusion, then the length of the cord should be kept long.
- Clear the child’s mouth and nose properly with a mucus sucker.
- Properly use mask and nasal catheter to provide oxygen.
- Wrap the baby properly in a sterile towel.
- Keep the child in a proper head-down position on the cot.
- To prevent the child from hemorrhagic condition, inj. Vitamin. Provide K 1 mg I/M.
- Handle the baby with extreme gentleness.
- Advise the baby to avoid bathing.
- Keep the child’s body temperature properly stable.
- Prevent the child from developing atelectasis.
- Prevent the child from developing infection.
- Provide proper nursing care to the child.
- Preterm babies are functionally immature, so they need special care.
Rh Incompatibility (Rh Incompatibility) :
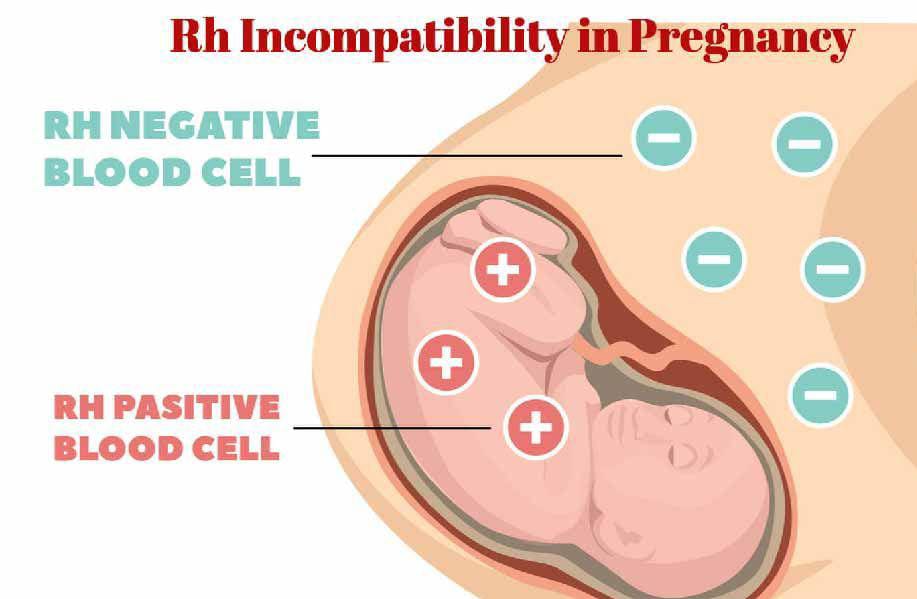
Rh Factor:
- Rh factor is a protein that is present on the surface of RBC (red blood cells). Which is called Rh positive and when this protein is not present on the RBC (Red Blood Cells) surface then that condition is called Rh negative.
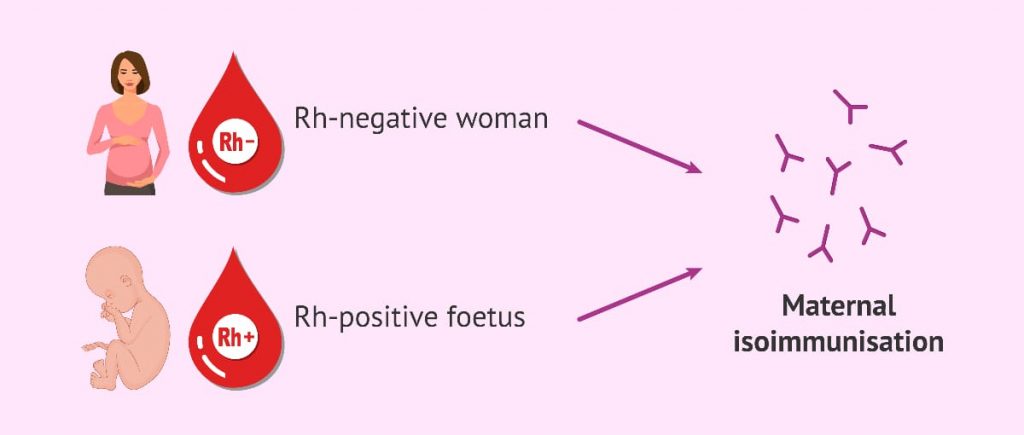
Rh Incompatibility:
- The condition of Rh incompatibility is also known as Hemolytic Disease of the Newborn (HDN).
- Rh Incompatibility The condition arises when the mother’s blood group is Rh – ve (blood group) and the blood group of the child developing in her womb is Rh +ve, then the condition of Rh incompatibility can arise in this condition.
Etiology:
- When the mother’s blood group is Rh -ve and the father’s is Rh+ ve, then The condition of Rh incompatibility may arise in the condition.
- Because of transfusion history.
- Immune response.
Sign And Symptoms:
- The amount of bilirubin increases due to the breakdown of RBCs. And the condition of jaundice may arise.
- Hypotonia,
- After birth the baby’s skin becomes yellowish and white.
- Lethargy,
- Low muscle tone,
- Swelling,
- Edema.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History Collection,
- Physical Examination,
- Polyhydroamnios,
- Higher amount of bilirubin than normal infant,
- Blood type test,
- Direct comb test,
- Fetal blood typing,
- Ultrasound,
- Middle Cerebral Artery Doppler.
Complications:
- Kernicterus,
- Hydrops Fetalis (severe edema in an unborn or newborn baby),
- Problems with movement, hearing, speech, etc. may occur.
- Seizures.
Management:
Provide Rh immunoglobulin injection.
Proper blood transfusion if the patient needs it.
Maintain the patient’s proper hydration status. This includes providing the patient with water, coconut water, fruit juice, which works to maintain the electrolyte levels in the body.
Maintain the patient’s electrolytes properly.
Provide the newborn with proper phototherapy.
Injury to the Nerve to the Neonate :
Facial Injury (Bells Palsy) Facial Injury (Bells Palsy):
- Direct forceps blade pressure on the facial nerve and excessive pressure on the facial nerve in the ramus of the mandible side during normal delivery can cause facial palsy. Its features include facial asymmetry, inability to close the eyes, rooting reflex on the affected side. When absent and crying, the angle of the mouth turns to the unaffected side. The shaking reflex is good. Recovery occurs in a few weeks due to good regenerative power and short length of the nerve. Protect the eyes with antiseptic ointment as they remain open even during sleep.
Brachial Palsy :
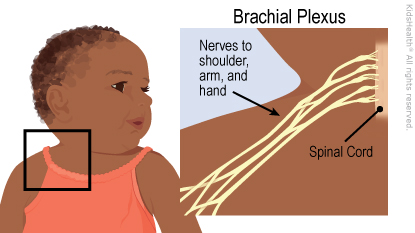
- Brachial palsy is caused by injury to the brachial plexus in shoulder dystocia or by traction on the shoulder or hyperextension of the neck during spontaneous vaginal delivery.
- Clinical types of brachial palsy include Erb’ palsy and Klumpke palsy.
1) Erb’s palsy:
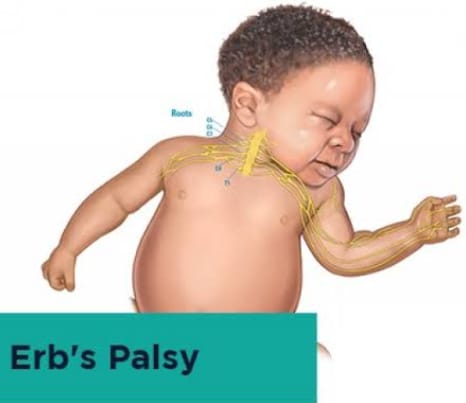
- Erb’s palsy is caused by injury to the C5 and C6 nerve roots. Its clinical features include paralysis of the arm with elbow extension, pronation of the forearm, and flexion of the wrist (waiter tip) on the affected side. Moro’s reflex is absent on the affected side. Permanent disability may occur in severe injuries. Treatment includes splinting of the arm, massage, and passive movements. Complete recovery usually occurs within a week or a month.
2) Klumpke’s palsy:
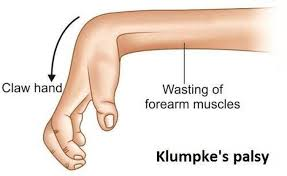
- The 7th and 8th cervical and 1st thoracic nerve roots Damage causes Klumpke palsy. Its features include paralysis of the forearm muscles with wrist drop and flaccid digits. The arm is flexed at the elbow. A flaccid hand and flexed fingers are seen with wrist extension. Damage to the cervical sympathetic chain of the 1st thoracic root causes conditions such as miosis (small, constricted pupil), tosis (drooping of the upper eyelid), and anhidrosis (a rare condition in which the sweat glands produce little or no sweat). Management includes arm splinting, placing cotton balls on the baby’s hands to prevent contractures, and gentle massage and passive movements. The prognosis is good but in severe lacerations and hemorrhages, permanent deformity remains. If paralysis lasts more than 3 months, then neuroplasty is also required.

Injury to the Bone: Bone injury can occur in the clavicle, humerus, and cervical spine. It is seen in difficult shoulder and breech delivery, in which green stick fracture is common. Depressed fracture is seen in the skull bone. Dislocation can occur in the hip joint, jaw, and cervical vertebrae, so callus formation is necessary for excellent prognosis. Immediate identification and its immediate management are important.
Injury to the Muscles: It is common in the sternomastoid muscles due to excessive lateral flexion of the neck in normal delivery, muscle injury is seen in difficult breech delivery and shoulder dystocia. On or after 7-8 days of birth, muscle fibers and blood vessels rupture, resulting in the formation of hematoma and presenting as a tumor. This condition is complicated by contractures and torticollis (stiff neck with muscle spasm). No specific management is required. Most often disappears within 6 months. Stretching of the neck muscles with gentle movements is helpful, but massage is not required. Torticollis persists even after 1-2 years. Surgical intervention is required.
Injury to the skin and subcutaneous tissue:Superficial abrasions, petechiae and bruising are seen after prolonged labor or forceps delivery. Spontaneous recovery occurs in 2-3 days. Local application of antibiotic lotion and hygienic practices can speed healing.
Injury to the viscera:Visceral injury can occur after difficult breech delivery and unskilled cardiac massage. Laceration of the liver capsule and spleen and adrenal hemorrhage can occur. The neonate may present with pallor, tachycardia, and features of shock. Correct hypovolemia and anemia to manage the condition. Repair viscera in surgical management. The prognosis is often poor.
Prevention of Birth Injuries: The incidence of birth injuries can be reduced by comprehensive antenatal and intranatal care.
Birth injuries can be prevented by skilled antenatal examination and identification and management of high-risk cases during the skilled antenatal period.
Birth injuries can be prevented by the following practices during the intranatal period.
To prevent injury to the brachial plexus or sternomastoid muscles, do not stretch the neck unnecessarily during shoulder delivery in spontaneous vaginal delivery. To prevent scalp injuries, perform episiotomy with care. To prevent cerebral anoxia, perform continuous fetal monitoring. To prevent birth injuries in forceps delivery, take precautions. Vaginal breech delivery should be performed by skilled personnel. Prolonged labor should be managed carefully.
Caput Succedaneum (Caput Succedaneum) :

- Edematous swelling occurs due to accumulation of serosanguinous fluid in the layers of the scalp, which is called caput succedaneum. It is caused by pressure from the girdle of contact. It can be the bony pelvis, dilating cervix or vulval ring. Due to low venous return, swelling and lymphatic drainage are seen.
- Caput sucadanium is also seen at the time of birth. And when pressed, a pit forms in it. Swelling is a bougie. And it crosses the suture line which disappears in 24-36 hours. It is mostly seen after membrane rupture.
Cephalohematoma (Cephalohematoma) :
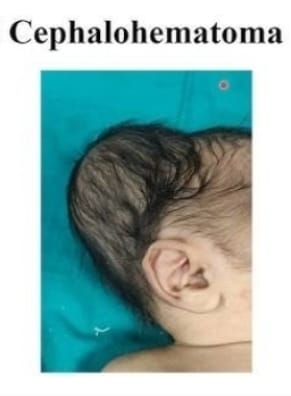
- A cephalohematoma is a condition in which blood collects under the pericranium and flat bones of the head that cover the skull bone, usually unilateral and over the parietal bone. It is caused by rupture of a small emissary vein from the skull and may be associated with a fracture of the skull bone. It can occur after forceps delivery but can also occur after normal labor. Ventouse application does not increase the incidence of cephalohematoma. It is never present at birth but develops gradually after 12-24 hours.
- This swelling is limited by the lines of the sutures of the pericranium of the skull which are fixed to the margins of the bone, soft, fluctuant and incompressible.
- It grows and disappears on its own within a few weeks, approximately 6 weeks.
Congenital Anomalies:
- Congenital anomalies are also called birth defects. Congenital anomalies: That is, any metabolic, biochemical, structural, and functional disorder present in a child at the time of birth is called congenital malformation. When a child has only a structural defect present at the time of birth, it is called “congenital malformation”.
- Congenital anomalies affect any part of the body and cause physical and developmental disabilities. These congenital anomalies are usually seen during the development of the child, i.e. during intrauterine life, due to any genetic factor, environmental influences, or a combination of both. Genetic factors include chromosomal abnormalities, gene mutations, environmental influences, maternal infections, exposure to harmful substances during pregnancy (alcohol and certain medications), maternal health conditions such as diabetes, and obesity, etc., and a combination of both.
- Congenital anomalies include central nervous system anomalies, cleft lip, cleft palate, Hatha disease, club foot, Down syndrome and genetic syndromes.
Etiology:
- Genetic factors include inherited genetic mutations and chromosomal abnormalities that are passed down from parents to their children.
Ex: Autosomal dominant disorders (Marfan syndrome),
Autosomal recessive disorders (cystic fibrosis),
X – linked genetic dish order (hemophilia),
And chromosomal abnormalities (Down syndrome).
Environmental factors
Certain types of environmental exposure during pregnancy can increase the risk of congenital anomalies. Such as, maternal exposure during intrauterine life Infections especially STORCH (syphilis toxoplasmosis, rubella, cytomegalovirus, herpes virus), - During pregnancy, the mother is exposed to teratogenic substances such as alcohol, tobacco, smoking, certain medicines, etc.
- During pregnancy, the mother is exposed to X-rays.
- During pregnancy, the mother takes certain drugs such as steroid hormones,
stilbestrol,
anticonvulsants, Folate antagonists, cocaine, lithium and thalidomide. - Due to maternal diseases such as diabetes, obesity, cardiac failure, malnutrition, iodine deficiency, folic acid deficiency etc.
- Due to abnormal environmental conditions such as bicornuate uterus, septate uterus, polyhydroamnios, oligohydroamnios, fetal hypoxia etc.
- Environmental pollution Due to.
Sign And Symptoms:
- Physical Abnormalities
- Many types of congenital anomalies are visible such as,
- Cleft lip,
- Cleft palate,
- Limb deformities
- (club foot),
- Facial features being abnormal,
- Growth pattern being abnormal (microcephaly and macrocephaly) etc.
2) Developmental delay
Some children with congenital anomalies experience delays in achieving developmental milestones. These usually involve motor skills, language, speech development, cognitive abilities, social and emotional development, etc.
3) Organ dysfunction
Some types of congenital anomalies can cause dysfunction in internal organs and their Signs and symptoms include,
Congenital heart disease (cyanosis, rapid breathing,
poor feeding,
failure to thrive, etc.).
Gastrointestinal tract anomalies (including
feeding difficulty,
nausea,
vomiting,
abdominal pain, and failure to pass meconium, etc.).
4) Neurological symptoms
Some types of congenital anomalies affect the central nervous system, causing seizures,
abnormal reflexes, muscle Symptoms such as weakness, paralysis, developmental regression, intellectual disabilities, etc. are seen.
5) Respiratory Symptoms
Some types of congenital anomalies affect the respiratory system such as
congenital diaphragmatic hernia,
choanal atresia (narrowing of the nasal airway or tissue) causing respiratory symptoms such as respiratory distress,
breathing difficulty,
rapid breathing and cyanosis. Death.
6) Genitourinary Abnormalities
Urinary tract abnormalities such as
genital abnormalities,
problems with kidney function, its symptoms include urinary tract infection,
difficulty in urinating,
abnormal genitalia etc.
7) Sensory impairment is seen
Congenital deafness,
Blindness.
List of Common Congenital Anomalies in Children
Common Congenital Anomalies in
1)Central Nervous System,
2) Congenital Heart Diseases,
3) Gastro intestinal system,
4) Respiratory system,
5) Genito urinary system,
6) Musculoskeletal abnormality,
7) Blood disorder,
8) Metabolic disorder 9) Endocrine abnormality,
10) Chromosomal abnormality
etc. System involvement occurs.
1) Central nervous system
Anencephaly, spina bifida occulta, spina bifida cystica in the central nervous system (Meningocele, Meningomyelocele), Hydrocephalus, Microcephaly, Macrocephaly, Porencephaly etc. are included.
2) Congenital Heart Disease,
Congenital Heart Disease includes Atrial Septal Defect (ASD), Ventricular Septal Defect (VSD),
Tetralogy of Fallot (TOF),
Coarctation of Aorta (COA),
Patent Doctrine Arteriosis (PDA),
Transposition of Great Artery.
Aortic Stenosis, pulmonary stenosis, mitral or aortic regurgitation, etc. are involved.
3) Gastrointestinal system,
Gastrointestinal system includes cleft lip, cleft palate, tracheoesophageal fistula, esophageal atresia, congenital pyloric stenosis, duodenal atresia, congenital megacolon (Hisprung’s disease), exomphalos, umbilical hernia, anorectal malformation, diaphragmatic hernia, femoral hernia, Involvement of geriatrics, congenital intestinal obstruction etc. occurs.
4) Respiratory system,
Respiratory system includes choanal atresia, tracheoesophageal fistula, congenital atelectasis, pulmonary agenesis, congenital strider, congenital cyanosis etc.
5) Genito-urinary System,
Genito-urinary system includes congenital hydronephrosis,
congenital polycystic kidney,
Hous Su kidney,
hypospadiasis,
epispadiasis, congenital phimosis, congenital hydrocele, undescended testis, congenital inguinal hernia, ambiguous genitalia etc.
6) Musculoskeletal abnormalities,
Musculoskeletal club foot, congenital dislocation of hip, developmental dysplasia of hip (DDH), Osteogenesis imperfecta, polydactyly, syndactyly, Marfan syndrome, muscular dystrophy etc.
7)Blood disorders,
thalassemia, hemophilia, sickle cell anemia, G6PD deficiency etc.
8)Metabolic disorders
Metabolic disorders include cystic fibrosis, phenylketonuria, G6PD deficiency, congenital lactose intolerance, Galactosemia, Wilson’s disease, etc.
9)Endocrine Abnormalities: Endocrine abnormalities include congenital hypopituitarism (dwarfism),
congenital hypothyroidism (cretinism),
congenital adrenal hyperplasia, congenital goiter, diabetes mellitus, etc.
10)Chromosomal Abnormalities
Chromosomal abnormalities include
Down syndrome (trisomy 21),
Edwards syndrome (trisomy 18), Patau syndrome
(trisomy 13),
Turner syndrome (Xo),
Klinefelter syndrome (XXY, XXXY).
11) other Anomalies
Congenital cataract, congenital glaucoma, rat’s blastoma, color blindness, congenital deafness, deaf and dumb, mental retardation, albinism, hemangioma, Pader Willi syndrome, Apert syndrome. etc. are congenital anomalies.
Diagnostic Evaluation (Diagnostic Evaluation):
- History Collection,
- Physical Examination,
- Imaging Studies,
- Ultrasound During Pregnancy,
- X-Ray,
- Magnetic Resonance Imaging,
- Computed tomography,
- Genetic testing,
- Laboratory testing,
- Blood test,
- Amniocentesis in early pregnancy (14 to 16 weeks),
- Assess the maternal serum alpha-phyto Protein(AFP),
- Antenatal Screening,
- Cardiac Evaluation,
- Neurological Assessment,
Complication:
- Physical disability,
- Limb deformity,
- Health problems such as arrhythmias due to congenital heart defects,
- Heart failure,
- Developmental mental delay,
- Such as motor skills, language and Cognitive impairment is observed.
- Psychological challenges are observed.
- Psychological impact is observed,
- Educational challenges due to developmental delay are observed.
Management:
- A child with congenital anomalies requires regular medical monitoring and follow-up to monitor their growth, development, and overall health status. This includes regular physical assessment, laboratory investigations, imaging studies, etc.
- Some types of anomalies require appropriate surgical intervention to treat them and alleviate symptoms. This surgical intervention is usually required for the reconstruction of any anatomical structure, be it a cardiac anomaly, limb deformity, cleft lip and cleft palate.
- Some types of congenital anomalies require medication treatment to relieve symptoms such as arrhythmias, heart failure, and blood clotting in congenital heart defects.
- Free rehabilitation therapy to treat certain types of congenital anomalies, including physical therapy, Speech therapy, occupational therapy, etc. are required.
- A child with a congenital anomaly needs to be provided with a nutritious diet and feeding for proper growth and development.
- A child with a congenital anomaly and his/her family members should be provided with adequate counseling and psychological support to cope with the condition.
- The child’s family members should be provided with adequate counseling and psychological support to help them cope with the condition.
- The child’s family members should be provided with adequate counseling and psychological support to help them cope with the condition. Provide complete education about the disease, its causes, symptoms and signs, and its treatment.
- Provide proper genetic counseling to the child’s family members and parents.
- Some types of congenital anomalies require life-long treatment, so all health care providers and family members should be properly collaborative and cooperative to provide proper treatment to the child.
- Children with congenital anomalies To provide adequate comprehensive care.
- To provide adequate psychological support to the parents of the child.
Prevention:
1) Preconception Care
Preconception care involves providing counseling and proper education to women of childbearing age, which During pregnancy, a woman can take proper health care.
It usually involves a healthy lifestyle, a balanced diet, maintaining an adequate weight, exercising regularly, avoiding harmful substances such as alcohol and smoking,
and taking proper treatment if there is any medical health problem.
2) Prenatal Care
Early and comprehensive prenatal care is needed to properly assess the health of the mother and child. Due to prenatal screening, if the child has any congenital anomaly, it is detected early and appropriate treatment is provided. This involves appropriate screening tests such as ultrasound and genetic testing and advising women to eat an adequate nutritious diet, drink adequate fluids, take folic acid supplements to prevent neural tube defects, get adequate sleep, avoid smoking and alcohol, and avoid contact with any harmful substances.
3) Genetic Counseling and Testing
Genetic counseling provides education to women and couples about the risks of having a child with any congenital or acquired anomalies, including family history, genetic factors, and previous Proper counseling is provided after assessment of pregnancy. Genetic counseling can be provided to women and couples to prevent congenital anomalies in the child.
4) Avoiding teratogenic exposure
Pregnant women should be properly educated to avoid exposure to teratogenic substances and harmful substances and any type of radiation, and to avoid taking harmful drugs that can cause congenital anomalies in the child. Such as over-the-counter drugs, herbal supplements, alcohol, tobacco, smoking, radiation, environmental toxins, etc., which increase the risk of anomalies.
5) Optimizing Maternal Health
Providing appropriate health care before and during pregnancy can help prevent congenital anomalies in the child. Risks can be prevented. If the mother has any long-term diseases, such as diabetes mellitus, hypertension, and thyroid disease, it should be treated properly.
If the mother has any type of infection, it should be treated immediately.
If the child has any nutritional deficiency, then adequate food and vitamin supplements should be provided to him.
6) Folic acid supplements
Taking adequate folic acid supplements before pregnancy and during early pregnancy can prevent neural tube defects in the child. Such as spina bifida, anencephaly etc. Women of child bearing age should be advised to take daily supplements of 400 to 800 micrograms of folic acid starting one month before conception and continuing till the first trimester after conception.
7) Environmental and Occupational Safety
Pregnant women should not be exposed to any kind of hazardous chemicals and pollution due to which anomalies can be prevented. Occupational safety guidelines and regulations should be followed regularly.
8) Screening and Prenatal Detection
Prenatal screening such as ultrasound, maternal serum screening, and non-invasive prenatal testing (NIPT) all these tests help in detecting any congenital anomalies and genetic abnormalities in the child. If early dissection is done, congenital defects can be prevented by adequate medical treatment.
Congenital anomalies in the child can be prevented by using all these preventive measures.
Newborn of HIV positive mother HIV / AIDS (Human immunodeficiency virus/acquired immunodeficiency syndrome) :

- Acquired Immunodeficiency Syndrome is a disorder caused by the Human Immunodeficiency Virus (HIV) in which there is a generalized dysfunction of the immune system. It affects both cellular and humoral immunity.
Mode of Action:
Two modes of transmission are mainly seen in newborns.
1) Horizontal Transmission: Horizontal transmission of HIV occurs through intimate sexual contact or exposure to parenteral blood or contact with body fluids containing visible blood.
2) Vertical (Perinatal) Transmission: Vertical transmission is usually the transmission of infection from an HIV infected pregnant woman to her fetus.
Sign And Symptoms:
At birth, most children with HIV appear healthy and if not treated within 2-3 months, signs and symptoms may develop:
Early sign of HIV:
- Repeated fungal infections, mouth and oral thrush (oral cavity and posterior pharynx).
- Poor weight gain,
- Lymphadenopathy (enlarged lymph nodes),
- Neurological problems,
- Multiple bacterial infections,
- Hepatomegaly,
- Pneumocystis carinii pneumonia (PCP) which usually occurs between 3 and 6 months of age.
Late signs of HIV:
- Diarrhea,
- Failure to Thrive,
- Developmental Delay,
- Hepatosplenomegaly,
- Chronic Pneumonia, Cough and Lymphoid Interstitial,
- Chronic Otitis Media,
- Malase,
- Fatigue,
- Weight Loss,
- Fever,
- Night Sweats,
- Nephropathy,
- Encephalopathy.
Diagnostic Evaluation (Diagnostic Evaluation) :
History Collection,
Physical Examination,
ELISA (Enzyme Linked Immuno Sorbent Assay),
Western Blot Test (This shows the presence of HIV antibodies and is useful in children over 18 months of age),
P24 Antigen: It is used to detect HIV antigen in children younger than 18 months. Two or more positive results are diagnostic for HIV infection.
CD4: Its Used to evaluate the child’s immune status, risk for disease progression, and need for Pneumocystis carinii pneumonia (PCP) prophylaxis after 1 year of age.
Management:
- Provide prophylaxis to infants born to HIV-infected women during the first year of life as indicated for the patient.
- Provide continuous prophylaxis to children diagnosed with HIV at 12 months of age.
- Provide antiretroviral therapy as a prescribed action of antiretroviral therapy to suppress viral replication to maintain immune function and delay disease progression.
- Provide highly active antiretroviral therapy to the child as appropriate.
General Care :
- Advise on proper hand washing.
- Notify the physician immediately if the child has conditions like weight loss, vomiting, diarrhea, malaise, altered activity level, or oral lesions.
- Properly check the child for signs and symptoms of opportunistic infections.
- Properly prescribe antiretrovirals to the child. Provide medication.
- Keep the child properly isolated.
- Keep the child’s immunizations up to date.
- Keep the child under proper monitoring and monitor the child’s daily weight.
- Provide the child with a proper calorie and protein rich diet.
- Properly cover the food Keep.
- Wear gloves if you are in contact with body fluids while caring for a child.
- Change the child’s diaper frequently and wear gloves properly when changing diapers.
- Fold soiled diapers inward and dispose of in a tightly covered plastic container.
- Clean spills with a bleach solution (10:1 ratio of bleach and water) Do.
- Dispose of garbage daily.
- Immunization against common childhood illnesses is recommended for all children who have been in contact with or infected with HIV.
- Immunize the child with pneumococcal and influenza vaccines.
- If the child is not severely immunocompromised, they should be vaccinated against mumps, measles, and rubella ( M.M.R.) Vaccine Administration.
Newborn of a Diabetic Mother :
- Newborn of a diabetic mother refers to a newborn or infant born to a mother who has diabetes. A mother who has diabetes, either pre-existing (type 1 or type 2) or gestational diabetes (diabetes that develops during pregnancy). This condition can affect the baby’s health and development in many ways, including the management of potential complications such as low blood sugar, respiratory problems, jaundice, and an increased risk of congenital anomalies, requiring careful monitoring and management immediately after birth.
Usually two types of diabetes can occur during pregnancy, such as,
1) Gestational diabetes,
2) Pre-gestational diabetes
1) Gestational diabetes: This type of diabetes occurs only during pregnancy because hormonal changes during pregnancy cause resistance to insulin. Here, the mother does not have diabetes before pregnancy.
2) Pre-gestational diabetes: In this condition, the woman already has a condition of diabetes such as insulin dependent diabetes.
Etiology:
- The growing fetus is supplied with nutrients and water by the placenta. To maintain pregnancy, a number of hormones are produced (cortisol, estrogen, human placental lactogen) that can block insulin. This usually occurs at 20-24 weeks of pregnancy.
- On the other hand, with the growth of the placenta, hormonal production also increases, which increases insulin resistance. Normally, the pancreas produces extra insulin to counteract insulin resistance, but gestational diabetes occurs when insulin production is not enough to counteract the effects of placental hormones.
- A woman with pre-existing diabetes has an increased need for insulin, e.g. Insulin-dependent mothers may require more insulin as pregnancy progresses.
Effects of diabetes in pregnancy on the fetus:
- The effects of diabetes during pregnancy on the fetus are a matter of concern because the increase in the mother’s blood sugar level during pregnancy is transferred to the fetus. This causes the child’s body to secrete more insulin, which causes tissue growth and fat deposition, causing the newborn to be larger than expected for the age of the pregnancy.
- There is a risk of congenital anomalies in newborns of diabetic mothers. Congenital anomalies such as heart, brain, spinal cord, urinary tract and gastrointestinal system problems may occur.
Other conditions:
Hypoglycemia,
Macrosomy,
Birth injury,
Respiratory distress.
Sign And Symptoms:
- Large size baby (due to excessive fat and glycogen accumulation in tissues),
- Face and cheekbones,
- Hyper bilirubinemia,
- Signs of hypoglycemia:
- Twitching,
- Lethargy,
- Seizures,
- Difficulties in feeding,
- Apnea,
- Cyanosis.
- Signs of respiratory distress:
- Cyanosis,
- Tachypnea.
- Nasal flaring,
- Grunting,
Management:
- Properly check for any signs and symptoms of respiratory distress.
- Properly check the child’s bilirubin level.
- Properly check the child’s blood glucose level.
- Properly monitor the child’s weight.
- Properly provide feeding to the child after the birth of the child.
- Properly check the child for edema.
- Properly assess the child for seizures and tremors.
- Properly assess the child’s calcium level.
- Properly provide oxygen if the child is in respiratory distress.
- Properly assess the child for any birth injury. To do.
Levels of Care in NICU (Levels of Care in NICU):

Neonatal Intensive Care Unit ( NICU ):
- Neonatal is a word formed by combining the following words Such as:
- NEW := new,
NATAL := birth or origin. - Neonatal Intensive Care Unit (NICU) is also called Intensive Care Nursery (ICN) where ill and premature newborns, infants are properly cared for.
Level of Care in N. I. C. U.( NICU ):
N. I. C. U. ( NICU ) is mainly divided into four categories as follows,
- 1) Level I : Well Newborn Nursery,
- 2) Level II : Special Care Nursery,
- 3) Level III : Neonatal Intensive Care Unit,
- 4) Level IV : Regional Neonatal Intensive Care Unit.
1) Level I : Well Newborn Nursery:
- Well Newborn Nursery is commonly known as Well Baby Nursery, this type of nursery has the ability to provide resuscitation at every delivery.
- It evaluates healthy newborn infants and provides them with proper care.
- It provides proper care to neonates born between 35 and 37 weeks.
- It provides care to neonates born between 35 and 37 weeks gestational age.
- It provides care to infants born at less than 35 weeks gestational age. During this time, neonatal care is provided to the neonate until it is transferred to the appropriate neonatal care unit.
They include,
Pediatrician,
Family Physician,
Nurse Practitioner,
and other advanced practice registered nurses.
2) Level II : Special Care Nursery:
- This is a special care nursery in which Level I nursery The capability to provide all the care of the neonate is involved.
- It usually provides care for neonates born at 32 weeks of gestation weighing 1500 grams or less and those who are physiologically immature are provided care in Level II Special Care Nursery.
- Infants who are able to feed and are in recovery position after intensive care are cared for in Special Care Nursery.
- In this, mechanical ventilation is provided for a brief duration and positive pressure is maintained continuously.
- Infants born less than 32 weeks gestational period and weighing less than 1500 grams are provided with care to stabilize them in this special care nursery before being transferred to the neonatal intensive care facility.
- Involvement of neonatologists, neonatal nurse practitioners, and all Level I health care providers
3) Level III : Neonatal Intensive Care Unit:
- Suspended life support care is provided in it.
- Comprehensive neonatal care is provided in it.
- It includes medical subspecialties, Immediate access to pediatric surgical specialties, pediatric anesthesiologists, and pediatric ophthalmologists is available. Facilities for providing immediate ventilatory support and respiratory support are also available. Facilities for computed tomography (CT) scans, magnetic resonance imaging (MRI), and echocardiography are also available. All Level I and Level II care providers are available, including pediatric surgeons, pediatric medical subspecialists, pediatric anesthesiologists, and pediatric ophthalmologists.
4) Level IV : Regional Neonatal Intensive Care Unit:
- This is a unit in which the highest level of neonatal care is provided.
- In it, all the care facilities of Level I, Level II and Level III are available.
- In it Extracorporeal membrane oxygenation (ECMO) facilities are also available.
