ENGLISH-NEW MIDWIFERY GNM TY UNIT 9 management of the high risk Labour
Unit : 9 management of the high risk labor

Obstructed Labor :
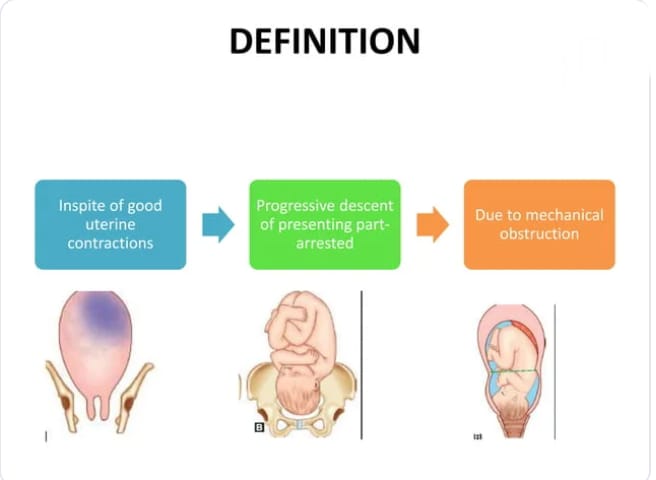
Definition:
- Obstructed Labor is a condition in which the presenting part of the fetus, which is progressively descending despite good (proper) uterine contractions, is arrested due to a mechanical obstruction. This is called “obstructed labor”. In obstructed labor, the fetus may die due to the fetus not getting adequate oxygen.
Etiology:
1)Fault in passage (Birth Canal),
2) Fault in Passage (Fits)
1)Fault in Passage (Birth Canal):
( a )Bonnie ,
( b )Soft Tissue Obstruction
( a )Bonnie :
- Contracted Pelvis,
- Cephalopelvic Disproportion ( CPD ),
- Abnormal pelvis ( Ex : android, anthropoid)
( b )Soft tissue obstruction:
- Cervical dystocia due to prolapse or previous operative scarring Due to,
- Cervical or broad ligament fibroid,
- Impacted ovarian tumor,
- Tumors in the rectum, bladder, and pelvic bone.
- Bicornuate uterus.
- Abnormalities in the uterus.
- Due to vaginal stenosis.
- Due to vaginal septum.
- Due to rigid perineum.
2) Fault in passenger (fits):
- Transverse lie,
- Brow presentation,
- Due to congenital malformation of the fetus (Ex: Hydrocephalus),
- Due to being a big baby,
- Occipito-posterior position,
- Compound Presentation,
- Locked Twins.
Sign And Symptoms:
Effect on Mother
Immediate
Immediate Excretion,
Dehydration,
Metabolic Acidosis,
Genital sepsis,
Injury to the genital tract,
Postpartum hemorrhage,
Shock.
Remote
Genito urinary fistula/ recto vaginal fistula,
Vaginal atresia,
Secondary amenorrhea.
Effect on the fetus
Asphyxia,
Acidosis,
Intracranial hemorrhage,
Infection.
Nursing Management:
- Identification of obstructed labor during the antenatal period of the mother so that early measures can be taken.
- Proper monitoring of the mother during the intranatal period and proper maintenance of the partograph for early detection of obstructed labor
- Preventing the mother from dehydration, ketoacidosis and Prevent sepsis and maintain the mother’s hydration status.
- Administer intravenous fluids to the mother, mainly Ringer lactate (RL) fluid, to correct dehydration and acidosis.
- Correct acidosis in the mother with 100 ml of 8.4% sodium bicarbonate.
- Monitor biochemical parameters, such as serum bicarbonate levels.
- Provide the mother with proper antibiotic medication such as,
administer 500 mg ampicillin and repeat it at 6 hour intervals. - Send blood sample to the laboratory for blood group and cross matching. And keep a blood bottle ready if operative interference is to be performed.
- Take a vaginal swab and send it to the laboratory for culture and sensitivity test.
- In the management of obstetric labor Early removal of obstruction through safe delivery. Do not give oxytocin or trial for safe delivery of the patient.
- If the baby is head down and the baby is alive, perform forceps delivery and then check for ureteral rupture and tarry stools.
- If the baby is dead, perform destructive operation and deliver.
- Do not perform internal version in obstructed labor.
- If the obstetrician If the case of labor is detected early and the condition of the fetus is good, perform a cesarean section.
- Symphysiotomy As an alternative to cesarean section, when there is contraction in the outlet, an opening is made in the symphysis pubis to widen the pelvic cavity.
Malposition:
Definition:
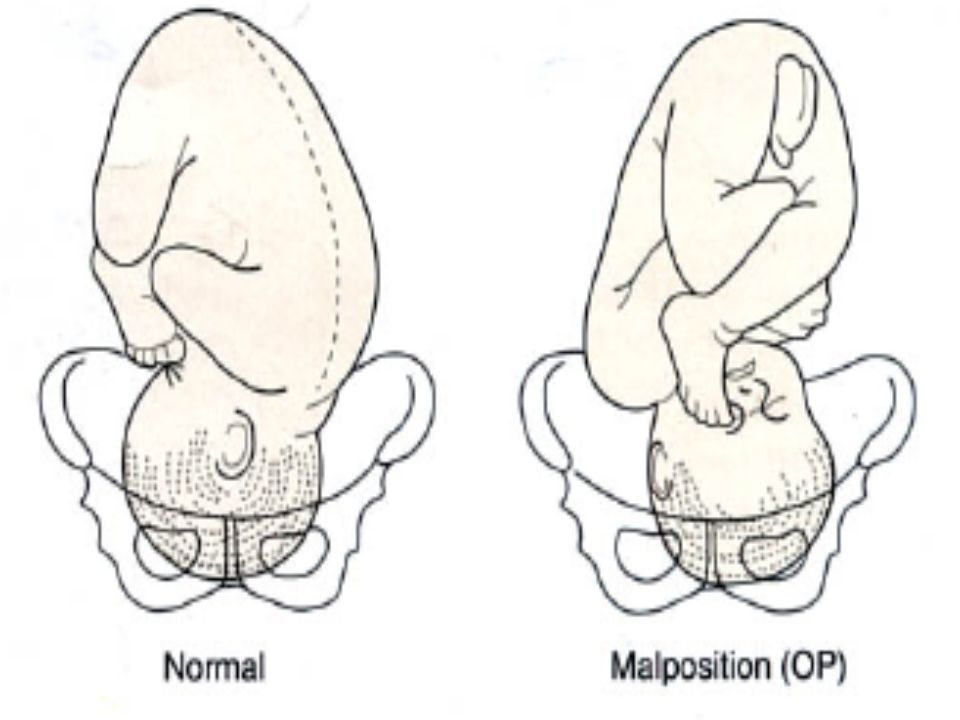
- Any position of the vertex during intrauterine life other than the flexed occipito anterior position is called malposition.
Occipito posterior position:
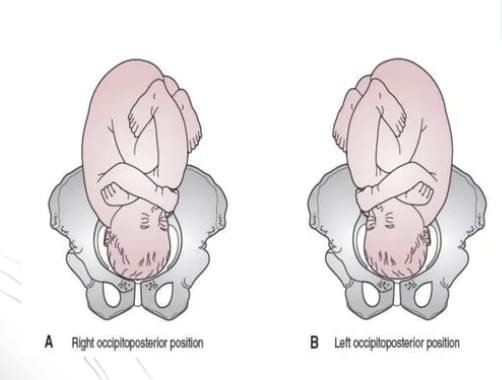
- When the occiput is placed on the right sacroiliac joint or directly above the sacrum in the vertex position of the fetus, it is called the occipito-posterior position.
- When the occiput is placed on the right sacroiliac joint, the condition is called the right occipito posterior (R.O.P) position and when it is placed on the left sacroiliac joint, it is called the left occipito posterior (L.O.P) position. When it points towards the sacrum, it is called a direct occipito posterior position.
- Occipito posterior is not an abnormal presentation of the fetus’s vertex during intrauterine life, but rather an abnormal position or malposition. When the occiput of the fetus in vertex presentation is in a posterior position (over the sacroiliac joint or directly over the sacrum) rather than in the anterior portion of the pelvis, the condition is called an occipito posterior position.
Etiology:
- Most of the time the etiology is not clear but the following are the responsible factors:
- 1.Fault in passage: Transverse narrowing of the midpelvis in android/anthropoid or platypeloid pelvis favors posterior position. In this, the anterior posterior diameter is larger, so the head engages it instead of the transverse diameter of the bream.
- 2. Passenger fault: In this, there is flexed head, large fit involvement.
- 3. Power fault: In this, uterine inertia, epidural analgesia in labor favors occipito posterior position.
- 4. Contracted pelvis: Here, especially android pelvis Occipito posterior leads to the condition.
- 5. Prematurity: Small fetuses can be in any diameter of the pelvic brim with any part of their head. Therefore, prematurity may be a potential for occipito-posterior position.
- A poorly flexed flat sacrum leads to deflection and occipito-posterior position.
Diagnostic Evaluation:
- Abdominal Examination,
Vaginal Examination,
Radiography. - Abdominal Examination:
Inspection: On inspection, the abdomen below the umbilicus appears flat.
Palpation: Fetal limb feels soft near the midline. Fetal back and anterior shoulder are away from the midline. Fetal head is not engaged and foot is not prominent.
Auscultation: F.H.S. In ROP, it is heard on the right side and in LOP, it is heard on the left side. - Vaginal examination,
- The bag of membranes may rupture due to the increase in length.
- The sagittal suture lies in any oblique diameter of the pelvis.
- The posterior fontanelle is felt towards the sacroiliac joint.
- The posterior fontanel fills more slowly due to the well flexed head in the occipito-anterior direction, while the anterior fontanel fills more easily due to the deflected head in the occipito-posterior direction.
- Radiography.
Mechanism of Labor:
- Engagement of Head: The head engages from the right oblique diameter in the right occipito posterior position (ROP) and from the left oblique diameter in the left occipito posterior position. The engaging transverse diameter of the head is biparietal (9.5 cm) and the anterior-posterior diameter suboccipito-frontal (10 cm) or occipito-frontal 11.5 cm.
- In favorable circumstances:
- 1. Flexion: If there are good uterine contractions, the head is well flexed and descends down until the head is above the pelvic floor.
- 2. Internal rotation of the head: The occiput is turned forward The 3/8th circle (135 degrees) of rotation comes behind the QBC, with this the neck torsion cannot remain suspended, so the solder rotates about 2/8th circle, which comes in the right oblique diameter in ROP and the left oblique diameter in LOP.
- There is still 1/8th part of the torsion remaining on the neck.
- The fit descends further down and the head is delivered in the occipito anterior position.
- Restitution: Head no. The movement of restitution is in the opposite direction of internal rotation to the extent of 1/8th of a circle.
- External rotation: External rotation occurs in the same direction as restitution through 1/8th of a circle as the solder rotates from the oblique to the anterior-posterior diameter of the pelvis.
- Birth of solder and trunk:
The process of expulsion is similar to the occipito anterior position. - Unfavorable Circumstances:
- Incomplete Forward Rotation/Deep Transverse Arrest: In this condition, the occiput rotates anteriorly 1/8 of a circle and the sagittal suture is in the biceps diameter. It does not rotate forward after that.
- Non-Rotation: Due to moderate deflection of the head, both the sinistra and occiput touch the pelvic floor simultaneously. Also, the occiput does not rotate. The sagittal suture remains in the oblique diameter. And the mechanism of the aggravation does not occur. That condition is called oblique posterior arrest.
- Malrotation: In excessive deflection of the head, the first sinistra touches the pelvic floor and its anterior 1/8 rth of a circle rotation causes the occiput to enter the sacral hollow. That position is called occipito sacral-position or persistent occipito posterior position (POP) of the vertex. If the conditions are favorable, i.e. the baby is of average size, good uterine contractions and an adequate pelvis, a “face to ubice” delivery occurs. When the conditions are unfavorable, an arrest occurs, which is called occipito-sacral arrest.
- Mechanism of “face to pubic” delivery:
- Descent: The descent continues until the root of the nose approaches the symphysis pubis.
- With flexion of the head The brow, vertex, and occiput emerge from the perineum and are born by face extension.
- Restitution: The head rotates 1/8 of a circle in the opposite direction of internal rotation, and the face is to the left of the mother in ROP and to the right in LOP.
- External rotation: The occiput rotates 1/8 of a circle in the same direction as restitution, and the face is to the left of the mother in ROP and to the right in LOP.
- External rotation: The occiput rotates 1/8 of a circle in the same direction as restitution, and the face is to the left of the mother in ROP and to the right in LOP.
- In persistent occipito-posterior, if it does not face to pubis on its own and goes into arrest, it is called occipito-sacral arrest.
Management:
Principles:
- Early diagnosis of occipito posterior position.
- Proper observation for the progress of labor.
- Provide proper and timely treatment to the patient.
- Diagnosis: Fetal heart sounds are not easily located due to the fetal back being on the flexion. If the membranes rupture early, perform an internal examination and assess for adequate pelvis.
- Early Cesarean Section: If the pelvis is inadequate, and there are obstetric complications such as pre-eclampsia, post-cesarean pregnancy, big baby, then a Cesarean section is required.
First Stage:
- In favorable circumstances, labor should be induced in the same manner as normal labor, but with certain precautions such as starting intravenous infusion to monitor labor progress due to the possibility of prolonged labor, and starting oxytocin infusion for labor stimulation in severe pain.
- Caesarean section is performed in unfavorable circumstances such as labor arrest, incoordinate uterine action, and fetal distress.
Second stage:
- Most often, delivery is spontaneous or by low forceps or ventouse due to anterior rotation of the occiput.
Unrotated and malrotated:
- If the condition of the fetus and mother is good, then continue continuous monitoring and watch for anterior rotation of the occiput and descent of the fetal head. In the occipito-sacral position, spontaneous face-to-pubic delivery can occur during this episode and deliver properly.
- Arrested occipito-posterior position: In this condition, perform abdominal and vaginal examination of the patient. When arrested in the occiput transverse or occiput oblique position, in suitable cases, vacuum extraction or manual rotation of the head is performed and forceps delivery is performed.
- In unsuitable cases, delivery is performed by cesarean section and craniotomy of the dead baby.
- Occitosacral arrest: If the head is engaged, the occiput is below the ischial spine, and a face-to-pubic delivery is performed using Keeland forceps in the unrotated head. If the occiput is at or above the ischial spine, a cesarean section is performed.
- Deep transverse arrest: If vaginal delivery is safe, forceps delivery is performed by a skilled obstetrician by manually rotating the ventouse or head with forceps application or rotation with forceps. If vaginal delivery is not safe, a cesarean section may be performed.
Third stage:
- To prevent postpartum hemorrhage, prophylactic intravenous ergometrine 0.25 mg should be given with delivery of the anterior solder. Observation for injury to the cervix and lower genital tract after vaginal operative delivery.
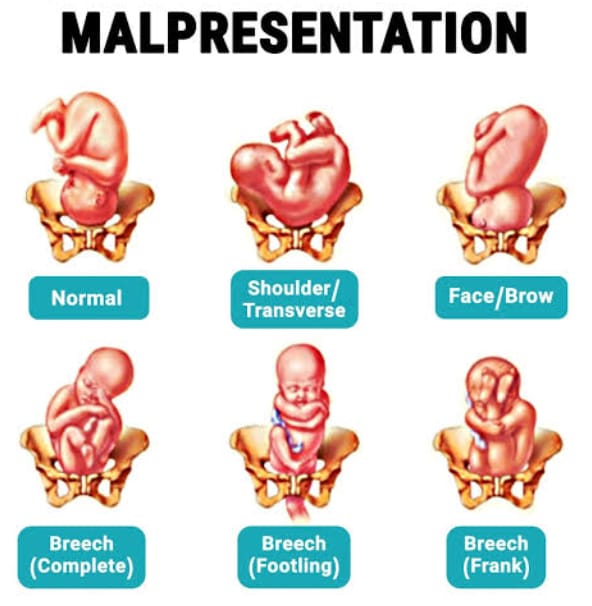
Malpresentation:
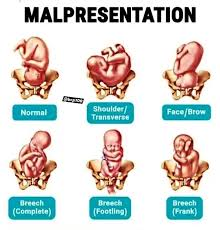
- Malpresentation is a condition in which any presentation other than the vertex as the presenting part during the intrauterine life of the fetus is called malpresentation.
- Breech presentation,
- Face presentation,
- Brow presentation,
- Solder Presentation,
- Compound Presentation.
Breech Presentation:
Definition:
- Breechpresentation a fits The most common malpresentation in the uterine cavity is in which the fetus lies longitudinally but the breech (buttocks) is the presenting part in the pelvic breech.
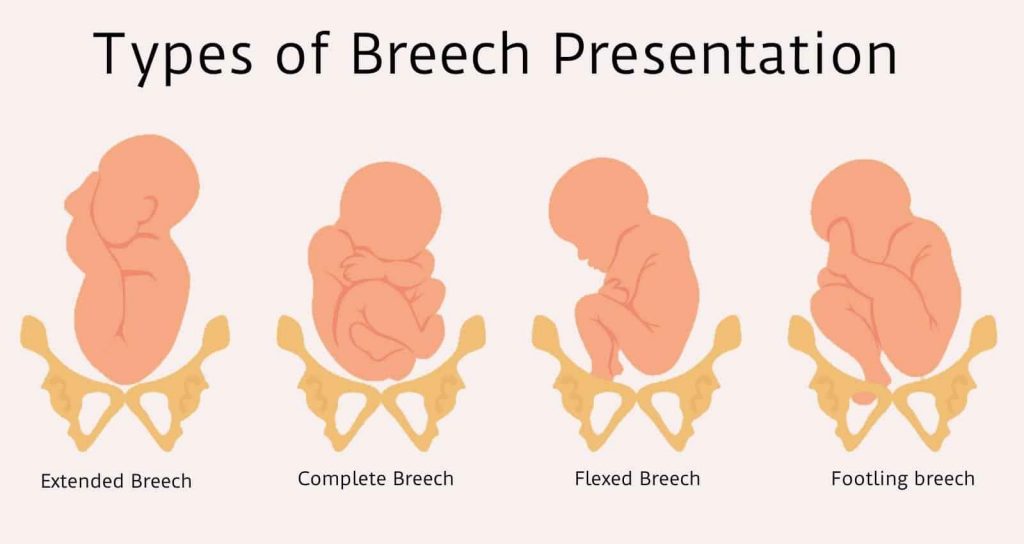
Attitudes/Classification/Variety of Breech Presentation:
There are two main types of breech presentation.
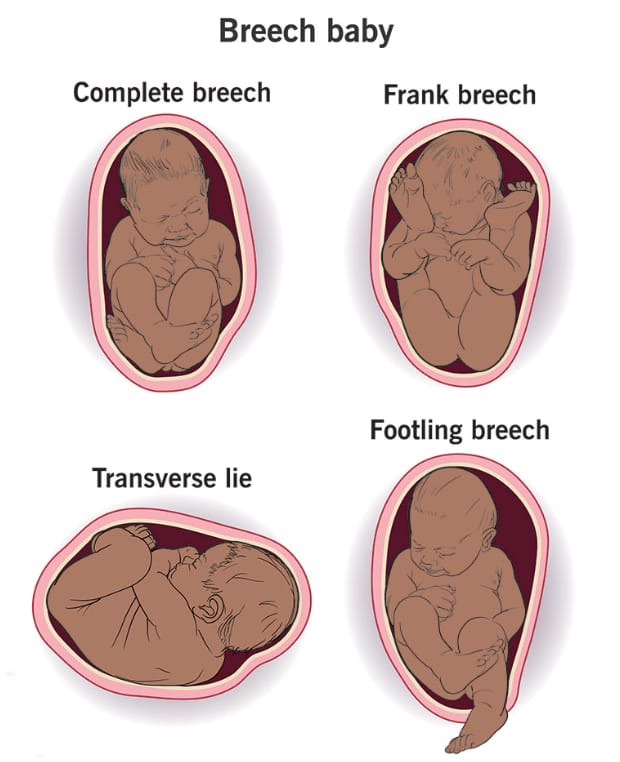
1) Complete (flexed breech),
2) Incomplete
There are three other types of incomplete.
a) Breech with extended legs (Frank Breech).
b) Footling presentation.
C) Ni presentation
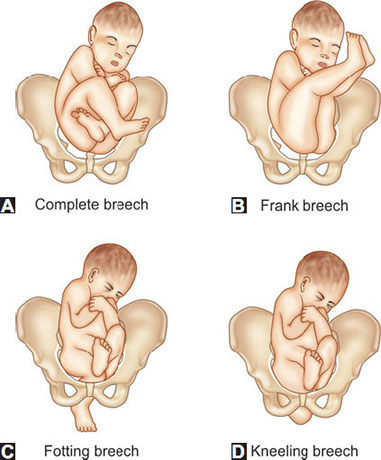
1) Complete (flexed breech),
- It maintains the normal attitude of full flexion. In complete breech, the legs of the fitter are bent at the ankles and the feet are bent at the knees and the feet are presented with the buttocks of the fitter. is.
- In which as a presenting part:
- 2 buttocks,
- External genitalia,
- The end is 2 feet.
2) Incomplete
In incomplete, the legs are extended to varying degrees in the podelic pole.
There are three other types of incomplete.
a) Breech with extended legs (Frank Breech).
b) Footling presentation.
C) Knee (Knee) presentation
a) Breech with Extended Legs (Frank Breech).
- In this condition, the legs of the fittest with breech are extended, i.e. the feet of the fittest are bent over the trunk of the fittest and the legs are straight from the knee (knee). The presenting part consists of 2 buttocks and external genitalia. This condition is more common (70%) in primigravida.
b) Footling presentation:
- In footling presentation, both the legs are partially extended, with one or both legs being the presenting part.
C) Knee Presentation:
- In knee presentation, the knee is extended but the knee is flexed, so the knee presents in a breezy position.
Etiology (Etiology):
Fault in passenger(fits):
- Incident, extended legs, prematurity,
- Twins,
- Hydrocephalus,
- Dead fetus.
Fault in passage (birth canal):
- Placenta previa,
Hydroamnios,
Oligohydroamnios,
Lack of tone of uterus and abdomen. - Maternal factors
Contracted pelvis,
Placental malformation,
Scanty like amniotic fluid,
Oligohydroamnios,
Uterine Abnormalities.
Diagnostic Evaluation:
History collection,
Physical examination,
Clinical,
Sonography,
Radiological
Clinical:
Fundal grip: If the head of the fetus is not part of the body, a hard globular mass is felt.
Head ballotment.
Lateral grip: The back side of the fetus is felt at one site and irregular extremities are felt at the other side.
Pelvic grip:
A soft broad and irregular mass-like structure is felt in the pelvic grip.
Fetal heart sound:
The fetal heart sound is heard in the umbilical region.
Vaginal examination of soft and irregular parts during pregnancy Fetal.
Sonography:
Sonography is used to confirm and confirm clinical diagnosis. If there is any congenital abnormality in the fetus, it can be identified.
In sonography, the gestational age of the fetus and its approximate weight are measured.
Radiology:
Radiology is done to confirm the diagnosis and to note the position of the head and limbs.
Mechanism of Labor:
In sacro anterior position
The principal movement occurs in three places.
1)Buttocks,
2)Solder,
3)Head.
1)Buttocks:
- The buttocks engage any one of the oblique diameters of the pelvis. Its engaging diameter is bi-trochanteric (10 cm) along the sacrum towards the iliopubic eminence. When the diameter passes through the pelvic brim, breech presentation is engaged. It continues to descend until the anterior buttocks touch the pelvic floor.
- Then the internal rotation of the anterior buttocks occurs 1/8th of a circle rotation behind the symphysis pubis. This is accompanied by lateral flexion of the trunk, leading to the descent of the trunk. And the anterior hip comes out first from under the symphysis pubis. Then the posterior hip is delivered.
- Then the trunk and lower limbs are delivered and restitution is done. In this, the buttocks are brought into the position where they were in the engaging oblique diameter.
Solder:
- Immediately after delivery of the buttocks and trunk, the bisacromial diameter (12 cm) is engaged in the same oblique diameter of the pelvis. The internal rotation of the solder occurs and it comes into the anterior-posterior diameter of the pelvic outlet. With this, the trunk is externally rotated 1/8th of a circle.
- Then, with anterior flexion of the delivered trunk, the posterior solder is delivered, followed by the anterior shoulder.
- In restitution, the trunk is untwisted, and in the left sacro anterior (LSA), the anterior solder turns right and in the right sacro anterior (RSA), it turns left.
- Then, the occiput is anteriorly rotated 1/8th of a circle, and the solder is delivered in the same direction. External rotation occurs.
- The fetal trunk now comes into a dorso anterior position.
Head:
- The suboccipitofrontal diameter of the head engages the opposite oblique diameter or transverse diameter of the buttock that was occupied.
- Flexion increases with descent. The occiput is internally rotated forward 1/8th or 2/8th of a circle and comes behind the symphysis pubis. The subocciput continues to descend until it comes below the symphysis pubis. Flexion of the head is delivered by the chin, mouth, forehead, vertex, occiput one after the other.
Management:
Assess the case for breech delivery, especially in primigravida, maternal age, complicating factors, baby’s size, pelvic capacity, CT scan,
M. Proper assessment of the I.I. Ultrasonography examination etc. is done.
When there is breech presentation, delivery is planned through two methods.
1) Elective Cesarean Section,
2) Spontaneous Labor and Vaginal Breech Delivery.
1) Elective Cesarean Section:
Indication: Big Baby,
Hyperextension of Head, Footling Presentation, or Pre When the weight at term is less than 1500 grams,
in obstetric or medical complications.
2) Spontaneous labor and vaginal breech delivery:
Indications:
Average fetal weight,
Flexed fetal head,
Adequate pelvis,
No obstetric or medical complications,
Emergency cesarean section and continuous labor monitoring available, and the presence of an experienced obstetrician.
Management of Vaginal Breech Delivery:
First Stage
Management is generally similar to normal labor except that if spontaneous labor begins, the chances of vaginal delivery increase. Pelvic assessment and vaginal examination should be performed after rupture of membranes to check for cord prolapse.
Start an intravenous line to the mother and provide Ringer lactated solution.
Do not give the mother for oral intake. Then send for blood group and cross matching.
Monitor the status of the fetus and progress of labor and provide oxytocin infusion for augmentation of labor.
Caesarean section should be indicated if there are any complications during the first labor, if labor does not progress, if there is fetal distress, if there is breech presentation or prolapse. There are three methods of vaginal breech delivery in the second stage: 1) Spontaneous 2) Assisted breech delivery is not the preferred method. 2) Assisted breech delivery is not the preferred method. –>
3) Breech extraction
In this, a small part of the fetus or the entire body is delivered by obstetricians. Since it causes trauma to the fetus and the mother, this method is rarely used.
Assisted Breech Delivery Breech delivery should be done only by a skilled obstetrician,
For that, an anesthetist, assistant instruments and suture material for the baby Resuscitation equipment should be kept ready by the neonatologist.
Steps
- When the anterior buttocks of the fetus are visible, place the patient on the labor table and when the buttocks distend the perineum, provide the patient with a lithotomy position.
Then perform antiseptic cleaning and empty the bladder through a catheter. - Give the patient a pudendal block. Episiotomy should be performed when the perineum is distended.
- Then advise the patient to apply bearing down efforts.
- Then the buttocks should be placed in flex breech position with the legs together and the fetus should not be touched until delivery up to the umbilical cord.
- After delivery of the trunk up to the umbilical cord, the umbilical cord should be taken downwards to one side. If the back is on the posterior side, rotate the trunk and bring it to the anterior side. Wrap the baby in a sterile towel. The twist prevents slippage and facilitates manipulation.
Delivery of Arms
- To prevent extension of the arms, the assistant should place his hand on the fundus and apply steady pressure during uterine contractions. When the scapula becomes visible, note the position of the hand. When the axilla becomes visible, deliver the arms one by one by simple locking with the fingers in each elbow and at that time, the baby’s lacunae Never pull from below to catch the fetus by covering it with a sterile towel.
Delivery of the After Coming Head
- The preferred time between delivery of the umbilicus to the mouth is five to ten minutes and is a crucial stretch. The following are common methods for delivery of the fetus:
1) Burn Marshall Method
- In this method, let the baby hang on its own weight and ask the assistant to apply suprapubic pressure in a downward and backward direction with his hands.
- So that there is more flexion of the head and a favorable diameter in the pelvic cavity, when the nape of the neck appears below the pubic arch, hold the baby between the two ankles with your fingers.
- Then keep the trunk in an upward and forward direction by keeping steady traction. During this time, hold the perineum with the left hand and let the face and brow be delivered one after the other. After the delivery of the mouth, remove the secretion from it with a mucus sucker. Depress the trunk for the delivery of the remaining head.
2) Forceps delivery
- After breech in forceps delivery For delivery of the coming head, the head should be in the pelvic cavity, in which ordinary forceps such as Das or specially designed piper forceps are used.
3) Malar flexion shoulder traction (modified Mauricio and Smiley weight technique):
- Keep the baby on the supinated left forearm and let the limb hang on both sides. Place the middle and index fingers of the left hand on the malleolus on both sides. This will maintain the flexion of the head.
- Then place the ring and little fingers of the pronated right hand on the baby’s right shoulder, index finger on the left shoulder and middle finger on the occipital region.
- Give traction in downward and backward directions until the nape of the neck is visible below the pubic arch. And the assistant should apply suprapubic pressure at that time to maintain flexion and maintain.
- Then the baby will be delivered by moving it in an upward and forward direction towards the mother’s abdomen, the face, brow and finally the trunk will be depressed to deliver the occiput and vertex.
- If the baby has asphyxia after delivery, resuscitate him immediately.
Face presentation (Face Presentation):
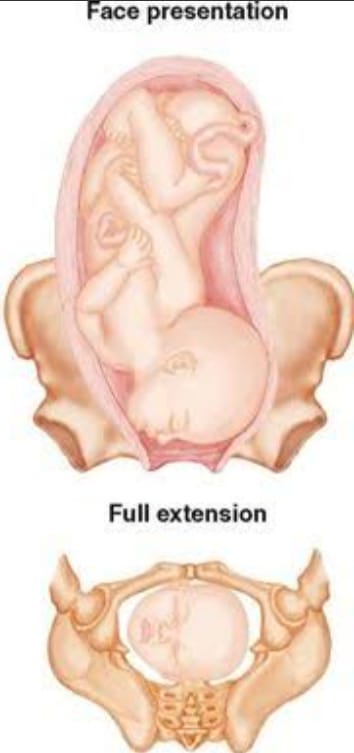
- Face presentation is a malpresentation of the fetus in the uterine cavity in which the lie of the fetus is longitudinal but with the chin as the presenting part while the head is in an attitude of complete extension.

Etiology:
- Fault in passage: Inlet contraction of the pelvis is important.
- Passenger Fault:
Large fetuses, pendulous abdomen in multipara
Favour breech presentation.
Malformed fetuses account for 15% of the incidence.
Anencephaly is usually in breech presentation. - Lateral oblique of the uterus is directed specifically towards the side towards which the occiput lies.
- Contracted pelvis is associated in about 40% of cases.
- Flat pelvis favors face presentation.
- The etiology of face presentation is not clear but associated factors such as multipara, contracted pelvis, flat pelvis, pelvic tumor and congenital malformations in the fetus, congenital goiter, cord twisting around the neck, increased tone of the extensor group in the neck muscles are seen in face presentation.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History taking,
Physical examination,
Diagnosis is sometimes done in late pregnancy and before labor.
Ultrasound to identify fetal presentation and fetal anomalies.
Clinically, vaginal examination helps to confirm breech presentation.
Abdominal Findings:
Inspection: Bulging of the flanks is not visible due to the S-shaped spine.
Palpation:
Mento anterior:
Lateral grip: Fetal limbs are anterior to the flank and back and palpation is difficult.
Pelvic grip: The head is large and does not engage, The side on which the back is located has a cephalic prominence, and the groove between the head and back is not prominent. - Auscultation: Fetal heart sounds are heard over the anterior chest wall on the limbus side.
- Vaginal examination: Vaginal examination should be performed gently, as eye injury may occur. The hard alveolar margin, nose malar eminence, supra orbital ridge, and mantum are palpated in the mouth.
- Sonography: Confirmation of diagnosis, Sonography is done to check the size of the fetus and congenital anomalies.
Mechanism of Labor:
- Engagement diameter is the diameter through the oblique diameter anterior or posterior to the brow.
- Engagement of the head is the mentovertical diameter.
- There is no mechanism of labor in an average-sized baby with a normal pelvis.
- The brow descends until it touches the pelvic floor.
- The hinge of the nose is at the symphysis pubis until internal rotation and descent down.
- The brow and vertex are followed by extension to deliver the face.
- There is no mechanism in the posterior brow position.
Management:
- The patient in breech presentation is referred to Level 2 care.
- If the patient has persistent breech presentation, cesarean section is considered the treatment of choice.
- Manual correction is rarely performed.
- If labor is obstructed and the baby is dead, craniotomy is performed.
- In the first stage, the diagnosis of breech presentation is made through abdominal and vaginal examination.
- Fetal size, malformations, and size of the pelvis are assessed.
- The partograph is properly maintained.
- A vaginal examination is performed when the membranes rupture to exclude a prolapsed cord. Care should be taken to avoid infection or injury to the eye during the examination.
- In case of cephalic disproportion or high risk pregnancy, a cesarean section is performed.
- The third stage is actively managed.
- The neonate is carefully and properly cared for.
- The throat is properly suctioned.
- The child is being properly oxygenated.
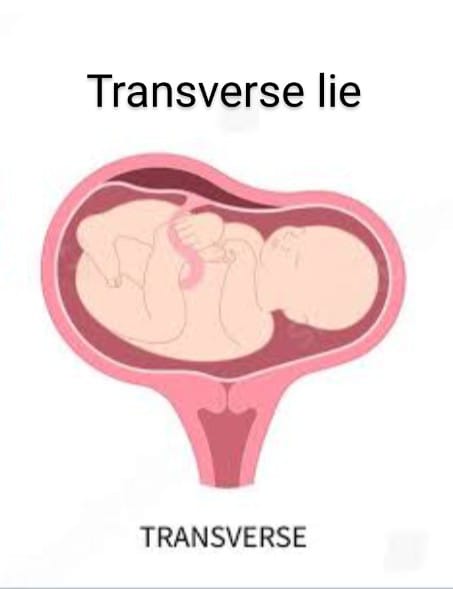
Transverse lie :
- “When the long axis of the fetus is horizontal to the axis of the mother’s spine or centralizes the uterus, it is called transverse lie”. Transverse lie is a serious complication in obstetrics. In transverse lie, the long axis of the fetus is in the mother’s crotch. And the solder is usually the presenting part. The fit is attached to the mother’s front or spine with its back. These positions are dorso-anterior and dorso-posterior.
Etiology:
- Multiparity: Lax and pendular abdomen, imperfect uterine tone, extreme uterine obliquity.
- Prematurity,
- Twins,
- Hydroamnios,
- Contracted pelvis,
- Placenta previa,
- Pelvic tumor,
- Congenital malformation of the uterus,
- Intrauterine death.
Diagnostic Evaluation :
- History Collection,
Physical Examination,
Abdominal Examination:
Inspection: The uterus appears broader and asymmetrical and the pear shape is not maintained.
Palpation: Fundal height is less than in the amenorrhea period.
Fundal grip: The fetal pole is not palpable.
Lateral grip: A soft, broad, and irregular breech is felt on one side of the midline and a smooth, hard, and globular head is felt on the other side. The head is usually placed at a lower level on an iliac fossa. - The back part is felt anteriorly on the long axis in the dorso-anterior part or irregular small parts are felt anteriorly in the dorso-posterior part.
- Pelvic grip: The lower pole of the uterus is emptied.
- Auscultation: F.H.S. is heard very easily below the umbilicus in the dorso-anterior position. Dorso-posteriorly, F.H.S. Located at a higher level.
- Sonar/X-ray
ultrasonography/radiography confirms the diagnosis. - Vaginal Examination:
- The presenting part is so high that it cannot be properly identified but some soft parts can be felt.
- The solder is identified by palpation
such as:
Acromion Processes
Scapula
Clavicle
Axilla
Ribs of the chest wall.
Management:
- During antenatal care, a woman identified as being in transverse lie is referred for Level II care by 34 weeks.
- In a Level II antenatal clinic, the diagnosis is clinically confirmed and its etiology is investigated.
- Quality antenatal care is provided every 2 weeks until 36 weeks and then weekly until term. She is admitted to the hospital from the 38th week.
- External cephalic version, like breech presentation, is performed after 37 weeks until early labor (20%).
- At the end of pregnancy (39-40 weeks), a cesarean section is performed.
- If it is transverse lie and with solder presentation before the membranes rupture, then external cephalic version is performed. If successful, then A.R.M. is performed. Then perform vertex vaginal delivery. If ECV fails, delivery is done by cesarean section.
- Caesarean section is performed in cases with high risk factors, i.e. placenta previa, uterine deformity, etc.
- Simultaneously the mother is referred to a level II care hospital in transverse lie.
- Caesarean section is performed if the fetus is live, mature with or without prolapse, or the orifice is completely or incompletely dilated.
- If the fetus is dead, a cesarean section is performed.
- If the fetus is small, dead, and deformed, an external pedicle version is performed and a breech delivery is performed.
- Sometimes decapitation and evisceration are also performed. Then the 3rd stage is actively managed.
Unstable lie :
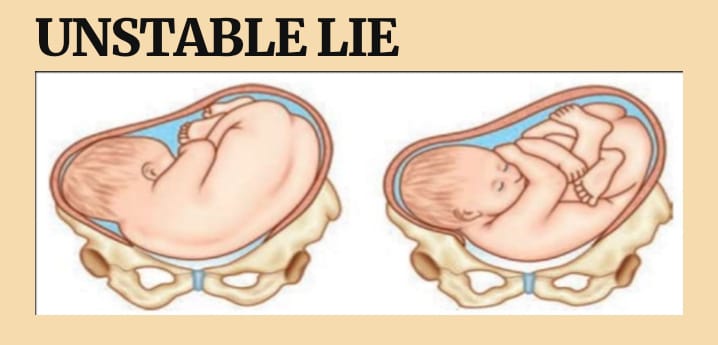
- “Unstable lie” is a condition where the fetus is not stable within the uterine cavity. “This is a condition where the presentation of the fetus continues to change continuously after the 36th week of pregnancy when it should be stable in the uterine cavity.” This word is used when.
- When the fetus is not in a continuously stable position in the uterine cavity and changes position frequently, which can complicate the labor process. An unstable lie can cause difficulties during delivery, as the fetus is not in the optimal position for a smooth birth. A fetus in an unstable lie requires careful monitoring and management to ensure a safe delivery.
Etiology:
- Excessive amniotic fluid (polyhydramnios),
- Inadequate amniotic fluid
- (oligohydramnios),
- Abnormal fetal presentation,
- Multiple pregnancy,
- Uterine anomalies,
- Abnormal uterine tone,
- Due to abnormal septation of the uterine cavity,
- Due to pelvic size and septation,
- Due to placental abnormalities,
- Increased activity of the fetus Due to,
- Reduced uterine tone with grand multipara and pendulous abdomen,
- Contacted pelvis,
- Pelvic tumor,
- Reduced muscle tone of uterine cavity due to multigravida.
Sign And Symptoms :
- Abnormal fetal position,
- Frequent changes in fetal position.
- Difficulties in palpating fetal position.
- Unusual and abnormal fetal heart rate pattern.
- Maternal discomfort and abnormal uterine contractions.
Diagnostic Evaluation:
- History collection,
- Physical Examination,
- Ultrasound imaging,
- Fetal heart rate monitoring,
- Abdominal palpation,
- Maternal history review,
- Pelvic examination.
Management:
- Properly check the presentation and lie of the mother during the antenatal period visit.
- External cephalic version is performed if not contraindicated.
- The patient should be admitted to the hospital only during 38 weeks of pregnancy.
- Proper investigation of the patient is done.
- These are to be excluded:
Placenta previa.
Contracted pelvis.
Congenital malformation of the fetus (to be done sonography).
In the presence of complicating factors (as above), elective caesarean section is performed. - In the absence of complicating factors, the patient is placed for induction and then ECV (external cephalic version) is done. If necessary, oxytocin drip is started Comes.
- After 1 hour, an internal examination is done to exclude cord presentation and then LRM (Low Rupture of Membranes) is done.
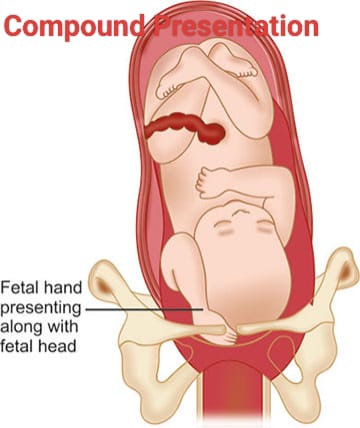
Compound Presentation:
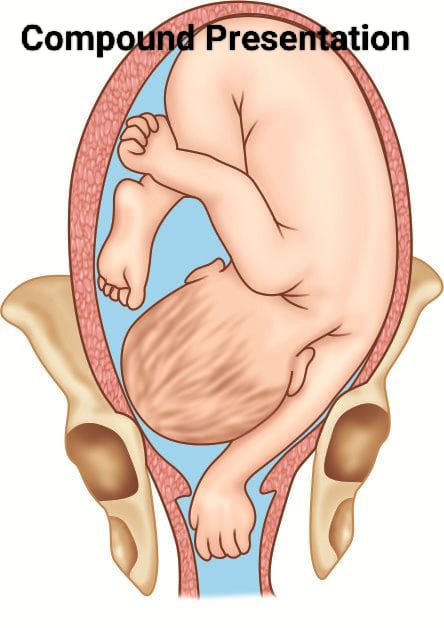
- When one or more fit extremities are present with the presenting part during intrauterine life, it is called compound presentation. When cephalic presentation is complicated by the presence of a hand or foot or both on the side of the head, or when one or both hands are present on the side of the breech, it is called compound presentation. In compound presentation, hands with head are the common presentation.
Etiology:
- Due to excessive amniotic fluid (polyhydroamnios),
- Due to multiple gestation,
- Uterine anomalies,
- Abnormal fetal presentation,
- Fetal hyperactivity,
- Inadequate uterine tone,
- Prematurity,
- Contracted pelvis,
- Pelvic tumor,
- Multiple pregnancy,
- Premature or Early ROM with High Head,
- Hydramenios
Sign And Symptoms:
- Abnormal fetal presentation.
- Labor progression becomes difficult and abnormal.
- Maternal discomfort increases.
- Fetal heart rate (FHR) becomes irregular.
- Complicated delivery or difficulties in engagement.
- Fetal hand and arm presentation.
Diagnostic Evaluation:
- History collection,
- Physical examination,
- Abdominal palpation,
- Fetal heart rate monitoring,
- Pelvic examination.
Management:
- Ultrasound to determine the position of the fetus Properly assessed.
- Manual rotation is done for proper repositioning of the fetus parts.
- Properly supportive care is provided to relieve maternal discomfort.
- Caesarean section is generally preferred in compound presentations.
- In case of dead fetuses, advice for destructive operation is provided.
- Forceps and vaginal deliveries are also performed in compound presentations but are generally considered high-risk.
Contracted Pelvis :
- Contracted pelvis is a condition in which the female bony pelvis is sufficiently abnormal in shape and size, due to which vaginal delivery remains difficult even in a normal size baby. That is, there are changes in the normal mechanism of labor. Which is called contracted pelvis. The female bony pelvis is divided into four sizes according to the shape of the inlet.
- 1. Gynecoid pelvis (round sep)( 50%),
- 2. Anthropoid pelvis (oval sep)( 25%),
- 3. Android pelvis (heart sep)( 20%),
- 4. Platypelloid pelvis (kidney sep)( 5%).
Etiology:
- Developmental factors: It can be due to hereditary or congenital factors.
- Such as,
- Nigel’s pelvis,
- Robert’s pelvis.
- Racial factors,
- Nutritional factors: Poor nutrition/malnutrition causes the condition of small pelvis.
- Hormonal factors: Excessive androgen secretion causes the condition of android pelvis.
- Metabolic factors: Such as rickets and osteomalacia.
- Trauma, diseases of bone or tumor: Fractures, tumors, tubercular arthritis, kyphosis, scoliosis, spondylolithiasis, coccygeal Deformity, poliomyelitis, hip joint disease.
Degree of contracted pelvis:
- 1.Minor degree or minor disproportion: Here the true conjugate is 9-10 cm. Vaginal delivery is possible.
- 2. Moderate degree or minor disproportion: Here true conjugate is 8-9 cm. Trial labor can be tried. And if it fails, then cesarean section is performed.
- 3. Severe degree or severe disproportion: Here true conjugate is less than 6 cm. It is considered preferable to perform a cesarean section.
Sign And Symptoms:
- Difficult Labor,
- Abnormal Fetal Presentation,
- Maternal Pelvic Pain,
- Frequent Urinary Tract Infection,
- Back Pain.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History collection,
- Physical examination,
- Imaging studies such as,
- X ray,
- Pelvic ultrasound,
- Computed tomography scan (CT scan),
- Magnetic resonance imaging (MRI),
- Pelvimetry,
- Clinical pelvic assessment.
Management :
The management of a contracted pelvis, which refers to a pelvis that is abnormally small and has an abnormal shape that can make the birth of a child difficult, requires careful assessment and intervention to ensure the safety of both the mother and child during labor and delivery.
1) Diagnosis and Assessment:
- Pelvimetry
Pelvimetry involves measuring the pelvis to assess its dimensions and shape. This measurement can be done clinically (external measurement) or radiologically (X-ray, MRI). - Take a complete history of the mother. Take a complete history of the mother to assess whether any difficulties have arisen in the mother previously at the time of delivery or at the time of cesarean delivery.
- Clinical evaluation of the mother Conduct a physical examination, which mostly includes pelvic measurements, which can properly assess whether the condition of the contracted pelvis is present or not.
2) Antenatal care:
- Early detection
- During the early period of pregnancy, through routine antenatal checkups or ultrasound examinations Early identification of contracted pelvis.
- Consultation
- If a woman has a high-risk pregnancy, she should be referred to an obstetrician specialist and a perinatologist for comprehensive management.
3) Labor management:
- Continuous Monitoring
- Closely monitor maternal and fetal conditions during labor, including proper monitoring of fetal heart rate and proper assessment of maternal vital signs.
- Labor Progress
- Continuously assess the labor process. If labor is slow or arrested, it indicates a condition of cephalopelvic disproportion.
- Positioning
- Providing the mother with proper position that provides optimal pelvic dimensions for labor progress.
4) Interventions During Labor:
- Artificial Rupture of Membranes
- If the membranes are in place and labor is progressing slowly, artificial rupture of membranes can be performed to improve the progress of labor.
- Oxytocin Infusion
- Provide oxytocin infusion to improve contractions and continuously monitor fetal and uterine contractions. Keep monitoring.
- Instrumental delivery:
- If the baby is in distress and vaginal delivery is possible, vacuum extraction or forceps delivery can be done.
5) Cesarean section:
- Indication
- When vaginal delivery is impossible, a cesarean section is performed to prevent any complications for the fetus and the mother.
- Timing
- When vaginal delivery is impossible, it is important to make a timely decision to perform a cesarean section to prevent any complications for the fetus and the mother.
6) Postpartum Care:
- Maternal Monitoring
- Close monitoring of the mother during the postpartum period can prevent any complications during the postpartum period such as conditions like postpartum hemorrhage.
- Neonatal Care
- Provide immediate newborn care after the birth of the newborn, especially when any complicated labor condition arises, to ensure that the newborn is properly well-being.
7) Counseling and Education:
- Education
- To educate the mother and her family members by providing them with complete information about the mother’s condition and the causes and interventions for its emergence.
- Future pregnancy planning
- Discuss the effect of a contracted pelvis on future pregnancy and delivery options.
8) Multidisciplinary Approach:
- Team Collaboration
- When there is a very complicated condition, all these specialists such as obstetricians, midwives, anesthetists, neonatologists should be available.
9) Psychological Support:
- The condition of contracted pelvis is stressful and emotionally challenging for the woman, so proper psychological support should be provided to the mother and family members.
- Thus, proper management of contracted pelvis is important to prevent complications for the mother and child.
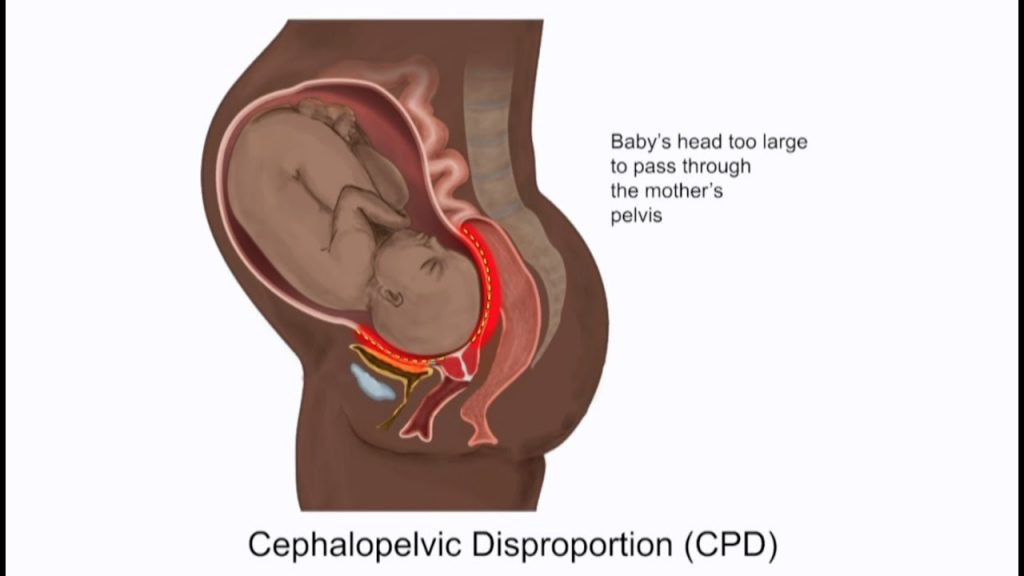
Cephalopelvic Disproportion (CPD):
Definition:
- The normal proportion between the size of the fetus and the pelvis is disturbed, which is called cephalopelvic disproportion (CPD). If there is a disparity (inequality) in the relationship between the fetal head and the maternal pelvis, this condition is called cephalopelvic disproportion (CPD). The disproportion can be either an average-sized baby with a small pelvis, or a big baby with a normal-sized pelvis, or a combination of both.
- In cephalopelvic disproportion (CPD),
- 1. Average-sized baby with a small pelvis.
- 2. Normal-sized baby with a big baby Baby.
- 3.The Combination of Both Factors.
Etiology :
- Large Baby:
- Hereditary Factor,
- Diabetes,
- Postmaturity,
- Multiparity.
- Abnormal Fetal Position.
- Contracted pelvis.
- Abnormally shaped pelvis.
- Fetal macrosomia,
- Abnormal fetal presentation,
- Hydrocephalus,
- Pelvic abnormality,
- Naturally small pelvis,
- Previous pelvic surgery,
- Ineffective uterine contractions,
- Prolonged labor,
- Genetic factors.
Sign And Symptoms (Sign And Symptoms):
- Difficult Labor,
- Prolonged Labor,
- Obstructed Labor,
- Abnormal Fetal Presentation,
- Fetal Distress,
- Abnormal fetal presentation,
- Maternal pelvic pain,
- Frequent urinary tract infection,
- Back pain.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History collection,
- Physical examination,
- Imaging studies such as,
- X ray,
- Pelvic ultrasound,
- Computed tomography scan (CT scan),
- Magnetic resonance imaging (MRI),
- Pelvimetry,
- Clinical pelvic assessment.
Management:
- Take a complete history of the mother Take a complete history of the mother to assess whether any difficulties have arisen in the mother previously at the time of delivery or at the time of cesarean delivery.
- Clinical Evaluation Complete physical examination of the mother, mostly pelvic measurements, due to which the condition of the contracted pelvis can be properly assessed.
- Pelvimetry
Pelvimetry measures the dimensions of the pelvis and its Measurements of the pelvis are performed to assess shape. This measurement can be done clinically (external measurement) or radiologically (X-ray, MRI).
Antenatal Care:
- Early Detection
Early identification of cephalopelvic disproportion through routine antenatal checkup or ultrasound examination during the early period of pregnancy. - Consultation
If a woman has a high-risk pregnancy, she should be referred to an obstetrician specialist for comprehensive management. Refer to a perinatologist. - Labor Management:
- Continuous Monitoring
Closely monitor maternal and fetal condition during labor, including proper monitoring of fetal heart rate and proper assessment of maternal vital signs. - Labor Progress
Continuously assess the labor process. If labor is slow or arrested, it indicates a condition of cephalopelvic disproportion. - Positioning
Provide the mother with proper position that provides optimal pelvic dimensions for labor progress. - Interventions During Labor:
- Artificial Rupture of Membranes
If the membranes are intact and labor is progressing slowly, artificial rupture of membranes can be performed to improve labor progress. - Oxytocin Infusion
Provide oxytocin infusion to improve contractions and continuously monitor the condition of the fetus and uterine contractions. - Instrumental delivery:
If the baby is in distress and vaginal delivery is possible, vacuum extraction or forceps delivery can be performed. - Caesarean section:
- Indications
Caesarean section when vaginal delivery is impossible is performed so that any complications that may occur to the fetus and the mother can be prevented. - Timing
When vaginal delivery is impossible, it is important to take the decision to perform a timely cesarean section so that complications that may occur to the fetus and the mother can be prevented. - Postpartum Care:
- Maternal Monitoring
Close monitoring of the mother during the postpartum period so that any complications that may occur during the postpartum period such as postpartum Conditions like hemorrhage can be prevented. - Neonatal Care
Providing immediate newborn care after the birth of the newborn, especially when any complicated labor condition arises, to ensure that the newborn is properly well-being. - Counseling and Education:
- Education
Education of the mother and her family members To educate them by providing complete information about the condition and the causes and interventions for its occurrence. - Future Pregnancy Planning
Discuss the effect of a contracted pelvis on future pregnancy and delivery options. - Multidisciplinary Approach:
- Team Collaboration
When there is a more complicated condition, obstetricians, midwives, anesthetists, neonatologists All specialists should be available. - Psychological support:
The condition of cephalopelvic disproportion is stressful and emotionally challenging for the woman, so proper psychological support should be provided to the mother and family members. - Thus, proper management of cephalopelvic disproportion is important to prevent complications for the mother and child.
Abnormal Uterine Actions:
Normal uterine action:
- In normal labor, coordinated uterine contractions progressively dilate the cervix and the fetal head descends, ultimately resulting in a successful vaginal delivery. The polarity of the uterus means that the upper segment of the uterus contracts and the lower segment relaxes. Normally, there are pacemakers on both upper sides of the uterus, due to which uterine contractions can occur properly.
- Now, abnormal uterine actions are such a condition in which the contraction of uterine muscles during labor changes from its normal frequency, duration, intensity, and pattern. This condition is called abnormal uterine actions. Due to these contractions, the condition of ineffective labor, prolonged labor can arise. When there is any deviation in the normal pattern of uterine contractions, it also affects the progress of labor, which It is called abnormal uterine actions. When there are any changes in the normal pattern of contractions and it affects the normal pattern of labor, it is called abnormal uterine action.
Type of the Abnormal Uterine Actions:
1.Hypotonic uterine action,
2.Hypertonic uterine action,
3.Uncoordinated uterine action,
4.Dysfunctional uterine action,
5.Prolonged uterine action.
1. Hypotonic uterine action: It involves weak and infrequent uterine contractions due to which effective cervical dilation cannot occur.
2. Hypertonic uterine action: It involves strong and frequent uterine contractions. Due to which uterine fatigue and labor process does not progress adequately.
3. In-coordinated uterine action: In this, there is dish organized uterine contraction in which the regular pattern of uterine contractions does not follow. Due to which the condition of ineffective labor progression arises.
4. Dysfunctional uterine action: In dysfunctional uterine action, hypotonic and hypertonic uterine action is involved. Due to which effective labor process cannot take place.
5. Prolonged uterine action: In this, uterine contractions are seen for a long duration, due to which fetal distress and uterine rupture can also occur.
Etiology:
- Uterine muscle fatigue,
- Hormonal imbalance (Ex: oxytocin),
- Uterine abnormality (Ex: fibroid, congenital anomalies),
- Fetal factors (macrosomia, abnormal presentation),
- Inadequate maternal pelvic size,
- Medication effects
- (analgesic, anesthetic)
- Dehydration, electrolyte imbalance,
- Previas uterus Surgery (scarring, adhesions),
- Emotional stress and anxiety,
- Infection and inflammatory conditions (chorioamnionitis),
- Multiple gestation (twins),
- Maternal health conditions (e.g. diabetes, hypertension),
- Nutritional deficiency (Essential vitamins and minerals in adequate amounts).
- Elderly primi gravida,
- Prolonged pregnancy,
- Fibroids,
- Emotional factors,
- Constitutional factors,
- Contracted pelvis,
- Malpresentation,
- Due to improper use of drugs such as sedatives, analgesics, and oxytocins,
- Premature attempt at vaginal delivery and instrumental vaginal delivery under light anesthesia.
- Advanced age of the mother Due to,
- Prolonged pregnancy.
Sign And Symptoms:
- Prolonged labor.
- Ineffective uterine contractions,
- Weak and infrequent uterine contractions,
- Fetal distress,
- Changes in fetal heart rate pattern,
- Maternal discomfort and pain,
- Failure to progress labor and cervical dilation,
Diagnostic Evaluation (Diagnostic Evaluation) :
- History Taking,
- Physical Examination,
- Fetal Monitoring,
- Uterine Monitoring,
- Ultrasound,
- Laboratory tests
Management:
Assessment and monitoring:
Continuous Fetal Monitoring:
- Continuous monitoring of the fetus. Assessing the well-being of the fetus. Properly assessing for any signs and symptoms of fetal distress.
- Regular maternal assessment: Properly monitoring the mother’s vital signs and assessing uterine contractions. Properly assess the condition of the mother’s cervical dilation.
During Labor Support:
- Hydration: Advise the mother to consume adequate amounts of water to prevent dehydration. Which plays an important role in affecting uterine function.
- Pain Management: Provide adequate amount of labor and a comfortable environment to relieve the mother’s pain and provide epidural analgesia to the mother. Due to which the discomfort during labor can be removed.
Positioning and Mobility:
- Anchorage Maternal Movement: Advise the mother to walk properly. Due to which uterine contractions can occur properly. And can be delivered easily.
Medication:
- Oxytocin administration: When uterine contractions are slow, hypotonic or ineffective, oxytocin should be administered to increase the frequency of uterine contractions.
- Tocolytic: When uterine contractions are slow, hypotonic or ineffective, oxytocin should be administered to increase the frequency of uterine contractions.
Mechanical Intervention:
- Amniotomy: Artificial rupture of membranes to enhance labor progress when labor is intact.
Surgical Intervention:
- Caesarean Delivery: If the labor process has failed and there is a condition of fetal distress, a caesarean delivery is required.
Postpartum Care:
- Monitoring for Recovery:
Properly assessing if there are any complications after delivery. - Counseling: Providing support and information for future pregnancies. Assess the potential risk of abnormal uterine actions.
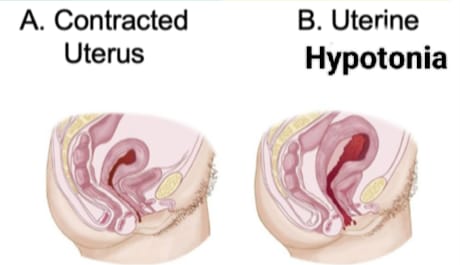
Uterine Inertia (uterine hypotonia/uterine inertia) :

- Uterine hypotonia condition also called uterine inertia is characterized by low or poor tone in the muscle fibers of the uterine cavity. This results in weak contractions of the uterine cavity which are infrequent and not very painful. Therefore, cervical dilation occurs slowly and the labor process usually lasts for a prolonged period. Uterine inertia is a common type of uterine dysfunction but is less serious and occurs early or later in labor.
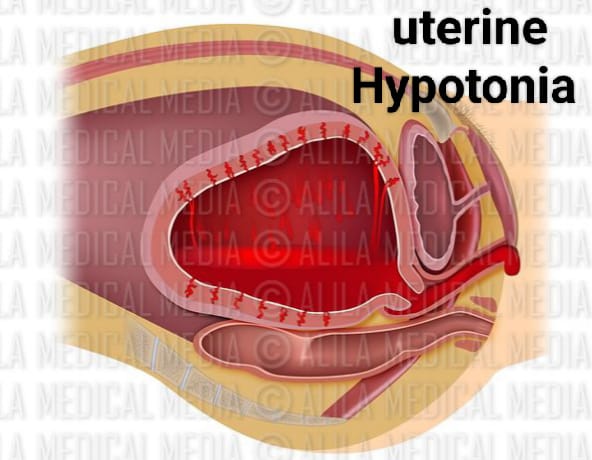
In uterine inertia, the normal pattern of uterine contractions is maintained to a lesser extent. And the intrauterine pressure remains below 25 mm of Hg during contractions. The intensity and duration of contractions decrease and the relaxation and interval between contractions increase.
Types of Uterine Inertia:
Uterine inertia is generally of two types:
1.Primary Uterine Inertia
2.Secondary Uterine Inertia.
1.Primary Uterine Inertia: Primary uterine inertia is usually when the uterus is unable to contract effectively during the onset of labor. The condition of inertia arises. This condition can usually be caused by maternal fatigue and hormonal imbalance.
2. Secondary Uterine Inertia: This type usually arises after the onset of initial effective contractions. Which are usually weak and can be caused by maternal exhaustion, fetal position issues and obstructions.
Sign And Symptoms :
- There is less pain during contractions.
- The uterus becomes less hard and the peak level of pain also fills the uterine wall.
- After contractions, the uterus becomes normal.
- The fetal heart sound (FHS) is normal and the fetal parts are well palpable.
- Uterine The intensity of contractions is diminished.
- The duration of uterine contractions is short.
- There is a good amount of relaxation between contractions.
- The interval increases.
- The general pattern of uterine contractions of labor is maintained.
- The member is intubated and the There is also evidence of cervical dilatation and a contracted pelvis, malposition, deflected head, or breech presentation.
Diagnostic Evaluation:
- History collection,
Physical examination, - Diagnosis is usually clinical Features and associated factors such as:
contracted pelvis,
malposition,
deflexed head,
malpresentation etc.
Pelvic examination,
ultrasound,
maternal history review,
labor progress monitoring,
laboratory tests.
Management:
- Provide the mother with a proper left lateral position and advise the mother to avoid the supine position.
- Carefully evaluate the mother’s condition.
- Properly assess whether the patient is in labor.
- Properly assess whether the patient is in labor through abdominal and pelvic examination for cephalopelvic disproportion or breech presentation.
- Properly catheterize for bladder emptying.
- Properly start the patient’s I.V. line to maintain hydration.
- Provide intra-muscular (I.M.) pethidine to relieve the patient’s pain.
- Perform artificial rupture of membranes (ARM) to increase contractility and start an oxytocin drip.
- If If uterine contractions do not increase even after starting the oxytocin drip, then a cesarean section is preferred.
- A cesarean section is planned in the following cases such as contracted pelvis, breech presentation and fetal and maternal distress.
- In vaginal delivery, increase the patient’s moral support and change the patient’s posture, avoiding the supine position and advising the mother to properly empty the bladder and if unable to empty, catheterization and intrauterine device should be used. Provide amniotic fluid and provide analgesics.
- Continuously monitor fetal heart sound (FHS).
- Continuously monitor the mother’s condition.
- Properly assess the condition of the mother and the baby after delivery.
- Properly provide reassurance to the mother after delivery.
- Provide the mother with proper work and quiet environment and advise her to take proper rest.
Incoordinated uterine action/abnormal polarity (Incoordinated uterine action/abnormal polarity) :
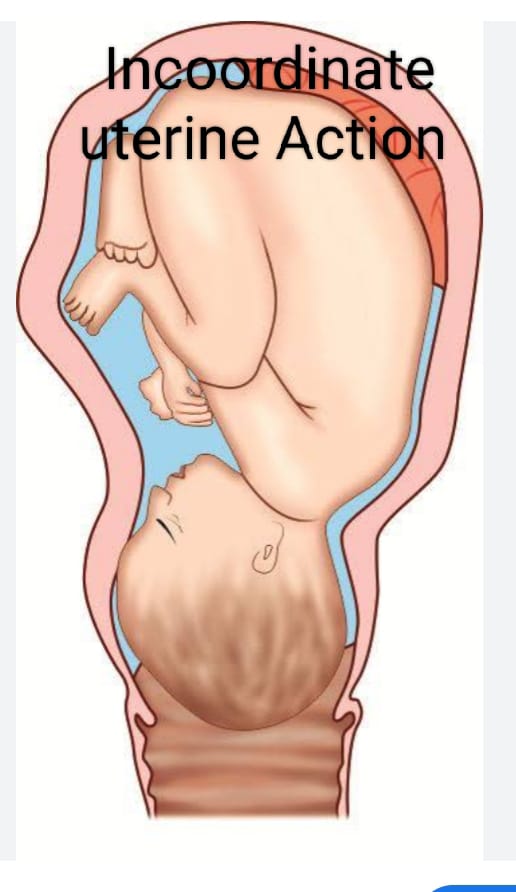
- Incoordinated uterine action is defined as irregular, ineffective, or poorly coordinated contractions of the uterine cavity. Unlike normal contractions, which are rhythmic and help in cervical dilation and descent of the fetus, incoordinated uterine action of the uterus can lead to prolonged labor and complications.
- This condition can be caused by factors such as hormonal imbalance, maternal stress, or previous uterine surgery. Incoordinated uterine action is a type of abnormal uterine action that occurs when the upper and lower parts of the uterine cavity cannot work in a coordinated manner. This can lead to a condition of long, difficult, and prolonged labor.
- These incoordinate uterine actions are mostly seen in the active stage of labor. In these, conditions like spastic lower uterine segment, colicky uterus, asymmetrical uterine contraction, constricting ring, generalized tonic contraction of uterus, cervical dystocia, due to which a hypertonic state arises in the uterus, which is called incoordinate uterine actions.
Etiology (Etiology):
- Due to hormonal imbalance,
- Due to structural abnormality of the uterine cavity,
- Due to abnormality in pelvic shape and size,
- Maternal factors such as stress, fatigue, anxiety, affect the pattern of contractions.
- Due to scar formation from previous surgery such as cesarean section or myomectomy.
- Medication: Due to overuse of uterotonics and other medications.
- Due to malposition of fetus: Which affects labor progress.
- Fetal position: Malpresentation of fetus affects labor process.
- Fetal position: Malpresentation of fetus affects labor process.
- Due to multiple gestation.
Sign And Symptoms Signs and Symptoms:
- Irregular uterine contractions,
- Ineffective labor progression,
- Prolonged Labor,
- Fetal distress,
- Maternal discomfort,
- Increased uterine tone,
- Failure to progress labor.
Diagnostic Evaluation (Diagnostic Evaluation) Evaluation) :
- History Collection,
- Physical Examination,
- Cervical Examination,
- Fetal Heart Rate Monitoring,
- Ultrasound,
- Pelvic Examination,
- Laboratory tests,
- Bishop score assessment.
Management:
- Provide proper position to mother.
- Mother Carefully evaluate the condition of the patient.
- Properly assess whether the patient is in labor.
- Properly assess whether the patient is in labor through abdominal and pelvic examination for cephalopelvic disproportion or breech presentation.
- Properly catheterize for bladder emptying.
- Properly connect the patient to an IV line to maintain hydration. Start.
- Provide intra-muscularly (I.M.) pethidine to relieve the patient’s pain.
- To increase the contractility, perform artificial rupture of membranes (ARM) and start oxytocin drip.
- If uterine contractions do not increase even after starting oxytocin drip, then cesarean section is preferred.
- The following cases Cesarean section is planned in conditions such as contracted pelvis, breech presentation and fetal and maternal distress.
- Increase moral support of the patient in vaginal delivery and change the patient’s posture to avoid supine position and advise the mother to properly empty the bladder and if unable to empty then catheterize and provide intravenous fluids and analgesics to the woman.
- Continuous monitoring of fetal heart sound (FHS) To do.
- Continuously monitor the mother’s condition.
- Properly assess the condition of the mother and the baby after delivery.
- Properly provide reassurance to the mother after delivery.
- Provide the mother with proper work and quiet environment and advise her to take proper rest.
Types of Incoordinated Uterine Contractions :
- Incoordinated uterine contractions are of the following types, such as,
- 1) Spastic lower segment,
2) Constriction ring or contraction ring or Schroder’s ring,
3) Cervical dystocia,
4) Generalized tonic contraction or uterine tetany,
5) Tonic uterine contraction and retraction or Bandels ring.
Spastic Lower Segment:
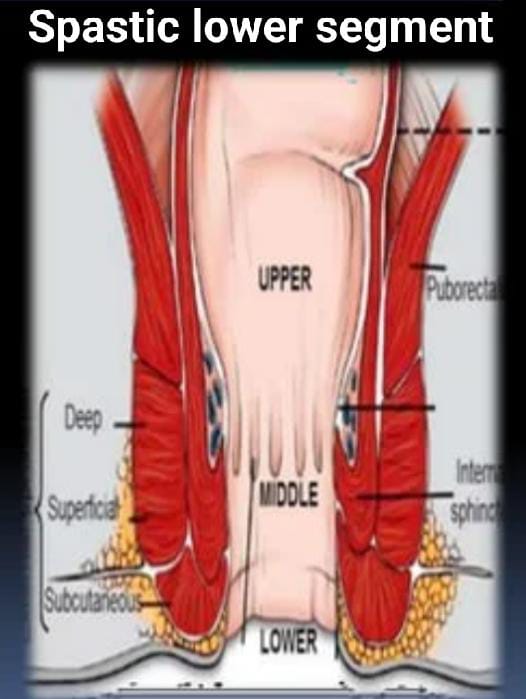
- Spastic lower segment of uncoordinated uterine contractions In this type of fundal domain, the fundal domain is reduced and the polarity is reversed. The pacemaker does not work in a proper rhythm and the contractions of the lower segment become strong. In this, there is inadequate relaxation between two contractions. And the basal tone is raised above 20 mm Hg. Also, fetal distress occurs.
- Characteristics of spastic lower segment:
- 1) Fundal domain: low,
2) Polarity: reversed,
3) Inadequate relaxation between two contractions,
4) Basal tone: raised above 20 mm Hg.
Etiology (Etiology):
- Uterine muscle fatigue: Prolonged and excessive contractions can cause spasms.
- Maternal factors: Conditions such as dehydration, electrolyte imbalance, and fatigue.
- Fetal factors: Large fetal size or abnormal presentation can increase pressure.
- Pelvic Abnormality: Pelvic abnormalities or contractures can increase pressure.
- Hormonal influences: Uterine tone can be affected due to imbalance of oxytocin and other hormones.
- Psychological factors: Muscle tension can increase due to stress and anxiety.
Sign And Symptoms Symptoms):
- Unbearable pain occurs which is referred to the back.
- Dehydration due to fatigue.
- Bladder becomes distended due to retention of urine.
- Stomach and bowel become distended.
- Uterine There is excessive hardening of the uterine cavity in the abdomen with pain before and after contractions.
- The uterus remains tender and tense even after the contractions have passed.
- The vaginal parts become difficult to palpate.
- The cervix becomes thick and edematous and hangs like a curtain.
- Various degrees of caput succedaneum may occur.
- The cervix may not dilate appropriately.
- There is a risk of fetal distress due to imperfect relaxation between contractions. Placental insufficiency may also cause distress.
Diagnostic Evaluation:
- History collection,
- Physical examination,
- Diagnosis is usually made based on clinical signs and symptoms.
- The patient experiences excruciating pain that may involve the back.
- Evidence of ketoacidosis and dehydration may also be seen. is.
- The bladder is frequently distended. There is retention of urine and distension of the stomach and the gut is visible.
- Premature attempts at a beer down are made.
- On palpating the abdomen:
- The uterus feels tender,
- gently Manipulation stimulates the hardening of the uterine cavity with pain which further starts uterine contractions.
- Fetal parts become difficult to palpate.
- Fetal distress appears early.
- During internal examination: Cervix which is thick, edematous, hangs loosely like a curtain and does not apply well to the presenting part.
- Inappropriate dilation of the cervix occurs.
- Abscesses of the membranes are seen.
- Meconium stained liquor may be present.
Management:
- Proper treatment of the patient Provide careful evaluation of the mother.
- Start the patient on an intravenous line. Then, correct the patient’s dehydration and ketoacidosis condition by rapid infusion of Ringer’s lactate (RL) solution.
- Provide medication as prescribed if the patient has a pain condition.
- Properly assess the general condition of the mother and fetus.
- Continuously monitor the fetal heart rate (FHR) and report any changes immediately.
- Provide proper psychological support to the woman.
- If there are conditions like malpresentation, contracted pelvis, maternal distress, fetal distress etc. then inform the patient to perform an urgent caesarean section.
- Before caesarean section, do a rapid 5% dextrose infusion to correct the mother’s dehydration and ketoacidosis condition.
- In a conservative approach,
- Advise the mother to take adequate rest.
- Sedate her with Inj like Inj. Pethidine 100 mg + Inj. Aspirin 50 mg I/M.
- Provide epidural analgesia if preferable.
- Maintain the nutritional status of the mother properly with 5% dextrose drip.
- Watch the fetus carefully.
Avoid oxytocin drip. - Provide proper psychological support to the woman and record and report properly.
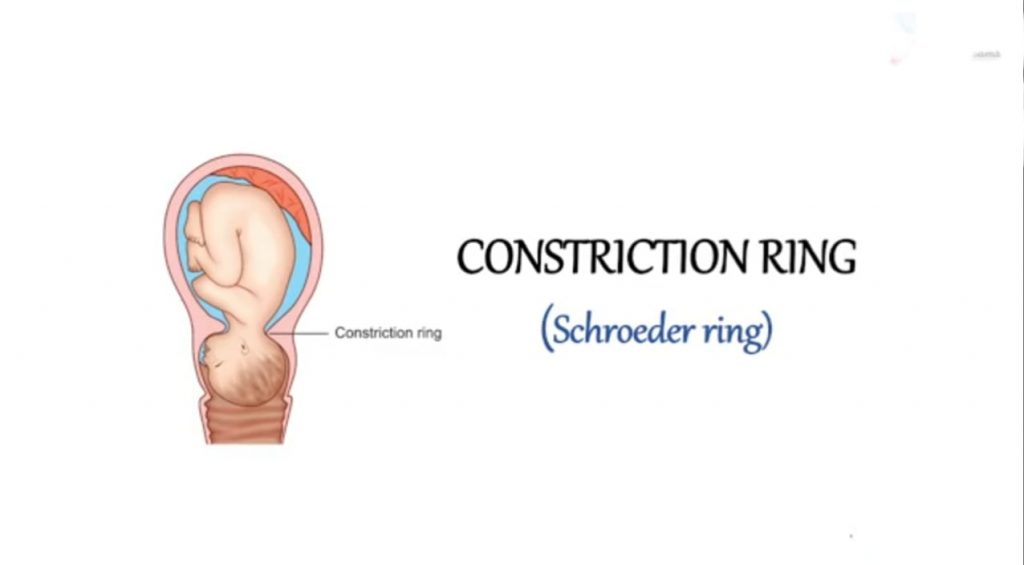
Constriction ring or contraction ring or Schroeders ring (Constriction ring or contraction ring or Schroeders ring) :
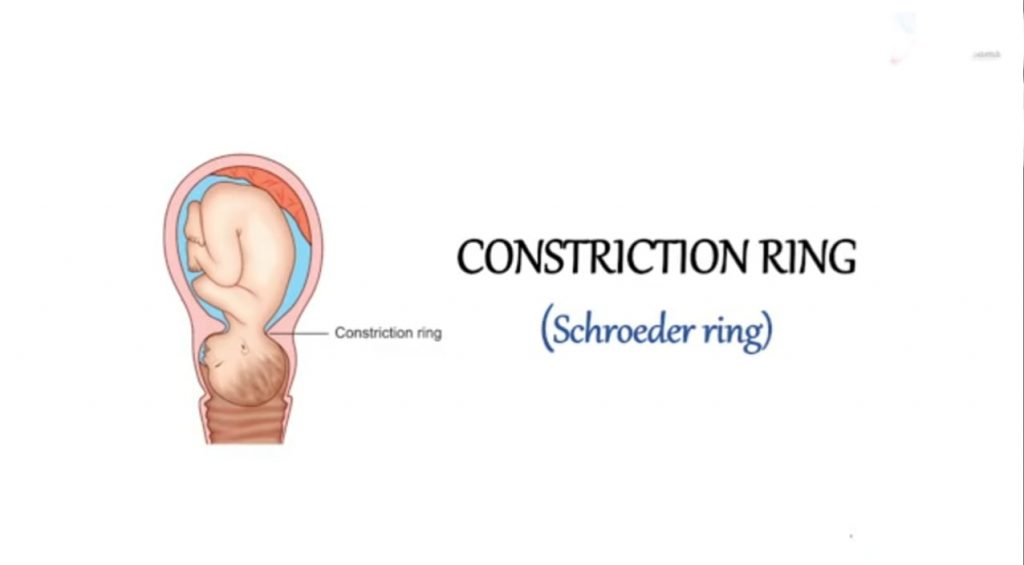
- A constriction ring is a form of uncoordinated uterine action where the constriction ring is formed during the 1st, 2nd and 3rd stages of labor due to localized spasm of the uterine muscles and at the junction of the upper and lower parts of the uterus. The ring of circular muscle fibers of the uterus is caused by localized spastic contractions. The constriction ring is situated at the junction of the upper and lower parts of the uterus around the constricted part of the uterus. As seen in the neck part in vertex presentation.

Location of Ring:
- The constriction ring is located around the junction of the upper and lower segments of the uterus. On the constricted part of the fetus and around the neck in cephalic presentation.
- It can be seen in all stages of labor.
It is usually reversible and complete.
Etiology:
- The exact cause is unknown. is.
- But in the associated etiology,
- malpresentation,
- malposition,
- due to rough and repeated intrauterine manipulation,
- due to improper use of uterine stimulants such as oxytocin infusion.
- Due to premature rupture of membranes.
- Due to premature attempt of instrumental delivery under light anesthesia.
- History Collection,
Physical Examination, - Constriction ring frequently precedes colicky uterus and the patient is usually primigravida.
- It is diagnosed by vaginal examination and by filling the uterine cavity with a hand inserted into it.
- It is suspected when the 2nd stage is prolonged for no apparent reason.
- In the 3rd stage, it is due to retained placenta and May cause uterine contractions with postpartum hemorrhage.
- The ring is not felt on the abdomen and is at risk of rupture due to the hypertonic state but the uterus does not rupture. It is seen in first stage of cesarean section, second stage of forceps application and third stage of manual removal (hourglass contractions).
- Properly assess the child for any breech presentation and malposition or disproportion.
- Provide the patient with analgesics such as pethidine and antispasmodics such as hyoscine.
- Treatment usually depends on the stage of labor.
Diagnostic Evaluation:
Management:
1st Stage:
- In the 1st stage, the diagnosis is made during C.S. after opening the uterine cavity. Therefore, the ring may have to be cut vertically to deliver the baby.
2nd Stage:
- During the second stage of labor, despite correct and judicious application of forceps, if the head fails to deliver, suspicion of constriction ring arises.
- The forceps blade After removal, the ring is confirmed by palpating.
- At this stage, a cesarean section is also performed. Otherwise, forceps are applied again.
- After applying the forceps, 0.5 ml of 1 in 1000 adrenaline hydrochloride is administered subcutaneously.
- Alternatively, 2 capsules of amyl nitrate are broken and inhaled.
- If If any of these measures fail to relax the ring, the patient may be provided with general anesthesia to complete the forceps delivery.
3rd Stage:
- Diagnosis is made during an attempt at manual removal.
- Planning anesthesia deep is usually effective. is.
- Alternatively adrenaline/amyl nitrate can be given.
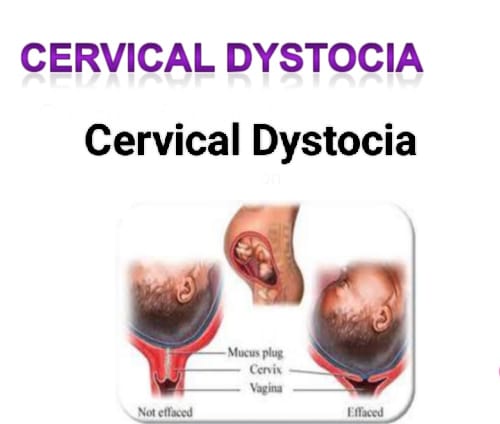
Cervical dystocia (Cervical Dystocia):
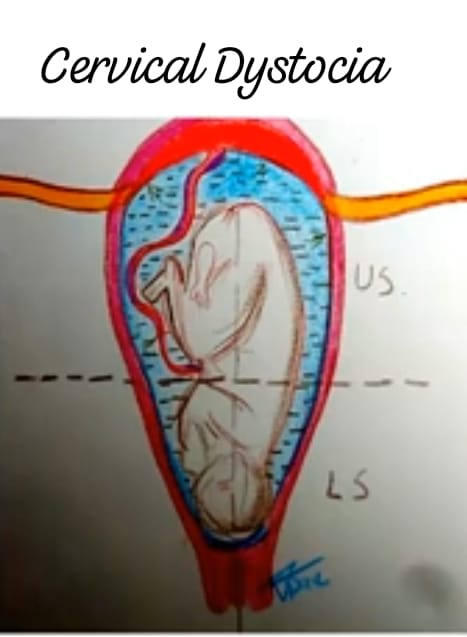
- Cervical dystocia is a condition where strong, regular uterine contractions are present but the cervix fails to dilate within a reasonable time, which can lead to difficulties in the labor process, which can lead to cervical dilation. Dystocia is called. Cervical dystocia is a condition in which cervical dilation does not progress properly due to inefficient uterine contractions, malpresentation, malposition, and spasms in the cervix.
Types of cervical dystocia (Types of cervical dystocia):
Generally, there are two types of cervical dystocia, such as,
1) Primary cervical dystocia,
2) Secondary cervical dystocia.
1) Primary Cervical Dystocia: Primary cervical dystocia usually occurs during the first child birth in which the normal pattern of uterine contractions is maintained but the external orifice fails to dilate.
In primary cervical dystocia,
the cervix is very thin and the head cannot be applied properly.
Initially uterine contractions are good but ultimately they become ineffective.
The anterior lobe is in the AD.
In this case, delivery may be accomplished by avulsion of the anterior lobe or by annular detachment of the cervix.
2) Secondary Cervical Dystocia: Secondary cervical dystocia is usually caused by scarring or rigidity of the cervix, cervical cancer, or the effects of a previous operation or delivery.
Sign And Symptoms:
- Prolonged labor,
- Failure to dilate the cervix despite good uterine contractions,
- Ineffective uterine contractions,
- Abnormal fetal positioning,
- Maternal discomfort such as pain and increased pressure in the pelvis.
- Fetal Distress.
Diagnostic Evaluation:
- History collection,
- Physical examination,
- Pelvic examination,
- Fetal monitoring,
- Ultrasound,
- Laboratory tests,
- Bishops score assessment.
Management:
- If there are complications with cervical dystocia, a cesarean section is performed.
- If the head is low down and the thin rim is behind the cervix, the rim can be manually vented and moved up during contractions or traction, or if the cervix is thin but half-dilated, forceps or ventouse extraction should be performed by placing the Duhrsense incision at the 2 and 10 o’clock positions.
- If the cervix is stenosis due to fibrosis and fails to dilate properly in a reasonable time and vaginal If delivery fails, a cesarean section is performed.
- If there is obstruction of the cervix, then a cesarean section is said to be the preferred method.
- The patient should be given analgesics such as pethidine and antispasmodics such as hyoscine medication.
- If the cervix is not properly dilated and there is a condition of fetal distress and the fetal head is not properly engaged, then a cesarean section is performed.
Generalized Tonic Contraction or Uterine tetany :
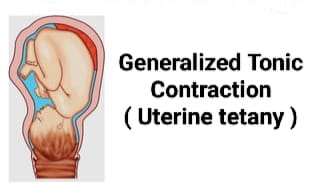
- Generalized tonic contractions refer to uterine tetany which is characterized by extremely prolonged (prolonged) uterine contractions. In this condition, the entire uterine cavity is retracted up to the level of the internal os.
- There is no physiological differentiation between the active upper uterine segment and the passive lower uterine segment.
- When uterine contractions cease, the entire uterus undergoes muscular spasm (tonic) holding the fetus within the uterine cavity.
Uterine tetany causes active retention of the fetus.
Etiology:
- Failure to remove obstructions by powerful contractions of the uterus.
- Irritation due to repeated unsuccessful attempts at artificial delivery.
- Improper use of oxytocin drugs.
Sign And Symptoms:
- Severe and continuous pain.
- The uterus becomes tense, hard, and small in size.
- Vital parts do not feel properly.
- Fetal heart sounds are not audible.
- Head is observed during vaginal examination.
- Vagina is edematous.
- Dehydration and ketoacidosis occur.
- On abdominal examination, the uterus is smaller in size, feels tense and tender.
- F.H.S. should not be audible.
- Vaginal Examination:
- Vagina should be dry and edematous.
Nursing Management:
- Correct dehydration and ketoacidosis by IV infusion of the patient.
- Provide antibiotics to control infection.
- Provide sedatives to relieve pain.
- If obstruction is suspected, cesarean section is performed.
- Deeply sedate the patient with intramuscular morphine for 15 mg or provide pethidine drip. i.e. 200 mg in 500 ml 5% dextrose at a rate of 50-60 drops per minute.
- Advise the patient to take adequate rest.
- The patient is given rest, when spontaneous delivery is possible or if there are no obstructions, spontaneous delivery is performed.
Tonic uterine contractions and retraction or bandles ring (Tonic uterine contractions and retraction or bandles ring) :
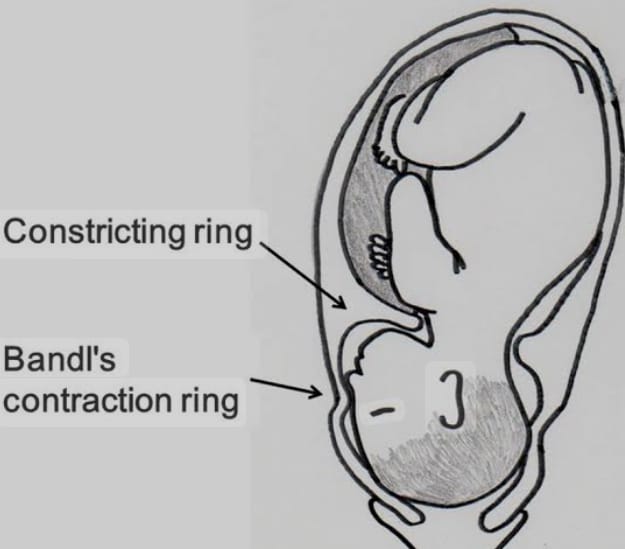
- A bandle’s ring is usually applied to the retraction ring, which is usually visible on the abdomen. A bandle’s ring causes uterine contractions due to obstructed labor. This is a transverse groove (depressed ridge) that usually occurs between the umbilicus and the symphysis pubis. It usually corresponds to the upper uterine segment and the lower uterine segment, which are usually visible on the abdomen. It can usually arise in the condition of obstructed labor and difficult labor. Bandlesian ring is usually an abnormal junction between two segments of the uterus. It is usually called a late sign of obstructed labor.
- How does the formation of the ring take place:
- There is a gradual increase in the intensity, duration and frequency of uterine contractions.
- The relaxation phase is less frequent and ultimately a state of tonic contraction develops.
- The retraction is usually continuous.
- In the 1st stage, the already thinned lower segment elongates through circumferential dilatation and progressively thins to accommodate the forces driven from the upper segment.
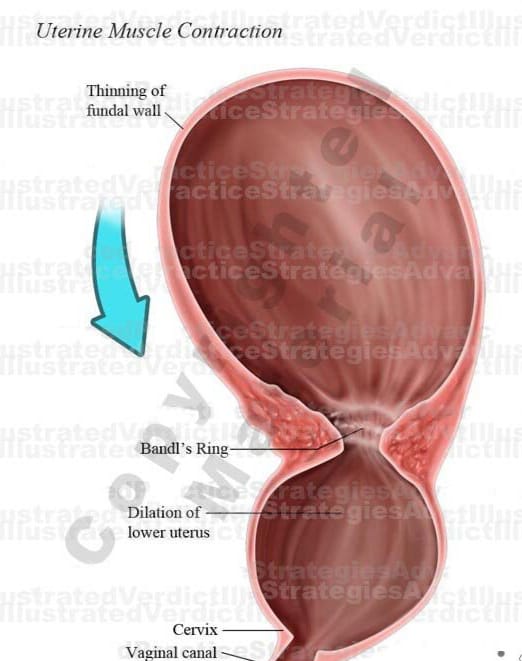
- A circular groove forms in the uterus between the active upper segment and the distended lower segment, which is called the pathological retraction ring. (called Bandel’s ring).
- In primigravida, further retraction ceases in response to obstruction and labor stabilizes due to uterine exhaustion.
- In multipara, uterine retraction continues with progressive circumflex dilatation and thinning of the lower segment.
- The Bandel’s ring moves closer and closer to the umbilicus and eventually the lower segment ruptures.
- Pathophysiology: In this, the intensity, duration and frequency of uterine contractions gradually increase, the relaxation phase decreases and finally tonic contractions occur, but retraction remains. To make room for the fetus coming from the upper segment, the length of the lower segment increases and it becomes thinner. Therefore, a circular groove is formed around the uterus between the active upper segment and the distended lower segment, which is called the pathological retraction ring or Bandels ring. If it increases, the fetus is put in a life-threatening condition and sometimes death can also occur.
In primi gravida, further retraction stops due to obstruction, labor stops and uterine exsorcises. After that, contractions start again when In multipara, as retraction continues, there is continuous dilatation and thinning of the progressive lower segment, so the Bandel’s ring moves closer to the umbilicus and finally the lower segment ruptures.
Sign And Symptoms:
- The patient becomes restless due to continuous pain and discomfort,
- The patient appears exhausted,
- Features of ketoacidosis are also seen.
- Hypertonic contractions are seen and maternal pulse and temperature increase.
- Abdominal Palpation: Upper segment is hard and tender and lower segment is distended and tender and fetal heart sound (FHS) is mostly absent.
- Fetal parts are not properly defined.
- Vaginal examination: Lower segment is over-pressed due to force of presenting part, ring is not felt and features of obstructed labour are seen. Vagina is dry, hot and has offensive discharge, full dilation of cervix and absence of membranes.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History Collection,
- Physical Examination,
- Ultrasound,
- Vital Monitoring,
- Pelvic examination,
- Cardiotocography (CTG),
- Blood tests,
- M.R.I. to identify rare anatomical abnormalities.
Management (Management):
Supportive therapy:
- Usually inj.morphine 15 mg I.M. is provided.
- 5% dextrose drip is started.
- Inj. Ampicillin 500 mg I/M is given.
- Treatment of ketoacidosis is done by I/V infusion of 5% dextrose and Ringer lactate solution.
- Definitive treatment:
- Rule out the presence of uterine rupture.
- If there is any obstruction, relieve the obstruction with minimal hazards to the mother.
- Do not attempt delivery if the fetus is dead or in a dead condition.
- Never perform internal version.
- Routinely explore the uterus after vaginal delivery to identify whether it has ruptured.
- Caesarean section is indicated in certain conditions.
- Infuse the patient with Ringer lactate solution to correct his condition of dehydration and ketoacidosis.
- If the patient is in pain, provide proper pain reliever/analgesic medication to relieve his pain condition.
- Provide proper antibiotic medication to the patient.
- Prevention: Perform partographic management of labor, early diagnosis for malpresentation, cephalopelvic disproportion and perform cesarean section To do.
Difference between Constriction Ring/ Contraction Ring and Retraction Ring/ Bandels Ring:
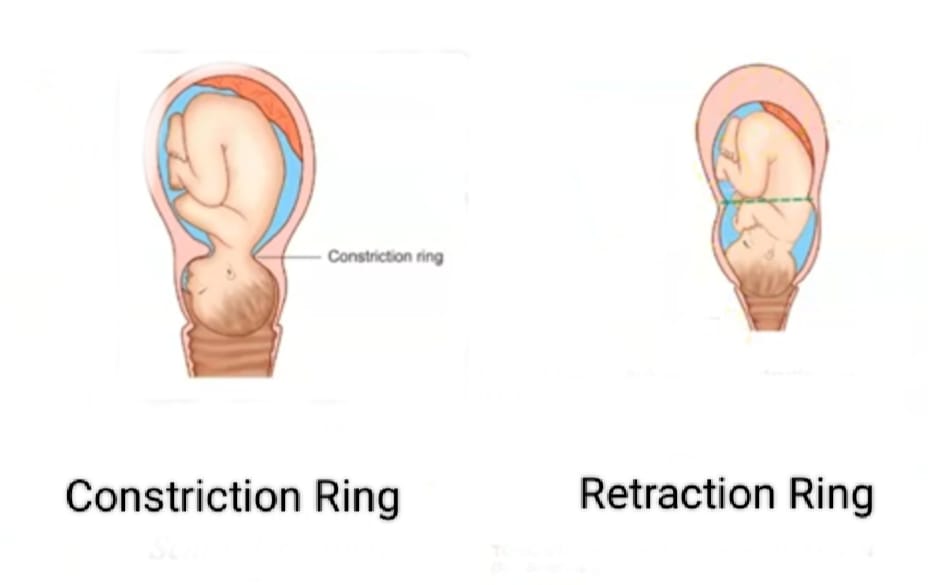
Constriction ring/ Contraction ring:
- 1.Nature: Constriction ring is caused by localized incoordinate uterine contractions.
- 2.Cause: Irritability in the uterus.
- 3.Situation: Any place but usually above and after the junction of the upper and lower segments. The position does not change.
- 4.Uterus: Abnormal polarity is seen.
- 5. Abdominal Examination:
- Uterus: Normal,
- F.H.S.: Present,
- Fetal part: Tender to palpation,
- Ring: Not felt.
- Round ligament: Not felt.
- 6. Vaginal Examination: Lower segment is not compressed by the presenting part.
- Ring is felt over the head.
- Features of obstructed labor are absent.
- 7. Result: Maternal exhaustion and fetal anoxia It is a late feature and the uterus does not rupture.
- 8.Treatment: Relax the ring and deliver or cut the ring if necessary.
Retraction ring/ Bandles ring:
- 1.Nature Retraction Ring Tonic Uterine Contractions and Retraction The final result is.
- 2.Cause: Obstructed labor occurs.
- 3.Situation: Always occurs at the junction of the upper and lobar segments and then gradually moves upwards.
- 4.Uterus: Normal polarity is seen.
- 5.Abdominal Examination:
- Uterus: Tense and tender.
- F.H.S.: Mostly absent.
- Fetal Part: Not easily palpated.
- Ring: Feels rough over groove.
- Round ligament: Stiff and tender.
- Vaginal examination: Lower segment is compressed by presenting part.
- Ring is not felt vaginally.
- Features of obstructed labor are present.
- Results: Maternal exsanguination, sepsis, fetal anoxia are seen. Usually, the uterus ruptures in multigravida.
- Treatment: If there is no ruptured uterus, perform cesarean delivery.
Pre Mature Rupture Of Membrane (PROM):

- When the rupture of membranes occurs after 37 weeks but before the onset of labor, it is called term PROM.
- If it occurs before 37 weeks are completed, it is called preterm (PROM). And when the membranes rupture for more than 24 hours before delivery, it is called prolonged rupture of membranes.
- It is associated with cervical incompetence, pathogenicity of the vaginal canal, and chorioamnionitis. is.
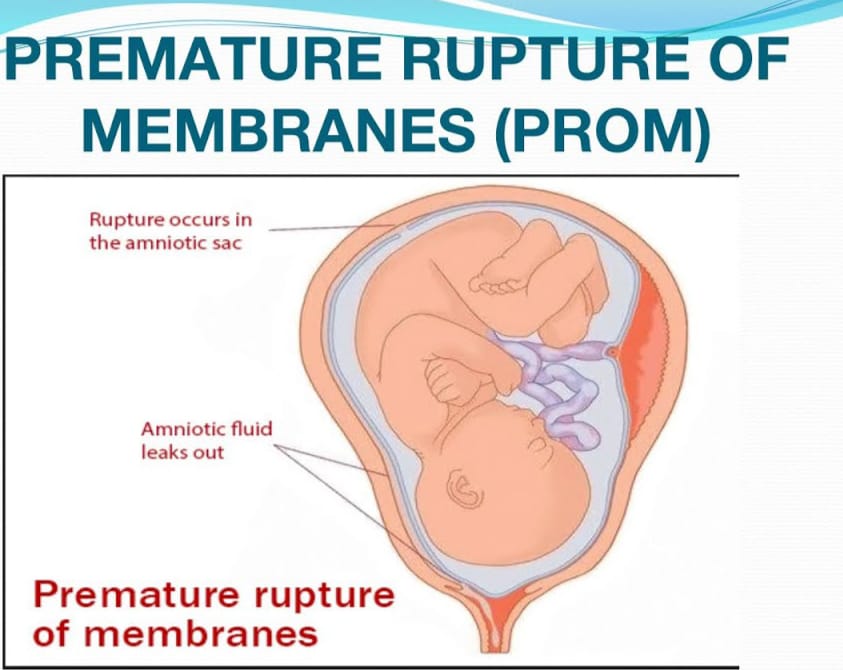
Etiology (Etiology):
- Its exudate is unknown,
- Possible causes include membrane friability,
- Low tensile strength,
- Polyhydroamnios,
- Cervical Incompetence,
- Multiple pregnancy,
- Infection,
- Short cervical length,
- Low BMI,
- History of preterm labor,
- Multiple pregnancy,
- Due to fragile membranes,
- Due to infections such as urinary tract infections and lower genital tract infections,
Sign And Symptoms (Sign And Symptoms) Symptoms):
Vaginal Discharge:
- Watery discharge escaping from the vaginal canal.
- Sudden release of amniotic fluid, often described as a “gush” or continuous leak.
- Contractions: Regular uterine Contractions.
- Fetal monitoring: Changes in heart rate.
- Symptoms of infection such as,
- Fever,
- Increased heart rate,
- Foul-smelling amniotic fluid,
- Cervical changes: such as cervical dilation and effacement during examination.
Risk of premature rupture of membranes:
- Preterm labor,
- Systemic infection in mother and newborn baby,
- Oligohydroamnios which can usually be caused by fetal problems such as pulmonary hypoplasia.
- Cord prolapse,
- Breath presentation due to prematurity,
- Antepartum hemorrhage,
- Psychological trauma to the mother due to long-term hospitalization.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History collection,
- Physical examination,
- Speculum examination,
- Watery discharge from the vagina,
- Examination of the fluid, PH >6,
- Ultrasonography.
- Complete Blood Count,
- Urinalysis,
- High Vaginal Swab for Culture,
- Ultrasonography.
Management (Management):
- First perform a speculum examination with aseptic precautions. Also, check the color of the amniotic fluid for cord prolapse and diagnosis.
- Do not perform vaginal examination.
- Proper bed rest should be given to the patient. Provide sterile vulval pads.
Danger:
- Start labor due to premature rupture of membranes.
- There is a high chance of ascending infection.
- Incidence of cord prolapse is high.
- Dry labor condition is observed due to continuous escape of the placenta.
- Fetal pulmonary hypoplasia is associated with threat and oligohydramnios.
Nursing Management:
- Transfer the patient to the proper hospital.
- Collect a complete history of the patient.
- Advise the patient to take proper bed rest.
- Perform an obstetric examination with proper care and precautions.
- Maintain sterile technique and perform a proper vaginal examination To do.
- Proper observation of cervical dilation and effacement.
- Intracervical swab is taken for gram stain, culture and sensitivity test of bacteria.
- Ultrasound guided abdominal amniocentesis is performed and then a sample of the amniotic fluid is collected for bacterial culture and sensitivity test.
- Fetal monitoring is done every 6 hours. is.
- The patient’s vital signs are checked every four hours, especially pulse and temperature are monitored.
- Antibiotics such as ampicillin 500 mg or cephalosporin
- 500 mg are given 6 hourly x 6 days. Alternatively, erythromycin therapy is given and metronidazole is currently used for 1 week.
- Once the diagnosis is confirmed, management is usually based on factors such as gestational age, whether the woman is in labor, any sepsis, and fetal survival rate, etc.
- Term PROM: In 90% of cases, spontaneous labor starts within 24 hours of rupture and during that time, assessment for infection and care should be provided. If labor has not started, induction and Cesarean section is performed in case of complications.
- Preterm PROM: Due to the risk of prematurity, the patient should be transferred to a well-equipped hospital if fit in utero.
- If the pregnancy is 34 weeks or more and labor does not start within 48 hours, then Cesarean section is performed in case of induction and obstetric complications.
- If the pregnancy is less than 34 weeks and there are no maternal and fetal indications, conservative treatment is provided. is done.
- The patient is given proper antibiotic and steroid medication.
Precipitate Labor:
- Precipitated labor is also called “rapid labor” and “rapid childbirth”. Precipitated labor is defined as abnormal rapid labor in which the total duration of the first and second stages of labor is less than two hours. This causes rapid and spontaneous expulsion of the infant. It is commonly seen in multipara women. Multipara is associated with a relaxed pelvic or perineal floor, multipara is associated with usually strong, forceful contractions and the absence of painful sensations during labor, which leads to the failure to report immediate birth, which leads to precipitated labor.
Etiology:
- Uterine hypertonicity,
- Multiparity,
- Abnormal fetal presentation,
- Favourable pelvic structure,
- Hormonal factors,
- Due to previous rapid labor,
Management:
- If the patient has a previous history of precipitated labor, then admit him to the hospital first.
- Uterine contractions during labor can be reduced with magnesium sulfate.
- Elective induction of labor To perform low rupture of membranes.
- Provide liberal episiotomy and control delivery of the head.
Nursing Management:
- As soon as the patient first arrives in the labor room, immediately assess the situation for precipitated delivery.
- Call for other help and do not leave the patient alone.
- Prepare sterile obstetrics or precipitated delivery packs for delivery.
- Provide information and psychological support to the patient about the condition.
- Give a liberal episiotomy and control the delivery of the head.
- Check for the umbilical cord around the neck.
- If the cord is loose, lift it out and clamp the tight cord twice and cut between the two clamps. Then, perform a controlled delivery of the solder.
- Provide a comfortable position to the mother after delivery. Check the fundus every 10-15 minutes in the first hour to extend the legs and massage if the fundus is soft or boggy.
- Record the delivery and examination of the placenta. Record the condition of the mother and baby and if there are any abnormalities, inform the obstetrician and take measures for its treatment.
Prolong Labor:
- When the combined duration of the first and second stages of labor exceeds 18 hours, it is called prolonged labor. Cervical dilation rate <10% in at least four hours of observation. 1 cm/hr and descent of the presenting part is <1 cm/hr is called prolonged labor.
Etiology:
- Fault in power:
Abnormal uterine contractions such as,
uterine inertia,
inability to lower the uterus,
epidural analgesia,
constriction ring. - Fault in passage:
Contracted pelvis,
Cervical dystocia,
Pelvic tumor,
Due to full bladder and rectum,
Cephalopelvic disproportion,
Android pelvis,
Resistance due to spasm of pelvic floor or perineum or old scar. - Passenger:
Malposition,
Malpresentation,
Big baby,
Congenital anomaly of fetus,
Big baby,
Deflexed head. - Other Causes: Due to early administration of analgesia and sedatives
Sign And Symptoms:
- Duration of labor extended.
- Weak and inadequate uterine Contractions.
- Delayed cervical dilation.
- Changes in fetal heart rate (FHR).
- Maternal fatigue and exhaustion.
- Pain and discomfort due to prolonged pressure on pelvic tissues.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History collection,
- Physical examination,
- Prolonged labor is not a diagnosis but rather an indication of an abnormality. To identify this, abdominal examination and vaginal examination are performed.
- Partographic analysis is performed to diagnose it, i.e. if the rate of cervical dilation is less than 1 cm/hour in nullipara and less than 1.5 cm/hour in multipara, then it is considered abnormal.
- Slow descent of the head occurs.
- Pelvic assessment,
- Radiography,
- CT scan,
- M.R.I. Intranatal imaging.
- Second stage is said to be prolonged when it lasts more than 2 hours in primigravida while it lasts more than 1 hour in multigravida.
Danger (Danger) :
- Fetal danger:
Hypoxia,
Intrauterine Infection,
Intracranial stress/hemorrhage,
Increased incidence of operative delivery, - Maternal Danger:
Distress,
Postpartum hemorrhage,
Trauma to genital tract,
Increased incidence of operative delivery,
Pupillary sepsis,
Subinvolution.
Management ):
- Identify the cause of prolonged labor and its effect on the mother and fetus.
- First stage delay: Identify the presentation, position and station of the fetus by vaginal examination.
- If uterine activity is low, amniotomy, oxytocin infusion and analgesics should be provided.
- Caesarean section is performed in conditions of malpresentation, malposition, big baby and cephalopelvic disproportion.
- Second stage delay: If the fetal heart sound (FHS) is good, expectant management and vaginal delivery or assisted or cesarean delivery is performed.
Nursing Management:
- Proper psychological support should be provided to the mother.
- Early identification of factors leading to prolonged labour and their early detection and proper treatment should be done.
- Properly maintenance of the partograph. Due to which it can identify the condition of prolonged labor early.
- Properly provide sedation to the mother if prescribed so that she can rest properly.
- Properly maintain the nutritional status of the mother.
- Properly provide the mother with intravenous fluids such as Ringer’s lactate (RL) solution to maintain her hydration status and treat the condition of ketoacidosis.
- Properly maintain the patient’s vital signs such as blood pressure and pulse, etc.
- Urine test is done to identify whether acetone is present in the urine.
- Properly check and record labor progress, orifice dilation, vital signs especially blood pressure, and skin color.
Induction Of Labour :
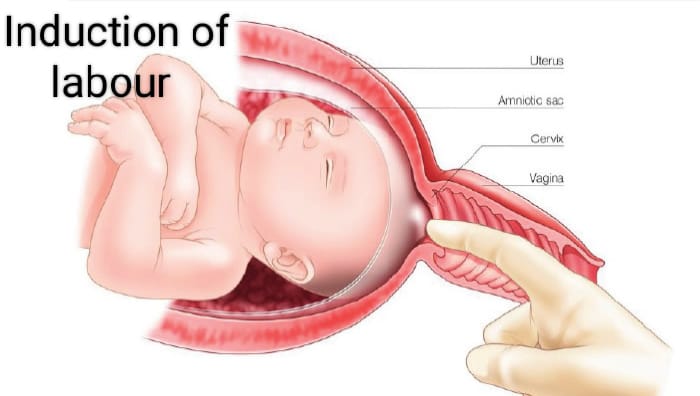
- Induction of labor means the initiation (start) of uterine contractions artificially after the period of viability of the fetus and before the spontaneous labor process starts, in which uterine contractions are started for vaginal delivery by medical, surgical or both combined methods.
- Purpose of induction of labor:
- Induction is done when the continuation of the pregnancy poses a risk to the health of the mother or fetus. It can happen. Therefore, for the safety of both, induction is indicated in cases.
Indications for Induction of Labor:
Induction of labor is required when there is any deviation in the normal physiological process of childbirth.
Maternal Indications:
- Prolonged pregnancy,
- Pre-eclampsia and eclampsia,
- Maternal medical complications such as diabetes mellitus, chronic renal failure, cardiac disease, hypertension, cholestasis, postmaturity, intrauterine death,
- Intrauterine growth Retardation,
- APH specifically abruptio placentae,
- Polyhydramnios associated with maternal distress,
- Oligohydramnios,
- Premature rupture of Membrane,
- Congenital malformation due to malformation.
Fetal Indications:
- Intrauterine growth retardation (IUGR) due to chronic placental insufficiency,
- Intrauterine Fetal death,
- Rh-isoimmunization,
- Unstable lie,
- Congenital malformation of the fetus.
Contraindications (Contraindications) :
- Contracted pelvis,
- Cephalopelvic disproportion (CPD),
- Malpresentation,
- Previous classical cesarean section or hysterotomy,
- Vaginal bleeding,
- Vaza Previa,
- Placenta previa,
- Active genital herpes infection,
- High risk pregnancy, heart disease, pelvic tumors,
- Obstetrics and medical complications with elderly primigravida,
- Umbilical cord prolapse,
- Or cord presentation,
- In cervical carcinoma,
- In HIV-positive women not taking highly active antiretroviral therapy
- In cervical carcinoma.
Caused by induction of labor Risk:
- Mother: Psychological upset,
Tendency of prolonged labor,
Increased need for analgesics,
Operative interference,
Morbidity. - Fits: Iatrogenic prematurity,
Hypoxia,
Uterine dysfunction,
Prolonged labor,
Operative delivery.
Method of Induction of Labor:
1.Medical,
2.Surgical,
3.Combined.
Medical: For medical induction, prostaglandins PGE2 (prostaglandin), PGE1 (misoprostol), oxytocin or mifepristone are used.
For medical induction Prostaglandins (PGE2): Affect locally contiguous cells, causing biomaterial contraction. However, PGE2 is responsible for cervical ripening while PGF2 is responsible for myometrial contractions. PGE2 dinoprostone intracervical application is used for cervical ripening. It is repeated after 6 hours, 3 to 4 doses can be given if necessary. After application, the patient should remain in bed for 30 minutes and her uterine activity and fetal heart rate should be monitored.
Misoprostol (PGE1): Currently used transvaginally or orally. 25 mg vaginally every four hours is used for cervical ripening and labor induction. A total of 6-8 doses can be given.
Oxytocin: It is an endogenous uterotonic. It stimulates uterine contractions. It is most effective when the cervix is ripe. It is given as an intravenous infusion.
Mifepristone: It is a progesterone receptor antagonist and blocks progesterone and glucocorticoid receptors. Used for vaginal cervical resection and labor induction.
Surgical Induction:
1) Artificial Rupture of Membranes (ARM),
2) Stripping the Membranes
Low Rupture of Membranes (LRM):
Procedure: Below the presenting part and above the internal OS A small amount of amniotic fluid is drained by rupturing the membranes. This is done in the labor room or operation theater with full aseptic precautions, emptying the bladder, placing the fetus in the lithotomy position using long cochlear forceps or amniotic hook, followed by the application of a sterile vulval pad and administration of antibiotics. After rupture of membranes, the color of the amniotic fluid, the station of the cervix, cord prolapse, and fetal heart rate should be assessed.
Indications: Antepartum hemorrhage (APH),
hydroamnios, severe preeclampsia, eclampsia.
Contraindications: Intrauterine fetal death, maternal AIDS, active genital herpes infection.
- Advantages:
Lowers blood pressure in pre-eclampsia and eclampsia,
Reduces maternal distress in hydroamnios,
Assessment of leaky amniotic fluid,
Internal fetal monitoring,
Assess uterine cavity,
Takes blood sample from fetal scalp,
Places catheter to measure intrauterine pressure,
Controls bleeding in antepartum hemorrhage (APH) and
Reduces tension in placental abruption and initiation of labor. - Risks: Cord prolapse, excessive amniotic fluid escape, placental abruption, traumatic amnionitis, etc.
- Striping the membranes: This procedure is useful for cervical ripening, before ARM and for induction of labor. Stripping of the membranes involves digital separation of the chorioamniotic membrane from the wall of the cervix and lower uterine segment. This releases endogenous prostaglandins from the membranes and decidua. This method is simple, safe and beneficial. Its criteria include the fetal head being applied to the cervix and the cervix being dilated to the extent that the examiner’s finger can reach it.
- Mechanical: Dilator
Releases prostaglandins from the membrane a decidua for labor induction and survival ripening. - Transcervical balloon catheter (Follis catheter): Extra-amniotic saline infusion is performed for cervical repair.
- Combined method: This The method uses both medical and surgical methods. Its advantages include being more effective than a single procedure, reducing the induction-delivery interval, thus reducing infection and the observation period.
Dystocia (Dystocia):
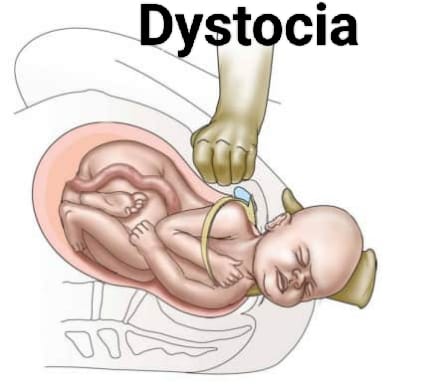
- Dystocia is a condition of difficult labor or difficult childbirth in which the labor process is slow and the progress associated with labor is slow and failure occurs.
- This The condition of dystocia is usually associated with an abnormality in the passage, an abnormality in the passenger, an abnormality in the power, and a combination of all these factors.
Fetal Macrosomia (Fetal Macrosomia):

- Fetal macrosomia Generalized fetal enlargement is called. When the birth weight of the fetus is usually 4 kilograms kg (4000 gm) and more, this condition is called fetal macrosomia.
Etiology:

- Hereditary,
- Maternal diabetes mellitus,
- Gestational diabetes mellitus,
- Obesity,
- Size of parents,
- Postmaturity,
- Multiparity,
- Prolonged pregnancy,
- Maternal age,
- Male feats.
Sign And Symptoms Signs and Symptoms:
- Prolonged labor,
- Weak and infrequent uterine contractions,
- Fetal distress,
- Maternal fatigue,
- Abnormal fetal presentation.
- Pelvic Discomfort,
- Cervical swelling and pain.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History Collection,
- Physical Examination,
- Pelvic Examination,
- Ultrasound,
- Fetal Heart Rate Monitoring,
- Amniotomy,
- Blood Test.
Management:
- Monitoring:
Regular assessment of the fetus and regular monitoring of the fetus’s growth and well-being through ultrasound. - Maternal Management:
Blood Glucose Control: Advise the mother with gestational diabetes to maintain her blood glucose levels properly. - Nutritional Guidance: Advise the mother to consume a well-balanced diet during pregnancy. and advice on weight management.
- Delivery Planning:
Vaginal Delivery: If the fetus is of a manageable size and correctly positioned, a trial labor is attempted. - Caesarean Section:
If the fetus is of a large size and vaginal delivery is impossible, the patient is advised for a caesarean section. - Intrapartum Monitoring:
To monitor fetal distress Continuous monitoring during the intrapartum period to monitor for any signs and symptoms. - Postpartum Care:
Continuous monitoring of the condition of the mother and fetus after delivery and proper monitoring for any complications such as hypoglycemia in the newborn. - Multidisciplinary Approach:
Proper collaboration with obstetrician, endocrinologist, nutritionist, and pediatrician for comprehensive care To do.
Hydrocefelus :
- Hydrocephalus is a Greek word that consists of hydro meaning “water” and cephalus meaning “head”. Hydrocephalus is an abnormal condition in which there is an abnormal accumulation of cerebrospinal fluid (CSF) in the ventricular system and subarachnoid space. This causes an increase in pressure inside the skull. This condition of hydrocephalus is usually caused by an imbalance in the production and absorption of cerebrospinal fluid due to obstruction in the SCF pathway. This causes dilation of the cerebral ventricles, enlargement of the head, cognitive impairment, seizures and other neurological problems.
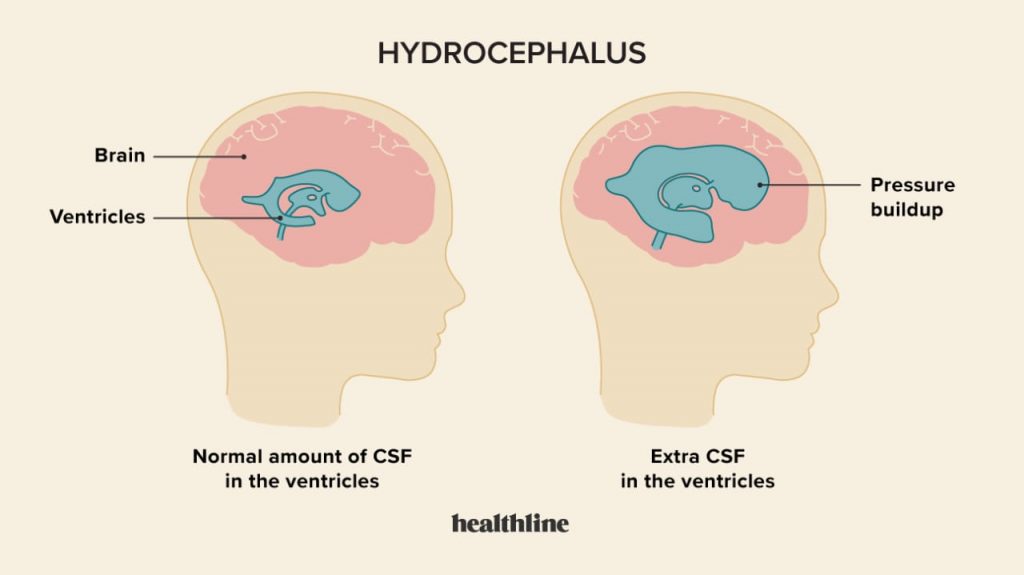
- C.S.F Pathway
- Cerebrospinal fluid is secreted from the choroid plexuses of the ventricles by ultrafiltration and active secretion.
- The cerebrospinal fluid passes from the lateral ventricles into the third ventricle through the foramina of Monro.
- This Cerebrospinal fluid from the third ventricles passes through the cerebral aqueduct (aqueduct of Salvia) ventricles into the fourth ventricles.
- The cerebrospinal fluid then passes through the foramina of Luschka and the foramina of Magendie into the basal cisterns and subarachnoid space. Cerebrospinal fluid is absorbed by the arachnoid villi in the venous channel and sinuses. About 20 ml of cerebrospinal fluid is secreted in about one hour. And 500 ml / day. The total amount of cerebrospinal fluid is 100 to 150 ml.
Etiology:
The condition of hydrocephalus is mainly congenital hydrocephalus, and acquired Hydrocephalus is of two types.
1) Congenital hydrocephalus:
Due to infections during intrauterine life such as,
STORCH (syphilis, toxoplasmosis, rubella, cytomegalovirus, herpes virus.),
Due to congenital brain tumors that obstruct the flow of cerebrospinal fluid.
Due to malformations at birth,
Due to intracranial hemorrhage,
Due to stenosis and maldevelopment of the duct,
Arachnoid cyst Due to maldevelopment, displacement of the brain stem and cerebellum from the foramen magnum (Arnold’s Chiri malformation), genetic factors.
2) Acquired hydrocephalus:
Due to brain infections such as meningitis, encephalitis.
Due to trauma such as birth trauma, head injury, intracranial hemorrhage.
Neoplasms such as tuberculoma, subdural hematoma and abscess, gliomas, ependymoma, astrocytoma, choroid plexus Papilloma, pseudotumor cerebri.
Chemical causes such as hypervitaminosis A.
Connective tissue disorders such as Hurler syndrome, achondroplasia,
Degenerative atrophy of brain,
Arteriovenous malformation, ruptured aneurysm.
3) Communicating hydrocephalus:
Bacterial meningitis,
Malignant meningitis,
Hemorrhage,
Increased venous pressure.
4) Noncommunicating hydrocephalus:
Due to congenital causes,
Due to acquired causes.
Types of hydrocephalus (types of hydrocephalus):
There are a total of four types of hydrocephalus.
1) Congenital hydrocephalus ,
2) Acquired Hydrocephalus ,
3) Communicating Hydrocephalus,
4) Noncommunicating Hydrocephalus.
1) Congenital Hydrocephalus :
Congenital hydrocephalus is present at birth. And it usually occurs due to any environmental factor and genetic factor during the fetal development period.
2) Acquired Hydrocephalus:
Acquired Hydrocephalus develops at the time of birth. And also develops thereafter. This acquired hydrocephalus is caused by any birth injury or birth trauma.
3) Communicating hydrocephalus:
In communicating hydrocephalus, there is no blockage in the ventricular system, basal cisterns, and spinal subarachnoid space. In this communicating hydrocephalus, there is excessive production of cerebrospinal fluid (CSF) and there is no adequate absorption of cerebrospinal fluid (CSF), due to which there is accumulation of fluid in the brain which is responsible for creating hydrocephalus.
4) Noncommunicating hydrocephalus:
This noncommunicating hydrocephalus is seen due to obstruction in any of the ventricular system (usually the aqueduct, foramina of Luschka and Magendie). This obstruction can usually be partial, intermittent and complete. This obstruction usually develops due to inflammation and obstructive lesions. Due to this blockage, the flow of spinal fluid inside the brain is impaired. This causes accumulation of fluid in the brain, which creates the condition of hydrocephalus.
Sign And Symptoms:
- Accumulation of cerebrospinal fluid in the ventricles of the brain.
- Excessive enlargement of the head.
- Sinus skull.
- Cranial sutures separate due to enlargement of the head.
- Bulging of the fontanelles,
- The scalp is swollen and the veins are dilated.
- Percussion of the skull produces a “cracked pot” resonance (macewen’s sign).
- Sunset sign (sclera visible above the iris) may be seen.
- The face appears small in relation to the head.
- Increased intracranial pressure.
- Hemiplegia.
- Crying is hoarse.
- Often papilloedema.
- Spasticity.
- Ataxia.
- Urinary incontinence.
- Progressive deterioration of mental function.
- Nausea.
- Vomiting.
- Restlessness.
- Irritability.
- Irregular and decreased respiration.
- Pulse a Decreasing.
- Convulsions.
- Fatigue.
- Stupor and coma.
- Headache.
- Lethargy.
- Apathy.
- Irritability.
- Confusion.
- Visual problems.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History Collection,
- Physical Examination,
- Antenatal: Sonography
- Measuring Head Circumference.
- Cranial Ultrasonography.
- X-ray.
- CT scan.
- M.R.I.
- Neurological examination.
- Ventriculography.
- Pneumoencephalography.
- Intracranial pressure monitoring.
- Neuro Psychological assessment.
- Genetic testing.
- Intracranial pressure monitoring.
Management:
- In breech presentation, the arrested head can be decompressed by perforating the sub-occipital region using a perforator or sharp pointed scissors under the guidance of two fingers of the left hand protecting the anterior vaginal wall. Other methods of head decompression are:
- Performing a laminectomy in the cervical region to open the spinal canal.
- During the procedure, the anterior vaginal wall is retracted with two Landens retractors.
- Uterine dressing forceps or a Drew-Smith catheter are pushed through the open spinal canal into the ventricle to drain fluid (e.g., open spina bifida).
- If the condition of hydrocephalus is mild and stable, then the child should be continuously monitored by healthcare personnel. This includes continuous monitoring of the child’s head circumference, developmental milestones, etc.
- If the child has mild symptoms, then provide adequate medication to reduce their symptoms.
- The carbonic anhydrase inhibitor, acetazolamide (Diamox), is used to reduce the production of CSF.
- Oral glycerol and isosorbide are used to reduce increased intracranial pressure in children.
- If the child has hydrocephalus due to any obstruction, surgical management is required.
- Performing a lumbar puncture to maintain the pressure of the cerebrospinal fluid.
- The most common method to treat the condition of hydrocephalus is the placement of a tube (a tube is a thin tube that is inserted into the brain) This tube is implanted and is delivered to other parts of the body and diverts the pathway of cerebrospinal fluid. Such as the abdominal cavity.)
- Endoscopic third ventriculostomy (ETV) is performed in certain cases such as non-communicating hydrocephalus in which the hydrocephalus condition arises due to obstruction. In this procedure, a hole is formed in the third ventricle, due to which the obstruction of the pathway of cerebrospinal fluid is bypassed and can go into the subarachnoid space where it is absorbed.
- Types of Shunt Procedures:
- 1) Ventriculoperitoneal shunt: In this procedure, one part of the shunt catheter is inserted into the anterior part of the lateral ventricles in the brain while the other end of the shunt is inserted into the skin of the peritoneal cavity. And the path of cerebrospinal fluid is diverted from the ventricles to the peritoneal cavity.
- 2) Ventriculopleural shunt (VPL): This shunt is similar to the ventriculoperitoneal shunt in which one end of the shunt catheter is inserted into the ventricles and the other end of the shunt catheter is inserted into the pleural cavity (around the lungs). Due to this shunt, the cerebrospinal fluid goes into the pleural cavity and is absorbed there.
- 3) Ventriculoatrial shunt: In ventriculoatrial shunt, to collect cerebrospinal fluid, the distal end of the shunt catheter is inserted into one ventricle of the brain and then the other end of the shunt catheter is inserted into the atrium of the heart through the jugular vein. This shunt procedure allows the cerebrospinal fluid to enter the bloodstream where it is absorbed.
- 4) Lumbar Peritoneal Shunt: In a lumbar peritoneal shunt, cerebrospinal fluid is diverted from the lumbar subarachnoid space (lower spine) to the peritoneal cavity. Which can cause cerebrospinal fluid to be absorbed into the abdominal cavity.
- 5) Ventriculoureteral shunt:
This type of shunt is usually used in older children and is usually done when all other types of shunts fail. This shunt diverts cerebrospinal fluid from the ventricles into the ureter.
Nursing Management:
Pre-operative Nursing Management
- Proper and continuous assessment of the child, including baseline health status, vital signs, neurological status, and hydration status of the child.
- Continuously monitor the child’s intracranial pressure.
- Continuously measure the child’s head circumference.
- Palpate the child’s fontanelles to assess for any increased intracranial pressure.
- Assess the child’s pupillary response and level of consciousness.
- Continuously monitor the child’s vital signs. To do.
- Provide the child with proper work and a quiet environment.
- Maintain aseptic technique while handling the child to prevent nosocomial infections.
- Continuously change the child’s position.
- Properly maintain the child’s nutritional status.
- Properly provide intravenous fluids to the child.
- Keep the child on Nil Per Oral.
- Continuously monitor the child’s intake output chart.
- Properly collaborate with other health care personnel for the proper care of the child.
- Surgery is a stressful condition for the child and his family members, so the child’s parents should be properly informed about it. Provide education and provide psychological support.
- Provide proper assurance and emotional support to the child’s parents.
Post-operative management:
- Continuously and closely monitor the child after surgery.
- Frequently monitor the child’s vital signs every fifteen to twenty minutes.
- Properly monitor the child’s neurological status.
- Frequently monitor the child’s body temperature if there is an alteration.
- Provide the child with a non-operative position to prevent pressure on the shunt.
- Provide the child with a flat position on the bed for 24 hours after surgery.
- Assess the child’s photos and notify immediately if depressed.
- Provide analgesic medication to relieve pain if the child is in pain.
- The child Assess for any complications after surgery.
- Provide the child with proper fluids and maintain their hydration status. Continuously monitor the child’s intake output chart. And continuously maintain the child’s electrolyte level.
- Provide the child with proper aseptic technique and dressing the surgical site.
- Provide proper support and education to the child and his family members.
Shoulder Dystocia (Shoulder Dystocia):
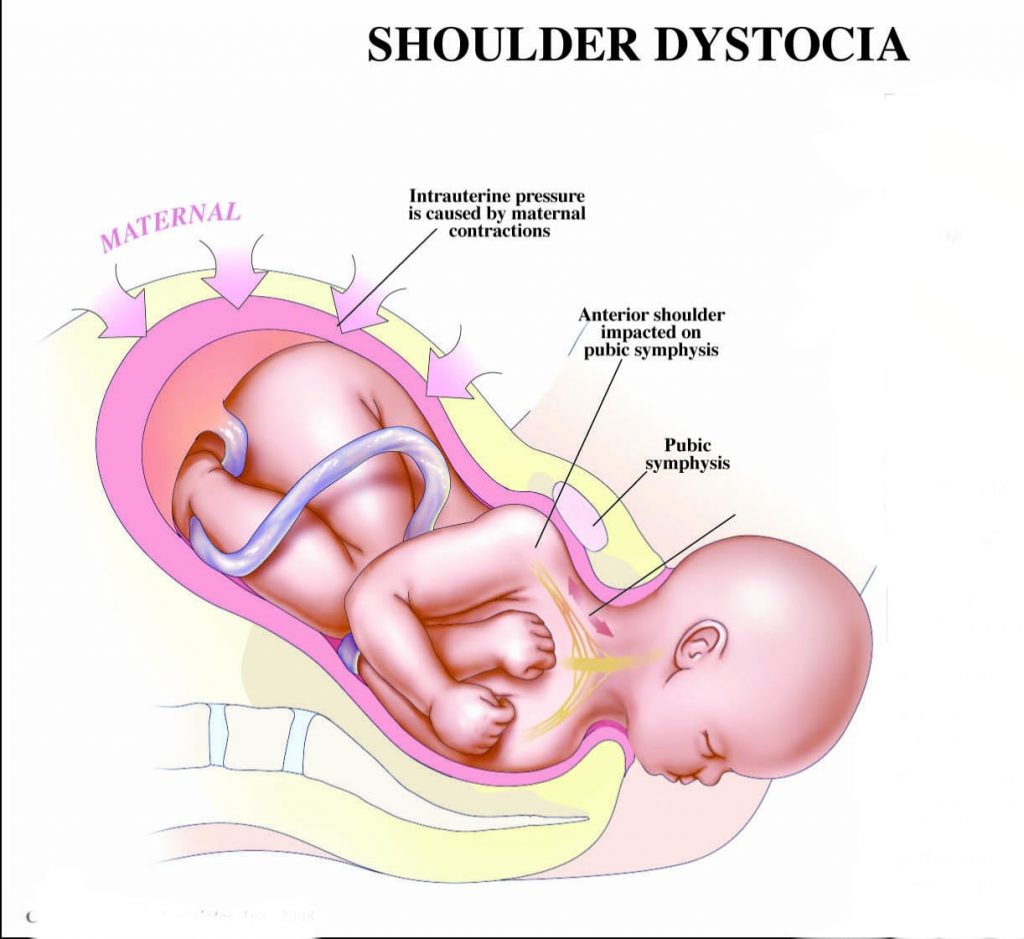
- The term shoulder dystocia is defined to describe a wide range of difficulties encountered in the delivery of the shoulder during labor. In which, during the labor process, the head of the fetus is delivered but its shoulder gets stuck in the pelvic bone of the mother, causing difficulty in delivery, i.e. the shoulder of the fetus cannot be delivered, then this condition is called shoulder dystocia.
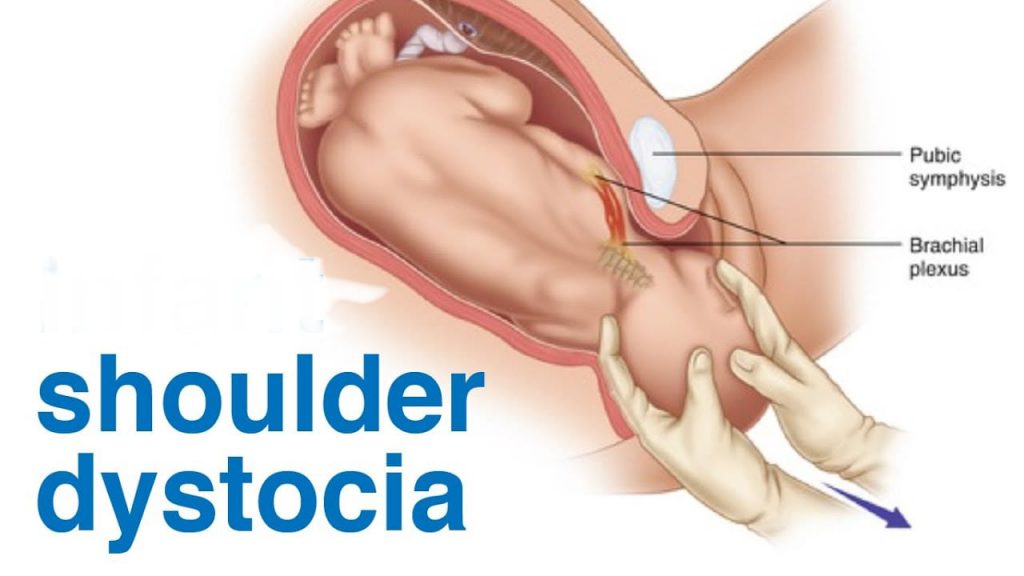
- Shoulder dystocia is an emergency in which the shoulder of a child gets stuck behind the mother’s pelvic bone after the head is delivered during childbirth. This can lead to complications for both mother and baby, including potential nerve damage or fractures in the child and increased risk of hemorrhage in the mother.
- In solder dystocia, the problem lies in the pelvic inlet.
- The anterior solder lies above the symphysis pubis.
- While the posterior solder lies in the sacral promontory.
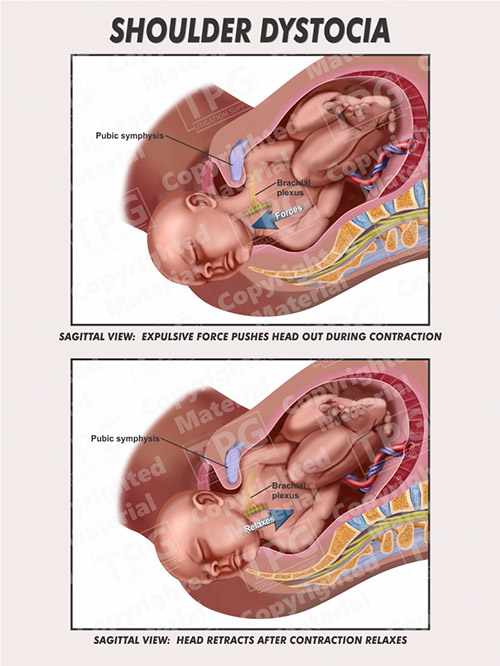
Etiology:
- Macrosomia,
- Abnormal fetal presentation,
- Narrow pelvic shape or deformity,
- Maternal obesity,
- Diabetes mellitus, (gestational or pre-existing)
- Previous Solder Dystocia,
- Rapid Labor,
- Due to the prolongation of the second stage of labor,
- Induction of Labor,
- Assisted Delivery (Forces or Vacuum Extraction).
Predisposing Factors:
- Fetal macrosomia (fetal weight greater than 4 kg (4000 gm) at birth),
- Maternal diabetes mellitus,
- Obesity,
- Medipelvic instrumental delivery,
- Post maturity,
- Multiparity,
- Anencephaly,
- Fiss ascites,
- Maternal age should be more than 35 years.
- Fetal distress,
- Short cord or cord tightly looped around the neck.
Sign And Symptoms:
- Turtle sign: This involves a phenomenon seen during childbirth where, after the delivery of the fetus’s head, it retracts back towards the perineum instead of starting to deliver the body. This condition indicates a potential condition of placenta dystocia, which indicates that the placenta is stuck behind the pelvic bone.
- Prolongation of the second stage of labor.
- Increases maternal perineal pressure and discomfort.
- Changes in fetal heart rate, such as bradycardia, are observed.
- Delayed delivery of the placenta.
- Increased risk of brachial plexus injury in newborns.
- Potential clavicular or humeral fracture in newborns.
- Maternal hemorrhage.
Diagnostic Evaluation:
- History Collection,
- Physical Examination,
- Fetal Heart Rate Monitoring,
- Ultrasound,
- Pelvic Examination,
- X ray,
- M.R.I.
Management:
- During management:
- Call for additional help.
Clear the infant’s mouth and nose.
Abduct the maternal thigh and bring it spirally towards the abdomen. Flexed.
If earlier mediolateral episiotomy has not been done, perform a wide mediolateral episiotomy. - Do not do during management:
- Do not panic if there is a condition of solder dystocia.
Do not apply traction on the baby’s head.
Do not apply fundal pressure. - Step – I: The head and neck of the fetus are grasped and moved to a posterior position and suprapubic pressure is applied towards the chest of the fetus. is.
- Step – II Roberts Maneuver: It involves abduction of the mother’s leg and flexing the leg on the mother’s abdomen.
- Step-III Woods Maneuver: It involves inserting two fingers into the posterior vagina and then rotating the posterior solder towards the anterior.
- Step: IV Delivery of Posterior Arm:
Identify the location of the posterior arm.
Direct the hand in the hollow of the sacrum.
Wrist and Grasp and splint the forearm.
Sweep over the chest and deliver the hand.
Deliver the posterior arm. - Step: V Clidotomy: In this, the girth of the shoulder is reduced. And one or both clavicles are cut.
- Zvenellis Maneuver: Used to manage some cases of shoulder dystocia during childbirth. In which when the head of the fetus gets stuck after the head comes out, the head of the fetus is pushed back into the birth canal in this procedure to relieve pressure on the cord and then the delivery is done by cesarean section.
Obstetric Emergencies:

Cord Prolapse :
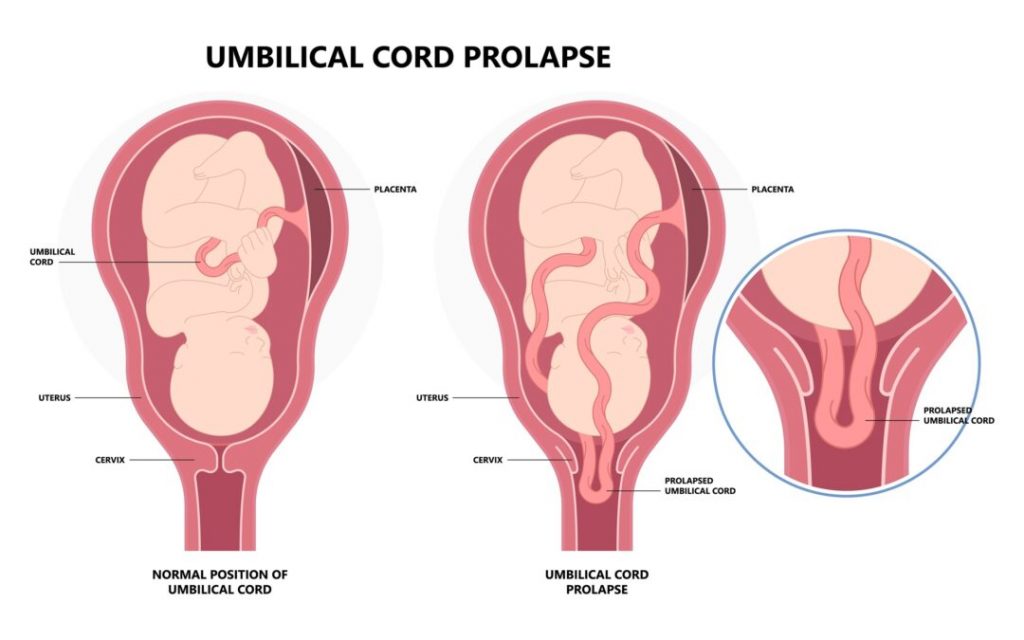
- Cord prolapse is a condition where the umbilical cord slips past the presenting part of the fetus during labor, and the membranes are not intact. This can cause compression of the cord and impair blood flow and oxygen supply to the fetus, increasing the risk of fetal distress. Cord prolapse is considered an obstetric emergency and often requires immediate intervention to ensure the safety of the fetus, such as providing the mother with proper positioning or performing a cesarean delivery.
- When the umbilical cord comes forward over the presenting part of the fetus and the umbilical cord is the presenting part but the membrane is not intact and due to this the circulating blood and oxygen supply in the cord is clamped off while passing through the birth canal, it is called cord prolapse. It is called an obstetric emergency.
- Cord Presentation: Cord presentation is a condition in which the umbilical cord is present in front of the presenting part of the fetus, i.e. as the presenting part, and the membrane is also intact. Thus, if the umbilical cord is present as the presenting part, this condition is called cord presentation.
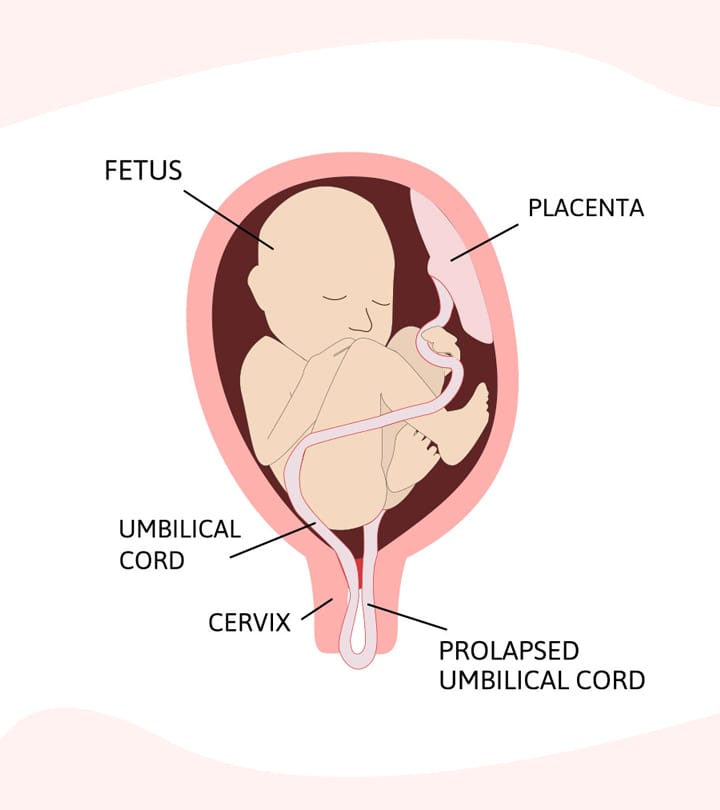
Types Of Cord Prolapse :
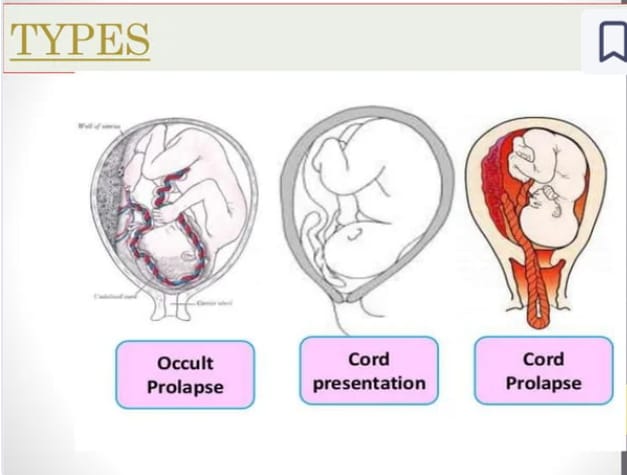
There are generally 3 types of cord prolapse.
1) Occult prolapse,
2) Cord presentation,
3) Cord prolapse.
1) Occult prolapse: In this, the umbilical cord is compressed. But it is not palpable and visible through the vagina. It can be detected when there are changes in fetal heart rate monitoring.
The cord is on the presenting side. But it is not felt by the finger in internal examination.
2) Cord presentation: Cord presentation is a condition in which the fetus is not In front of the presenting part, the umbilical cord is present and the membrane is intact. Thus, if the umbilical cord is present as the presenting part, this condition is called cord presentation.
3) Cord prolapse: When the umbilical cord comes in front of the presenting part of the fetus and the umbilical cord is present as the presenting part but the membrane is not intact and due to this, the circulating blood and oxygen supply in the cord gets clamped off while passing through the birth canal, it is called cord prolapse. is.
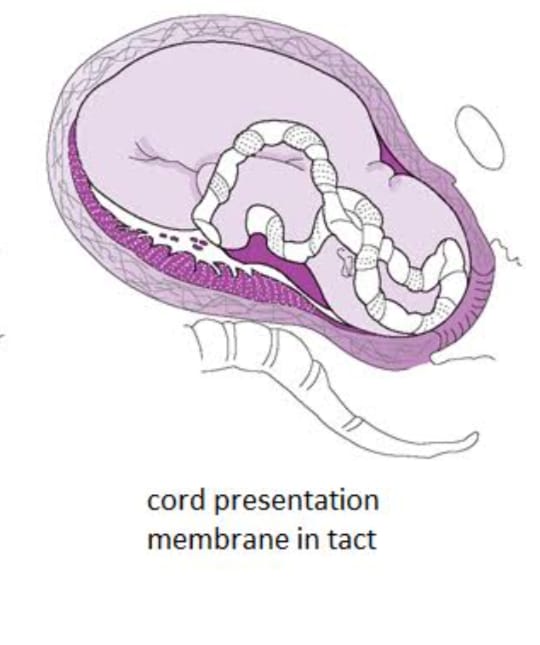
Etiology:
- Malpresentation,
- Contracted pelvis,
- Prematurity,
- Low birth weight <2.5kg,
- Fetal congenital anomalies
- Twins,
- Hydroamnios,
- Minor degree placenta previa,
- Low rupture of membranes,
- Manual rotation of the head,
- Version,
- Induction,
- Long cord (longer than 100 cm),
- Due to abnormal presentation and position of the fetal head, such as,
- Breech presentation,
- Face and brow presentation,
- Solder presentation,
- Occipito posterior position,
- High head,
- Polyhydroamnios,
- Multiple pregnancy.
Diagnostic Evaluation :
- History collection,
- Physical examination,
- Ultrasound,
- Vaginal examination,
- 1) Occult prolapse: Diagnosis is difficult if the pattern of fetal heart sound (FHS) If there is a constant variable deceleration in the fetus, then there may be occult prolapse.
- 2) Cord presentation: The pulsation of the cord is felt through the intact membrane.
- 3) Cord prolapse: The cord is felt directly, and if the fetus is alive, then the pulsation occurs in the cord. Many times the pulsation does not occur in the cord but the fetus may be alive.
- The fetus should be declared dead and confirmed by USG and auscultation.
Management:
- Management usually depends on whether the baby is alive or dead.
- If the baby is dead, confirm it by ultrasound and wait for spontaneous delivery.
- If the baby is alive and vaginal delivery is possible, deliver it by forceps and ventouse.
- If vaginal delivery is not possible,
First aid management is to relieve pressure on the cord. Minimize and stop oxytocin infusion. - Check for cord prolapse in all cases after membrane rupture.
- Surgical induction: Check for cord prolapse before and after amniotomy and, if possible, prepare for cesarean section in amniotomy operation theatre.
- After diagnosis of cord presentation, prepare patient for cesarean section if immediate delivery is not possible. And until then, exaggerated Sims lateral position Give. In rare cases, if the cervix is 7-8 cm dilated, if there is no fetal distress, keep a watch and perform forceps and breech delivery.
- Cord prolapse: First, properly assess whether the baby is alive or dead. Check maturity and survival dilation.
- If the baby is alive, then cesarean section is the best method. Before preparing for cesarean, insert 400 to 750 ml of normal saline into the bladder through a catheter and fill the bladder and empty the bladder before cesarean delivery.
- If immediate safe vaginal delivery is possible, forceps delivery in vertex presentation and breech extraction in breech presentation should be performed. If the baby is stillborn, wait for spontaneous delivery after confirmation of diagnosis.
- If the midwife suspects cord prolapse during vaginal examination, she should immediately inform the supervisor.
- Take immediate action after diagnosing a cord problem.
Amniotic Fluid Embolism:
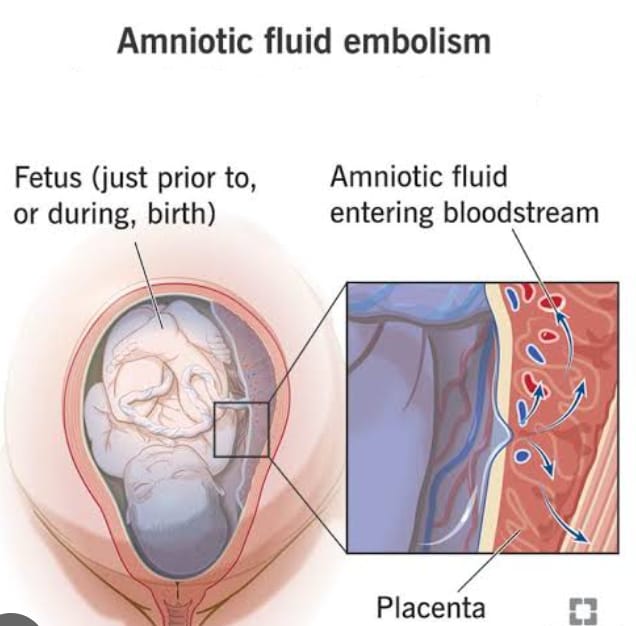
- Amniotic fluid embolism is a condition in which the pressure of the contracting uterus causes the accidental infusion of amniotic fluid into the mother’s bloodstream or into the maternal circulation from the uterus or placental site. This condition can be fatal to the mother, as the debris-laden amniotic fluid is deposited in the pulmonary arterioles and produces symptoms of pulmonary embolism. This condition is a common cause of maternal death during labor.
Etiology:
- Defect in membranes,
- After rupture of membranes or premature separation of placenta (abruptio placentae),
- Rapid or precipitated labor,
- Multiparity,
- Advanced maternal age,
- Drugs,
- Due to uterine trauma during manipulation,
- During cesarean section.
Sign And Symptoms (Signs and Symptoms):
- Sudden onset of maternal respiratory distress such as,
- Severe dyspnea and cyanosis,
- Chest pain,
- Coughing with frothy pink sputum,
- Shock disproportionate to blood loss,
- Vomiting,
- Restlessness and anxiety,
- Convulsion,
- Seizures,
- Heart Failure,
- In pulmonary AD,
- Fetal bradycardia,
- If delivery is not made, a condition of fetal distress may occur,
- If immediate treatment is not provided, maternal or fetal death may occur within minutes
- Disseminated in complications Intravascular coagulation (DIC) may occur.
Diagnostic Evaluation:
- History Collection,
- Physical Examination,
- Blood Gas Analysis,
- Complete Blood Count (CBC),
- Coagulation Profile,
- Fibrinogen,
- Arterial blood gases,
- Electrolyte level monitoring,
- Imaging studies (chest x-ray),
- Electrocardiogram,
- Echocardiogram,
- MRI (if further evaluation is needed),
- Serum tryptase,
- Cervical histopathology.
Management:
- Call for medical help and provide immediate treatment to the patient.
- Immediately initiate emergency or resuscitative measures to maintain the patient’s life.
- Give oxygen 8-10 liters/minute via face mask or 100% oxygen via resuscitation bag and assist in immediate resuscitation.
- Prepare the patient for intubation and mechanical ventilation.
- Intravenous crystalloid (Ringer’s) or colloids (Hemacel) for volume replacement and Administer fresh frozen plasma (FFP), platelet concentrates, packed red blood cells and autotransfusion (collecting the patient’s own blood from the operated area).
- Give aminophylline for respiratory distress and heparin in acute conditions of disseminated intravascular coagulation (DIC) as per instructions.
- Properly monitor maternal and fetal condition.
- Monitor hourly urine output by placing an indwelling urinary catheter.
- Provide the patient with proper side lying position.
- Prepare for emergency birth when the mother’s condition stabilizes.
- Properly record and report monitoring.
- Provide reassurance and emotional support to the mother and family members.
- Complications of amniotic fluid Embolism:
- Disseminated intravascular.
Cardiopulmonary collapse.
Coagulation.
Acute renal failure.
Atonic uterus.
Hypotension.
Fetal distress/death.
Obstetric Shock:
- Obstetric shock is a condition in which the inability of the mother’s circulatory system to provide the body with the oxygen and nutrients it needs and to remove waste substances, and the inadequate amount of circulation causes tissue perfusion to be poor, resulting in generalized cellular hypoxia. This condition is called shock.
- Shock is a condition that can arise due to the inability of the circulatory system to provide oxygen and nutrients to the tissues as required./Shock is usually a state In which tissue perfusion is compromised, causing cellular hypoxia, it is defined as a syndrome initiated by acute hypoperfusion that can lead to a condition of tissue hypoxia. And conditions of vital organ dysfunction may arise. Shock is usually a systemic disorder that can affect multiple organ systems.
Classification / Etiology of Shock:
1. Hypovolemic shock: It is characterized by decreased circulatory blood volume and may be hemorrhagic or nonhemorrhagic. Hemorrhagic shock occurs due to postpartum/post-abortal hemorrhage, ectopic pregnancy, placenta previa, abruptio placentae, ruptured uterus, and obstetric surgery. Non-hemorrhagic shock occurs due to nausea, vomiting, diuresis, supine hypotensive syndrome, and fluid loss if amniotic fluid is removed rapidly.
2. Septic shock (endotoxic shock): Septic abortion, chorioamnionitis, pyelonephritis, Postpartum endometritis, the patient goes into septic shock.
3. Cardiogenic shock: Cardiogenic shock is seen in myocardial infarction, cardiac arrest, cardiac tamponade.
4. Extracardiac shock: Pulmonary embolism, amniotic fluid embolism, anaphylactic drug, neurogenic, chemical injury etc. are responsible for shock.
Antepartum Causes:
Abruptio placentae,
Placenta previa,
Trauma.
Postpartum Causes:
Retained placenta,
Atonic uterus,
Rupture uterus,
Coagulopathy,
Laceration
Sign And Symptoms:
- Grayish blue/ pale skin,
- Cold and clammy skin,
- Severing,
- Perspiration,
- Drymouth,
- Pyrexia,
- Sub-normal temperature,
- Rapid and weak pulse,
- Slow bounding pulse,
- Rapid breathing but as the mother’s condition worsens, breathing becomes shallow, slow and finally unconscious.
- Blood pressure is initially normal then low, but is not recorded due to 40% volume loss.
- Urine output decreases.
Management:
- Early diagnosis of signs of shock and providing a comfortable position to the patient. Ex: Provide lateral position in supine hypotensive syndrome.
- Start resuscitative measures immediately and maintain airway and elevate foot end.
- Provide oxygen to the patient at 6-8 liter/min.
- Correct the patient’s acidosis condition.
- Stop bleeding in hemorrhagic shock.
- I.V. to replace fluids Provide infusion and transfusion to expand volume. Ex: Provide blood transfusion, normal saline in crystalloid, Hemacil in colloid, etc.
- Check cardiac efficiency and prevent circulatory overload and cardiac failure.
- Provide instructions on medications, antibiotics, vasodilators, diuretics, corticosteroids, and insulin A S to maintain normal blood glucose in septic shock
- If If the shock is due to psychological stress, provide support, encouragement, and emotional security.
- Provide proper psychological support to the patient’s family members.
- Check the mother’s vital signs and fetal heart sound (FHS) every 15 minutes and record them properly.
- Properly maintain the patient’s intake output and other recordings.
Vasa Previa :
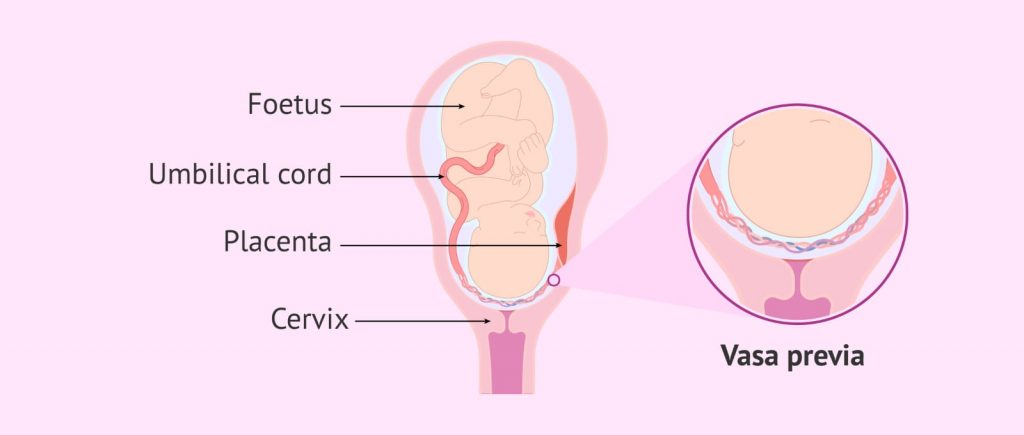
- Vasa previa is an obstetric complication in which the fetal blood vessels pass across or near the internal orifice of the uterus and are in front of the presenting part. When the supporting membrane ruptures, these vessels are at risk of rupture because they are unsupported by the umbilical cord or placental tissue. These complications can arise during labor and delivery.
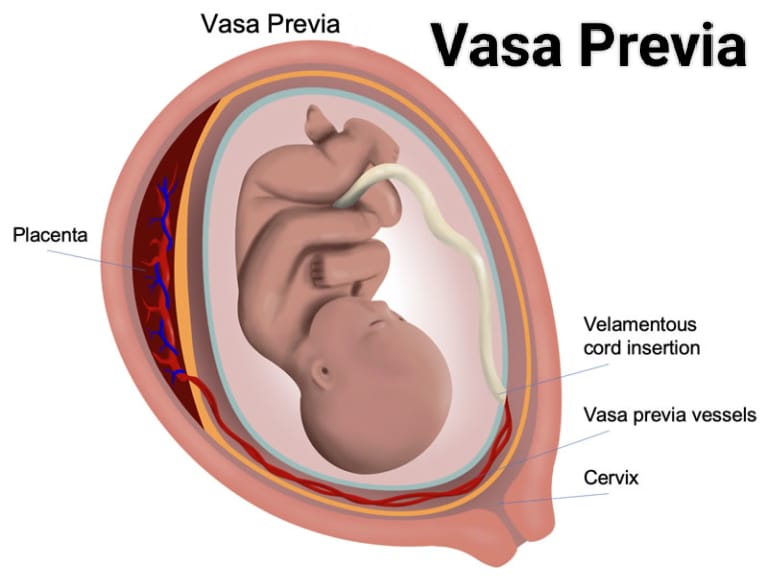
Etiology:
- A low lying placenta can be caused by scarring of the uterus due to previous miscarriages and D and C (dilation and curettage).
- An abnormally or unusually formed placenta can be a bilobed placenta or a succentrate-low placenta.
In-vitro fertilization pregnancies and multiple pregnancies (twins and triplets).
Velamentas Due to insertion of umbilical cord.
Risk factors of vasa previa:
- Placenta previa,
- Velamentous insertion of umbilical cord,
- Multilobed Placenta,
- Multiple pregnancy.
Sign And Symptoms Signs and Symptoms:
- Painless vaginal bleeding (2nd and 3rd trimester).
- Darker red blood (because the baby’s blood is dark, bright red blood is the mother’s blood).
- Fetal Bradycardia.
Diagnostic Evaluation:
- History Collection,
- Physical Examination,
- Ultrasonography:
- Transvaginal sonography in combination with color Doppler helps detect vasa previa as early as the 16th week of pregnancy.
- Noting the triad sign:
- Painless vaginal bleeding,
- Membrane rupture,
- Fetal bradycardia or death.
Management:
- If blood vessels rupture, hospitalize the mother in the 3rd trimester to ensure rapid access to medical care.
- A cesarean section should be performed around 35 weeks of pregnancy.
- Healthy delivery by cesarean section is the only treatment plan to follow. A cesarean section should be planned as early as possible to avoid emergencies and late enough to prevent complications related to prematurity. Usually, if the mother is normal without any risk, a cesarean section is recommended at 35-36 weeks.
Rupture Of The Uterus (Rupture Of The Uterus) :
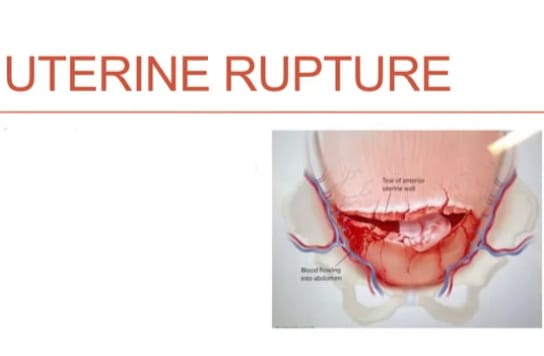
- If there is a breakdown in the continuity of the uterine wall at any time during pregnancy, this condition is called Rupture of the Uterus. This is an obstetric emergency that occurs during labor, sometimes during late pregnancy.
- A breakdown in the continuity of the uterine wall (endometrium, myometrium, and serosa) occurs after 28 weeks of pregnancy. This is called rupture of the uterus. In which small ruptures occurring in the early months are called perforation.
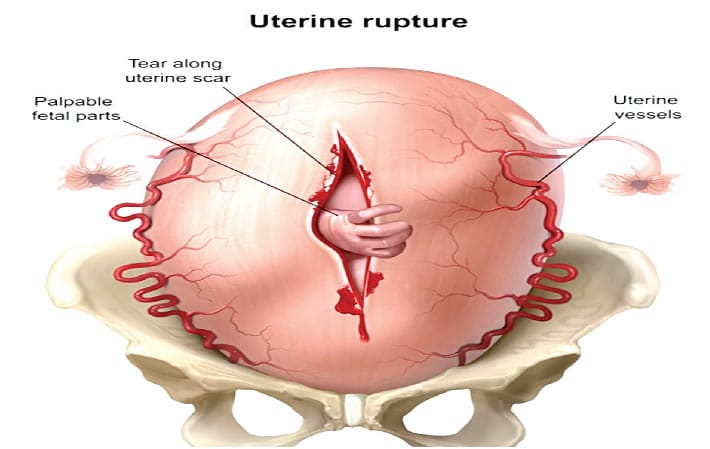
Types Of Uterine Rupture (ટીપ્સ ઓટેરાઇન રુપચ્ચર) :
1.Complete Rupture,
2.Incomplete Rupture.
1.Complete Rupture: Complete rupture is the sudden rupture of the uterus along with its peritoneal covering. It occurs mostly due to scar loosening in the upper segment and in obstetric and non-obstructive type spontaneous rupture. In complete rupture, the fetus comes out of the uterus with or without the placenta.
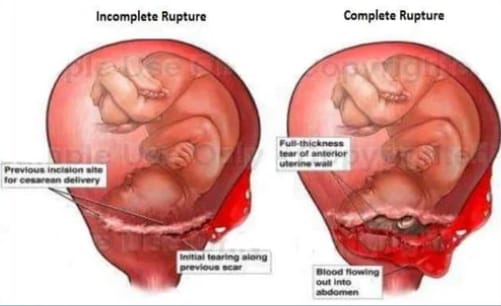
2. Incomplete Rupture: In incomplete rupture, the peritoneum is intact, i.e. there is no involvement of the peritoneal membrane and it is mostly caused by extension of the lower segment scar/cervical scar. In this, the fetus and placenta remain inside the uterine cavity. Or parts of the fetus are occupied in the layers between the broad ligaments.
Etiology:
Spontaneous rupture,
Scar rupture,
Iatrogenic/traumatic rupture.
Spontaneous rupture:
Dilatation and curettage operation or manual removal of placenta If the uterine wall is previously damaged,
grand multipara,
congenital malformation of the uterus, then spontaneous rupture occurs during pregnancy. It mostly occurs during the last trimester.
Uterine rupture can occur due to obstructed labor (obstructive rupture) and grand multipara (non-obstructive rupture) during labor.
Scar rupture:
Uterine rupture occurs due to classical cesarean or hysterotomy during pregnancy and labor.
Iatrogenic/Traumatic Rupture:
Oxytocin,
Prostaglandins,
Forcible external version,
Blowing on the abdomen,
Internal podelic version,
Manual removal of placenta,
Forcep or breech extraction,
Oxytocin and destructive operations cause uterine rupture.
Warning sign of ruptured uterus:
Intermittent pain on the right side as the uterus rotates on its axis and tilts to the right side.
Lower abdominal pain.
Pulse rate less than 100/minute.
Chances of shock increase.
In these cases, when the abdomen is opened, the baby is found to be dead.
Vaginal bleeding.
Dull abdominal pain.
Sign And Symptoms:
- Acute abdominal pain,
- Sudden and severe pain in the abdomen.
- Vaginal bleeding.
- Profuse and sudden vaginal bleeding.
- Decreased fetal heart rate.
- Fetal movement decreases or is absent.
- Hypotension (low blood pressure due to blood loss).
- Tachycardia (increased maternal heart rate due to shock).
- Signs of shock such as pallor, diaphoresis, and confusion.
- Fetal body parts become palpable.
- Abdominal tenderness.
- Changes in uterine tone, such as uterine hypertonicity or hypotonicity.
Diagnostic Evaluation:
- History Collection,
- Physical Examination,
- Ultrasound,
- Fetal Heart Rate Monitoring,
- Laboratory Tests,
- Complete Blood Count Test,
- CT Scan,
- MRI (Magnetic Resonance Imaging),
- Laparotomy.
Management:
- Proper antenatal care to pregnant women.
- Screening for cases of obstructed labor, previous cesarean section, hysterotomy, myomectomy and grand multipara, etc. and referring them for Level II care.
- If the patient is severe, resuscitation is done. It is life saving.
- Like,
a.Inj. Morphine sulphate 15 mg I.M is given.
b. Infusion of 5% dextrose and Ringer lactate is started.
c Blood is arranged for immediate transfusion. - The patient is given antibiotics such as:
- Inj. cefotaxime 1g I/V × 6 hourly.
- Inj. gentamicin 80 g I/M × 8 hourly.
- The patient’s pulse and blood pressure are checked every 15 minutes.
- The patient and her husband should be informed about the possibility of hysterectomy and sterilization and their consent should be obtained.
- The patient is prepared for laparotomy.
- Immediate and quick laparotomy is performed under general anesthesia through a longitudinal incision.
- If the patient’s condition is low, then a subtotal hysterectomy is performed quickly.
- When the patient’s condition permits and there is colporrhexis, then a complete hysterectomy is performed.
- Depending on the clinical condition, either a laparotomy is performed after resuscitation or, in acute conditions, resuscitation and laparotomy are performed together.
- After laparotomy, hysterectomy is the surgery for uterine rupture unless there is a sufficient reason to preserve it.
- In cases of scar rupture, repair is performed where the margins are clear.
- In patients with clean cut scar rupture who have the desired number of children, repair and sterilization are performed.
- If rupture occurs outside the hospital, the patient is immediately shifted to a larger hospital.
- The patient is kept cool and comfortable.
- The patient should be provided with appropriate pain relieving drugs such as,
Pethidine (100 mg) - If the above sterile solutions are not available, shock is treated by elevating the feet in bed and giving intravenous infusion of saline or glucose-saline or rectal infusion of tap water.
Nursing Management:
- Mandatory hospital delivery of high risk mothers.
- Maternal shock or fetal distress is a warning sign for the midwife.
- Monitoring of maternal vital signs and fetal heart sound (F.H.S.) is done.
- Keep the mother on a ventilator.
- Call a doctor at signs of complete or incomplete rupture.
- Transfer the mother to a well-equipped hospital in the community.
- Assist in resuscitation, medical and surgical management of the mother.
- Provide reassurance to the mother, husband and family members.
Post Partum Hemorrhage ( PPH ):
- Postpartum hemorrhage is a condition in which excessive amounts of bleeding occur from the genital tract after the birth of the baby until the end of the postpartum period (the period after the birth of the baby up to 6 weeks) that adversely affects the general condition of the mother, as evidenced by an increase in pulse rate and a fall in blood pressure. So this condition is called postpartum hemorrhage (PPH).
- If there is 500 ml or more of blood loss after vaginal delivery, 1000 ml or more after cesarean section,
and ,
if there is 1500 ml or more of blood loss after cesarean hysterectomy, then this condition is called postpartum hemorrhage (PPH).
Types of Postpartum Hemorrhage (PPH).
There are two main types of postpartum hemorrhage:
1) Primary postpartum Hemorrhage,
2) Secondary Postpartum Hemorrhage.
1) Primary Postpartum Hemorrhage: Bleeding that occurs within 24 hours after the birth of the baby is called primary postpartum hemorrhage. It usually occurs in the first two hours after delivery. Its other two types are:
a) Third stage hemorrhage
b) True postpartum hemorrhage
a) Third stage hemorrhage:
Third stage hemorrhage occurs before the expulsion of the placenta.
b) True postpartum hemorrhage: True postpartum hemorrhage occurs within 24 hours after the expulsion of the placenta.
2) Secondary postpartum hemorrhage: Bleeding occurring after 24 hours after the birth of the baby and during the postpartum period (up to 6 weeks) is called delayed postpartum hemorrhage, late postpartum hemorrhage or secondary postpartum hemorrhage.
Etiology:
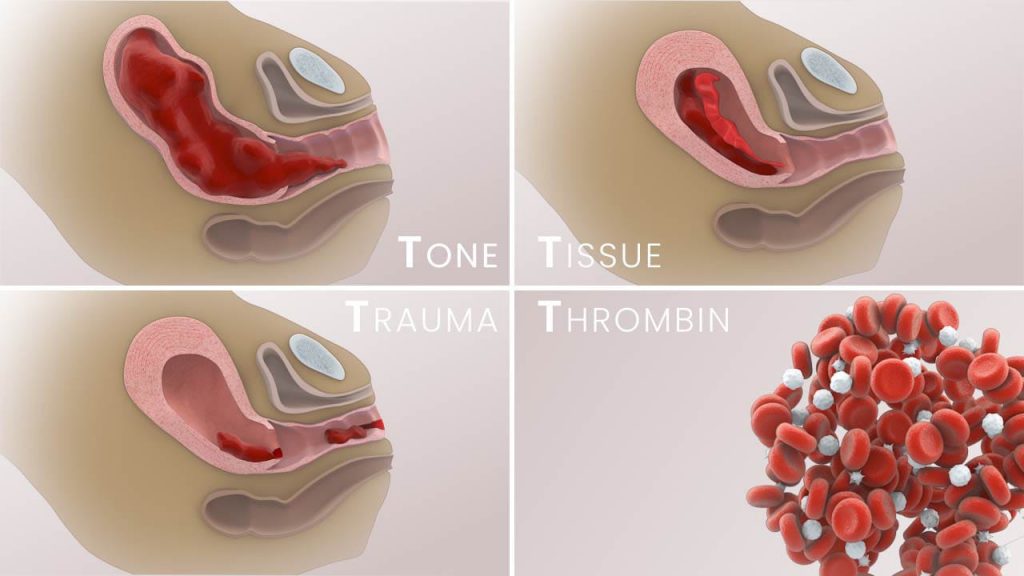
1) Atonic uterus(tone),
2) Traumatic (Trauma),
3) Retained Tissue (Tissue),
4) Blood Coagulation Disorder (Thrombin).
1) Atonic Uterus: 80% of postpartum hemorrhages are caused by atonic uterus. In this, the uterine sinus ruptures after the placenta separates, due to which the uterine muscles do not contract and retract properly, and the building continues, which can lead to the condition of postpartum hemorrhage. It is seen in the following conditions:
Grandmultipara,
Multiple Pregnancy,
Hydroamnios,
Over distension of the uterus in a large baby,
Malnutrition and anemia,
Antepartum hemorrhage, Prolonged labor,
Anesthesia,
Use of oxytocin for induction or augmentation of labor,
Malformation of the uterus,
Uterine fibroids,
Properly managed third stage of labor,
Retained placenta
2) Traumatic: About 20% of postpartum hemorrhage (PPH) is caused by trauma to the genital tract after operative delivery and involves the cervix, vagina, perineum, paraurethral region and ruptures the uterus.
3) Retained Tissue: Postpartum hemorrhage can occur due to bits of placenta and blood clots remaining in the uterus.
4) Blood coagulation disorders: Abruptio placentae, jaundice, thrombocytopenic purpura, HELLP syndrome, intrauterine death or sepsis.
Signs and symptoms of primary postpartum hemorrhage:
- Vaginal bleeding is Most often seen externally.
The effects of blood loss depend on the pre-delivery hemoglobin level, the degree of hypervolemia, and the rate of blood loss. - Changes in maternal vitals, i.e. blood pressure, are seen after a blood volume loss of 20 to 25%. Rarely, rapid blood loss can cause death within minutes.
On the abdomen and uterus:
- Traumatic hemorrhage is contracted and atonic hemorrhage is flabby and hard to massage.
Management of Primary Postpartum Hemorrhage:
- Postpartum hemorrhage is a major cause of maternal morbidity and mortality and cannot always be prevented, but its incidence can be reduced by identifying its risk factors.
Preventive measures for postpartum hemorrhage:
- Antenatal:
Make efforts to improve the health status of the woman and prevent anemia. - High risk multipara delivery should be done in a well equipped hospital.
- Every patient should have their blood group done.
- Previous cesarean delivery should be confirmed by ultrasonography or M. R. I. Placenta accreta can be detected by observing the location of the placenta.
- Delivery in morbid adherent placenta should be done by a senior obstetrician.
Intranatal:
- Active management of the third stage can reduce postpartum hemorrhage by about 60%.
- If labor has been induced or augmented with oxytocin, oxytocin infusion should be given for at least one hour after delivery.
- In difficult labor or instrumental delivery, observe for utero-vaginal canal trauma after delivery.
- After delivery, observe for about two hours during which the uterus is hard and contracted before sending to the ward.
- Forces, Giving local or epidural anesthesia in ventouse or breech delivery.
- Spontaneous separation and delivery of placenta in cesarean section.
- Examination of placenta and membranes after delivery.
Antenatal management:
- Assess the health status of the patient, especially the patient’s hemoglobin level should be maintained properly.
- If the hemoglobin level is properly maintained, any complications due to blood loss can be prevented.
- Transfer the mother who is at high risk to a well-equipped hospital.
Intranatal Management:
- Administer sedative and analgesic drugs during the intranatal period.
- Avoid hasty delivery. The baby’s head is delivered. Then its trunk takes at least 2 to 3 minutes to be delivered.
- Fully manage the care of the third stage in high-risk patients.
- After delivery of the placenta, properly assess whether the placenta has been delivered completely or not and assess whether any bits of placenta are retained in the uterus.
- Injection oxytocin is 10 units / IM or if 20-40 units, oxytocin should be added to 1000 ml normal saline or Ringer lactate solution and infused.
- Explore the uterovaginal canal and note whether there is any trauma due to difficult labor or instrumental delivery.
- Keep the patient under observation for at least two hours after delivery.
- Continuously note the mother’s vital signs during that time.
- Call health care personnel for additional information.
- Administer two large gauzes intravenously through a cannula.
- Send the blood to the laboratory for blood grouping and cross-matching.
- Administer adequate amount of intravenous fluid to the mother.
- Properly note the mother’s vital signs.
- If bleeding is due to atonic uterus, gently rub the fundus with the fingertips.
- If it is soft and relaxed, gently massage the fundus in a circular motion to properly remove blood clots.
- If bits of placenta or clot are retained in the uterine cavity, remove them properly.
- Further repeat the injection of oxytocin.
- To return the uterus to its tone, administer methyl PGF2 intramuscularly or transabdominally into the myometrium and repeat as needed.
- If the uterus is still atonic, perform manual compression.
- By manual compression, pressure can be applied to the placental side to control bleeding.
- Tight intrauterine packing can be done under general anesthesia to control postpartum hemorrhage.
- If the above measures fail, hysterectomy is performed as a last resort.
General Steps for Management of Postpartum Hemorrhage:
- Start intravenous therapy,
- Properly catheterize the mother.
- Start blood transfusion if necessary.
- Note whether the placenta has been delivered properly or not and if the placenta has not been delivered, assess whether it is separate or unseparated properly.
- If the placenta is If the placenta is not separated, remove it bimanually.
- If the placenta is undelivered but separated, assess where the placenta is present in the uterine cavity. That is, assess whether the placenta is present in the lower segment of the uterine cavity, in the part of the cervix or on the vagina.
- If the placenta is present in the lower segment of the uterine cavity, remove it by controlled cord traction.
- If controlled cord traction fails, perform bimanual compression and if that also fails, perform hysterectomy as a last resort.
- If the separated placenta is on the cervix or vagina, grasp it and remove it. If that fails, Remove the placenta by bimanual compression and if that fails, perform hysterectomy as a last resort.
- If the placenta is delivered, remove the retained bits of placenta in the uterine cavity properly.
- If the placenta clots cannot be removed, provide injection of Syntocin 40 IU International Unit 1 Liter Intravenous Infusion. Due to which the patient’s clots can be removed.
- Then assess the mother’s complete vital signs.
- Provide the mother with a properly comfortable position and advise her to take proper rest.
- Provide the mother with proper reassurance.
2) Secondary Post Partum hemorrhage:
- Bleeding that occurs after 24 hours after the birth of the baby and up to 6 weeks after delivery is called delayed partum hemorrhage, late partum hemorrhage or secondary post-partum hemorrhage. It usually takes 8 to 14 days to build up.
Etiology of Secondary Postpartum Hemorrhage:
- Because of bits of cotyledon or membrane remaining in the uterine cavity,
- Because of infection,
- Because of endometritis,
- If there is placental site subinvolution,
- Because of the wound of cesarean section,
- Because of estrogen therapy,
- Because of cervical carcinoma,
- Because of placental polyps,
- Due to premature inversion of the uterus,
Signs and Symptoms of Secondary Postpartum Hemorrhage:
- Heavy lochia discharge that appears bright red in color,
- Lochia discharge being offensive,
- Fever,
- High pulse rate,
- Subinvolution of uterus,
- Anemia,
- Sepsis,
Nursing Management of Secondary Postpartum Hemorrhage:
- Properly assess the amount of blood loss.
- Properly provide blood transfusion to the patient.
- Properly identify the cause of postpartum hemorrhage.
- Provide 10 units of inj.oxytocin IM (intramuscular) or if intravenous (IV) then add 20 units of oxytocin to 500 ml of normal saline or ring-rectified solution and provide infusion to the patient to prevent post-partum hemorrhage.
- Provide proper antibiotic medication to the patient.
- Advise the patient to take complete bed rest.
- If the patient has any retained bits of placenta, then To remove properly.
- If the patient is bleeding even in a minor amount, then it should not be ignored as it can be an alarm signal of postpartum hemorrhage.
- Properly remove the retained product by sponge holding, ovum forceps or gentle curettage.
- If the bleeding is due to trauma to the cervico-vaginal canal, then it should be controlled with hemostatic sutures.
- If the patient is delivered in an unhygienic environment, administer anti-tetanus serum and anti-gas gangrene serum to the patient.
- If the patient is anemic, provide blood transfusion.
- Properly monitor the patient’s vital signs, initially every four hours, and then twice a day.
- Give the patient ferrous gluconate (300 mg TDS) or ferrous sulfate (200 mg TDS) Provide orally.
- Properly provide folic acid (5 mg) to the patient.
- Provide proper work and comfortable environment to the mother.
- Advise the mother to take proper follow-up.
General Management of Postpartum Hemorrhage:
Postpartum hemorrhage is a major cause of maternal morbidity and mortality, therefore, proper and effective management of postpartum hemorrhage is important to prevent complications.
Management of postpartum hemorrhage involves a systemic approach that includes controlling bleeding, stabilizing the mother, and identifying the cause of postpartum hemorrhage.
1) Immediate Action:
- Early Recognition
Early identification of signs and symptoms of postpartum hemorrhage such as excessive bleeding (more than 500 ml if vaginal delivery and more than 1000 ml if cesarean section), tachycardia, hypotension, pallor and signs of shock. - Call for Help
Notify senior obstetrician, anesthesiologist and other necessary health care personnel to assist in the management of postpartum hemorrhage. Do. - Assessment Quantity of Blood Loss
Properly assess the amount of blood loss. - Clinical Assessment
Perform a focused clinical examination to assess uterine tone, size, and any signs of trauma and to assess whether retained product is present. - Establish intravenous (IV) access
Post Large-sized intravenous (IV) access should be established for rapid fluid administration and medication administration in women with parturient hemorrhage. - Oxygen Administration
Provide supplementary oxygen to maintain tissue oxygenation.
2) Pharmacological Management
- Uterotonic Medication
Uterotonic agents should be administered to stimulate uterine contractions and control bleeding. - Oxytocin
Oxytocin is the first-line agent in which a bolus dose of 10 to 40 units in 1 liter of crystalloid solution should be given as an infusion over 10 to 30 minutes.
Followed by
Infusion of 40 units in 1 liter of IV fluid over 4-6 hours. - Misoprostol
If oxytocin is not available, 800 mcg rectally and Administer 600 orally.
3) Non-pharmacological management:
- Uterine massage
Gently massage the uterine fundus to enhance uterine contractions and control bleeding. - Balloon tamponade
After giving uterotonic drugs in postpartum hemorrhage and uterine If bleeding continues even after massage, use a balloon tamponade (Bakery balloon and Follis catheter) to apply pressure against the uterine wall to achieve hemostasis and control bleeding.
4) Surgical intervention
- Manual removal of placenta
If there is evidence of placental tissue in the uterine cavity, provide anesthesia Manual removal of the placenta. - Compression sutures
Uterine compression sutures are applied to mechanically compress the uterus and control bleeding. - Uterine artery ligation
Uterine artery ligation is performed as a surgical option in some cases to reduce blood flow to the uterus. - Hysterectomy
When bleeding cannot be controlled by other measures and the patient’s condition is deteriorating Hysterectomy is performed as an emergency measure.
5) Supportive Care and Monitoring:
- Fluid Administration
To improve the patient’s tissue perfusion, administer adequate intravenous fluids to the patient, such as:
Normal saline
Or Ringer lactate solution. - Blood Transfusion
When there is excessive bleeding, provide blood transfusions as needed. - Monitoring
The patient’s vital signs, urine output, and level of consciousness Continuous monitoring. - Repeat hematological and biochemical tests to assess response to treatment.
- Psychological support
Postpartum hemorrhage (PPH) is a traumatic condition, so provide proper psychological support to the patient and her family members.
6) Prevention
- Antenatal Care
Early identification of risk factors for postpartum hemorrhage during the antenatal period so that they can be managed early and complications can be prevented. - Active Management of Third Stage of Labor
Use of prophylactic uterotonic medication to prevent postpartum hemorrhage and reduce the risk of uterine atony. - Skilled Birth Attendance Trained personnel should be available to immediately recognize and manage obstetric emergencies.
7) Follow-up and Documentation:
- Post Management Care
Advise the patient to take proper follow-up so that recovery can be monitored and if the patient has an anemic condition, it can also be assessed. - Documentation
Properly document the event that occurred, the interventions performed for it, and the patient’s response to the treatment, etc. - Thus, proper management of postpartum hemorrhage is important to prevent complications caused by conditions like postpartum hemorrhage in women after childbirth.
Atonic Uterus (Atonic Uterus):
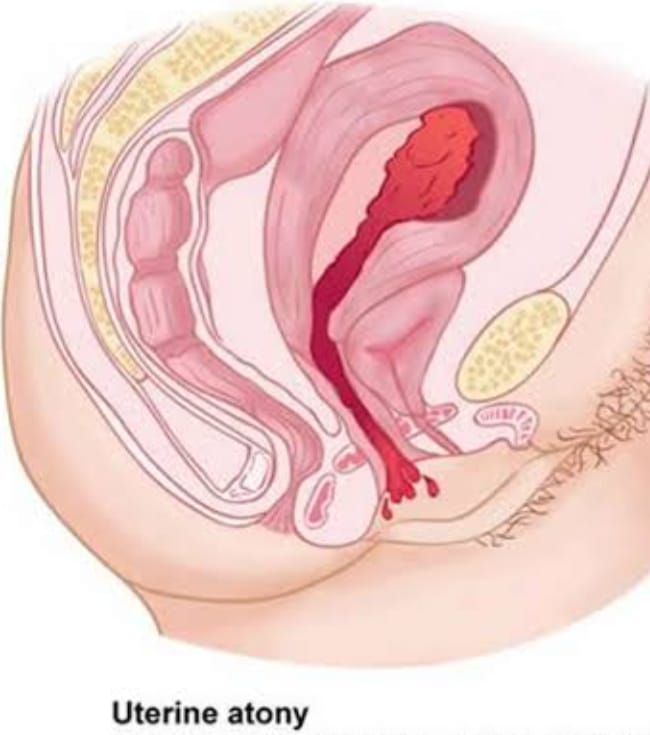
- Atonic uterus is a condition in which the uterus fails to contract with normal strength, duration, and interval during childbirth. In other words, the uterus is weak and lacks normal tone. It can arise due to serious complications of the third stage of pregnancy. A uterus without tone and which is the cause of PPH. In which the uterus relaxes.
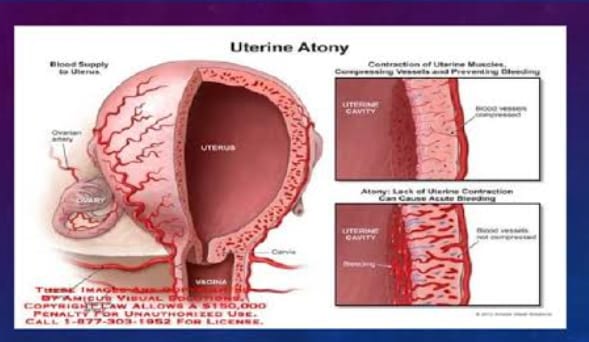
Risk Factors or Causes of Atonic Uterus:
- Placenta Previa or Abruptio Placenta,
- Retained Placenta,
- Incomplete Separation of Placenta,
- If there are some missing fragments in the placenta such as the absence of part of the maternal surface, then the remaining placental tissue should be properly removed.
- Excessive bleeding,
- Increases heart rate,
- Low blood Pressure,
- Uterine enlargement,
- Pelvic pain and discomfort,
- Looking for signs of shock.
- History Collection,
- Physical Examination,
- Vital Sign Monitoring,
- Hemoglobin and Hematocrit Level Assessment,
- Ultrasound,
- Bimanual Examination,
- Blood coagulation test.
Sign And Symptoms:
Diagnostic Evaluation:
Management:
1. Uterine massage:
- Uterine massage is the first step in the management of atony of the uterus. Uterine massage is performed until uterine contractions start continuously.
2. Pharmacological therapy:
- Oxytocin: This initiates rhythmic contractions.
- Compresses the spiral arteries of the uterus, which helps prevent bleeding.
- Methylergometrine:
It is not used due to its side effects such as hypertension. - Carboprost can be used in cases where oxytocin cannot be used. Prostaglandins are never given intravenously as this can be fatal.
- If necessary, arrange for blood transfusions and provide blood transfusions.
- If bleeding continues:
- Examine the placenta for completeness.
- If the placenta contains missing fragments such as the absence of part of the maternal surface, remove the remaining placental tissue properly. To do.
- Properly assess clotting status. If a clot does not form after 7 minutes or if a soft clot breaks down easily, it suggests a condition of coagulopathy. Which should be managed immediately.
- If bleeding continues even after taking the above measures, follow the points below.
- Perform manual compression until bleeding stops and the uterus starts to contract.
- Alternatively compress the aorta.
- If bleeding continues, the uterus or Ligation of the utero-ovarian artery.
- If bleeding does not stop even after ligation, perform a subtotal hysterectomy.
Injuries To The Birth Canal:
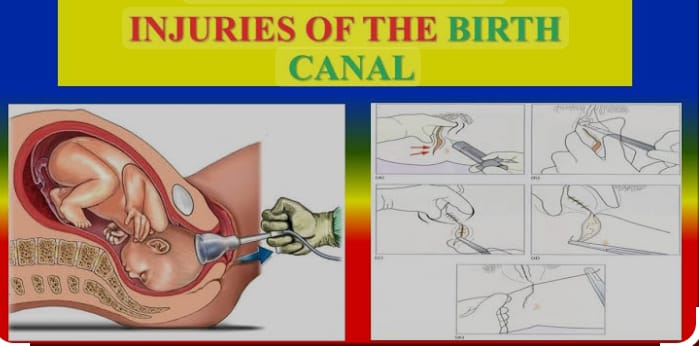
- Birth canal ie Any structure that forms the birth canal, if injured during delivery, labor or childbirth, is called a birth canal injury. During childbirth, the genital tract is commonly injured. In this injury,
- Vulvar injury
- Perineal injury
- Vaginal injury
- Cervical injury
- Pelvic hematoma
- Rupture of the Uterus
- Visceral injury involving the bladder, rectum, and urethra.
Injuries to Vulva:
- If the vulva is injured during childbirth and labor, this The condition is called injury to the vulva.
- Common sites include,
posteriorly vulvar skin laceration,
involvement of a para-urethral tear on the inner aspect of the labia minora.
Injury to the Perineum:
- Perineal injury is usually caused by mismanagement of the second stage of labor.
Etiology:
- The reasons may be:
- This causes excessive stretching of the perineum Stretching:
Large baby
Face to pubis arch
Shoulder delivery (posteriorly one)
Forces delivery - Due to rapid stretching of the perineum:
- Due to rapid delivery of the head during uterine contractions.
Precipitate labor.
Due to breech delivery. - Due to inelastic perineum and rigid perineum during elderly primi gravida.
Due to scar formation during previous operations Due to.
Ex: Episiotomy or perineorrhaphy,
Vulval edema.
Degrees of Perineal Tear:
Degrees of Perineal Tear
There are three degrees of perineal tear:
1st degree: In this, there is an involvement of laceration, in which the hymen, forechest, lower part of the vagina and perineal skin are involved, but the perineal body remains intact.
2nd degree: In this, there is an involvement of the posterior vaginal wall in the laceration. And there is involvement of varying degrees of the perineal body. And then the anal sphincter is involved.
3rd degree (complete): It involves major laceration of the posterior vaginal wall and also involves the perineal body surface and involves the anal sphincter and may or may not involve the anal canal and sometimes the rectum.
Management:
- The recent tear should be repaired immediately after delivery of the placenta as this reduces the chances of infection and minimizes blood loss.
- If the wound is delayed, i.e., more than 24 hours, it is repaired.
- However, if it is delayed more than 24 hours, then the complete tear should be repaired after 3 months.
- A 3rd degree tear requires good light exposure, adequate assistance including an anesthetist, and necessary instruments.
- The repair is done in the lithotomy position. The vagina, vulva, and perineal region are swabbed with antiseptic Dettol solution.
- The perineal skin, vaginal mucosa, and perineal muscles surrounding the tear are infiltrated with 1% lignocaine hydrochloride (10-20 ml).
- In a complete perineal tear, the rectum and anal canal are first closed from top to bottom with chromic catgut No. 00 using interrupted stitches using a covered or traumatic needle, and a knot is placed inside the lumen.
- The muscle wall and pararectal fascia are then sutured again using interrupted stitches using a traumatic needle.
- The torn end of the sphincter ani externus exposed by Ellis forceps is reconstructed with a figure of eight stitch using 0′ chromic catgut number supplemented by other interrupted sutures. ‘
Thus, a 3rd degree perineal tear is converted into a 2nd degree.
If the tear is incomplete, the vaginal mucosa should be sutured first. The first suture is placed at or above the apex of the tear. - The vaginal wall is sutured with interrupted sutures using chromic catgut number ‘0’ covered round body needle from top to bottom until it reaches the forechest.
- Next the perineal muscles are repaired with interrupted sutures using No. 0 catgut.
- The perineal skin is sutured with chromic catgut or nylon silicone gut using a cutting needle.
- After suturing, daily care of the perineal skin is done.
- The wound should be dressed after each urination and defecation to keep it clean and dry. Dressing is done by swabbing with a cotton swab soaked in an antiseptic solution and then applying an antiseptic powder or ointment. (Furacin or Neosporin).
- To relieve pain, magnesium sulfate compresses or infrared heat can be used. Analgesic medication can be given when needed.
- The patient is allowed to get out of bed after 24 hours.
- The patient is given a low residual diet consisting of milk, bread, eggs, biscuits, fish, sweets etc. from the second day onwards.
- The patient is given Milk of Magnesia 8 ml twice a day starting from the second day and increasing to 15 ml on the third day.
- If the patient fails to pass stool even with Milk of Magnesia, the patient is given a compound enema (olive oil, liquid paraffin, glycerin and normal swine).
- For 5-7 days, one of these intestinal antiseptics is to be continued or as prescribed by the doctor, namely:
- Tab. Neomycin 250 mg four times a day.
Cap. Sulphathiazole 1 mg BD daily.
Tab. Metronidazole 2 tablets four times a day.
Tab. Sulphaguanidine 2 tablets four times a day.
Vaginal Tear :
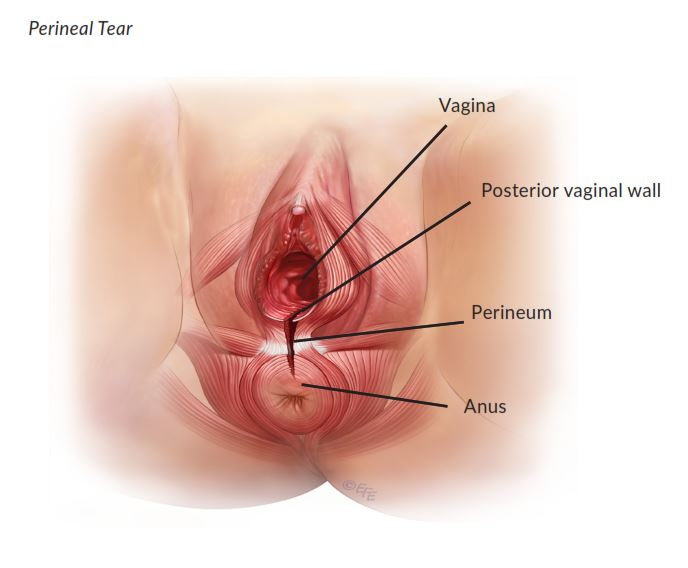
Isolated vaginal laceration/laceration without involvement of the perineum or cervix is commonly seen after instrumental or manipulative delivery. In these cases, the laceration is extensive and often associated with brisk hemorrhage. The TER may extend in any direction and may be either superficially limited or deep into the paravaginal tissues.
Nursing Management:
- TER associated with brisk hemorrhage requires exploration under general anesthesia with good lighting.
- TER is a common Repair is done using chromic catgut No. 0 with interrupted and continuous sutures.
- In addition to sutures, in cases of extensive lacerations, hemostasis can be achieved by intravaginal plugging with roller gauze soaked in glycerin and acriflavine.
- The plug should be removed after 24 hours.
Calporexis (Calporexis):
- Rupture of the vaginal vault is called colporrhexis.
Types:
- 1.Primary: Where only the vault is involved.
- 2.Secondary: When it is associated with cervical turbinate (normal) is.
- It is said to be complete when the peritoneum is opened.
Treatment:
- If the tear is limited to the vault including the accessible part of the cervix, the repair is done from below.
- If the cervical tear is lower In the segment or to the major branches of the uterine vessels extends up to the high up. After the damage, laparotomy is performed together with resuscitative measures.
Cervical Tear :
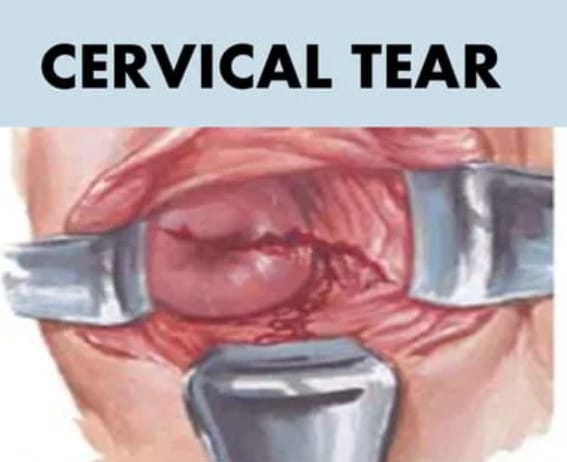
- During first deliveries, a minor degree of cervical laceration is inevitable. Extensive injury is rare. Cervical laceration involves a laceration or injury to the cervix, which is the lower part of the uterus that connects to the vagina. This can happen during childbirth, especially if there is prolonged labor or if there is significant pressure.
- Cervical lacerations can vary in severity, ranging from minor lacerations to more extensive lacerations that may require medical intervention. Symptoms may include bleeding, pain, and difficulty urinating or having a bowel movement. Proper assessment and care are important to prevent complications.
Etiology:
- Due to prolonged labor process,
- Due to forceps or vacuum expression,
- Due to large fetal size,
- Due to multiple pregnancy,
- Due to abnormal fetal position,
- Due to previous cervical surgery,
- Due to rigid cervix,
- Due to strong uterine contractions.
Sign And Symptoms (लक्षनो तथा चिन्हो (सिन एंड अधिक्ष Symptoms):
- Vaginal erection,
- Pelvic pain,
- Abnormal discharge,
- Difficulties in bowel movements and urination.
- Visible tar is visible.
Diagnostic Evaluation (Diagnostic Evaluation) :
- History Collection,
- Physical Examination,
- Speculum Examination,
- Ultrasound,
- Colposcopy,
- Laboratory tests.
Danger:
Early danger,
Late danger
- Early Danger:
Deep cervical tear causes involvement of major blood vessels which can lead to severe postpartum hemorrhage.
Pelvic cellulitis.
Thrombophlebitis. - Late Danger:
Ectropion,
Cervical incompetence with mid-trimester abortion.
Management:
- A cervical tear associated with bleeding should be repaired immediately after delivery of the placenta.
- It should be repaired under general anesthesia in the lithotomy position with good light.
- In this, the anterior and posterior margins of the torn cervix are closed with sponge-holding forceps Grasp.
- The assistance gently pushes the fundus downward. This makes the tar more accessible for effective suturing.
- First, the apex has to be identified and the first vertical mattress is sutured using a covered round body needle and chromic catgut number ‘0’ placed just above the apex. The wall thickness of the cervix is measured.
- Bleeding stops immediately.
- A similar mattress suture is used to repair the remaining scar. (These sutures prevent rolling of the edges).
- If there is a condition of cervical tear, provide the woman with lithotomy position.
- Properly repair the tear by providing general anesthesia.
- Properly clean the local area by exposing it.
- Properly grasp the anterior and posterior margins of the cervix with sponge-holding forceps.
- Ask the assistant to lower the fundus. Due to this, the tar is more accessible and the sutures can be done effectively.
- Identify the apex and suture it using a round body needle with chromic catgut number O through the first vertical mattress above the apex. Make sure you have taken the entire thickness of the cervix.
Nursing Management:
- Properly assess the woman’s condition.
- Properly check the woman’s vital signs.
- How many Properly check the amount of blood loss.
- Inform the obstetrician and provide assistance in repairing the tear immediately.
- Maintain proper aseptic technique while repairing.
- Properly provide antibiotic medication after providing a test dose.
- Properly provide psychological support to the woman and her family members.
- Providing proper work and environment to women.
Pelvic Hematoma:
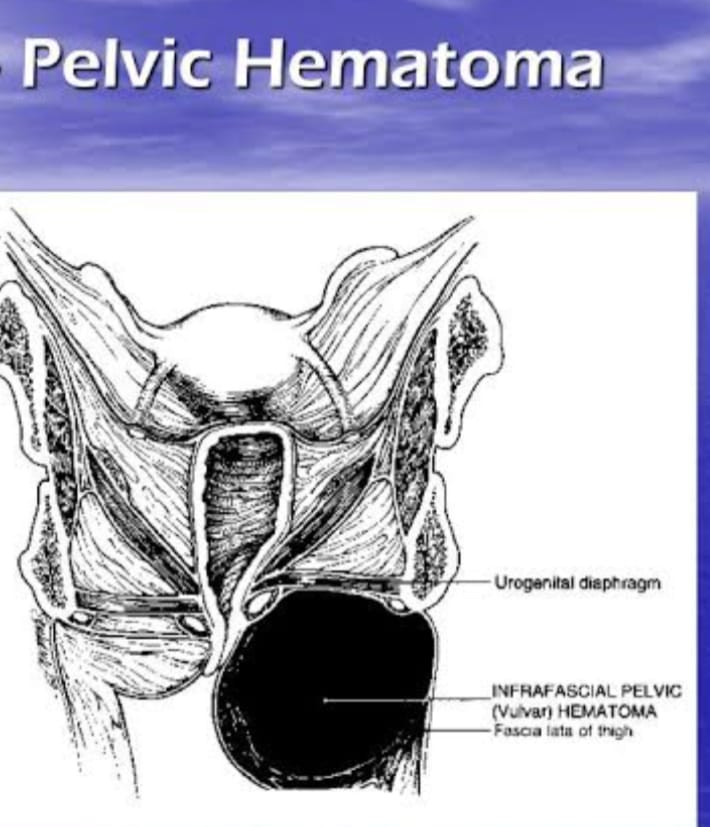
- Pelvic hematoma is a condition in which blood collects anywhere between the pelvic peritoneum and the perineal skin. This condition is called pelvic hematoma.
Anatomical Type:
Depending on the hematoma, whether it is present below or above the levator ani, it is called:
1. Infralevator hematoma (common)
2. Supralevator hematoma (rare)
1. Infralevator hematoma (common): The most common is a vulval hematoma. Vulval hematoma is a form of concealed traumatic hemorrhage in the connective tissues of the vulva and vagina.
Etiology:
- It can be caused by:
- Vaginal or perineal wounds or episiotomy wounds such as Due to improper hemostasis during repair.
- Failure to take precautions while suturing the apex of the uterus.
- Failure to eliminate dead space while suturing the vaginal wall.
- Rupture of the perovaginal venous plexus either spontaneously or after instrumental delivery
- Rupture of subcutaneous veins.
Sign And Symptoms (Signs And Symptoms):
- Persistent and severe pain in the perineal region.
- When there is extension into the ischio-rectal fossa, there may be rectal tenesmus or bearing down aftertaste.
- Urinary retention may also occur.
- Signs of pelvic hematoma:
- Variable degree of shock.
- Local On examination, there may be a tense swelling on the vulva that is dusky purple in color and tender to the touch.
Management:
- Provide general anesthesia and early detection of hematoma within the operating theater.
- All procedures should be performed with proper aseptic precautions Maintain and perform.
- Resuscitative measures are taken at the same time.
- The wound is reopened or an incision is made along the line of maximal distension, usually near the introitus.
- The blood clot is scooped out and the bleeding point is secured.
- Usually, a oozing surface is visible near the sutures and a rubber drain can be placed in that area for 24 hours. is.
- Prophylactically, antibiotics are given or drainage of the hematoma is done under general anesthesia. Analgesic medication is provided to manage pain.
Supralevator hematoma:
This is a rare type of hematoma and is not commonly seen.
Etiology:
- The causes of supralevator hematoma are:
- Cervical laceration or primary colporrhexis (vault rupture)
Lower uterine segment rupture - Spontaneous rupture of the paravaginal venous plexus adjacent to the vault.
Diagnostic Evaluation:
- Diagnosis is usually late (as pain, vaginal bleeding appear late).
- After delivery, features of unexplained shock and internal hemorrhage increase suspicion.
- On abdominal examination: There is swelling over the inguinal ligament pushing the uterus to contact the lateral side.
- Vaginal examination reveals:
By bulge Occlusion of the vaginal canal.
Boggy swelling belt through the fornix.
Management:
- If there is a condition of shock, treat it immediately.
- Make proper arrangements for laparotomy.
- The broad ligament, which is the anterior leaf of the peritoneum, is incised and the blood is scooped out.
- If visible, the bleeding point is ligated securely.
- To prevent uterine damage, random blind sutures should not be applied.
- If the bleeding is continuous, the anterior division of the internal iliac artery is tied.
Rupture Of The Uterus :
- If there is a breakdown in the continuity of the uterine wall at any time during pregnancy, this condition is called Rupture of the Uterus. This is an obstetric emergency that occurs during labor, sometimes during late pregnancy.
- A breakdown in the continuity of the uterine wall (endometrium, myometrium, and serosa) occurs after 28 weeks of pregnancy. This is called rupture of the uterus. In which small ruptures occurring in the early months are called perforation.
Types of Uterine Rupture:
1.Complete Rupture,
2.Incomplete Rupture.
1.Complete Rupture: Complete rupture is the sudden rupture of the uterus along with its peritoneal covering. It is most often caused by scar tissue in the upper segment and is associated with obstetric and non-obstructive It occurs in spontaneous rupture of the type. In complete rupture, the fetus comes out of the uterus with or without the placenta.
2. Incomplete rupture: In complete rupture, the peritoneum is intact, i.e. there is no involvement of the peritoneal membrane and it is mostly caused by extension of the lower segment scar/cervical scar. In this, the fetus and placenta remain inside the uterine cavity. Or parts of the fetus are occupied in the layers between the broad ligaments.
Etiology:
Spontaneous rupture,
Scar rupture,
Iatrogenic/traumatic rupture.
Spontaneous rupture:
Dilatation and curettage operation or manual removal of placenta If the uterine wall is previously damaged,
grand multipara,
congenital malformation of the uterus, then spontaneous rupture occurs during pregnancy. It mostly occurs during the last trimester.
Uterine rupture can occur due to obstructed labor (obstructive rupture) and grand multipara (non-obstructive rupture) during labor.
Scar rupture:
Uterine rupture occurs due to classical cesarean or hysterotomy during pregnancy and labor.
Iatrogenic/Traumatic Rupture:
Oxytocin,
Prostaglandins,
Forcible external version,
Blowing on the abdomen,
Internal podelic version,
Manual removal of placenta,
Forcep or breech extraction,
Oxytocin and destructive operations cause uterine rupture.
Warning signs of ruptured uterus:
- Intermittent pain on the right side as the uterus rotates on its axis and tilts to the right side.
- Lower abdominal pain.
- Pulse rate less than 100/minute.
- Chances of shock increase.
- In these cases, when the abdomen is opened is, the baby is found to be dead.
- Vaginal bleeding.
- Dull abdominal pain.
Sign And Symptoms :
- Acute abdominal pain,
- Sudden and severe pain in the abdomen.
- Vaginal bleeding.
- Profuse and sudden vaginal bleeding.
- Decreased fetal heart rate.
- Fetal movement decreases or is absent.
- Hypotension (low blood pressure due to blood loss).
- Tachycardia (increased maternal heart rate due to shock).
- Signs of shock such as pallor, diaphoresis, and confusion.
- Fetal body parts become palpable.
- Abdominal tenderness.
- Changes in uterine tone, such as uterine hypertonicity or hypotonicity.
Diagnostic Evaluation:
- History collection,
- Physical Examination,
- Ultrasound,
- Fetal Heart Rate Monitoring,
- Laboratory Test,
- Complete Blood Count Test,
- CT Scan,
- MRI(Magnetic Resonance Imaging),
- Laparotomy.
Management:
- Provide proper antenatal care to pregnant women.
- Screening of cases of obstructed labor, previous cesarean section, hysterotomy, myomectomy and grand multipara, etc. and referring them for Level II care.
- If the patient is critical, resuscitation is done. It is life saving.
Like,
a.Inj. Morphine sulphate 15 mg I.M is given.
b.Infusion of 5% dextrose and Ringer lactate is started.
c. Blood is arranged for immediate transfusion. - The patient is given antibiotics such as:
- Inj. cefotaxime 1g I/V × 6 hourly.
Inj. Gentamicin 80 g I/M × 8 hourly. - Check the patient’s pulse and blood pressure every 15 minutes.
- The patient and her husband should be informed about the possibility of hysterectomy and sterilization and their consent should be obtained.
- The patient is prepared for laparotomy.
- Immediate and quick laparotomy are performed under general anesthesia through a longitudinal incision is.
- If the patient’s condition is low, then a subtotal hysterectomy should be performed quickly.
- When the patient’s condition permits and there is colporrhexis, then a complete hysterectomy is performed.
- Depending on the clinical condition, either a laparotomy is performed after resuscitation or in acute conditions, resuscitation and laparotomy are performed together.
- After laparotomy, hysterectomy It is a surgery for uterine rupture unless there is a good reason to preserve it.
- In cases of scar rupture, repair is done where the margins are clear.
- Clean cut scar rupture patients with the desired number of children are repaired and sterilized.
- If the rupture occurs outside the hospital, the patient is immediately transferred to a larger hospital.
- The patient is kept cool and comfortable is.
- Provide the patient with appropriate pain relieving drugs such as,
pethidine (100 mg) - If the above sterile solutions are not available, shock is treated by elevating the feet in bed and giving intravenous infusion of saline or glucose-saline or tap water by rectal infusion.
Nursing Management:
- Mandatory hospital delivery of high risk mothers.
- Maternal shock or fetal distress is a warning sign for the midwife.
- Monitoring the mother’s vital signs and fetal heart sound (F.H.S.).
- Keeping the mother on a breathalyzer.
- Call a doctor at signs of complete or incomplete rupture.
- Transfer the mother to a well-equipped hospital in the community.
- Assist in resuscitation, medical and surgical management of the mother.
- Provide reassurance to the mother, husband and family members.
Visceral injury to other organs (Visceral injury to other organs) :
- Visceral injuries including,
bladder,
rectum,
urethra. - Bladder causes:
trauma,
slugging fistula - Trauma: It can be caused by:
Instrumental vaginal delivery such as destructive operation or forceps delivery especially with Killand forceps. - Abdominal operative procedures such as, ruptured uterus For abdominal operative procedures such as hysterectomy or cesarean section.
- Slopping fistula:
This is gradually becoming rare in developing countries. - It results from the prolonged compression effect on the bladder between the head and the symphysis pubis in obstructed labor.
Diagnostic Evaluation
- History collection,
Physical examination, - Diagnosis is made by:
- Dribbling of urine immediately after operative delivery.
- Passing bloodstained urine after cesarean section or hysterectomy.
Margins are clean with oozing surface Cut.
In sloughing fistula:
- History of prolonged labor
- Dribbling of urine occurs at various intervals
- After delivery (5-7 days).
- Due to devitalized and necrotic margins.
- A chunk of tissue is missing.
Nursing Management:
- In traumatic fistulas, immediate local repair is preferable is.
- In favorable conditions, a self-retaining catheter is introduced and kept in place for 10-14 days or more.
- Urinary antiseptics are administered.
- The patient is advised to wash the bladder daily (not more than 30 ml). The lotion is provided with acriflavinelin 10,000.
- Under favorable conditions, the fistula may close spontaneously. If it fails, it will have to be repaired after 3 months.
- In a sloughing fistula, repair should not be attempted and instead a self-retaining catheter is placed.
- Repair is to be done after 3 months.
- Retained placenta is a condition in which the placenta is not expelled for 30 minutes during the 3rd stage of labor, i.e. after the birth of the baby, i.e. This condition is called retained placenta.
Retained Placenta:

Etiology:
- Causes of retained placenta are:
- The placenta has completely separated but due to poor voluntary expulsive efforts especially in exhausting and prolonged labour the placenta remains retained.
Simple adherent placenta due to uterine atony:
Grand multipara,
Over distension of Uterus,
Due to the condition of prolonged labor,
Uterine malformation,
Due to larger placental surface.
Partial/complete separation of placenta can occur due to retained placenta due to the following:
Constriction ring (hour-glass constriction), Hour-glass constriction occurs due to mismanagement of the 3rd stage of labor, i.e. due to fiddling with the uterus or overzealous massage of the uterus.
Morbid adherent placenta: Partially or rarely complete.
Due to faulty technique to expel the placenta before it separates.
A full bladder stops adequate uterine contractions and retraction, causing the placenta to remain in the uterus. Difficulties in expulsion of the placenta may arise.
Other causes such as,
Poor voluntary expulsive efforts,
Atonic uterus: due to grand multipara, over distension of uterus, prolonged labor, uterine malformation, due to large placental surface area.
Morbid adherent placenta: partial or rarely, complete.
Constriction ring (due to hour-glass constriction).
Attempt to deliver the placenta prematurely.
Sign And Symptoms (Signs and Symptoms):
- Postpartum hemorrhage,
- Uterine atony,
- Foul smelling vaginal discharge,
- Abdominal pain and tenderness,
- Prolonged lochia The condition of being present.
- Symptoms of anemia such as fatigue, weakness and pallor due to blood loss are seen.
Danger:
- Hemorrhage,
- Shock,
- Pupillary sepsis,
- Risk of recurrence in next pregnancy.
Management:
- Complete observation for bleeding during delivery of placenta.
- If the bladder is full, empty it through a catheter.
- If bleeding occurs during this period, manage as per third stage hemorrhage.
- If the placenta is separated, remove it by controlled cord traction.
- Properly note the mother’s vital signs.
- If the placenta is unseparated and retained in the uterine cavity, Manual removal.
- If there are complications with retained placenta, provide treatment and remove the placenta manually.
- Provide proper work and a comfortable environment for the patient.
Inversion Of Uterus:

- Inversion of the uterus is a rare, serious complication of the third stage, in which the uterus protrudes slightly or completely from the inside outwards. This is called inversion of the uterus. The inversion often starts with a dimple in the fundus of the uterus and continues until the uterus is completely inverted outwards. Its incidence is approximately 1 in 20,000 deliveries.
Purple Uterus Degree of Inversion
There are three degrees of inversion of the uterus:
1.First degree
2.Second degree
3.Third degree
1.First degree: In the first degree, the depressed fundus reaches the internal orifice or there is a dimpling in the fundus.
2.Second degree: In this, the body of the uterus is inverted up to the level of the internal orifice. The fundus protrudes into the vagina through the external orifice. In the first and second degree there is incomplete inversion.
3. Third degree (complete inversion): In this stage, the uterus and cervix are completely inverted.
The fundus protrudes outside the vaginal introitus.
In the advanced 3rd degree, there is inversion of the vagina.
The endometrium is visible outside the vulva with or without the placenta.
Etiology:
Spontaneous (40%),
Induced (60%).
Spontaneous (40%):
- Spontaneous inversion of the uterus is rare but if present, it may be accompanied by sneezing, cuffing, or bearing down. As in cases of effusions, it may be due to local tony of the placental site on the fundus associated with a sharp rise in intra-abdominal pressure. It is sometimes linked to:
- Short cord,
- Placenta accreta,
- Fundal attachment of placenta.
Induced (60%):
- Inversion of the uterus is seen due to mismanagement of the 3rd stage of labor.
- When the uterus is atonic, the cord is pulled (pulled).
- Improper credence on an atonic uterus.
- It is due to the use of improper/faulty technique in manual removal of the placenta.
- Delivery Due to pulling of the short cord on the fundus during delivery.
- Forced expulsion of the placenta due to downward pressure on the uterus.
Sign And Symptoms Signs and Symptoms:
- Acute lower abdominal pain with a bearing down sensation.
- Shock,
- Cupping or dimpling of the fundus on abdominal examination.
- When there is a complete degree of involution in bimanual examination, a pear-shaped, reddish purple colored mass is seen outside the vulva which can be diagnosed by sonography.
- Inversion can usually be caused by 3rd stage labor.
- In acute inversion, a condition of shock may also arise due to blood loss.
- In chronic inversion,
- Persistent Vaginal bleeding,
- Pelvic pain,
- Something protruding from the vagina.
- Difficulty passing urine.
Sign:
- There may be evidence of shock.
A mild to moderate degree of anemia may occur.
First degree inversion involves cupping of the fundus.
Bimanual examination shows protrusion of the fundus into the uterine cavity. - In the 2nd degree, the fundus cannot be felt bimanually.
A round and firm swelling with a soft bleeding surface is felt in the vagina as the cervix protrudes outwards, and the swelling is often covered by the placenta. - In the 3rd degree, on the abdominal The fundus cannot be felt. The mass protrudes outside the vulva.
Nursing Management:
- Proper management of the third stage in this condition is important to prevent complications.
- Provide intravenous fluids such as Ringer lactate solution to the patient to prevent shock.
- Arrange proper blood transfusion for the patient.
- Immediate treatment in recent cases is replacement of the uterus under general anesthesia To do.
- Provide the patient with inj. Retrodrin IV for 15 minutes.
- The part of the uterus lying close to the cervix should be pushed in first and then the part of the fundus should be pushed in.
- If the placenta is still adherent, it should not be removed before manual replacement, unless a large part of the placenta interferes with manual replacement.
- After replacement, when Methergin 0.2 mg is given intravenously, hand is placed inside the uterus.
- Inj. Oxytocin is administered I.v. It is provided in a drip to prevent recurrence of inversion.
- Provide proper blood transfusion to the patient.
- If symptoms of shock are seen, elevate the patient’s feet.
- Provide general anesthesia to the patient and replace the uterus.
- Control the condition of vaginal hemorrhage by tight gauze plugging.
- Oxytocin should not be given while the uterus is still inverted.
- If the recent case has occurred after a few days, manual replacement is attempted as soon as possible.
- If that fails, Sullivan’s hydrostatic method is performed under general anesthesia.
- The uterus is pushed into the vagina.
- –> Vaginal douching is done with an antiseptic solution by placing the douche nozzle in the posterior vaginal wall and preventing the douche from coming out. Inj. Oxytocin is provided.
- In case of chronic case, operative treatment is advised by incision of the posterior part of the ring by Holten’s method per abdomen or cutting of the anterior part of the ring by Spinelli’s method per vagina.
