ENGLISH-MSN 2 UNIT 2 BREAST DISORDERS(UPLOADED)
UNIT 6 BREAST DISORDERS .
INTRODUCTION
- The breast has 15-20 lobes
- The breast has small lobules. Connected to the lactiferous duct by small tubes.
- The lactiferous duct acts as a reservoir for milk after delivery and the dark brown areola is part of the breast.
- The areola is supplied with blood, venules, lymph, and blood supply.
Blood supply:-
- The branches of the thoracic artery and the axillary artery provide blood supply to the breast.
Venous drainage:-
- Thoracic, axillary and mammary venous drainage
Lymph drainage:
- It includes axillary lymphatic vessels
Nerve supply:-
- Thoracis and axillary nerves (4th, 5th, 6th thoracic nerve)
Breast function:
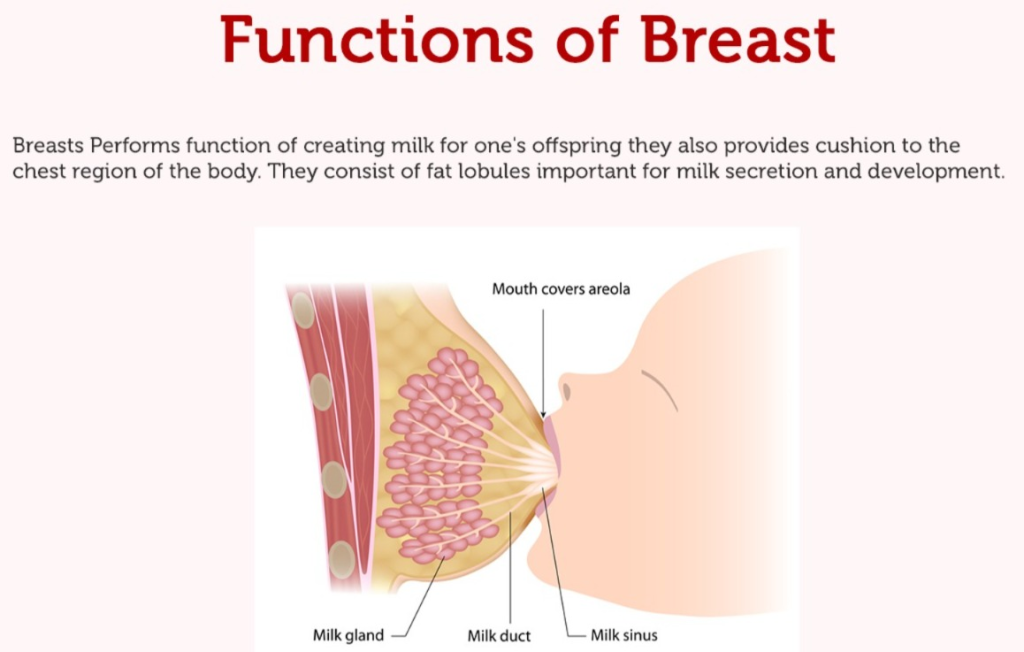
The secretion and ejection of milk are dependent on two types of hormones.
1) anterior pituitary
- The anterior pituitary stimulates the hormone prolactin, which causes the secretion of milk from the breast.
2) posterior pituitary
- posterior pituitary The hormone oxytocin stimulates and it helps the baby Breast ejects milk after sucking.
Anatomy of breast :
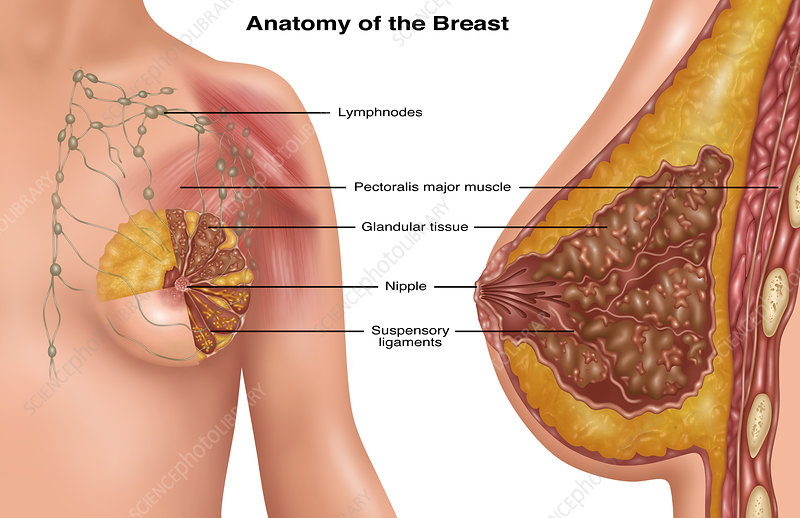
Breast or Mammary Gland is a special glandular organ in the female, whose main job is to provide nutrition to the newborn through Milk Production and Lactation. Breast is an organ related to the Reproductive System of the Female and is located in the front of the Chest above the Pectoralis Major Muscle.
Location of Breast
The breast is spread out in the front of the Chest as follows:
- Top of the Second Rib From
- Down to the Sixth Rib
- From the Sternum in the middle
- Outside to the Midaxillary Line
The upper part of the breast extends towards the armpit, which is called the Axillary Tail of Spence.
Structure of the Breast:
Breast is a milk-producing organ located in the upper part of the female chest. The components inside the breast are as follows:
1.Mammary glands:
- The main milk-producing gland is the Mammary Gland.
- Each breast contains about 15–20 Lobes.
- Each lobe is made up of smaller lobules.
- The lobules contain alveoli where milk production takes place.
2.Alveoli:
- There are small round cells where milk is produced.
- A hormone called prolactin is responsible for milk production.
3.Lactiferous ducts:
- The milk obtained from the alveoli is produced by the ducts (ducts).
- These ducts go through a single path to the nipple.
4.Lactiferous sinuses:
- The enlarged part at the end of the ducts where the milk used to stop.
- Milk is a nipple It stays here for some time before moving towards.
5.Nipple:
- The external part of the breast from which milk comes out.
- The colored portion around each nipple is called the areola.
6.Areola:
- It contains small glands called Montgomery’s glands, which keep the nipple moisturized.
7.Adipose tissue:
- The fatty tissue surrounding the breast that cushions and supports it.
Function of the Breast:
The main function of the breast is – lactation, i.e. the function of feeding the baby with milk. Its function is mainly under hormonal control.
Main functions:
1.Milk Production:
- After the birth of the baby, the alveoli produce milk due to the prolactin hormone.
2.Milk Ejection:
- When the baby drinks milk, the milk is released due to the hormone oxytocin – which is called the let-down reflex.
3.Nourishment to the Baby:
- Milk contains antibodies, proteins, fats and lactose which are essential for the development of the baby.
4.Immunological Protection:
- Breast milk contains antibodies like IgA which protect the baby from infection transmission
5.Bonding between Mother and Child:
- During breastfeeding, the hormone oxytocin creates an emotional bond between the mother and the child.
Hormonal Function (Hormonal Functions) :
- Prolactin helps in the production of milk
- Oxytocin helps in the ejection of milk
- Estrogen plays a role in the development of the breast
- Progesterone helps in the development of the gland
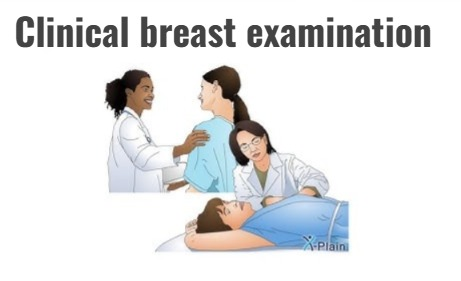
Inspection of breast:
There are 4 main sitting positions of the client used for clinical breast examination. Each client should be examined in each position.
- 1. The client is seated with his arms at his sides.
- 2. The client is sitting with her arms raised above her head.
- 3. The client is sitting and pushing her arms toward her hips.
- 4. The client is sitting and learning while the examiner helps her support and balance.
While the client is performing these maneuvers, observe the breast. Check for symmetry, bulging, retraction, fixation.
When there is no abnormality in the breast and to prevent the pressure on the suspensory ligament of the breast from invading the suspensory ligament in the breast, ask them to do positions 2 and 4.
Normal finding of breast:
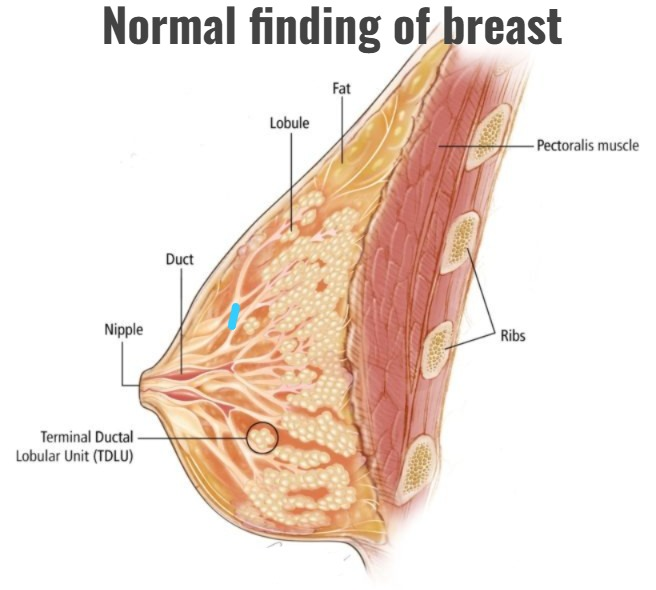
Normal findings of the breast during inspection:
- Both breasts are of the same Size and Has Shape.
- The Skin of the breast is smooth and healthy.
- There is no dimpling or puckering.
- The Nipple is in the middle and protrudes.
- There is no Nipple Discharge.
- Areola is the dark colored area around the nipple. Small Montgomery Glands may be seen in it.
Palpation of breast:
- Palpate the breast with imaginary concentric circles, following a clockwise rotary motion, from the peripheral to the middle of the breast towards the nipple. Breast The best time to examine is one week after the menstrual cycle.
- Evaluate each breast for the presence of a mass or discharge
General findings:
- 1. No mass or lump is evident.
- 2. Tenderness is not found in barley.
- 3. There is no secretion from the nipple of the breast.
HEALTH HISTORY:
1.General information:
- •age and marital status
- •Past medical surgical history
- •Injury
- •Bleeding
- Any breast problem
- •Medication
- •Use of any hormonal contraceptive
- •Use of any over the counter products
- •Vitamins
- •Herbal supplements
2. Gynecological and obstetric history:
- •menarche
- •Date of last menstrual period
- •Pregnancy
- •miscarriage
- •abortion
- •deliveries
- •lactation history •family history of breast cancer
Physical examination:
Screening and early detection:
- It is important to get screened for breast cancer before symptoms appear. Screening can help doctors find and treat cancer early. A doctor may recommend the following screening tests for women who are familiar with how their breasts usually look and feel and should report any changes to their health care provider right away.
- Breast self-exam (BSE) is an option for women in their 20s. Females can do a monthly breast self-exam (BSE) to check for any changes in their breasts.
- Annual mammograms are recommended starting at age 40 and continuing as long as a female is in good health. A mammogram is an X-ray picture of the breast. Mammograms can often show lumps in the breast before they can be felt.
- Clinical Breast Examination (CBE) Every 3 years for women in their 20s and 30s and every year for women 40 and older. A complete clinical breast examination can take about 10 minutes. During a clinical breast examination, the health care provider will: Examines your breasts. The health care provider looks for differences in size or shape between your breasts. The skin of your breasts is checked for lumps, dimpling, or other unusual signs. The nipple of the breast is squeezed to check the breast milk.
Clinical breast examination:
- A clinical breast examination (CBE) is a physical examination of the breasts performed by a health professional. A clinical breast examination (CBE) is used along with a mammogram to screen women for breast cancer. A clinical breast examination (CBE) is also used to screen for other breast problems.
- A clinical breast examination may be part of a routine checkup. Talk to your health professional about how often you need to have your breasts examined. Women with breast implants should also have regular clinical breast examinations. Clinical breast exams are performed to: 1. Find any lumps or changes in the breast that could mean a serious problem is present, such as breast cancer 2. Check for other breast problems that may require further treatment, such as mastitis or fibroadenoma.
Procedure:
- Clinical Breast The examination is performed by a health professional. The female will have to remove her clothes above her waist. She will be given a gown to wear during the examination.
- First, the health professional will ask questions about any problems she has, her medical history, and her risk factors for breast cancer. Talk to the health professional about any areas of her breasts that you may be concerned about.
- The health professional will then examine each breast, underarm, and collarbone area to check for changes in breast size, skin changes, or signs of injury or infection, such as bruising or redness. During this part of the exam, the woman is asked to raise her arms above her head, place her hands on her hips or lean forward, and press the muscles under each breast with her hands. She may lie flat on the table and place her hands behind her head while the health professional examines the breast tissue.
- The health professional will feel each breast for any unusual or painful areas or for firm lumps. A breast lump is any lump that is new, large, hard, or otherwise different from other lumps or the rest of the breast tissue.
- The health professional will gently press on the breast tissue from about 1 inch (2.5 cm) below the breast to the collarbone. He or she will also examine her axilla (armpit area) and neck for swollen glands (lymph nodes).
- The health professional will gently press on the nipple of the breast to check for any secretions and check for any discharge.
Result of clinical breast examination:
Normal and abnormal
Normal Findings
- A milky discharge may occur in a female who is breastfeeding or after breast stimulation, which is known as galactorrhea.
- The breast, nipple, and the area around the breast appear normal, and both breasts are usually about the same in size and shape.
- The nipple is usually protruding and has no lesions. There are no lesions, ulcers, or rashes.
- Breast tissue can usually be soft or slightly firm.
- It is common for some women to have some firm glandular tissue in the lower part of the breast or under the nipple.
- It is common for many women to have lumpiness or thickening of tissue in both breasts during their menstrual cycle.
- Often more glandular tissue is found in the upper outer quadrant, which is considered normal.
Abnormal Findings
- A lump or thickened area in one or both breasts Feel.
- The following changes may be seen in the skin of the breast:
- Dimpling
- Puckering
- Skin Thickening
- Peau d’orange appearance (skin like orange peel)
- Nipple retraction or Nipple inversion may be seen.
- Redness, scaly rash, ulcer or soreness may be seen on the nipple.
- Painful lump, redness, warmth or swelling may occur, which can be caused by the following reasons:
- Mastitis
- Breast Abscess
- Breast Cancer
Bloody discharge or Spontaneous nipple discharge (without stimulation) is abnormal.
The upper outer quadrant of the breast contains the most breast tissue and breast cancer is most common in this area.
BREAST SELF EXAMINATION:

Breast self examination is done to check for any abnormal masses, lumps, or nodules in the breast.
PURPOSES:
1) To see if there is any abnormality in the breast.
2) To take early notice of breast cancer.
3) To see if there is any abnormality in the breast.
Time:
1) Breast self-examination is usually done once a year in normal women.
2) If there is breast cancer, it should be done twice a year
3) It is done once a month during menopause.
4) It is done once a month during the reproductive age.
There are a total of 5 steps for breast self-examination:
1)Step 1 :
Stand in front of the mirror.
Then look at the breast to see if there is any lump in it. Check for any abnormalities such as redness, discharge, abnormal size, inverted nipples, swelling, dimpling, bulging, etc. to see if there is any abnormality in the breast.
Step2:
In this step, place your hands behind your head, then turn your head forward with your hands and look in the mirror to see if the size of the breast is symmetrical.
Step 3:
In this step, place your hand on your waist and then lean forward and check the size of the breast, cement and whether there is any lump.
Step4 :
In this step, stand in front of the mirror.
Then raise your left hand.
Then palpate the left breast with the first three fingers of your right hand.
First of all, circular Palpate in motion.
Palpate it from outside to inside.
Then quiz the nipple.
See if there is any discharge in it.
Now palpate the right breast in the same way.
Through this step, it is known whether there is any lump mass in the breast.
Step5:
Then squeeze the nipple to see if there is any discharge.
Thus, through breast self examination, it is known from this step whether there is any abnormality in the breast and if breast cancer is to occur, it is known at the first opportunity comes.
Diagnostic test:
Breast MRI:
- MRI The scanner uses a high-powered magnet and computer to create detailed images of the breast and surrounding structures. It is especially useful in screening adult females with dense breast tissue who may be at high risk of developing breast cancer.
- MRI is also useful in determining the stage of breast cancer to help determine the most appropriate treatment. Breast MRI can add additional information to a mammogram and is only added in specific cases.
Breast Ultrasound:
- Breast ultrasound, also known as sonography or ultrasonography, is used when an abnormal cyst (fluid-filled mass) is found on a mammogram or during a clinical physical examination.
- Ultrasound does not provide as much detail as a mammogram image and is not approved by the U.S. Food and Drug Administration (FDA) for breast imaging. Not approved as a screening tool for cancer.
Ductogram:
- A ductogram is useful for evaluating patients with nipple discharge from the breast. A thin plastic tube is inserted into the nipple of the breast, and a contrast dye is injected into the breast.
Nipple smear (Nipple discharge exam):
- A sample of blood or abnormal fluid that leaks from the nipple of the breast is examined under a microscope to see if cancer cells are present.
- Ductal lavage : Sterile water is injected into the nipple of the breast, then cancer cells are collected and examined. This test is used only in women at high risk of breast cancer
Mammography :
- This is a low-dose X-ray picture of the internal structure
- Breast The mammography machine compresses each breast and takes low-dose X-rays. In a mammogram machine, each breast is compressed and then X-rayed. Mammograms are used for the detection and screening of breast cancer. Mammograms are used to detect tumors, cysts, and the evolution of specific areas of a breast through screening and physical examination.
Digital Mammogram:
- A mammogram is a digital, computer-readable format that takes electronic images of each breast.
Biopsy:
- A sample of tissue is taken from an area of the breast that appears normal during a physical examination, mammogram, or other imaging study.
- A biopsy is done with a needle or minor surgery. There are 5 types of biopsy.
- Fine Needle Aspiration (FNA) Biopsy: The doctor may use a needle to take a sample of tissue from a breast lump. A thin needle is inserted into the area that looks abnormal and removes fluid and tissue (aspirate). This is the simplest type of biopsy and is most often used for lumps in the breast that can be easily felt.
- Core needle breast biopsy: A large, hollow needle is inserted into the breast, and a tube-shaped piece of breast tissue (core) is removed. A core biopsy allows for a more detailed evaluation of the breast tissue than an FNA biopsy.
Stereotactic breast biopsy:
- This biopsy uses computer-generated pictures to help the health care provider determine the exact location of normal breast tissue.
Surgical biopsy:
- Breast to check for cancer Part of the lump is surgically removed.
Sentinel node biopsy:
- This type of biopsy is used to find out how far the cancer has spread.
- In this type of biopsy, the health care provider locates the primary tumor and removes the lymph nodes.
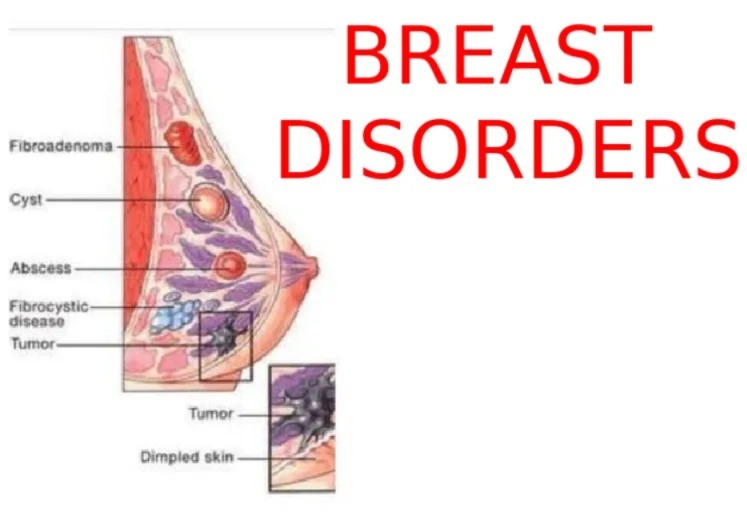
DISORDER OF BREAST :
MASTITS (mastitis):
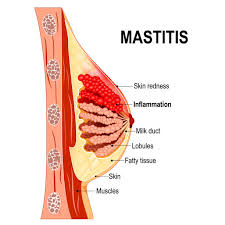
- Mastitis a breast tissue Mastitis is an infection and inflammation of the breast, which is characterized by pain, swelling, and redness.
There are 2 types of mastitis.
- 1. puerperal
- 2. Non- puerperal
1. Puerperal mastitis:
- This occurs due to blockage or excessive milk production after pregnancy, lactation and delivery.
2.Non-puerperal
- This is not caused by pregnancy or lactation. This causes lesions on the breast.
Etiology:
- Bacteria : streptococcus staphylococcus
- Milk stasis- Breast Due to lack of lactation, milk collects in the breast.
- This is more common in the puerperal (post-delivery) period (6 weeks after delivery)
- Hormonal changes: estrogen
- Progesterone
- Dead cell buildup in the milk duct
- HIV
- diabetes
- wearing too tight clothes
- Maternal stress
- breast If trauma has occurred from an accident
Clinical manifestations:
- Breast discharge
- Swelling
- Lump
- Pain
- High grade fever
- Lesion on breast
- Skin redness
- Inflammation on breast
- Tender or warm breast
- Body ache
- Malaise
- Fatigue
- Breast engorgement
- Chills
- Rigor
Management:
- 1.medical management
- 2. surgical management
- 3. nursing management
1.medical management:
Analgesic medicine:
- This medicine is given for breast pain.
Eg.ibrupofen
- This medicine is safe during breastfeeding.
- This medicine does not harm the baby either.
Antibiotic medicine:
- This medicine is given to reduce the infection in the breast.
- Eg.cephalexin
- Erthromycine
Antipyretic medicine:
- This medicine is given to cure fever caused by infection.
2.surgical management:
- If an abscess is found in the breast, drainage is done.
- Local anesthesia is given, after which the breast is removed. The abscess that has accumulated in the breast is drained by needle aspiration.
- If the abscess is deep, it is drained by giving general anesthesia in the operation room and making a small incision.
Nursing management:
- Encouraging the mother to breastfeed
- Tell the mother to breastfeed even if the affected breast is painful.
- Frequent breastfeeding can prevent engorgement in the breast and block the milk duct.
- Before and after breastfeeding, apply left compression on the breast to relieve pain.
- If left compression does not work, then apply the breast only after breastfeeding. Apply ice packs to provide comfort and release.
- Do not use ice packs before breastfeeding as it reduces the flow of milk.
- Encourage the mother to take painkiller medicine to reduce pain.
- Instruct the mother to drink 10 glasses of water a day and eat a well-balanced diet.
- A breastfeeding mother should consume 500 more calories a day.
- Dehydration and poor nutrition reduce milk supply, so advise the patient to drink more water and eat a good diet
- If discharge is seen from the nipple, wash the nipple gently and allow it to dry. Then put on clothes.
- If there is excessive discharge, ask to use a disposable breast pad.
- This disposable breast pad absorbs the discharge.
- The mother should breastfeed her baby. Ask them to put cabbage leaves on it. Because cabbage leaves help reduce infection, replace them when they become rotten. Ask the mother to massage the breasts. Ask the mother to wear supportive clothes. PREVENTION: Equal breast size in both breasts Feeding.
- While breastfeeding, empty both breasts completely to prevent engorgement and to prevent blocked ducts.
- Use good breastfeeding technique to prevent soreness.
- Drink plenty of fluids to reduce dehydration.
- Wear supportive clothing (bra).
- Rest.
- Apply left compression to the breast before breastfeeding.
- Maintain hygiene.
- Hand washing
- Clean the nipple
- Clean the breast
- Keep baby clean
BREAST ABSCESS :
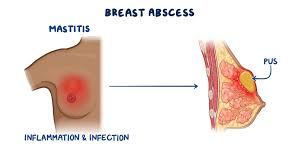
- Sometimes, a bacterial infection can cause a collection of pus in a local area just under the skin. When this pus forms in the breast, it is called a breast abscess. It can be painful and requires immediate medical attention to avoid complications.
- The type of bacteria that most often causes breast infections is Staphylococcus aureus. The bacteria can enter through a crack in the skin of the breast or through a crack in the nipple of the breast. The resulting infection, called mastitis, invades the fatty tissue of the breast, causing swelling and pressure on the milk ducts.
Cause and risk factor:
- Breast abscesses most commonly occur in women between the ages of 18 and 50, especially if they are breastfeeding.
There are two categories of breast abscess:
- 1. Lactational (puerpereal) abscess
- 2.non-lactational abscess
1. Lactational (puerperal) abscess:
- Formations are found in the peripheral areas of the breast, usually in the upper and outer sections. Breast abscesses can often be caused by mastitis. In this case, they are called lactational abscesses. They can occur in the milk ducts that carry milk to the nipple of the breast in a breastfeeding woman.
2. Non-lactational abscess:
- Found in the subareolar or lower parts of the breast. In women who are not breastfeeding, bacteria can enter the breast through a crack or sore.
- Breast nipple – This is a non-breastfeeding abscess.
Symptoms:
- Pain in the affected breast
- Redness, swelling, and tenderness in an area of the breast
- Fever
- Breast engorgement
- Itching
- Nipple discharge
- Nipple tenderness
- Tender or enlarged lymph nodes in the armpit on the affected side
Management:
- First the lump needs to be examined. If it is an abscess, the patient will be referred to a surgeon immediately for examination and treatment.
- An ultrasound scan can confirm the diagnosis of an abscess and determine whether there is more than one collection of pus.
- The abscess will need to be drained to remove the fluid (pus) from the breast.
- If the abscess is small, a needle and syringe will be used to remove the fluid. However, if there is a small or large abscess, an incision or incision will be made to remove the fluid.
- The patient will first be given a local anesthetic to numb the skin
- The pus is drained from around the abscess and using ultrasound. Breast Broad-spectrum antibiotic medicines used to treat abscesses will be given
Prevention:
- 1. If an abscess is present, do not breastfeed with the infected breast and consult a doctor if breastfeeding is desired.
- 2. Wash the breast daily with mild soap and water. Wipe away dry secretions and gently pat the breasts dry with a clean towel.
- 3. After breastfeeding, clean the nipples and areolas with boiled, cooled water and cotton.
- 4. At the end of the breast feed, let the breasts dry naturally in the air.
- 5. Apply lanolin cream daily to prevent cracking of the nipples and areolas.
- 6. Take a warm bath and apply a cold compress to the infected area.
- 7. Apply a warm, moist compress to the affected area several times a day.
- 8. Maintain a regular breastfeeding schedule or manually pump milk.
GAYNECOMASTIA (Gynecomastia) :
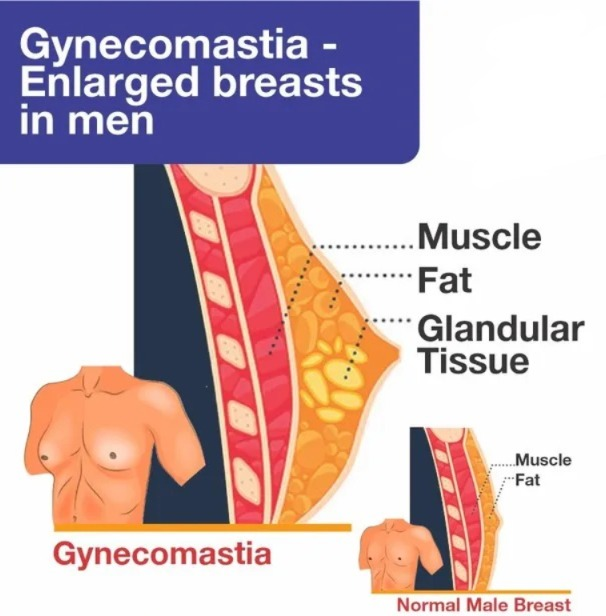
- Gynecomastia is the overdevelopment of male breasts. In response to too much estrogen (a female hormone) or too little testosterone (a male hormone), the breast tissue swells and swells, forming a breast bud (enlarged breast). Gynecomastia can affect one or both breasts, sometimes unevenly.
Cause and risk factor: Causes and risk factors:
- In newborns, gynecomastia is caused by estrogen from the mother. Breast buds are common in baby boys. Breast buds gradually disappear by 6 months of age, but in some children they may persist for a longer period.
- In preteen boys, gynecomastia can also be caused by an estrogen-producing tumor.
- In adolescent boys, gynecomastia is caused by the hormonal changes of puberty. Gynecomastia is seen in many boys during early to mid-puberty. It usually goes away within 6 months to 2 years
- In adult men, gynecomastia is usually caused by another condition.
Grade of gynecomastia:
- Grade one gynecomastia is small and can be seen with the naked eye but as you move up the grades and reach grade 4, it becomes obvious and severe.
Grade-1
- Severity- very mild
- This involves a localized button of tissue around the areola It is deposited.
Grade-2
- Severity-mild to high
- Breast enlargement increases moderately and is seen up to the edge of the areola.
Grade-3
- Severity – high to identifiable
- In this, the breast enlargement extends beyond the areolas and the chest wall extends to the skin
Grade-4
- Severity- severe to visibly feminine
- In this, enlargement of the breast along the skin boundary is seen and feminization of the breast is seen.
Diagnostic investigation:
- History collection
- Physical examination blood test
- Mammograms
- CT scan
- MRI
- Testicular USG
Management:
1. Medicine:
- Breast Medicines used to treat cancer and other conditions, such as tamoxifen (Soltamox) and raloxifene (Evista), may be helpful for some men with gynecomastia.
2. Surgery to remove excess breast tissue:
- If the patient continues to have breast enlargement despite initial treatment and observation, the doctor may advise surgery. There are two options for gynecomastia surgery:
- Liposuction. This surgery removes fat from the breast, but does not remove the breast gland tissue.
- Mastectomy. This type of surgery removes the breast gland tissue. Surgery is often performed endoscopically, which means that surgery is performed using only small incisions.
Tumor and malignancy of breast :
1.Breast cyst
2.breast cancer
Breast cyst :
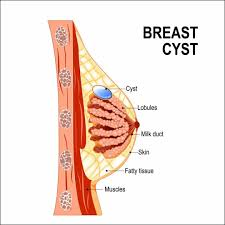
- A breast cyst is a fluid filled sac within the breast. A patient may have one or more sacs in the breast. They often appear as a round or oval lump with distinct edges. These breast In structure, breast cysts usually look like soft lumps or water-filled balloons, but sometimes breast cysts can be firm.
Cause
- The cause of breast cysts is unknown. Some evidence suggests that excess estrogen in the body may play a role in the development of breast cysts. Breast cysts develop when excess growth of glands and connective tissues (fibrocystic changes) blocks the milk ducts, causing them to enlarge and fill with fluid.
Microcysts:
- Microcysts appear very small but can be seen during imaging tests, such as mammography or ultrasound.
Macrocysts:
- Macrocysts are large enough to be felt and can grow to about 1 to 2 inches (2.5 to 5 cm) in diameter. Large breast cysts can put pressure on nearby breast tissues, causing pain and discomfort in the breast.
Clinical manifestations:
- A smooth, easily movable round or oval lump in the breast is seen.
- Breast pain or tenderness in the area of the lump
- Premenstrual lump enlargement and tenderness
- Lump reduction and resolution of other signs and symptoms after period
Management:
- Breast cysts do not require treatment unless the cyst is large and painful or uncomfortable. In that case, draining the fluid from the breast cyst may relieve symptoms. Typical treatment includes needle aspiration biopsy. Aspirated cysts often recur; surgery may be required for definitive treatment. Surgical removal of a breast cyst is an option only in unusual circumstances.
- If the breast If the cyst recurs month after month, the breast cyst has blood-tinged fluid, and it shows other worrisome signs, surgery may be considered.
- Using oral contraceptives to regulate the menstrual cycle may help reduce the recurrence of breast cysts.
- Stopping hormone replacement therapy during the postmenopausal years may also reduce cyst formation.
- If the patient is experiencing breast pain from the cyst, encourage them to take acetaminophen or ibuprofen.
- Encourage the surrounding breast tissue to wear a supportive bra to relieve some discomfort.
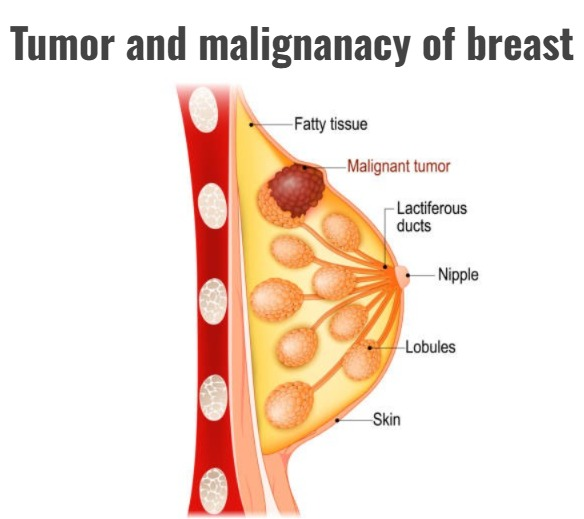
Breast cancer:
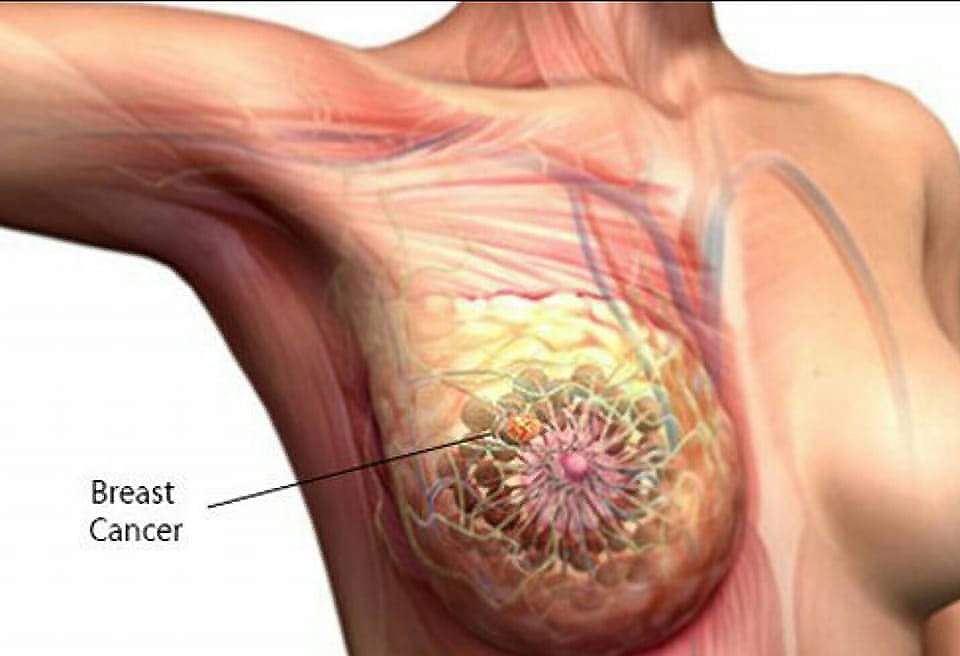
Introduction:
- Breast cancer is the abnormal and uncontrolled growth of breast cells, which results in a tumor, which can be malignant. It is called breast cancer. Breast cancer can occur anywhere in the breast, but it is most common in the upper outer parts of the breast, where there is excess tissue. Breast cancer arises from the cells of the lobule of the breast, which is a milk-producing gland or duct.
Etiology:
- drinking alcohol.
- age: in women over 60 years old )
- Gender: most in female
- personal history of breast cancer
- family history,
- certain breast change
- reproductive and menstrual history,
- atypical Hyperplacia (atypical hyperplasia),
- Hormonal replacement therapy (estrogen and progesterone),
- oral contraceptive use,
- overweight and Obesity,
- lack of physical activity,
STAGES:-
Stage-o :- carcinoma in situ
stage-1:- less than 02 cm tumor was grown.
Lymph node involvement is absent.
Stage-2 – more than 02 cm but less than 05 cm tumor was grown,
and still lymph node involvement is absent.
Stage-3 :- The size of the tumor cannot be found
Lymph node involvement is seen and spread to the axillary area is seen.
Stage-4 : In this stage, the cancer spreads from nearby organs to distant organs.
clinical manifestations (symptoms and signs):
- axillary and Supraclavicular lymph node enlarges.
- a lump or thickening in or near the breast or in the underarm area.
- There is a change in the size and shape of the breast.
- The skin of the breast areola and nipple becomes red, swollen and scaly.
- Irritation and dimpling of the skin.
- Pain in the breast.
- Pain and tenderness in the nipple.
- The nipple is turned inward in the breast.
- Discharge comes out of the nipple.
Diagnostic evaluation:
- mammography ( mammography).
- History tacking and physical examination (History taking and physical examination)
- Biopsy (biopsy),
- X Ray (x-ray),
- ct scan (ct scan),
- MRI
Management:
A. Surgery:
Surgery is the most common treatment for breast cancer. There are many types of surgery.
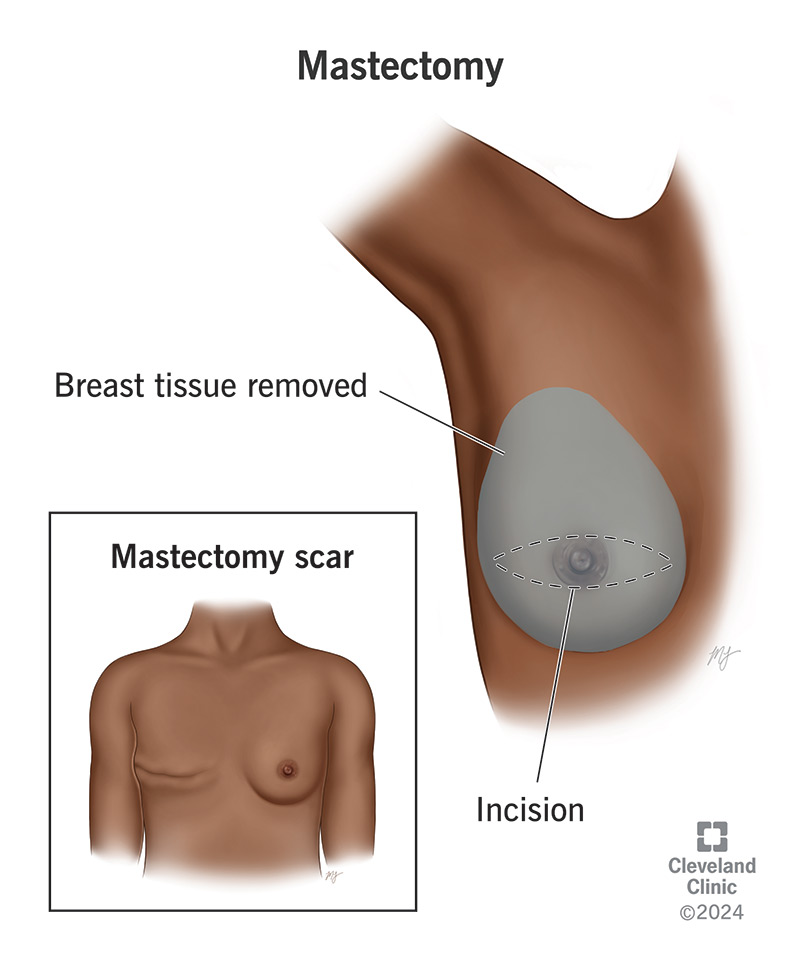
Mastectomy: A mastectomy is an operation to remove cancer. This procedure is usually done for carcinoma in situ (stage-0). In most cases, the surgeon will remove the breast from the armpit. Removes lymph nodes.
Total mastectomy: In a total (simple) mastectomy, the surgeon removes the entire breast.
It also removes the lymph nodes in the armpit.
Radical mastectomy:
A radical mastectomy removes the breast, pectoralis major and minor, and axillary lymph nodes.
Modified Radical Mastectomy:
- The surgery removes the entire breast, and most
- The lymph nodes under the arm are removed.
- Often, the chest muscle is removed …
- NURSING MANAGEMENT OF A PATIENT AFTER MASTECTOMY:
Nursing management :
Preoperative nursing intervention:
1 Monitoring of adverse effects of radiation therapy such as Weakness, Sore throat, Cough, Nausea,.
2. Monitor for adverse effects of chemotherapy, bone marrow suppression, nausea and vomiting, alopecia, weight gain or loss, weakness, stomatitis, anxiety and depression.
3. Understand that a diagnosis of breast cancer is a devastating and emotional shock for a woman. Provide psychological support to the patient throughout the diagnosis and treatment process.
4. Involve the patient in planning and treatment.
5. Describe surgical procedures to alleviate fear.
6. Explain to the patient the effects of chemotherapy and develop treatment for alopecia, weakness.
7. Administer anti-inflammatory medications as directed for patients receiving therapy.
postoperative nursing care:
•Nursing diagnosis:
1.Risk for infection related to surgical incision
- Ineffective tissue perfusion related to lymphedema
- Acute pain related to surgery
- Disturbed body image related to breast changes or loss of breast
- Impaired skin integrity related to surgical incision and radiation
- Decisional conflict about treatment related to concerns about risks and benefits
- Interrupted family processes r/t effect of surgery & therapy on family roles and relationships
- Fear related to disease process/prognosis
Expected outcome:
1. Stay free from infection.
2. Maintain adequate tissue perfusion.
3. Experience less pain or discomfort during the patient’s recovery.
4. Regardless of her decision regarding recovery, maintain a positive body image.
5. Maintain skin integrity.
6. Evaluate personal values and treatment options and determine a treatment no course of action.
7. Together with her daughters, advise her to support her during her illness.
8. Identify the sources of her fears and be kind to her to reduce the fear.
Nursing interventions:
1. Elevate the extremities of the surgical site to relieve pain and edema. Elevating the arms reduces stress on the surgical incision and increases blood circulation.
2. Ice packs are helpful to reduce discomfort and swelling.
3. A small pillow placed in the armpit also reduces discomfort levels and increases drainage of fluid due to gravity.
4. Instruct her to be careful when moving her arm sideways, avoid repetitive activities, not to lift heavy objects, and not to exercise vigorously until the stitches are removed.
5. Administer IV or IM opioid analgesics (Vicodin) for moderate pain. Instruct to take pain medication when pain is experienced on a regular schedule.
Add Ibuprofen (Advil or Motrin) or Tylenol to Vicodin…
Post mastectomy exercise:
1.hand wall climbing:
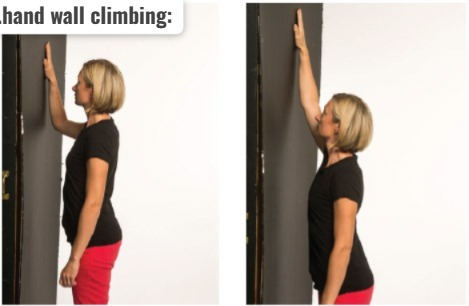
- Stand facing the wall with your toes 6-12 inches from the wall.
- Bend your elbows and place your hands against the wall at shoulder level. Slowly move both hands up,
- Keep moving your hands up until you feel pain.
2.rope turning:
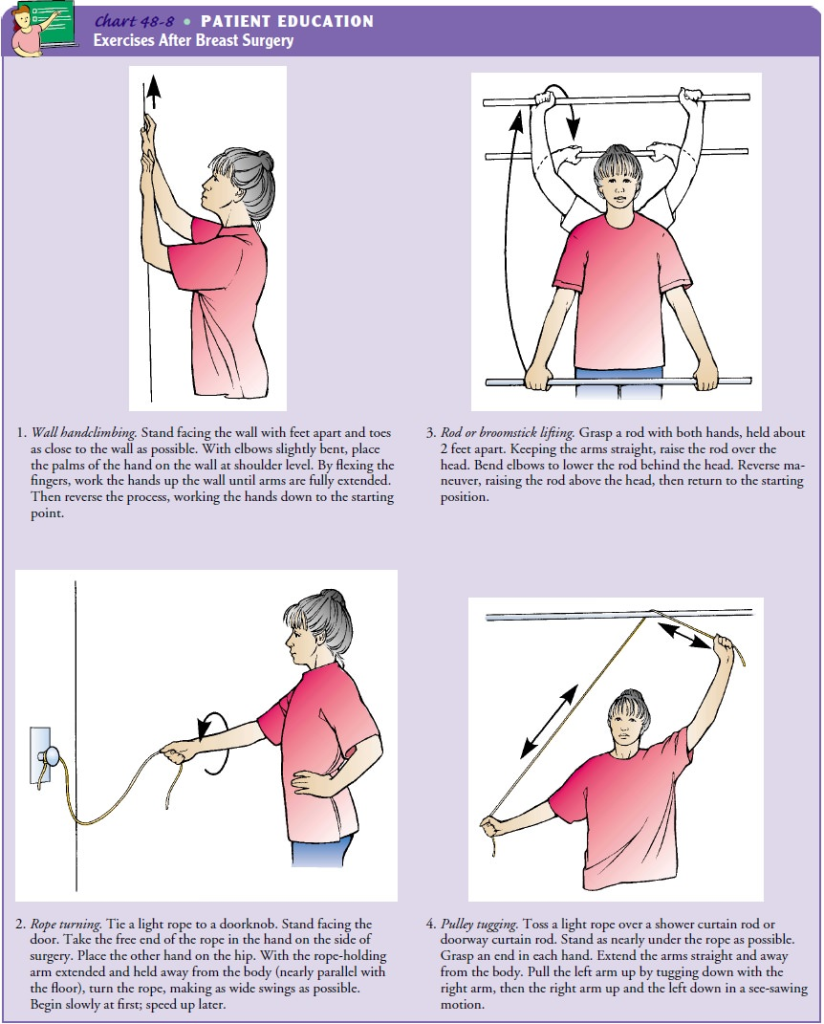
- Tie the rope to the door handle. Hold the rope with the hand on the side of the operation. Stand back from the door until the arm is extended away from the body, parallel to the floor. Swing the rope to make the circle as wide as possible.
3. Rod or broomstick lifting:
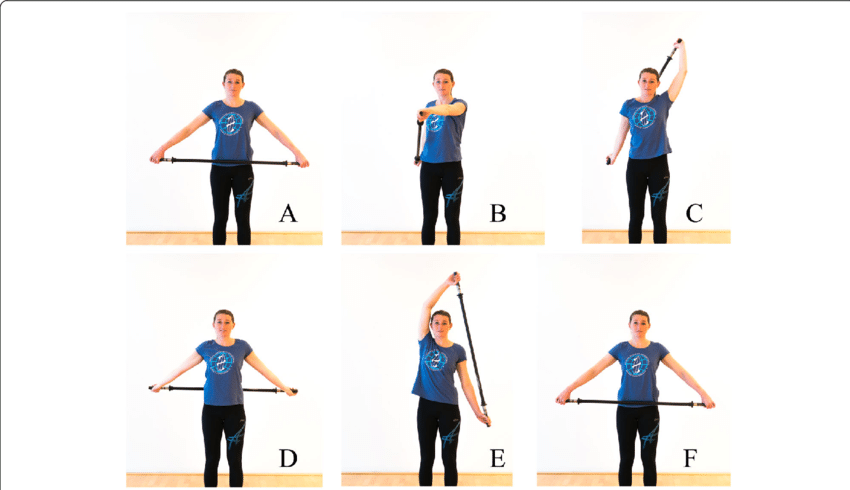
- Hold the rod with both hands about 2 feet apart. Keeping your arms straight, raise the rod above your head. Bend your elbows to lower the bar behind your head. Reverse the maneuver and raise the bar above your head, then repeat.
4. Pulley tugging:

- Toss a light rope over the shower curtain rod. Hold one end of the rope in each hand. Pull down on the rope on the opposite side and slowly raise the arm as high as comfortable. Reverse the motion by lowering the operated side (in a see-saw motion) and lowering the non-operated arm. Instead of a rope, the patient can use a towel and move the towel like we use it to wipe our backside.
5.Elbow circles:

- While sitting or standing, place your right hand on your right shoulder and your left hand on your left shoulder. Raise your elbow until you feel a stretch. Make circles with your elbows. Start small and then make larger circles. Change directions with your circles. Repeat this 2 or 3 times.
