P.B.B.Sc.-2016-Medical-Surgical-paper-no.1 (UPLOAD) (DONE)
PAPER SOLUTION OF P.B.B.Sc.NURSING-F.Y-MEDICAL SURGICAL NURSING-SAURASHTRA UNIVERSITY-GUJARAT-2016
SECTION-I
1 Long essay: (any one) 01X15=15
(a) Define urinary calculi.02
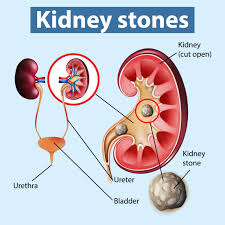
Urinary calculi, also known as kidney stones or renal calculi, are solid masses made up of crystals that form in the urinary tract. These stones can vary in size, ranging from as small as a grain of sand to as large as a golf ball. Urinary calculi can develop anywhere in the urinary tract, including the kidneys, ureters (the tubes that carry urine from the kidneys to the bladder), bladder, or urethra (the tube that carries urine from the bladder out of the body).
(b) Explain briefly the types of urinary calculi.03
Urinary calculi, or kidney stones, can be classified into several types based on their composition. The most common types of urinary calculi include:
- Calcium Stones: Calcium stones are the most prevalent type of urinary calculi, accounting for approximately 80% of all cases. They are primarily composed of calcium oxalate, though some may also contain calcium phosphate. Factors such as high dietary intake of oxalate-rich foods, low fluid intake, and certain medical conditions can increase the risk of calcium stone formation.
- Uric Acid Stones: Uric acid stones form when there are high levels of uric acid in the urine, leading to the precipitation of uric acid crystals. These stones are commonly associated with conditions such as gout, which is characterized by elevated levels of uric acid in the blood. Uric acid stones are less common than calcium stones but can be more challenging to detect on standard X-rays.
- Struvite Stones: Struvite stones, also known as infection stones, are composed of magnesium ammonium phosphate. They typically form in the presence of urinary tract infections caused by certain bacteria that produce urease, an enzyme that raises urine pH and promotes stone formation. Struvite stones can grow rapidly and may lead to complications such as kidney damage or obstruction.
- Cystine Stones: Cystine stones are rare and form as a result of a genetic disorder called cystinuria, which leads to excessive excretion of cystine in the urine. Cystine is an amino acid that is not very soluble in urine, making individuals with cystinuria more prone to developing cystine stones. These stones tend to be larger and may require specialized treatment.
- Other Types: In addition to the above types, other less common types of urinary calculi may include mixed stones (combinations of different minerals), drug-induced stones (associated with certain medications), and less common mineral compositions such as ammonium acid urate stones.
(c) Describe the pathophysiology of urinary calculi. 04
Pathophysiology
Stone growth starts with the formation of crystals in supersaturated urine which then adhere to the urothelium, thus creating the nidus for subsequent stone growth.
The biological processes that anchor crystals to the urothelium are incompletely understood.
Many, but not all, calcium oxalate stones develop on Randall’s plaques which are composed of calcium phosphate (= hydroxyapatite) crystals.
These grow to erode the urothelium, forming a nucleus for calcium oxalate deposition.
More recent theories focus on the role of cell surface molecules which favour or inhibit crystal adhesion.
Urothelial injury and repair after a stone episode may increase surface expression of these molecules to favour further crystal adhesion.
Thus ‘stones beget stones because there may be a residual nucleus on which further stones may form and/or upregulation of molecules favouring crystal adhesion.
Stone prevention focuses on identifying and ameliorating the risk factors for crystal formation.
(d) Discuss the surgical treatment of patient with urinary calculi.06
Surgical treatment…
The surgical treatment of urinary calculi, or kidney stones, involves various procedures depending on factors such as the size, location, and composition of the stones, as well as the patient’s overall health and medical history.
Extracorporeal Shock Wave Lithotripsy (ESWL):
- ESWL is a non-invasive procedure used to treat kidney stones located in the kidney or upper ureter.
- During ESWL, shock waves are generated outside the body and focused on the stone, causing it to break into smaller fragments that can be passed out of the body through urine.
- This procedure is typically performed on an outpatient basis and does not require incisions.
Percutaneous Nephrolithotomy (PCNL):
- PCNL is a minimally invasive procedure used to treat large or complex kidney stones, typically those larger than 2 cm in diameter.
- During PCNL, a small incision is made in the patient’s back, and a nephroscope is inserted through the incision and into the kidney.
- The stones are then broken into smaller pieces using a laser or pneumatic lithotripter and removed through the nephroscope.
- PCNL is performed under general anesthesia and may require a short hospital stay for recovery.
Ureteroscopy (URS):
- URS is a minimally invasive procedure used to treat stones located in the ureter or kidney.
- During URS, a thin, flexible ureteroscope is inserted through the urethra and bladder, and then into the ureter or kidney.
- The stone is visualized using a camera attached to the ureteroscope, and then either removed using small baskets or broken into smaller fragments using laser lithotripsy.
- URS can be performed as an outpatient procedure under general or local anesthesia, depending on the patient’s preference and medical condition.
Open Surgery:
- Open surgery for kidney stones is rarely performed today and is usually reserved for complex cases where other methods are not feasible.
- During open surgery, a large incision is made in the patient’s side or abdomen, and the stone is directly accessed and removed from the kidney or ureter.
- Open surgery carries a higher risk of complications and requires a longer recovery time compared to minimally invasive procedures.
OR
(a) Define the jaundice 02
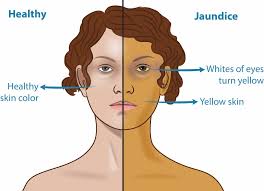
Jaundice is a medical condition characterized by yellowing of the skin, mucous membranes, and whites of the eyes (sclera) due to elevated levels of bilirubin in the bloodstream. Bilirubin is a yellow pigment produced during the breakdown of red blood cells. Normally, bilirubin is processed by the liver and excreted in bile, but when there is an issue with the liver’s function or bile ducts, bilirubin can accumulate in the body, leading to jaundice.
(b) Describe the types of jaundice -03
ANSWER:-
- Pre-hepatic Jaundice: Also known as hemolytic jaundice, pre-hepatic jaundice occurs when there is an excessive breakdown of red blood cells (hemolysis), leading to an increased production of bilirubin. Conditions that can cause pre-hepatic jaundice include hemolytic anemia, sickle cell disease, and certain genetic disorders.
- Hepatocellular Jaundice: Hepatocellular jaundice, also referred to as hepatocellular or intrahepatic jaundice, occurs when there is impairment or damage to liver cells (hepatocytes), resulting in reduced bilirubin processing and excretion. Hepatocellular jaundice can be caused by various liver diseases and conditions, including viral hepatitis (such as hepatitis B or hepatitis C), alcoholic liver disease, drug-induced liver injury, and liver cirrhosis.
- Post-hepatic Jaundice: Post-hepatic jaundice, also known as obstructive jaundice, occurs when there is an obstruction in the bile ducts that prevents the flow of bile from the liver to the intestines. As a result, bilirubin cannot be excreted properly, leading to its accumulation in the bloodstream and subsequent jaundice. Causes of post-hepatic jaundice include gallstones, tumors in the bile ducts or pancreas, strictures (narrowing) of the bile ducts, and pancreatic cancer.
- Neonatal Jaundice: Neonatal jaundice is a common condition in newborn babies characterized by yellowing of the skin and eyes within the first few days of life. It is usually caused by the immaturity of the newborn’s liver, leading to difficulty processing and excreting bilirubin. Neonatal jaundice is often benign and resolves on its own, but in some cases, it may require medical intervention.
(c) Explain the pathophysiology of jaundice -04
ANSWER:-
Pathophysiology of jaundice
Jaundice occurs when there’s an accumulation of bilirubin in the body, leading to yellowing of the skin and eyes. Bilirubin is a yellow pigment produced during the breakdown of hemoglobin from old red blood cells.
The pathophysiology of jaundice varies depending on its type:
- Pre-hepatic jaundice: In conditions such as hemolytic anemia or malaria, there’s an increased breakdown of red blood cells, releasing more bilirubin than the liver can process. This overwhelms the liver’s ability to conjugate and excrete bilirubin, leading to its accumulation in the bloodstream and subsequent jaundice.
- Hepatic jaundice: In liver diseases like hepatitis or cirrhosis, the liver’s ability to process bilirubin is impaired. This can be due to inflammation, damage to liver cells, or decreased function of hepatocytes, the liver’s main functional cells. As a result, bilirubin cannot be properly conjugated and excreted, leading to its accumulation in the bloodstream and jaundice.
- Post-hepatic jaundice: In conditions such as gallstones or tumors blocking the bile ducts, bile flow from the liver to the intestine is obstructed. Bilirubin, along with bile salts, cannot be excreted into the intestine and instead accumulates in the bloodstream, causing jaundice.
(d) Discuss the nursing management of client with jaundice 06
Nursing management of jaundice
The nursing management of a patient with jaundice involves several key aspects:
- Assessment: Nurses should monitor the patient’s vital signs, level of consciousness, skin color, and scleral icterus (yellowing of the eyes). They should also assess for signs of dehydration, abdominal pain, pruritus (itching), and any complications related to jaundice.
- Fluid and electrolyte management: Patients with jaundice may be at risk of dehydration due to increased fluid loss from vomiting, diarrhea, or decreased oral intake. Nurses should monitor fluid intake and output, administer intravenous fluids as needed, and monitor electrolyte levels to prevent imbalances.
- Nutrition: Patients with jaundice may have poor appetite or difficulty digesting fats. Nurses should provide small, frequent meals that are high in carbohydrates and low in fats. They should also encourage oral fluid intake and monitor for signs of malnutrition.
- Skin care: Pruritus is a common symptom of jaundice, and patients may experience itching due to bilirubin deposition in the skin. Nurses can provide comfort measures such as cool baths, gentle moisturizers, and anti-itch medications to relieve itching and prevent skin breakdown.
- Monitoring and management of complications: Nurses should monitor for complications such as hepatic encephalopathy, bleeding disorders, and infections. They should assess for signs of hepatic coma, altered mental status, or bleeding, and intervene promptly if complications arise.
- Education and support: Nurses play a crucial role in educating patients and their families about the causes of jaundice, treatment options, and strategies to manage symptoms at home. They should provide information about medications, dietary modifications, and signs of complications, as well as offer emotional support and encouragement.
- Collaboration with the healthcare team: Nurses should collaborate with physicians, pharmacists, dietitians, and other healthcare professionals to develop and implement a comprehensive care plan for patients with jaundice. They should communicate effectively and advocate for the patient’s needs to ensure optimal outcomes.
2 .Short answers: (any three) 3×5=15
(A) Diagnostic test of diabetes mellitus
The diagnosis of diabetes mellitus typically involves several tests to measure blood glucose levels. Here’s a detailed overview:
- Fasting Plasma Glucose (FPG) Test: This test measures blood glucose levels after an overnight fast (8-12 hours). A level of 126 mg/dL (7.0 mmol/L) or higher on two separate tests indicates diabetes.
- Oral Glucose Tolerance Test (OGTT): After an overnight fast, a person drinks a sugary solution, and blood glucose levels are measured 2 hours later. A blood glucose level of 200 mg/dL (11.1 mmol/L) or higher indicates diabetes.
- Hemoglobin A1c (HbA1c) Test: This test measures the average blood glucose level over the past 2-3 months. A result of 6.5% or higher indicates diabetes.
- Random Plasma Glucose Test: This test measures blood glucose levels at any time of the day, regardless of when the person last ate. A blood glucose level of 200 mg/dL (11.1 mmol/L) or higher, along with symptoms of diabetes, indicates diabetes.
- Glycated Albumin (GA) Test:
This test measures the percentage of glycated albumin in the blood, which reflects average blood glucose levels over the previous 2-3 weeks.
- Fructosamine Test:
Similar to the glycated albumin test, this measures glycated serum proteins, providing an average glucose level over the previous 2-3 weeks.
- Continuous Glucose Monitoring (CGM):
This involves wearing a device that continuously measures glucose levels in interstitial fluid for several days, providing a detailed picture of glucose fluctuations throughout the day.
- Urine Tests:
While less common now, urine tests for glucose and ketones may also be used, although they are less reliable than blood tests.
(B) Care of orthopaedic patient with plaster caste

Caring for a patient with a plaster cast requires attention to several key areas:
- Positioning and Elevation: Ensure the limb with the cast is elevated to reduce swelling and promote circulation. Avoid placing pillows directly under the cast, as this can create pressure points.
- Skin Care: Regularly inspect the skin around the cast for signs of irritation, redness, or pressure sores. Keep the skin clean and dry, but avoid getting the cast wet.
- Mobility and Exercises: Encourage gentle movement of unaffected joints to prevent stiffness and muscle atrophy. However, advise against putting weight or pressure on the casted limb.
- Pain Management: Monitor the patient for any signs of discomfort or pain, and provide appropriate pain relief medication as prescribed by the doctor.
- Nutrition: Ensure the patient maintains a healthy diet to support healing and prevent complications. Adequate protein intake is particularly important for tissue repair.
- Hygiene: Advise the patient to keep the cast dry and clean. If the cast gets wet, it should be dried thoroughly to prevent skin irritation and infection.
- Monitoring: Regularly assess the neurovascular status of the limb by checking for changes in sensation, color, temperature, and pulse. Any significant changes should be reported to the healthcare provider immediately.
- Follow-up Appointments: Ensure the patient attends scheduled follow-up appointments with the orthopedic surgeon for cast checks and possible adjustments.
- Education: Provide the patient and their caregivers with thorough instructions on cast care, warning signs of complications, and when to seek medical attention.
- Emotional Support: Having a cast can be frustrating and limiting for patients, so offer encouragement and support to help them cope with the challenges of immobilization.
(c) Peritonitis
Definition
Peritonitis is inflammation of the peritoneum, the membrane lining the inner wall of the abdomen and covering the abdominal organs.
👉 Causes
It’s usually caused by infection, commonly bacterial or fungal, resulting from a perforation or rupture in the abdomen.
◾ Causes include
appendicitis,
perforated ulcers,
abdominal trauma,
pancreatitis, and infections spreading from other organs.
👉Signs and symptoms of peritonitis include ..
severe abdominal pain that worsens with movement or touch,
abdominal tenderness,
bloating,
fever,
chills,
nausea,
vomiting,
and decreased appetite.
In severe cases, symptoms may progress to shock and altered mental status.
👉 Nursing management of peritonitis involves:
- Assessment: Nurses monitor vital signs, assess abdominal pain, and observe for signs of infection and complications.
- Pain management: Administering pain medication to alleviate discomfort and promote patient comfort.
- Fluid and electrolyte balance: Monitoring fluid intake and output, administering intravenous fluids, and monitoring electrolyte levels to maintain hydration and electrolyte balance.
- Antibiotic therapy: Administering antibiotics as prescribed to treat the underlying infection.
- Surgical intervention: Assisting with preoperative and postoperative care for patients undergoing surgery to repair the underlying cause of peritonitis, such as perforated organs or abscess drainage.
- Wound care: Providing wound care for surgical incisions and monitoring for signs of infection.
- Nutritional support: Providing nutritional support through enteral or parenteral nutrition as needed to support healing and recovery.
- Education: Educating the patient and family about the condition, treatment plan, signs of complications, and strategies for preventing recurrence.
(D) Infertility
Definition of infertility
Infertility is defined as the inability to achieve pregnancy after a year of regular, unprotected intercourse. It can also refer to the inability to carry a pregnancy to term.
👉Types
Infertility can be categorized into primary and secondary types.
- Primary infertility: Couples who have never been able to conceive despite regular, unprotected intercourse.
- Secondary infertility: Couples who have previously conceived but are unable to do so again, either with the same partner or a new one.
👉 Causes
The causes of infertility can vary widely and may affect one or both partners. Some common causes include:
- Ovulation disorders: Irregular or absent ovulation can make conception difficult.
- Sperm issues: Low sperm count, poor sperm motility, or abnormal sperm shape can hinder fertilization.
- Fallopian tube damage or blockage: Conditions such as pelvic inflammatory disease or endometriosis can damage the fallopian tubes, preventing the egg from meeting the sperm.
- Uterine or cervical abnormalities: Structural issues in the uterus or cervix can make it difficult for fertilization or implantation to occur.
- Age: As women age, their fertility declines due to a decrease in the quantity and quality of eggs.
- Endocrine disorders: Hormonal imbalances, such as polycystic ovary syndrome (PCOS) or thyroid disorders, can affect ovulation and fertility.
- Lifestyle factors: Factors such as obesity, excessive alcohol consumption, smoking, and drug use can impact fertility in both men and women.
- Genetic factors: Certain genetic conditions can affect reproductive health and fertility.
👉Diagnosis and treatment
Diagnosis of infertility typically involves a series of tests and evaluations for both partners to identify any underlying causes. Some common diagnostic methods include:
- Medical history: Understanding the couple’s medical history, including previous pregnancies and any past reproductive issues.
- Physical examination: Examination of both partners to check for any physical abnormalities that may affect fertility.
- Ovulation testing: Monitoring hormone levels and ovulation patterns in the female partner through blood tests and ultrasound.
- Semen analysis: Evaluating the quality and quantity of sperm in the male partner’s semen sample.
- Imaging tests: Such as hysterosalpingography (HSG) or transvaginal ultrasound to assess the condition of the uterus and fallopian tubes.
- Additional tests: Depending on the suspected cause, further tests such as genetic testing, laparoscopy, or endometrial biopsy may be recommended.
Once a diagnosis is made, treatment options can be explored. Treatment for infertility depends on the underlying cause and may include:
- Medications: Hormonal medications to stimulate ovulation in women or improve sperm production and quality in men.
- Surgery: To correct structural issues such as blocked fallopian tubes, uterine abnormalities, or varicoceles (enlarged veins in the scrotum).
- Assisted reproductive technologies (ART): Including intrauterine insemination (IUI), in vitro fertilization (IVF), intracytoplasmic sperm injection (ICSI), and donor egg or sperm.
- Lifestyle changes: Such as maintaining a healthy weight, quitting smoking, reducing alcohol consumption, and managing stress.
- Counseling: Emotional support and counseling may be beneficial for couples coping with infertility.
(e) Acni vulgaris

Definition of acni vulgaris
Acne vulgaris is a common skin condition characterized by the presence of comedones (blackheads and whiteheads), papules, pustules, nodules, and/or cysts. It typically affects areas of the skin with a high density of sebaceous glands, such as the face, chest, and back.
👉 Pathophysiology
Acne vulgaris occurs due to a combination of factors, including:
- Excess Sebum Production: Sebaceous glands produce an excessive amount of oil (sebum), which can clog hair follicles and contribute to acne formation.
- Abnormal Follicular Keratinization: Normal shedding of dead skin cells becomes disrupted, leading to the accumulation of cells within the hair follicles and the formation of comedones.
- Proliferation of Propionibacterium acnes (P. acnes): This bacterium is part of the normal skin flora, but in acne, it proliferates within clogged follicles, leading to inflammation and the formation of papules and pustules.
- Inflammation: The presence of P. acnes and the release of inflammatory mediators trigger an immune response, leading to redness, swelling, and the formation of inflammatory acne lesions like papules, pustules, nodules, and cysts.
- Genetic Factors: Genetics play a role in determining an individual’s susceptibility to acne.
- Hormonal Influences: Androgens, particularly testosterone, can stimulate sebum production, making acne more common during puberty, menstruation, pregnancy, and conditions like polycystic ovary syndrome (PCOS).
- Environmental Factors: Factors such as diet, stress, and exposure to certain chemicals or medications can also influence acne development, though their exact roles are still being researched.
👉 Symptoms
The symptoms of acne vulgaris can vary in severity and may include:
- Comedones: Open comedones (blackheads) and closed comedones (whiteheads) are non-inflammatory acne lesions caused by blocked hair follicles.
- Papules: Small, raised bumps that may be red and tender to the touch.
- Pustules: Similar to papules but with a white or yellow center filled with pus.
- Nodules: Large, painful, solid lumps beneath the surface of the skin caused by deep inflammation.
- Cysts: Painful, pus-filled lesions deep within the skin, often larger than nodules and prone to scarring.
- Redness and Inflammation: The affected areas of the skin may appear red, swollen, and inflamed due to the body’s immune response to bacteria and blocked follicles.
- Scarring: Severe acne lesions, particularly nodules and cysts, can lead to scarring as the skin attempts to heal.
- Hyperpigmentation: Dark spots or patches of skin discoloration may occur as a result of inflammation or post-inflammatory changes.
👉 Causes
Acne vulgaris can be caused by a variety of factors, including:
- Hormonal Changes: Fluctuations in hormone levels, particularly during puberty, menstruation, pregnancy, and conditions like polycystic ovary syndrome (PCOS), can lead to increased sebum production and acne.
- Genetics: A family history of acne can increase the likelihood of developing the condition. Certain genetic factors can influence sebum production, follicular keratinization, and inflammatory responses in the skin.
- Excessive Sebum Production: Overproduction of oil by the sebaceous glands can lead to clogged pores and acne formation.
- Bacterial Infection: Propionibacterium acnes (P. acnes), a type of bacteria that normally resides on the skin, can proliferate within clogged hair follicles and contribute to inflammation and acne lesions.
- Follicular Hyperkeratosis: Abnormal shedding of skin cells within hair follicles can lead to the formation of comedones (blackheads and whiteheads).
- Inflammation: Inflammatory responses triggered by factors such as bacterial infection, hormonal changes, and immune system reactions can lead to redness, swelling, and the formation of inflammatory acne lesions.
- Dietary Factors: While the role of diet in acne is still debated, some studies suggest that certain dietary components, such as high glycemic index foods and dairy products, may exacerbate acne in some individuals.
- Stress: Psychological stress can exacerbate acne by increasing inflammation and hormone levels, though it’s not a direct cause.
- Environmental Factors: Exposure to pollutants, harsh chemicals, and certain medications may contribute to acne development or exacerbation in some individuals.
Understanding these factors can help in managing and treating acne effectively.
👉 Treatment
Treatment for acne vulgaris typically involves a combination of topical medications, oral medications, and skincare practices. Here are some common treatments:
Topical Treatments:
- Benzoyl Peroxide: Kills bacteria, reduces inflammation, and helps to unclog pores.
- Topical Retinoids: Derived from vitamin A, these medications promote cell turnover, prevent clogged pores, and reduce inflammation.
- Topical Antibiotics: Help reduce P. acnes bacteria on the skin and decrease inflammation.
- Azelaic Acid: Helps to unclog pores, reduce inflammation, and inhibit the growth of P. acnes bacteria.
Oral Medications:
- Oral Antibiotics: Used for moderate to severe acne to reduce P. acnes bacteria and inflammation.
- Oral Contraceptives (for females): Can help regulate hormonal fluctuations that contribute to acne.
- Isotretinoin (Accutane): Reserved for severe, treatment-resistant acne, isotretinoin reduces sebum production, prevents acne formation, and has long-lasting effects.
Other Treatments:
- Chemical Peels: Help to exfoliate the skin and unclog pores, reducing the appearance of acne lesions.
- Laser and Light Therapies: Can target P. acnes bacteria and reduce inflammation.
- Extraction: Manual removal of comedones and other acne lesions by a dermatologist.
- Intralesional Corticosteroid Injections: Used for treating severe nodular or cystic acne lesions.
- Skincare Practices:
- Gentle Cleansing: Washing the face twice daily with a mild cleanser to remove excess oil, dirt, and bacteria without stripping the skin.
- Non-comedogenic Products: Using skincare and makeup products labeled as non-comedogenic to avoid clogging pores.
- Sun Protection: Using oil-free, non-comedogenic sunscreen to protect the skin from sun damage without exacerbating acne.
3.Very short essays: (any four) 4×2=8
(a) Digoxin toxicity
Digoxin toxicity
It is eliminated primarily through kidneys; therefore, it has a half-life of 36-48 hours in patients who have normal kidney function and 3.5-5 days in patients who are anuric. Therapeutic levels of digoxin are 0.8-2.0 ng/mL. The toxic level is >2.4 ng/mL
The lethal dose of digoxin is considered to be 20-50 times the maintenance dose taken at once. In healthy adults, a dose of less than 5 mg seldom causes severe toxicity, but a dose of more than 10 mg is almost always fatal
👉Digoxin toxicity occurs when the levels of digoxin, a medication used to treat heart conditions like heart failure and certain arrhythmias, become too high in the bloodstream.
👉 Symptoms of digoxin toxicity can vary and may include:
- Nausea and vomiting:
◾ Digestive disturbances are common early symptoms of digoxin toxicity.
- Loss of appetite:
◾ Decreased appetite or aversion to food may occur.
- Blurred vision or visual disturbances:
◾Digoxin toxicity can affect vision, causing blurriness, changes in color perception, or seeing halos around lights.
- Confusion or disorientation:
◾ Cognitive symptoms such as confusion, disorientation, or difficulty concentrating may develop.
- Fatigue:
◾Increased tiredness or weakness beyond what is typical for the individual.
- Headaches:
◾Persistent or severe headaches may occur
(b) Otalgia
Otalgia
👉Otalgia is a medical term used to describe ear pain.
◾ It can result from various causes, including infections, inflammation, trauma, or referred pain from nearby structures like the throat or teeth.
◾ Common causes include otitis media (middle ear infection), otitis externa (swimmer’s ear), temporomandibular joint (TMJ) disorders, dental issues, or even sinus infections.
◾ Proper diagnosis by a healthcare professional is essential to determine the underlying cause and appropriate treatment.
(c) Sickle cell disease
sickle cell
👉Sickle cell disease is a genetic disorder where red blood cells become rigid and sticky, taking on a crescent shape (sickle) instead of their usual round shape.
◾This can cause various complications, including pain, anemia, and organ damage.
Symptoms:
- Pain:
◾ Episodes of pain, often called crises, can occur when sickle-shaped red blood cells block blood flow and oxygen to tissues and organs.
- Anemia:
Sickle cells have a shorter lifespan than normal red blood cells, leading to a shortage of red blood cells and anemia.
- Organ damage:
◾Sickle cells can block blood flow to organs, leading to damage and complications such as stroke, acute chest syndrome, and organ failure.
👉Cause:
Sickle cell disease is caused by a mutation in the gene that tells your body to make hemoglobin, the red, iron-rich compound .
◾When oxygen levels are low, such as during physical exertion or stress, the abnormal hemoglobin S molecules can cause red blood cells to become rigid and form the characteristic sickle shape.
(d) Thrombophlebitis
Thrombophlebitis
👉Thrombophlebitis is the inflammation of a vein, usually in the legs, caused by a blood clot.
◾ It can result from factors like prolonged immobility, injury to the vein, or underlying medical conditions.
👉Symptoms:
◾Symptoms include pain, swelling, redness, and warmth along the affected vein.
👉Treatment:
◾Treatment typically involves medication to thin the blood and reduce inflammation, as well as measures to alleviate symptoms and prevent complications such as pulmonary embolism.
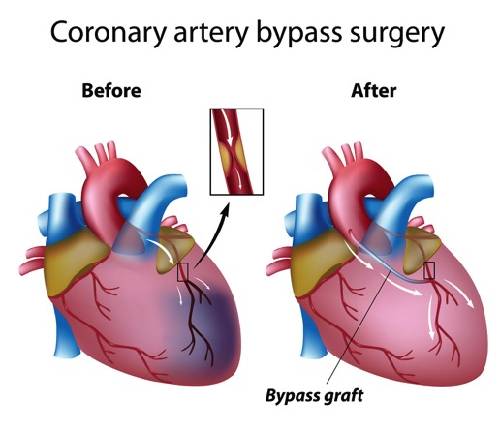
(e) CABG
CABG
👉 stands for Coronary Artery Bypass Grafting, a surgical procedure to treat coronary artery disease.
◾ It involves taking a healthy blood vessel from elsewhere in the body and grafting it onto the coronary arteries to bypass blockages.
◾This restores blood flow to the heart muscle, relieving symptoms like chest pain and reducing the risk of heart attack.
◾ It’s typically done when other treatments, like medication or angioplasty, aren’t sufficient.
◾The surgery can be performed using different techniques, including traditional open-heart surgery or minimally invasive approaches.
SECTION -II
1 .Long essay: (any one) 1X10=10
(a) Define the breast tumor. 02
Breast tumors
👉 Breast tumors are abnormal growths of cells within the breast tissue.
◾ They can be benign (non-cancerous) or malignant (cancerous).
◾ Benign tumors are usually harmless and do not spread to other parts of the body, while malignant tumors can invade nearby tissues and metastasize to other organs.
◾ Common types of breast tumors include fibroadenomas, cysts, ductal carcinoma in situ (DCIS), invasive ductal carcinoma (IDC), and invasive lobular carcinoma (ILC). Diagnosis typically involves imaging tests like mammograms and biopsies.
◾ Treatment options depend on the type, size, and stage of the tumor and may include surgery, chemotherapy, radiation therapy, hormone therapy, or targeted therapy.
(B) Explain briefly the diagnostic test of breast tumor. 03
Diagnostic tests for breast tumors typically include:
- Mammogram: X-ray imaging of the breast used to detect abnormalities like lumps or masses.
- Ultrasound: Sound waves create images of the breast tissue to further evaluate abnormalities found on a mammogram or to differentiate between solid masses and fluid-filled cysts.
- MRI (Magnetic Resonance Imaging): Uses magnetic fields and radio waves to produce detailed images of the breast, often used in combination with mammography for high-risk patients or to further evaluate abnormalities.
- Biopsy: Removal of a sample of breast tissue for examination under a microscope to determine if cancer is present and, if so, what type it is (e.g., benign or malignant).
- Breast MRI-guided biopsy: Similar to a standard biopsy but guided by MRI imaging for targeting specific areas of concern identified on breast MRI scans.
(c) Explain the postoperative care of women with mastectomy. 05
Postoperative care following a mastectomy involves several aspects to ensure proper healing and support for the patient:
- Wound Care:
◾Monitor the surgical incision site for any signs of infection, such as redness, swelling, or discharge. Follow the surgeon’s instructions regarding wound dressings, cleaning, and when to remove sutures or staples.
- Pain Management:
◾Administer pain medication as prescribed to alleviate discomfort. Ensure the patient understands how to use pain medication safely and is aware of any potential side effects.
- Drain Care:
◾ If surgical drains are placed during the mastectomy to remove excess fluid from the surgical site, educate the patient on how to care for them. This may include emptying and measuring the drainage, keeping the drains clean, and monitoring for signs of infection.
- Activity and Movement:
◾Encourage gentle movement and exercises to promote circulation and prevent stiffness, but advise against strenuous activities or heavy lifting for a certain period as per the surgeon’s instructions.
- Lymphedema Prevention:
◾Instruct the patient on techniques to reduce the risk of lymphedema, such as avoiding tight clothing or jewelry on the affected side, practicing gentle arm exercises, and being cautious with activities that may strain the arm or shoulder.
- Emotional Support:
◾Offer emotional support and counseling to address any concerns or anxieties the patient may have regarding body image, self-esteem, or coping with the diagnosis and treatment of breast cancer.
- Follow-up Appointments:
◾Schedule regular follow-up appointments with the surgeon and other members of the healthcare team to monitor healing progress, address any complications, and discuss long-term care and follow-up.
- Educational Resources:
◾ Provide educational resources and information about support groups, rehabilitation programs, and resources for breast cancer survivors to help the patient navigate life after mastectomy.
OR
(a) Define the heart failure. 02
Definition of health failure
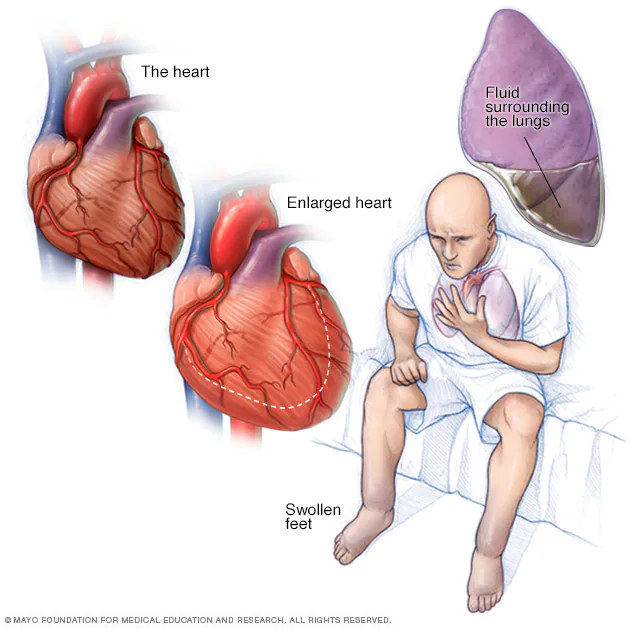
Heart failure occurs when the heart is unable to pump enough blood to meet the body’s needs. This can happen due to various reasons, including weakened heart muscles, heart valve problems, high blood pressure, or coronary artery disease. Symptoms can include shortness of breath, fatigue, swelling in the legs, and difficulty exercising. Treatment typically involves medications, lifestyle changes, and sometimes procedures or surgery.
b) Explain the pathophysiology of heart failure. 03
Pathophysiology
Heart failure can result from various underlying conditions that affect the heart’s ability to pump blood effectively.
◾Here’s a simplified explanation of the pathophysiology:
- Impaired Pumping Function:
The heart’s pumping ability weakens due to conditions such as coronary artery disease, hypertension, heart valve disorders, or damage from previous heart attacks. This leads to reduced cardiac output, the amount of blood pumped by the heart per minute.
- Compensatory Mechanisms:
The body attempts to compensate for the decreased cardiac output by activating several mechanisms:
- Neurohormonal Activation: The sympathetic nervous system and renin-angiotensin-aldosterone system are activated to increase heart rate and constrict blood vessels, maintaining blood pressure. However, over time, these mechanisms can worsen heart function.
- Ventricular Remodeling: The heart undergoes structural changes, such as enlargement of the chambers and thickening of the ventricular walls, in an attempt to improve pumping efficiency. However, this remodeling can ultimately weaken the heart muscle further.
- Decreased Tissue Perfusion: As cardiac output decreases, tissues and organs receive less oxygen and nutrients, leading to symptoms such as fatigue, shortness of breath, and fluid retention.
- Fluid Retention and Congestion: As the heart struggles to pump blood efficiently, fluid may accumulate in the lungs (pulmonary congestion) or in the peripheral tissues (peripheral edema), leading to symptoms such as shortness of breath and swelling.
- Progression:
Without effective treatment, heart failure typically worsens over time, leading to increasing symptoms and complications such as arrhythmias, kidney dysfunction, and eventually, multiorgan failure.
(c) Discuss the management of client with heart failure. 05
Management
The management of heart failure involves a combination of lifestyle modifications, medications, and sometimes medical procedures.
Lifestyle Modifications:
- Diet: Following a heart-healthy diet low in sodium and saturated fats can help manage fluid retention and reduce strain on the heart.
- Exercise: Regular physical activity, tailored to the individual’s capabilities, can improve heart function and overall health.
- Fluid Intake: Monitoring fluid intake, including limiting alcohol and caffeine consumption, helps prevent fluid overload.
- Smoking Cessation: Quitting smoking reduces cardiovascular risk and improves heart function.
Medications:
- Diuretics: These medications help reduce fluid buildup in the body, relieving symptoms such as shortness of breath and swelling.
- Angiotensin-Converting Enzyme (ACE) Inhibitors or Angiotensin II Receptor Blockers (ARBs): These drugs help relax blood vessels, lower blood pressure, and improve cardiac function.
- Beta-Blockers: Beta-blockers reduce heart rate, blood pressure, and the workload on the heart, improving symptoms and slowing disease progression.
- Aldosterone Antagonists: These medications can help reduce fluid retention and improve survival in certain patients with heart failure.
- Sacubitril/Valsartan: This medication is a combination of a neprilysin inhibitor and an ARB, which has been shown to reduce mortality and hospitalizations in patients with heart failure with reduced ejection fraction.
Medical Devices:
- Implantable Cardioverter-Defibrillator (ICD): For patients at high risk of life-threatening arrhythmias, an ICD can help restore normal heart rhythm.
- Cardiac Resynchronization Therapy (CRT): This therapy involves implanting a device that coordinates the contractions of the heart’s ventricles, improving cardiac function in certain patients with heart failure.
Surgical Interventions:
- Coronary Artery Bypass Grafting (CABG): For patients with severe coronary artery disease, CABG may improve blood flow to the heart muscle.
- Heart Valve Repair or Replacement: Repairing or replacing damaged heart valves can improve cardiac function and reduce symptoms.
Regular Monitoring and Follow-Up:
- Monitoring symptoms, fluid status, and cardiac function through regular check-ups and diagnostic tests helps adjust treatment as needed and prevent complications.
The nursing management of heart failure
Assessment and Monitoring:
- Conduct a thorough assessment of the patient’s cardiac status, including symptoms, vital signs, heart sounds, fluid balance, and oxygen saturation.
- Monitor for signs of worsening heart failure, such as increased dyspnea, orthopnea, paroxysmal nocturnal dyspnea, fatigue, edema, and weight gain.
- Assess for potential precipitating factors or exacerbating conditions, such as infections, arrhythmias, electrolyte imbalances, medication non-adherence, or dietary indiscretions.
Patient Education:
- Educate the patient and family members about heart failure, its causes, symptoms, and treatment options.
- Provide guidance on medication adherence, dietary modifications (e.g., sodium restriction), fluid management, and lifestyle modifications (e.g., smoking cessation, regular exercise).
- Teach patients to recognize and report signs and symptoms of worsening heart failure and when to seek medical attention.
Medication Management:
- Administer prescribed medications as ordered, including diuretics (e.g., furosemide), angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor blockers (ARBs), beta-blockers, and mineralocorticoid receptor antagonists (MRAs).
- Monitor the patient’s response to medications, assess for adverse effects, and adjust dosages as needed under the direction of the healthcare provider.
- Educate patients about the purpose, dosage, side effects, and importance of adherence to prescribed medications.
Fluid and Sodium Management:
- Monitor fluid intake and output, daily weights, and signs of fluid overload or dehydration.
- Encourage patients to adhere to fluid and sodium restrictions as prescribed to prevent fluid retention and exacerbation of heart failure symptoms.
- Educate patients about strategies to minimize fluid retention, such as elevating the legs, avoiding excessive salt intake, and limiting alcohol consumption.
Oxygen Therapy:
- Administer supplemental oxygen as prescribed to relieve dyspnea and improve oxygenation in patients with respiratory distress.
- Monitor oxygen saturation levels and respiratory status regularly to assess the effectiveness of oxygen therapy.
Symptom Management:
- Implement measures to relieve symptoms such as dyspnea, fatigue, and edema, including positioning (e.g., sitting upright), providing supplemental oxygen, and administering diuretics as prescribed.
- Assist patients with activities of daily living (ADLs) and provide support for symptom management and coping strategies.
Collaboration and Referral:
- Collaborate with other members of the healthcare team, including physicians, pharmacists, dietitians, and physical therapists, to optimize patient care and outcomes.
- Refer patients to cardiac rehabilitation programs, social services, or other support services as needed to address psychosocial, nutritional, or rehabilitation needs.
2.Short answers: (any three) 3×5=15
(a) Hiatal hernia

defination :
◾hiatal hernia occurs when part of the stomach pushes up through the diaphragm muscle into the chest cavity. This can cause acid reflux, heartburn, and other symptoms.
👉 Causes:
◾Hiatal hernias can be caused by various factors, including:
- Weakness in the diaphragm muscle.
- Increased pressure in the abdominal cavity due to pregnancy, obesity, coughing, or straining during bowel movements.
- Age-related changes in the diaphragm.
- Injury to the area.
◾These factors can contribute to the weakening or disruption of the diaphragm, allowing the stomach to protrude into the chest cavity.
👉Signs and symptoms of a hiatal hernia can vary but may include:
- Heartburn: A burning sensation in the chest or throat.
- Acid reflux: Regurgitation of stomach acid into the esophagus, causing a sour taste in the mouth or discomfort.
- Chest pain: Often mistaken for heart-related pain, but typically occurs after meals or when lying down.
- Difficulty swallowing: Due to the protrusion of the stomach into the chest cavity, it can affect the function of the esophagus.
- Belching or hiccups: Excessive belching or hiccups can occur, especially after eating.
- Feeling full quickly: A sensation of fullness even after consuming small amounts of food.
- Nausea or vomiting: Some individuals may experience nausea or vomiting, particularly if the hernia causes stomach contents to become trapped.
👉Nursing management for hiatal hernia typically involves:
- Education: Providing information about the condition, its causes, symptoms, and management options.
- Lifestyle modifications: Advising on dietary changes (such as avoiding spicy or acidic foods), weight management, and avoiding tight clothing.
- Medication administration: Administering medications as prescribed by a healthcare provider to reduce acid production or relieve symptoms.
- Positioning: Encouraging patients to sit upright during and after meals to reduce pressure on the stomach.
- Monitoring: Assessing symptoms and monitoring for any complications, such as gastrointestinal bleeding or obstruction.
- Referral: Referring patients to other healthcare providers for further evaluation or treatment if necessary, such as surgery for severe cases.
(B) Complications of fracture
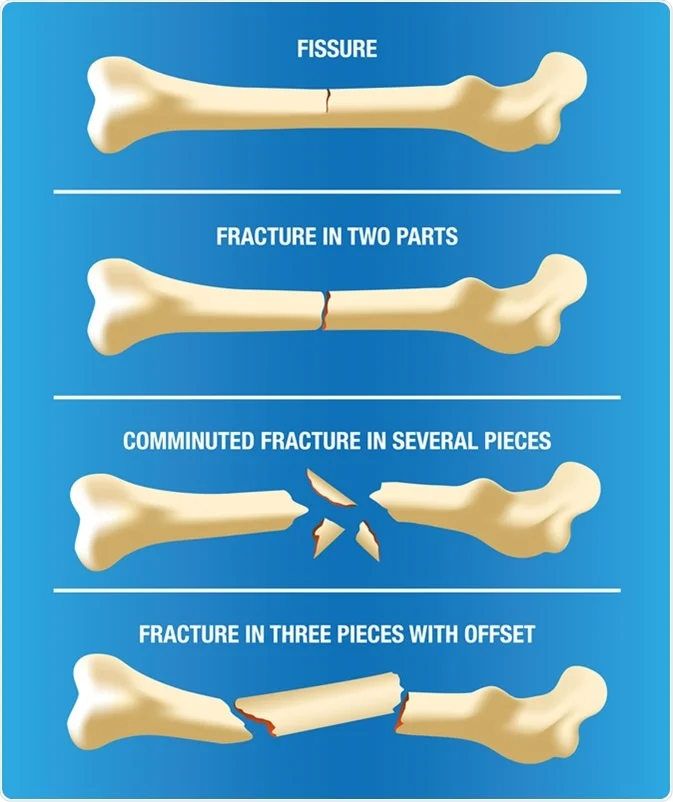
Fractures
◾Fractures can lead to various complications, including:
- Delayed Healing: ◾Fractures may take longer than expected to heal, especially in older adults or those with underlying health conditions like osteoporosis.
- Nonunion:
◾When bones fail to heal properly, resulting in a nonunion, where the bone ends do not reconnect.
- Malunion:
If the fractured bone heals in an incorrect position, it can lead to malunion, causing functional impairment or deformity.
- Infection:
Fractures can be an entry point for bacteria, leading to infections like osteomyelitis (bone infection) or cellulitis (soft tissue infection).
- Compartment Syndrome: Swelling or bleeding in the injured area can increase pressure within the muscles, nerves, and blood vessels, leading to compartment syndrome, which requires immediate medical attention to prevent tissue damage.
- Nerve or Blood Vessel Damage: Fractures may injure nearby nerves or blood vessels, causing numbness, tingling, weakness, or reduced blood flow to the affected area.
- Deep Vein Thrombosis (DVT): Immobility following a fracture can increase the risk of DVT, a blood clot in a deep vein, which can be life-threatening if it travels to the lungs (pulmonary embolism).
- Chronic Pain: Some fractures can lead to long-term or chronic pain, especially if nerves are damaged or if the fracture affects weight-bearing joints.
- Stiffness and Reduced Range of Motion: Immobilization during healing can lead to stiffness and reduced range of motion in nearby joints.
- Degenerative Joint Disease (Osteoarthritis): Fractures involving joints may increase the risk of developing osteoarthritis in the affected joint over time.
- Psychological Impact:
Fractures can impact a person’s mental health, causing anxiety, depression, or post-traumatic stress disorder (PTSD), especially if the injury is severe or if it results in long-term disability.
(C) Fluid calculation for burn injury
Fluid calculation
◾Calculating fluid requirements for burn injuries is crucial for managing patients to prevent hypovolemic shock and maintain tissue perfusion. Here’s a detailed approach:
- Assessment of Burn Severity: Determine the total body surface area (TBSA) affected by burns using the Rule of Nines or Lund and Browder chart. Assess the depth of burns (superficial, partial-thickness, or full-thickness) as it influences fluid loss.
- Parkland Formula:
The Parkland formula is commonly used for fluid resuscitation in burn patients within the first 24 hours:
- For adults: 4 mL/kg/%TBSA burn
- Half of the calculated volume is given in the first 8 hours post-burn, and the remaining half over the subsequent 16 hours.
- For example, for a 70 kg adult with 20% TBSA burns:
- (4 mL/kg × 70 kg × 20%) ÷ 2 = 2800 mL in the first 8 hours and 2800 mL in the next 16 hours.
- Fluid Choice: Use crystalloids such as lactated Ringer’s solution or normal saline for fluid resuscitation.
- Monitoring:
Continuously monitor vital signs, urine output, central venous pressure (if available), and serum electrolytes to adjust fluid therapy accordingly.
- Ongoing Fluid Replacement:
Beyond the initial 24 hours, adjust fluid therapy based on the patient’s urine output, vital signs, and clinical status. Typically, maintenance fluids are provided along with additional replacement for ongoing losses, estimated based on wound assessment and input-output monitoring.
- Compensating for Evaporation Losses:
Consider the insensible fluid losses due to evaporation, especially in extensive burns. These can be significant and may require additional fluid replacement.
- Considerations for Children: For pediatric patients, fluid calculation may vary. Use weight-based calculations and adjust according to age-specific considerations.
- Special Considerations:
Patients with inhalation injuries, pre-existing medical conditions, or concomitant trauma may require tailored fluid management.
- Preventing Fluid Overload: While ensuring adequate fluid resuscitation is essential, avoid overhydration, which can lead to complications such as pulmonary edema.
- Multidisciplinary Approach:
Burn management often involves a multidisciplinary team, including burn surgeons, intensivists, nurses, and nutritionists, to optimize patient care.
(d) Retinal detachment
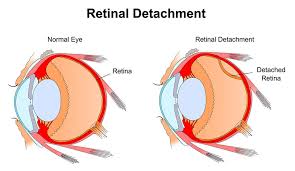
Retinal detachment
Retinal detachment is a serious eye condition where the retina—the layer of tissue at the back of the eye that detects light—is lifted or pulled from its normal position. This detachment can cause vision loss if not promptly treated.
◾There are three main types of retinal detachment:
◾ rhegmatogenous,
tractional,
exudative.
- Rhegmatogenous Retinal Detachment: This is the most common type and occurs when a tear or hole forms in the retina, allowing fluid to pass through and separate the retina from the underlying tissue. Risk factors include aging, previous eye surgery, and severe nearsightedness.
- Tractional Retinal Detachment: This occurs when scar tissue on the retina’s surface contracts and causes the retina to pull away from the underlying tissue. It is often associated with conditions like diabetic retinopathy.
- Exudative Retinal Detachment:
- Causes:
- Retinal detachment can occur due to several factors, including:
- Age-related changes, such as shrinkage of the vitreous gel inside the eye (vitreous detachment), which can pull on the retina.
- Trauma or injury to the eye.
- Conditions that increase the risk of retinal tears or breaks, such as severe nearsightedness (myopia), previous eye surgery, or family history of retinal detachment.
- Inflammatory eye diseases or tumors.
- Fluid accumulation underneath the retina (serous retinal detachment).
- Retinal detachment can occur due to several factors, including:
- Symptoms:
- The symptoms of retinal detachment may include:
- Sudden onset of floaters, which are dark spots or specks that appear to float in the field of vision.
- Flashes of light, described as seeing “lightning streaks” or “flashes of light” in the affected eye.
- A shadow or curtain-like effect in the peripheral vision, which may progress towards the center of vision if left untreated.
- Blurred or distorted vision.
- Loss of peripheral or central vision, depending on the extent and location of the retinal detachment.
- The symptoms of retinal detachment may include:
- Diagnosis:
- Diagnosis of retinal detachment typically involves a comprehensive eye examination by an ophthalmologist. This may include:
- Visual acuity testing.
- Dilated eye examination to evaluate the retina and vitreous.
- Imaging tests such as ultrasound or optical coherence tomography (OCT) to assess the extent and location of the detachment.
- Diagnosis of retinal detachment typically involves a comprehensive eye examination by an ophthalmologist. This may include:
- Treatment:
- The treatment for retinal detachment depends on the severity and type of detachment, as well as other factors such as the patient’s overall health and visual acuity. Options may include:
- Retinal detachment repair surgery, which may involve techniques such as scleral buckling, pneumatic retinopexy, vitrectomy, or laser photocoagulation to reattach the retina and seal retinal tears.
- In some cases, if the detachment is detected early and is small, the ophthalmologist may monitor the condition closely without immediate intervention, especially if the detachment is caused by a small retinal tear that has not yet progressed.
- The treatment for retinal detachment depends on the severity and type of detachment, as well as other factors such as the patient’s overall health and visual acuity. Options may include:
- Prognosis:
- The prognosis for retinal detachment depends on various factors, including the extent and location of the detachment, the promptness of treatment, and the underlying health of the eye. In many cases, early diagnosis and appropriate treatment can lead to successful reattachment of the retina and preservation of vision. However, if left untreated or if the detachment involves the macula (the central part of the retina responsible for sharp, central vision), permanent vision loss may occur.
(e) Meningitis.
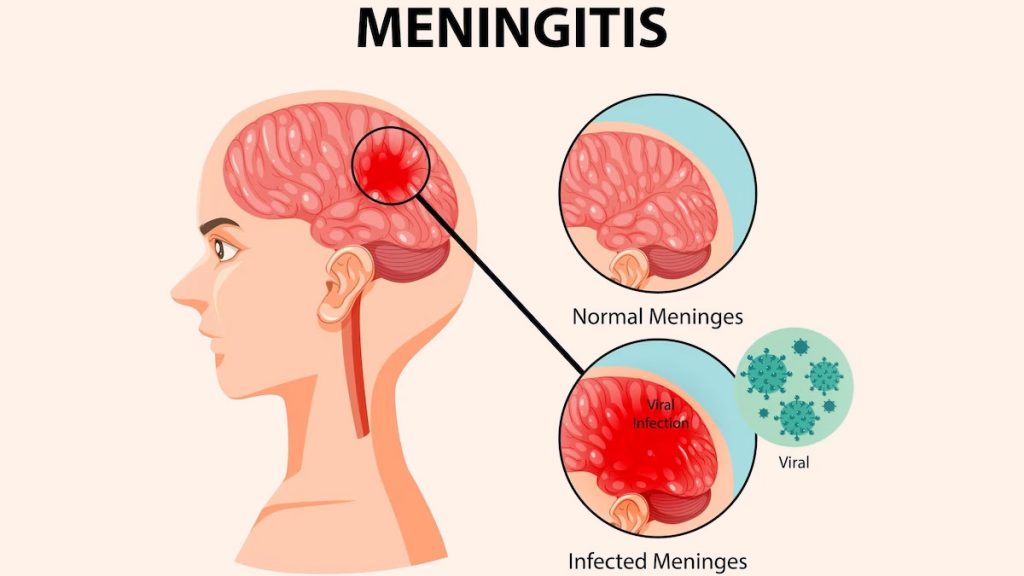
defination:
◾Meningitis is an inflammation of the protective membranes covering the brain and spinal cord known as the meninges. It’s typically caused by an infection, often bacterial or viral, and can lead to serious complications if not treated promptly. Symptoms may include headache, fever, stiff neck, and sensitivity to light.
👉causes:
◾Meningitis can be caused by various factors, primarily infections.
◾ The most common causes are bacteria and viruses, but fungi, parasites, and even non-infectious factors like certain medications or autoimmune disorders can also trigger meningitis.
◾ Bacterial meningitis is often more severe and requires immediate medical attention, while viral meningitis tends to be less severe and often resolves on its own.
👉The signs and symptoms :
- Sudden high fever
- Severe headache
- Stiff neck
- Nausea and vomiting
- Sensitivity to light (photophobia)
- Confusion or difficulty concentrating
- Sleepiness or difficulty waking up
- Seizures
- Skin rash (especially in meningococcal meningitis)
- In infants, symptoms may include irritability, poor feeding, and a bulging fontanelle (soft spot on the head).
👉The nursing management of meningitis involves various aspects of care, including:
- Assessment: Regular assessment of the patient’s vital signs, neurological status, and symptoms to monitor for any changes or complications.
- Monitoring: Continuous monitoring of fluid intake and output, neurological signs, and response to treatment.
- Isolation precautions: Depending on the cause of meningitis, appropriate isolation precautions may be necessary to prevent the spread of infection to others.
- Medication administration: Administering antibiotics or antiviral medications as prescribed by the healthcare provider to treat the underlying infection.
- Comfort measures: Providing comfort measures such as pain management, maintaining a quiet and dimly lit environment, and assisting with repositioning to reduce discomfort.
- Fluid management: Ensuring adequate hydration through intravenous fluids and monitoring for signs of dehydration or fluid overload.
- Education: Providing education to the patient and their family about the signs and symptoms of meningitis, the importance of completing the full course of medication, and any necessary follow-up care.
- Preventing complications: Taking measures to prevent complications such as seizures, increased intracranial pressure, and shock through appropriate interventions and monitoring.
- Support: Providing emotional support to the patient and their family during the stressful period of illness and recovery.
- Collaboration: Collaborating with other members of the healthcare team, including physicians, pharmacists, and other specialists, to ensure comprehensive care for the patient.
3 .Very short essay : 6X2=12
(A) Four opportunistic infections of AIDS
our common opportunistic infections associated with AIDS include:
- Pneumocystis pneumonia (PCP): A fungal infection of the lungs.
- Candidiasis: A fungal infection that can affect the mouth, throat, and genitals.
- Tuberculosis (TB): A bacterial infection that primarily affects the lungs but can spread to other parts of the body.
- Toxoplasmosis: A parasitic infection that can affect the brain and other organs.
(B) Renal biopsy
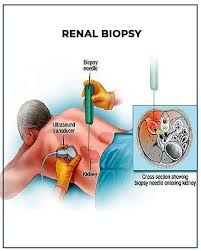
Renal biopsy:
◾A renal biopsy is a medical procedure where a small piece of kidney tissue is removed for examination under a microscope. It’s typically done to diagnose the cause of kidney disease.
👉 Here’s an overview of the process:
- Preparation:
Before the biopsy, your doctor will review your medical history and may perform blood tests to assess your kidney function and clotting ability.
- Procedure: During the biopsy, you’ll lie on your stomach or side on an examination table. The area over your kidney is numbed with a local anesthetic. Using imaging guidance, such as ultrasound or CT scan, a thin biopsy needle is inserted through your skin and into the kidney to obtain a small tissue sample.
- Aftercare: After the biopsy, you’ll need to lie still for several hours to minimize the risk of bleeding. You may need to stay in the hospital overnight for observation, especially if you’re at higher risk of complications. Your doctor will monitor you closely for signs of bleeding or other complications.
- Results: The tissue sample is sent to a laboratory for analysis. It may take a few days to receive the results. Your doctor will discuss the findings with you and develop a treatment plan based on the diagnosis.
(C) Four Emergency drugs used in OT
Emergency drugs commonly used in operating theaters (OT) include:
- Epinephrine: Used to treat severe allergic reactions (anaphylaxis), cardiac arrest, and certain types of shock.
- Atropine: Administered to treat bradycardia (slow heart rate), asystole (absence of cardiac activity), and to decrease salivation during surgery.
- Adenosine: Used to treat certain types of abnormal heart rhythms, such as supraventricular tachycardia.
- Lidocaine: Administered for local anesthesia and for the treatment of certain types of irregular heartbeats (arrhythmias).
(d) Lumbar puncture

Lumbar puncture
◾A lumbar puncture, also known as a spinal tap, is a medical procedure where a thin needle is inserted into the lower part of the spinal column to collect cerebrospinal fluid (CSF).
◾CSF surrounds the brain and spinal cord, and analyzing it can help diagnose various conditions such as infections, bleeding, or neurological disorders.
◾The procedure is typically performed with the patient lying on their side with knees drawn up to the chest to open up the spinal column.
◾After sterilizing the area and numbing it with a local anesthetic, the needle is carefully inserted between two lumbar vertebrae to access the spinal canal without damaging the spinal cord.
◾The collected CSF is then sent to a laboratory for analysis.
◾Lumbar punctures are commonly used in diagnosing conditions like meningitis, encephalitis, multiple sclerosis, and certain cancers affecting the central nervous system.
◾While generally safe, complications can occur, including headache, bleeding, infection, or nerve damage. Therefore, it’s crucial for the procedure to be performed by trained medical professionals in a controlled environment.
(e) Four functions of nurse in the OPD
n an outpatient department (OPD), nurses typically perform various functions including:
- Assessment and Triage: Nurses assess patients’ conditions, prioritize their needs, and determine the urgency of care required.
- Patient Education: They educate patients about their conditions, treatment plans, medications, and self-care techniques to promote better health outcomes.
- Administering Treatments: Nurses administer medications, injections, vaccinations, and other treatments as prescribed by physicians.
- Monitoring and Follow-up: They monitor patients’ vital signs, observe for any changes in condition, and provide follow-up care or referrals as needed.
(f) Four problems related to old age.
Here are four common issues related to old age:
- Health Concerns: As people age, they often face increased risks of various health issues such as chronic diseases, mobility problems, cognitive decline, and sensory impairments.
- Social Isolation: Older adults may experience social isolation due to factors like retirement, loss of friends and family members, limited mobility, or living alone, which can lead to loneliness and depression.
- Financial Insecurity: Many seniors encounter financial challenges, including insufficient retirement savings, rising healthcare costs, and difficulty managing expenses on a fixed income.
- Elder Abuse: Unfortunately, some older adults face abuse, neglect, or exploitation, whether physically, emotionally, financially, or through neglect, often at the hands of caregivers or family members.